Embed Size (px)
Citation preview

Healthcare Reform and the New Administration:
The First 90 Days
Leadership Training Conference
Tuesday, April 21, 2009
11:15 am -12:00 pm

2
Session Presenter
Richard L. Clarke, DHA, FHFMA
President & CEO
HFMA

3
Learning Objectives
• Identify the direction of key healthcare reform proposals in Washington
• Understand the implications of these proposals for the healthcare industry
• Identify specific reform issues that could affect your chapter’s strategic planning

4
Key Healthcare Reform Players
• Administration• Kathleen Sebelius – HHS Secretary Nominee• Nancy-Ann DeParle – Director, White House Office of Health Reform• Peter Orszag – Director, OMB
• Senate• Sen. Max Baucus – Chair, Senate Finance • Sen. Edward Kennedy – Chair, Senate Health, Education, Labor & Pensions • Sen. Chuck Grassley – Ranking Member, Senate Finance
• House• Rep. Pete Stark – Chair, Health Subcommittee, Ways & Means• Rep. Henry Waxman – Chair, Commerce & Energy

5
What Has Happened So Far?
• SCHIP Reauthorization• American Recovery and Reinvestment Act of 2009 (ARRA)
• Increased Medicaid Support• Subsidization of COBRA• Healthcare IT Funding• Comparative Effectiveness Research
• Proposed Budget for FY2010• $630 Billion Healthcare Reform “Reserve Fund”• Medicare Fee-for-Service → Bundled Payment ($26 billion over 10 years)• Pay-for Performance for Acute Inpatient Services ($12 billion over 10
years)

6
Measures Under Consideration
• Public Insurance Plan Option• Employer “Play or Pay” Requirements• Individual Coverage Mandates• Mandatory Charity Care Minimums

7
$0.0
$1.0
$2.0
$3.0
$4.0
$5.0
$6.0
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
$4.6
$1.1
$1.4
$2.1$2.5
$0.7
$0.8
$1.0
$0.0
$1.0
$2.0
$3.0
$4.0
$5.0
$6.0
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
$5.2
$1.3
$1.6
$2.3
$2.5
$0.7
$0.8
$1.0
Projected Growth, Current Policy Revenue Growth with Path Policies
Expenditure (trillions) Expenditure (trillions)
Total Nat’l Health Expenditure
Physician & other professional
HospitalAll other
The Big Picture: A Perspective onReform Costs & Savings
Estimates by The Lewin Group for The Commonwealth Fund’s Path to a High Performance U.S. Health System: A 2020 Vision and the Policies to Pave the Way, February 2009.
8
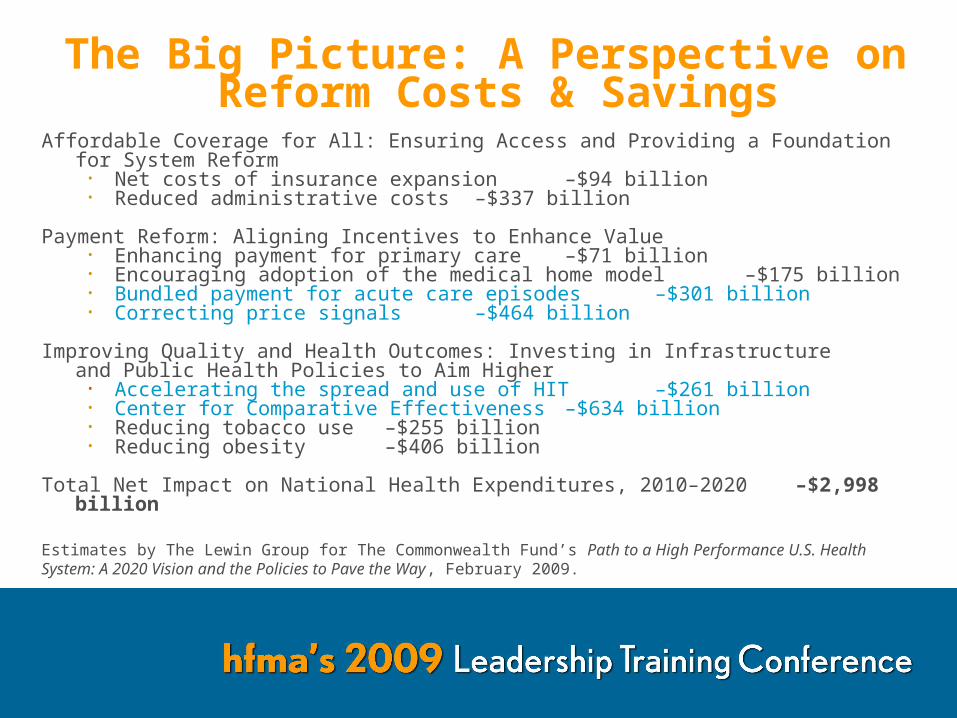
The Big Picture: A Perspective on Reform Costs & Savings
Affordable Coverage for All: Ensuring Access and Providing a Foundation for System Reform• Net costs of insurance expansion –$94 billion• Reduced administrative costs –$337 billion
Payment Reform: Aligning Incentives to Enhance Value• Enhancing payment for primary care –$71 billion• Encouraging adoption of the medical home model –$175 billion• Bundled payment for acute care episodes –$301 billion• Correcting price signals –$464 billion
Improving Quality and Health Outcomes: Investing in Infrastructureand Public Health Policies to Aim Higher
• Accelerating the spread and use of HIT –$261 billion• Center for Comparative Effectiveness –$634 billion• Reducing tobacco use –$255 billion• Reducing obesity –$406 billion
Total Net Impact on National Health Expenditures, 2010–2020 –$2,998 billion
Estimates by The Lewin Group for The Commonwealth Fund’s Path to a High Performance U.S. Health System: A 2020 Vision and the Policies to Pave the Way, February 2009.

9
The Big Picture: Another View• Conclusions of the CBO’s Analysis of Health Reform Proposals (Dec.
2008)
• Adjusting insurance market to reduce use of minimally beneficial treatments would likely require higher enrollee cost sharing or tighter management of enrollees’ care.
• Wider health IT adoption or more preventive medical care would generate either modest cost reductions or increases in healthcare spending within a 10-year budgetary time frame.
• Reducing the level or slowing the growth of healthcare spending would require substantial changes in payment incentives to providers.

10
Where Are Hospitals Today?More than half of hospitals report negative total margins.

11
Where Are Hospitals Today?Patient revenue has declined for almost half of hospitals.

12
Where Are Hospitals Today?Over 60% of hospitals report negative charity care and bad debt impacts.

13
Issues to Watch: Charity Care
• IRS Exempt Organizations Hospital Study (Feb. 2009)• Average percentage of total revenues spent on community benefit = 9%• Unevenly distributed:
9% of hospitals reported 60% of aggregate community benefit expenditures
14% of hospitals reported 63% of aggregated uncompensated care expenditures
• Senator Grassley’s response: “The Treasury Department could do a lot of good. . .by reestablishing. . .charity care requirements, and if it looks like that can’t get done, then Congress will have to step in.”

14
Issues to Watch: ARRA
0%
25%
50%
75%
100%
Year 1 Year 2 Year 3 Year 4
“Meaningful” users of HIT will receive additional payments from Medicare…
Percentage of HIT Medicare Share Payments Received Based on When Eligible
…while non-adopters will have their Medicare market basket update reduced
75%
50%
25%
0%
25%
50%
75%
100%
Percentage of Market Basket Update Received by Non-Adopters
2010 - 2013
2014 2015 2016Eligible in:
2015 2016 2017
Source: HFMA, “Analysis of the SCHIP Bill and ARRA,” www.hfma.org/library/

15
Issues to Watch: Public Health Plan
• The Cost and Coverage Impacts of a Public Plan (The Lewin Group, April 2009)
• If plan open to all individuals and employers, reimbursing at Medicare rates, hospital total margins fall $36 billion (4.6% of net revenues) in 2010.
• If plan excludes large employers, reimbursing at Medicare rates, hospital margins increase by $11.3 billion in 2010.
• Physician net incomes decline under both scenarios.

16
Impact of Public Plan
Source: Lewin Group, The Cost and Coverage Impacts of a Public Plan, April 2009

17
Where HFMA Stands: Healthcare Reform
• Accurate Reporting of Charity Care/Community Benefit• P&P Board Statement 15, cited by IRS as guide in all
representations regarding charity care• Public Disclosure of Financial and Operating Information
• P&P Board Statement 18, cited by SEC as “market practice” for healthcare industry disclosures
• Transparency of Healthcare Costs• PATIENT FRIENDLY BILLING® Project
• Payment Reform

18
Where HFMA Stands:Payment Reform
• Basic Principles of Payment Reform• Quality• Alignment• Fairness• Simplification• Societal Benefit

19
Where HFMA Stands:Payment Reform
Source: HFMA, Healthcare Payment Reform: From Principles to Action (2008)

20
Where HFMA Stands:Payment Reform – Next Steps
HFMA is identifying best practice changes that providers can use to adapt to the incentives provided by healthcare reform
• Developed a compendium of payment reform demonstration projects
• Surveying participants involved in these projects• Organization structure changes• Physician integration• Investment in financial operations• Budgeting / modeling
• Researching alternate physician alignment models

21
Where HFMA Stands
www.hfma.org/paymentreform

22





























