Embed Size (px)
Citation preview
Heart Disease in Pregnancy
Dr Laurence O’Toole MD FRCP
Consultant Cardiologist
Sheffield Teaching Hospitals NHS FT
Royal College of Physicians Regional Update Tankersley Manor
22nd May 2017
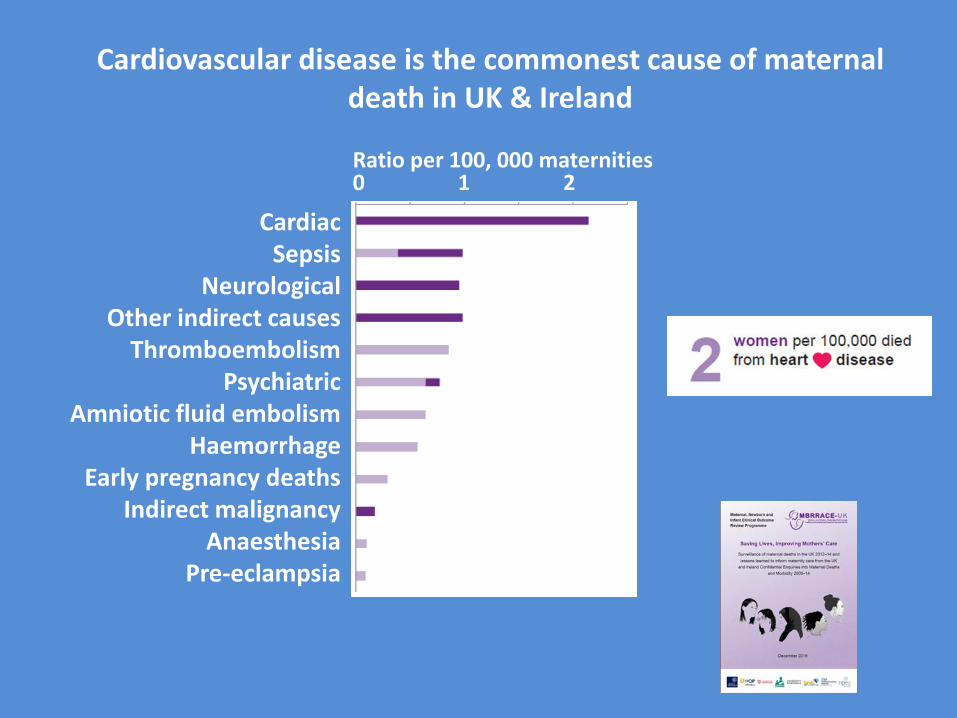
Cardiac Sepsis
Neurological Other indirect causes
Thromboembolism Psychiatric
Amniotic fluid embolism Haemorrhage
Early pregnancy deaths Indirect malignancy
Anaesthesia Pre-eclampsia
0 1 2 Ratio per 100, 000 maternities
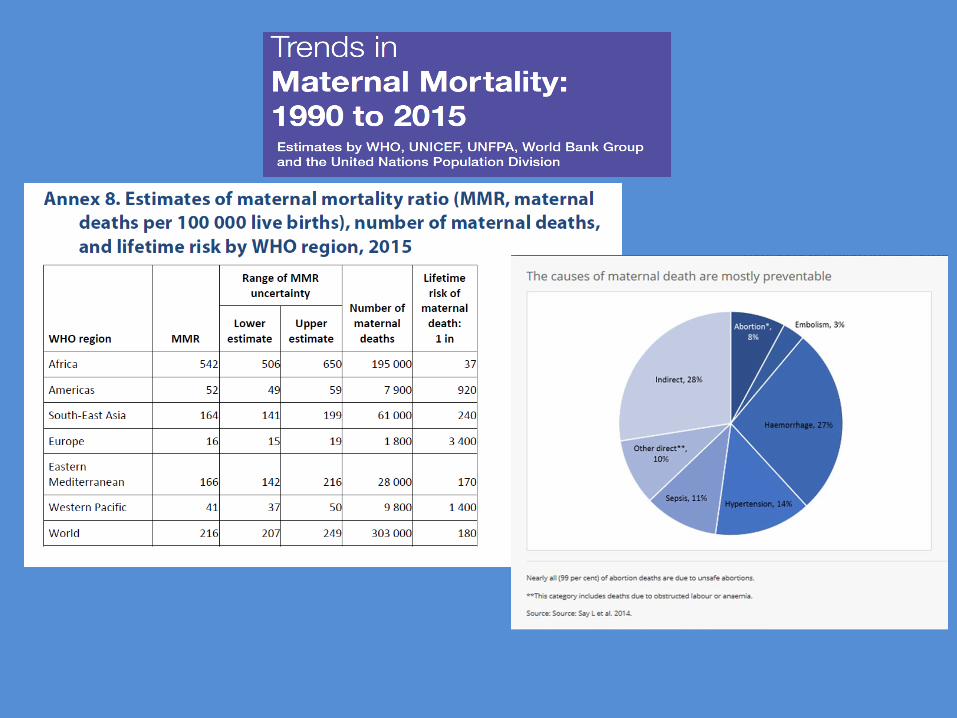
Cardiovascular disease is the commonest cause of maternal death in UK & Ireland
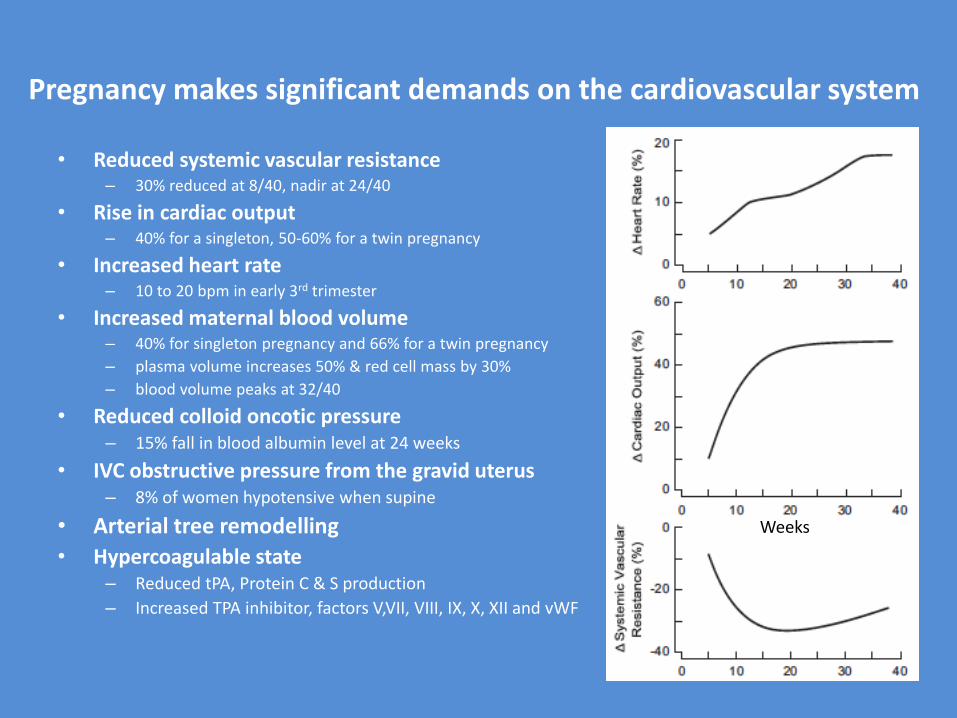
Pregnancy makes significant demands on the cardiovascular system
• Reduced systemic vascular resistance – 30% reduced at 8/40, nadir at 24/40
• Rise in cardiac output – 40% for a singleton, 50-60% for a twin pregnancy
• Increased heart rate – 10 to 20 bpm in early 3rd trimester
• Increased maternal blood volume – 40% for singleton pregnancy and 66% for a twin pregnancy
– plasma volume increases 50% & red cell mass by 30%
– blood volume peaks at 32/40
• Reduced colloid oncotic pressure – 15% fall in blood albumin level at 24 weeks
• IVC obstructive pressure from the gravid uterus – 8% of women hypotensive when supine
• Arterial tree remodelling
• Hypercoagulable state – Reduced tPA, Protein C & S production
– Increased TPA inhibitor, factors V,VII, VIII, IX, X, XII and vWF
Weeks
Labour and delivery make very significant demands on the cardiovascular system
• Labour increases CO by a further 10-30% in 1st stage and 50% in 2nd stage – 500ml auto transfusion which each uterine contraction
– Sympathetic stimulation from pain & anxiety
• Post-delivery there is a marked increase in CO (80% in first hour)
– Uterine involution
– Relief of aorto-caval compression
• It takes 6 months for restoration of normal physiology
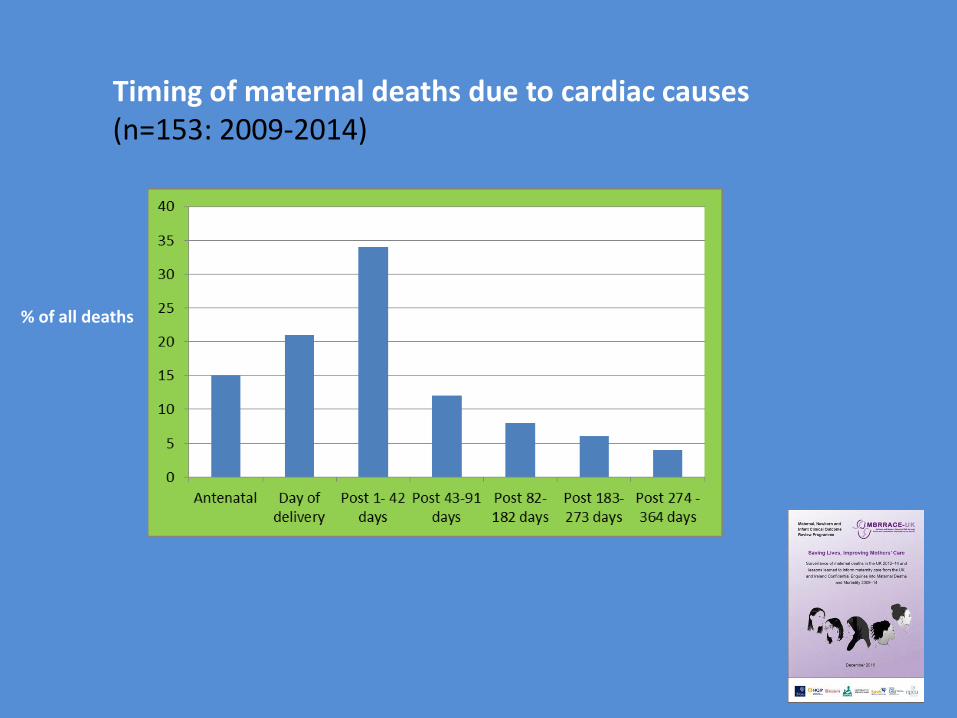
Timing of maternal deaths due to cardiac causes (n=153: 2009-2014)
% of all deaths
Who can’t tolerate a pregnancy?
Fixed Cardiac Output
Susceptible Vasculature
Who can’t tolerate a pregnancy?
Fixed Cardiac Output
Severe systemic ventricular dysfunction (LVEF <30%)
Pulmonary arterial hypertension
Obstructive symptomatic left heart lesion (e.g. AS or mitral stenosis)
Susceptible Vasculature
Marfan ascending aorta over 45mm diameter
Bicuspid aortic valve over 50mm diameter
Native severe aortic coarctation
WHO Class IV risk
Who probably can’t tolerate a pregnancy?
Fixed Cardiac Output
Systemic right ventricle
Fontan circulation
Cyanotic heart disease
Other complex congenital heart disease
LVEF 30-40%
Asymptomatic severe aortic stenosis
Susceptible Vasculature
Aortic dilatation: 40–45 mm in Marfan syndrome
45–50 mm in BAV aortopathy
Mechanical valve
WHO Class III risk
Which groups of woman are at risk?
Complex Adult Congenital Heart Disease
Prosthetic Mechanical Heart Valves
Personal or family history of cardiomyopathy or aortopathy
Survivors of childhood cancers (the ‘late effects’ group)
Immigrants from areas with high prevalence of rheumatic fever
IVF pregnancies – Health Tourists
Past cardiac ischaemic events or multiple risk factors for such
General principles of management of pregnancy in women with heart disease: (1)
• Ideally all women with congenital or acquired heart disease should receive multi-disciplinary preconception counselling before pregnancy
• Guidance must be given early.
“A teenager with a late repair of a VSD and persisting pulmonary hypertension died three days after delivery….despite full ITU support. It is unclear if she received pregnancy or contraceptive counseling from paediatric cardiology services. She was referred to the adult congenital heart disease clinic when she found herself pregnant and elected to continue the pregnancy. With increasing symptoms, she was delivered at 34/40.”
General principles of management of pregnancy in women with heart disease: (2)
• Early review and risk assessment by a MDT (obstetricians, anaesthetists & cardiologists) required.
• Optimise mother’s CV status during pregnancy
• Monitor for deterioration
• Address foetal issues
• Develop a clear, well documented and widely distributed plan for labour and the puerperium
General principles of management of pregnancy in women with heart disease: (3)
• Mode of delivery? – ‘Spontaneous vaginal delivery with low-dose regional anaesthesia and
careful fluid management preferred in most cases’
– But the C/section rate in women with significant heart disease is high
• Induction may be appropriate • (eg optimisation of timing of delivery in relation to anticoagulation or
availability of specific medical staff or for deteriorating maternal function
• Effective pain relief important – Reduces rise in CO from pain and anxiety
– Low-dose regional anaesthesia
• Limit maternal effort – The managed second stage • Assisted delivery (Ventouse/Forceps)
General principles of management of pregnancy in women with heart disease: (4)
• Place of delivery – ?is a cardiac theatre appropriate
• Post labour HDU/ICU/CCU • usually 24 to 48 hours
• Senior post-partum obstetric and cardiology review important
• Early cardiology follow up
• Early discussion about risks of future pregnancy & robust contraception
The majority of pregnant women who die of a cardiovascular disease have not been identified as being ‘at risk’.
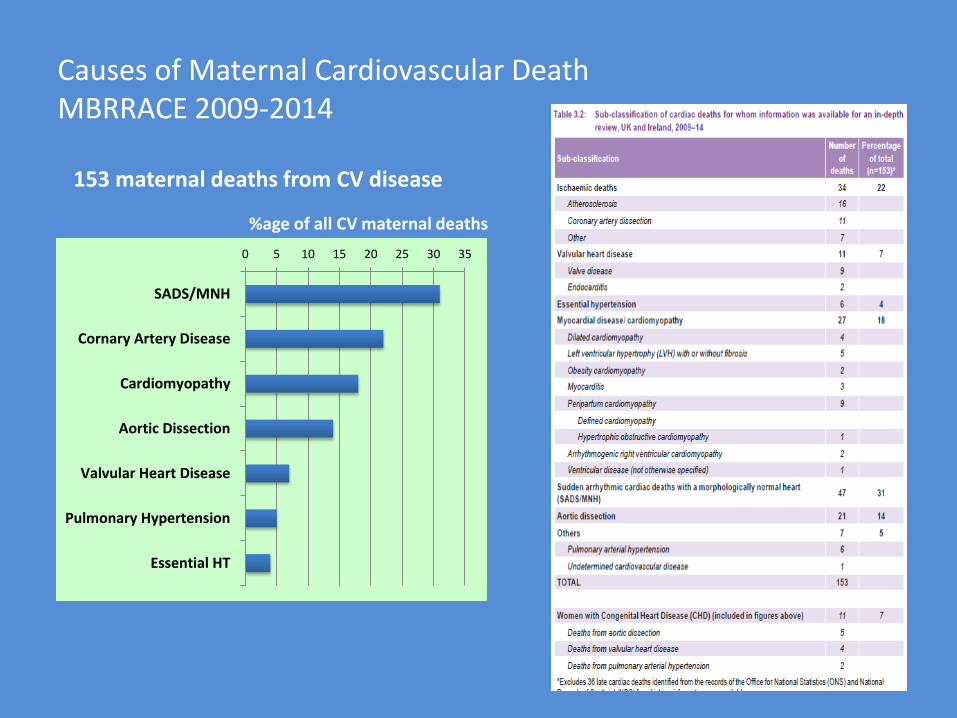
Causes of Maternal Cardiovascular Death MBRRACE 2009-2014
0 5 10 15 20 25 30 35
SADS/MNH
Cornary Artery Disease
Cardiomyopathy
Aortic Dissection
Valvular Heart Disease
Pulmonary Hypertension
Essential HT
%age of all CV maternal deaths
153 maternal deaths from CV disease
Sudden Cardiac Death with Morphologically Normal Heart
Diagnosis of exclusion (includes a negative drug screen)
Mortality rate in pregnancy is probably the same as the non-pregnant rate
81% arrested out of hospital and few had prodromal symptoms
A young Caucasian woman had a normal delivery of her third baby. Two weeks postpartum she collapsed at home but despite exemplary resuscitation could not be revived. Her autopsy was ‘negative’; her BMI was normal, and her heart was normal weight. Review by a cardiac pathologist confirmed the likelihood that she died from SADS/ MNH since all other possible causes had been excluded.
Sudden Cardiac Death with Morphologically Normal Heart
Screening of proband and first degree relatives will identify a genotype for an ion channelopathy in about 50% of families
The Ion channelopathies
Long QT syndromes
Brugada syndrome
Catecholaminergic Polymorphic VT
Progressive Cardiac Conduction Defect
Idiopathic VF
Wolfe-Parkinson-White (with AF)
MBRRACE review screening for inherited cardiac conditions largely not done and only 2 of 53 identified with a disorder
Aortic Dissection
Risk increased 25 times in late pregnancy
Usually aortic root dilatation leading to tamponade
40% of the mothers who died presented with premonitory chest pain that went unrecognised
A woman who had delivered a few days earlier presented by ambulance in the middle of the night to the Emergency Department with severe sudden onset chest and neck pain. Her pregnancy had been complicated by disabling symphysis pubis dysfunction. On arrival at A&E she was anxious and described severe pain starting in the neck and radiating in waves to the chest and back. She was clear that the pain was different to the ‘all over pain’ of her symphysis pubis dysfunction. She was seen by junior doctors who considered pulmonary embolism or anxiety attack as possible diagnoses. They decided on the latter and sent her home without investigation or senior review. She died suddenly at home a few days later. Post mortem confirmed dissection of the entire aorta with a bicuspid aortic valve.
Aortic Dissection
Predisposing conditions
Marfan syndrome
Bicuspid aortic valve with aortopathy
Familial thoracic aortic syndrome
Vascular Ehlers-Danlos syndrome
Loeys-Dietyz syndrome
Coarctation of the aorta esp. complex repairs
Aortitis
In MBRRACE, in 15 of 21 maternal deaths no cause established.
CARDIAC ISCHAEMIA
34 deaths
Half atherosclerotic:
10 acute MI, 6 sudden deaths with CAD+
Almost all of the atherosclerotic deaths were in women with risk factors
Mean age 34, BMI 27, half smokers
One third coronary artery dissection
Mean age 34, half smokers, BMI 24
One-sixth other causes – arteritis, Takotsubo CM, myocardial bridging
CARDIOMYOPATHY
MBRRACE data
27 deaths from cardiomyopathy
Most frequent mode of death was out of hospital arrest after delivery
9 considered peri-partum cardiomyopathy
‘Consider cardiomyopathy in the ∆∆ dyspnoea in pregnancy’
Orthopnoea and PND are ‘not symptoms of pregnancy’
‘Don’t withold investigations and treatment on the grounds of pregnancy and breast-feeding’
CARDIOMYOPATHY
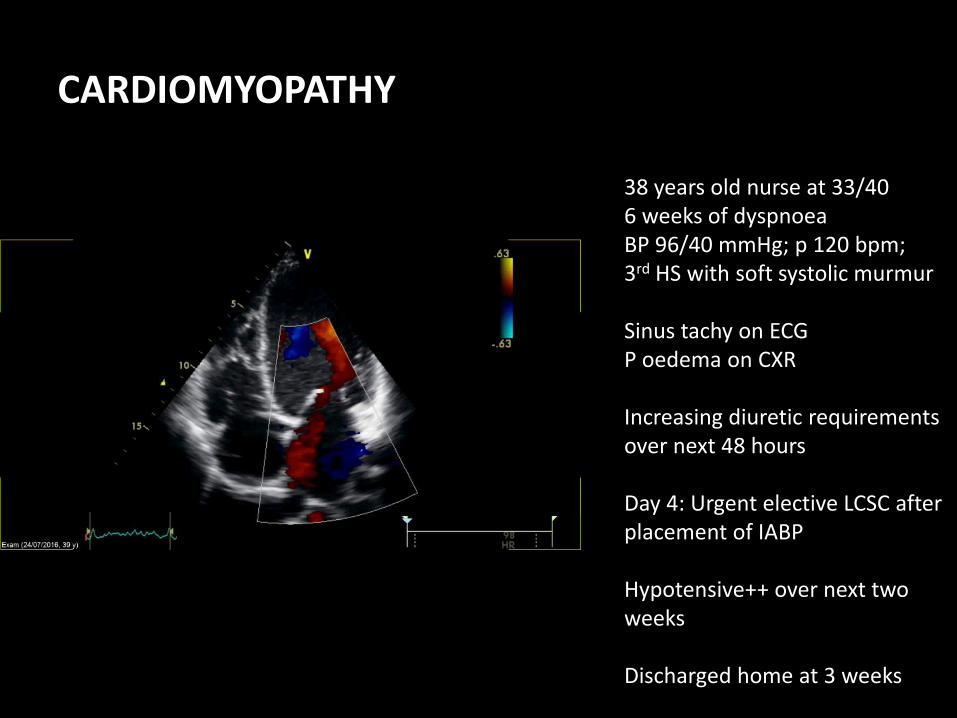
38 years old nurse at 33/40 6 weeks of dyspnoea BP 96/40 mmHg; p 120 bpm; 3rd HS with soft systolic murmur Sinus tachy on ECG P oedema on CXR Increasing diuretic requirements over next 48 hours Day 4: Urgent elective LCSC after placement of IABP Hypotensive++ over next two weeks Discharged home at 3 weeks
CARDIOMYOPATHY
Shown with permission
During her pregnancy a woman presented on five occasions within two weeks to different hospitals and her GP complaining of cough, dyspnoea and orthopnoea. She was noted to be tachycardic. She was prescribed multiple courses of antibiotics to which she failed to respond but no further investigations were done. Eventually a diagnosis of peripartum cardiomyopathy was made and she was delivered by Caesarean section. Despite insertion of an intra-aortic balloon pump, Extracorporeal Membrane Oxygenation (ECMO) and attempted Left Ventricular Assist Device (LVAD) insertion, she died shortly postpartum.
CARDIOMYOPATHY
CARDIOMYOPATHY 29 years old primip 4 weeks post partum 3 presentations with dyspnoea 2 courses of antibiotics Echo eventually Moved to CCU given diuretics, ACEi and … bisoprolol 2.5 mg stat Hypotension+ Inotropic support induced VT Moved to NGH Survived with support One year on.. Current VO2 max 20.3 LV no improvement
PERIPARTUM CARDIOMYOPATHY
Idiopathic Cardiomyopathy in the last trimester to 6/12 postpartum
1 in 3000 pregnancies
More often in..
African ancestry
Age >30 years
Multiparity
Preg induced hypertension
Usually partial to complete recovery of LV function in 2 to 6 months
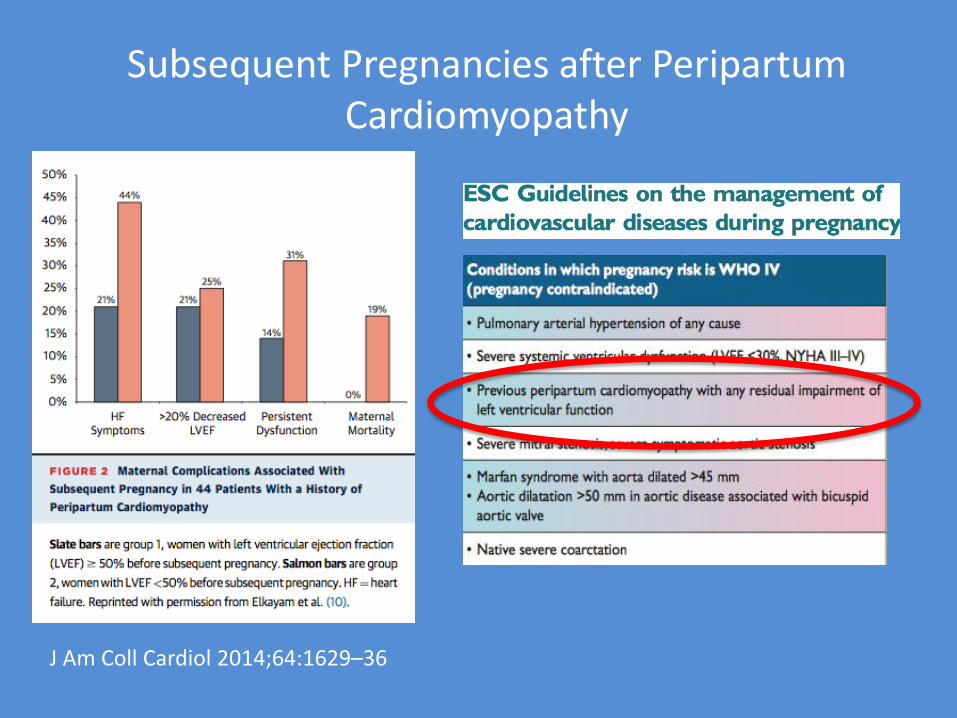
Subsequent Pregnancies after Peripartum Cardiomyopathy
J Am Coll Cardiol 2014;64:1629–36
VALVULAR HEART DISEASE
Regurgitant lesions not causing symptoms before pregnancy are generally well tolerated
Symptomatic or severe obstructive lesions are not well tolerated.
Mechanical heart valve prostheses represent very high risk pregnancies
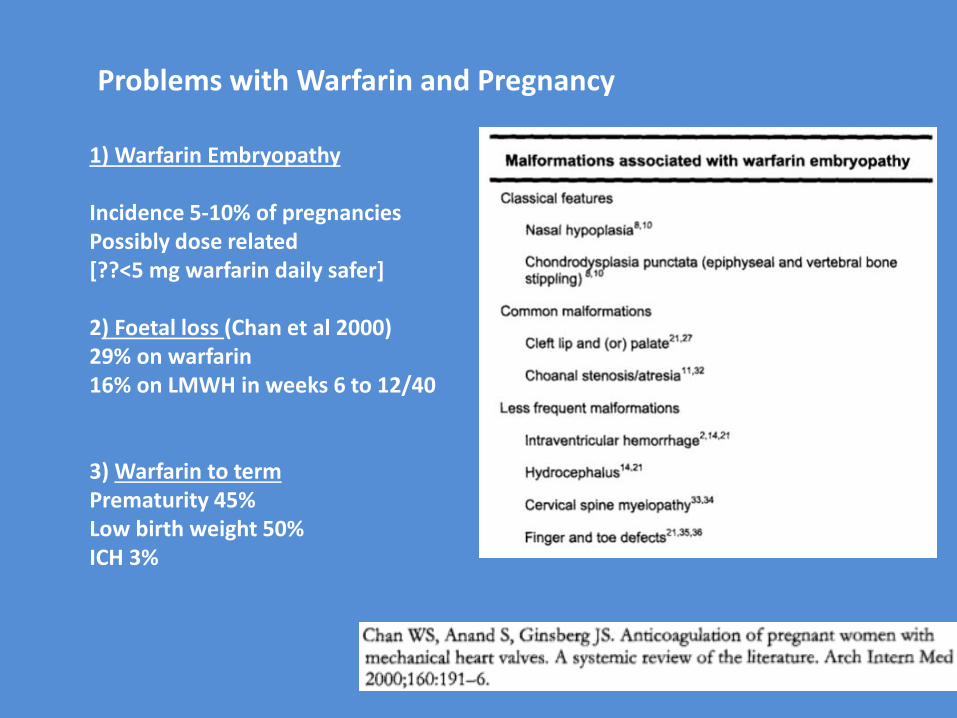
Problems with Warfarin and Pregnancy
1) Warfarin Embryopathy Incidence 5-10% of pregnancies Possibly dose related [??<5 mg warfarin daily safer] 2) Foetal loss (Chan et al 2000) 29% on warfarin 16% on LMWH in weeks 6 to 12/40 3) Warfarin to term Prematurity 45% Low birth weight 50% ICH 3%
VALVULAR HEART DISEASE
• Surveyed the 210 Consultant-led obstetric units in the UK
• Poor maternal outcomes
• Death / ICU admission / Valve thrombosis
• Valve dysfunction resulting in HF or death
• Bleeding requiring blood transfusion or return to theatre
• Poor foetal outcomes
• Miscarriage and stillbirth / Neonatal death
• Foetal abnormality / Apgar score <7 at 5 minutes / Neonatal unit
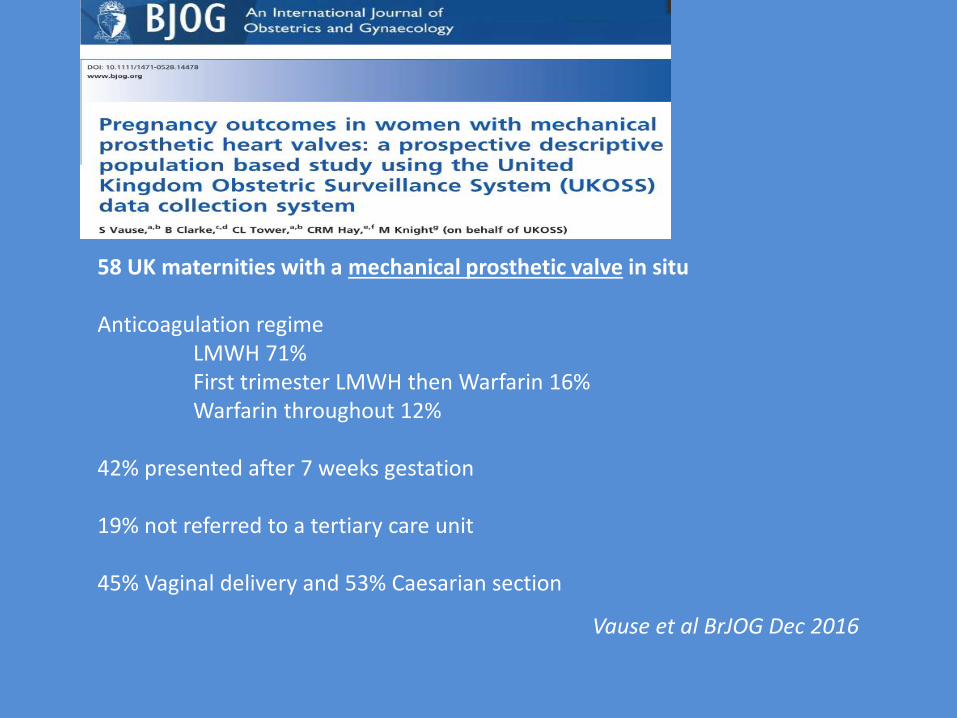
58 UK maternities with a mechanical prosthetic valve in situ Anticoagulation regime LMWH 71% First trimester LMWH then Warfarin 16% Warfarin throughout 12% 42% presented after 7 weeks gestation 19% not referred to a tertiary care unit 45% Vaginal delivery and 53% Caesarian section
Vause et al BrJOG Dec 2016
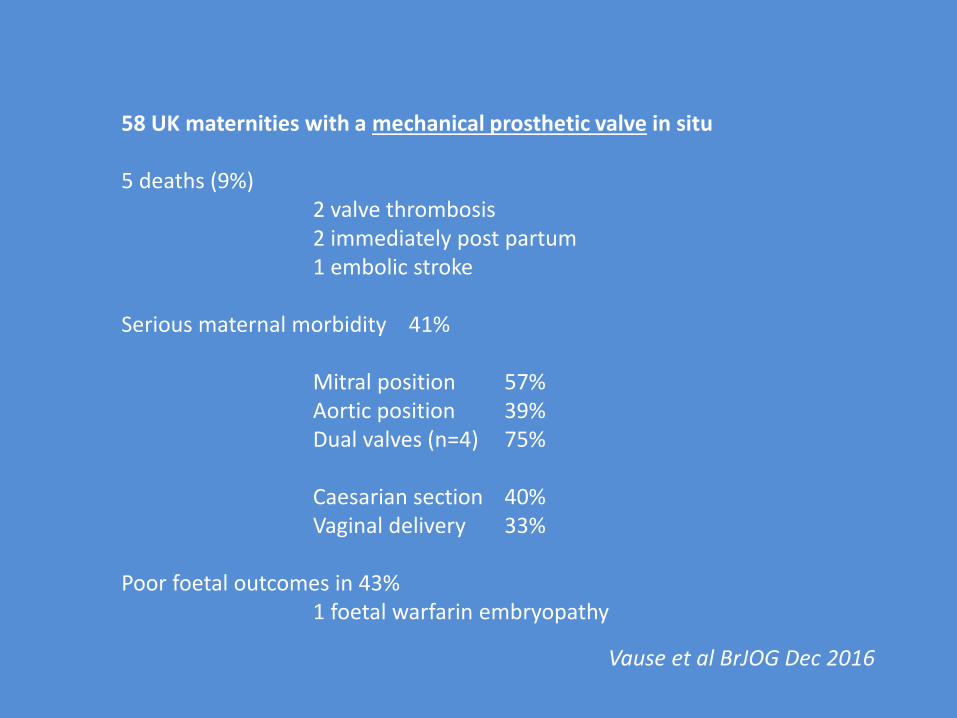
58 UK maternities with a mechanical prosthetic valve in situ 5 deaths (9%) 2 valve thrombosis 2 immediately post partum 1 embolic stroke Serious maternal morbidity 41% Mitral position 57% Aortic position 39% Dual valves (n=4) 75% Caesarian section 40% Vaginal delivery 33% Poor foetal outcomes in 43% 1 foetal warfarin embryopathy
Vause et al BrJOG Dec 2016
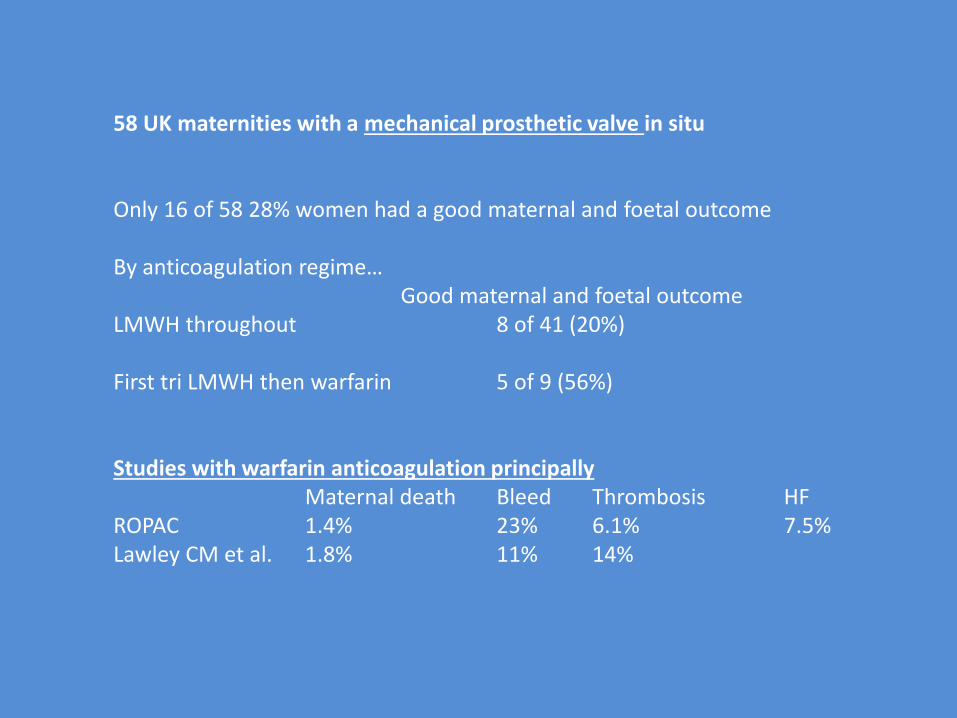
58 UK maternities with a mechanical prosthetic valve in situ Only 16 of 58 28% women had a good maternal and foetal outcome By anticoagulation regime… Good maternal and foetal outcome LMWH throughout 8 of 41 (20%) First tri LMWH then warfarin 5 of 9 (56%) Studies with warfarin anticoagulation principally Maternal death Bleed Thrombosis HF ROPAC 1.4% 23% 6.1% 7.5% Lawley CM et al. 1.8% 11% 14%
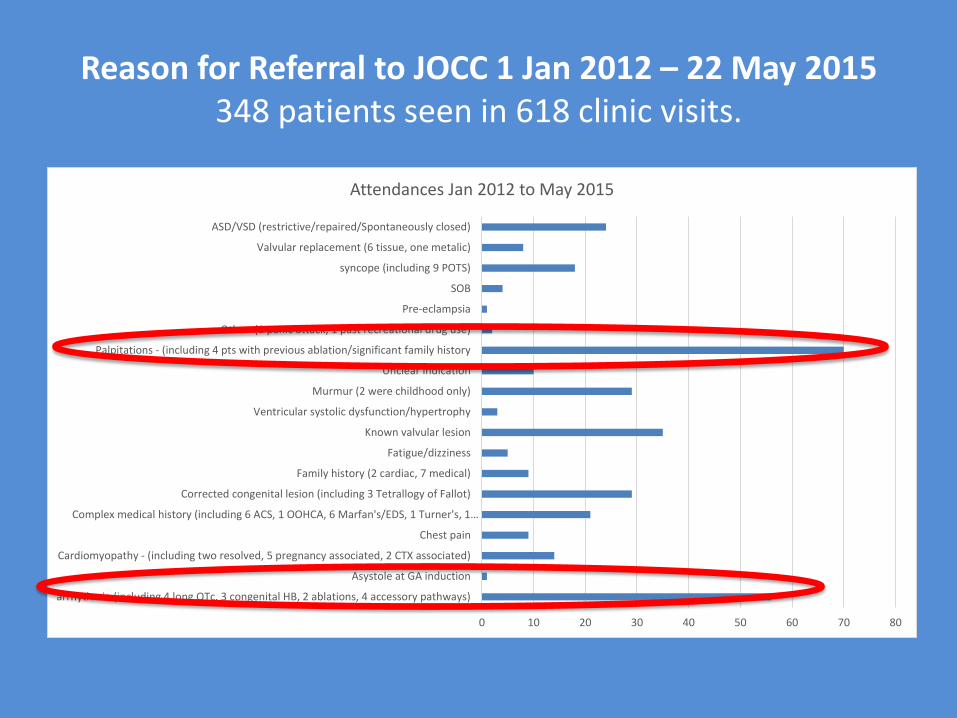
Reason for Referral to JOCC 1 Jan 2012 – 22 May 2015 348 patients seen in 618 clinic visits.
0 10 20 30 40 50 60 70 80
arrhythmia (including 4 long QTc, 3 congenital HB, 2 ablations, 4 accessory pathways)
Asystole at GA induction
Cardiomyopathy - (including two resolved, 5 pregnancy associated, 2 CTX associated)
Chest pain
Complex medical history (including 6 ACS, 1 OOHCA, 6 Marfan's/EDS, 1 Turner's, 1…
Corrected congenital lesion (including 3 Tetrallogy of Fallot)
Family history (2 cardiac, 7 medical)
Fatigue/dizziness
Known valvular lesion
Ventricular systolic dysfunction/hypertrophy
Murmur (2 were childhood only)
Unclear indication
Palpitations - (including 4 pts with previous ablation/significant family history
Other (1 panic attack, 1 past recreational drug use)
Pre-eclampsia
SOB
syncope (including 9 POTS)
Valvular replacement (6 tissue, one metalic)
ASD/VSD (restrictive/repaired/Spontaneously closed)
Attendances Jan 2012 to May 2015
Heart Disease in Pregnancy
CONCLUSION
Women with heart disease need expert multidisciplinary assessment at the onset of reproductive capacity or at diagnosis of CV disease and before each pregnancy
Pregnancy represents a significant cardiovascular stress for women with significant heart disease
Specialist multidisciplinary assessment in pregnancy is best practice
Heart Disease in Pregnancy
CONCLUSION
Women with heart disease need expert multidisciplinary assessment at the onset of reproductive capacity or at diagnosis and before pregnancy
Pregnancy represents a significant cardiovascular stress
Specialist multidisciplinary assessment in pregnancy is best practice

• Early recognition
• Prompt multidisciplinary risk assessment
• Optimisation
• Monitoring
• Delivery planning
• Surveillance and optimisation post delivery
General principles of management of pregnancy in women with heart disease





























