Embed Size (px)
Citation preview

- Draft Background Paper 10 -
Health sHealth sHealth sHealth systems, ystems, ystems, ystems, public health ppublic health ppublic health ppublic health programsrogramsrogramsrograms,,,, and and and and
social dsocial dsocial dsocial determinanteterminanteterminanteterminants of hs of hs of hs of healthealthealthealth
Thailand
Jadej Thammatach-aree
Director of Bureau of Policy and Planning,
National Health Security Office (NHSO); Thailand

- Draft Background Paper 10 -
2
Disclaimer
WCSDH/BCKGRT/10/2011
This draft background paper is one of several in a series commissioned by the World Health Organization for the
World Conference on Social Determinants of Health, held 19-21 October 2011, in Rio de Janeiro, Brazil. The goal of
these papers is to highlight country experiences on implementing action on social determinants of health. Copyright
on these papers remains with the authors and/or the Regional Office of the World Health Organization from which
they have been sourced. All rights reserved. The findings, interpretations and conclusions expressed in this paper are
entirely those of the author(s) and should not be attributed in any manner whatsoever to the World Health
Organization.
All papers are available at the symposium website at www.who.int/sdhconference. Correspondence for the authors can
be sent by email to [email protected].
The designations employed and the presentation of the material in this publication do not imply the expression of any
opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory,
city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps
represent approximate border lines for which there may not yet be full agreement. The mention of specific companies
or of certain manufacturers' products does not imply that they are endorsed or recommended by the World Health
Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the
names of proprietary products are distinguished by initial capital letters. The published material is being distributed
without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the
material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its
use.

- Draft Background Paper 10 -
1
Introduction
The development of society can be reflected in the quality of its population’s health, how reasonably
health is distributed across social level, and the effectiveness of health care risk protection provided
from public policy (World Health Organization. 2008). These determinants have effects on health in
complex ways. Social determinant of health associated with the socioeconomic and political context
such as governance, social and public policies. It influences social living and behavior of people
(Dedmon 2010). Health inequalities arise from unequal distribution of such determinants, which create
or limit the ability of the poor to seek for health care and healthy behaviour.
In order to reduce health inequity, taking action on well-planned disease control and treating existing
diseases might not be only ways to improve health equity. Social and economic concerns are also crucial
determinants (Marmot 2005). In Sweden, for example, incorporated social, economic and health issues
into public health objectives to ensure good health on equity for its entire population. Of which, these
factors determine the consequences of social structures toward personnel health-related behaviours.
The objectives are set in eleven domains which are; (1) Participation and influence in society (2)
Economic and social security (3) Secure and favourable conditions during childhood and adolescence
(4) Healthier working life (5) Healthy and safe environments and products (6) More health-promoting
services (7) Effective protection against communicable diseases (8) Safe sexuality and good
reproductive health (9) Increased physical activity (10) Good eating habits and safe foods (11) Reduced
use of tobacco and alcohol, in order to build a society free from illicit drugs and doping and a reduction
in the harmful effects of excessive gambling (Hogstedt, Lundgren et al. 2004).
Equality in health is mainly determined by the increasing access to care and the decreasing catastrophic
expenditure in population (Kutzin 1998). Conceptual framework for actions of social determinant of
health proposed by Solar and Irwin (2007) indicated that there were two main factors affecting inequity.
They are structural and intermediary determinants. Structure determinant incorporated context,
structural mechanism and individual resultant socioeconomic position while intermediary determinants
embodied material circumstances, psychosocial circumstances, behavioural and/or biological factors,
and health system (Solar and Irwin 2007). Examples of health system affecting determinant of health
are human resource, health care financing, and health service delivery. Evidence showed that health

- Draft Background Paper 10 -
2
system movement is the key role of improving equitable access to care and protect impoverishment of
people from health expenditure (Marmot 2007).
Thailand is an example of improving social determinant of health by implementing universal health
coverage (UHC). It took a big bang change to universal health coverage (UHC) by extending coverage to
nearly 30 percent of overall population who were previously uninsured (Towse, Mills et al. 2004). The
important action was the financial reform that moved funding from supply side allocation to demand
side by using budget per capitation for responsible catchment area resulting in shifting fund from urban
hospitals to the building up of primary care units. The goal of the reform was to balancing health
opportunities across the different socioeconomic groups and to narrowing the gap between the rich and
the poor. The processes of this movement could be ideas for other countries for the moving of policy, not
only for achievement of the UHC but can be applied to other policy issues. The aim of this report is to
determine the process of health system to support the social determinant of health relating to universal
health coverage implementation.
Developing of universal Developing of universal Developing of universal Developing of universal health coverage in Thailand health coverage in Thailand health coverage in Thailand health coverage in Thailand
The development of Thai universal health coverage could be traced back to 1974 when it established
workmen compensation fund to cover private employees who were injured from working. The coverage
for employees who have illness not related to work came later in 1990 denoted as social security
scheme (SSS). At the beginning, it covered only companies with more than 20 employees and expanded
to cover more than 10 employees in 1994. Then the benefit covers every company with more than one
employee in 2002. Another public health insurance scheme, the Civil Servant Medical Benefit Scheme
(CSMBS) was set up in 1978 covering all government employees and dependants which are spouses,
parents, and not more than two children under 18. At the same time, government set up the low income
card scheme (LICS) for poor people in 1975 and expanded to community base health insurance scheme
(CBHI) based on maternal and child health in 1983. This led to change from community base financing
to voluntary health insurance by moving the management of funds from village level to involvement in
sub-district level by introducing health card scheme (HCS) in 1991. The newest scheme; the Universal
coverage scheme (UCS), was set up in 2001 by combining all the rest of population who were LICS, HCS,
fee exemption groups, and uninsured people. Consequently, after 2001, Thailand health care coverage

- Draft Background Paper 10 -
3
is mainly three schemes including SSS, CSMBS, and UC scheme. The details of universal health
coverage in Thailand are shown below.
Before 1974
Fee Exemption
1974 WCF
1975 LICS
1980 CSMBS
1981
Type B fee exemption
1983 CBHI
1990 SSS
1991 HCS
Traffic Accident Protection Program (TAP) 1993
Poor people
Near poor
Uninsured
2002 UCS implemented nationwide
Year Private employee Government
employee Population covered by Universal Coverage Scheme (UCS)
Adapted from: NHSO 2010
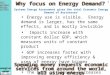
The historical milestone is described against the economic capacity of the country measured in term of
Gross National Income per capita between 1970 and 2009. The development of health insurance
coverage relates to GNI per capita, for example in 1975 Thailand introduced LIC when the GNI per
capita was $390 USD. During the period of low income state, Thai health system moved by introducing
LIC, CSMBS which Thailand experiences showed that in the situation of low GNI per capita in 1975.
Community based health insurance scheme was introduced in 1983 when GNI was $760 USD. Finally,
UHC was implemented in the period of economic crisis when GNI per capita is about $1,900 USD.

- Draft Background Paper 10 -
4
390
710
760
1490
2,700
1,900
0
1,000
2,000
3,000
4,000
1970
1972
1974
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
US $
1997: Asian
financial crisis
1990 SHI
introduced
1980 CSMBS
introduced
1983 CBHI
introduced
1975 Low Income
scheme introduced
2002 Universal
Coverage for entire
population achieved
2001: 29% of
population are
uninsured
From: Tangchareonsathien 2010
Health expenditure has increased steadily since UHC were implemented. The ratio of private financing
source reduced from approximately 45% in 2000 to 25% in 2008. The proportion was nearly the same
as OECD countries which were 73.6% of health financing across EU countries in 2008 (OECD 2010). The
percentage reduction of private financing implied the decline risk of household expenditure in health
care.

- Draft Background Paper 10 -
5
From: Prakongsai et al. (2009)
The diagram below showed how health system in terms of financial reform played an important role in
improving equitable access of health service and health outcomes of the population. Household and
individual pay tax or contribution to government in order to pooling financial risk depends on their
working status. Private employees in formal sectors pay contribution to SSS while government officers
and the rest of population pay tax. Government allocated the collective fund to different schemes by
using different mechanisms which were tripartite contribution for SSS and general tax for CSMBS and
UC scheme. Different insurance schemes contracted provider in different payment system with some
different benefit packages, for example, UC scheme covers prevention and promotion of services for all
people in the country while SSS and CSMBS cover only curative and some rehabilitation services. UC
scheme also had matching fund with local government to provide preventive care especially in
behavioral modification activities.
56%45% 47% 47% 54% 55% 55% 56%
63% 63% 64% 64%
75%
73% 68%
55%53%
53% 46%45%
45% 44% 44%
36%36%
37%37%
25%
27% 32%
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Year
Millio
n B
ah
t
Public f inancing sources Private f inancing sources

- Draft Background Paper 10 -
6
HA = Hospital AccrditationContribution
enterprise
Government
Insured/Uninsured
population
Benefit
package
Direct &
indirect tax
ContributionService
SSS CSMBS UC scheme
Equity and Access
Financial resources
Performance
Activity
health and well-
being
Local government
General Tax
General Tax
Capitation
OP&IP Capitation for OP
DRG with global budget for IP
Public and private contract
FFS for OP
DRG for IP
Matching fund for Prevention&Promotion
Payroll tax
Contribution
Initiative of UC scheme in equity using matching fund with local governmentInitiative of UC scheme in equity using matching fund with local governmentInitiative of UC scheme in equity using matching fund with local governmentInitiative of UC scheme in equity using matching fund with local government
Financial arrangement of the implementation of UC scheme is mainly four approaches. Of which, are
shifting the main source of health care financing from out of pocket payment to general tax, removing
financial barriers to health service by limit co-payment at 30Baht or one dollar (exchange rate of 30
Baht= 1 dollar) per episode of service (abolish copayment in 2006), changing provider payment from
historical allocations to closed ended payments, and promoting the use of primary care by contract PCU
as the main contractor. UC scheme is designed to offer comprehensive benefit package covering from
prevention& promotion, curative, and rehabilitation. The prevention& promotion can be divided into
three main activities including National Priority Program, P&P for expressed demand, and P&P for area
base problem. The P&P area base aims to promote people participation process and efficient use of
resource by people in the sub district level to manage the prevention and promotion problem in the area
(National Health Security Office 2011).

- Draft Background Paper 10 -
7
According to the National Health Security Act 2002, it announced that in order to provide good health for
all, the National Health Security Office (NHSO) has mandate to promote the collaboration in local levels
to ensure health access for people in community. Under the provision of the act, from 2006 NHSO
provides fund to the sub-district administrators. The sub-district or “Tambon” administrators who have
interested in the fund will enroll and be financed by per capita payment (40 Baht or $1.3 USD in 2010).
Each sub-district authority needs to pay contribution to the fund according to the size of the authority,
20%, 30% and 50% for small, middle and large size respectively. Private financing can be included if
available.
The most important rule for using the fund is there is essential to set up a collaboration group consisting
of local administrators, their residents and delegations from local health authorities. Fund is managed
by the committee and can be paid for only four purposes; managing the fund effectively, providing
services according to the benefit packages, supporting health facilities in the area, and solving the
health problems in community. In 2010, there are 5,504 local authorities or 70% of overall Tambon
included in the project (Samnuanklang, Srithamrongswat et al. 2011). The fund helps fostering
preventive activities such as chronic diseases screening, epidemic control, intensive health care for
elderly and disabled, also sanitation such as eradicating the mosquito larvae and rubbish recycle, all of
which, roots from the locals’ ideas.
Empowerment is the key success of this project, not only one but all three local clusters; the local
administrators, the health officers and the locals. Achievement is proved thru the information gained,
working in team, transparency and building up the same goals. Although, the achievement of the
program in terms of health outcome could not be concluded, some evidence showed progression of
some issues. For example from health examination survey, no access to screening for hypertension
declined from 71% in 2003 to 55% in 2008 (Srithamrongswat 2010).
Different characteristic of three public health insurance schemesDifferent characteristic of three public health insurance schemesDifferent characteristic of three public health insurance schemesDifferent characteristic of three public health insurance schemes
Since Thailand has three main public health insurance schemes after UC implementation covering
99.47% of its entire population (National Health Security Office 2010), the different characteristic of
these schemes led to health inequity of beneficiary between schemes.

- Draft Background Paper 10 -
8
The CSMBS and UCS are financed by general tax whereas the SSS is financed by payroll tax with
tripartite contribution, shared by employer, employee and the government with 1.5% of salary.
Population coverage under CSMBS was about 5 millions (8% of population) and SSS was about 10
millions (16% of population) while UC scheme covered about 47 millions (75% of population). For
service delivery, CSMBS beneficiaries can receive services at any public hospitals with the retrospective
FFS payment on outpatient service and DRG on inpatient service. For SSS, they must receive services at
the registered contractors’ hospital with more than 100 beds, which can be either private or public
hospitals and are mostly located in Bangkok and urban areas. The payment method for the SSS is
inclusive capitation for both outpatient and inpatient, with the adjusted compensation according to
volume of use and risks. The UC scheme members require to receive services at the registered
contracting units for primary care which almost all of them are public facilities. If the registered facilities
cannot provide proper treatment, the patient will be referred to the higher level of health facility. The
different characteristics of the three public health insurance schemes are shown in the table below.

- Draft Background Paper 10 -
9
CSMBS SSS UC scheme
Scheme nature Fringe benefit Mandatory Citizen entitlement
Population Government employees, pensioners and their dependants (parents, spouse, children under 18)
5 Million (8%)
Formal-sector private employees, establishments/ firms of more than one worker since 2002
9.84 Million (15.8%)
The rest of population who are not covered by SSS and CSMBS
47 Million (75%)
Source of finance
General tax
(~323 US$/Cap*)
Tripartite from employer, employee, government rate 1.5% of salary
(maximum salary: 441 US$)
(health care 37 US$ /Cap, total 63 US$/Cap)
General tax
(62 US$/Cap)
Management organization
Comptroller general under ministry of finance
Social security office under ministry of labor and welfare
National Health Security Office (NHSO)
Benefit package No preventive care
No explicit exclusion
Special bed
Small number of limited condition e.g. Non medical plastic surgery
Small number of limited condition
Include Prevention & promotion
Service delivery Public provider only, Private in emergency, selected disease (2011
Public and private hospital more than 100 beds (50% private
Public and private contracting unit for primary care(CUP)
Payment OP: Fee-for-service
IP: DRGs
Capitation both OP and IP OP: Capitation
IP: DRGs with global budget

- Draft Background Paper 10 -
10
Adapted from: (Mills, Tangchareonsathien et al. 2005)
The characteristic of beneficiary under each scheme is different. The UCS mainly covers poor people.
Nearly 50% of population in the scheme are categorize into poorest quintile one and two while SSS
covers poorest quintile only 7% nearly the same as CSMBS which is 6%.
From: Limwatananon et al.(2009)
The difference of payment methods leads to the inequity of services given among the three schemes.
There has been evidence supporting the belief that services provided to beneficiaries under the three
schemes are different. For example, from the data of health and welfare survey 2005, SSS increased
the probability of ambulatory care visits by 41% compared to UC scheme membership, while there was
no significant difference between UC scheme and CSMBS groups (Thammatacharee 2009). In terms of
quality, evidence from claims data showed that readmission in chronic complication of DM patient in UC
scheme had 23% higher chance of readmission compared to SSS and CSMBS.
Greater access to selective care by the CSMBS patients is also obvious for two selected health
interventions based on the national IP data from all types of hospitals during 2004-2007. Both
Cesarean section and laparoscopic cholecystectomy were much more common in CSMBS than in UC
and SSS. These gaps are consistent over the 4-year period. One explanation of this result was that there
24%
1%9%
26%
1% 3%
24%
4%
6%
24%
7% 6%
18%
34% 21%
16%
38%
23%
11%
48%55%
12%
35%
57%
0%
20%
40%
60%
80%
100%
UC SS CS UC SS CS
2003 2007
20% poorest Quintile 2 Quintile 3 Quintile 4 20% richest

- Draft Background Paper 10 -
11
was incentive for physicians to provide services more frequent than the other schemes because of the
fee-for-service payment system (Limwattananon, Limwattananon et al. 2010).
49% 48%51%
47% 47%
52%50%
51%53%
55% 55% 55% 56%54%
51%
24%22% 23% 23%
25% 24%22%
18%
30%
26% 26%28%
27% 27%26%
23%21%
22%20%
24%22%
24% 24% 24%26%
28%27%
29%28% 28%
0%
10%
20%
30%
40%
50%
60%
Qtr
1
Qtr
2
Qtr
3
Qtr
4
Qtr
1
Qtr
2
Qtr
3
Qtr
4
Qtr
1
Qtr
2
Qtr
3
Qtr
4
Qtr
1
Qtr
2
Qtr
3
2004 2005 2006 2007
CS
SS
UC
45%47% 48%
50%52%
50% 51%53% 54% 55% 56%
54%56% 58% 59%
17% 17% 16% 17%18%
20% 20%22% 21% 20% 19% 20%
16% 16% 17% 17% 18% 18% 19% 20% 20% 20% 20% 20% 20% 21% 21%
0%
10%
20%
30%
40%
50%
60%
Qtr
1
Qtr
2
Qtr
3
Qtr
4
Qtr
1
Qtr
2
Qtr
3
Qtr
4
Qtr
1
Qtr
2
Qtr
3
Qtr
4
Qtr
1
Qtr
2
Qtr
3
2004 2005 2006 2007
CS
SS
UC
Cesarean section Laparoscopic cholecystectomy
From: Limwatananon et al. (2009)
This pattern is also consistent in the prescription of expensive drug. Propensity to receive expensive
drugs is shown by monthly time-series over five years in the graphs below. CSMBS patients utilized very
much more expensive drugs than patients in SSS and UC scheme. For example, Angiotensin receptor
blockers were prescribed to CSMBS patient more than 20% while SSS and UC scheme were less than
10% during four year period from 2003 to 2007. This prescription pattern was the same as other
expensive drugs such as Statins, Coxibs and the anti-platelet drug, Clopidogrel.

- Draft Background Paper 10 -
12
Angiotensin II receptor blockers
0
5
10
15
20
25
30
35
40
45
50
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
2003 2004 2005 2006 2007
CS
SS
UC
Single source statins and new antihyperlipidemia
0
5
10
15
20
25
30
35
40
45
50
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
2003 2004 2005 2006 2007
CS
SS
UC
Clopidogrel
0
5
10
15
20
25
30
35
40
45
50
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
2003 2004 2005 2006 2007
CS
SS
UC
Coxibs
0
5
10
15
20
25
30
35
40
45
50
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
Ja
n
Ap
r
Ju
l
Oc
t
2003 2004 2005 2006 2007
CS
SS
UC
From: Limwatananon et al. (2009)
In general, CSMBS consumes more resources than other two schemes. With its fee-for- service
reimbursement model, the total expenditure of CSMBS was dramatically increased every year especially
after 2001. The main incretion was outpatient service while inpatient service seemed to be stable after
implementation of prospective payment by using DRG payment in 2006.

- Draft Background Paper 10 -
13
From: Comptroller General Department, Ministry of Finance
These findings have allowed the inequity issue among the schemes become more intense. The major
critics are; who pay more and who pay less, or what kind of benefits should be added for scheme which
paid more. The rationale behind SSS is that beneficiaries contributed for health service each month
from salary and they also pay general tax while UC scheme pay only tax without contribution but SSS
seems to get the same service or less in some situations. CSMBS members believe that they accepted
low salary compared to private since they needed to have more privilege of health service when they
retired. UC scheme by law had a section to allow merging fund from CSMBS, SSS and TAP but they did
not enough knowledge how to move in the way as mention in the act although some propose that this
should be a basic benefit package that everyone in the country could receive while each scheme can
add some privilege benefit to their beneficiaries such as special room. This issue might still the debate
in Thai society for a long time.
How healHow healHow healHow health inequity issues moved in th inequity issues moved in th inequity issues moved in th inequity issues moved in Thailand?Thailand?Thailand?Thailand?
The inequity in Thailand has begun to be a policy issue since 1975. The government introduced the low
income card in order to help the poor patients obtained health care from public facilities without charge.
The initial idea was not complicated since it covered only the poor who had income per year lower than
-2%
23%
12%13%
20%
12%
6%
10%
-2%
15%
12%
16%
20%46,588
61,304
37,004
54,904
46,481
17,058
26,043
20,476
16,44013,587
9,954
3,1566,000
4,316
62,196
13,905
21,896
30,833
38,803
9,5097,007
1,729 2,3373,374
5,8664,826
45,531
1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Annual grow th (real term) Total expenditure (million Baht) Outpatient (million Baht) Inpatient

- Draft Background Paper 10 -
14
1,000 Baht ($30 USD approximately in 2010 rate) (Suksiriserekul 1998). Normally, the National
Economic and Social Development Plan have been implemented through the government policies. When
it came to the era of the fifth five-year National Economic and Social Development Plan (1982-1986),
the inequity problems were apparently emphasized in the plan that it aimed to solve impoverishment of
the people in the specified areas. Consequently, public facilities have been widespread to the rural, for
example, community hospitals covered in most districts (Termpitayapaisit and Paem 2009). Health
welfare scheme was reconsidered to separate the card holders into 3 types; elderly, children and the
poor (Suksiriserekul 1998).
In the sixth five-year National Economic and Social Development Plan (1987-1991), the plan stated to
increase the country development capacity, the economic grew prosperously reflected in the GDP growth
around 10.9% per year. Nonetheless the political and social movements to improve inequity, income
disparity has become wider (Termpitayapaisit and Paem 2009). Gini coefficient1 for income distribution
has increased more rapidly from 0.45 in 1975 to 0.49 in 1988 and to 0.54 in 1992 (Sakunphanit and
Suwanrada 2011). Many of the poor dared not to use the low income cards due to doubt in the quality of
care given for free. Insufficient and inappropriate budget distribution of low income card also presented
(Suksiriserekul 1998).
Social problems and inequity became more explicit after the global economic crisis in late 1997; in
addition, the circumstance also brought the Thai health care reform to light. An independent institute,
Health System Research Institute Research (HSRI) with an assistant team from Asian Development
Bank (ADB) provided evidence-based recommendation that Thai health system needed to be reformed
in order to achieve equity, efficiency and quality (Pannarunothai and Srithamrongsawat 2000). The
reform plan originally was to combine the three public health insurance schemes into one universal
coverage scheme. However this idea met resistance from civil servants in other government sectors who
benefited from running the other two schemes(Towse, Mills et al. 2004).
1 Gini coefficient is a measurement of inequality of distribution. The value is between 0 and 1, 0 means total
equality which 1 means total inequality.

- Draft Background Paper 10 -
15
Apart from the financial issue, distribution of health workforce was also problematic. The ratio of
population per doctor was different across regions in Thailand. Northeastern area has the highest
population per doctor proportion in the country which emphasis the disparity gap when comparing with
that in Bangkok area. However, the situation tends to improve so far. There were a few policies to ease
the problem such as the increasing production of doctors and the new university admission system that
promote the rookies to work in rural areas. As a result, the ratio of population per doctor in the
Northeastern region increased from 7,614 in 2001 to 2,870 in 2009.
Region 2001 2002 2003 2004 2005 2006 2007 2008 2009
Bangkok 760 952 924 879 867 886 850 955 565
Central 3,375 3,566 3,301 3,134 3,054 2,963 2,683 2,839 1,864
Northern 4,488 4,499 4,766 4,534 3,768 3,351 3,279 3,386 2,002
Southern 5,127 4,984 4,609 3,982 4,306 3,789 3,354 3,694 2,250
Northeastern 7,614 7,251 7,409 7,466 7,015 5,738 5,308 5,028 2,870
From: (Wibulpolprasert 2010)
Universal Coverage Move in Thailand Universal Coverage Move in Thailand Universal Coverage Move in Thailand Universal Coverage Move in Thailand
To move important policy such as universal coverage in Thailand, there is an approach proposed by Prof.
Prawase Wasi called “Triangle that moves the mountain”. Mountain is a symbol representing tough
problem. Triangle stands for a system consisting three mountain movers, working together, such movers
are; 1) research-based knowledge, 2) social movement or social learning and 3) regulations form
political movement (Wasi 2000). Thailand has long been invested in research and capacity building
before proposing policy option in moving to universal health coverage. For example, cumulative
experience provider payment both fee for service in CSMBS and capitation in SSS result in moving to
capitation payment in UC scheme(Tangcharoensathien, Prakongsai et al. 2007). Social movement from
NGOs to mobilize more than 50,000 people to support universal health coverage bill played an
important role for parliament to consider the bill. Political movement was a crucial part of universal
health coverage in Thailand. Leadership of politician with influenced campaign of “30 Baht cure all

- Draft Background Paper 10 -
16
disease” and bridging political movement with evidence helped universal health coverage moved
rapidly.
Dr. Sanguan Nitayarumphong, who was a very first campaigner of universal health coverage move in
Thailand gave details of universal coverage program move in his book “Struggling along the path to
universal health care for all” into three phases as shown in diagram below (Nitayarumpong 2006). The
main three steps comprised of policy move, implementation, and sustainability of the program. The
policy move was based on the concept of triangle that moves the mountain of Dr. Prawas Wasi as
mention above. From his experience, he proposed two important policies to various political parties
during election which were 1) generation of revenue into public health finance program by using sin tax
and 2) universal health care (UHC) coverage. Of which, the Thai Rak Thai party leader accepted the
second one to be policy of the party.
The other important issue was how to apply that policy of UHC. This implementation plan was crucial as
a policy movement. The UHC implementation composed of three reform issues which were new health
care financing, new budget allocation, and new health care delivery model. The proposal of new health
care financing was based on objective of reduce out of pocket payment system and equalize health care
financing by collective financing mechanism.
Tax finance was one of easily way to generate the adequate level of government revenue. Since 1978,
past experiences from the public insurance schemes have provided ideas for the new budget allocation
mechanism. For examples, CSMBS payment by fee-for-service proved that it encouraged the increasing
health care costs. SSS provided a successful story of using capitation both in outpatient and impatient
service to limit the costs. Low income card gave experience of using prospective case based payment by
diagnosis related groups (DRGs). Furthermore, a global budget in provincial level under a number of
beneficiaries provided information of closed end budget management(Towse, Mills et al. 2004).
Another important movement was the new idea of direct contracting to the primary care units (PCUs);
the fund could flow directly to the PCUs instead of general or regional hospitals. A PCU was a unit in the
network of primary care consisting of a district hospital and health centers in the catchment area. A new
concept of creating health by people was introduced to promote good health.

- Draft Background Paper 10 -
17
However, this movement is still in a long way to success since there is need to change attitude of both
beneficiaries and providers.
Adapted from: Wasi P. (2000), Nitayarumphong (2006)
As mentioned above, policy move and implementation is a tough and long process of movement not only
the UHC program but also other important policy issue. However, the harder movement is how to sustain
the program in the system in order to achieve the policy objectives. The crucial sustainability of a policy
move is to manage the triangle continuously. Further knowledge of how to improve health system and
popular support of the program must be maintained while the political decision making must not be
allowed to decline. In UHC movement, there are three challenges that support the program including
assuring quality of care, job satisfaction for healthcare provider, and effective management. Quality of
care of the UHC in Thailand is the most important measurement to assess the value of UHC. Lacking of
quality of care would turn people back to the old system and end up with collapse of the program. To
develop full confidence for the society on UHC, the quality of personnel and technical service should be
enhanced; timely diagnosis with effective treatment should be improved.

- Draft Background Paper 10 -
18
Concurrently, UHC could not survive without sustaining the worker confidence. The UHC has created
tremendous workload and misunderstanding about job security and technology advancement.
Therefore, maintaining satisfaction of healthcare personnel by using both financial and non financial
incentive is a prime concern of the government. The last burden of sustaining UHC is that social want to
receive high quality of care with proper tax burden. The system needs to be transparent, accountable,
and incorporate public participation. The addressed problems need to rapidly solve to maintain
atmosphere of ongoing improvement. The budget allocation needs to be more efficient. The system
needs to be more equitable and efficient.
Even though the UHC achievement in Thailand has progressed constantly, there are still problems of
some issues, for example, whether Thailand should follow the solidarity idea as the European countries
or based on ability to pay as leaded by the USA. The solution of any problems in health system cannot
solve easily without comprehensive knowledge, good planning of implementation, sustaining solutions
and continuous improvement of implementation.
Adapting this conceptual framework into the implementation, UHC in Thailand was planned as a rapid
move by dividing the implementation into four phases to coverage people all the country within two
years. The first phase was to cover beneficiaries in six provinces. After that, the scheme expanded to
fifteen provinces within six months. The third phase was to spread out to all provinces in the country
except Bangkok. Then the final phase was to implement in Bangkok.
Case study of political move in stateless people rights Case study of political move in stateless people rights Case study of political move in stateless people rights Case study of political move in stateless people rights
One example of implementing conceptual framework of political movement related to UHC move was
the return rights of stateless people in Thailand.
In Thailand, there are groups of people who are identified as undocumented person, refugees, minority,
migrant workers or a common term, stateless person. Such of these people share one problem in
general, they do not have Thai nation. Many of them, for example minorities or undocumented persons,
were Thai born and have long been stayed in the country waiting in the process for citizenship.
Possession of Thai nationality is not only for living with respect in social, but also a crucial access to
fundamental rights especially, the right to healthcare services. Before the era of UC, stateless persons
used to have ‘low income health card’ that they used to get care in public health facilities with none of

- Draft Background Paper 10 -
19
charges. Nonetheless, after launching UCS, the low income health card became invalid and these
people were excluded from UC eligibility. The reason was because stateless people do not have Thai
nationality and by interpreting the National Health Security Act 2002 that universal coverage was
reserved only for Thais. As a result, 457,409 people were withdrawn from the universal coverage (NHSO
2010). Consequences of the UHC implementation, stateless persons were denied access to free health
services in public facilities. The reason given was that government did not allocate any budgets for them.
In one case, a severe patient had to tell a lie to healthcare officer that she had enough money to pay for
treatment, actually she did not otherwise she would not get the adequate services. Another case of a
cancer patient, he passed away and left a huge debt to his family which they did not know how they
could pay back.
In addition to unable to obtain personnel health care, social problems followed. Contagious diseases
such as malaria, tuberculosis, severe diarrhea and sex transmitted diseases were concentrated among
the stateless people. Rare cases were found in new areas, especially the borderlines. Bad debts were
financial burden for hospitals of humanity without any support from the government. In 2008, for
stateless persons who got services from public health facilities, the health expenditure of 468 million
Baht or 117 million USD was reported (NHSO MOPH and HISRO 2009).
This problem had been in public awareness and there were attempts from various sectors to move ‘the
mountain’ forward. In 2005, the National Security Council offered the cabinet the strategic plans for
dealing with citizenship and the rights of stateless person. Nonetheless, the strategies were agreed
especially in education problem, but there was lack of practical procedures to pursue in health issue. At
that time, the National Health Security Board (NHSB) proposed the cabinet to approve the health
insurance for stateless person, twice in 2005 and 2006 but both were rejected for the concern of
national security. However, the movement has gone forward by launching a series of six studies to
identify the health problems of statelessness in Thailand in order to scope the problems conducted in
2008 by NGO researchers, probe the current situations and design the appropriate solutions for this
matter. At the same time, the NHSB proposed the cabinet for reconsidering the health insurance issue,
again it was rejected and the cabinet advised to seek for stakeholders’ views. Therefore, the National

- Draft Background Paper 10 -
20
Health Assembly held a forum consisting of a range of government agencies, for examples, from the
National Security Council, Ministry of Public Health, Ministry of Education, Ministry of Labour, Ministry of
Interior, Immigration Office and the National Health Security Office. The forum agreed in principle that it
was the responsibility of the government to establish good health for its residences. Therefore, giving
health security for stateless persons would be providing fundamental rights of human to support and
strengthen the system as a whole. In 2010, NHSB once again tendered the proposal to the cabinet. The
cabinet finally approved. Accordingly, the targeted stateless people, 600,000 approximately were then
entitled to the UCS with the rights to access healthcare equally to Thai under UCS. The cost of health
care was 2,067 Baht/Capitation since this group of people is mainly in the working age group with some
of children as shown below; therefore, overall Baht/capitation was lower than Baht/capitation of overall
people. In addition, a communicable diseases control fund was set up particularly for bordered hospitals
in order to support their control of disease activities. This success story could prove that success
movement of important policy issue from three pillars, knowledge, political movement, and civic
movement.
From: NHSO 2010

- Draft Background Paper 10 -
21
Evidence of health equity achievement in Thailand from Universal Coverage SchemeEvidence of health equity achievement in Thailand from Universal Coverage SchemeEvidence of health equity achievement in Thailand from Universal Coverage SchemeEvidence of health equity achievement in Thailand from Universal Coverage Scheme
The implementation of the UCS as the attempt to provide access to health for all and protect household
catastrophic has shown the positive effects in a number of studies. For examples of financial evidence,
there were percentage reductions of financial health indicators. Of out-of-pocket paid for health per
household income gradually declined as the most obvious in the lowest income deciles, from 6.4% in
1992 to 2.3% in 2006 (Prakongsai, Limwattananon et al. 2009). This result corresponded to another
study (Somkotra and Lagrada 2008) which found that the richer income quintiles were at more tendency
to pay from their own resources.
Kakwani index Share of healthcare finance Type of health
payments 2000 2002 2004 2006 2000 2002 2004 2006
Out of pocket
payments
-0.150 -0.076 -0.076 -0.045 33.7% 27.9% 26.4% 23.2%
Direct tax 0.391 0.416 0.442 0.362 18.0% 18.8% 20.8% 24.5%
Indirect tax -0.096 -0.069 -0.043 -0.083 33.4% 38.2% 37.1% 35.2%
Private insurance
premium
-0.362 -0.391 -0.323 NA 9.6% 9.2% 8.9% NA
SHI contribution 0.165 0.112 0.105 NA 5.3% 5.9% 6.8% NA
Private insurance
premium & SHI
contribution
NA NA NA -0.049 NA NA NA 17.1%
Overall Kakwani index -0.004 0.001 0.034 0.041 100.0% 100.0% 100.0% 100.0%
From: Limwattananon, Vongmongkol et al. (2011)
Catastrophic health spending which specified as a stage that out-of-pocket payment for health higher
than the threshold of 10% of total household consumption decreased steadily in all income quintiles

- Draft Background Paper 10 -
22
during the UC implementation with the power to reduce spending in the poor group the most (Somkotra
and Lagrada 2008; Prakongsai, Limwattananon et al. 2009). For healthcare induced impoverishment
indicator, usually, out-of-pocket cost borne by inpatient services was the main cause of impoverishment.
However, in the UC period this figure went down from 11.9% in 2000 to 2.6% in 2004 (Prakongsai,
Limwattananon et al. 2009). Data from Health and Welfare Survey in various year showed that the
incidence of catastrophic health expenditure reduced in both poorest quintiles and least poor quintiles
with more reduction on poorest quintiles as shown in the table below (Limwattananon, Vongmongkol et
al. 2011). Although there was still 2% of the population faced with catastrophic expenditure, this was
significantly lower in poorest quintiles which was 0.9%, compared to least poor quintiles which was
3.3%.
Income quintiles 2000 2002 2004 2006
Q1 (poorest) 4.0% 1.7% 1.6% 0.9%
Q5 (least poor) 5.6% 5.0% 4.3% 3.3%
All quintiles 5.4% 3.3% 2.8% 2.0%
From: Limwattananon, Vongmongkol et al. (2011)
Regarding the service coverage findings, after implementing the UC there was wider and greater
outpatient utilization, particularly the lower income quintiles at health centres and district hospitals as
demonstrated by negative concentration indices (CI) (Prakongsai, Limwattananon et al. 2009). The CI
ranges from -1 to +1. A CI of zero means an equal distribution of particular indicator throughout the
economic gradients. A negative CI indicates a concentration among who are poorer group while a
positive CI reflects concentration in richer group. Mother and child health also distributed quite well
though, the wealthy mothers appeared to have better access to antenatal and delivery care due to the
higher level of education (Limwattananon, Tangcharoensathien et al. 2010). In addition, child
malnourishments also concentrated on poorer group. The CI was between -0.065 in wasting to -0.219 in
under weight. Additionally, the high cost benefit packages which once were excluded from the UCS
caused either barriers to adequate treatment or bankrupt by health spending to poor patients

- Draft Background Paper 10 -
23
(Prakongsai, Palmer et al. 2009). Equity in service utilization in outpatient and inpatient were shown
below. The negative value meant that service pro poor while positive value meant pro rich. Data
analyzed from Health and Welfare Survey in various year showed that for ambulatory care in health
centres, district hospitals, and provincial hospitals were pro poor while university hospitals seem to pro
rich. This result can be implied that district health centres, district hospitals, and provincial hospitals
performed well in terms of pro poor utilization. This might be due to the geographical proximity to rural
population who are vastly poor. This pattern was consistent before and after UHC implementation meant
that pro poor utilization was maintained. However, the pro rich pattern of university and private hospital
might be explained that main customers of these hospitals are CSMBS and SSS patients who are better
off than UC scheme patients. This pattern was similar in hospitalization of inpatients.
2001 2003 2006 2007
Ambulatory care -0.167 -0.219 -0.148 -0.119
Health centre -0.303 -0.351 -0.285 -0.292
District hospital -0.291 -0.304 -0.258 -0.258
Provincial hospital -0.051 -0.085 -0.007
University hospital
-0.045a
0.295 0.437 0.364
Private hospital 0.419 0.395 0.482 0.525
Hospitalization -0.080 -0.138 -0.068 -0.090
District hospital -0.315 -0.288 -0.232 -0.284
Provincial hospital -0.123 -0.090 -0.129
University hospital
-0.070a
0.040 0.204 0.394
Private hospital 0.325 0.321 0.407 0.470
From: Limwattananon, Vongmongkol et al. (2011)

- Draft Background Paper 10 -
24
References
1. Dedmon, R. E. (2010). "Health in Asia and the Pacific." Asian Biomedicine (Research Reviews and News)
3(5).
2. Hogstedt, C., B. Lundgren, et al. (2004). "Background to the new Swedish public health policy." Scandinavian
Journal of Public Health 32(Supplement 64): 6-17.
3. Kutzin, J. (1998). Enhancing the insurance function of health systems : A proposed conceptual framework.
Achieving Universal Coverage of Health Care. S. Nitayarumpong and A. Mills. Nonthaburi, Office of Health
Care Reform: 238.
4. Limwattananon, C., S. Limwattananon, et al. (2010). Analysis of practice variations due to payment methods
across health insurance schemes. Paper presented at Country Development Partnership in Health workshop 30
April – 2 May 2009, Siam City hotel, Bangkok.
5. Limwattananon, S., V. Tangcharoensathien, et al. (2010). "Equity in maternal and child health in Thailand."
Bulletin of the World Health Organization 88(6): 420-427.
6. Limwattananon, S., V. Vongmongkol, et al. (2011). The equity impact of Universal Coverage: health care
finance, catastrophic health expenditure, utilization and government subsidies in Thailand.
7. Marmot, M. (2005). "Social determinants of health inequalities." The Lancet 365(9464): 1099-1104.
8. Marmot, M. (2007). "Achieving health equity: from root causes to fair outcomes." The Lancet 370(9593):
1153-1163.
9. Mills, A., V. Tangchareonsathien, et al. (2005). Harmonization of health insurance schemes: A policy analysis.
Nonthaburi, National Health Security Office: 28.
10. National Health Security Office (2010). The Annual Report 2009 (In Thai). Nonthaburi, National Health
Security Office (NHSO).
11. National Health Security Office (2011). Fund management manual of national health security (in Thai).
Nonthaburi, NHSO
12. NHSO MOPH and HISRO (2009). Building the Health Insurance for the Stateless, National Health Security
Office, Ministry of Public Health and Health Insurance Service Research Office: 23.
13. Nitayarumpong, S. (2006). Struggling Along the Path to Universal Health Care For All. Nonthaburi, National
Health Security Office (NHSO).
14. OECD (2010). Health at a Glance, Organisation for Economic Co-operation and Development.
15. Pannarunothai, S. and S. Srithamrongsawat (2000). "Benchmarks of fairness for health system reform: the tool
for national and provincial health development in Thailand." Human resources for health development journal
4(1): 13-26.
16. Prakongsai, P., S. Limwattananon, et al. (2009). "The equity impact of the universal coverage policy: lessons
from Thailand." Innovations in health system finance in developing and transitional economies. Bingley:
Emerald.
17. Prakongsai, P., N. Palmer, et al. (2009). "The Implications of benefit package design: the impact on poor Thai
households of excluding renal replacement therapy." Journal of International Development 21(2): 291-308.
18. Sakunphanit, T. and W. Suwanrada (2011). The Universal Coverage Scheme. Sharing Innovative Experiences:
Successful Social Protection Floor Experiences, United Nations Development Programme (UNDP),
International Labour Organization (ILO), United Nations Children’s Fund (UNICEF) and World Health
Organization (WHO). 18.
19. Samnuanklang, M., S. Srithamrongswat, et al. (2011). The Evaluation of Tambon’s Health Promotion Fund,
HISRO.
20. Solar, O. and A. Irwin (2007). "A conceptual framework for action on the social determinants of health."

- Draft Background Paper 10 -
25
21. Somkotra, T. and L. P. Lagrada (2008). "Payments for health care and its effect on catastrophe and
impoverishment: Experience from the transition to universal coverage in Thailand." Social Science & Medicine
67(12): 2027-2035.
22. Srithamrongswat, S. (2010). Funding health promotion and prevention–the Thai experience. Geneva, World
Health Organization.
23. Suksiriserekul, S. (1998) "Reviewing and Brainstorming for Research Topics on Health Insurance Scheme for
the Poor." 86.
24. Tangcharoensathien, V., P. Prakongsai, et al. (2007). "Achieving Universal Coverage in Thailand: What
Lessons Do We Learn?", from http://ssrn.com/paper=1111870.
25. Termpitayapaisit, A. and T. Paem (2009). National Economic and Social Development Plan Bangkok, NESDB.
26. Thammatacharee, J. (2009). Variations in the performance of three public insurance schemes in Thailand,
LSHTM (University of London): 372.
27. Towse, A., A. Mills, et al. (2004). "Learning from Thailand's health reforms." BMJ 328(7431): 103-105.
28. Wasi, P. (2000). "Triangle that moves the mountain" and health systems reform movement in Thailand."
Human Resources Health Develop J 4: 106-10.
29. Wibulpolprasert, S. (2010). Thailand Health Profile 2008-2010, Printing Press, The War Veteran Organization
of Thailand
30. World Health Organization. (2008). Health in Asia and the Pacific. New Delhi, India, World Health
Organization, South-East Asia Region, Western Pacific Region.

- Draft Background Paper 10 -
www.who.int/social_determinants/www.who.int/social_determinants/www.who.int/social_determinants/www.who.int/social_determinants/