Embed Size (px)
Citation preview

Healthy Living: A Chronic Disease Prevention and
Management Strategy
Submitted to the Regina Qu’Appelle Health Region’s
Primary Health Care Steering Committee February, 2009

ACKNOWLEDGEMENTS The Regina Qu’Appelle Health Region’s Healthy Living: A Chronic Disease Prevention and Management Strategy is the sum total of the efforts of many individuals, programs and service delivery areas. Special thanks are extended to the members of the Regina Qu’Appelle Health Region’s Chronic Disease Prevention and Management Strategy Committee for their guidance and diligence in developing and reviewing this strategy, and their attendance and input during our six committee meetings and three strategic planning sessions as well as their individual consultations (See Appendix 1). Numerous stakeholders involved gave the benefit of their knowledge and experience and shared their time to review and provide their input and feedback through consultation sessions that were held throughout the region. A sincere appreciation and thanks are extended to these stakeholders for their valuable contributions (See Appendix 2). The Regina Qu’Appelle Health Region’s Primary Health Care Steering Committee also provided oversight and direction to the overall development of the strategy. Their support and guidance were essential and helped shape the final document. Special thanks is also given to Chronic Care Prevention and Management representatives from the southern health regions and from Saskatoon’s Health Region for their insight and support, to the Regina Qu’Appelle Health Region’s Health Science Library and the Canadian Agency for Drugs and Technologies in Health for their research assistance. Appreciation is extended to Dr. C. Vuksic for the invitation to present and obtain feedback from the Department of Family Medicine and the forty‐eight family physicians in attendance. This appreciation is also extended to Dr. R. Abdulla, Head of the Department of Medicine for the invitation to present to twenty‐seven specialists in the Department of Medicine, providing an opportunity to request input into the strategy development process. Throughout the review of the current state, I took the opportunity to listen to those suffering from chronic conditions within the Regina Qu’Appelle Health Region and question them about their health journey. The development of a tool to evaluate the effect on family care providers and the use of the patient assessment of chronic illness care tool will help to further develop a picture of the journey experienced. As Strategy Development Consultant for the Regina Qu’Appelle Health Region’s Chronic Disease Prevention and Management Strategy, I would like to extend my deepest appreciation to all those who have given of their time to assist with the development of this strategy. Their passion and dedication was motivating! The Regina Qu’Appelle Health Region has a great deal to be proud of in the compassion, commitment and integrity of their employees. Their desire to provide quality care to the residents of this region and those surrounding is truly inspiring. Website for the Regina Qu’Appelle Health Region’s Healthy Living: A Chronic Disease Prevention and Management Strategy is www.rqhealth.ca/programs/primary_healthcare/primary.shtml. Brenda Collacott Development Consultant, Chronic Disease Prevention and Management Primary Health Care Initiatives Regina Qu’Appelle Health Region December, 2008

Table of Contents
EXECUTIVE SUMMARY..................................................................................................I
1 Background ............................................................................................................... 1
1.1 The RQHR Environment ................................................................................... 2
2 Where do we want to be? Vision, Key Principles and Strategy Framework for RQHR Chronic Disease Prevention and Management ........................................... 3
2.1 Vision ................................................................................................................ 3 2.2 Key Principles................................................................................................... 3 2.3 Strategy Framework: The Expanded Chronic Care Model.............................. 3
3 How will we know when we get there? Key Measures of Success ......................... 4
4 Where are we now and how do we get there? Current state, the Expanded Chronic Care Model and proposed strategies for improvement ............................. 5
4.1 Build Healthy Public Policy.............................................................................. 5 4.2 Create Supportive Environments ...................................................................... 6 4.3 Strengthen Community Action .......................................................................... 7 4.4 Delivery System Design .................................................................................... 8 4.5 Decision Support............................................................................................. 11 4.6 Clinical Information Systems.......................................................................... 13
5 Budget...................................................................................................................... 15
6 Conclusion............................................................................................................... 16
7 References ............................................................................................................... 17

Appendices
Appendix 1: _______________________________________________________ Page 18 RQHR Chronic Disease Prevention and Management Strategy Development Steering Committee Appendix 2: _______________________________________________________ Page 19 Stakeholders Consulted Throughout the Chronic Disease Prevention and Management Strategy Development Process Appendix 3: _______________________________________________________ Page 20 Health Promotion, Population and Public Health Service
— Prepared by Anna Engel, Manager Population and Public Health Services, May 2008 Appendix 4: _______________________________________________________ Page 29 Chronic Disease Management Programs and Services Inventory
— Prepared by Joyce Butler, Development Consultant, Primary Health Care Initiatives, May 2008 Appendix 5: _______________________________________________________ Page 61 RQHR Chronic Disease Prevention and Management Current State (Short List)
— Prepared by Brenda Collacott, Strategy Development Consultant, Primary Health Care Initiatives. June, 2008 Appendix 6: _______________________________________________________ Page 65 RQHR- CDPM: Organization/ Budget/ Location/ Physician Support)
— Prepared by Brenda Collacott, Strategy Development Consultant, Primary Health Care Initiatives, August, 2008 Appendix 7: _______________________________________________________ Page 69 RQHR: CDPM IT / Capacity/Partners Spreadsheet
— Prepared by Brenda Collacott, Strategy Development Consultant, Primary Health Care Initiatives, August, 2008 Appendix 8: _______________________________________________________ Page 73 Strengths, Gaps and Opportunities identified within the RQHR CDPM
— Prepared by Brenda Collacott, Strategy Development Consultant, Primary Health Care Initiatives, October, 2008 Appendix 9: _______________________________________________________ Page 79 Population and Public Health Services (The determinants of health Canadian Community Health Surveys 2003, 2005, 2007) Appendix 10: ______________________________________________________ Page 83 RQHR: Patient and Program Outcome Measurement Tools presently used or planned to be used — Prepared by Brenda Collacott, Strategy Development Consultant, Primary Health Care Initiatives, September 2008
Appendix 11: ______________________________________________________ Page 89 Assessment of Chronic Illness Care Tool, Version 3.5 (ACIC) (For systems and provider practices) Appendix 12: _____________________________________________________ Page 100 Assessment of Care for Chronic Conditions (Patient Assessment of Chronic Illness Care: (PACIC)

Healthy Living: A Chronic Disease Prevention and Management Strategy
EXECUTIVE SUMMARY Page I
EXECUTIVE SUMMARY The Regina Qu’Appelle Health Region’s Healthy Living: A Chronic Disease Prevention and Management Strategy addresses four key questions:
Where do we want to be? How will we know when we get there? Where are we now? How do we get there?
Where do we want to be? The title of this report, “Healthy Living: A Chronic Disease Prevention and Management Strategy” envisions continuous advances in health and quality of life by preventing chronic disease among Regina Qu’Appelle Health Region residents and by decreasing the risks associated with many chronic conditions. An integrated, interdisciplinary and inter-sectoral approach is taken and care is provided in a seamless manner, to address the underlying determinants of health, common risk factors, health issues and problems in the population groups. Ultimately the population is healthier, and the right health-related behavior decision is made easy. How will we know when we get there? The Chronic Disease Prevention and Management Strategy Committee has selected as Regina Qu’Appelle Health Region’s starting point a combination of six process and outcome measures to measure our success. They are:
Number of Populations with Chronic Conditions Standards that are met by Regina Qu’Appelle Health Region’s next Accreditation Canada survey.
Regina Qu’Appelle Health Region’s overall score using the Assessment of Chronic Illness Care (Version 3.5 tool) (see Appendix 11).
Percentage of Most of the Time or Always ratings on the Patient Assessment of Chronic Illness Care tool (see Appendix 12).
Acute care hospitalization rates for chronic obstructive pulmonary disease, congestive heart failure, and diabetes ambulatory care sensitive conditions.
Percentage of emergency room visits related to chronic conditions. Percentage change in Statistics Canada: Canadian Community Health Survey
Regina Qu’Appelle Health Region indicator profile results. Where are we now and how do we get there? Regina Qu'Appelle Health Region provides an array of CDPM services and programs under a number of different portfolios. Despite the excellent work being done within these programs, the burden of chronic illness within region is increasing.

Healthy Living: A Chronic Disease Prevention and Management Strategy
EXECUTIVE SUMMARY Page II
The RQHR selected The Expanded Chronic Care Model: Integrating Population Health Promotionvi developed by staff of the Vancouver Island Health Authority, as the framework for strategy development. The Expanded Chronic Care Model (ECCM) necessitates system reform focused on population health promotion and chronic disease prevention, more pro-active care and more informed, activated patients and communities. The model outcomes are healthier populations and improved functional and clinical outcomes for individuals. RQHR CDPM services were reviewed in their current state and analyzed according to the ECCM. Based on this review and analysis 49 strategies for improvement are proposed. They are listed below. Eleven strategies identified as having priority for implementation in Phase 1 appear in bold font. COMMUNITY Build Healthy Public Policy STRATEGY 4.1.1: Collect, share and utilize both health data / evidence and stakeholder input across the organization to support the advocacy and development of Healthy Public Policy. STRATEGY 4.1.2: Increase the capacity of RQHR staff / departments to champion and advocate for Healthy Public Policy. STRATEGY 4.1.3: Continue and increase partnerships with community, as well as internal and external stakeholders. Create Supportive Environments STRATEGY 4.2.1: Collect, share and utilize both health data / evidence and stakeholder input across the organization to create supportive environments. STRATEGY 4.2.2: Increase awareness within the RQHR and community of available programs and services. STRATEGY 4.2.3: With internal and external partners, continue to create environments within the RQHR and community that support healthy living. Strengthen Community Action STRATEGY 4.3.1: Collect, share and utilize both health data / evidence and stakeholder input across the organization to identify strategies to strengthen community action. STRATEGY 4.3.2: Increase awareness within the RQHR and community of available programs and services.

Healthy Living: A Chronic Disease Prevention and Management Strategy
EXECUTIVE SUMMARY Page III
STRATEGY 4.3.3: Increase the capacity of RQHR staff / departments to build community development into program / service planning. STRATEGY 4.3.4: Broaden and sustain partnerships to enhance and develop programs / services that strengthen communities and build capacity. HEALTH SYSTEM Self Management Support/ Develop Personal Skills STRATEGY 4.4.1: Support CDPM staff and programs to consistently use recognized best practices to effectively support patient self-management and behavior change (includes staff training and skill development, appropriate policies and process development, program design and performance management). STRATEGY 4.4.2: Advocate for and obtain sustainable funding for the Live Well™ with Chronic Conditions programming and actively market it to the public and care providers. STRATEGY 4.4.3: Establish mechanisms and ensure adequate resources to support consistent, on-going patient follow-up in all programs. STRATEGY 4.4.4: Enhance public and staff awareness of CDPM programs and services through the use of printed materials, local media, HealthLine and the RQHR website. Delivery System Design STRATEGY 4.5.1: Create a CDPM organizational structure to enhance linkages, coordination and communication across the various programs and services. STRATEGY 4.5.2: Maintain a CDPM Steering Committee to support integration and coordination, with appropriate sub-committee formation. STRATEGY 4.5.3: Establish a RQHR CDPM management position. STRATEGY 4.5.4: Identify a physician leader to work collaboratively with the CDPM manager. STRATEGY 4.5.5: Undertake team development efforts within and across CDPM teams as required. STRATEGY 4.5.6: Explore opportunities to facilitate improved collaboration and communication between physician specialists / specialized care teams and family physicians/ PHC teams.

Healthy Living: A Chronic Disease Prevention and Management Strategy
EXECUTIVE SUMMARY Page IV
STRATEGY 4.5.7: Build strength through multi-disciplinary teams and/or multi-sectoral teams. Investigate incentives for specialists to work more collaboratively with teams and/or family physicians. STRATEGY 4.5.8: Develop a navigation system especially for high risk patients and those with multiple chronic conditions. STRATEGY 4.5.9: Enhance care provider awareness of CDPM, CDPM resources and tools, and CDPM programs and services in the region and community and identify mechanisms to keep practitioners up-to-date and well informed regarding current resources. STRATEGY 4.5.10: Ensure that community development approaches are part of planning within all CDM programs. STRATEGY 4.5.11: Investigate the benefits and feasibility of a single entry point for patients, whether one location or one central contact and referral point. Consider the benefits and opportunities of co-location for integration of programs and services. STRATEGY 4.5.12: Identify opportunities to deliver care using multiple care providers in a clinic format. STRATEGY 4.5.13: Develop a holistic approach by strengthening the mental health (depression care) component across every chronic condition program. STRATEGY 4.5.14: Increase the capacity of all CDPM staff to screen for depression (identify) and determine an appropriate plan to address mild to severe conditions. STRATEGY 4.5.15: Integrate mental health primary care supports / services into all CDPM programs. STRATEGY 4.5.16: Provide all chronic condition management programs with priority access to mental health expertise. STRATEGY 4.5.17: Expand collaborative care with psychiatrists. STRATEGY 4.5.18: Consider and implement extended hours of operation if identified as a community need. STRATEGY 4.5.19: Investigate the development of an Obesity Prevention and Management Program in partnership with other programs and agencies. STRATEGY 4.5.20: Utilize the principles of clinical practice redesign to improve access where wait lists exist.

Healthy Living: A Chronic Disease Prevention and Management Strategy
EXECUTIVE SUMMARY Page V
STRATEGY 4.5.21: Clearly identify and communicate the screening guidelines used for priority access to various CDM programs. STRATEGY 4.5.22: Develop a comprehensive and coordinated approach to screening and diagnosis for chronic diseases. STRATEGY 4.5.23: Enhance partnerships with the community to develop lifestyle programming. STRATEGY 4.5.24: Ensure all CDPM programs address the cultural and spiritual needs of patients as part of holistic care. Provide increased resources for traditional and pastoral services. Decision Support STRATEGY 4.6.1: Collect, share and utilize health data across the organization to support program-based decisions. STRATEGY 4.6.2: Implement systems that support dissemination and consistent use of established best practice guidelines and where needed, develop RQHR protocols in the absence of national or provincial best practice guidelines. STRATEGY 4.6.3: Explore the opportunities for Shared Health Care delivery models and were feasible, pilot and evaluate their effectiveness. STRATEGY 4.6.4: Foster “care team champions” throughout the system. STRATEGY 4.6.5: Establish and maintain systems and process to support the collection, analysis and use of outcome data by all CDPM programs. This may require both human and technical resources. STRATEGY 4.6.6: Determine benchmarks for outcomes: use for comparison of patient outcomes and for planning services. STRATEGY 4.6.7: Employ regular patient experience surveys to provide opportunity for patient feedback. Clinical Information Systems STRATEGY 4.7.1: Develop a regional CDPM clinical information management strategic plan which will provide CDPM programs with full functionality to support best practices in client care, team communication and outcome measurement. The strategy will identify short term solutions to be used until the provincial PHC EMR and CDM Toolkit is available. STRATEGY 4.7.2: Ensure adequate administrative support in all CDM programs and expand IT expertise to implement and fully utilize current and future systems.

Healthy Living: A Chronic Disease Prevention and Management Strategy
EXECUTIVE SUMMARY Page VI
STRATEGY 4.7.3: Work with the RQHR Information Technology department to develop processes/ policies to improve staff access to systems like PIP and Lab Viewer. STRATEGY 4.7.4: Standardize the collection and analysis of patient outcome measures. Budget The Regina Qu'Appelle Health Region will require new and ongoing resources to implement the strategies proposed in this plan. The estimated funding requirements for Phase 1 are included in this document. Conclusion The organization of Regina Qu’Appelle Health Region chronic disease prevention and management services and programs is very complex, but we are well positioned to implement this strategic plan. We have many dedicated managers and staff committed to CDPM and we have valuable relationships with a number of important community partners. This document is intended to be a “living document” which will be revised over the course of time, to ensure that the strategy encompasses a truly client-centered and holistic approach to assist and support people in a direction of wellness. In its evolution, the document will also aim to align with the operational priorities of the Regina Qu’Appelle Health Region to ensure consistency and commitment to healthy living and chronic disease prevention and management.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 1
1 Background The growing prevalence and impact of chronic conditions is a serious concern across Canada and internationally, people are looking for solutions to many of the same problems. The prevalence of chronic conditions continues to grow worldwide and is expected to increase due to an aging population and rising trends in risk factors (e.g. obesity)i. Chronic health conditions are more common among the elderly, women, those living in rural areas and those of lower socio-economic statusi vii viii. A chronic condition simply defined is any condition which necessitates ongoing adjustments by the involved person with health care system interactions ii. As identified in Population Patterns of Chronic Health Conditions in Canada (December, 2007) one third of Canadians, about nine million people have at least one of seven select chronic health conditions: arthritis, cancer, chronic obstructive pulmonary disease (COPD), diabetes, heart disease, high blood pressure and mood disorders iii. The prevalence increases to almost three quarters of seniors 65 years and olderiii, and Saskatchewan has the highest percentage of seniors in Canadaiv. As a result, the prevalence of two or more select chronic health conditions is therefore higher in Saskatchewan than the Canadian averageiii. People with chronic health conditions use health care services more often and more intensively than those without, and the intensity of use increases as the number of health problems increaseiii.
The development of a Saskatchewan provincial chronic disease prevention and management (CDPM) strategy is increasing as a priority for the Ministry of Health. To date the actions by the Ministry include:
Funding the start-up costs for a provincial self management support program called “Live Well™ with Chronic Conditions”.
Preliminary work on a chronic disease management information system. Preliminary work on the development of a provincial CDPM strategy. Transfer of funding in 2008-09 to the Regional Health Authorities to support our
continued involvement in the Health Quality Council’s Chronic Disease Management Collaboratives.
The Regina Qu’Appelle Health Region (RQHR) also identified the need for a CDPM strategy and therefore hired a consultant to:
establish a CDPM Strategy Committee to guide the strategy development, assess the current state of RQHR CDPM programs and services, identify appropriate performance measures related to high priority areas, and develop a written strategy for the region.
Prior to the commencement of this work, and in order to establish a baseline for improvement, RQHR underwent accreditation using Accreditation Canada’s Populations with Chronic Conditions standards. Of the 64 standards, RQHR met 35.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 2
A list of RQHR Population and Public Health (PPH) programs and services related to chronic disease prevention (see Appendix 3) was developed. An inventory was also completed of specific RQHR chronic disease management (CDM) programs (see Appendix 4). Both documents identified the many and varied programs and services available within the region. The RQHR programs and services included in the inventory and in the development of this strategy were limited to those aimed at preventing or managing Diabetes, Chronic Renal Insufficiency (CRI), Chronic Obstructive Pulmonary Disease (COPD), Heart Disease, Depression and Obesity. This was because of the prominence of these conditions within the region’s population, their many common preventable risk factors and their interrelatedness. While limiting the review also assisted in managing the strategy’s scope, it is expected that the strategy will be used as a framework for better integration of all RQHR CDPM services. Broad consultations with groups and personal interviews were conducted regionally, provincially and nationally. Information was collected through internet and literature searches. A massive amount of exceedingly complex data was systematically collected and organized using Ontario’s Trillium Health Centre’s Short List format for Chronic Disease Prevention and Management Servicesix. Once compiled (see Appendices 5, 6 and 7), it was evaluated, summarized and shared with the CDPM Strategy Committee (see Appendix 8). Information was also collected on the demographics of the population servediii, iv, vii, viii, with a review of the overall quality of perceived health through review of the Canadian Community Health Survey Reportv. This document is intended to be a “living document” which will be refined and revised over time, to ensure that the strategy encompasses a truly client-centered and holistic approach to assist and support people in a direction of wellness. In its evolution, the document will also aim to align with the operational priorities of the RQHR to ensure consistency and commitment to healthy living and chronic disease prevention and management.
1.1 The RQHR Environment The RQHR is the largest health care delivery system in southern Saskatchewan serving the needs of 245,276 residents within the regionxi, as well as those in the southern half of the province who receive service through tertiary care programs. Approximately 82% of the region’s population is situated in Regina, and 18% are situated rurally. Of the population, 14% are those over the age of 65 and 12% of the population are First Nations peoplesiii.
RQHR PPH Services compared outcome results from Statistics Canada’s Indicator Profiles from the Canadian Community Health Surveys from 2003, 2005 and 2007 with Saskatchewan and national data. From this information, it is clear that for RQHR residents, behaviors to prevent chronic illness are worsening v (see Appendix 9). This is confirmed by the recent release of the Canadian Institute for Health Information: Health

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 3
Indicators 2008 Reducing Gaps in Health, A Focus on Socio-Economic Status in Urban Canadaviii.
2 Where do we want to be? Vision, Key Principles and Strategy Framework for RQHR Chronic Disease Prevention and Management
2.1 Vision The title of this report, Healthy Living: A Chronic Disease Prevention and Management Strategy envisions continuous advances in health and quality of life by preventing chronic disease among RQHR residents and by decreasing the risks associated with many chronic conditions. There is a common understanding of, and messaging about healthy living, health promotion and chronic disease prevention. An integrated, interdisciplinary and inter-sectoral approach is taken to address common risk factors, health issues and problems involving the underlying determinants of health in population groups. Chronic disease management is provided as required predominately at the community level in a seamless system, which is clearly identified, easily accessible and engages the individual and their family. It provides effective support for self management thereby reducing the negative impact of these conditions on peoples’ day-to-day lives. Ultimately the population is healthier, and the right health-related behavior decision is made easy.
2.2 Key Principles The CDPM Strategy Committee determined that the RQHR CDPM strategy should incorporate the following principles which are consistent with the values of the region:
Evidence-based decision making. Client and community centered. Safe care for the patient. Ethical and integrated service delivery. Participatory with a strong partnership base. Timely “equal” access to services. Comprehensive service delivery.
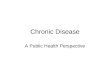
2.3 Strategy Framework: The Expanded Chronic Care Model The RQHR selected The Expanded Chronic Care Model: Integrating Population Health Promotionvi , developed by staff of the Vancouver Island Health Authority, as the framework for strategy development. It is based on the original Chronic Care Modelvi, developed at the MacColl Institute for Healthcare Innovation, and further refined by the Robert Wood Johnson Foundation. Both models have been used world wide to guide system reform for chronic illness care. The Expanded Chronic Care Model (ECCM) necessitates system reform focused on population health promotion and chronic disease prevention, more pro-active care and

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 4
more informed, activated patients and communities. The model outcomes are healthier populations and improved functional and clinical outcomes for individuals.
The model includes two key systems: the community and the health system that exists within the community. The porous border between the two represents interchanges occurring between the health system and the community. The community consists of three elementsii, vi:
Building Healthy Public Policy, Creating Supportive Environments, and Strengthening Community Action.
The Health System has four components, but they actually straddle both systems:
Self management and the development of personal skills to self manage, The Delivery System design/ and the re-orientation of health services, Decision Support, and Clinical Information Systems.
These areas will be described in more detail in section 4 of this document.
3 How will we know when we get there? Key Measures of Success The importance of establishing indicators to measure the success of CDPM programs and services has been recognized by a number of health care organizations across Canada. More and more evidence is required to demonstrate that the resources being expended actually prevents and/or reduces chronic disease and actually makes a difference for the client/patient seeking services and care. Better accountability for the use of resources requires indicator development and outcome measurement for programs and services delivered across the health care system from population health promotion through to primary prevention, secondary and tertiary levels of care.
Community
Health System
Build HealthyPublic Policy
Create Supportive
EnvironmentStrengthen
Community Action
Self-Management/Develop
Personal SkillsDelivery System
Design/Re-orient Health
Services
DecisionSupport
InformationSystems
Productive Interactions & Relationships
Population Health Outcomes/Functional & Clinical Outcomes
InformedActivated
Patient
ActivatedCommunity
PreparedProactivePractice
Team
Prepared ProactiveCommunity Partners
Expanded Chronic Care Model: Integrating Population Health Promotion
(Barr, Robinson, Marin-Link, Underhill, Dotts, Ravensdale, Salivaras. (2003). The expanded chronic care model. Hospital Quarterly Vol.7 No.1. 2003.)
Community
Health System
Build HealthyPublic Policy
Create Supportive
EnvironmentStrengthen
Community Action
Self-Management/Develop
Personal SkillsDelivery System
Design/Re-orient Health
Services
DecisionSupport
InformationSystems
Productive Interactions & Relationships
Population Health Outcomes/Functional & Clinical Outcomes
InformedActivated
Patient
ActivatedCommunity
PreparedProactivePractice
Team
Prepared ProactiveCommunity Partners
Expanded Chronic Care Model: Integrating Population Health Promotion
(Barr, Robinson, Marin-Link, Underhill, Dotts, Ravensdale, Salivaras. (2003). The expanded chronic care model. Hospital Quarterly Vol.7 No.1. 2003.)
Community
Health System
Build HealthyPublic Policy
Create Supportive
EnvironmentStrengthen
Community Action
Self-Management/Develop
Personal SkillsDelivery System
Design/Re-orient Health
Services
DecisionSupport
InformationSystems
Productive Interactions & Relationships
Population Health Outcomes/Functional & Clinical Outcomes
InformedActivated
Patient
ActivatedCommunity
PreparedProactivePractice
Team
Prepared ProactiveCommunity Partners
Community
Health System
Build HealthyPublic Policy
Create Supportive
EnvironmentStrengthen
Community Action
Self-Management/Develop
Personal SkillsDelivery System
Design/Re-orient Health
Services
DecisionSupport
InformationSystems
Productive Interactions & Relationships
Population Health Outcomes/Functional & Clinical Outcomes
InformedActivated
Patient
ActivatedCommunity
PreparedProactivePractice
Team
Prepared ProactiveCommunity Partners
Community
Health System
Build HealthyPublic Policy
Create Supportive
EnvironmentStrengthen
Community Action
Self-Management/Develop
Personal SkillsDelivery System
Design/Re-orient Health
Services
DecisionSupport
InformationSystems
Productive Interactions & Relationships
Population Health Outcomes/Functional & Clinical Outcomes
InformedActivated
Patient
ActivatedCommunity
PreparedProactivePractice
Team
Prepared ProactiveCommunity Partners
Community
Health System
Build HealthyPublic Policy
Create Supportive
EnvironmentStrengthen
Community Action
Self-Management/Develop
Personal SkillsDelivery System
Design/Re-orient Health
Services
DecisionSupport
InformationSystems
Community
Health System
Build HealthyPublic Policy
Create Supportive
EnvironmentStrengthen
Community Action
Self-Management/Develop
Personal SkillsDelivery System
Design/Re-orient Health
Services
DecisionSupport
InformationSystems
Productive Interactions & Relationships
Population Health Outcomes/Functional & Clinical Outcomes
InformedActivated
Patient
ActivatedCommunity
InformedActivated
Patient
ActivatedCommunity
InformedActivated
Patient
ActivatedCommunity
PreparedProactivePractice
Team
Prepared ProactiveCommunity Partners
PreparedProactivePractice
Team
Prepared ProactiveCommunity Partners
PreparedProactivePractice
Team
Prepared ProactiveCommunity Partners
Expanded Chronic Care Model: Integrating Population Health Promotion
(Barr, Robinson, Marin-Link, Underhill, Dotts, Ravensdale, Salivaras. (2003). The expanded chronic care model. Hospital Quarterly Vol.7 No.1. 2003.)

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 5
Accreditation Canada is currently leading a national initiative to identify three indicators as a starting point for evaluating progress. The CDPM Strategy Committee has selected as RQHR’s starting point a combination of six process and outcome measures, consistent with those being considered by the Accreditation Canada Working Group. They are:
Number of Populations with Chronic Conditions Standards that are met by Regina Qu’Appelle Health Region’s next Accreditation Canada survey.
Regina Qu’Appelle Health Region’s overall score using the Assessment of Chronic Illness Care (Version 3.5 tool) (see Appendix 11).
Percentage of Most of the Time or Always ratings on the Patient Assessment of Chronic Illness Care tool (see Appendix 12).
Acute care hospitalization rates for chronic obstructive pulmonary disease, congestive heart failure, and diabetes ambulatory care sensitive conditions.
Percentage of emergency room visits related to chronic conditions. Percentage change in Statistics Canada: Canadian Community Health Survey
Regina Qu’Appelle Health Region indicator profile results. Measurement tools are available for each of these indicators. Over the next year, further discussion will occur by the CDPM Strategy Committee regarding the processes for collecting and reporting this information and specific targets for each indicator. Many RQHR CDPM service areas have also identified specific clinical and functional outcomes for their clients (see Appendix 10), but the availability and use of validated evaluation tools to track and monitor these outcomes is currently inconsistent.
4 Where are we now and how do we get there? Current state, the Expanded Chronic Care Model and proposed strategies for improvement
RQHR CDPM services were reviewed in their current state and analyzed according to the ECCM. Details are available in Appendices 5, 6, 7, 8 and 10. The following is a summary of this analysis and proposed strategies for improvement.
Community
The underlying principles of this component are removing barriers, ensuring meaningful participation of community members and organizations, developing partnerships with sectors outside of health, applying multiple upstream strategies that look beyond the immediate issue to the root cause, and utilizing evidence to inform practice and policy.
4.1 Build Healthy Public Policy This element focuses on developing and implementing policies designed to improve population health, involving working towards organizational and governmental policy and legislation that fosters greater equity in society and leads to ensuring safer and healthier goods, services and environments. The aim is to make the healthier choice the

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 6
easier choice, not only for individuals, but for companies, organizations and governments. RQHR CURRENT STATE PPH Services and other RQHR staff are actively involved in the development of healthy public (social) policies. Many of these have a direct or indirect impact on chronic disease prevention and management (see Appendix 3). PROPOSED STRATEGIES STRATEGY 4.1.1: Collect, share and utilize both health data / evidence and stakeholder input across the organization to support the advocacy and development of Healthy Public Policy. STRATEGY 4.1.2: Increase the capacity of RQHR staff / departments to champion and advocate for Healthy Public Policy. STRATEGY 4.1.3: Continue and increase partnerships with community, as well as internal and external stakeholders.
4.2 Create Supportive Environments This element involves working to create conditions for living that are safe, stimulating, satisfying and enjoyable in order to achieve optimal levels of health in social and community environments. RQHR CURRENT STATE
PPH Services provide programs and services to support health across the various life stages in a variety of social and physical environments (see Appendix 3).
Home Care provides services to assist individuals to remain in their homes with added supports (see Appendix 4).
Regional chronic disease management programs (such as MEDEC) provide education and services within schools, workplaces, and child care settings to support individuals with chronic conditions, enabling them to participate and function effectively in these settings and remain in the community.
PROPOSED STRATEGIES STRATEGY 4.2.1: Collect, share and utilize both health data / evidence and stakeholder input across the organization to create supportive environments. STRATEGY 4.2.2: Increase awareness within the RQHR and community of available programs and services. STRATEGY 4.2.3: With internal and external partners, continue to create environments within the RQHR and community that support healthy living.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 7
4.3 Strengthen Community Action Strengthening Community Action involves working with community groups to set priorities and achieve goals to enhance the holistic health of the community. By empowering and encouraging effective public participation, health promotion and prevention aims to support people in finding their own ways in managing the health of their community. RQHR CURRENT STATE PPH Services works to build community capacity by engaging community and providing educational and skill building programs (see Appendix 3). PROPOSED STRATEGIES STRATEGY 4.3.1: Collect, share and utilize both health data / evidence and stakeholder input across the organization to identify strategies to strengthen community action. STRATEGY 4.3.2: Increase awareness within the RQHR and community of available programs and services. STRATEGY 4.3.3: Increase the capacity of RQHR staff / departments to build community development into program / service planning. STRATEGY 4.3.4: Broaden and sustain partnerships to enhance and develop programs / services that strengthen communities and build capacity.
Health System The ECCM describes a health system that promotes a culture of safe, coordinated, high quality care, with visible supports in place for effective improvement strategies aimed at comprehensive system change. The activities involved with the delivery of health care services and population health promotion are integrated, and have an impact on both the health care organization and the community.
4.4 Self Management Support/Develop Personal Skills Self Management support and the development of personal skills emphasize the patient’s central role in the management of their chronic condition. It is promoted by incorporating a coaching model of service delivery; and expanding access to health education, health resource information, self directed learning packages, emotional support and community support programs. RQHR CURRENT STATE
Various RQHR chronic disease management (CDM) and education programs currently utilize many elements of self management support and development of personal skills with their clients (see Appendix 5).

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 8
Some of the fundamental components, principles and techniques of patient self management are not consistently applied across all of the programs (see Appendix 10). This may be a result of lack of staff knowledge / skills and/or appropriate design and processes and/or resources.
The region has initiated a patient self-management program called “Live Well™ with Chronic Conditions” program and sessions have been offered in the city and a limited number of rural locations.
Staff knowledge and skills related to self-management best practices varies. Staff training in skills such as motivational interviewing has been offered within some programs.
Many region CDM programs have established partnerships with non-governmental organizations to facilitate patient self-management and community support programs. Additional opportunities exist.
A wide range of education materials pertaining to various chronic conditions are available for patients, but information is not always consistent and it may not meet the needs of all clients (see Appendix 5).
Follow-up does not occur consistently in all programs, in some cases due to workload or lack of recall mechanisms.
In some cases there is a lack of awareness of RQHR CDPM programs and services amongst the public and RQHR staff. Region staff are also unaware of all the community based, non-health sector services which could further support client self management.
PROPOSED STRATEGIES STRATEGY 4.4.1: Support CDPM staff and programs to consistently use recognized best practices to effectively support patient self-management and behavior change (includes staff training and skill development, appropriate policies and process development, program design and performance management). STRATEGY 4.4.2: Advocate for and obtain sustainable funding for the Live Well™ with Chronic Conditions programming and actively market it to the public and care providers. STRATEGY 4.4.3: Establish mechanisms and ensure adequate resources to support consistent, on-going patient follow-up in all programs. STRATEGY 4.4.4: Enhance public and staff awareness of CDPM programs and services through the use of printed materials, local media, HealthLine and the RQHR website.
4.5 Delivery System Design Identification, building, training, and equipping interdisciplinary teams to deliver integrated chronic disease prevention and management services are emphasized. Role definition and distribution of tasks amongst team members is necessary. There are positive, supportive learning opportunities for team members to assist them to learn and apply new skills and create structured, planned interactions to support

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 9
evidence-based care. Staff understand the importance of literacy and culture in the care they provide. Clinical case management is provided for complex clients, with the assurance of regular follow-ups. Healthcare professionals are reoriented to become promoters of health, rather than simply part of the repair service. Teams expand beyond multi-disciplinary health-care professionals to all those who can contribute to providing services in a more holistic way.
RQHR CURRENT STATE
OVERALL CDPM ORGANIZATION RQHR provides an array of CDPM services under a number of different
portfolios (see Appendix 6), each with their own leadership, priorities and goals. Many of these services and programs operate independently which can make integration, coordination and communication a challenge.
In many service delivery areas of the RQHR, administrative leaders work collaboratively with a physician co-lead, however there is not a specific CDPM administrative leader or physician co-leader (see Appendix 6).
CHRONIC DISEASE MANAGEMENT (CDM) TEAMS
There are many established multi-disciplinary Primary Health Care (PHC), and CDM teams.
In some case, barriers exist which hamper access to and communication between the specialists / CDM programs and family physicians / PHC teams. Opportunities for greater collaboration and enhanced communication exist.
Currently, no consistent clinical case management services are available for complex or high risk patients.
ACCESS
Growing patient volumes have resulted in wait lists exist in some areas, ranging from weeks to months to years in duration (see Appendix 5).
While a wide range of CDM services are provided, barriers to access exist due to program location (e.g., urban only), hours of operation, referral process, wait lists, etc. Some services are offered in rural locations, in other instances outreach services to rural locations are offered by traveling staff or via Telehealth. Lack of transportation and child care services as well as cultural / spiritual barriers are also issues.
Co-ordination of services between various chronic disease programs does not presently exist, except in limited situations resulting in multiple appointments with different care areas for the patient.
Mental health support for chronic disease patients is lacking. CDM staff have limited capacity to identify and assist their clients who are dealing with mental health and/or depressive disorders.
Access to long term sustainable funding is a concern for some programs within the region (COPD Rehabilitation Program, CHF Clinic, Retinopathy Eye Screening, Cardiac Rehabilitation, Mental Health) (see Appendix 6).

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 10
The care provided is not given consistently in a manner that the patient can understand or that fits their culture or world view of health (see Appendix 8). Improved staff cultural awareness and cultural competency need to occur, as our health region becomes increasingly multi-cultural.
The RQHR has identified Aboriginal Health as one of their overall strategic themes. Current achievements in this area include Native Health Services and establishment of the Eagle Moon Health Office.
PROPOSED STRATEGIES STRATEGY 4.5.1: Create a CDPM organizational structure to enhance linkages, coordination and communication across the various programs and services. STRATEGY 4.5.2: Maintain a CDPM Steering Committee to support integration and coordination, with appropriate sub-committee formation. STRATEGY 4.5.3: Establish a RQHR CDPM management position. STRATEGY 4.5.4: Identify a physician leader to work collaboratively with the CDPM manager. STRATEGY 4.5.5: Undertake team development efforts within and across CDPM teams as required. STRATEGY 4.5.6: Explore opportunities to facilitate improved collaboration and communication between physician specialists / specialized care teams and family physicians/ PHC teams. STRATEGY 4.5.7: Build strength through multi-disciplinary teams and/or multi-sectoral teams. Investigate incentives for specialists to work more collaboratively with teams and/or family physicians. STRATEGY 4.5.8: Develop a navigation system especially for high risk patients and those with multiple chronic conditions. STRATEGY 4.5.9: Enhance care provider awareness of CDPM, CDPM resources and tools, and CDPM programs and services in the region and community and identify mechanisms to keep practitioners up-to-date and well informed regarding current resources. STRATEGY 4.5.10: Ensure that community development approaches are part of planning within all CDM programs. STRATEGY 4.5.11: Investigate the benefits and feasibility of a single entry point for patients, whether one location or one central contact and referral point. Consider the benefits and opportunities of co-location for integration of programs and services.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 11
STRATEGY 4.5.12: Identify opportunities to deliver care using multiple care providers in a clinic format. STRATEGY 4.5.13: Develop a holistic approach by strengthening the mental health (depression care) component across every chronic condition program. STRATEGY 4.5.14: Increase the capacity of all CDPM staff to screen for depression (identify) and determine an appropriate plan to address mild to severe conditions. STRATEGY 4.5.15: Integrate mental health primary care supports / services into all CDPM programs. STRATEGY 4.5.16: Provide all chronic condition management programs with priority access to mental health expertise. STRATEGY 4.5.17: Expand collaborative care with psychiatrists. STRATEGY 4.5.18: Consider and implement extended hours of operation if identified as a community need. Strategy 4.5.19: Investigate the development of an Obesity Prevention and Management Program in partnership with other programs and agencies. STRATEGY 4.5.20: Utilize the principles of clinical practice redesign to improve access where wait lists exist. STRATEGY 4.5.21: Clearly identify and communicate the screening guidelines used for priority access to various CDM programs. STRATEGY 4.5.22: Develop a comprehensive and coordinated approach to screening and diagnosis for chronic diseases. STRATEGY 4.5.23: Enhance partnerships with the community to develop lifestyle programming. STRATEGY 4.5.24: Ensure all CDPM programs address the cultural and spiritual needs of patients as part of holistic care. Provide increased resources for traditional and pastoral services.
4.6 Decision Support In the ECCM, decision support is enhanced through the development and implementation of evidence-based guidelines, integrated care pathways and treatment protocols. These guidelines and protocols are shared with the patient. Specialists are paired with primary care providers to support the care of more complex patients.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 12
Likewise, primary care providers are also linked with health promotion professionals who have expertise in strategies for being well and staying well. RQHR CURRENT STATE
Relevant data and epidemiological reports from PPHS are not consistently used to assist with planning for chronic disease programs and services.
Evidence-based care guidelines for most chronic conditions are available, but are not consistently used by all practitioners throughout the RQHR.
Evidence-based guidelines are not consistently shared with patients. Care pathways exist within some programs but are lacking in others. Few
pathways address integration and/or coordination between programs and services. Specialist accessibility for primary care providers is variable, and dependent upon
the specialist. Reportedly, remuneration options are available to support telephone consults by specialists, but they are not always used.
A Shared Health Care pilot project involving a psychiatrist and family physicians is currently underway. This approach is widely supported in the literature.
Shared Care could also be enhanced through the development of care teams, within PHC sitesxii.
Barriers exist to the timely and simple transfer of information between specialists / family physicians / primary care practitioners / CDM programs. Additional jurisdictional barriers hamper communication with federally funded on-reserve care providers.
Lack of a method to easily share client information between care team members is an impediment to the flow of a client through the system and along the continuum of care.
RQHR has active Research and Performance Support and Quality Improvement departments to support limited quality improvement activities and outcome measurements in the CDPM programs.
PROPOSED STRATEGIES STRATEGY 4.6.1: Collect, share and utilize health data across the organization to support program-based decisions. STRATEGY 4.6.2: Implement systems that support dissemination and consistent use of established best practice guidelines and where needed, develop RQHR protocols in the absence of national or provincial best practice guidelines. STRATEGY 4.6.3: Explore the opportunities for Shared Health Care delivery models and were feasible, pilot and valuate their effectiveness. STRATEGY 4.6.4: Foster “care team champions” throughout the system. STRATEGY 4.6.5: Establish and maintain systems and process to support the collection, analysis and use of outcome data by all CDPM programs. This may require both human and technical resources.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 13
STRATEGY 4.6.6: Determine benchmarks for outcomes: use for comparison of patient outcomes and for planning services. STRATEGY 4.6.7: Employ regular patient experience surveys to provide opportunity for patient feedback.
4.7 Clinical Information Systems In the ECCM, clinical information systems are maximized and improved to support such things as care planning, shared access to client information, integrated scheduling, client access to resources, client registries and clinical reminders. They also help to monitor the performance of the care team and the care system. Clinical information systems are also used by health care providers to gather, share and use information about the communities in which their patients live, including such things as demographics, cultural, social and economic trends, community needs and strengths. RQHR CURRENT STATE
Currently a strategic plan for clinical information systems to support CDPM does not exist in the region.
Most programs and staff have access to a computer, however no access to information management programs which support CDPM. Key functionality such as client registries, recalls and reminders, team communication and monitoring of client outcomes does not exist.
Only a few of these information systems have patient care reminders built in (e.g. MIQS used in chronic renal insufficiency (CRI) and other renal programs).
The limited availability of electronic medical records (EMR) also hampers CDM. Currently only CRI and the Congestive Heart Failure (CHF) clinic have an EMR, and their function is limited to internal use.
The region is actively involved with the selection of a provincial PHC EMR System which has a CDM component. Reportedly it will be three to five years before this system will be widely available
The CDM Toolkit, used by physician practices involved in the Health Quality Council CDM Collaboratives will be available for use across a variety of chronic conditions in approximately four years.
The current lack of information systems hampers the ability to monitor team performance related to patient clinical and functional outcomes.
Some programs utilize spreadsheets to track some aspects of patient outcomes but this is time consuming and the lack of ability to analyze, share and utilize the results is problematic.
Many programs lack the necessary administrative support and IT expertise. Many CDPM staff do not have access to existing information management
programs such as PIP (Pharmacy Information Program), or the Lab Viewer due to lack of awareness, and/or internal and external policies.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 14
PROPOSED STRATEGIES STRATEGY 4.7.1: Develop a regional CDPM clinical information management strategic plan which will provide CDPM programs with full functionality to support best practices in client care, team communication and outcome measurement. The strategy will identify short term solutions to be used until the provincial PHC EMR and CDM Toolkit is available. STRATEGY 4.7.2: Ensure adequate administrative support in all CDM programs and expand IT expertise to implement and fully utilize current and future systems. STRATEGY 4.7.3: Work with the RQHR Information Technology department to develop processes/ policies to improve staff access to systems like PIP and Lab Viewer. STRATEGY 4.7.4: Standardize the collection and analysis of patient outcome measures.
5 Implementation Plan and Managing Change – Phase 1 The CDPM Strategy Steering Committee recognizes the collective and individual importance of these strategies; however it is clear that implementation must be appropriately sequenced and phased. Priorities for Phase 1, which is anticipated to occur over approximately one to two years, are as follows: STRATEGY 4.5.1: Create a CDPM organizational structure to enhance linkages, coordination and communication across the various programs and services. STRATEGY 4.5.2: Maintain a CDPM Steering Committee to support integration and coordination, with appropriate sub-committee formation. STRATEGY 4.5.3: Establish a RQHR CDPM management position. STRATEGY 4.5.4: Identify a physician leader to work collaboratively with the CDPM manager. STRATEGY 4.5.11: Investigate the benefits and feasibility of a single entry point for patients, whether one location or one central contact and referral point. Consider the benefits and opportunities of co-location for integration of programs and services. STRATEGY 4.6.1: Collect, share and utilize health data across the organization to support program-based decisions. STRATEGY 4.6.2: Implement systems that support dissemination and consistent use of established best practice guidelines and where needed, develop RQHR protocols in the absence of national or provincial best practice guidelines. STRATEGY 4.6.6: Determine benchmarks for outcomes: use for comparison of patient outcomes and for planning services.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 15
STRATEGY 4.6.7: Employ regular patient experience surveys to provide opportunity for patient feedback. STRATEGY 4.7.1: Develop a regional CDPM clinical information management strategic plan which will provide CDPM programs with full functionality to support best practices in client care, team communication and outcome measurement. The strategy will identify short term solutions to be used until the provincial PHC EMR and CDM Toolkit is available. STRATEGY 4.7.3: Work with the RQHR Information Technology department to develop processes/ policies to improve staff access to systems like PIP and Lab Viewer. The CDPM Steering Committee acknowledges that further consultation is required with the appropriate stakeholders to flesh out some of these strategies. In particular, more discussion is required about the CDPM organizational structure as well as the specific roles of the management position and physician leader, and whether the responsibilities of these positions should have operational or strategic responsibilities, or both. The committee agrees however, that in order to effectively implement this Healthy Living strategy a dedicated management position is needed.
6 Budget The following chart reflects the costs that are known at this time to implement Phase 1, including establishing a CDPM management position and a physician leader, and employing the PACIC tool to obtain patient feedback.
Description 2008-09 Baseline
$000s
2009-10 Cost/
(Saving) $000s
2010-11 Cost/
(Saving) $000s
2011-12 Cost/
(Saving) $000s
2012-13 Cost/
(Saving) $000s
OOS CDPM Management position
80 108 111 117
Physician CDPM leader 30 50 51.5 53Clerical and consumables 10 20 21 22PACIC Tool Administration 10 10 10 10Total Cost/(Saving) 130 188 193.5 202 The Manager and physician co-leader position would be advertised upon funding. It is expected that it would take until July 1, 2009 to recruit the manager and September 1, 2009 for the physician. Financial data assumptions and notes: • capital - computer and office set up • 1 OOS manager: assumed that start date would be July 1, 2009, and a step increase
and inflation of 3% per year • 0.2 of a physician FTE 3% per year increase. • There are no expected savings or impact on other agencies.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 16
7 Conclusion The burden of chronic conditions and the negative impact on individuals, families and society is increasing as the number of new cases continues to grow every year. Turning this around takes time. The process of change can be slow, and therefore we need to prepare now. This Healthy Living strategy provides a sound framework and reasonable approaches for moving toward a more collaborative and coordinated system of service delivery; for getting from where we are now to where we want to be. We have identified our priorities for action, the required human and financial resources to get us started and the indicators we will use to measure our progress. The RQHR is well positioned to implement this strategic plan. We have many dedicated managers and staff committed to CDPM and we have valuable relationships with a number of important community partners. The upcoming months will be very exciting as more detailed planning occurs and the Phase 1 strategies are implemented. Ten years from now, people served by RQHR CDPM programs will be healthier. They will experience better coordination and integration of our services, more effective linkages between the RQHR and the broader community, and they will reap the benefits of enhanced evidence-based practice.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 17
8 References i Canadians’ Experiences with Chronic Illness Care in 2007, A Data Supplement to Why Health Care Renewal Matters: Learning from Canadians with Chronic Health Conditions. Health Council of Canada. ii The Chronic Care Model website: http://www.improvingchroniccare.org iii Population Patterns of Chronic Health Conditions in Canada-Health Council of Canada-December 2007. A Data Supplement to Why Health Care Renewal Matters: Learning from Canadian with Chronic Health Conditions. iv A Health Profile of Saskatchewan Seniors, Population Health Branch/Community Care Branch, Saskatchewan Health, Canada, 2006) www.health.gov.sk.ca/mc_publications.html ISBN 1-55157-051-3 v Statistics Canada, 2003, 2007 Indicator Profiles from the Canadian Community Health Survey, Canada. Catalogue No. 82-221-XWE2008001 vi Barr, V.J., Robinson, S., Barin-Link, B., Underhill, L., Dotts, A., Ravensdale, D., Salivaras, S. (2003). The Expanded Chronic Care Model: An Integration of Concepts and Strategies from Population Health Promotion and the Chronic Care Model. Hospital Quarterly. Vol 7, No 1. vii Canadian Institute for Health Information, Health Indicators 2008 (Ottawa: CIHI, 2008) Focus on Ambulatory Care Sensitive Conditions. ISBN 978-1-55465-270-9 (PDF) viii Canadian Institute for Health Information, Health Indicators 2008 (Ottawa: CIHI, 2008 Reducing Gaps in Health: A Focus on Socio-Economic Status in Urban Canada. http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=media_24nov2008_e ix Improving Chronic Disease Management in your Community: a six step strategy to assist you on your journey. An initiative of Trillium Health Centre in partnership with many others. Sponsored by PRIISME™, an initiative of GlaxoSmithKline Inc. March, 2008. x Accreditation Canada’s Website: https://www3.accreditation-canada.ca/OrgPortal/Node_TMQPR.aspx?index=17 xi RQHR’s Primary Health Care: Strategic Plan 2008-2013. Submitted to Saskatchewan Ministry of Health, October 2008. xii Healthier Places to Live, Work and Play. A Population Health Promotion Strategy for Saskatchewan. www.health.gov.sk.ca

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 18
APPENDIX 1 RQHR Chronic Disease Prevention and Management Strategy Committee
Marci Scott Primary Health Care Strategic Planner Co-Chair Karen Butler RQHR Diabetes Initiative and MEDEC Manager Co-Chair Sharon Banning Urban Primary Health Care Manager Glorianne Bjerland Manager, Home Care- Nursing Areas 10 and 20 Jody Burnett Chronic Disease Management Collaborative Facilitator Stephanie Cook Manager Clinic Nutrition Services Heather Dorgan Manager Rural Community Health Anna Engel Manager Health Promotion Morag Granger Manager, Public Health Nursing, Population and Public Health Dr. Maurice Hennink Deputy Medical Health Officer, Population and Public Health Services Chris Horton Manager Renal Program Dorothy Lloyd Aboriginal Health Consultant: Eagle Moon Health Office Karen McDermaid Manager Rural Pharmacy Services Brad McDougall Quality Assurance Colleen Molnar Manager, Mental Health Clinic Sheryl O’Quinn Manager Respiratory Services Dr. Elan Paluck Director Research and Performance Support Maggie Petrychyn Rural Primary Health Care Manager Bill Semchuk Manager Clinical Pharmacy Linda Slotsve Coordinator Cardiac Rehabilitation Charlene Talbot Eye Centre Colleen Gaudio Recorder: Confidential Administrative Assistant Joyce Butler Guest Facilitator: Primary Health Care Development Consultant
Strategy Development Workshop Oct 21’08 Strategy Development Workshop Nov 4’08

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 19
APPENDIX 2 Stakeholders Consulted throughout the Chronic Disease
Prevention and Management Strategy Development Process Zahid Abbas .......................... Epidemiologist, RQHR Dr. Ram Abdulla ................... Head, Department of Medicine, RQHR Dr. Geeta Achyuthan ............ Primary Care Physician, RQHR Bev Alfano............................. Manager, Eye Centre, RQHR Karen Barber ........................ Director of Quality Improvement, Health Quality Council, SK Phyllis Bend .......................... Coordinator Cardiac Rehab and Risk Reduction, University of Regina. Jan Besse .............................. Executive Director, Neuro, Rehab and Long Term Care, RQHR Judy Bird............................... Representative Eagle Moon Health Office, RQHR Bev Birns............................... Manager Home Care and Community Services Rural Areas,- Population and Public
Health, Fort Qu’Appelle, RQHR Sharon Bishop....................... 5A- Stroke Prevention Clinic Dr. Lourens Blignaut ............ Incoming PHC Medical Consultant-Primary Care Physician, RQHR Dr. John Brown .................... Program Manager Adult Therapy, Mental Health Clinic, Mental Health and Addictions
Services, RQHR Lenore Bryant ....................... Manager Home Care Rural Areas- Broadview, RQHR Myrna Bye............................. Manager, Hemodialysis Unit, Renal Program, RQHR Lorri Carlson ........................ Manager, Mental Health and Addictions Services, RQHR Lisa Clatney .......................... Program Director: COPD/Depression/Access, Sask. Health Quality Council Arthur Colclough .................. Manager Special Projects- Information Technology, RQHR Bob Croft .............................. Croft Planning and Design; Specialty Chronic Disease Centre Ken Dornstauder................... Manager, Therapy and Adult Rehabilitation, RQHR Vicki Ehrlich ......................... Manager, Congestive Heart Failure Clinic, RQHR Virginia Elliott ...................... Manager Information Technology- RQHR George Fayant ...................... Representative Eagle Moon Health Office, RQHR Gwen Gordon........................ Director of Health Promotion, Saskatchewan Heart and Stroke Foundation Brian Graham....................... President and CEO, Saskatchewan Lung Association Janice Haffner ...................... Vice-President of Health Initiatives, Saskatchewan Lung Association. Dave Hedlund ....................... Executive Director, Mental Health and Addictions Services Brenda Homes ...................... Pediatric Out-Patient Asthma Program, RQHR Brenda Jackman ................... Saskatchewan Ministry of Health. HEALTHLINE-Online Cora Jensen .......................... Associate Director of Health Promotion, Heart and Stroke Foundation of Saskatchewan Randy Knapp ........................ Executive Director- Information Technology Dr. Barb Konstantynowicz.... Primary Care Physician, RQHR Barb Layton .......................... Manager Screening Program for Breast Cancer Early Detection, Population Health
Division, Saskatchewan Cancer Agency. Deanna Mantee..................... Student Representative, Eagle Moon Health Office, RQHR Sarah Matysio....................... Croft Planning and Design: Specialty Chronic Disease Centre Dr. Stuart McMillan ............. Outgoing PHC Medical Consultant-Primary Care Physician, RQHR Dr. D.R. Murthy.................... CHF Clinic, RQHR Terry Nielson ........................ Intake Program Manager, Mental Health Clinic, Mental Health and Addictions Services,
RQHR. Glenda Popowich.................. Clinical Program Manager HealthLine - Telephone Michael Redenbach............... Vice President, Primary Health Care, RQHR Kimberley Schmidt ................ Manager, Saskatchewan Health Information Network (SHIN). Donna Smeets ....................... Service Supervisor, Home Care Rural Areas, Broadview, RQHR Rebecca Toye ........................ Director, Therapy Services Acute Care, RQHR Dr. Chris Vuksic ................... Senior Medical Officer for Medical Services-Primary Care Physician, RQHR Dale Young ........................... Manager Population and Public Health, Podiatry, RQHR

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 20
Health Promotion
APPENDIX 3 Population and Public Health Services: Strategic Priority: Program Areas:
Nutrition Active Living Partners for Healthy Living
Tobacco Control Seniors Healthy Living Program Dental Health
Education & Awareness ▪ Presentations, displays, media (based on request) ▪ Weekly newspaper columns (provincial0 ▪ Resource Development: - Food Criteria Document - Menu Planning ▪ Nutrition Month Campaign ▪ Grocery Store Tours ▪ Regional publications (e-link; Health News, etc.)
▪ Presentations, displays, media (based on request) ▪ Resources (Regina Seniors Active Living Guide) ▪ Active Living Promotion (brochure; busbacks; ad for theatres) ▪ Family Symposium
▪ Smoke-free Workplaces Media Campaign ▪ Presentations and media interviews as requested ▪ Smoke-free Homes, Cars, MUD’s ▪ Cessation: Quit Smoking Packages ▪ Regional publications (e-link; Health News, etc.)
▪ Educational Sessions on a variety of health and cultural diversity topics targeting seniors ▪ Seniors Wellness Groups (Rural West) ▪ Displays and media (as requested)
▪ Presentations, displays, media (based on request) ▪ Dental Health Month Campaign ▪ Educational Session: Spit Tobacco ▪ Dental Health Education Resources ▪ Regional publications (e-link; Health News, etc.)
Strengthening Communities/Building Capacity
▪ On-line self-study course for Nutrition Coordinators ▪ Healthy foods in Schools: Making Healthy choices the Easy Choices Toolkit ▪ Body Image Kits ▪ Friendship Centre Nutrition Workshops & Food Policy (Rural West) ▪ Teacher Workshops ▪ * Hello Parents! (Public Health Nursing) ▪ * Prenatal Program ▪ * Healthy Lifestyles Program (Al Ritchie)? ▪ * TOPS (Al Ritchie) ▪ Food Security Initiatives ▪ * Preschool Activity/Healthy Eating Project – PAINT (Rural East) ▪ * School Nutrition Kits (Rural East)
▪ Activity Club ▪ Senior Physical Activity Sampler ▪ Positive Steps Fall Prevention & Exercise Program ▪ Active Living Toolkits (for schools & preschools) ▪ * Playground Leadership Program (Rural East) ▪ Active Living Workshops (Rural East) ▪ Moving Towards Health and Happiness Workshops ▪ Literacy Education Activity and Play (LEAP) Master Training Workshop ▪ * Preschool Activity/Healthy Eating Project – PAINT (Rural East) ▪ * School Nutrition Kits (Rural East)
▪ * Smoking Cessation Counseling (Al Ritchie) ▪ Contraband ▪ First Nations/Metis Support ▪ Counter Advertising ▪ Smokeless Tobacco ▪ Partnership/support for the Pharmacists’ Association of SK and its PACT Program
▪ Fluoride Mouth Rise Program (FMR)
Supportive Social & Physical Environments
▪ * Healthy Food of the Month Program (rural) ▪ * Breastfeeding Support Centre ▪ * Food For Life Store (Al Ritchie) ▪ * Brain Snacks ▪ * Cooking Circle (Four Directions)
▪ in motion workplaces ▪ Workplace in motion (Grenfell Health Centre) ▪ Ready Set Go ▪ Built Environments ▪ Alternative Transportation ▪ * Lifestyle Promotion ▪ * Drop-in activity classes (Four Directions) ▪ * Hip Hop Step (Four Directions)
▪ Dental Health Day (4D)
Healthy Public Policy ▪ School Food Policy ▪ RQHR Food & Nutrition Policy ▪ Food Costing Report ▪ Baby Friendly Initiative ▪ Infant and Child Nutrition & Growth Standards ▪ Community Food Security Public Policy Statement
▪ RQHR CHC Physical Activity Guidelines ▪ in motion Daycares ▪ Whitmore Walkers ▪ in motion (Rural West)
▪ Policy Papers ▪ Ban Tobacco Advertising & Promotion ▪ SAHO resolution ▪ Smoke-free Homes, Cars, MUD’s ▪ Cessation ▪ Tobacco Taxation
▪ SAHO Resolutions
Knowledge Development & Exchange (includes research & surveillance)
▪ School Food Policy Indicator ▪ Nutrition Update Newsletter ▪ In-services to Public Health Nurses; Educations Students at University of Regina ▪ Presentations to Annual General Meeting; Management Meetings; Board; etc. ▪ Preceptor for dietetic interns
▪ In-services to Public Health Nurses ▪ Presentations to Annual General Meeting; Management Meetings; 2008 in motion Manulife National Physical Activity Institute, etc. ▪ Preceptor for Kinesiology Students
▪ Presentations to the Board; MHO’s; 5th National Conference on Tobacco or Health (2007); etc. ▪ Tobacco Free Saskatchewan Network
▪ Preceptor for Nursing Students ▪ Dental Health Screening Program Report ▪ Spotlight on Oral Health Newsletter ▪ In-services to Public Health Nurses. Schools, etc. ▪ Presentations to Annual General Meeting; Management Meetings; etc.
Assessment /Treatment ▪ * Child Health Clinics ▪ * Parenting Plus (Rural East) ▪ Blood Pressure Checks
▪ Flu Clinics ▪ Screening & varnishing services for high risk children in schools & preschools ▪ Consultations
* Health promotion provided by other departments/sites

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 21
Draft: March 05, 2008 Evidence-Based Practice:
Healthy Public Policy; Creating Supportive Environments; Strengthening Community Action
Nutrition: On-line self-study course for Nutrition Coordinators: The course was developed by the PHNSWG and will provide support and training in healthy eating for nutrition coordinators in schools across Saskatchewan. The course will be pilot-tested in a number of schools across the province. An RQHR Public Health Nutritionist will oversee piloting this course at Herchner School in Regina for January 2008. Healthy Foods in Schools: Making Healthy Choices the Easy Choices Toolkit: PHNSWG developed the kit to complement the goal of healthier school food environments and school food and nutrition policies. The kit is promoted by local Public Health Nutritionists within each health region. It is also available at the Heart and Stroke Foundation website. There are a total number of 4 kits within the RQHR, including 2 for Regina and one each for rural areas (Grenfell; Fort Qu’Appelle). Body Image Kits: Two new kits are available for schools and community; one for Grades 4-6 and one for Grades 7-9. Friendship Centre Nutrition Workshops & Food Policy (Rural West): RQHR Community Dietician and File Hills Community Dietician provides workshops for youth and staff at the Qu’Appelle Valley Friendship Centre including meal preparation, nutritious ingredients and cooking techniques. RQHR Community Dietician reviews menus and food choices made by the Qu’Appelle Valley Friendship Centre’s staff. Targets First Nations youth between the ages of 15 and 24 years of age. Teacher Workshops: Hello Parents!: Free weekly drop-in session for parents of babies under 1 year of age and topics range from positive parenting to feeding your baby, baby’s growth and development, etc. Offered Tuesday afternoons at PPHS North Office and Thursday afternoons at the East Office. Prenatal Program: Healthy Lifestyles Program: Meetings are once a month in the evening. This program, facilitated by the Centre’s nutritionist, offers a supportive group environment for women who are concerned about weight loss. Guest speakers are often brought in to discuss topics of interest to the group. Past topics have included meal planning, label reading, physical activity and healthy eating. TOPS Group: The Centre offers it space to a Take Off Pounds Sensibly group. They meet every Monday at the Centre. Most members live in the Al Ritchie community. Food Security Initiatives: RQHR Public Health Nutritionist provides consultation and representation for food security initiatives within RQHR, SK and Canada, including Food Secure Saskatchewan. The Public Health Nutritionist was invited as partner to provide food security advice on a Sustainability Action Plan for the core Neighborhood in Regina. PPHS Sask. Rep on The National Advisory Committee (NAC) on Food Security Projects (NSNC/AHPRC) led to development of food security research tools : 1) “Thought About Food? A Workbook on Food Security & Influencing Policy” 2) Food Costing, 3) DVD (CPNP). NAC food security research tools were: a) nominated for a national Communications Award b) used to conduct food costing within RQHR & SK c) piloted in SK (train the trainer model) d) were used in conjunction with three roundtables on food security e) used to develop food security inventory in regions. A description of RQHR food security initiatives is available electronically on the Food Secure Saskatchewan website. Attendance by RQHR community members at the 2006 train-the-trainer workshop contributed to the formation

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 22
of the first local neighborhood partnership, resulting in the Al Ritchie Food for Life Store. Health promotion seed money served to attract initial funding from outside stakeholder. In-kind financial and nutrition consultation help sustain community’s efforts. Policy and costing tools have been developed in consultation with and for use by stakeholders at provincial, regional and neighbourhood levels. The Food Costing Report was completed spring 2006; report available on RQHR website. Food security network created during round tables, enabling RQHR communities & institutions to be part of a larger integrated provincial strategy. Neighborhood-driven Food for Life Store continues to make fresh food available to the community. Food Inc.: a feasibility study conducted by U of R MBA student which led to the formation of community-driven R Mobile Store. Preschool Activity/Healthy Eating Project –Physical Activity, Information, and Nutrition Tips (PAINT): The pilot project was developed to improve health and prevent chronic disease through increasing physical activity and healthy nutrition for pre-school children. Results of the Early Development Instrument survey done through Prairie Valley School Division indicated that overall, kindergarten children in the school division are arriving at school with a below desirable school readiness indicator in the domain of physical well-being, gross and fine motor skills. The program is targeted to informal day care providers and pre-school programmers in Grenfell, Wolseley and Broadview areas. These groups were surveyed for knowledge level and recognition of their role in providing activity and healthy nutrition for children in their care, and a workshop was developed with their input. A Physical Activity/Healthy Eating Kit was developed and workshop participants will be trained on how to use the resource. School Nutrition Kit (Rural East): Resources for teachers to increase knowledge of and promote healthy eating, active living and healthy body image. Healthy Food of the Month Program: Nutrition services in Grenfell are working to increase access to nutritious foods by working collaboratively with grocery stores to feature (bring into stores) one healthy/healthier food option each month. The program was piloted in Grenfell in 2007 with plans for expansion to other communities within RQHR Rural East for 2008. Breastfeeding Support Centre: Breastfeeding mothers and babies are invited to drop-in for free advice and practical help from a lacatation consultant or public health nurse. Open Wednesdays at PPHS North Office and Fridays at Maternity Visiting Program at RGH. Food For Life Store: The Al Ritchie Health Centre is a key partner in this community driven initiative. The Food For Life Store offers a variety of fresh fruit and vegetables as well as dairy products, bread, pasta and ground beef to residents of the Al Ritchie neighbourhood. The store operates on a non profit basis which allows prices to remain low. The store is open every Monday from 10:30 a.m. to 2:30 p.m. and is operated by volunteers and supported by a volunteer board of directors made up of community residents. Partial funding is provided by Conexus Credit Union and the Regina Qu’Appelle Health Region. Brain Snacks: Brain Snacks: Food and Nutrition Services Dietitians provide 30-minute lunch-and-learn sessions on a variety of nutrition topics. Each presentation features a healthy food item which will be served at the session as well as in the cafeterias at the RGH, PH and WRC. Sessions will take place in several region locations, including one rural setting and a telehealth session. Cooking Circle: 4D Healthy Lifestyles Support Group: Provides nutrition and activity education in a supportive environment aimed at weight loss and healthy lifestyles. School Food Policy: Regional Public Health Nutritionists and Community Dietitians in collaboration with the PHNSWG continue to work with schools and school boards as they develop healthy food/nutrition policies and guidelines to improve access to healthy food choices in school environments. To further support the policy work within schools, the region established a Public Health Services School Nutrition Committee in 2006. The PHNSWG have established the School Food Policy Health Promoter Indicator project to collect data to track the number of school food and nutrition policies within RQHR and the province. RQHR Food & Nutrition Policy: It has been recognized that health regions play a critical role in influencing food choices and modeling healthy behaviours. RQHR Public Health Nutritionists have been the leads in advocacy work that has led up to the current Food and Nutrition policy work within RQHR. They facilitated the successful submission and support of a SAHO resolution in 2006.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 23
They developed a poster presentation resource with Media Services called “Leading by Example- Health Region Food and Nutrition Policies”. In 2007, Population and Public Health Services in partnership with Nutrition and Food Services began preliminary discussions to increase accessibility of healthy food choices within RQHR workplaces. Development of a policy framework is planned for early 2008, with implementation and evaluation to follow. Food Costing Report: Food costing is important as a food security advocacy tool when planning for healthy eating. It outlines basic food costs for individuals and families in the province. The 2006 Food Costing Report was completed by PHNSWG and disseminated by RQHR Public Health Nutritionists within RQHR and the community in 2007. The next report is due in 2008. Baby Friendly Initiative: The Regina Health District (RHD) approved Policy 1.1.1 Breastfeeding and the Baby Friendly Initiative (BFI) in 1995 – a first in Saskatchewan. RQHR working toward BFI designation in hospital and community by 2012 or sooner RQHR follows internationally recognized best practice standards. Public Health Nutritionist provides RQHR representation on provincial and regional Breast Feeding committees, including the RQHR Breastfeeding Advisory Committee. The goal is to have RQHR designated as Baby Friendly by 2012. On-going and current BFI work includes: 1) RQHR follows internationally recognized best practice standards 2) 3 informational brochures have been developed 4) an additional Breastfeeding Support Centre was added to address the increased need for support services with families with breastfeeding concerns; and commencing 2008, RQHR facilities will pay fair retail price for all infant nutritional products offered within these facilities. Infant and Child Nutrition and Growth Standards: Public Health Nutritionist provides representation on the PHNSWG Early Childhood Committee who: 1) develops, revises, trains, and oversees implementation of nutrition and growth standards and protocols in collaboration with nursing and other health providers; ensures that resources support standards and are consistent with breastfeeding and BFI policy; collaborates with nursing managers and provides input to provincial nursing guidelines for CHC’s; contributes to national position statements directly or through CPS and adopts them for provincial implementation. Public Health Nutritionist reviews SK HealthLine protocols. Community Food Security Public Policy Statement: RQHR Public Health Nutritionist participated in the development of a Community Food Security public policy statement/position paper for Dietitians of Canada. School Food Policy Indicator: RQHR Public Health Nutritionist, in affiliation with the Public Health Nutritionists of Saskatchewan Working Group have established the School Food Policy Health Promoter Indicator project to collect data to track the number of school food and nutrition policies within RQHR and the province. Child Health Clinics: Child health clinics are available throughout the region. In addition to immunization, Public Health Nurses provide developmental and healthy weights screening and promote nutrition and activity. Parenting Plus: This is a home visitation and family support program for parents with newborns in the Rural East part of the RQHR (includes 5 First Nations communities). Program staff consist of 3 Family Support Workers and a Program Manager. The program was developed in response to the evidence that: 1) this area has lower than provincial average levels of income and education, higher rates of use of social assistance and increasing numbers of single parent families and 2) importance of first years of life in development of high levels of health. The home visiting curriculum is also used by KIDS First and includes nutrition and active living components.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 24
Active Living: Active Living Promotion: The *Region in motion Communications Committee received funding (from Saskatchewan in motion) to develop a communications strategy. Components of the 2007 strategy included: 1) a brochure “Smart Start” targeting inactive adults 2) Bus Boards to promote SummerActive and the Regina in motion website 3) an Ad to run prior to each movie at the Rainbow Cinema 4) submissions to the City of Regina Leisure Guide and Physicians Newsletter on upcoming events and availability of new resources and 5) re-design of their website. Family Symposium: The Active Living Health Promotion Coordinator works collaboratively on the Regina in motion (RIM) Preschool Committee. This community event is part of a larger preschool strategy and a Family Symposium with Silken Laumann is planned for May 2008 to create awareness of childhood inactivity. Activity Club (formerly known as the Walking Club): This is a self-directed program that encourages non-competitive activity within schools and communities. Teachers are invited to implement a walking program in schools with resources and information package. A mail-out is completed to 150 schools within the RQHR annually. The program is also promoted rurally. Senior Physical Activity Sampler: Since 2001, the *Regina in motion Older Adult Committee has coordinated a community-wide event for seniors to access exercise instruction and recreation opportunities. Seniors also develop new skills by trying various types of activity including ballroom dancing, container gardening, laughter yoga, group exercises, etc., offered at the event. Positive Steps Falls Prevention & Exercise Program: Since 2000, resources have been developed and distributed to provide information and awareness on falling including Positive Steps Fall Prevention handbook, DVD’s and videos. Active Living Toolkits: Active Living resources are made available in a toolkit for elementary and high schools to incorporate physical activity into existing programs. There are 2 kits available within the RQHR. Preschool Active Living Toolkits: Active Living resources are made available in a toolkit for preschools and daycares to incorporate physical activity into existing programs. There are 2 kits available within the RQHR. Playground Leadership Program: Program goals are to: 1) provide opportunity for children to increase their physical activity by learning new games and having fun 2) encourage positive attitude towards physical activity and 3) reduce bullying. In 2006, RQHR Health Promotion Coordinators in partnership with South East Saskatchewan Association for Culture, Recreation and Sport (SECARS) piloted this program and provided training to school facilitators and youth leaders. There are plans to expand the program to Regina. Active Living Workshops: The Qu’Appelle Valley Friendship Centre in partnership with File Hills Qu’Appelle Tribal Council and RQHR Community Services provides Active Living workshops for First Nations Youth between the ages of 15-24. Moving Towards Health and Happiness Workshops: The Active Living Health Promotion Coordinator works collaboratively on the Regina in motion (RIM) Preschool Committee. Workshops are part of a larger preschool strategy and provided for care givers to incorporate daily physical activity into existing daycare and preschool programs.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 25
Literacy Education Activity and Play (LEAP) Master Training Workshop: The Active Living Health Promotion Coordinator works collaboratively on the Regina in motion (RIM) Preschool Committee. Workshops are part of a larger preschool strategy and will be provided in 2008/09 to teach public health professionals, day care owners/workers, educators, etc. to train people to lead LEAP workshops in their communities. The goal is to have 5 master trainers each for Regina and Saskatchewan trained to deliver LEAP workshops. School Nutrition Kit (Rural East): See Nutrition. Preschool Activity/Healthy Eating Project –Physical Activity, Information, and Nutrition Tips (PAINT): See Nutrition. in motion Workplaces: The Partners for Healthy Living work collaboratively on the *Regina in motion Workplace Committee. This committee works to increase the number of workplaces that are designated as in motion. As a region RQHR has declared themselves in motion, and their *Lifestyles Committee in turn works with RQHR sites to assist them in achieving their in motion designation. Workplace in motion (Grenfell Health Centre): Develop Activity Room and provide in motion lunch n’ learns and events (as identified by staff). Ready Set Go: In partnership with the YMCA and Access Communications, an exercise instruction program is available to seniors in their home on local Channel 7. It can be used as a winter activity alternative for seniors. Six original shows have run in 3 different time slots per week since 2006 and is on-going. The show has been taped is available on DVD and there are plans to complete another series of 6 exercise sessions for winter 2008-2009. Built Environments: Health Promotion staff work collaboratively on several Regina in motion (RIM) committees. Built environments that facilitate more active lifestyles and reduce barriers to physical activity are desirable because of the positive relationship between physical. RIM established a new *Regina in motion Built Environments Committee in 2007. This committee attended consultation and planning meetings with the city of Regina and stakeholders in the Regina Downtown Redevelopment planning in December of 2007 and will participate in follow-up meetings in March of 2008. Other work planned for the committee includes: 1) the development of “Built Environment” public education materials 2) provision of public education forums on the importance of built environments and 3) development of an advocacy strategy appropriate for various target groups including City Councillors, School Board Officials, Developers, etc.
Alternative Transportation: Promotion staff work collaboratively on several Regina in motion (RIM) committees. The *Alternative Transportation Subcommittee is a subcommittee of City of Regina’s Green Ribbon Community Climate Change Advisory Committee. City-wide initiatives from this committee include: 1) walk, bike and ride survey to identify the barriers that keep Regina residents from using alternative transportation modes 2) promotion and support for new bike lanes in transition area and other parts of the city 3) carpooling and linking of carpoolers via website and 4) the Mitsubishi City Chase (hosted in Regina in Aug. 2007). A car sharing cooperative is being examined. Lifestyle Promotion: Employee Health and Safety Services promotes healthy lifestyle choices for all RQHR employees and encourages them to foster healthy lifestyles within their families and communities. Lifestyle Promotion Supports in motion initiatives; provides resources for employees including the “Body Bulletin” publication; and supports Fitness Classes and facilities within the RQHR. RQHR Child Health Clinics (CHC) Physical Activity Guidelines: Physical Activity Guidelines were developed and integrated into existing CHC protocols. The guidelines are a tool for Public Health Nurses to use and distribute during CHC visits. DVD’s were developed for CHC’s to play in waiting areas during parent visits. Complimentary resources are to be developed including a poster for each CHC and information sheets for parents. in motion Daycares: The Active Living Health Promotion Coordinator works collaboratively on the Regina in motion (RIM) Preschool Committee. Work is being done to add a physical activity component as one of the standards in the licensing process. Daycares who meet the criteria will be designated as in motion Daycares.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 26
Whitmore Walkers: in motion (Rural West): Work with workplaces, communities, senior groups and schools to encourage and activate in motion policy.
Tobacco Control: Smoke-free Workplaces Media Campaign: The goal of the 2008 campaign (January 20-26th) was to alert the public and provincial policy makers that 1 out of every 3 Saskatchewan workers works in an environment that is not smoke-free and the threat to workers’ health. The advertisement was utilized by other health regions and the Canadian Cancer Society and was run throughout the province. RQHR will also partner with the Smokers HelpLine and the Regina Leader Post to promote Weedless Wednesday, January 23. Smoke-free workplaces will also be promoted on World No Tobacco Day, May 31, 2008. Smoke-Free Homes, Cars, Multi-unit Dwellings (MUD’s): Work with the Canadian Smoke-Free Housing Coalition to promote smoke-free MUD’s. Provide information to the public and stakeholders on this emerging issue. Develop and implement strategies to promote smoke-free areas in homes and support a public-supported law to ban smoking in cars with children. Cessation: Health Promotion provides “quit smoking” information/packages (7 Ways to make quitting easier) and support to clients & residents (available on the website at rqhealth.ca). Initiate steps to develop cessation policy for RQHR patients, clients, residents and staff. Smoking Cessation Counselling: Dr. Bromley attends the Al Ritchie Centre Thursday and Friday afternoons to offer smoking cessation therapy. His appointments are usually for one hour with an average of three to four sessions being required for optimum results. Contraband: Educate health workers and others about the problems of contraband in Saskatchewan. First Nations/Metis Support: Identify strategies to support tobacco reduction strategies within First Nations and Metis communities. Counter Advertising: Operate the Tobacco Free Saskatchewan Network [TFSN] to provide health workers and others with information about tobacco reduction activities in Saskatchewan and tobacco industry activities Smokeless Tobacco: Use results from Smokeless Tobacco Survey to initiative prevention initiatives with youth. Partnership between Dental Health Coordinators and the Canadian Cancer Society to provide educational session targeting youth (Grade 9’s) in Saskatchewan around spit tobacco. Partnership/support for the Pharmacists’ Association of SK and its PACT Program: Letter drafted and sent to support the Pharmacist’s Association of SK and their PACT program (Partnership to Assist with Cessation of Tobacco). Program outlines a broad, pharmacy-based strategy to screen, recommend therapy and provide follow-up to support behavior change regarding tobacco use. There are 32 trained PACT pharmacists throughout Saskatchewan 97 in Regina and 5 in Saskatoon.. Future plans for PACT include training more pharmacists and more tobacco users successfully quitting with the support and counseling of a pharmacist. Policy Papers: In 2004, a report (“Building on Successes: Reducing Tobacco Use in Saskatchewan, Recommendations for 2008-2010”) identified the most effective tobacco reduction strategies. In 2008, a follow-up report on best practices has been developed (“Building on Successes: Reducing Tobacco Use in Saskatchewan”) and will be distributed to health groups and policy makers.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 27
Ban Tobacco Advertising and Promotion: Support and promote precedent-setting ban on tobacco product displays. Monitor implementation of the Tobacco Control Act and identify concerns. Support proposed federal regulations to ban displays. SAHO Resolution: In 2007, the Health Promotion Coordinator facilitated the successful submission and support of an RQHR resolution to SAHO which was passed by delegates at the annual meeting. The resolution supported amending OH&S and Regulations to provide 100% smoke-free workplaces for all Saskatchewan workers. Tobacco Taxation: Monitor tobacco taxes across Canada and if necessary, work with health group to support taxation. Tobacco Free Saskatchewan Network: Distribution list of over 200 people around the province and nationally. It provides information about tobacco control issues and call to action when required. It keeps people informed/up-to-date on issues. Seniors Healthy Living Program: Educational Sessions: Public Health Nurses, through partnerships with many community partners, provide educational sessions to seniors on a number of health topics. The program is coordinated throughout the Regina community and is free of charge (registration is not required). Seniors’ Wellness Groups (Rural West): Education sessions offered in conjunction with Home Care clinics by professionals within RQHR and external to RQHR. Blood Pressure Checks: Public Health Nurses provide blood pressure checks in some of their educational sessions. Flu Clinics: Public Health Nurses coordinate and are involved in adult community immunization clinics within Regina.
Dental Health: Educational Session: Dental Health Program supports and partners with the Canadian Cancer Society, who will deliver educational sessions targeting Grade 9 students on chew tobacco (October 2008). Gruen VonBehrens will visit 10 communities around the province to talk to grade 9 students about the danger of using chew tobacco. Fluoride Mouth Rinse Program: There are 37 school based fluoride mouthrinse programs (18 in Regina, 19 rural). Basically the criteria is that the programs are implemented in “high risk” schools (20% of the children screened had obvious decay). Implementation can often depend on the support and cooperation of the principal and school staff. The grades participating range from Kindergarten to Grade 9 and vary from school to school. Only children who have returned a signed consent card are able to participate. Of the eligible 3,147 children (meaning the number of children in the participating grades) there are 2,832 children rinsing for a combined participation rate of 89.9%. One of the greatest challenges can be finding “volunteers” to run the programs (volunteers are supervised by a Dental Health Educator/Coordinator). In the participating schools there are a total of 28 school staff and 2 community volunteers who mix and dispense the rinse. (51 students help in one way or another). The cost for each child to participate is relatively inexpensive (approx. cost per child $1.50/year). There is an initial start up cost for the trays, jugs and pumps, file boxes etc. The fluoride powder, tissue, cups, garbage bags consent cards etc .are ordered in June for the following school year.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 28
Dental Health Day: The Dental Health Coordinators in partnership with Four Directions, will be providing screening and varnishing services one day per month. The services are free of charge for clients of Four Directions and will be promoted on site. SAHO Resolution(s): SAHO resolution in 2007 for provincial children’s dental health program. SAHO resolutions in 2008 for: 1) provincial children’s dental health program and 2) examination of the key components of a health services model that will improve the oral health of seniors, but of particular benefit to seniors who are homebound, disadvantaged or institutionalized. Dental Health Screening Program Report Kindergarten and Grade One 2003-2004: A Dental health Screening was conducted during the 2003-2004 school year to assess oral health needs and to identify children in need of dental treatment. The next survey will be 2009. Screening and Varnishing Services: Dental Health Coordinators have identified and targeted high dental risk/need schools through the process of the screening program. Dental screening and varnishing services are provided to children in these schools. Children are monitored through selective screenings, referrals and individual follow-up. Consultations: Consultations with parents as a result of referrals from heath professionals and concerned individuals.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 29
APPENDIX 4
CHRONIC DISEASE MANAGEMENT PROGRAMS & SERVICES INVENTORY
May 6, 2008
Prepared by Joyce Butler Development Consultant
Primary Health Care Initiatives

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 32
TABLE OF CONTENTS
INTRODUCTION.................................................................................................................................................................34 Programs and Services for People with Chronic Conditions........................................................................................34
1. Programs and Services for People with Chronic Cardiovascular Disease .......................................................34 2. Programs and Services for People with Diabetes ...............................................................................................37 3. Programs and Services for People with Chronic Kidney Disease .....................................................................41 4. Programs and Services for People with Chronic Mental Health and Addictions Challenges..........................45 5. Programs and Services for People with Chronic Respiratory Disease .............................................................50 6. Other Programs, Services and Positions to Support People with Chronic Conditions / At Risk....................52
SUMMARY, NEXT STEPS & QUESTIONS FOR CONSIDERATION ................................................................................57 APPENDIX I........................................................................................................................................................................59 APPENDIX II .......................................................................................................................................................................60
— Acknowledgements —
This inventory document would not be possible without the assistance of many. The information provided in this document has been derived from a combination of program descriptions as they appear in documents, client education pamphlets, on the RQHR Intranet
and internet sites and conversations with various people within RQHR. Contributors and managers were provided opportunity to affirm or edit the document contents. Much appreciation is expressed to all who contributed.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 33
Introduction RQHR is committed to the development of a Chronic Disease Prevention and Management Strategy with a view to decrease the incidence and prevalence of chronic disease within RQHR, improve access and coordination of services for clients, and improve client and health care provider satisfaction. Significant in this strategy development is the development of an inventory of current programs and services followed by assessment of our current state. It is anticipated such an assessment will lead to identification of strengths and gaps in service delivery and increased opportunity for informed decision making for moving forward. This inventory document focuses on programs and services currently provided by RQHR in caring for people living with prominent preventable chronic conditions, namely cardiovascular disease, diabetes, kidney disease, mental illness including addictions and respiratory disease. We know that cardiovascular diseases, chronic obstructive pulmonary disease (COPD) and type 2 diabetes are among the most prominent chronic diseases and are largely preventable. Given the concomitant incidence of kidney disease, and the high disease burden associated with chronic mental disorders and addictions, programs and services aimed at treating these are also addressed. In both 2005-6 and 2006-7, the largest volumes of RQHR admissions for ambulatory care sensitive conditions were due to asthma, COPD, diabetes and congestive heart failure. Data summaries for admissions and unplanned readmissions for 2005-6 and 2006-7 are provided in Appendix I. The prevalence of risk factor within RQHR residents, excerpted from the RQHR Health Status Report, 2004, is provided in Appendix II. RQHR programs and services related specifically to cancer treatment are not included in this inventory. Nor are programs and services for people with long term musculo-skeletal conditions, lifelong conditions present at birth or other long term conditions usually attributed to accidents. It also does not include community programs and services not under the jurisdiction of RQHR. A separate inventory of RQHR programs and services focused on health promotion and illness prevention is a work in progress under the leadership of Anna Engel, Manager of Health Promotion, Population and Public Health Services. It is anticipated the two documents combined will comprise a comprehensive inventory for chronic disease prevention and management programs and services currently provided by RQHR.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 34
Programs and Services for People with Chronic Conditions 1. Programs and Services for People with Chronic Cardiovascular Disease
Program/Service
& Leadership Description Service Location(s) Referrals
Cardiac Rehabilitation Program Val Roy, Administrative Director, Cardio sciences Program
The Cardiac Rehabilitation Program provides an outpatient program of education and exercise for individuals and their families who are learning to live with heart disease. The program is designed to help people who have had a cardiac event such as a heart attack, angina, angioplasty, and heart surgery make lifestyle changes. Monthly education sessions are provided by dietitians, exercise specialists, pharmacists, registered nurses and social workers. Six classes include:
• Living with Heart Disease, • Risk Factors and Lifestyle Modifications, • Medications, • Stress/Emotional Factors, • Heart Smart Eating Habits and • Exercise.
Follow-up educational sessions are offered to support and maintain lifestyle changes. An individualized cardiac rehabilitation exercise program is provided for RQHR patients by the Dr. Paul Schwann Centre at the University of Regina.
The Cardiac Rehabilitation Program is located at Regina General Hospital
Eligible cardiac patients are identified during their stay on the inpatient units and invited to participate after discharge. Self-referrals and referrals from physicians and other health professionals are accepted for educational classes. The Cardiac Rehabilitation Coordinator works closely with the Stroke Prevention Coordinator and the exercise specialist at the Dr. Paul Schwann Centre. Patients must be

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 35
Program/Service & Leadership
Description Service Location(s) Referrals
The exercise is supervised by an exercise specialist, cardiac nurse and/or a physician. Exercise programs include periodic blood pressure and ECG monitoring.
referred by a physician for the exercise program at the Dr. Paul Schwann Centre.
Congestive Heart Failure Clinic Vicki Ehrlich, Project Manager, Cardio science / Resp /Critical Care Val Roy, Administrative Director, Cardio sciences Program
The Congestive Heart Failure Clinic is an outpatient clinic that provides care and treatment to patients with congestive heart failure to reduce hospital admissions, reduce length of stay in hospital and improve quality of life for patients. Patients are treated by an interdisciplinary team of health care professionals including physicians, nurses, pharmacists, dietitians, and palliative care.
The Congestive Heart Failure Clinic is located at Pasqua Hospital
Patients are referred by their physician.
Heart Health Services Heather Dorgan, Rural Community Health Services (Grenfell) Bev Birns, Manager, Home Care / Community Services, Fort Qu’Appelle
Rural dietitians provide individual and group educations sessions focused on heart healthy eating, how to decrease risk as well as prevent another heart attack or stroke. These education sessions are similar to those provided by dietitians at the Lipid Clinic in Regina.
Multiple rural locations: Grenfell, Broadview, Moosomin, Wolseley, Whitewood, Indian Head, Montmartre, Fort Qu’Appelle, Lestock, Balcarres and Raymore.
Patients must be referred by their physician.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 36
Program/Service & Leadership
Description Service Location(s) Referrals
Lipid Clinic Stephanie Cook, Manager, Clinical Nutrition Services, Nutrition and Food Services Bill Semchuk, Manager – Clinical, Pharmacy
This program has been established to meet the needs of clients with lipid disorders throughout the RQHR and Southern Saskatchewan. Its intent is to provide a coordinated, multi-disciplinary and cost-effective approach to management of clients with various lipid disorders by providing educational and consultative services. Depending on the treatment plan, the patient will receive services from a dietitian, and may receive services from an endocrinologist and a pharmacist.
Outpatient services are available at MEDEC 2nd Floor, Medical Office wing, Regina General Hospital
Patients must be referred by their physician. Regular updates on the progress of the patient are provided.
South Sask Stroke Prevention Clinic Joy Jackson, Manager, RGH Unit 5A, Neurosciences
The goal of the Stroke Prevention Clinic is to reduce the number of strokes through public education and early identification and treatment of people at risk for stroke. This weekly outpatient clinic is a fast track system for people who exhibit signs or impending signs of stroke, e.g. TIA. Patients are assessed by a Neurologist usually within 1 to 2 weeks of referral. Diagnostic tests are expedited and treatment is commenced in a timely fashion with some patients being admitted to hospital. A Clinical Nurse Specialist provides teaching and counseling for patients, families and staff. Group classes are offered on a regular basis and include information on how strokes occur, risk factors, healthy eating, medications, stress and exercise.
The Clinic is located at Regina General Hospital.
Patients are referred by their physician or physicians in the emergency department. The Clinical Nurse Specialist works closely with the Cardiac Rehabilitation Coordinator.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 37
2. Programs and Services for People with Diabetes The RQHR is committed to delivery quality diabetes prevention and treatment to the residents of southern Saskatchewan. RQHR diabetes services and programs include treatment for those with diabetes aimed at lessening the effect of the disease, prevention treatment and education for those at risk of developing diabetes and public education for those wanting more information on prevention of diabetes.
Program/Service & Leadership
Description Service Location(s) Referrals
Diabetes Education Program (DEP) Bev Birns, Manager, Home Care /Community Services, Ft. Qu’Appelle
The Diabetes Education Program’s diabetes nurse educator and dietitian offer individual and group education to adults with pre-diabetes, type 1 and 2 diabetes or gestational diabetes. The diabetes nurse educator provides training and skills needed to start insulin therapy and adjust insulin dosage. Although this program provides similar services to the Rural East Diabetes Education Program, the programs are not connected, coordinated or integrated with each other in any way.
Fort Qu’Appelle, Lestock, Balcarres and Raymore
Self referrals and physician referrals are accepted
Endocrinology Services Vice President, Medical Admin
Two Endocrinologists provide medical assessment and specialized care for adults with diabetes, thyroid problems, osteoporosis and other endocrine disorders. Children can be referred to a pediatric endocrinologist in Saskatoon.
Regina Referral from a physician is required.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 38
Program/Service & Leadership
Description Service Location(s) Referrals
Eye Screening Clinics Bev Alfano, Manager, Eye Centre
The Regina Eye Centre, Medical Media and the Regional Diabetes Initiative have joined together to offer eye screening clinics for diabetic retinopathy. These clinics are available to people who have been diagnosed with diabetes and have not seen an optometrist or ophthalmologist within the past two years.
Eye Centre (PH) Multiple sites planned for the future
Appointments are made through the various regional Diabetes programs ,
Foot Care and Podiatry Services Lenore Bryant, Manager Home Care, Rural Areas Donna Smeets, Manager Home Care, Rural Areas Bev Birns, Manager, Home Care / Community Services, Ft. Qu’Appelle Dale Young, Acting Manager, Population & Public Health, Podiatry
Annual foot examinations by a trained care provider to check for loss of feeling, and changes in the feet are recommended for people with diabetes.
People with diabetes who have lost sensation in their feet or who have developed other foot problems should be under the care of a podiatrist (foot doctor). The Podiatry Program provides foot treatment and advice for all age groups. It promotes well-being, mobility and independence. Services are provided by a Podiatrist and a Podiatry nurse.
In Regina and some rural areas, people with diabetes can use one of the private nail/foot care companies for nail care services.
In many rural sites, RQHR Home Care nurses provide nail and skin care services, often at Wellness Clinics or special Foot Clinics.
In Regina, the Podiatry Program is located at Regina General Hospital. Once a month
Referral from a physician or a health professional is required to access Podiatry services. Persons with diabetes and/or peripheral vascular disease receive priority care. Clients can self refer for nail/skin care to private companies and Home Care clinics.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 39
Program/Service & Leadership
Description Service Location(s) Referrals
podiatry clinics are also held in Balcarres, Fort Qu’Appelle, Grenfell, Lestock, Moosomin and Raymore.
MEDEC (Metabolic and Diabetes Education Centre) Karen Butler, Manager, MEDEC
MEDEC provides diabetes education, care and support to adults, youth and children with • type 1 and type 2 diabetes, • pre-diabetes (IFG/IGT), • gestational diabetes (GDM), • hypoglycemia, or • polycystic ovarian syndrome (PCOS). • Insulin pump therapy and continuous glucose
monitoring Group classes and individual sessions are offered by Diabetes Nurse Educators and Diabetes Nutrition Educators; The Diabetes Nurse Educator also provides training and skills need to start insulin therapy and insulin dosage adjustment. The Pregnancy and Diabetes Clinic provides specialized, comprehensive diabetes management and prenatal care for women with type 1 and type 2 diabetes during pregnancy, and for women with gestational diabetes, who require insulin therapy.
Outpatient services are available at MEDEC 2nd Floor, Medical Office wing, Regina General Hospital
In-patient diabetes nurse education services are available at RGH, PH and WRC.
Self-referrals and referrals from physicians and other health professionals are accepted.
Physician referral is required to attend the Pregnancy and Diabetes Clinic

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 40
Program/Service & Leadership
Description Service Location(s) Referrals
Rural East Diabetes Education Program Heather Dorgan, Manager, Rural Community Health Services (Grenfell)
A chronic condition nurse educator and dietitian offer individual and group education to adults with pre-diabetes, type 1 and 2 diabetes or gestational diabetes, and other chronic conditions. The staff also provides services to promote healthy lifestyles and prevent chronic conditions.
In the Moosomin area, there is a hospital pharmacist with certification in diabetes education who offers individual and group education to people with type 1 diabetes, type 2 diabetes, pre-diabetes or gestational diabetes.
Although this program provides similar services to the Diabetes Education Program, the programs are not connected, coordinated or integrated with each other in any way.
Grenfell, Broadview, Wolseley, Whitewood, Moosomin and area, Indian Head and Montmartre
Self-referrals and referrals from physicians and other health professionals are accepted.
Special Focus Initiatives for People with Diabetes
• Targeted funding from the Ministry supports the Regional Diabetes Initiative – The Diabetes Sub Committee and its three working groups plan, coordinate and evaluate diabetes prevention and management in the region; focus is on the development and delivery of a coordinated multi-sectoral holistic approach. The committee’s work is support by a part time Regional Diabetes manager position.
• Priority areas of the Regional Diabetes strategy include: prevention of type 2 diabetes; quality care to reduce
complications; support for health care providers; surveillance and first Nations and Métis issues.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 41
3. Programs and Services for People with Chronic Kidney Disease The Regina Qu'Appelle Health Region's Renal Program offers services to the residents of southern Saskatchewan.
Program/Service & Leadership
Description Service Location(s) Referrals
Chronic Renal Insufficiency (CRI) Program Chris Horton, Manager, Integrated Renal Program
The CRI Program provides a multidisciplinary team approach to educating patients and their families/caregivers, as well as, other health professionals regarding Chronic Kidney Disease (CKD), providing expert clinical assessments and lab monitoring and recommending and supervising therapies to optimize renal function. The overall goal, of the Program, is to delay or halt the progression of CKD and to delay the need for renal replacement therapy.
The multidisciplinary team ensures a coordinated approach to CKD care and management for patients in the Southern half of Saskatchewan. The team consists of Nephrologists, Nurses, a Social Worker, a Dietitian, Pharmacists, a Diabetes Nurse Educator, an Access Nurse and other health care providers as needed.
A recent study of the program found that as a direct result of the program, the progression of kidney disease was delayed by more than 10 percent in nearly half of the clients serviced (47%).
The CRI Program is located on Unit 4E at Regina General Hospital. Each patient is seen initially in Regina and follow up appointments, for some patients, can be arranged through Telehealth.
Patients are referred by their physician to the Nephrologists who then refer the patients to the CRI Program.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 42
Program/Service & Leadership
Description Service Location(s) Referrals
Hemodialysis Unit and Satellite Hemodialysis Units Myrna Bye, Manager, Renal (Hemodialysis) Unit Chris Horton, Manager, Integrated Renal Program
Hemodialysis is a treatment option for patients, living in southern Saskatchewan, who have end-stage renal disease and require renal replacement therapy. In Hemodialysis the patient’s blood is cleansed of wastes/toxins and fluid by using a dialyzer (blood filter) and a dialysis machine, usually 2-3 times each week. On going monitoring and support are provided by the Nurses, Social Workers, Pharmacists, Dietitian and Access Nurse, as well as, other health care providers, as needed. The Satellite Hemodialysis Units work closely, with RQHR’s Renal Unit to provide dialysis treatments closer to home, for patients living in rural Saskatchewan communities. The RQHR provides staff training and orientation, clinical support, CES support for repair and maintenance of the dialysis machines. Patients are under the care of Nephrologists from Regina.
The unit is located on 1A at Regina General Hospital. Satellite units are located in Yorkton, Moose Jaw, Estevan and Swift Current
Referral from a physician is required. Approval by the Nephrologist is required, prior to transfer to a Satellite Unit

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 43
Program/Service & Leadership
Description Service Location(s) Referrals
Home Dialysis Training Unit Chris Horton, Manager Integrated Renal Program
Peritoneal Dialysis is a treatment option for patients, living in southern Saskatchewan, who have end-stage renal disease and require renal replacement therapy. In peritoneal dialysis, wastes and water are removed from the patient’s blood by introducing fluid in the peritoneal cavity, leaving it to dwell there, draining it out and repeating the process. The Home Dialysis Unit also provides patients and their families/caregivers with information sessions about peritoneal dialysis as a treatment option. The Unit teaches patients and/or their families/caregivers how to safely perform peritoneal dialysis independently at home, provides ongoing follow-up care and support to home dialysis patients in an out-patient setting and assists patients in maintaining an optimal level of wellness. Training and ongoing support are provided by Home Dialysis Training Nurses, Social Worker, Pharmacist, Diabetic Educator Dietitian and Access Nurse.
The unit is located on Unit 4E at Regina General Hospital. Patients are taught to perform/manage their own treatments at home on a daily basis.
Referral from a physician is required.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 44
Program/Service & Leadership
Description Service Location(s) Referrals
Transplant Program Chris Horton, Manager, Integrated Renal Program
The Regina Transplant Program, a branch of the Saskatchewan Transplant Program, provides transplant education to patients and families, facilitates workups and the listing of patients on the waiting list, coordinates and participates in organ and tissue donations and promotes transplant awareness and education to health care providers and the public. The Transplant Program also offers post transplant clinics where post-kidney transplant patients are seen and assessed by a transplant Nephrologist and the Transplant Coordinators.
The Regina Transplant Program is located on Unit 4E at Regina General Hospital.
Patients are referred by their Nephrologist
Special Focus Initiatives for People with Kidney Disease
• Twin Valleys Chronic Renal Disease Prevention and Management Plan – This plan, developed in 2006, provides a vision and strategies for enhanced services for residents within the Twin Valleys Primary Health Care site that prevent or delay complications associated with kidney disease.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 45
4. Programs and Services for People with Chronic Mental Health and Addictions Challenges Mental Health & Addictions Services provides acute inpatient, transitional day treatment and follow-up outpatient mental health care for children, youth and adults, in both urban and rural settings and a wide range of treatment options for people with addictions. Addictions Services provides a wide range of community-based programs for people with addictions. Some programs are specifically for people dependent on alcohol or drugs, and include support, education and counseling for their family members. These programs range from individual or group education and treatment, to harm reduction approaches, such as methadone. Other programs provide treatment for individuals with pathological gambling problems, or provide education and support to their families and friends. Programs and services indicated in this document are those focused primarily on caring for people with long term or chronic mental health & addictions challenges.
Program/Service & Leadership
Description Service Location(s) Referrals
Addictions Services Lorri Carlson, Manager, Addictions Services Heather Dorgan, Manager, Rural Community Health Services (Grenfell) Bev Birns, Manager, Rural Community Health & Home Care (Fort Qu’Appelle)
Addiction Services provide a range of community-based services both rurally and in Regina for people who are having significant problems related to substance abuse / misuse.
In Regina, Addiction Services is located at 2110 Hamilton Street, 2nd floor.
Addiction Services in the rural areas of the Regina Qu'Appelle Health Region are located in Grenfell and Fort Qu'Appelle with satellite clinics in numerous other rural communities.
Referrals from family physicians, SGI, and self referrals are accepted.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 46
Program/Service & Leadership
Description Service Location(s) Referrals
Adult Community Mental Health Clinics Colleen Molnar, Manager, Mental Health Clinic Dr. John Brown, Program Manager, Adult Therapy, Mental Health & Addictions Heather Dorgan, Manager, Rural Community Health Services (Grenfell) Bev Birns, Manager, Rural Community Health & Home Care (Fort Qu’Appelle)
The Adult Mental Health Clinics are part of a continuum of treatment and support services available for adults (age 18 and over). They provide a wide range of community-based services for people who are having significant problems related to their mental health and well being.
Rural Adult Mental Health Clinics offer services similar to the Adult Community Program and Rehabilitation Programs in Regina. Rural residents may access Regina-based programs that are not available in the rural areas through one of the rural mental health workers.
In Regina the Mental Health Clinic is located at 2110 Hamilton Street, 3rd floor.
The Mental Health Clinics in the rural areas of the Regina Qu'Appelle Health Region are located in Grenfell and Fort Qu'Appelle with satellite clinics in numerous other rural communities.
Referrals from family physicians and self referrals are accepted.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 47
Program/Service & Leadership
Description Service Location(s) Referrals
Harm Reduction Methadone Clinic Lorri Carlson, Manager, Addictions Services
This is a harm reduction program for injection drug users that also includes a recovery option. Program goals include improving the social determinants of health for injection drug users and other at-risk individuals, and to reduce injection drug use, drug-related crime rates and Hep C and HIV infection rates in Regina and area.
The Harm Reduction Methadone Clinic is located at 1048 Albert Street
Referrals are accepted from individuals (self-referral) or from other agencies, doctors, the courts, employers, schools, counselors and employee Family Assistance Programs.
Problem Gambling Programs
Lorri Carlson, Manager, Addictions Services
A wide variety of problem gambling programs are offered including Dual-diagnosis Group program, Woman’s Group, Family Support Group, individual counseling, day treatment program, aboriginal problem gambling program and other therapeutic groups. The Aboriginal Problem Gambling Program offers a wide range of services including assessments, referrals, treatment programs and counseling services for individuals, families and groups. Programs are based on a harm reduction model. Services, provided by an Aboriginal Counsellor, use the concept of the medicine Wheel to deal with the four major aspects of a person’s life – mind, body, spirit, emotion.
Most Problem Gambling Programs are located at 2110 Hamilton Street, Regina.
The Aboriginal Problem Gambling Program is located at the Randall Kinship Centre, 1692 Albert Street, Regina
Referrals are accepted from Employee Family Assistance Programs, counselors and family physicians. Self-referrals are welcome.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 48
Program/Service & Leadership
Description Service Location(s) Referrals
Elders are made available on request and at times attend groups. The Day Treatment Program is designed for individuals who require intensive treatment for their gambling problem, usually in addition to the treatment they may currently be receiving. This program has been developed as a provincial resource and is available to any Saskatchewan resident.
Rehabilitation Program Cathy Keenan-Arp, Program Manager, Rehabilitation, Mental Health & Addictions
The Rehabilitation Program provides long-term case management and rehabilitation services for clients who have a long-term serious mental illness. Ongoing support and counselling enables clients to achieve and maintain mental wellness and their optimal level of independence in the community.
Other services available to Rehabilitation Program clients include a supportive residential placement program, vocational counselling, family education and support, medication management (including an injection medication clinic) and financial services.
Services are provided on-site, at the Mental Health Clinic and in the community.
Referral to this program must be made by a psychiatrist.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 49
In addition, the following community based organizations are funded by Mental Health & Addictions Services:
• Autism Resource Centre
• Canadian Mental Health Association, Regina Branch –provides a variety of programs for the long-term mentally ill.
• Detox Centre
• Mobile Crisis Service In.
• Phoenix Residential Society –operates a number of supported living, vocational and treatment programs for persons with long term mental illness.
• Pine Lodge
• Rainbow Youth Centre

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 50
5. Programs and Services for People with Chronic Respiratory Disease
Program/Service & Leadership
Description Service Location(s) Referrals
Adult Asthma Education Program Sheryl O’Quinn, Manager, Respiratory Services
Asthma education is provided to outpatients, 18 years or older, with a view to assist the patient and family physician in achieving control of asthma. A Registered Respiratory Therapist instructs clients in facts about asthma, the roles of medications, basic skills for medication delivery devices, environmental controls (trigger) and development of an action plan.
The Adult Asthma Education Program is delivered at Wascana Rehab Centre
Self-referrals and referrals from physicians are accepted.
Chronic Obstructive Pulmonary (COPD) Rehabilitation Program Sheryl O’Quinn, Manager, Respiratory Services
This program is focused on the promotion of self management to slow the progress of COPD including the importance of regular exercise, good nutrition, breathing exercises, chest clearance techniques, relaxation techniques, coping skills, activities of daily living and psychosocial support skills. The program is delivered by Respirologists, Respiratory Therapists and Exercise Therapists. One of the Respiratory Therapists is specially trained in COPD management and is the Program Coordinator. Dietitians, psychologists, social workers, and pharmacists also assist with the program.
The program is delivered at Southland Mall
Patients are referred by a physician

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 51
Program/Service & Leadership
Description Service Location(s) Referrals
Home Oxygen Assessment and Testing Sheryl O’Quinn, Manager, Respiratory Services
RQHR provides home oxygen testing for patients with respiratory related medical disorders. Testing is provided by Respiratory Services and is designed for assessment and treatment of the disorder as well as for ongoing management of the medical condition.
Outpatient exercise testing and overnight oximetry is available at WRC. In and out patient exercise testing and oximetry is performed at RGH and PH. Rural Home care coordinators also do this testing.
Patients are referred by a physician
Sleep Disorders Clinic Sheryl O’Quinn, Manager, Respiratory Services
The Sleep Disorders Program helps people who have problems getting a good night’s sleep because of snoring, sleep apnea, insomnia, restless legs or other conditions. The clinic has an outpatient clinic and a sleep laboratory where patients are monitored during sleep. Services are provided by a Sleep Specialist, Health Information Medical Practitioners and Respiratory Therapists/Polysomnographers.
The Sleep Disorders Clinic is located at Regina General Hospital
Patients are referred by their family physician
Ventilator Programs Sheryl O’Quinn, Manager, Respiratory Services
Respiratory Services supports Home-ventilated Client Services and the Long Term Ventilation Program. The goal of the long term ventilation program is the management of the chronic respiratory condition and to maintain/improve patient quality of life.
Services are provided at WRC and in client homes within Regina

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 52
Program/Service & Leadership
Description Service Location(s) Referrals
A Respiratory Educator / Community Therapist assists patients and families with the training of caregivers and manages home ventilation services, performing scheduled ventilator and patient checks at regular intervals and responds to concerns and calls for assistance.
6. Other Programs, Services and Positions To Support People With Chronic Conditions / At Risk
The following programs, services and positions are not specific to the management of any one chronic condition but rather support people with any chronic condition, those who present with more than one chronic condition and / are considered to be at risk.
Program/Service & Leadership
Description Service Location(s) Referrals
Al Ritchie Community Health Centre Dale Young, Manager, Population & Public Health
Al Ritchie Community Health Centre offers a range of programs and services for people living with chronic conditions, primarily diabetes including support and prenatal education for women with gestational diabetes. Programs and services focused on health promotion and illness prevention are described in a separate Population and Public Health inventory document
Al Ritchie Community Health Centre
Self-referrals and referrals from health professionals are accepted.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 53
Program/Service & Leadership
Description Service Location(s) Referrals
Chronic Conditions Nurse Educator North Central: Morag Granger, Manager, Population & Public Health Twin Valleys: Heather Dorgan, Manager, Population & Public Health
The Chronic Conditions Nurse Educator (CCNE) provides nursing services and education to people with pre-diabetes, diabetes and other chronic conditions. The nurse also provides services to promote healthy lifestyles and prevent chronic conditions. These new positions were created in 2007 in accordance with the visions and strategies for primary heath care for North Central Regina and Twin Valleys (Wolseley, Grenfell, Broadview, Whitewood and First Nations of Sakimay, Ochapowace, Cowessess and Kahkewistahaw).
Services are provided at 2 Primary Health Care Sites:
• Twin Valleys • North Central
Regina
Self-referrals and referrals from physicians and other health professionals are accepted.
Clinical Nutrition Services Stephanie Cook, Manager, Clinical Nutrition Services, Nutrition and Food Services Heather Dorgan, Rural Community Health Services (Grenfell) Bev Birns, Manager, Home Care/ Community Services, Fort Qu’Appelle
Nutrition intervention can help prevent malnutrition and improve nutritional status as well as prevent, delay, onset, or decrease impact of many conditions thus enhancing clients well being. In view of potential benefits of nutrition intervention, early identification of clients who may benefit from nutrition counseling is essential. Dietitians are available for educating and counseling within Regina Hospitals, at regular rural clinics and also provide ambulatory nutrition services in a number of situations.
Services are provided at Regina Hospitals and clinics in Indian Head, Wolseley, Grenfell, Broadview, Whitewood, Moosomin, Fort Qu’Appelle, Lestock, Raymore and Balcarres
Patients must be referred by a physician for services within Regina. Self-referrals and referrals from health professionals are accepted in the rural clinics.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 54
Program/Service & Leadership
Description Service Location(s) Referrals
First Nations and Métis Services Stephanie Cavers, Director, Aboriginal Health, Eagle Moon Health Office
RQHR offers assistance and support to First Nations and Métis people through the Eagle Moon Health Office (766-7190) and Native Health Services (Pasqua Hospital 766-2232; Regina General Hospital 766-4155).
Self-referrals and referrals from health and other professionals are accepted.
Four Directions Community Health Centre Morag Granger, Manager, Population & Public Health
Four Directions Community Health Centre offers a variety of programs and services for individuals and families living with chronic conditions, primarily diabetes, including diabetes support group, support for women with gestational diabetes, and Living in Balance. Programs and services focused on health promotion and illness prevention are described in a separate Population and Public Health inventory document.
Four Directions Community Health Centre
Self-referrals and referrals from health professionals are accepted.
HealthLine John Masters, Director, HealthLine
HealthLine provides reliable information on health related topics including advice for people with chronic conditions. The information is provided by registered nurses and is intended to help people better understand and manage their own health and the health of their families. It can help people to know when to contact their physician or other health care professional.
Services are provided by telephone or on line
Anyone can contact HealthLine. HealthLine may advise patients to contact a physician or other health care provider and may assist with way finding.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 55
Program/Service & Leadership
Description Service Location(s) Referrals
Home Care Betty Lou Whitley, Director, Home Care
Home Care provides a range of services for people living with chronic conditions. Services are intended to support and supplement families and other community resources and may include medication administration, assistance with insulin administration, blood sugar and blood pressure monitoring, assistance with personal care, education, etc.
Services are provided in various communities, Regina and rural.
Anyone can make a referral to home care
Live Well™ with Chronic Conditions Ruth Meier, Manager, Home Care
Live Well™ with Chronic Conditions offers support and education for those living with pre-diabetes, diabetes and / or chronic conditions. It is a self management peer led program open to individuals with any chronic condition. Participants meet in groups to learn symptom management, goal setting, nutrition and exercise, communication skills, how to access community resources, and other management techniques.
Services are provided in various communities, Regina and rural.
Self referrals are welcome
Neuromodulation Clinic Joy Jackson, Manager, RGH Unit 5A, Neurosciences
The Neuromodulation clinic is an outpatient clinic for patients with chronic pain, tremors, and spasticity to be assessed by a Neurosurgeon for surgical implant to improve quality of life. Surgical implants include intrathecal pump for pain management, deep brain implant or spinal cord stimulator. Patients who are deemed to be good candidates are admitted for further assessment and surgical implant.
The Clinic is located at Regina General Hospital, Unit 5A
Patients are referred by their physician.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 56
Program/Service & Leadership
Description Service Location(s) Referrals
Weight Management Stephanie Cook, Manager, Clinical Nutrition Services, Nutrition and Food Services.
Clients participate in a series of classes on nutrition and weight management. A variety of issues regarding healthy eating and the importance of physical activity are covered.
Patients are referred by physicians
Other Special Focus Initiatives for Chronic Disease Prevention and Management
Other initiatives focused on enhanced services for people with chronic conditions that are currently underway include:
• Ambulatory Care Sensitive Conditions – project focused on reduced reliance on inpatient care for some services with a view to improve and enhance overall system capacity.
• Health Quality Council Chronic Disease Management Collaborative - The Saskatchewan Chronic Disease
Management (CDM) Collaborative is a major quality improvement initiative organized by the Health Quality Council to improve the care and health of people living with diabetes and coronary artery disease (CAD) in Saskatchewan, and to improve access to physician practices. RQHR employs a Collaborative Facilitator who works with physician practices throughout the RQHR in developing their capability to deliver rapid, sustainable and systematic improvements in the care provided to persons with diabetes and coronary artery disease.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 57
Summary, Next Steps & Questions for Consideration The development of this inventory is one phase in the development of a RQHR chronic disease prevention and management strategy. It provides factual information about programs and services currently provided by RQHR in caring for people living with prominent preventable chronic conditions. It is not inclusive of all programs and services. RQHR programs and services related specifically to cancer treatment are not included in this inventory. Nor are programs and services for people with lifelong conditions present at birth or other long term conditions usually attributed to accidents. The next phase includes an assessment of the current state, informed in part by this inventory. It is anticipated such an assessment will lead to identification of strengths and gaps in service delivery and increased opportunity for informed decision making for moving forward. The following comments and questions are intended to serve as food for thought. It is clearly evident the RQHR provides a number of programs and services for people with prominent preventable chronic conditions and the responsibility for chronic disease management does not rest within any one department or portfolio but rather is shared throughout RQHR. Some programs and services are available only in Regina while others are provided in communities throughout the health region.
• What are the individual and collective strengths of programs and services for people living with chronic conditions?
• What do providers hear from clients about their experiences?
• What are the greatest issues or challenges patients experience in accessing services for care related to their chronic condition(s)?
• What are the greatest issues or challenges providers experience in caring for people with chronic conditions?
• How many clients are served? Are they served in a timely fashion?
• Are there gaps in service delivery? If so, what are the gaps?
• What are the outcomes of each of the programs/services? What results are reported?

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 58
• What are the opportunities for improving outcomes for patients?
The level of coordination and/or integration between programs and services in providing care for people with chronic conditions is not clearly articulated and may simply have not been provided as the information was provided / gathered. Perhaps this warrants further investigation as RQHR proceeds with development of a chronic disease prevention and management strategy.
• How do RQHR programs and services connect, communicate and integrate when providing care for patients with chronic conditions? What connections exist for patients?
• Is there a need for enhanced linkages / coordinated seamless services particularly when people present with more
than one chronic condition?
• What are the opportunities for enhancing / improving coordination and integration of patient care? What outcomes would we anticipate?
The programs and services described in this document focus on treatment and management of chronic conditions. Almost all of the programs/services are accessed by referral from family physicians and/or other health care providers once a chronic condition is diagnosed. Some program and service descriptions speak to reducing consequences through early diagnosis and treatment; some speak to reducing disease progression and complications. Primary prevention is addressed in a separate document. It is not clear who, if anyone, actually identifies and then screens high risk groups/communities/populations.
• Does the RQHR have a role in determining and screening people who are high risk for chronic conditions? Would this lead to improved outcomes?

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 59
APPENDIX I Regina Qu'Appelle Health Region Ambulatory Care Sensitive Conditions – Summary
2005-06 All cases 2006-07 All cases 2005-06 Unplanned Readmissions 2006-07 Unplanned Readmissions
ACSC Data Total ACSC Data Total Readmit Description Readmit Description
Angina Count of ACSC 125 Angina Count of ACSC 128 ACSC DataUnplanned 8-28 Days
% of total readmits ACSC Data
Unplanned 8-28 Days
% of total readmits
Sum of LOS 507 Sum of LOS 446 Angina Count of ACSC 2.0 4% Asthma Count of ACSC 5.0 15%Average of ELOS 4.0 Average of ELOS 4.2 Sum of LOS 10.0 Sum of LOS 6.0Average of LOS 4.1 Average of LOS 3.5 Average of ELOS 5.1 Average of ELOS 2.7
Asthma Count of ACSC 413 Asthma Count of ACSC 304 Average of LOS 5.0 Average of LOS 1.2Sum of LOS 904 Sum of LOS 654 Asthma Count of ACSC 6.0 13% COPD Count of ACSC 18.0 55%Average of ELOS 2.4 Average of ELOS 2.4 Sum of LOS 12.0 Sum of LOS 188.0Average of LOS 2.2 Average of LOS 2.2 Average of ELOS 3.5 Average of ELOS 9.9
COPD Count of ACSC 321 COPD Count of ACSC 272 Average of LOS 2.0 Average of LOS 10.4Sum of LOS 2351 Sum of LOS 2262 COPD Count of ACSC 26.0 57% Diabetes Count of ACSC 2.0 6%Average of ELOS 7.1 Average of ELOS 7.7 Sum of LOS 172.0 Sum of LOS 9.0Average of LOS 7.3 Average of LOS 8.3 Average of ELOS 6.6 Average of ELOS 5.0
Diabetes Count of ACSC 138 Diabetes Count of ACSC 199 Average of LOS 6.6 Average of LOS 4.5Sum of LOS 1030 Sum of LOS 1519 Diabetes Count of ACSC 2.0 4% Heart Failure Count of ACSC 3.0 9%Average of ELOS 5.6 Average of ELOS 6.5 Sum of LOS 4.0 Sum of LOS 29.0Average of LOS 7.5 Average of LOS 7.6 Average of ELOS 4.0 Average of ELOS 9.1
Heart Failure Count of ACSC 172 Heart Failure Count of ACSC 186 Average of LOS 2.0 Average of LOS 9.7Sum of LOS 1883 Sum of LOS 1576 Heart Failure Count of ACSC 6.0 13% Hypertension Count of ACSC 1.0 3%Average of ELOS 8.3 Average of ELOS 8.0 Sum of LOS 56.0 Sum of LOS 1.0Average of LOS 10.9 Average of LOS 8.5 Average of ELOS 10.7 Average of ELOS 2.9
Hypertension Count of ACSC 33 Hypertension Count of ACSC 31 Average of LOS 9.3 Average of LOS 1.0Sum of LOS 225 Sum of LOS 107 Hypertension Count of ACSC 1.0 2% Seizures Count of ACSC 4.0 12%Average of ELOS 4.9 Average of ELOS 3.3 Sum of LOS 8.0 Sum of LOS 9.0Average of LOS 6.8 Average of LOS 3.5 Average of ELOS 6.4 Average of ELOS 1.7
Seizures Count of ACSC 81 Seizures Count of ACSC 74 Average of LOS 8.0 Average of LOS 2.3Sum of LOS 271 Sum of LOS 389 Seizures Count of ACSC 3.0 7% Total Count of ACSC 33.0Average of ELOS 2.7 Average of ELOS 3.9 Sum of LOS 4.0 Total Sum of LOS 242.0Average of LOS 3.3 Average of LOS 5.3 Average of ELOS 2.0 Total Average of ELOS 7.2
Total Count of ACSC 1283 Total Count of ACSC 1194 Average of LOS 1.3 Total Average of LOS 7.3Total Sum of LOS 7171 Total Sum of LOS 6953 Total Count of ACSC 46.0Total Average of ELOS 4.9 Total Average of ELOS 5.5 Total Sum of LOS 266.0Total Average of LOS 5.6 Total Average of LOS 5.8 Total Average of ELOS 6.2
Total Average of LOS 5.8
Summary- All RQHR
Prepared by Leeann Carr (HIMS) and Ali Bell (R1S)

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 60
APPENDIX II Prevalence of Risk Factors within RQHR Residents According to the RQHR Health Status Report, 2004
• the Canadian Community Health Survey, 2003 revealed o 41% of Regina Qu’Appelle Health Region males and 25.7% of females aged 18 years and over are considered
overweight or obese. Regional males in each age group were more likely to be overweight or obese; the proportion of those who are
overweight continues to rise with increasing age. o a large proportion of Regina Qu'Appelle Health Region residents were not active enough to obtain the health benefits of
physical activity o 78.3% of all Regina Qu'Appelle Health Region respondents had consumed alcohol in the previous 12 months. More than
50% of respondents reported drinking more than once a month, including 4.5% that were drinking every day. The reported use of alcohol was highest in 20 to 34 years age group (90.1%), followed by 35-49 year age group (87.9%), 50-64 years age group (77.6%) and 65 years or older (66.2%).
• tobacco industry products are the leading cause of premature preventable death, disability, and disease in Canada1, in Saskatchewan and in the Regina Qu’Appelle Health Region. Of all risk factors for disease, tobacco smoking is responsible for the greatest burden on the health of Canadians. o In the Regina Qu’Appelle Health Region more than 400 residents die each year due to tobacco-related diseases. This
represents 21% of deaths in the Region2. One-half of long-term smokers die prematurely3 due to cancers, cardiovascular disease and respiratory diseases.
o While tobacco consumption has decreased in Saskatchewan over the last two decades, current trends in mortality attributable to smoking reflect the smoking behaviour of the population two to three decades earlier.
o Tobacco use among Aboriginal Canadians is much higher than the national prevalence. Thus, tobacco is a significant health concern with this group.
Fifty-six percent of First Nations people and 57% of Métis people smoke. Smoking rates among Aboriginal youth are particularly high: 54% of 11 to 19-year-olds and 65% of 20 to 25-year-
olds smoke4.
1 Makomaski Illing, E.M. and Kaiserman, M.J. Mortality Attributable to Tobacco Use in Canada and its Regions, Canadian Journal of Public Health 95(1), 38-44. 2 Ellison, L, Mao,Y and Gibbons, L, Projected Smoking-Attributable Mortality in Canada, 1991-2000. Chronic Diseases in Canada, 16(2), Spring, 1995. 3 Pan American Health Organization, Regional Office of the World Health Organization. (2002). Developing Legislation for Tobacco Control. 4 Health Canada, Tobacco Use Among Aboriginal Peoples, 1995

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 61
APPENDIX 5: RQHR - CHRONIC DISEASE PREVENTION & MANAGEMENT CURRENT STATE PROGRAMS & SERVICES - JUNE, 2008 - (Short List)Adopted from (Format developed by Ann Stirling, Trillium Health Centre)
RQHR Health System
PROGRAM TITLE
TYPE
PHYS
ICIA
N R
EFER
RAL
REQ
UIR
ED
WAI
T TI
ME
(R/T
cap
acity
)
LEN
GTH
OF
PRO
GR
AM
IND
IVID
UAL
/ G
RO
UP
PHYS
ICIA
N (p
art o
f pro
gram
)
NU
RSI
NG
Adm
in s
uppo
rt
Med
ical
Med
ia
DIE
TIC
IAN
RT
(Pol
ysom
nogr
aphe
rs)
PSYC
HO
LOG
IST
HEA
LTH
INFO
MED
ICAL
PR
ACTI
TIO
N
KIN
ISIO
LOG
IST/
Exs.
The
rapi
st
SW Com
mun
ity S
uppo
rt/H
ome
Serv
ices
/Mea
l Ser
vice
s/ S
itter
Ser
vice
Volu
ntee
r
OT/
PT
Supe
rvis
or
PHAR
MAC
ISTS
MED
ICAT
ION
MAN
AGEM
ENT
VOLU
MES
CLI
NIC
AL P
ATH
WAY
S
PRO
CES
S M
AP C
OM
PLET
ED
COMMENTS
Prim
ary
Prev
entio
n
Mai
nten
ance
Seco
ndar
y Pr
even
tion
Long
Ter
m
Man
agem
ent
See Appendix 10 for more detail R
N
ACN
P
LPN
/ CN
S
Reg
Psy
ch
RN
ACN
P
PHAR
M
EXER
CIS
E
DIE
T
SMO
KIN
G
ALC
OH
OL
STR
ESS
MG
MT
SELF
MG
MT.
LITE
RAC
Y G
RAD
E LE
VEL
LAN
GU
AGES
Respiratory Programming Paed Asthma Clinic Ed x yes 3 mos* Clinic I/F
0.1 FTE
0.1 FTE x Ed x/P Gr 6*
Eng?? 32**
x x * July/08. ** June '07-June'08
Adult Asthma Education Program x x x no none I0.2 FTE
x10 Eng n/a
x x
COPD Rehab Exs & Ed. Program x x x yes 1yr/60 people
12 w ks & Ongoing exerise program
G x x1
FTE x0.5 FTE x x x x x x 10 Eng
10 per program session, 60 per year
x x 90 clients have initiated prog. to date
Home Oxygen Assessment & Testing x x yesWRC- 3 - 5w ks,
PFL- 6 mos Test only I x x x 10 Eng25-30 per
w eekx x
Diagnostic testing w ait time is too long, nothing greater than 3 mos target.
Sleep Disorders Clinic x x x yes5 yrs/ 1300
peopleTest and follow up I x x
5 + 1
supervisor 6FTE
2 FTE x 10 Eng
60 per month x x
RTs are Polysomnographers. Diagnostic w ait list too long for patients w ith suspected sleep apnea
Ventilator Programs x x x yes none LT I X3
FTE x 10 Eng5-6
home,10 WRC
x x
Pilot for 1 yr. (approx 6 people have their programming contracted by Vital Air through SAIL and receive no coverage through RQHR - w ere prior to 2001)
Home Care:Live Well™ With Chronic Conditions Programming
x? NoDepends on
location & class #s
6 w ks G x x x x x x x x Gr 6 Eng 72
Program started about 1 yr ago (Summer 2007??) for all chronic conditions. Unable to determine # of Respiratory clients service provided for.
Home Care: Regular Programming
x x x No None n/a I x
x Urban: 100 x? 3
125 HHA x
Total 14 x x x
Population & Public Health x ? ? No
*Drop in. 2 w ks for healthy
baby program/Active
Living/ Heart Healthy.
? *
*1FT-CCNE/1 FT NPs/PHNs
2*.9FTE (Fed)
*.6 FTE
1 FTE x Eng
*Four Directions programming. Obstetrician for 2- 1/2 days/ mos.FMU: 3- 1/2 days/w k??

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 62
APPENDIX 5: RQHR - CHRONIC DISEASE PREVENTION & MANAGEMENT CURRENT STATE PROGRAMS & SERVICES - JUNE, 2008 - (Short List)Adopted from (Format developed by Ann Stirling, Trillium Health Centre)
RQHR Health System
PROGRAM TITLE
TYPE
PHYS
ICIA
N R
EFER
RAL
REQ
UIR
ED
WAI
T TI
ME
(R/T
cap
acity
)
LEN
GTH
OF
PRO
GR
AM
IND
IVID
UAL
/ G
RO
UP
PHYS
ICIA
N (p
art o
f pro
gram
)
NU
RSI
NG
Adm
in s
uppo
rt
Med
ical
Med
ia
DIE
TIC
IAN
RT
(Pol
ysom
nogr
aphe
rs)
PSYC
HO
LOG
IST
HEA
LTH
INFO
MED
ICAL
PR
ACTI
TIO
N
KIN
ISIO
LOG
IST/
Exs.
The
rapi
st
SW Com
mun
ity S
uppo
rt/H
ome
Serv
ices
/Mea
l Ser
vice
s/ S
itter
Ser
vice
Volu
ntee
r
OT/
PT
Supe
rvis
or
PHAR
MAC
ISTS
MED
ICAT
ION
MAN
AGEM
ENT
VOLU
MES
CLI
NIC
AL P
ATH
WAY
S
PRO
CES
S M
AP C
OM
PLET
ED
COMMENTS
Prim
ary
Prev
entio
n
Mai
nten
ance
Seco
ndar
y Pr
even
tion
Long
Ter
m
Man
agem
ent
See Appendix 10 for more detail R
N
ACN
P
LPN
/ CN
S
Reg
Psy
ch
RN
ACN
P
PHAR
M
EXER
CIS
E
DIE
T
SMO
KIN
G
ALC
OH
OL
STR
ESS
MG
MT
SELF
MG
MT.
LITE
RAC
Y G
RAD
E LE
VEL
LAN
GU
AGES
Cardio-vascular Programming
Cardiac Rehab Education Programx* x No none 6 sess. G/I 1 FT nil (22h) (22h) (22h) (22h)
EdEd Ed Ed Ed Ed
xGr 6 Eng
180 cardiac
pts. x x
* Spousal primary prevention ( ) hrs donated by other departments.
Cardiac Rehabilitation Exercise Prog. (Dr. Paul Schwann Centre U of R.)
x* x x x Yes 1 mos. 36 attendances
I/G x x Guest Vol x Emerg MD
x Ed Ed Ed Ed x Gr 6 Eng 227** x x
Program started in 1981. * Primary Prevention for Spouses. ** Total on program for Cardiac Rehab and Chronic Disease Prog is 758
Congestive Heart Failure Clinic x x x Yes none LT I x x x x x x x x x x ? Gr.6 E/F 37 x x Program started March/08
Lipid Clinic x X X2-
5yrs N/Y 3-6w ks 4w ks I/G x xx x
Edx
Ed Ed Edx Gr 6-
8 Eng 920 x xVolumes 2007 stats
RQHR. Stroke Prevention Clinic (formerly South Sask Stroke Prevention Clinic)
Ed x NoYes & NP
12 days (range 0-30 days)*
1-2 attendances I x 1 FTE
0.2 FTE
0.2 FTE x ** Ed Ed Ed Ed Ed x
Gr6- 8 Eng
350-360 /yr x x
* Target 1-2 days. ** Pharmacist used on the w ard. Program going since 1993.
Heart Health Services:Rural East
x x No 4-6 w ks I x .2FT
x x
? Eng ?
x x
Ft. Qu'Appelle/Wolseley/Grenfell largest # based on Physicians referrals. Clinics average 1.5 every 2 w ks.
Heart Health Services:Rural West x x No ? * Ix x x
Gr 5 Eng ?x x * based on individual needs. 1 Dietitian
for Ft.Quappelle
Living Well with Stroke:(Heart & Stroke Foundation of Sask.)
1
1 SW trained from SWADD-WRC in 1999, another trained Mar'07 no record of programs to date. (unsure if second individual still employed by RQHR).**No one in rural areas w here there has been an identif ied need.
Heart to Heart Program (Heart & Stroke Foundation of Sask)
1CCNE
1 CCNE from Four Directions, and 1 Safety Consultant WRC trained March 2008- No programs to date.** Programs offered in the past in Moosomin, presently no facilitator available in this area.
Home Care:Live Well™ With Chronic Conditions Programming x? No
Depends on location & class
#s 6 w ks Gx x x x x x x x
Gr 6 Eng Max 90 Program started about 1 yr ago (Summer 2007??)
Home Care: Regular Programming
x x x No None n/a I x
x Urban: 100 x? 3
125 HHA x
Total 14 x x x
Population & Public Health
x ? ? ? No
*Drop in. 2 w ks for healthy
baby program/Active
Living/ Heart Healthy. ? *
*1FT-CCNE/1 FT NPs/PHNs 2
*.9FTE (Fed)
.4 FT Ment.Hea
lth
1 FTE
x Eng
*Four Directions programming. Obstetrician for 2- 1/2 days/ mos.FMU: 3- 1/2 days/w k??

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 63
APPENDIX 5: RQHR - CHRONIC DISEASE PREVENTION & MANAGEMENT CURRENT STATE PROGRAMS & SERVICES - JUNE, 2008 - (Short List)Adopted from (Format developed by Ann Stirling, Trillium Health Centre)
RQHR Health System
PROGRAM TITLE
TYPE
PHYS
ICIA
N R
EFER
RAL
REQ
UIR
ED
WAI
T TI
ME
(R/T
cap
acity
)
LEN
GTH
OF
PRO
GR
AM
IND
IVID
UAL
/ G
RO
UP
PHYS
ICIA
N (p
art o
f pro
gram
)
NU
RSI
NG
Adm
in s
uppo
rt
Med
ical
Med
ia
DIE
TIC
IAN
RT
(Pol
ysom
nogr
aphe
rs)
PSYC
HO
LOG
IST
HEA
LTH
INFO
MED
ICAL
PR
ACTI
TIO
N
KIN
ISIO
LOG
IST/
Exs.
The
rapi
st
SW Com
mun
ity S
uppo
rt/H
ome
Serv
ices
/Mea
l Ser
vice
s/ S
itter
Ser
vice
Volu
ntee
r
OT/
PT
Supe
rvis
or
PHAR
MAC
ISTS
MED
ICAT
ION
MAN
AGEM
ENT
VOLU
MES
CLI
NIC
AL P
ATH
WAY
S
PRO
CES
S M
AP C
OM
PLET
ED
COMMENTS
Prim
ary
Prev
entio
n
Mai
nten
ance
Seco
ndar
y Pr
even
tion
Long
Ter
m
Man
agem
ent
See Appendix 10 for more detail R
N
ACN
P
LPN
/ CN
S
Reg
Psy
ch
RN
ACN
P
PHAR
M
EXER
CIS
E
DIE
T
SMO
KIN
G
ALC
OH
OL
STR
ESS
MG
MT
SELF
MG
MT.
LITE
RAC
Y G
RAD
E LE
VEL
LAN
GU
AGES
Diabetes Programming
MEDEC x x x x NoDependent on priority 24-48 hrs to 5 mos.
LT I/G6.6 1 in CRI
2.9
3.3
0.8 x Ed Ed Ed Ed Ed Ed
Pictoral to Gr.8
Eng/ ltd others
1305 clients/yr x x
Ongoing Education & mgmt based on client need.
Endocrinology Consulting x x x Yes48 to 72 hrs to
8 mos. LT I x 1.6 x 579 pts/yrx
Retinopathy:Eye Screening Clinics x x x x No ? * **LT I.014 FTE 25 hrs/yr
.04 FTE 2- 76 hrs total/yr
2 FTE
.013 FTE 24 hrs/y
2- total 120 hrs/y
x 100 *** x X*: camera dow n, ** Dependent on degree of pathology, *** Anticipated target 250/y. Pilot 1 yr 6 mos. Funding concerns. They have identif ied screening criteria.
Podiatry Services (Pop. & Pub. Health) (x) x x xYes (MD/HCP)
None LT* I2.6
FTE* 2 FTE
1.5 FTE
1 FTE Ed Ed Ed Ed x Gr 6 Eng
1800 pt visits
annuallyx x
(x) Partial. LT*: Depends on severity. 2.6 FTE*: Podiatrists, not M.D. N/A: Not available
Rural Diabetes Education Program (DEP)
x x x No ? LT I/G x 0.2 1 x x* Ed Ed Ed Ed Ed x Gr.5 Eng ? x x x*:Community Pharmacist
Rural East DiabetesEducation Program x xNo I
x.3FT
xCertif ied Diabetic Nurse Educator & Chronic Disease Educator. Pharmacist in Moosomin.
Home Care:Live Well™ With Chronic Conditions Programming x? No
Depends on location & class
#s 6 w ks Gx x x x x x x x
Gr 6 Eng Max 90 Program started about 1 yr ago (Summer 2007)
Home Care: Regular Programming
x x x No None n/a I x
x Urban: 100 x? 3
125 HHA x
Total 14 x x x
*227 ongoing patients
* 2007 Calendar yr 321 Diabetic patients admitted w ith 227 ongoing.
Population & Public Healthx x x x No
*Drop in. 2 w ks for healthy
baby program. ? I/G **1FT-CCNE 2
*.9FTE (Fed)
.4 FT Ment.Hea
lth 1 FT x x Eng
*Four Directions programming. Obstetrician for 2- 1/2 days/ mos.FMU: 3- 1/2 days/w k??
Chronic Renal Insufficiency Programming CRI Program x x x Y/S 15 people LT I x 5F/T 3 2 F/T 1 2 ?x ?x ?x ? ? ?Eng 780 x x
Wait relative to May 16/08. Volumes:April/08
Hemodialysis Y/S No w ait LT I ?47 F/T
233 F/T 0 1 F/T 1.5 1 x x General Info provided Gr 6
Mult Lang 220 x x Volumes April/08. Access Nurse
Home Dialysis Training Program x x xY/N &S No w ait LT
x x x x 68 + 1 paed
x Volumes April/08. Access Nurse
Transplant Program Y/S Yes (47) ?x
??x Wait ? Provincial/ Transplant
Coordinators
Home Care:Live Well™ With Chronic Conditions Programming x? No
Depends on location & class
#s 6 w ks Gx x x x x x x x
Gr 6 Eng Max 90 Program started about 1 yr ago (Summer 2007??)
Home Care: Regular Programming
x x x No None n/a I x
x Urban: 100 x? 3
125 HHA x
Total 14 x x x
Population & Public Health x

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 64
APPENDIX 5: RQHR - CHRONIC DISEASE PREVENTION & MANAGEMENT CURRENT STATE PROGRAMS & SERVICES - JUNE, 2008 - (Short List)Adopted from (Format developed by Ann Stirling, Trillium Health Centre)
RQHR Health System
PROGRAM TITLE
TYPE
PHYS
ICIA
N R
EFER
RAL
REQ
UIR
ED
WAI
T TI
ME
(R/T
cap
acity
)
LEN
GTH
OF
PRO
GR
AM
IND
IVID
UAL
/ G
RO
UP
PHYS
ICIA
N (p
art o
f pro
gram
)
NU
RSI
NG
Adm
in s
uppo
rt
Med
ical
Med
ia
DIE
TIC
IAN
RT
(Pol
ysom
nogr
aphe
rs)
PSYC
HO
LOG
IST
HEA
LTH
INFO
MED
ICAL
PR
ACTI
TIO
N
KIN
ISIO
LOG
IST/
Exs.
The
rapi
st
SW Com
mun
ity S
uppo
rt/H
ome
Serv
ices
/Mea
l Ser
vice
s/ S
itter
Ser
vice
Volu
ntee
r
OT/
PT
Supe
rvis
or
PHAR
MAC
ISTS
MED
ICAT
ION
MAN
AGEM
ENT
VOLU
MES
CLI
NIC
AL P
ATH
WAY
S
PRO
CES
S M
AP C
OM
PLET
ED
COMMENTS
Prim
ary
Prev
entio
n
Mai
nten
ance
Seco
ndar
y Pr
even
tion
Long
Ter
m
Man
agem
ent
See Appendix 10 for more detail R
N
ACN
P
LPN
/ CN
S
Reg
Psy
ch
RN
ACN
P
PHAR
M
EXER
CIS
E
DIE
T
SMO
KIN
G
ALC
OH
OL
STR
ESS
MG
MT
SELF
MG
MT.
LITE
RAC
Y G
RAD
E LE
VEL
LAN
GU
AGES
Mental Health and Addictions Services-Depression
Adult Community Program x x x No 4-5 w ks Epis I/G x x x
Basi
c Ed
uca
Basi
c Ed
uca
x x
As re
q
Eng ** x xCapacity for new assessments is 576, ongoing caseload 350. Wait times avg. 4-5 w ks Urgent spots every w k.
Rural East- Adult Comm Prog x x ? No 4-6 w ks
Rural West- Adult Comm Prog x x Some No ? ?LT Ix x
?x x
Gr 5 Eng ?x x
Rehabilitation Program (Regina) x x x Y/S 4-6 w ks ?LT I x/S ? x Caseload capacity 640. 4-6 w k+ w ait time
Rehabilitation Program Grenfell 1/mos
Rehabilitation Program (Ft. Qu'App 1/mos)
Population & Public Health xObesity
Weight Management x 2 x* X*Gr 6-
8 Eng
* Limited services available 0.4 FTE Dietician dedicated to obesity. 0.25 FTE Ed Prog Functional Rehab Prog. And 0.5 FTE for General OP 0.1 FTE for Paeds dietician and obesity.
Rural West Dietitian Access x* x Limited access rurally more for diabetics or cardio conditions.
Rural East Dietitian Access x x Limited access rurally more for diabetics or cardio conditions.
Bariatric Surgical Assessment Clinicx
3yrsX X Yes 300 3 yrs I/G Surg x x 3 x x x x x x Ed Ed x x * Gr
6-8Eng 100 X X
Edmonton prog. Tools/pathw ay. 1 yr funding from Sask. Health. 6 mos demonstration of commitment and 2.5 yr follow -up. 3 and 6 mos follow -ups. Series of must attend education sessions. Education graded as per need (could be pictures if needed) Goal for 1 yr is 100 people.
Population & Public Healthx ? ? ? No
*Drop in. 2 w ks for healthy
baby program. ? **1FT-CCNE 2
*.9FTE (Fed)
.4 FT Ment.Hea
lth x Eng
*Four Directions programming. Obstetrician for 2- 1/2 days/ mos.FMU: 3- 1/2 days/w k??

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 65
Speci
alty C
are
Support
S
erv
ices
Rest
ora
tive
Continuin
g
Care
Pri
mary
Health
Care
RQ
HR
Sask
. H
ealth
Gra
nts
Fee f
or
Serv
ice
Donations
/ Fu
nd R
ais
ing
Tota
l B
udget
Rura
l
Urb
an
Rura
l
Urb
an
Speci
alis
t
Fam
ily
Physi
cian
Respiratory
Programming
Cardiac-vascularProgramming
APPENDIX 6: RQHR -CDP&M- ORGANIZATION / BUDGET / LOCATION / PHYSICIAN SUPPORT - AUGUST, 2008 - (Short List) (Format developed by Brenda Collacott- RQHR)
RQHR Health System PROGRAM TITLE
Organizational Structure Portfolio Funding / Budget
Service Location
Physician Support COMMENTSRQHR Community
Paed Asthma Clinic x 0
Initial start up costs ( Small
Pharmaceutical donations)
Nil RGH-1B Dr. Talukdar * There is no funding allocated from RQHR for this program,
Small pharmaceutical donations assist w ith the service provision.
Adult Asthma Education Program x $6,000/yr $6,000/yr WRC Dr. R. H. Abdulla
COPD Rehab Exs & Ed. Program x *see comment
$50,000 August
7/08
Donations: $32,000
Equipment,
Southland Mall
Dr. R. H. Abdulla
Pilot Project 07-08 * Cost incl approx $4-$5,000 per month in w ages for RT's and ET's and another $500- 1,000 per month in general operating expenses. Currently space is rent-free
but w ould cost $60,000 per yr.
Home Oxygen Assessment & Testing x x(Rural) * see comment
x Home Care
WRC-OP. RGH & PH
OP/IP
Dr. R. H. Abdulla *Approx $30-$35,000 in costs related to salaries
Sleep Disorders Clinic x $400,000 SGI: $200,000 $600,000 RGH Dr. Sridhar
Ventilator Programs x $113,000
$113,000
WRC Pt's Home Dr. R. H.
Abdulla & Dr. Sridhar
Home Vent Program Pilot 1 yr 2008-09, Costs for LTV are closer to $250,000/yr- w ill be over-budget mostly due to
salaries. Approx $20-25,000 per year for supplies/equipment.
Home Care: Live Well™ Programming x $20,000 $20,000 x x x x
There has been no Live Well ™ programming offered in Rural West, but Regina and Regina Beach held a total of 6
classes (5 & 1) and Rural East held 3 classes (One each at Broadview , Ochapaow ace and Cow esses) Classes are held anyw here in the RQHR w hen there are 12 interested
people and peer leaders available.
Home Care: Regular Programming x x x4211 Albert
St. x x
Population & Public Health X x x x x Dr. M. Hennink
Cardiac Rehab Education Program x Telehealth* RGH & PHDr. G. J. Garbe
( Dept. Head:Cardio)
Plans to deliver program via telehealth 2 x per year.
Cardiac Rehabilitation Exercise Prog. (Dr. Paul Schwann Center, U of R)
x $90,000 Approx. $180,000
Paul Schw ann
U of R
Dr. G. J. Garbe (Dept.
Head:Cardio )
Dr. B. Pillay, Dr. V. Scott
Congestive Heart Failure Clinic x PH -2CDr. D. R.
Murthy(Med. Director)
Lipid Clinic x xRGH Med.
Off ice Wing MEDEC
Dr. Mohammed, Dr. Mann
RQHR Stroke Prevention Clinic (formerly South Sask. Stroke Prevention Clinic)
x RGH- 5A Dr. C.P.V. Nair (Dept. Head)
The name change occurred this fall, w ith the hopes that there w ill be more stroke prevention clinics in other Regions
starting up.
Heart Health Services (Rural East & Rural West)
x x x
Home Care: Live Well™ Programming x $20,000 $20,000 x x x x
There has been no Live Well ™ programming offered in Rural West, but Regina and Regina Beach held a total of 6
classes (5 & 1) and Rural East held 3 classes (One each at Broadview , Ochapaow ace and Cow esses) Classes are held anyw here in the RQHR w hen there are 12 interested
people and peer leaders available.
Home Care: Regular Programming x x x4211 Albert
St. x x
Population & Public Health x x Dr. M. Hennink Registered Dietitian provides nutritional counselling re lipids.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 66
Speci
alty C
are
Support
S
erv
ices
Rest
ora
tive
Continuin
g
Care
Pri
mary
Health
Care
RQ
HR
Sask
. H
ealth
Gra
nts
Fee f
or
Serv
ice
Donations
/ Fu
nd R
ais
ing
Tota
l B
udget
Rura
l
Urb
an
Rura
l
Urb
an
Speci
alis
t
Fam
ily
Physi
cian
Diabetes
Programming
Chronic
Renal
Insufficiency
Dr. M. HenninkxPopulation & Public Health
xx4211 Albert
St.
There has been no Live Well ™ programming offered in Rural West, but Regina and Regina Beach held a total of 6
classes (5 & 1) and Rural East held 3 classes (One each at Broadview , Ochapaow ace and Cow esses) Classes are held anyw here in the RQHR w hen there are 12 interested
people and peer leaders available.
Home Care: Regular Programming x x x
x x$20,000 x x Home Care: Live Well™ Programming x $20,000
? Dr. Shoker, or Dr. Hassan
(S'toon) RGH- 4E?Transplant Program x
? Dr.S. Karunakaran
RGH- Unit 4EHome Dialysis Training Program x ?
Dr. C.B. Wilson ?CCAx 10M RGH-1AProgramming
Hemodialysis x ? x
Dr. C. B. Wilson (Dept Head)
RGH- Unit 4E
?CRI Program x
Dr. M. HenninkPrimarily Chronic Conditions Nurse w ith support from
dietitian, Community Development Coordinator etc. * Four Directions and Albert St.
x*Population & Public Health x x
x x4211 Albert
St.
There has been no Live Well ™ programming offered in Rural West, but Regina and Regina Beach held a total of 6
classes (5 & 1) and Rural East held 3 classes (One each at Broadview , Ochapaow ace and Cow esses) Classes are held anyw here in the RQHR w hen there are 12 interested
people and peer leaders available.
Home Care Rural & Urban: Regular Programming
x x x
x x$20,000 x x x $20,000 Home Care: Live Well™ Programming
*RQHR offers No basic skin/nail care services w ithin the city. Clients must f ind a private provider.
x only
Based in Fort Qu'Appelle. Monthly clinics in Belcarres, Lestock & Raymore, Moosomin, Whitew ood, Broadview ,
Wolseley, Indian Head.
Rural Home Care: Foot & Nail Care Service
x x* x requested
Dr. Henninkxx (RD & CCNE)
xRural Diabetes Education Program (DEP)
x (Moosomin-Pharmicist)
Dr. A Rohrmann Budget includes funds from RQHR and fee for service. $553,619.00 Satellite Clinics
RGH- Med Off ice Wing
Home Care/Sat
ellite Clinics
x* Eye Screening planned in Rural, but hasn't happned yet, due to camera damage: reduced clinics as a result. Increase to one on site clinic per month and every second month have
travelling clinic
Podiatry Services x x* x*
Dr. Garcia equipment donated
Preliminary Projection $260,000
Pending PH -3rd Fl.
One endo is on staff, the other is in private practice. Need for a third endocrinologist has been identif ied. No Pediatric
Endocrinologist in Regina- a major gap.
Retinopathy/ Eye Screening Clinics x ? (Adhoc)
RGH- Med. Off ice Wing
Dr. S.S. Mann. Dr. E.
Mohammed x Dr. MannEndocrinology Consulting
Dr. S.S. Mann (Dept. Head)
Currently Dept. Head has limited involvement w ith the program or regional big picture.
RGH Med Off Wing + In pts RGH, PH & WRC
MEDEC x x*
Community
APPENDIX 6: RQHR -CDP&M- ORGANIZATION / BUDGET / LOCATION / PHYSICIAN SUPPORT - AUGUST, 2008 - (Short List) (Format developed by Brenda Collacott- RQHR)
RQHR Health System PROGRAM TITLE
Organizational Structure Portfolio Funding / Budget
Service Location
Physician Support COMMENTSRQHR

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 67
Speci
alty C
are
Support
S
erv
ices
Rest
ora
tive
Continuin
g
Care
Pri
mary
Health
Care
RQ
HR
Sask
. H
ealth
Gra
nts
Fee f
or
Serv
ice
Donations
/ Fu
nd R
ais
ing
Tota
l B
udget
Rura
l
Urb
an
Rura
l
Urb
an
Speci
alis
t
Fam
ily
Physi
cian
Mental Health
and Addictions
Services -
Obesity
Programming
Dr. M. HenninkPopulation & Public Health x
Allied Health U
of R. Dr.Kaban1 yr Pilot
ProjectBariatric Surgical Assessment Clinic x
Registered Dietitian counsels re: w eight management. Based in Fort Qu'Appelle and Grenfell w ith clinics in Balcarres, Lestock, Moosomin, w hitew ood, Broadview , Wolseley,
Indian Head.
x*
Obesity programming is a small portion of w hat service is presently provided. .4 FTE Dietician for Obesity, .5 FTE OP
Program and .1 FTE for Paeds.
Rural Community Dietician Services x x
? Dr. Achyuthan
WRC/ RGH/PH
xWeight Management x
Dr. M. HenninkPopulation & Public Health x
Dr. Natarajan(Dept
Head) x 2110
Hamilton
Based in Fort Qu'Appelle and Grenfell w ith clinics in Balcarres, Lestock, Moosomin, Whitew ood, Broadview ,
Wolseley, Indian Head.
Rehabilitation Program x x
Dr. Emsliexx x
Depression
Rural Adult Community Programs
Dr. Natarajan(Dept
Head)
2110 HamiltonAdult Community Program x ?
Community
APPENDIX 6: RQHR -CDP&M- ORGANIZATION / BUDGET / LOCATION / PHYSICIAN SUPPORT - AUGUST, 2008 - (Short List) (Format developed by Brenda Collacott- RQHR)
RQHR Health System PROGRAM TITLE
Organizational Structure Portfolio Funding / Budget
Service Location
Physician Support COMMENTSRQHR

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 68
COMMENTS
A B C A B CRespiratory Programming 2003 84 0
2004 119 02005 97 02006 96 02007 30 02008 1 2-3 mos 19 (6 mos) 0
2005-06
2006-07
2007-08 0 0 0 0 0 0 Not Available 02003-04
2004-05
2005-06 252006-07 40 1.5 yrs 40-502007-08 60 1 yr 40-50 90 or less
2005-06 02006-07 0
2007-08
30 WRC 300-PF
WRC- 3-5 wks. PFL 6
mos.1120 (WRC 496, PF
632) 02005-06 1100 5 yrs2006-07 1200 5 yrs
2007-081300 5 yrs
606-see comment
450-see comment
2005-06 WRC: 92006-07 WRC: 9
2007-080 0 0 0 0 0 2 or less
Home LTC: 6,WRC: 10/12
2005-06 n/a n/a n/a n/a n/a n/a n/a n/a2006-07 n/a n/a n/a n/a n/a n/a n/a n/a
2007-08 3 varies75 (2007)* 10
(2008)
2005-06
2006-07
2007-08
NW: 46,688.75, SW: 40,579.26, SC 38,165.75
2005-06
2006-07
2007-08
Volumes based on a unit o f service= 1 hr. Largest service areas based on vo lumes 1.
NW Regina, 2. SW Regina, 3. SCentral Regina.Able to determine # new admissions, but not # visits for a diagnosis. Data based on primary diagnosis, not co-morbidities.
Population & Public Health
xxHome Care: Regular Programming
Procura Program
(Unable to track by
diagnosis)
Paper in Pt's home.
Electronic in off ice.
Excel*
Volumes based on total number attending, unknown if Respiratory Conditions were part
of co-morbidity.* (RQHR reports) 72 what Live Well Prog reports.
xHome Care: Live Well™ Programming Paper Excel x x x/o
xx x/oVentilator Programs Paper PaperExcel for Home Pts
only
Volumes increasing for admission & ongoing up to approx 700-750 per
year.Sleep Disorders Clinic
Pathw ays & ACCURO
Electronic (Vendor for
Prov. Project.)
PHS & ACCURO x
xHome Oxygen Assessment & Testing Pathw ays PaperPaper & RTStats
Database, Pathw ays
COPD Rehab Exs & Ed. Program Manual Paper Manual (setting up data base)
x
Volumes based on calendar year. Wait time depends on Dr. Talukdar and RNs availability and space. Usually 2nd and
4th Wed. of each month: Full days)
Adult Asthma Education Program Pathw ays Paper Nil x x
Med
ical
Imag
ing
Paed Asthma Clinic Pathw ays Paper Pathw ays & Paper x
Ren
al P
rogr
ams
Inpa
tient
Uni
ts
WR
C: O
T/PT
/SLP
Clin
ical
En
gine
erin
g.
Eye
Scre
enin
g C
linic
Foot
Scr
eeni
ng
Clin
icPs
ycho
logi
st
Orth
otic
Lab
s
Cas
t Clin
icO
stom
y &
Wou
nd
Car
eM
EDEC
Lipi
d C
linic
Hom
e C
are
Staf
f
LTC
- Sta
ff
RQ
HR
(Reg
. Die
titi
CH
F C
linicVolumes:
Ongoing Follow-up (Fiscal) Ph
ysic
ians
Phar
mac
ists
Exs
. The
rapi
st
YEA
RS
Wait List Wait Times
Volumes Admission (Fiscal:
April- Mar)
APPENDIX 7: RQHR - CHRONIC DISEASE PREVENTION & MANAGEMENT CURRENT STATE- IT/CAPACITY/PARTNERS - AUGUST, 2008 - (Short List) (Format developed by Brenda Collacott- RQHR)
RQHR Health System PROGRAM TITLE
IT CAPACITYPARTNERS / STAKEHOLDERS (Potentially needing file
information access)
Bookin
gs
Medic
al R
eco
rd
Data
Colle
ctio
n

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 69
COMMENTS
A B C A B CRespiratory Programming 2003 84 0
2004 119 02005 97 02006 96 02007 30 02008 1 2-3 mos 19 (6 mos) 0
2005-06
2006-07
2007-08 0 0 0 0 0 0 Not Available 02003-04
2004-05
2005-06 252006-07 40 1.5 yrs 40-502007-08 60 1 yr 40-50 90 or less
2005-06 02006-07 0
2007-08
30 WRC 300-PF
WRC- 3-5 wks. PFL 6
mos.1120 (WRC 496, PF
632) 02005-06 1100 5 yrs2006-07 1200 5 yrs
2007-081300 5 yrs
606-see comment
450-see comment
2005-06 WRC: 92006-07 WRC: 9
2007-080 0 0 0 0 0 2 or less
Home LTC: 6,WRC: 10/12
2005-06 n/a n/a n/a n/a n/a n/a n/a n/a2006-07 n/a n/a n/a n/a n/a n/a n/a n/a
2007-08 3 varies75 (2007)* 10
(2008)
2005-06
2006-07
2007-08
NW: 46,688.75, SW: 40,579.26, SC 38,165.75
2005-06
2006-07
2007-08
APPENDIX 7: RQHR - CHRONIC DISEASE PREVENTION & MANAGEMENT CURRENT STATE- IT/CAPACITY/PARTNERS - AUGUST, 2008 - (Short List) (Format developed by Brenda Collacott- RQHR)
RQHR Health System PROGRAM TITLE
IT CAPACITYPARTNERS / STAKEHOLDERS (Potentially needing file
information access)
Bookin
gs
Medic
al R
eco
rd
Data
Colle
ctio
n
YEA
RS
Wait List Wait Times
Volumes Admission (Fiscal:
April- Mar)
Volumes: Ongoing
Follow-up (Fiscal) Ph
ysic
ians
Phar
mac
ists
Exs
. The
rapi
st
Hom
e C
are
Staf
f
LTC
- Sta
ff
RQ
HR
(Reg
. Die
titi
CH
F C
linic
Cas
t Clin
icO
stom
y &
Wou
nd
Car
eM
EDEC
Lipi
d C
linic
Eye
Scre
enin
g C
linic
Foot
Scr
eeni
ng
Clin
icPs
ycho
logi
st
Orth
otic
Lab
s
Ren
al P
rogr
ams
Inpa
tient
Uni
ts
WR
C: O
T/PT
/SLP
Clin
ical
En
gine
erin
g.M
edic
al Im
agin
g
Paed Asthma Clinic Pathw ays Paper Pathw ays & Paper x
Volumes based on calendar year. Wait time depends on Dr. Talukdar and RNs availability and space. Usually 2nd and
4th Wed. of each month: Full days)
Adult Asthma Education Program Pathw ays Paper Nil x x
COPD Rehab Exs & Ed. Program Manual Paper Manual (setting up data base)
x
Home Oxygen Assessment & Testing Pathw ays PaperPaper & RTStats
Database, Pathw ays
x
Sleep Disorders ClinicPathw ays &
ACCURO
Electronic (Vendor for
Prov. Project.)
PHS & ACCURO xVolumes increasing for admission & ongoing up to approx 700-750 per
year.
Ventilator Programs Paper PaperExcel for Home Pts
only x x/o x
Home Care: Live Well™ Programming Paper Excel x x x/o xVolumes based on total number attending,
unknown if Respiratory Conditions were part of co-morbidity.* (RQHR reports) 72 what
Live Well Prog reports.
Home Care: Regular Programming
Procura Program
(Unable to track by
diagnosis)
Paper in Pt's home.
Electronic in office.
Excel* x x
Volumes based on a unit of service= 1 hr. Largest service areas based on vo lumes 1.
NW Regina, 2. SW Regina, 3. SCentral Regina.Able to determine # new admissions, but no t # visits fo r a diagnosis. Data based on primary diagnosis, no t co-morbidities.
Population & Public Health

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 70
COMMENTS
A B C A B CDiabetes 2005-06 Av of 332 clients, all types 1398 clients 4000 visitsProgramming 2006-07 Av of 327 clients,all types 1205 clients 4436 visits
2007-08Av of 280 clients, all types 24-48hrs
Up to 5 mos. 1305 clients 4692 visits
2005-06 Av of 144 pts, all types 420 pts 1258 visits2006-07 Av of 138 pts, all types 619 pts 1462 visits
2007-08 Av of 125 pts, all types 48-72 hrsUp to 8 mos. 579 pts 1554 visits
2005-06 n/a n/a n/a n/a n/a n/a n/a n/a2006-07 n/a n/a n/a n/a n/a n/a 37/40 n/a
2007-08 ??
80 since Jan'08*Approx
250/yr.
? 200- Follow-up.? 50
Treatment
2005-06
2006-07
2007-08 0 0 0 600 * *2005-06 101 clients 43 visits2006-07 123 clients 36 visits
2007-08
Up to a mos for initial. 12 to 18 mos for f/u visit 76 clients 38 visits
2005-06 RD 91 clients RD 33 visits2006-07 RD 104 clients RD 72 visits
2007-08
CCNE 47 clients. Pharmacist: 30 N/P (52 Active)
CCNE 19 visits,
Pharmacist 33 Follow ups
2005-06
2006-07
2007-08
2005-06 n/a n/a n/a n/a n/a n/a n/a n/a2006-07 n/a n/a n/a n/a n/a n/a n/a n/a
2007-08 3 varies75 (2007)* 10
(2008)
Home Care: Regular Programming
Procura Program
(Unable to track by
diagnosis)
Paper in Pt's home.
Electronic in off ice.
Excel2007 Cal
yr. n/a n/a 321 Diabetic Pts227 Ongoing Diabetic Pts.
x* See Upper Sections for Home Care
total volumes. They do track their Diabetic Admissions & Discharges.
2005-06
2006-07
2007-08
Volumes based on total number attending, unknown if Diabetes was part of co-
morbidity..* (RQHR reports) 72 what Live Well Prog reports.
Population & Public Health (CCNE in North Central Regina)
x/o xx xHome Care: Live Well™ Programming Paper Excel
* April 1/07 to March 31/08, # seen on initial visit.** Number seen on follow-up by Dietitian. CCNE has not had a full yr of data collected
yet.
Home Care: Regular Programming (Includes Foot & Nail Care in Rural East & Rural West)
Rural East Diabetes Education Program (Dietitian and Chronic Conditions Nurse Educator) Moosomin:(Pharmacist)
Manual (Grenfell excel spread
sheet, no linkages rurally)
PaperDietitian Client Tracking Prog
(Designed by M. Hartness- Sun Country
Rural Diabetes Education Program (DEP)
Paper PaperACCESS Data
Base (Limited for their needs)
ox xxx x Podiatry Services Paper Paper Manual (Going to ACCURO- Fall '08)
x o
* Currently trialing new camera.. Anticipate about 250 screenings per yr. 20% require
treatment, and 80% are followed up. This does not included pre-diabetics. (June, 2008)1 yr.
pilot project, now running 14 mos. Communication to Fam Phys by Specialist.
xx x
Endocrinologists also w ork in Lipid Clinic
Retinopathy/Eye Screening ClinicsPaper. Trying
Pathways for 3rd time.
Paper file: Free standing elect.
prog. for angiograms and
photographs
Excel Prog.and Finance pkg for
charge statistics.x
x xx
MEDEC clerical staff also support Lipid Clinic
Endocrinology ConsultingComputer
based Pathw ays
Paper Paper x
xx xx xx xMEDECComputer based-
Pathw aysPaper
Aw aiting CDM- ToolKit, some Excel
databases
Med
ical
Imag
ing
Ren
al P
rogr
ams
Inpa
tient
Uni
ts
WR
C: O
T/PT
/SLP
Clin
ical
En
gine
erin
g.
Eye
Scre
enin
g C
linic
Foot
Scr
eeni
ng
Clin
icPs
ycho
logi
st
Orth
otic
Lab
s
Cas
t Clin
icO
stom
y &
Wou
nd
Car
eM
EDEC
Lipi
d C
linic
Hom
e C
are
Staf
f
LTC
- Sta
ff
RQ
HR
(Reg
. Die
titi
CH
F C
linicVolumes:
Ongoing Follow-up (Fiscal) Ph
ysic
ians
Phar
mac
ists
Exs
. The
rapi
st
YEA
RS
Wait List Wait Times
Volumes Admission (Fiscal:
April- Mar)
APPENDIX 7: RQHR - CHRONIC DISEASE PREVENTION & MANAGEMENT CURRENT STATE- IT/CAPACITY/PARTNERS - AUGUST, 2008 - (Short List) (Format developed by Brenda Collacott- RQHR)
RQHR Health System PROGRAM TITLE
IT CAPACITYPARTNERS / STAKEHOLDERS (Potentially needing file
information access)
Bookin
gs
Medic
al R
eco
rd
Data
Colle
ctio
n

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 71
COMMENTS
A B C A B C2005-06
2006-07
2007-08 15** 780*2005-06 0 0 0 0 0 02006-07 0 0 0 0 0 02007-08 0 0 0 0 0 0 220*2005-06
2006-07
2007-08 0 68 + 1 ped.*2005-06
2006-07
2007-08 46/1* ??2005-06 n/a n/a n/a n/a n/a n/a n/a n/a2006-07 n/a n/a n/a n/a n/a n/a n/a n/a
2007-08 3 varies75 (2007)* 10
(2008)
2005-06
2006-07
2007-08 n/a n/a *2005-06
2006-07
2007-08
2005-06
2006-07
2007-08 * 1-3 mos.2005-06
2006-07
2007-08
Adults: 4-6 wks. Child & Youth 2-4
wks152 New
Admissions
356 active: 78 Mood
Disorders*
2005-06
2006-07
2007-08
2005-06
2006-07
2007-08 232* 2mos. 7mos.
2005-06
2006-07
2007-08
APPENDIX 7: RQHR - CHRONIC DISEASE PREVENTION & MANAGEMENT CURRENT STATE- IT/CAPACITY/PARTNERS - AUGUST, 2008 - (Short List) (Format developed by Brenda Collacott- RQHR)
PROGRAM TITLE
IT CAPACITYPARTNERS / STAKEHOLDERS (Potentially needing file
information access)
Bookin
gs
Medic
al R
eco
rd
Data
Colle
ctio
n
YEA
RS
Wait List Wait Times
Volumes Admission (Fiscal:
April- Mar)
Volumes: Ongoing
Follow-up (Fiscal) Ph
ysic
ians
Phar
mac
ists
Exs
. The
rapi
st
Hom
e C
are
Staf
f
LTC
- Sta
ff
RQ
HR
(Reg
. Die
titi
CH
F C
linic
Cas
t Clin
icO
stom
y &
Wou
nd
Car
eM
EDEC
Lipi
d C
linic
Eye
Scre
enin
g C
linic
Foot
Scr
eeni
ng
Clin
icPs
ycho
logi
st
Orth
otic
Lab
s
Ren
al P
rogr
ams
Inpa
tient
Uni
ts
WR
C: O
T/PT
/SLP
Clin
ical
En
gine
erin
g.M
edic
al Im
agin
g
CRI Program MIQSMIQS
(Available to all in CRI progs)
MIQS x * April 16/08. ** May/08 Communication via the Specialist.
Hemodialysis MIQS MIQS (Elect. Med. Rec.)
MIQS * * Communication via the Specialist
Home Dialysis Training Program MIQS MIQS MIQS * * April 16/08. Communication via the Specialists.
Transplant Program
MIQS (access to all Prov.
Files)MIQS MIQS x * 46 Cadaveric/ 1 Living. Wait
dependent on availability of donors.
Home Care: Live Well™ Programming Paper Excel x x x/o xVolumes based on total number attending, unknown if CRI was part of co-morbidity..* (RQHR reports) 72 what Live Well Prog
reports.
Home Care: Regular Programming
Procura Program
(Unable to track by
Paper in Pt's home.
Electronic in office.
Excel x* See sections above for total
volumes, #'s of CRI clients unknow n.
Population & Public Health
Adult Community Program Manual PaperACCESS Data
Base (Limited for their needs) * Program screens prior to
admission.
Rural East - Adult Community Prog
Mental Health Info system Scheduler
Paper
Mental Health Info System only used rurally ? CAFUS/ ACCESS-Limited
* Diagnosis could be bipolar, dysthemia or deprssion.
Rural West - Adult Comm. ProgrTo check w ith
Janet Bidel
Rehabilitation Program
Pathways (Ment. Health app'ts do
not show for other depts.
Paper ? *Psychiatry Wait List (Staff Shortages) June 1/2008.
Population & Public Health

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 72
COMMENTS
A B C A B CObesity 2005-06 2-3 w ks 319Programming 2006-07 355
2007-08 N/A 4-6 w ks 3702005-06
2006-07
2007-08 N/A N/A2005-06
2006-07
2007-08 N/A N/A 26 Initial 11 Follow -ups2005-06
2006-07
2007-08 300?1-3 yrs 100 /yr Target
2005-06
2006-07
2007-08
Program capped at 300 referrals. Referrals continue beyond this cap, presently in excess of an additional
300 clients.
Population & Public Health
xxBariatric Surgical Assessment Clinic ManualMaintained at Allied Health
Detailed database maintained (BAROS)
x
Rural East Dietitian
Manual (Grenfell excel spread
sheet, no linkages rurally)
PaperDietitian Client Tracking Prog
(Designed by M. Hartness- Sun Country
Numbers unknow n, need identif ied as great, but no present tracking system
used.
Rural West Dietitican AccessTo check w ith
Janet Bidel
Weight Management Manual Paper Volumes Only (Excel)
Med
ical
Imag
ing
Ren
al P
rogr
ams
Inpa
tient
Uni
ts
WR
C: O
T/PT
/SLP
Clin
ical
En
gine
erin
g.
Eye
Scre
enin
g C
linic
Foot
Scr
eeni
ng
Clin
icPs
ycho
logi
st
Orth
otic
Lab
s
Cas
t Clin
icO
stom
y &
Wou
nd
Car
eM
EDEC
Lipi
d C
linic
Hom
e C
are
Staf
f
LTC
- Sta
ff
RQ
HR
(Reg
. Die
titi
CH
F C
linicVolumes:
Ongoing Follow-up (Fiscal) Ph
ysic
ians
Phar
mac
ists
Exs
. The
rapi
st
YEA
RS
Wait List Wait Times
Volumes Admission (Fiscal:
April- Mar)
APPENDIX 7: RQHR - CHRONIC DISEASE PREVENTION & MANAGEMENT CURRENT STATE- IT/CAPACITY/PARTNERS - AUGUST, 2008 - (Short List) (Format developed by Brenda Collacott- RQHR)
RQHR Health System PROGRAM TITLE
IT CAPACITYPARTNERS / STAKEHOLDERS (Potentially needing file
information access)
Bookin
gs
Medic
al R
eco
rd
Data
Colle
ctio
n

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 73
APPENDIX 8
Assessment of Current State - “Strengths, Gaps and Opportunities” This document summarizes the strengths, gaps and opportunities of the current state of RQHR CDPM services and programs. The gaps identified are prominent enough to be identified as areas which need further discussion regarding potential strategy development. It should be noted that these gaps were not relevant to every service area. The summary follows the same sequence as Accreditation Canada’s 2008 Populations with a Chronic Condition standards. POPULATION HEALTH OUTCOMES/FUNCTIONAL AND CLINICAL OUTCOMES: Strengths: The CDPM Committee has identified the Expanded Prevention and Management Model
for Chronic Disease as the Model to be used as a framework for strategy development. The model outcomes are described in terms of Population Health Outcomes and Functional and Clinical Outcomes.
Within Population and Public Health a large amount of data is collected. pertaining to chronic disease
The Region has active Research and Performance Support and Quality Improvement Departments to support quality improvement activities and outcome measurement.
Many of the RQHR chronic disease related programs use some sort of evaluation tool.
Gaps: Utilization of a quantitative outcome evaluation tool for patient care or program
evaluation for chronic disease prevention and management does not presently consistently occur.
Utilization of patient outcome measurement tools in the establishment of the patient’s treatment plan does not occur consistently
We presently do not have the administrative capacity to undertake continuous (regular) patient and program evaluation.
Evaluation tools used in many programs focus on patient volumes, and not necessarily on patient outcomes.
Utilization of the data collected by Population and Public Health (Epidemiology) does not occur consistently in all service delivery areas.
It is not well known across CDM service delivery areas what data is available through Population and Public Health
Often measurement tools are developed by programs in response to a perceived problem rather than as a means for pro-active tracking and monitoring.
Patient outcome results are not regularly reported.
Opportunities: Within health care generally, more attention is being paid to Outcomes
Measurement, and it is starting to become a part of organizational culture within the RQHR. .
PACIC (Patient Assessment of Chronic Illness Care) and the ACIC (Assessment of Chronic Illness Care) are previously developed, valid and reliable outcomes measurement tools. They are available to the RQHR and can be used as internal measures and measures to compare to other service delivery programs.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 74
COMMUNITY 8.1 BUILD HEALTHY PUBLIC POLICY Strengths:
RQHR Population and Public Health has a role in advocating for social policy development. Many of these policies have a direct and/or indirect relationship with chronic disease prevention and management.
Gaps:
There is no clear process when the need for policy development is identified by those providing the care in Chronic Disease Management to bring these ideas forward.
Opportunities:
The process of evaluation of the current state has given us an opportunity to improve the communication between Population and Public Health and the Care management side of Chronic Condition programming.
8.2 CREATE SUPPORTIVE ENVIRONMENTS Strengths:
RQHR Population and Public Health provides numerous services to create a supportive environment at Health Centers, (ie: Four Directions and the Al Ritchie Center, and supporting community programming such as “In Motion”.
A Challenge:
Health promotion and education experts are beginning to realize that education alone does not necessarily result in action and change by individuals.
Gaps: Availability of interpreter services will be limited as of April 1, 2009, as the Open Door
Society will no longer be able to provide this service. (Privacy and Confidentiality issues need to be addressed) The Region will require adequate resources to provide this service.
Opportunities:
Opportunities in schools, workplaces etc. to make them healthier places for CD prevention and for those already living with a CD.
Eagle Moon has the availability of a grant to have “system navigators” on staff to link Métis individuals and community services within RQHR (Lestock).
Bring the services to the community. Develop partnerships outside of the community to allow the service access to
happen. 8.3 STRENGTHEN COMMUNITY ACTION Strengths:
The RQHR offers programs through our health centers for those with multiple problems this is being achieved through the Al Ritchie and Four Directions Health Centers.(Not considered by some to be Community Action).
The RQHR utilizes and benefits from numerous partnerships within the community at all levels.
The RQHR is committed to engaging community members as partners in planning, developing and evaluating health services.
The RQHR is committed to the principles of community development.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 75
There are instances of effective partnerships between region programs and NGOs i.e.: Region with CDA, Kidney Foundation etc.
A Challenge:
Community development is a long process.
Gaps: We do not fully utilize the partnerships available, nor do we acknowledge those
partnerships. We don’t have a mechanism for tracking immunization and flu shots for those with
chronic conditions. Communication can be a challenge with such a large organization The benefits of health promotion and chronic disease prevention are difficult to
measure in the short term. Opportunities:
The Community in many ways demonstrates its desire for involvement, this needs to be directed and focused to areas of greatest need.
HEALTH SYSTEM 8.4 SELF MANAGEMENT/ DEVELOP PERSONAL SKILLS Strengths:
There are many different disease specific education programs available to the client that can be accessed on a self- referral basis to assist the individual in self-management.
The education materials generally are available in a variety of literacy levels, and languages as needed, aside from a few areas.
There are education programs available to assist staff in the coaching of the individual to develop the personal skills required for self-management. ie: Three Minute Empowerment, Motivational Interviewing, PACE (a comprehensive guide to counseling for healthy active living to assist health care providers in effectively increasing their patients’ physical activity levels and improving their eating habits), and STEP (Step Test Exercise Prescription) education.
Live Well ™ with Chronic Conditions; a peer led program to assist in problem solving and self management programming is available within the region.
Gaps:
Access to some of these programs are limited because of capacity issues.( COPD Rehab Education Programming, Mental Health: Depression Management with Chronic Disease Conditions)
The Region offers a very small amount of weight management programming. The emphasis due to capacity limits are placed on the most severe problems, minimal assistance is available to prevent obesity.
Formalized Self Management Support is not a consistent component of all RQHR Chronic Disease management programs..
Patients tell us that the programs are not holistic in nature. In certain chronic condition programs information provided to patients is in-consistent. Not all health care providers involved in chronic disease management programs are
trained in self management /personal skill development facilitation. No sustainable funding for co-ordination of the Live Well ™ with Chronic Conditions
Program. Programming is splintered for those with co-morbid conditions.
.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 76
Opportunities: The education programming consistency is being worked on by the Diabetes Sub-
Committee to ensure consistency of Diabetes Education programming throughout the health region.
8.5 DELIVERY SYSTEM DESIGN
Strengths:
Health line (telephone and on-line) offers general information on risks for chronic diseases and has some screening capabilities.
Access to disease specific education programming is available to the patient on self referral in a number of areas.
Access to Mental Health and Addictions services and Diabetes programming and Lipid Clinic(Urban) is by self referral.
Most family physicians do some screening for chronic disease Screening for Diabetic eye complications is being started, with the plan to go Rural. Screening for Diabetic foot complications is being done with plans for expanded and
enhanced prevention and management clinics. The region offers a cross section of services in most areas ( the exception being weight
management programming) Services are primarily offered in the Urban center where the largest population base
is, or where funding partnerships have provided opportunities such as space or equipment for service provision. The exception is diabetes education.
Creativity in developing programs as seen in the funding base partnerships developed for COPD Rehabilitation Programming, the Sleep Disorders Programming and the CHF clinic.
Gaps:
Not everyone has a telephone or a computer to access Health Line. Utilization of Health line (telephone) by consumers for information about certain
Chronic Conditions is limited. Many members of the public don’t necessarily recognize risk factors in themselves or
take action to get themselves screened. Education about prevention doesn’t necessarily lead to changes in behavior. Patient education materials are not always at an appropriate literacy level.(e.g.
Respiratory Program materials are at a grade 9 to 10 level). Not everyone has a family physician. Not everyone sees their family physician when they have one. Limited access to diagnostics, and limited awareness of options available to facilitate
diagnosis. (Ultrasound: 2 yrs for a Carotid bruit, but 2 months if accessed through Stroke Prevention Clinic)
Lack of public and provider awareness as to how to access services within the Region.
Limited or varied services available rurally. The services are not necessarily available in our rural communities, or within the zones in the urban center where the need is the greatest.
We have waitlists for services greater than 4 weeks, in some areas reaching as high as 5 years. This decreases the momentum for change once diagnosis is made.
CD programs and services report under a number of different portfolios within the RQHR, with different leaders, differing goals and differing priorities.
Some RQHR CD programs with common patients operate in isolation from one another.
CD managers perceive a lack of resources to effectively meet the needs of the CD population.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 77
Many programs are operating at their maximum capacity and still have backlogs and wait-lists.
Many programs have not yet had the opportunity or support to perform efficiency assessments.
Many physicians don’t understand how patients are triaged for program access. Reportedly many patients are not attending programming when referred. (Location
access, wait lists, welcome received) Stories are relayed about individuals falling through the cracks of the delivery system. Mental Health and Addictions programs, out of necessity use strict inclusion and
exclusion criteria to assist with the management of the volume of service required. (Lack of access for patients with mild to moderate problems from Mental Health Services. Staff in the CDM programs don’t feel they have the skills and resources to help their patients with mild to moderate depression.)
Reportedly Mental Health in Saskatchewan is the most under-funded nationally. Class 3 Chronic Renal Insufficiency individuals are not being consistently screened. . Lack of long term sustainable funding for the COPD Rehabilitation Program and CHF
programming, and to a lesser degree the Sleep Disorders Clinic. Several programs are provided as add-ons to present service delivery, there is no
direct funding for services offered. There is not one point of entry for patients, this is especially problematic for those
having co-morbidities, and for integration of services. Inconsistent acknowledgement/recognition of partners who have provided funding
for services that would otherwise not be available. Opportunities:
The RQHR Chronic Disease Management Collaborative Facilitator has expertise in program efficiency improvement/ clinical practice redesign. This position could be a potential resource for programs who are interested in improving patient access.
The RQHR project currently underway to review the location of Ambulatory Care Services and make recommendations for relocation outside of the acute care facilities may provide a potential opportunity to co-locate certain CD services.
Some CD service areas are looking into potential partnering for service provision to needed service areas. Potential partnering by programs for mobile clinics, or satellite operations may be possible.
There is the opportunity to share resources. THREATS
Lack of ongoing, sustainable funding for programs such as COPD Rehabilitation Programming, and CHF Clinic, and the further impact this can have on Ambulatory Care Sensitive Condition Outcomes.
8.6 DECISION SUPPORT Strengths:
Some service delivery areas have some very strong advocates as Physician Support, which help support the patient as well as the program. (ie: Dr. Murthy for the CHF Clinic)
Some care providers have enhanced skills and or increased interest to assist patients to make informed decisions about their CD management.
Early access to information inclusive of literature or Specialists through self referral to education programs and early access to Specialty Clinics. (such as CHF or Stroke clinics)

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 78
Gaps: The current remuneration model for Specialists seems to lack incentives for them to
provide effective and efficient decision supports to primary care providers or for sharing care. Reportedly it appears that remuneration is available, but it is not consistently used.
Information not easily available regarding clinic access, or programs available within the region.
Opportunities:
There are ongoing discussions with the SMA and the Ministry of Health regarding
remuneration options for CD management. Changes have been made within the past year in regard to funding for some Chronic Diseases for our Primary Care Physicians. Future discussions may help to narrow the gap.
8.7 CLINICAL INFORMATION SYSTEMS Strengths:
The majority of RQHR CDPM programs and services have access to computers. The Region is actively involved in a provincial electronic medical record procurement
project in Primary Health Care.
Gaps: An electronic medical record will not be available through the provincial process for 3
to 5 years There is not consistent, reliable or complete information available on incidence and
prevalence of chronic conditions either by volume or geography. The type of information that is being collected and how it is collected is inconsistent
across the service delivery areas. The number of people with co-morbid conditions is unknown. All areas do not have access to information that they need for optimum client
service. (PIP(Pharmacy Information Program) / Lab Viewer)
Opportunities: Development work regarding information systems is going on provincially. The RQHR is actively involved in the development work. There are some potential options available to improve the current information systems
through the RQHR IT Department.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 79
APPENDIX 9: Population and Public Health Services (The determinants of health- Canadian Community Health Surveys 2003, 2005, 2007) A review was undertaken with the help of the RQHR Epidemiologist through Population and Public Health, where a comparison of the outcome results from Statistics Canada’s Indicator Profiles from the Canadian Community Health Survey from 2003, 2005 and 2007. In this review perception of having very good to excellent health in the RQHR is lower than the National and Saskatchewan averages, the RQHR score has dropped since 2003 and 2005. This was also consistent for our perceived mental health.
(Figure 9.1. Source : Statistics Canada (Figure 9.2. Source: Statistics Canada) (Catalogue No. 82.221-XWE2008001 ISSN 1496-3922) RQHR’s population when asked their perception of their life stress for those 15 years of age and older as being quite a lot, is the lowest it has been since 2003, and it is lower than National and Saskatchewan provincial averages in 2007.
(Figure 9.3. Source: Statistics Canada)
Perceived health, very good or excellent
58.460.1 59.659.2
58.1
56.2
61.5 61.8
53.0
48
50
52
54
56
58
60
62
64
Perc
enta
ge o
f res
pond
ents
CAN 58.4 60.1 59.6SK 59.2 58.1 56.2RQHR 61.5 61.8 53.0
2003 2005 2007
Perceived mental health (good or excellent)
71.672.9 72.7
71.3 70.7 70.7
76.5
74.4
69.1
64
66
68
70
72
74
76
78
Perc
enta
ge o
f res
pond
ents
CAN 71.6 72.9 72.7SK 71.3 70.7 70.7RQHR 76.5 74.4 69.1
2003 2005 2007
Life Stress (Quite a lot, 15 years and older)
24 22.8 22.420.2 20.8
18.6
23.9 22.9
16.6
0
5
10
15
20
25
30
Perc
enta
ge o
f Res
pond
ents
CAN 24 22.8 22.4SK 20.2 20.8 18.6RQHR 23.9 22.9 16.6
2003 2005 2007

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 80
Despite this, we have higher rates of blood pressure than the National average, but less than the present provincial average for 2007, but RQHR has increased since 2003 and 2005.
(Figure 9.4 Source: Statistics Canada) As a health region the RQHR has a higher reported rate of obesity than the National or Saskatchewan provincial reported average. The population of RQHR no longer considers themselves overweight, they are now in the obese range. This has increased since 2003 and 2005.
(Figure 9.5. Source: Statistics Canada) (Figure 9.6. Source: Statistics Canada) The RQHR population drinks more than five drinks in one occasion at least once a month in the year previous. RQHR is higher than the National and Sask. Provincial averages and is higher than it has been since 2003 (Figure 9.7). The Activity levels during leisure time rated as being active or moderately active is less than the National average and only slightly more than the Saskatchewan provincial average. All areas have markedly reduced since 2003 and 2005 (Figure 9.8).
High Blood Pressure
14.4 14.915.915 15.9
17.215.6
14.216.4
02468
101214161820
Perc
enta
ge o
f Res
pond
ents
CAN 14.4 14.9 15.9SK 15 15.9 17.2RQHR 15.6 14.2 16.4
2003 2005 2007
Body Mass Index, self-reported, adult (18 years and over) overweight
33.3 33.4 32.435.3 35.6
32.536.7 36.7
29.4
05
10152025303540
Perc
enta
ge o
f res
pond
ents
CAN 33.3 33.4 32.4SK 35.3 35.6 32.5RQHR 36.7 36.7 29.4
2003 2005 2007
Body Mass Index, self-reported, adult (18 years and over), obese
14.9 15.5 16
19.7 20.6 20.8
17.1 17.1
22.8
0
5
10
15
20
25
Perc
enta
ge o
f res
pond
ents
CAN 14.9 15.5 16SK 19.7 20.6 20.8RQHR 17.1 17.1 22.8
2003 2005 2007

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 81
(Figure 9.7. Source: Statistics Canada) (Figure 9.8. Source: Statistics Canada) RQHR is slightly less than the Saskatchewan provincial average for daily or occasional smokers, both are higher than the National average, and the rate has increased since 2003 and 2005.
(Figure 9.9. Source: Statistics Canada) The RQHR has also seen over two times the increase in the number diagnosed with Diabetes. The numbers continue to increase since 2003, and are much higher than the National average (Figure 9.10).
Five or more drinks on one occasion, at least once a month in the past year
20.7 21.8 21.822.624.9 24.2
22.224
27.6
0
5
10
15
20
25
30
Perc
enta
ge o
f res
pond
ents
CAN 20.7 21.8 21.8SK 22.6 24.9 24.2RQHR 22.2 24 27.6
2003 2005 2007
Participation and activity level (sometimes or often)
31.2 29.6 31.231.2 32.835.3
30.733.8
35.8
0
5
10
15
20
25
30
35
40
Perc
enta
ge o
f Res
pond
ents
CAN 31.2 29.6 31.2SK 31.2 32.8 35.3RQHR 30.7 33.8 35.8
2003 2005 2007
Current smoker, daily or occasional
22.9
21.7 21.9
23.8 23.8
25.9
24.2
21.6
25.5
19
20
21
22
23
24
25
26
27
Perc
enta
ge o
f res
pond
ents
CAN 22.9 21.7 21.9SK 23.8 23.8 25.9RQHR 24.2 21.6 25.5
2003 2005 2007

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 82
( Figure 9.10. Source: Statistics Canada) In general we as a health region appear to be loosing ground in the determinants of health. The collection of this information, and the sharing of it does occur, but the timeliness of it is a factor, as the information is usually two years old before it is generally released.
Diabetes Management
4.6 4.95.8
4.75.1
5.7
3.3
5.3
7.2
0
1
2
3
4
5
6
7
8
Perc
enta
ge o
f rep
onde
nts
CAN 4.6 4.9 5.8SK 4.7 5.1 5.7RQHR 3.3 5.3 7.2
2003 2005 2007

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 83
APPENDIX 10: RQHR CHRONIC DISEASE MANAGEMENT PROGRAMMING & PATIENT OUTCOME MEASUREMENT TOOLS PRESENTLY USED OR PLANNED TO
BE USED. September, 2008
(NOTE: Areas in italics are planned) RESPIRATORY PROGRAMMING: PEDIATRIC ASTHMA EDUCATION PROGRAM PATIENT CLINIC OUTCOME MEASURES TARGETSAn “Action Plan” is established, but there are no outcome measurement tools presently used for this program. (It could be that the establishment of an Action Plan is an outcome to be evaluated).
PROGRAM OUTCOME MEASURES TARGETS
ADULT ASTHMA EDUCATION PROGRAM PATIENT CLINIC OUTCOME MEASURES TARGETSClient Peak Flow Tests St. George’s Questionnaire
PROGRAM OUTCOME MEASURES TARGETS
COPD REHABILITATION EXERCISE & EDUCATION PROGRAM PATIENT CLINIC OUTCOME MEASURES TARGETS 6 Minute Walk Test pre and post 12 week program St. George’s Questionnaire
% change % change
PROGRAM OUTCOME MEASURES TARGETS Client Questionnaires: Pre program, at 6 wks and post program Group percentage change
% change (Presently 26% improvement overall.
HOME OXYGEN ASSESSMENT AND TESTING PROGRAM PATIENT CLINIC OUTCOME MEASURES TARGETS(No specific patient assessment tools used) PROGRAM OUTCOME MEASURES TARGETS

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 84
SLEEP DISORDERS CLINIC PATIENT CLINIC OUTCOME MEASURES TARGETS Patient treatment compliance Plan to do Quality of Life Surveys.
% of compliance
PROGRAM OUTCOME MEASURES TARGETS Lab: Plan to do patient satisfaction surveys. Clinic: Client Satisfaction Surveys
VENTILATOR PROGRAMS PATIENT CLINIC OUTCOME MEASURES TARGETSPlanned client quality of life questionnaires for long term home ventilation programs.
PROGRAM OUTCOME MEASURES TARGETSPlan to do client satisfaction survey
CARDIO-SCIENCE: CONGESTIVE HEART FAILURE CLINIC PATIENT CLINIC OUTCOME MEASURES TARGETS Blood Pressure Quality of Life Indicators Weight measurement daily (Follow-up by telephone daily with Clinic Coordinator)
Less than 140/90
PROGRAM OUTCOME MEASURES TARGETS Hospital Admissions Length of Stay Number of people referred to Cardiac Rehab Number of people referred for Diabetic Education
LIPID CLINIC PATIENT CLINIC OUTCOME MEASURES TARGETS Weight/ BMI Lipid Values/Ratios Blood Pressure Medication tracked by Pharmacist and Dietitian
Less than 140/90
PROGRAM OUTCOME MEASURES TARGETS

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 85
CARDIAC REHABILITATION EDUCATION PROGRAM PATIENT CLINIC OUTCOME MEASURES TARGETS Client baseline information questionnaire (In the process of developing clinical outcomes to evaluate the program.)
PROGRAM OUTCOME MEASURES TARGETS Client Satisfaction Questionnaire.
CARDIAC REHABILITATION EXERCISE PROGRAM PATIENT CLINIC OUTCOME MEASURES TARGETSBlood pressure: taken 4 times initially, then once per week. ECG monitoring: strip completed on admissions Cardiac Rehab Evaluation: 6 min walk test and Grip Strength. (3 walk tests are completed, with reassessment at 6 and 12 wks.) SF-36 Determinants of Health Duke Activity Status completed again at 6 and 12 wks. Risk Stratification Tool Heart Rate Lab Work Access (a problem)
PROGRAM OUTCOME MEASURES TARGETSClient Satisfaction.
RQHR STROKE PREVENTION CLINIC (Formerly South Saskatchewan Stroke Prevention Clinic) PATIENT CLINIC OUTCOME MEASURES TARGETS(No specific validated patient assessment tools used) Only 1-2 visits- unable to measure change over time.
PROGRAM OUTCOME MEASURES TARGETSStroke Research: Episodic research to evaluate program ie. Wait times, medication usage etc. Benchmarked against Canadian Best Practice Recommendations for Stroke Care (updated 2008).

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 86
DIABETES: DIABETES PROGRAMMING: MEDEC (Presently unable to track any patient performance measures. They are awaiting the implementation of the CDM-Toolkit, where they expect to be able to evaluate the following)DEP has an ACCESS database which contains key indicators for all patients but they have some challenges re: ability to run reports and do enquiries. PATIENT CLINIC OUTCOME MEASURES TARGETS Patient’s A1C levels. When their A1C was measured. At least one LDL test result Blood Pressure< 130/80 On an ASA/ ACE or ARB or a Statin Date of Last Eye Screen and know when next one is due Date of Last Foot Screen and know when next one is due.
PROGRAM OUTCOME MEASURES TARGETS Some volume data for each of the three diabetes education programs is tracked.(Each program keeps its own stats using similar definitions but different methods. Statistics are kept based on fiscal year. Each program is to submit volume stats to the Regional Diabetes Sub Committee, but there have been challenges with that. The number of new patients (admissions) and the number of follow up visits is collected. At present MEDEC cannot determine the number of people actively following with the program. The other two programs are able to do this. The number of clients on wait lists are monitored at month end, wait time is tricky as MEDEC triages so wait time depends on priority rating assigned to the referral. (At present there is no good way to track wait times other than manual chart audits). Ambulatory Care Sensitive Condition admission rates. Rates of hospitalized or ER visits for hypo and hyper glycemia. Rates of Lower Extremity Amputations (LEA) for people with diabetes > 20 yrs of age. Data from Ministry of Health on incidence and prevalence rates of diabetes, and prevalence of some co-morbidities are periodically reported to the regions. In future, with access to a suitable information system, the Diabetes Sub Committee hopes that we can track the following: Mean A1C levels for patient groups Number(or percentage) of people with A1C level measured in past 6 months. Number ( or percentage) of people with BP level<140/90 Number (or percentage) of people who currently smoke Number (or percentage) of people with diabetes with at least 1 LDL
75% pts with A1C <7 75% of pts BP<130/80

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 87
level done. Number ( or percentage) of people with diabetes on ASA/ ACE or ARB or on a Statin Number of people with diabetes who have had an eye exam in past year. Number of people with diabetes who have had a foot exam in past year. Number of people seen for patient education. The percentage of people with diabetes in the region being seen at the diabetes programs.
75% of pts TC/HDL <4
RETINOPATHY- EYE SCREENING PATIENT CLINIC OUTCOME MEASURES TARGETS (An evaluation is done including medical history and medications, duration and type of diabetes, age, date of last exam) Incidence of Pathology Recommended Referral
PROGRAM OUTCOME MEASURES TARGETSVolumes seen Priority Indicators:
• Percentage of pathology found related to age of patient. • Ratio of those receiving photos without drops. (Used to identify
need for clinical specialist to order the drops).
CHRONIC RENAL INSUFFICIENCY: CHRONIC RENAL INSUFFICIENCY PROGRAMMING PATIENT CLINIC OUTCOME MEASURES TARGETSBlood Pressure Lab work results
PROGRAM OUTCOME MEASURES TARGETSVolumes of clients seen are the only measures used for program outcomes at present

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 88
HOME CARE: HOME CARE PROGRAMMING: HYPERTENSION COMMUNITY CLINICAL PATHWAY PATIENT CLINIC OUTCOME MEASURES
TARGETS
Blood Pressure * Unless otherwise stated by Physician: Non diabetic< 140/90, Diabetic < 130/80
PROGRAM OUTCOME MEASURES TARGETS
DEPRESSION CARE: DEPRESSION CARE (MENTAL HEALTH & ADDICTIONS PROGRAMMING) PATIENT CLINIC OUTCOME MEASURES TARGETS ASIST Program used to determine Therapeutic Alliance and Session Outcome Measurements for individual Adult Therapy services (Mental Health Clinic).
- Reduced symptoms per client report. - Client satisfaction with therapeutic alliance
PROGRAM OUTCOME MEASURES TARGETS
OBESITY MANAGEMENT: OBESITY MANAGEMENT PATIENT CLINIC OUTCOME MEASURES TARGETS Patient’s weight/ height: BMI Waist Girth Measurement
Adults: >18.5 & <24.9 BMI ** Adults 65+>18.5 & <25.0-29.9 Children: BMI Growth Charts Men< 40 inches (102 cms) Women< 35 inches (88cms)** Not for pregnant females.
PROGRAM OUTCOME MEASURES TARGETS (Not applicable as no formal program)
Resource: http://www.capitalhealth.ca?Especiallyfor/WeightWise/Body_Mass_Index_and_Waist_Cir.. Updates: Respiratory Care Programming: Sheryl O’Quinn: October 1, 2008

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 89
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
Appendix 11 Assessment of Chronic Illness Care Version 3.5
Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the ICIC/IHI team. We would like to get your phone number and e-mail address in the event that we need to contact you/your team in the future. Please also indicate the names of persons (e.g., team members) who complete the survey with you. Later on in the survey, you will be asked to describe the process by which you complete the survey. Your name:
Date: ________/________/________ Month Day Year Names of other persons completing the survey with you: 1. 2.
Organization & Address:
3.
Your phone number: (______) __ __ __ - __ __ __ __ Your e-mail address:
Directions for Completing the Survey
This survey is designed to help systems and provider practices move toward the “state-of-the-art” in managing chronic illness. The results can be used to help your team identify areas for improvement. Instructions are as follows: 1. Answer each question from the perspective of one physical site (e.g., a practice, clinic, hospital, health plan) that
supports care for chronic illness.
Please provide name and type of site (e.g., Group Health Cooperative/Plan) ________________________________
2. Answer each question regarding how your organization is doing with respect to one disease or condition.
Please specify condition ________________________________ 3. For each row, circle the point value that best describes the level of care that currently exists in the site and
condition you chose. The rows in this form present key aspects of chronic illness care. Each aspect is divided into levels showing various stages in improving chronic illness care. The stages are represented by points that range from 0 to 11. The higher point values indicate that the actions described in that box are more fully implemented.
4. Sum the points in each section (e.g., total part 1 score), calculate the average score (e.g., total part 1 score / # of
questions), and enter these scores in the space provided at the end of each section. Then sum all of the section scores and complete the average score for the program as a whole by dividing this by 6.
For more information about how to complete the survey, please contact: Judith Schaefer, MPH tel. 206.287.2077; [email protected] Improving Chronic Illness Care A National Program of the Robert Wood Johnson Foundation Group Health Cooperative of Puget Sound 1730 Minor Avenue, Suite 1290 Seattle, WA 98101-1448

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 90
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
Assessment of Chronic Illness Care, Version 3.5
Part 1: Organization of the Healthcare Delivery System. Chronic illness management programs can be more effective if the overall system (organization) in which care is provided is oriented and led in a manner that allows for a focus on chronic illness care.
Components Level D Level C Level B Level A Overall Organizational Leadership in Chronic Illness Care
Score
…does not exist or there is a little interest. 0 1 2
…is reflected in vision statements and business plans, but no resources are specifically earmarked to execute the work. 3 4 5
…is reflected by senior leadership and specific dedicated resources (dollars and personnel). 6 7 8
…is part of the system’s long term planning strategy, receive necessary resources, and specific people are held accountable. 9 10 11
Organizational Goals for Chronic Care
Score
…do not exist or are limited to one condition. 0 1 2
…exist but are not actively reviewed. 3 4 5
…are measurable and reviewed. 6 7 8
…are measurable, reviewed routinely, and are incorporated into plans for improvement. 9 10 11
Improvement Strategy for Chronic Illness Care
Score
…is ad hoc and not organized or supported consistently. 0 1 2
…utilizes ad hoc approaches for targeted problems as they emerge. 3 4 5
…utilizes a proven improvement strategy for targeted problems. 6 7 8
…includes a proven improvement strategy and uses it proactively in meeting organizational goals. 9 10 11
Incentives and Regulations for Chronic Illness Care
Score
…are not used to influence clinical performance goals. 0 1 2
…are used to influence utilization and costs of chronic illness care. 3 4 5
…are used to support patient care goals. 6 7 8
…are used to motivate and empower providers to support patient care goals. 9 10 11
Senior Leaders
Score
…discourage enrollment of the chronically ill. 0 1 2
…do not make improvements to chronic illness care a priority. 3 4 5
…encourage improvement efforts in chronic care. 6 7 8
…visibly participate in improvement efforts in chronic care. 9 10 11
Benefits
Score
…discourage patient self-management or system changes. 0 1 2
…neither encourage nor discourage patient self-management or system changes. 3 4 5
…encourage patient self-management or system changes. 6 7 8
…are specifically designed to promote better chronic illness care. 9 10 11
Total Health Care Organization Score ________ Average Score (Health Care Org. Score / 6) _________

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 91
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
Part 2: Community Linkages. Linkages between the health delivery system (or provider practice) and community resources play important roles in the management of chronic illness.
Components Level D Level C Level B Level A Linking Patients to Outside Resources
Score
…is not done systematically. 0 1 2
…is limited to a list of identified community resources in an accessible format. 3 4 5
…is accomplished through a designated staff person or resource responsible for ensuring providers and patients make maximum use of community resources. 6 7 8
… is accomplished through active coordination between the health system, community service agencies and patients. 9 10 11
Partnerships with Community Organization
Score
…do not exist. 0 1 2
…are being considered but have not yet been implemented. 3 4 5
…are formed to develop supportive programs and policies. 6 7 8
…are actively sought to develop formal supportive programs and policies across the entire system. 9 10 11
Regional Health Plans
Score
…do not coordinate chronic illness guidelines, measures or care resources at the practice level. 0 1 2
…would consider some degree of coordination of guidelines, measures or care resources at the practice level but have not yet implemented changes. 3 4 5
…currently coordinate guidelines, measures or care resources in one or two chronic illness areas. 6 7 8
…currently coordinate chronic illness guidelines, measures and resources at the practice level for most chronic illnesses. 9 10 11
Total Community Linkages Score ___________ Average Score (Community Linkages Score / 3) _________

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 92
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
Part 3: Practice Level. Several components that manifest themselves at the level of the individual provider practice (e.g. individual clinic) have been shown to improve chronic illness care. These characteristics fall into general areas of self-management support, delivery system design issues that directly affect the practice, decision support, and clinical information systems. ------------------------------------------------------------------------------------------------------------------------------------------------------------- Part 3a: Self-Management Support. Effective self-management support can help patients and families cope with the challenges of living with and treating chronic illness and reduce complications and symptoms.
Components Level D Level C Level B Level A Assessment and Documentation of Self-Management Needs and Activities
Score
…are not done. 0 1 2
…are expected. 3 4 5
…are completed in a standardized manner. 6 7 8
…are regularly assessed and recorded in standardized form linked to a treatment plan available to practice and patients. 9 10 11
Self-Management Support
Score
…is limited to the distribution of information (pamphlets, booklets). 0 1 2
…is available by referral to self-management classes or educators. 3 4 5
…is provided by trained clinical educators who are designated to do self-management support, affiliated with each practice, and see patients on referral. 6 7 8
…is provided by clinical educators affiliated with each practice, trained in patient empowerment and problem-solving methodologies, and see most patients with chronic illness. 9 10 11
Addressing Concerns of Patients and Families
Score
…is not consistently done. 0 1 2
…is provided for specific patients and families through referral. 3 4 5
…is encouraged, and peer support, groups, and mentoring programs are available. 6 7 8
…is an integral part of care and includes systematic assessment and routine involvement in peer support, groups or mentoring programs. 9 10 11
Effective Behavior Change Interventions and Peer Support
Score
…are not available. 0 1 2
…are limited to the distribution of pamphlets, booklets or other written information. 3 4 5
…are available only by referral to specialized centers staffed by trained personnel. 6 7 8
…are readily available and an integral part of routine care. 9 10 11
Total Self-Management Score_______ Average Score (Self Management Score / 4) _______

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 93
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
Part 3b: Decision Support. Effective chronic illness management programs assure that providers have access to evidence-based information necessary to care for patients--decision support. This includes evidence-based practice guidelines or protocols, specialty consultation, provider education, and activating patients to make provider teams aware of effective therapies.
Components Level D Level C Level B Level A Evidence-Based Guidelines
Score
…are not available. 0 1 2
…are available but are not integrated into care delivery. 3 4 5
…are available and supported by provider education. 6 7 8
…are available, supported by provider education and integrated into care through reminders and other proven provider behavior change methods. 9 10 11
Involvement of Specialists in Improving Primary Care
Score
…is primarily through traditional referral. 0 1 2
…is achieved through specialist leadership to enhance the capacity of the overall system to routinely implement guidelines. 3 4 5
…includes specialist leadership and designated specialists who provide primary care team training. 6 7 8
…includes specialist leadership and specialist involvement in improving the care of primary care patients. 9 10 11
Provider Education for Chronic Illness Care
Score
…is provided sporadically. 0 1 2
…is provided systematically through traditional methods. 3 4 5
…is provided using optimal methods (e.g. academic detailing). 6 7 8
…includes training all practice teams in chronic illness care methods such as population-based management, and self-management support. 9 10 11
Informing Patients about Guidelines
Score
…is not done. 0 1 2
…happens on request or through system publications. 3 4 5
…is done through specific patient education materials for each guideline. 6 7 8
…includes specific materials developed for patients which describe their role in achieving guideline adherence. 9 10 11
Total Decision Support Score_______ Average Score (Decision Support Score / 4) _______

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 94
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
Part 3c: Delivery System Design. Evidence suggests that effective chronic illness management involves more than simply adding additional interventions to a current system focused on acute care. It may necessitate changes to the organization of practice that impact provision of care. Components Level D Level C Level B Level A Practice Team Functioning
Score
…is not addressed. 0 1 2
…is addressed by assuring the availability of individuals with appropriate training in key elements of chronic illness care. 3 4 5
…is assured by regular team meetings to address guidelines, roles and accountability, and problems in chronic illness care. 6 7 8
…is assured by teams who meet regularly and have clearly defined roles including patient self-management education, proactive follow-up, and resource coordination and other skills in chronic illness care. 9 10 11
Practice Team Leadership
Score
…is not recognized locally or by the system. 0 1 2
…is assumed by the organization to reside in specific organizational roles. 3 4 5
…is assured by the appointment of a team leader but the role in chronic illness is not defined. 6 7 8
…is guaranteed by the appointment of a team leader who assures that roles and responsibilities for chronic illness care are clearly defined. 9 10 11
Appointment System
Score
…can be used to schedule acute care visits, follow-up and preventive visits. 0 1 2
…assures scheduled follow-up with chronically ill patients. 3 4 5
…are flexible and can accommodate innovations such as customized visit length or group visits. 6 7 8
…includes organization of care that facilitates the patient seeing multiple providers in a single visit. 9 10 11
Follow-up
Score
…is scheduled by patients or providers in an ad hoc fashion. 0 1 2
…is scheduled by the practice in accordance with guidelines. 3 4 5
…is assured by the practice team by monitoring patient utilization. 6 7 8
…is customized to patient needs, varies in intensity and methodology (phone, in person, email) and assures guideline follow-up. 9 10 11
Planned Visits for Chronic Illness Care
Score
…are not used. 0 1 2
…are occasionally used for complicated patients. 3 4 5
…are an option for interested patients. 6 7 8
…are used for all patients and include regular assessment, preventive interventions and attention to self-management support. 9 10 11
Continuity of Care
Score
…is not a priority. 0 1 2
…depends on written communication between primary care providers and specialists, case managers or disease management companies. 3 4 5
…between primary care providers and specialists and other relevant providers is a priority but not implemented systematically. 6 7 8
…is a high priority and all chronic disease interventions include active coordination between primary care, specialists and other relevant groups. 9 10 11

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 95
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
(From Previous Page) Total Delivery System Design Score_______ Average Score (Delivery System Design Score / 6) _______ Part 3d: Clinical Information Systems. Timely, useful information about individual patients and populations of patients with chronic conditions is a critical feature of effective programs, especially those that employ population-based approaches.7, 8
Components Level D Level C Level B Level A Registry (list of patients with specific conditions)
Score
…is not available. 0 1 2
…includes name, diagnosis, contact information and date of last contact either on paper or in a computer database. 3 4 5
…allows queries to sort sub-populations by clinical priorities. 6 7 8
…is tied to guidelines which provide prompts and reminders about needed services. 9 10 11
Reminders to Providers
Score
…are not available. 0 1 2
… include general notification of the existence of a chronic illness, but does not describe needed services at time of encounter. 3 4 5
…includes indications of needed service for populations of patients through periodic reporting. 6 7 8
…includes specific information for the team about guideline adherence at the time of individual patient encounters. 9 10 11
Feedback
Score
…is not available or is non-specific to the team. 0 1 2
…is provided at infrequent intervals and is delivered impersonally. 3 4 5
…occurs at frequent enough intervals to monitor performance and is specific to the team’s population. 6 7 8
…is timely, specific to the team, routine and personally delivered by a respected opinion leader to improve team performance. 9 10 11
Information about Relevant Subgroups of Patients Needing Services
Score
…is not available. 0 1 2
…can only be obtained with special efforts or additional programming. 3 4 5
…can be obtained upon request but is not routinely available. 6 7 8
…is provided routinely to providers to help them deliver planned care. 9 10 11
Patient Treatment Plans
Score
…are not expected. 0 1 2
…are achieved through a standardized approach. 3 4 5
…are established collaboratively and include self management as well as clinical goals. 6 7 8
…are established collaborative an include self management as well as clinical management. Follow-up occurs and guides care at every point of service. 9 10 11
Total Clinical Information System Score_______ Average Score (Clinical Information System Score / 5) ________

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 96
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
Integration of Chronic Care Model Components. Effective systems of care integrate and combine all elements of the Chronic Care Model; e.g., linking patients’ self-management goals to information systems/registries. Components Little support Basic support Good support Full support Informing Patients about Guidelines
Score
…is not done. 0 1 2
…happens on request or through system publications. 3 4 5
…is done through specific patient education materials for each guideline. 6 7 8
…includes specific materials developed for patients which describe their role in achieving guideline adherence. 9 10 11
Information Systems/Registries
Score
…do not include patient self-management goals. 0 1 2
…include results of patient assessments (e.g., functional status rating; readiness to engage in self-management activities), but no goals. 3 4 5
…include results of patient assessments, as well as self-management goals that are developed using input from the practice team/provider and patient. 6 7 8
…include results of patient assessments, as well as self-management goals that are developed using input from the practice team and patient; and prompt reminders to the patient and/or provider about follow-up and periodic re-evaluation of goals. 9 10 11
Community Programs
Score
…do not provide feedback to the health care system/clinic about patients’ progress in their programs. 0 1 2
…provide sporadic feedback at joint meetings between the community and health care system about patients’ progress in their programs. 3 4 5
…provide regular feedback to the health care system/clinic using formal mechanisms (e.g., Internet progress report) about patients’ progress. 6 7 8
…provide regular feedback to the health care system about patients’ progress that requires input from patients that is then used to modify programs to better meet the needs of patients. 9 10 11
Organizational Planning for Chronic Illness Care
Score
…does not involve a population-based approach. 0 1 2
…uses data from information systems to plan care. 3 4 5
…uses data from information systems to proactively plan population-based care, including the development of self-management programs and partnerships with community resources. 6 7 8
…uses systematic data and input from practice teams to proactively plan population-based care, including the development of self-management programs and community partnerships, that include a built-in evaluation plan to determine success over time. 9 10 11

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 97
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
Components Little support Basic support Good support Full support Routine follow-up for appointments, patient assessments and goal planning
…is not ensured. 0 1 2
is sporadically done, usually for appointments only. 3 4 5
is ensured by assigning responsibilities to specific staff (e.g., nurse case manager). 6 7 8
is ensured by assigning responsibilities to specific staff (e.g., nurse case manager) who uses the registry and other prompts to coordinate with patients and the entire practice team. 9 10 11
Guidelines for chronic illness care
…are not shared with patients. 0 1 2
…are given to patients who express a specific interest in self-management of their condition. 3 4 5
…are provided for all patients to help them develop effective self-management or behavior modification programs, and identify when they should see a provider. 6 7 8
…are reviewed by the practice team with the patient to devise a self-management or behavior modification program consistent with the guidelines that takes into account patient’s goals and readiness to change. 9 10 11
Total Integration Score (SUM items): __________ Average Score (Integration Score/6) = __________

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 98
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
Briefly describe the process you used to fill out the form (e.g., reached consensus in a face-to-face meeting; filled out by the team leader in consultation with other team members as needed; each team member filled out a separate form and the responses were averaged). Description:
Scoring Summary (bring forward scoring at end of each section to this page)
Total Org. of Health Care System Score _______ Total Community Linkages Score _______ Total Self-Management Score _______ Total Decision Support Score _______ Total Delivery System Design Score _______ Total Clinical Information System Score _______ Total Integration Score _______ Overall Total Program Score (Sum of all scores) _______ Average Program Score (Total Program /7) _______

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 99
Copyright 2000 MacColl Institute for Healthcare Innovation, Group Health Cooperative
What does it mean? The ACIC is organized such that the highest “score” (an “11”) on any individual item, subscale, or the overall score (an average of the six ACIC subscale scores) indicates optimal support for chronic illness. The lowest possible score on any given item or subscale is a “0”, which corresponds to limited support for chronic illness care. The interpretation guidelines are as follows: Between “0” and “2” = limited support for chronic illness care Between “3” and “5” = basic support for chronic illness care Between “6” and “8” = reasonably good support for chronic illness care Between “9” and “11” = fully developed chronic illness care It is fairly typical for teams to begin a collaborative with average scores below “5” on some (or all) areas the ACIC. After all, if everyone was providing optimal care for chronic illness, there would be no need for a chronic illness collaborative or other quality improvement programs. It is also common for teams to initially believe they are providing better care for chronic illness than they actually are. As you progress in the Collaborative, you will become more familiar with what an effective system of care involves. You may even notice your ACIC scores “declining” even though you have made improvements; this is most likely the result of your better understanding of what a good system of care looks like. Over time, as your understanding of good care increases and you continue to implement effective practice changes, you should see overall improvement on your ACIC scores.

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 100
© Copyright 2004 MacColl Institute for Healthcare Innovation, Group Health Cooperative
APPENDIX 12
Assessment of Care for Chronic Conditions
None of
the time A Little of the Time
Some of the Time
Most of the Time Always
1. Asked for my ideas when we made a treatment plan.
1
2
3
4
5
2. Given choices about treatment to think about.
1
2
3
4
5
3. Asked to talk about any problems with my medications or their effects.
1
2
3
4
5
4. Given a written list of things I should do to improve my health.
1
2
3
4
5
5. Satisfied that my care was well organized.
1
2
3
4
5
6. Shown how what I did to take care of myself influenced my condition.
1
2
3
4
5
7. Asked to talk about my goals in caring for my condition.
1
2
3
4
5
8. Helped to set specific goals to improve my eating or exercise.
1
2
3
4
5
9. Given a copy of my treatment plan.
1
2
3
4
5
10. Encouraged to go to a specific group or class to help me cope with my chronic condition.
1
2
3
4
5
11. Asked questions, either directly or on a survey, about my health habits.
1
2
3
4
5
Staying healthy can be difficult when you have a chronic condition. We would like to learn about the type of help with your condition you get from your health care team. This might include your regular doctor, his or her nurse, or physician’s assistant who treats your illness. Your answers will be kept confidential and will not be shared with your physician or clinic.
Over the past 6 months, when I received care for my chronic conditions, I was:

Healthy Living: A Chronic Disease Prevention and Management Strategy Page 101
© Copyright 2004 MacColl Institute for Healthcare Innovation, Group Health Cooperative
None of
the time A Little of the Time
Some of the Time
Most of the Time Always
12. Sure that my doctor or nurse thought about my values, beliefs, and traditions when they recommended treatments to me.
1
2
3
4
5
13. Helped to make a treatment plan that I could carry out in my daily life.
1
2
3
4
5
14. Helped to plan ahead so I could take care of my condition even in hard times.
1
2
3
4
5
15. Asked how my chronic condition affects my life.
1
2
3
4
5
16. Contacted after a visit to see how things were going.
1
2
3
4
5
17. Encouraged to attend programs in the community that could help me.
1
2
3
4
5
18. Referred to a dietitian, health educator or counselor.
1
2
3
4
5
19. Told how my visits with other types of doctors, like an eye doctor or surgeon, helped my treatment.
1
2
3
4
5
20. Asked how my visits with other doctors were going.
1
2
3
4
5
Group Health Version 8/13/03
Over the past 6 months, when I received care for my chronic conditions, I was: