Embed Size (px)
Citation preview
HEALTHCARE CAPTIVES
DEALING WITH THE "NEW NORMAL" IN HEALTHCARE
William M. Cassetta
IMAC 2013Pre-Forum TutorialGrand CaymanDecember 3, 2013
2
HEALTHCARE CAPTIVES – THE NEW NORMAL
Historically, the institutional healthcare system has been designed to heal and cure patients, with a focus on services in the acute care setting.

3
HEALTHCARE CAPTIVES – THE NEW NORMAL
In the “new normal”, institutional health care will focus on “population health management”.
4
HEALTHCARE CAPTIVES – THE NEW NORMAL
Healthcare captives were formed primarily to help manage medical professional liability risk.
5
HEALTHCARE CAPTIVES – THE NEW NORMAL
In the “new normal”, captives will be challenged to help manage financial risk that extends far beyond medical professional liability.
6
HEALTHCARE CAPTIVES – THE NEW NORMAL
Don’t risk a lot to save a little. Retain risk that is controllable and predictable. Transfer risk that is volatile or unpredictable. Retain “owned” risk and transfer “non-owned” risk
Will these continue to be the precepts of alternative risk financing in the “new normal”?

7
HEALTHCARE CAPTIVES – THE NEW NORMAL
Employing physicians in large numbers
• Perfect Storm – health systems want to provide full range of services; physicians fear payment changes if they remain in private practice
• Is it really “employment”? Integration into corporate culture of parent?
Willingness to adapt to working for someone else?
Compensation models often resemble private practice
‒ So, newly “employed” physicians have demands that cannot be ignored
8
HEALTHCARE CAPTIVES – THE NEW NORMAL
Tail Coverage
• Commercial market prices tail coverage unrealistically
• Cost of tail coverage is often a critical factor in the employment negotiation
• Physicians might have potential personal benefits if they remain insured by their commercial carriers
What about providing tail coverage through our captive?
9
HEALTHCARE CAPTIVES – THE NEW NORMAL
Distinguish ability to provide tail coverage from advisability of providing tail coverage
• Limited opportunity for coordinated defense
• Was physician’s prior practice in an unfamiliar/adverse venue?
• Does the medical specialty have an especially long tail?
• Was the physician insured under a policy with a “claims asserted” trigger?
• Does the sponsoring organization wish to assume risk for practice outside the sponsor’s facilities?
• What if the physician quits/is terminated?
• Premium tax/potential income tax issues
10
HEALTHCARE CAPTIVES – THE NEW NORMAL
Potential New Best Friend – Physician Insurance Companies?
• New willingness by physician carriers to entertain collaborative arrangements with health systems
Concerns about shrinking non-employed physician market
Recognition that “preferred provider” status with predominant health system may produce greater market share
Apparent willingness to consider nearly any proposed program structure
‒ 100% risk transfer
‒ Quota shares
‒ Assumption of prior acts liability only
‒ Access to underwriting services
Reluctance due to historical animosity between hospitals and physicians’ carriers
11
HEALTHCARE CAPTIVES – THE NEW NORMAL
New Exposures/Threats• Class action claims
‒ Will current opportunity to limit retained risk be available in the future as excess carriers reconsider “batch” coverage provisions?
• Negligent credentialing claims
• New “agency” theories in clinically integrated networks and ACOs
• Claims alleging failure to provide care based on economic incentives
• Antitrust claims for excluding/terminating providers from CIN/ACO
• Privacy breaches‒ Who “owns” the electronic medical record that can be accessed by multiple unrelated
providers?
• eMedicine
• Quality Improvement fatigue
• Increasing role of non-physician providers
• Aggressive tax enforcement
• The insurance market cycle
12
HEALTHCARE CAPTIVES – THE NEW NORMAL
IT WON’T BE EASY, BUT IT WILL BE INTERESTING!

WWW.HONIGMAN.COM
Healthcare Captives –Dealing with the “New Normal” in Healthcare
Tom HermesDirector - Towers Watson
IMAC 2013Pre-Forum Tutorial
Grand CaymanDecember 3, 2013
14
Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
Uncertainty Effects Healthcare Captive Programs
Worldwide economic instability continues Real and manufacturing crises continue
Insurance cycle turning?? Could affect availability and affordability
Affordable Care Act (AKA Obama Care) Major restructuring of healthcare industry
– Potential changes to historical risks are not represented in current data– Changes generate new potential causes of loss requiring coverage – no data
towerswatson.com
© 2013 Towers Watson. All rights reserved.
15
Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
The Medical Professional Liability Cycle
Is the Medical Professional Liability (MPL) insurance cycle turning
Property, workers compensation, and commercial auto markets firming
Last MPL cycle turned positive in 2002 (12 years ago) – change is due
Tort reform erosion continues
Major healthcare restructuring creating potential new liability issues
Never events (absolute liability?)
Systematic risk (E.D. System flaws)
Government scrutiny/reporting requirements (Section III) (stents)
Increased public awareness of outcomes (higher expectations)
Some evidence that large claim severity is increasing (while frequency flat)
Increased frequency of class action/batch cases (cardiac stents)
towerswatson.com
© 2013 Towers Watson. All rights reserved.
16

Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
Hard Market Cycle Generally Requires a “Perfect Storm”
Substantial increases in frequency and/or severity of claims
Early cycles were frequency driven
Most recent cycle was large loss severity driven
Significant decline in investment return affects leverage
Cash flow underwriting allows loss ratios excess of 100%
Excess market capacity limited (market demands high attachments/prices)
Historically insureds buy down (per claim/agg. limits) during soft market ultimately resulting in significant working layer losses for excess market
Adverse loss development on prior years loss reserves
Often driven by late reserve development on large cases
HOWEVER
towerswatson.com
© 2013 Towers Watson. All rights reserved.
17
Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
Hard Market Cycle Generally Requires a “Perfect Storm” (continued)
While there is some evidence of increased severity of large claims, overall trend indications remain moderate (≤ 5%)
Investment returns remain low but relatively stable
Commercial underwriting is more stable – significant excess capacity
As systems have formed, insureds have taken larger retentions with no aggregates – excess markets are not in the working layer
Low investment income requires better underwriting
Actuarial data improved substantially
Claims reporting, settlement and payment patterns accelerated
Increased healthcare risk management/safety focus has lowered trends
Loss reserve development on prior years is still favorable (graphs)
towerswatson.com
© 2013 Towers Watson. All rights reserved.
18

Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
Medical Malpractice Ultimate Loss Est. by Coverage Year/Valuation Date
towerswatson.com
© 2013 Towers Watson. All rights reserved.
19
Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
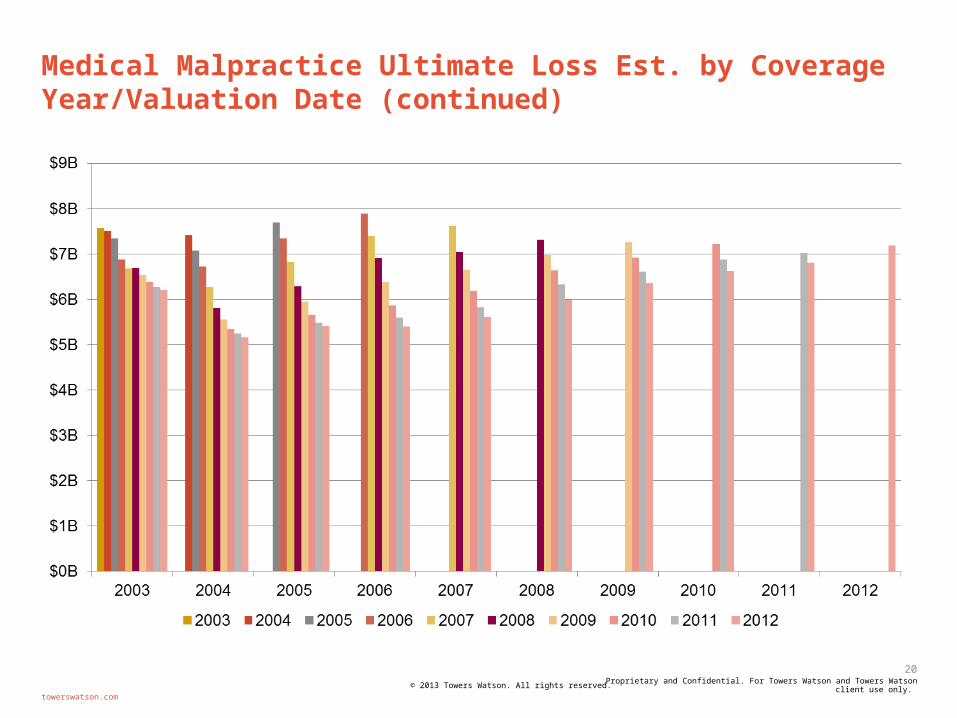
Medical Malpractice Ultimate Loss Est. by Coverage Year/Valuation Date (continued)
towerswatson.com
© 2013 Towers Watson. All rights reserved.
20
Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
The New Normal
Healthcare captives under Affordable Care Act
Primary Challenges
Physician “Employment”/Alignment
Mergers/Acquisitions/Affiliations/Partnerships/JOA’s/Management Agreements/Purchasing Agreements
Other healthcare systems/hospitals
Other healthcare entities
Supply chain
towerswatson.com
© 2013 Towers Watson. All rights reserved.
21

Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
The New Normal (continued)
Current Issues
Combining coverage for taxable/non taxable/Governmental entities
Mergers result in multiple captives requiring consolidation
New acquisition currently participates in a group captive with multi-year withdrawing commitments
Deals negotiated without risk management involvement or review
Branding/agency theories – don’t own or control it but legally responsible
Managed care exposures/credentialing risk
Diversity of coverage (system at $100M, affiliated/owned entity at $1M)
towerswatson.com
© 2013 Towers Watson. All rights reserved.
22
Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
The New Normal (continued)
“New” exposures/threats
While professional liability remains the primary focus of healthcare captives, other exposures will take on increased significance
– Cyber liability
– Managed care liability (provider/insured)
– Medical stop loss (employee/provider?)
– E&O/D&O/EPL
– Governmental Errors & Omissions
towerswatson.com
© 2013 Towers Watson. All rights reserved.
23
Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
Don’t Forget the Mission
Captive Mission Statement (in 10 words of less)
Minimize risk
Minimize cost of risk
Support parent business (mission)
towerswatson.com
© 2013 Towers Watson. All rights reserved.
24

Proprietary and Confidential. For Towers Watson and Towers Watson client use only.
Bill’s Precepts Still Important When Considering Coverage
Don’t risk a lot to save a little
Retain risk that is controllable and predictable
Transfer risk that is volatile or unpredictable
Retain “owned” risk and transfer “non-owned” risk
towerswatson.com
© 2013 Towers Watson. All rights reserved.
25
Healthcare Captives –Dealing with the “New Normal” in
Healthcare
Shulamith Klein, Chief Risk OfficerEmory University – Emory Healthcare
IMAC 2013Pre-Forum Tutorial
Grand CaymanDecember 3, 2013

Facts & Figures
• Academic health system (Atlanta, GA)
• Clinical arm of Emory University
• 6 hospitals (tertiary, geriatric, orthopaedic)
• Multi-specialty, primary care outpatient clinics
• Nursing & rehab
• Clinical & research affiliates
27

Facts & Figures
• $2.4 billion net revenue
• $72 million charity care
• 15,000 staff employees
• 1,300 employed physicians
• 1,900 hospital beds
• 61,700 inpatient hospital admissions
• 3.8 million outpatient service visits
28

Conservative in purpose,broad in scope
excessreinsurance
(commercial)
$3mm/$3mmbuffer layer
(captive)
$3mm/claim (captive)
29
• medical professional & general liability• staff & employed physicians• course & scope of employment• no prior acts coverage• full program limits for all insureds
____________• batch coverage• clarity around clinical trials • volunteer activity• punitive damages• patient’s personal property
The perfect storm
• Weak economy • Workforce shortages• Baby boomers retiring• Rising healthcare costs • Market consolidation• Health care reform• Stress on AMC tripartite mission
30
The end of the ball for all Cinderellas
• Transition from fee-for-service to accountable care
• Payment models based on clinical outcomes, service, and safety
• Less revenue per patient
31
Emory Healthcare strategy
• Demonstrate VALUE by providing highest quality care cost-effectively
• RE-INVEST in select capital projects and tripartite AMC mission
• GROW STRATEGICALLY by participating in market consolidation
32

New normal #1“clinically integrated network”
• employed and community physicians with Emory privileges
• limited clinical performance data
• hybrid use electronic med record and paper
• employed, community, and independent physicians
• founded on clinical quality, efficiency, & collaboration
• quality data tracked for all participants
• shared savings based on quality metrics
• universal use of electronic med record
33
Old World New World

New normal #2“prior acts coverage”
• pre-employment tail purchased through prior carrier
• captive provides 1st dollar coverage upon hiring
• community hires: pre-employment retro date rolls into MagMutual primary policy
• MagMutual provides 1st dollar coverage for 2 years
• excess through captive • post-2 years, tail options for
pre-employment includes captive (except for ob’s)
34
Old World New World
New normal #3“collaborative physician insurer
relationships”
• MagMutual largest insurer Georgia private physicians
• covers majority non-Emory codefendants
• finger-pointing between co-defendants
• primary insurer for Emory community hires
• clinical site visits• valuable risk mgt resource• residents participate in
Patient Safety Program• open dialogue regarding
litigation strategy
35
Old World New World
An enlightened liability program
excessreinsurance
(commercial)
$3mm/$3mmbuffer layer
(captive)
$3mm/claim (captive)
36
• prior acts coverage for pre-employment exposures
• increased risk of vicarious liability for independent participants in network
• captive excess of MagMutual for community hires
• filling gaps between captive & MagMutual (“DIC”)
• collaboration with non-Emory co-defendant
Developing areas potential exposure
• Management liability errors and omissions• Clinical trials (other than bodily injury)• Healthcare regulatory liability• Third party legal advice• Miscellaneous errors and omissions
37
38
A team working together…
EMORY HEALTHCARE
INSURANCEBROKER
FUND CUSTODIAN
CAPTIVEMANAGER
AUDITOR
ACTUARY
COMMERCIALINSURER
INVESTMENTMANAGER
LEGALCOUNSEL
INSURANCEBROKER
CAPTIVEMANAGER
AUDITOR
ACTUARY
COMMERCIALINSURER
INVESTMENTMANAGER
LEGALCOUNSEL
FUND CUSTODIAN
FUND CUSTODIAN





























