Embed Size (px)
Citation preview
1 Health System Design: Blueprint Initiative Phase 2Health System Design: Blueprint Initiative Phase 21
Health System Design:
Blueprint Initiative Phase 2Models of Care updated with Programmatic Refinement Session Updates
September 30, 2009
A Healthier Tomorrow
2 Health System Design: Blueprint Initiative Phase 2
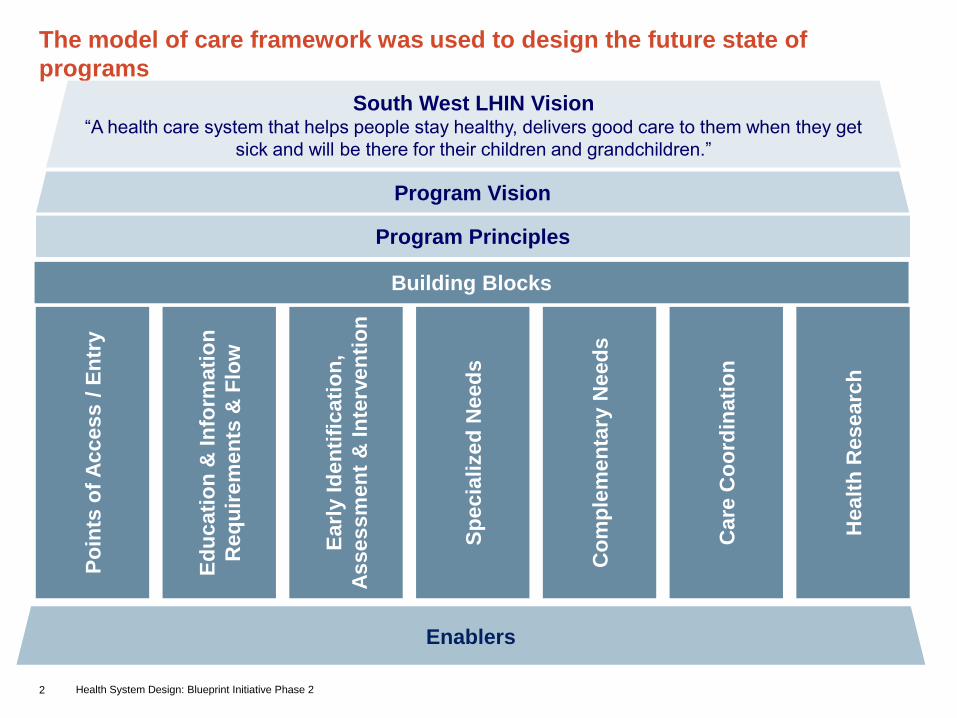
The model of care framework was used to design the future state of
programs
Enablers
South West LHIN Vision “A health care system that helps people stay healthy, delivers good care to them when they get
sick and will be there for their children and grandchildren.”
Program Vision
Program Principles
Building Blocks
Po
ints
of
Access /
En
try
Ed
ucati
on
& I
nfo
rmati
on
Req
uir
em
en
ts &
Flo
w
Earl
y I
den
tifi
cati
on
,
Assessm
en
t &
In
terv
en
tio
n
Sp
ecia
lized
Need
s
Co
mp
lem
en
tary
Need
s
Care
Co
ord
inati
on
Healt
h R
esearc
h

3 Health System Design: Blueprint Initiative Phase 2
ProvincialLHIN-wideSub-LHINLocal
Life Span Lens
The building blocks were further refined when evaluated against the
three “lenses”
Continuum of Care Lens
Service Delivery Lens
“We need to create a simple
path for people to navigate
through the health care system
throughout their life.”
Symposium Participant

4 Health System Design: Blueprint Initiative Phase 2
Models of Care
5 Health System Design: Blueprint Initiative Phase 2
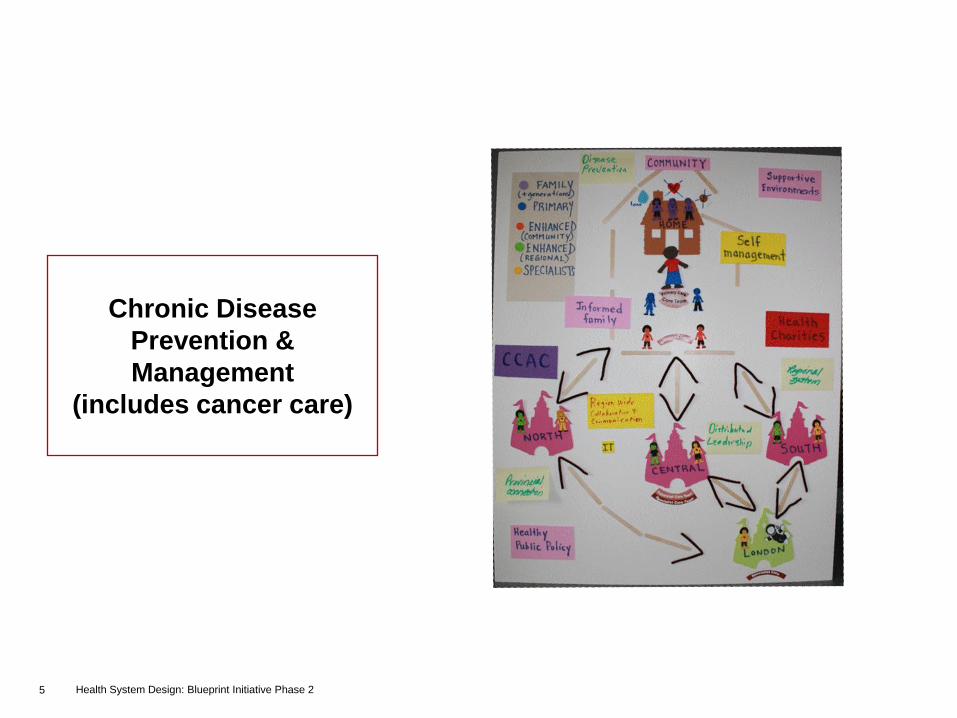
Chronic Disease
Prevention &
Management
(includes cancer care)

6 Health System Design: Blueprint Initiative Phase 2
The model of care has been developed upon the guiding vision
elements and principles
Vision
Elements
• Empower / Involve Individuals
• Broad Partner Spectrum
• Quality of Life and Health Status
• Collaboration
• “A Person‟s Perspective” – healthy people managing their disease who know where to get the help they need to manage their disease
• Delivering value
• Shared committment to screening and early identification
Principles
• Person-Centred: The holistic health needs of the individual and the caregiver/support network through their life journey should be the focus for our integrated system of care, including LHIN-funded and non-LHIN funded services. Integrated system of care should include LHIN-funded and non-LHIN funded services which involves and empowers the individual
• Interdisciplinary: A shared model of care will be provided by an interdisciplinary team. Promote and facilitate interdisciplinary teamwork in the area of chronic disease through strengthened communication. Ensuring access to the most appropriate health care providers available (i.e. NP, SW, etc.) Chronic disease prevention and management teams are responsive to the needs of the local communities.
• Self-Management: The person and family members/caregivers afflicted with a chronic disease manages his/her condition(s) in partnership with an interdisciplinary team. Level of self-management is customized upon the individual‟s capacity.
• Accessible: The model aims to provide comprehensive, integrated, and coordinated CDPM services throughout the LHIN regardless of personal barriers to care (i.e. without a physician, social determinants of health, geographic limitation)
• Evidence-based: Increase individual, as well as health care provider knowledge of and adherence to current evidence-based clinical practice guidelines and standards of care for CDPM.
• Provides Equitable and Consistent Quality of Care: People with a chronic disease in our LHIN should received consistent quality of care services based on evidence
• Cultural Safety: Service will be delivered with cultural and linguistic competency, sensitivity, and compassion to other circumstances that affect individuals and families. “Call to Caring”
• Outcome Oriented: Services are focused to be delivered holistically and drive person-experience outcomes. Measure and report chronic disease performance measure at the individual patient, health professional, and LHIN-level
• Knowledge Transfer: Spread and share innovations in delivery of disease-specific care with health providers across the LHINs, individuals/families, and globally.
• Sustainability and Accountability: Leverage existing resources (using scarce resources wisely), infrastructure, and knowledge.
• Scalable: This model is a foundation that can be leveraged to multiple chronic diseases based on infrastructure and modifiable risk factors.

7 Health System Design: Blueprint Initiative Phase 2
Providers
• Increased focus on
preventing chronic
illnesses within a
local capacity
• Availability of
standardized tools
to aid health care
professionals in
care delivery
• Improved
satisfaction of
providers
• Strengthened relationship between health
care providers across the continuum of care
and service delivery model
• Inter-professional teams that are linked to
individual practitioners at a local level. They
will serve as a vehicle to care delivery
• Enhanced reliance on self-management
across the continuum – involving individual
as part of health care team
• Standardized, consistent approach to care
provision
• Health care providers to evaluate, identify,
and manage entire suite of chronic illnesses
• Focus on marginalized population (cultural,
etc)
Model of care focuses on keeping care close to home through
sufficient local capacity, effective partnerships across health/non-
health organizations, and self-management
How is this model different from
today’s service delivery model?
What are the benefits of the
Model of Care?
Individuals/ Families
• Empowerment of
individual/family
members in
managing their own
care
• Emphasis on
providing care
closer to home
• Improved person
satisfaction
• Improved clinical
outcomes

8 Health System Design: Blueprint Initiative Phase 2
Overview of Chronic Disease Prevention & Management Model
Pri
ma
ry C
are
–L
oc
al D
eli
ve
ry
En
han
ced
Care
–
Su
b-L
HIN
De
live
ry
Sp
ec
iali
st
Ca
re –
LH
IN-w
ide d
eli
ve
ry
• Individuals/ families will access
services through local resources or
self referral
• Local resources comprised of various
disciplines will be able to cross-refer
individuals/families to inter-
professional health programs as
needed
GPS
GPS
GPS
GPS
• Sub-LHIN organizations provide
enhanced care, managing
specialized needs
• The integrated care plan will evolve
as health needs are evaluated
• If individual requires complex,
specialized care, he/she will be
referred to sub-LHIN and LHIN
centres
• HHR will educate person and
conduct an integrated, holistic
assessment providing primary care
and targeted enhanced care
services
• If further specialization is required,
will refer to sub-LHIN organizations
Self-Management
GPSGuided Practical Solutions
1
1 2 3
3
2
4
4
Interdisciplinary
health programs
9 Health System Design: Blueprint Initiative Phase 2
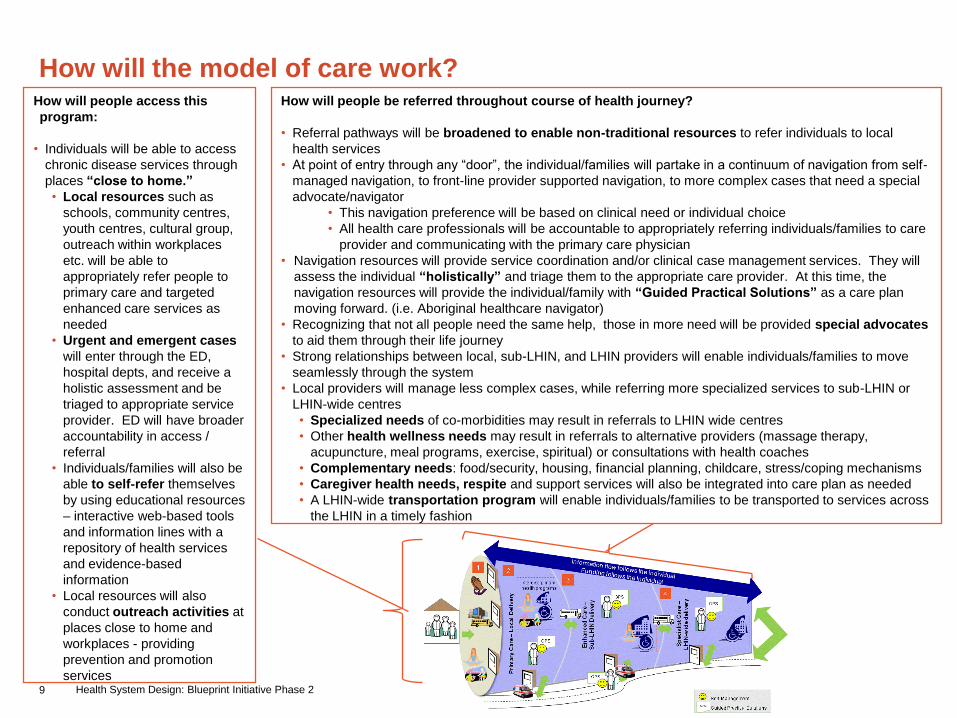
How will the model of care work?How will people access this
program:
• Individuals will be able to access
chronic disease services through
places “close to home.”
• Local resources such as
schools, community centres,
youth centres, cultural group,
outreach within workplaces
etc. will be able to
appropriately refer people to
primary care and targeted
enhanced care services as
needed
• Urgent and emergent cases
will enter through the ED,
hospital depts, and receive a
holistic assessment and be
triaged to appropriate service
provider. ED will have broader
accountability in access /
referral
• Individuals/families will also be
able to self-refer themselves
by using educational resources
– interactive web-based tools
and information lines with a
repository of health services
and evidence-based
information
• Local resources will also
conduct outreach activities at
places close to home and
workplaces - providing
prevention and promotion
services
How will people be referred throughout course of health journey?
• Referral pathways will be broadened to enable non-traditional resources to refer individuals to local
health services
• At point of entry through any “door”, the individual/families will partake in a continuum of navigation from self-
managed navigation, to front-line provider supported navigation, to more complex cases that need a special
advocate/navigator
• This navigation preference will be based on clinical need or individual choice
• All health care professionals will be accountable to appropriately referring individuals/families to care
provider and communicating with the primary care physician
• Navigation resources will provide service coordination and/or clinical case management services. They will
assess the individual “holistically” and triage them to the appropriate care provider. At this time, the
navigation resources will provide the individual/family with “Guided Practical Solutions” as a care plan
moving forward. (i.e. Aboriginal healthcare navigator)
• Recognizing that not all people need the same help, those in more need will be provided special advocates
to aid them through their life journey
• Strong relationships between local, sub-LHIN, and LHIN providers will enable individuals/families to move
seamlessly through the system
• Local providers will manage less complex cases, while referring more specialized services to sub-LHIN or
LHIN-wide centres
• Specialized needs of co-morbidities may result in referrals to LHIN wide centres
• Other health wellness needs may result in referrals to alternative providers (massage therapy,
acupuncture, meal programs, exercise, spiritual) or consultations with health coaches
• Complementary needs: food/security, housing, financial planning, childcare, stress/coping mechanisms
• Caregiver health needs, respite and support services will also be integrated into care plan as needed
• A LHIN-wide transportation program will enable individuals/families to be transported to services across
the LHIN in a timely fashion

10 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
How will the system stay connected to the individuals/families?
•As needed, navigation resources or HHR will step up to provide service coordination
and/or clinical case management services. Clinical resources will be equipped with
the right skill sets and tools to provide clinical case management.
•Throughout the time in the system, HHR will be kept up to date on the individual's
GPS and health status. As it evolves through the journey of the individual,
navigators/ advocates will be informed.
• Health information will be shared across sectors through an EHR/personal
health record
•HHR will stay be attuned to the individuals needs as they go through life stages and
health statuses. Advanced care planning to proactively prepare for long term care
services that may be needed (i.e. end-of-life care)
•Certain individuals will be provided health coaches to provide mentorship in staying
healthy
•Individuals will also be able to access lay coaches for support (people from the
community who are equipped with information and prepped to support
individuals/families)
How will individuals be assessed and treated?
•Local resources will function more as inter-professional
teams. This will enable them to provide integrated
assessments on the individual across entire suite of
chronic diseases
•Based upon health care needs of the individual, different
disciplines will be able to cross-refer to other providers
as appropriate
•Throughout health assessments/treatments, the health
care professional will emphasize self-management and
accountability as a necessary step to taking control of
one‟s own health
• Tactics such as motivational interviewing will
provide a „positive‟ assessment of the individual‟s
health

11 Health System Design: Blueprint Initiative Phase 2
How will information be communicated?
•Information flow will follow the individual through their health journey.
This will occur through a real-time, easily accessible electronic
health record (EHR) available to health providers across the
continuum of care and geographic location
•The EHR will be connected to a personal health portal which will
enable individuals to access and share health information as needed
(i.e. with alternative care providers) – keep track of their GPS
•Health information will consist of standard guidelines which are
evidence-based and span the continuum of care and life span
•Health care professionals will be equipped with tools such as
“information sheets” and inventory of services to enable care
coordination across organizations
How will the model of care work? (cont’d)
How will funding be coordinated across sectors?
•Funding will follow the individual – be directed to providers who
bear burden of delivering care
•Collaboration across ministries so that funding is seamless to
the individual/family
•LHIN will manage priorities and implementation to control
funding across sectors
•Change in fee structures to accommodate CDPM approach
•Flexible funding model to enable individuals to manage their
own care delivery
•Innovative healthcare solutions: Platform to discuss successes
and failures in field and also provide funding for healthcare
innovations
12 Health System Design: Blueprint Initiative Phase 2
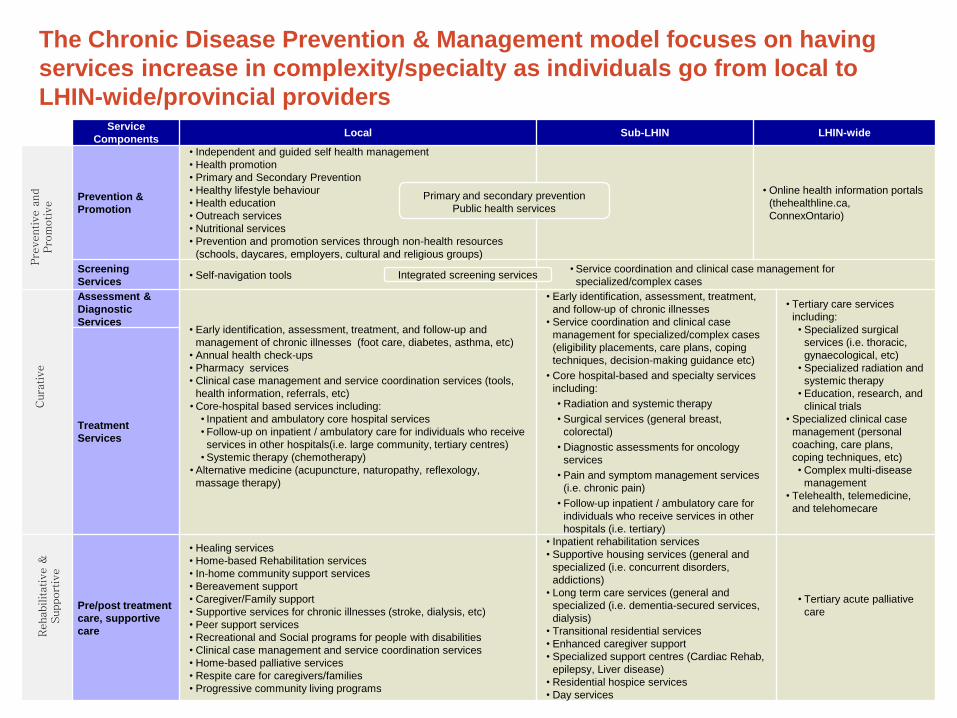
The Chronic Disease Prevention & Management model focuses on having
services increase in complexity/specialty as individuals go from local to
LHIN-wide/provincial providersService
ComponentsLocal Sub-LHIN LHIN-wide
Prevention &
Promotion
• Independent and guided self health management
• Health promotion
• Primary and Secondary Prevention
• Healthy lifestyle behaviour
• Health education
• Outreach services
• Nutritional services
• Prevention and promotion services through non-health resources
(schools, daycares, employers, cultural and religious groups)
• Online health information portals
(thehealthline.ca,
ConnexOntario)
Screening
Services• Self-navigation tools
• Service coordination and clinical case management for
specialized/complex cases
Assessment &
Diagnostic
Services• Early identification, assessment, treatment, and follow-up and
management of chronic illnesses (foot care, diabetes, asthma, etc)
• Annual health check-ups
• Pharmacy services
• Clinical case management and service coordination services (tools,
health information, referrals, etc)
• Core-hospital based services including:
• Inpatient and ambulatory core hospital services
• Follow-up on inpatient / ambulatory care for individuals who receive
services in other hospitals(i.e. large community, tertiary centres)
• Systemic therapy (chemotherapy)
• Alternative medicine (acupuncture, naturopathy, reflexology,
massage therapy)
• Early identification, assessment, treatment,
and follow-up of chronic illnesses
• Service coordination and clinical case
management for specialized/complex cases
(eligibility placements, care plans, coping
techniques, decision-making guidance etc)
• Core hospital-based and specialty services
including:
• Radiation and systemic therapy
• Surgical services (general breast,
colorectal)
• Diagnostic assessments for oncology
services
• Pain and symptom management services
(i.e. chronic pain)
• Follow-up inpatient / ambulatory care for
individuals who receive services in other
hospitals (i.e. tertiary)
• Tertiary care services
including:
• Specialized surgical
services (i.e. thoracic,
gynaecological, etc)
• Specialized radiation and
systemic therapy
• Education, research, and
clinical trials
• Specialized clinical case
management (personal
coaching, care plans,
coping techniques, etc)
• Complex multi-disease
management
• Telehealth, telemedicine,
and telehomecare
Treatment
Services
Pre/post treatment
care, supportive
care
• Healing services
• Home-based Rehabilitation services
• In-home community support services
• Bereavement support
• Caregiver/Family support
• Supportive services for chronic illnesses (stroke, dialysis, etc)
• Peer support services
• Recreational and Social programs for people with disabilities
• Clinical case management and service coordination services
• Home-based palliative services
• Respite care for caregivers/families
• Progressive community living programs
• Inpatient rehabilitation services
• Supportive housing services (general and
specialized (i.e. concurrent disorders,
addictions)
• Long term care services (general and
specialized (i.e. dementia-secured services,
dialysis)
• Transitional residential services
• Enhanced caregiver support
• Specialized support centres (Cardiac Rehab,
epilepsy, Liver disease)
• Residential hospice services
• Day services
• Tertiary acute palliative
care
Cura
tive
Rehabilitative &
Support
ive
Pre
ventive a
nd
Pro
motive
Primary and secondary prevention
Public health services
Integrated screening services
13 Health System Design: Blueprint Initiative Phase 2
Implications of Chronic Disease Prevention & Management model of
care
• Enabling “true self-
management”, will require
individuals to have easy
access to evidence-based
health information and
inventory of health services
• Developing effective
working relationships with
health care professionals
and navigators/advocates
• Seamless referral system and development of integrated care plans, Guided
Practical Solutions, will require stronger relationships among stakeholders
across health and social agencies
• Accountability for all providers in taking necessary education/communication
steps to refer individuals/families to appropriate provider
• Development of relationships with health/non-health providers outside of
traditional care settings – leveraging the “Partnerships for Health” initiative
• Shift to local resources will require increased capacity of front-line resources
within community with regards to:
• Knowledge and understanding of all health services across the
continuum
• Understanding of person‟s health care history and social considerations
• Consistent interpretation and application of privacy laws to enable information
sharing across health sectors, social agencies, alternative care providers, and
ministries (regulated and non-regulated health professionals)
• Changes in funding model will require enhanced collaboration between
ministries and empowerment of LHIN to manage health priorities
• Changes in hospital budgeting to accommodate the future state of healthcare
delivery
• Accountability agreements across health care providers to ensure
collaboration and shared flow of funds towards healthcare initiatives
Health Care Professionals Individuals/Families

14 Health System Design: Blueprint Initiative Phase 2
Mental Health &
Addictions

15 Health System Design: Blueprint Initiative Phase 2
The model of care has been developed upon the guiding vision
elements and principles
Vision
Elements
• Person-directed
• Equitable and timely access
• Empowerment and support (all providers, individuals, families, caregivers)
• Culturally sensitive and appropriate
• Inclusion and acknowledgement of other bodies of knowledge and experience
• Holistic
• Continuous research and innovation to drive practice and standards of care
• Ability to respond to people‟s needs throughout one‟s life span
• Social inclusion of individuals with mental health and addictions issues
• Eradication of discrimination towards individuals with mental health and addictions issues
Principles
• Shared care philosophy
• Partnerships with Primary Care
• Recovery-oriented
• Empowerment through education (provider, individual, family)
• Keep it simple
• Keep it local
• Person/family focus – people are assets
• Population oriented
• Evidence based practice
• Innovation and integration
• Sustainability
• Partnerships
• Flexible/responsive
• Comprehensiveness

16 Health System Design: Blueprint Initiative Phase 2
• Increase timely access through multiple entry
points “any door is the right door”
• Expand focus to prevention and early
identification in alignment with provincial mandate
• Equips the system with resources to provide
increased support for those individuals with mild
to moderate mental health and addictions
challenges
• Development of collaborative partnerships across
health sectors and continuum of care
• Implementation of “Most Responsible Provider”
for individuals with complex needs (include
navigation and clinical case management)
• Promote and expand capabilities of current
platforms to provide a “health information bank”
for individuals/families/ caregivers and local
health resources (i.e. ConnexOntario)
• Standardized, consistent approach to care
provision
Through shared care and collaborative partnerships across health
and non-health entities, the model of care facilitates coordinated
access for individuals / families affected by any degree of mental
illness or addictionHow is this model different from
today’s service delivery model?
Providers
• Involved care
management of
individuals with
complex needs
• Seamless referral
of individuals /
families across
health and other
sectors
What are the benefits of the
Model of Care?
Individuals/ Families
• Empowerment of
individual/family
members in
managing their own
care – Individual is
part of health team
• Emphasis on
providing care
closer to home
• Early identification
and management of
individual‟s needs in
order to enable
people to optimize
their level of
function and quality
of life in their
community and
home environment
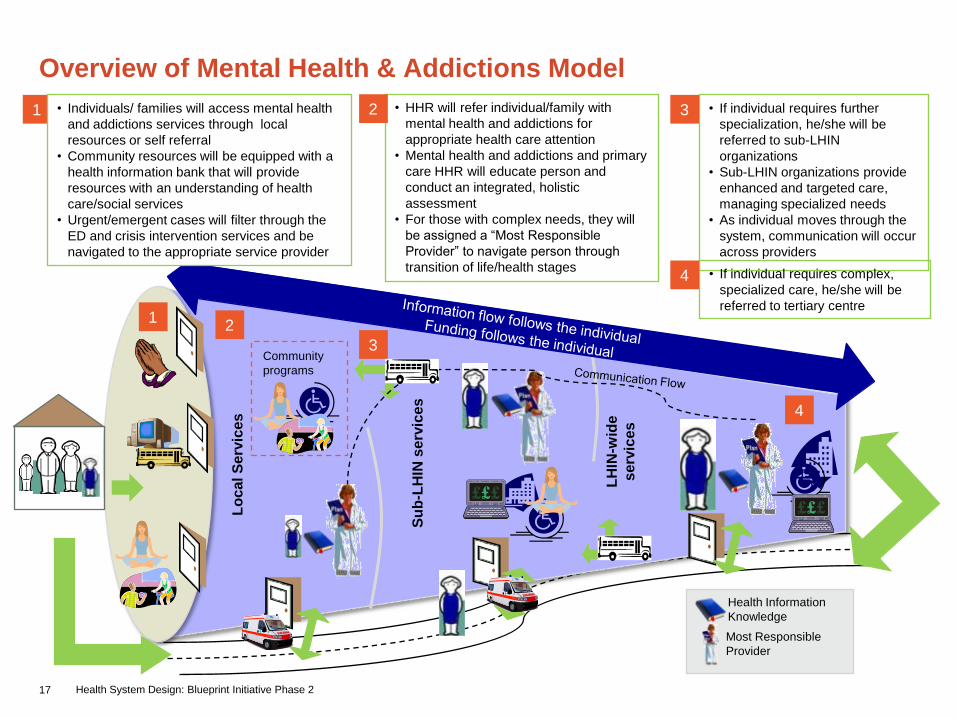
17 Health System Design: Blueprint Initiative Phase 2
Overview of Mental Health & Addictions Model
Lo
cal S
erv
ices
Su
b-L
HIN
se
rvic
es
LH
IN-w
ide
serv
ices
• If individual requires further
specialization, he/she will be
referred to sub-LHIN
organizations
• Sub-LHIN organizations provide
enhanced and targeted care,
managing specialized needs
• As individual moves through the
system, communication will occur
across providers
• If individual requires complex,
specialized care, he/she will be
referred to tertiary centre
• HHR will refer individual/family with
mental health and addictions for
appropriate health care attention
• Mental health and addictions and primary
care HHR will educate person and
conduct an integrated, holistic
assessment
• For those with complex needs, they will
be assigned a “Most Responsible
Provider” to navigate person through
transition of life/health stages
Health Information
Knowledge
1
1
3
2
4
4
Community
programs
Most Responsible
Provider
3• Individuals/ families will access mental health
and addictions services through local
resources or self referral
• Community resources will be equipped with a
health information bank that will provide
resources with an understanding of health
care/social services
• Urgent/emergent cases will filter through the
ED and crisis intervention services and be
navigated to the appropriate service provider
2
18 Health System Design: Blueprint Initiative Phase 2
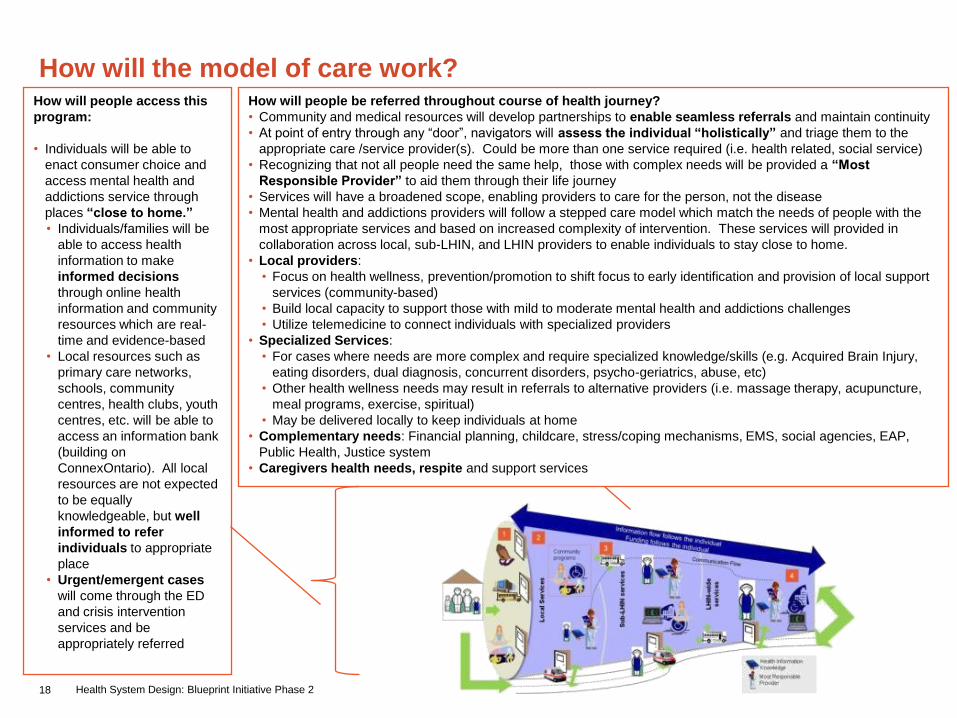
How will the model of care work?How will people access this
program:
• Individuals will be able to
enact consumer choice and
access mental health and
addictions service through
places “close to home.”
• Individuals/families will be
able to access health
information to make
informed decisions
through online health
information and community
resources which are real-
time and evidence-based
• Local resources such as
primary care networks,
schools, community
centres, health clubs, youth
centres, etc. will be able to
access an information bank
(building on
ConnexOntario). All local
resources are not expected
to be equally
knowledgeable, but well
informed to refer
individuals to appropriate
place
• Urgent/emergent cases
will come through the ED
and crisis intervention
services and be
appropriately referred
How will people be referred throughout course of health journey?
• Community and medical resources will develop partnerships to enable seamless referrals and maintain continuity
• At point of entry through any “door”, navigators will assess the individual “holistically” and triage them to the
appropriate care /service provider(s). Could be more than one service required (i.e. health related, social service)
• Recognizing that not all people need the same help, those with complex needs will be provided a “Most
Responsible Provider” to aid them through their life journey
• Services will have a broadened scope, enabling providers to care for the person, not the disease
• Mental health and addictions providers will follow a stepped care model which match the needs of people with the
most appropriate services and based on increased complexity of intervention. These services will provided in
collaboration across local, sub-LHIN, and LHIN providers to enable individuals to stay close to home.
• Local providers:
• Focus on health wellness, prevention/promotion to shift focus to early identification and provision of local support
services (community-based)
• Build local capacity to support those with mild to moderate mental health and addictions challenges
• Utilize telemedicine to connect individuals with specialized providers
• Specialized Services:
• For cases where needs are more complex and require specialized knowledge/skills (e.g. Acquired Brain Injury,
eating disorders, dual diagnosis, concurrent disorders, psycho-geriatrics, abuse, etc)
• Other health wellness needs may result in referrals to alternative providers (i.e. massage therapy, acupuncture,
meal programs, exercise, spiritual)
• May be delivered locally to keep individuals at home
• Complementary needs: Financial planning, childcare, stress/coping mechanisms, EMS, social agencies, EAP,
Public Health, Justice system
• Caregivers health needs, respite and support services

19 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
How will the system stay connected to the
individuals/families?
• Throughout the time in the system, HHR will be able to
keep atop of the individual‟s health status through
access to:
• EHR/personal health record shared across sectors
• Individuals/families will be equipped with care
coordination (navigation and clinical case
management) services to best match their needs.
• Individuals with complex needs will be connected with a
“Most Responsible Provider” to provide close contact
throughout the health care system
• These resources will help transition individuals
through life and health stages by staying attuned with
their health needs and building a relationship with
their families throughout their journey. (i.e.
knowledge transfer)
• System will provide enhanced peer support models to
support clients and families dealing with mental illnesses
and addictions as needed
How will individuals be assessed and treated?
• Local resources (i.e. Primary care, pastoral, teachers, etc) will play a key role in
referring individuals to mental health and addictions providers „help get
individuals/families where they need to be‟
• HHR will holistically assess and create treatment plans that place a strong
emphasis on accountability
• Health care professionals will assess individual for not only mental health and
addictions, but other chronic illnesses and complementary needs
• They will provide screening, early identification, assessment, treatment, and
follow-up services
• The converse will also be true – providers caring for individuals whose primary
reason for care is that of a physical condition, will also be better educated and
cognizant of key signs/symptoms related to potential mental health and
addictions related issues
• Throughout health assessments/treatments, the health care professional will
emphasize self-management as a necessary step to taking control of one‟s
own health
• Resources will be equipped with simple, straightforward tools which will be
reliant on local requirements such as case mix, urban vs. rural, etc
• HHR will conduct outreach activities for early intervention of specialized needs
20 Health System Design: Blueprint Initiative Phase 2
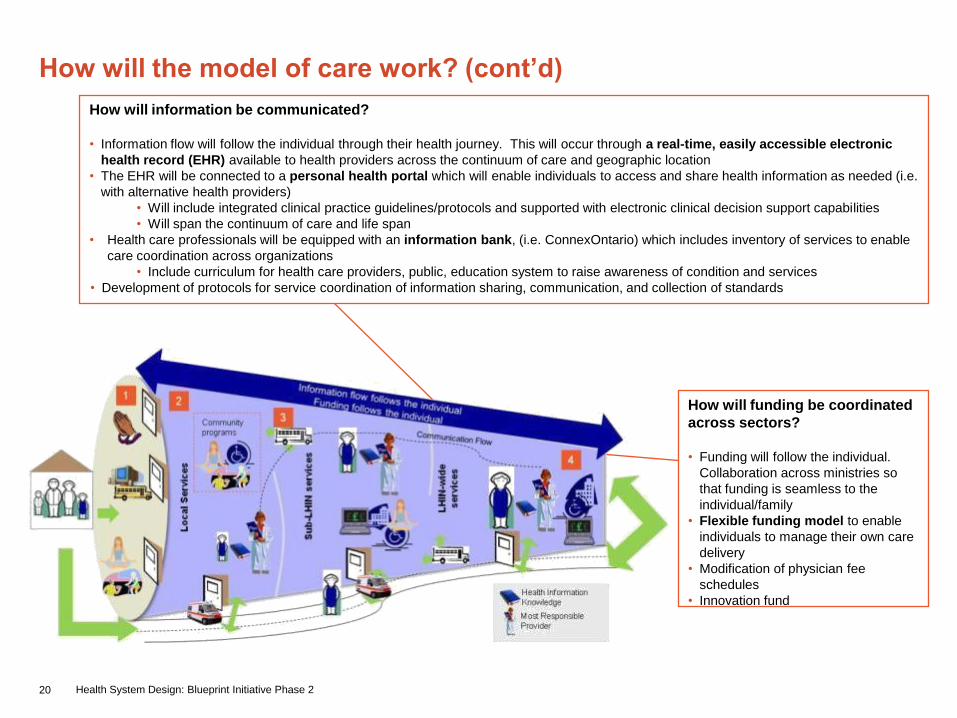
How will information be communicated?
• Information flow will follow the individual through their health journey. This will occur through a real-time, easily accessible electronic
health record (EHR) available to health providers across the continuum of care and geographic location
• The EHR will be connected to a personal health portal which will enable individuals to access and share health information as needed (i.e.
with alternative health providers)
• Will include integrated clinical practice guidelines/protocols and supported with electronic clinical decision support capabilities
• Will span the continuum of care and life span
• Health care professionals will be equipped with an information bank, (i.e. ConnexOntario) which includes inventory of services to enable
care coordination across organizations
• Include curriculum for health care providers, public, education system to raise awareness of condition and services
• Development of protocols for service coordination of information sharing, communication, and collection of standards
How will the model of care work? (cont’d)
How will funding be coordinated
across sectors?
• Funding will follow the individual.
Collaboration across ministries so
that funding is seamless to the
individual/family
• Flexible funding model to enable
individuals to manage their own care
delivery
• Modification of physician fee
schedules
• Innovation fund

21 Health System Design: Blueprint Initiative Phase 2
Implications of Mental Health and Addictions model of care
• Enabling “true self-management”, will require
individuals to have easy access to evidence-
based health information and inventory of
health services
• Developing effective working relationships
with health care professionals and
navigators/advocates
• Shift to local resources will require increased capacity of front-line resources
within community with regards to:
• Knowledge and understanding of all health services across the
continuum
• Understanding of person‟s health care history and social considerations
• Care and management of individuals with mild to moderate conditions
and their families
• Defined roles and responsibilities of HHR providing mental health and addictions
services through a stepped care model. Identification of who is responsible for
care, what is the focus, and what they do (www.nice.org.uk)
• Health care professionals need more education, resources, understanding
(attitudinal change), and skill development to appropriately provide services
through the transition period from youth to adults to seniors.
• Develop trust and accountability with partners beyond traditional boundaries (i.e.
health and non-health)
• Increased need for infrastructure (i.e. transportation, e-health) to enable
collaboration across health sectors
• Consistent interpretation and application of privacy laws to enable information
sharing across health sectors, social agencies, alternative care providers, and
ministries
• Changes in funding model will require enhanced collaboration between
ministries and empowerment of LHIN to manage health priorities
• Increase in service capacity to effectively manage mental health and addictions
services (supportive housing, peer support groups, psychiatrists, problem
gambling, etc)
Providers Individuals/Families

22 Health System Design: Blueprint Initiative Phase 2
The Mental Health and Addictions model focuses on having services
increase in complexity/speciality as individuals/families go from local to
LHIN-wide providersService
ComponentsLocal Sub-LHIN LHIN-wide
Prevention &
Promotion
• Independent and guided self health management
• Health promotion
• Healthy lifestyle behaviour
• Health education
• Outreach services (i.e. mobile)
• Nutritional services
• Online health
information portals
(ConnexOntario)
• Antistigma/discriminatio
n reduction
Screening
Services
• Universal, standardized screening for all mental health and
addictions illnesses
• Self-navigation tools
• Specialized screening services for mental health
and addictions
Assessment &
Diagnostic
Services
• Early identification, assessment, treatment, follow-up and
management of mental health and addictions services
• Life skills training
• Psychotherapy
• Clinical case management and service coordination services (tools,
health information, referrals, etc)
• Core-hospital based services including:
• Acute mental health and addictions services, eating disorders
• Follow-up on inpatient / ambulatory care for individuals who
receive services in other hospitals(i.e. large community, tertiary
centres)
• Pharmacy services
• Alternative medicine (acupuncture, naturopathy, reflexology,
massage therapy)
• Early identification, assessment, treatment, follow-up
and management of mental health and addictions
services
• Primary health care services (concurrent disorders,
dual diagnosis, psychogeriatrics)
• Service coordination and clinical case management
for specialized/complex cases (eligibility placements,
care plans, coping techniques, decision-making
guidance etc)
• Crisis intervention services
• Core hospital-based and specialty services
including:
• Psychogeriatrics, acute mental health and
addictions services, eating disorders, schedule 1
inpatient beds including additional beds for
paediatric services
• Follow-up inpatient / ambulatory care for
individuals who receive services in other hospitals
(i.e. tertiary)
• Psychiatric assessment and intervention
• Tertiary care /
psychiatric hospitals
services including:
• Paediatric mental
health and
addictions services,
forensic psychiatry,
24/7 residential
addictions treatment
programs, ABI
• Education, research,
and clinical trials
• Specialized clinical
case management
(personal coaching,
care plans, coping
techniques, intensive
case management ,etc)
• Telehealth,
telemedicine, and
telehomecare
Treatment
Services
Pre/post
treatment care,
supportive care
• Consumer / family initiatives
• Social rehabilitation and recreation services
• Caregiver education
• Healing services
• Home-based Rehabilitation services
• Caregiver/Family support
• Peer support services
• Service coordination services
• Respite care for caregivers/families
• Community withdrawal management
• Inpatient rehabilitation services
• Supportive housing services (concurrent disorders,
addiction, etc)
• Long term care services (i.e. dementia-secured
units)
• Transitional residential services
• Enhanced caregiver support
• Residential hospice services
• Day program services
Cura
tive
Rehabilitative &
Support
ive
Pre
ventive a
nd
Pro
motive Primary and secondary prevention
Public health services
• Community mental health and addictions services:
• Mental health and addictions counselling services
• Primary health care services for mental health and
addictions
• Mental health and addictions case management
• Crisis intervention services
• Problem gambling
• Community substance withdrawal management services
23 Health System Design: Blueprint Initiative Phase 2
Women’s Health &
Paediatric Services
Women‟s Health & Paediatrics
model of care refers to the delivery of
services to child-bearing women and
children. Other women health needs
will be addressed in other models.

24 Health System Design: Blueprint Initiative Phase 2
The model of care has been developed upon the guiding vision
elements and principles
Vision
Elements
Population served: Women; Infants; children and youth
Elements:
• Family/client centered care
• Accessible/ease of navigation
• „Wholistic‟
• Provide evidence informed quality of care
• Maintain transparency and accountability
• Strength/capacity based (individual)
• Culturally appropriate/competent
• Integrated care delivery
Principles
• Collaborative across the LHIN and ministries and agencies outside of health
• Sharing resources
• Engages clients and promotes ability and self-management/fostering resiliency
• Timely access
• Fosters a safe environment
• Considers the individual in context of family and community
• Supports life transitions
• Developmentally appropriate
• Continuous coordinated care
• Create and maintain efficiency and effectiveness
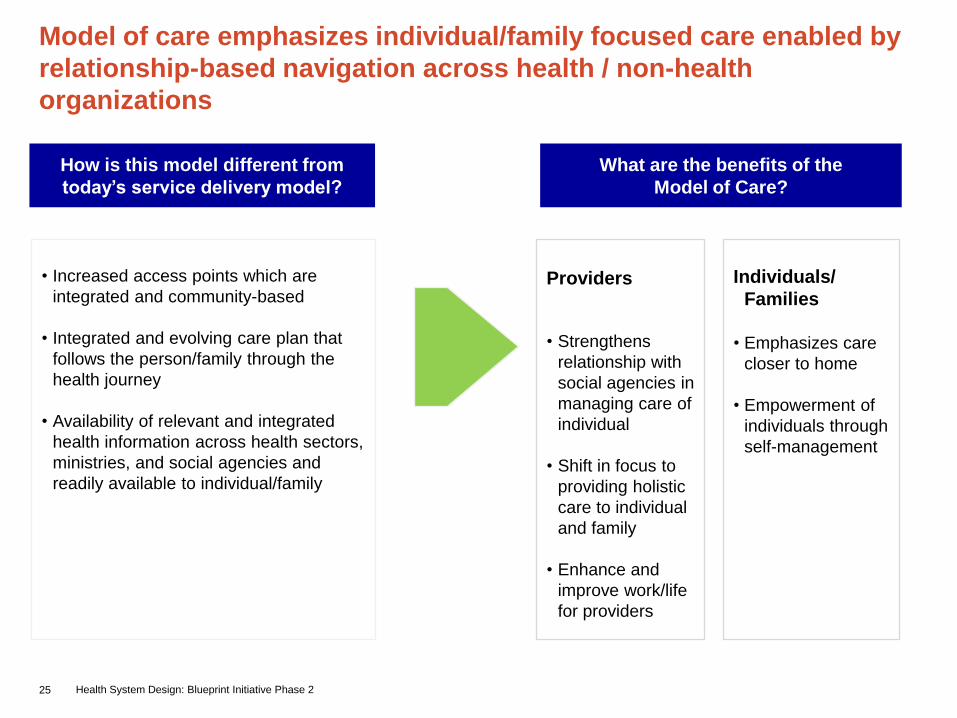
25 Health System Design: Blueprint Initiative Phase 2
• Increased access points which are
integrated and community-based
• Integrated and evolving care plan that
follows the person/family through the
health journey
• Availability of relevant and integrated
health information across health sectors,
ministries, and social agencies and
readily available to individual/family
Model of care emphasizes individual/family focused care enabled by
relationship-based navigation across health / non-health
organizations
How is this model different from
today’s service delivery model?
Providers
• Strengthens
relationship with
social agencies in
managing care of
individual
• Shift in focus to
providing holistic
care to individual
and family
• Enhance and
improve work/life
for providers
What are the benefits of the
Model of Care?
Individuals/
Families
• Emphasizes care
closer to home
• Empowerment of
individuals through
self-management

26 Health System Design: Blueprint Initiative Phase 2
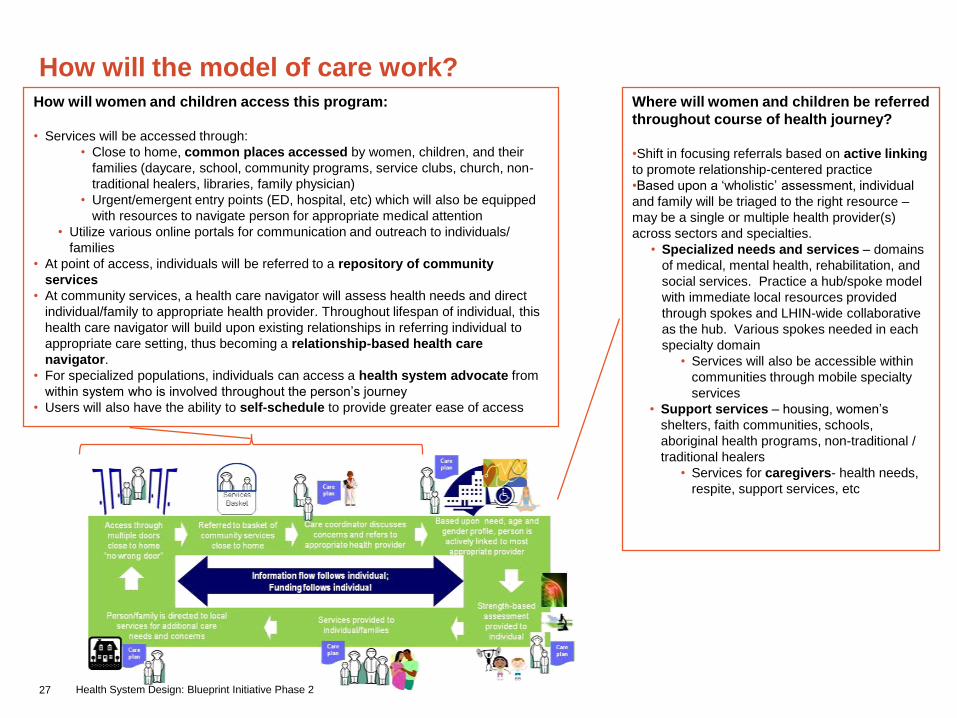
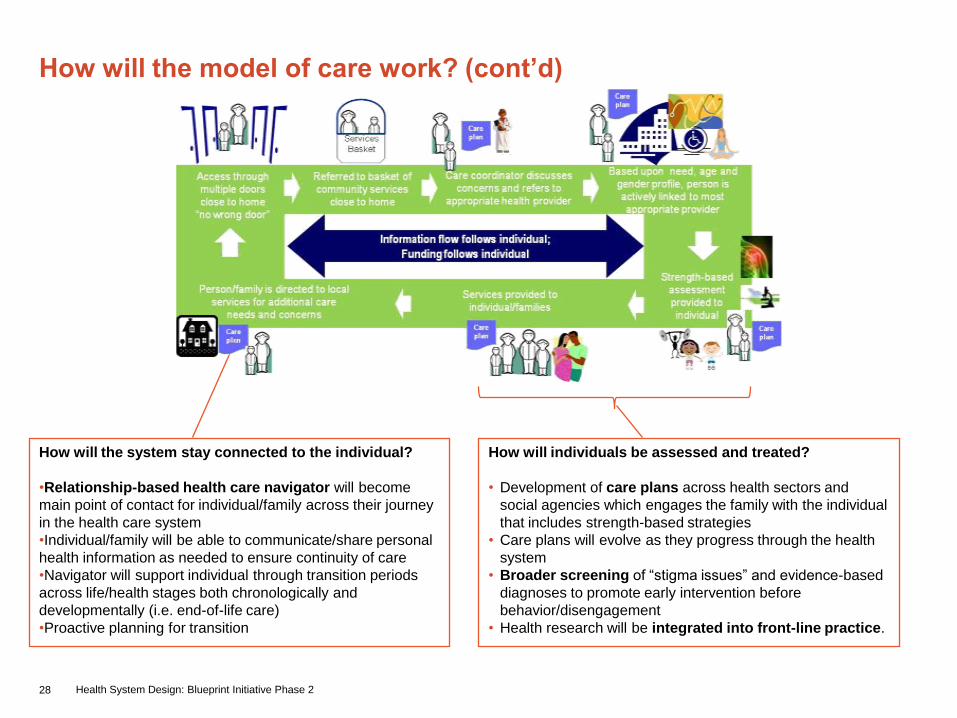
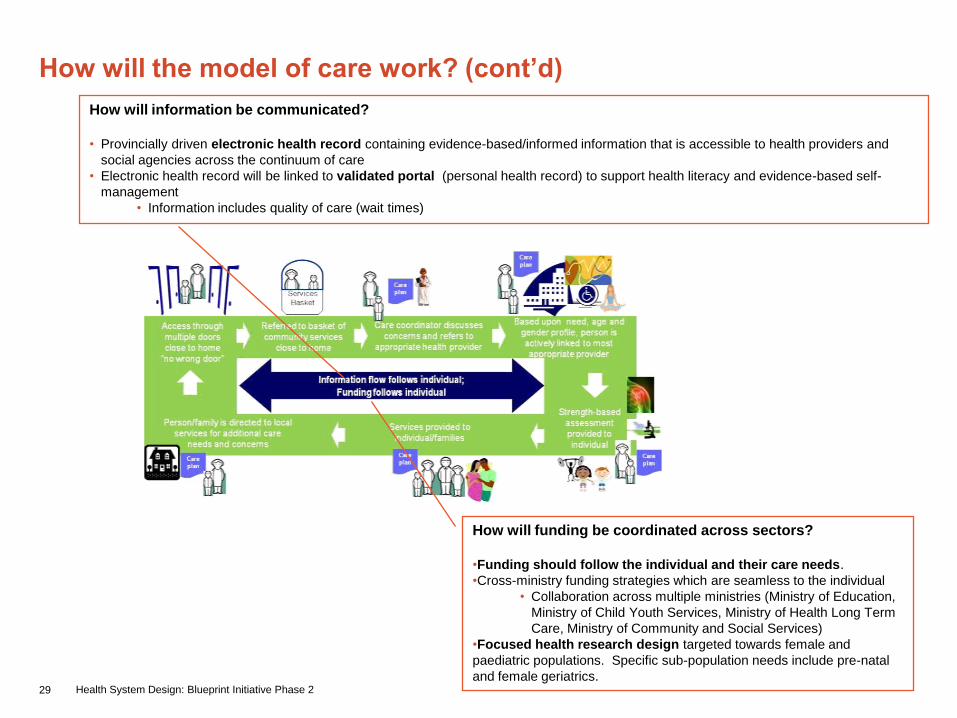
Overview of Women’s Health & Paediatrics model of care
Access through
multiple doors
(e.g. primary care)
close to home
“no wrong door”
Referred to basket of
community services
close to home
Care coordinator discusses
concerns and refers to
appropriate health provider
Based upon need, age and
gender profile, person is
actively linked to most
appropriate provider
Strength-based
assessment
provided to
individual
Services provided to
individual/families
Information flow follows individual;
Funding follows individual
Person/family is directed to local
services for additional care
needs and concerns
Care
plan
Care
plan
Care
plan
Care
planCare
plan
Services
Basket
The following figure reflects an individuals‟ ongoing interaction within the model over the course of their
lifespan. Further details explaining each element are available in subsequent slides.
27 Health System Design: Blueprint Initiative Phase 2
How will the model of care work?How will women and children access this program:
• Services will be accessed through:
• Close to home, common places accessed by women, children, and their
families (daycare, school, community programs, service clubs, church, non-
traditional healers, libraries, family physician)
• Urgent/emergent entry points (ED, hospital, etc) which will also be equipped
with resources to navigate person for appropriate medical attention
• Utilize various online portals for communication and outreach to individuals/
families
• At point of access, individuals will be referred to a repository of community
services
• At community services, a health care navigator will assess health needs and direct
individual/family to appropriate health provider. Throughout lifespan of individual, this
health care navigator will build upon existing relationships in referring individual to
appropriate care setting, thus becoming a relationship-based health care
navigator.
• For specialized populations, individuals can access a health system advocate from
within system who is involved throughout the person‟s journey
• Users will also have the ability to self-schedule to provide greater ease of access
Where will women and children be referred
throughout course of health journey?
•Shift in focusing referrals based on active linking
to promote relationship-centered practice
•Based upon a „wholistic‟ assessment, individual
and family will be triaged to the right resource –
may be a single or multiple health provider(s)
across sectors and specialties.
• Specialized needs and services – domains
of medical, mental health, rehabilitation, and
social services. Practice a hub/spoke model
with immediate local resources provided
through spokes and LHIN-wide collaborative
as the hub. Various spokes needed in each
specialty domain
• Services will also be accessible within
communities through mobile specialty
services
• Support services – housing, women‟s
shelters, faith communities, schools,
aboriginal health programs, non-traditional /
traditional healers
• Services for caregivers- health needs,
respite, support services, etc
28 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
How will individuals be assessed and treated?
• Development of care plans across health sectors and
social agencies which engages the family with the individual
that includes strength-based strategies
• Care plans will evolve as they progress through the health
system
• Broader screening of “stigma issues” and evidence-based
diagnoses to promote early intervention before
behavior/disengagement
• Health research will be integrated into front-line practice.
How will the system stay connected to the individual?
•Relationship-based health care navigator will become
main point of contact for individual/family across their journey
in the health care system
•Individual/family will be able to communicate/share personal
health information as needed to ensure continuity of care
•Navigator will support individual through transition periods
across life/health stages both chronologically and
developmentally (i.e. end-of-life care)
•Proactive planning for transition
29 Health System Design: Blueprint Initiative Phase 2
How will information be communicated?
• Provincially driven electronic health record containing evidence-based/informed information that is accessible to health providers and
social agencies across the continuum of care
• Electronic health record will be linked to validated portal (personal health record) to support health literacy and evidence-based self-
management
• Information includes quality of care (wait times)
How will the model of care work? (cont’d)
How will funding be coordinated across sectors?
•Funding should follow the individual and their care needs.
•Cross-ministry funding strategies which are seamless to the individual
• Collaboration across multiple ministries (Ministry of Education,
Ministry of Child Youth Services, Ministry of Health Long Term
Care, Ministry of Community and Social Services)
•Focused health research design targeted towards female and
paediatric populations. Specific sub-population needs include pre-natal
and female geriatrics.
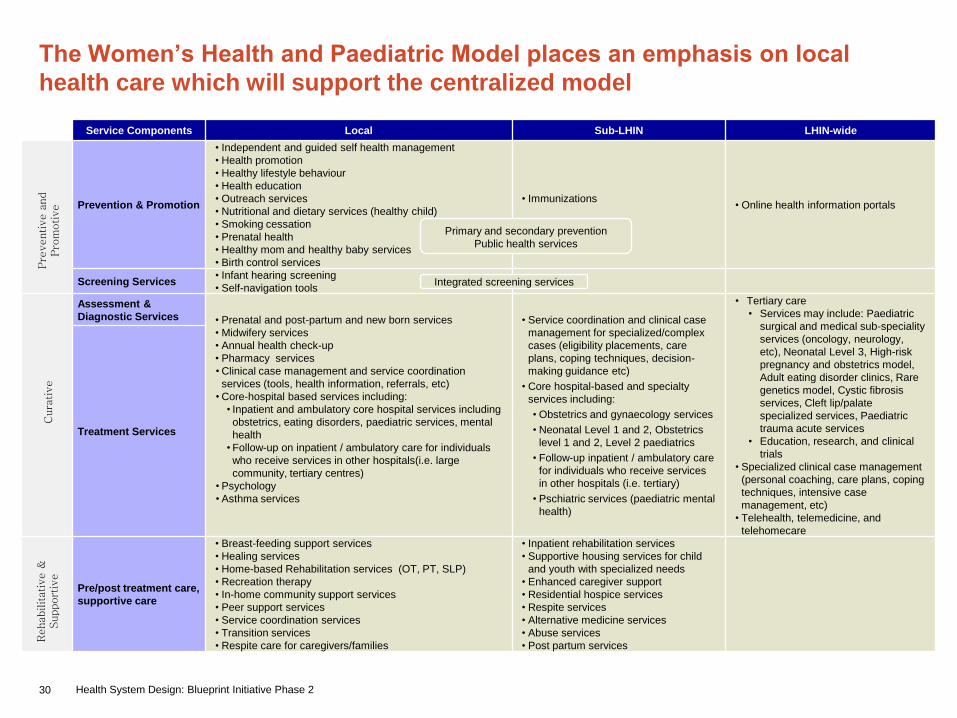
30 Health System Design: Blueprint Initiative Phase 2
The Women’s Health and Paediatric Model places an emphasis on local
health care which will support the centralized model
Service Components Local Sub-LHIN LHIN-wide
Prevention & Promotion
• Independent and guided self health management
• Health promotion
• Healthy lifestyle behaviour
• Health education
• Outreach services
• Nutritional and dietary services (healthy child)
• Smoking cessation
• Prenatal health
• Healthy mom and healthy baby services
• Birth control services
• Immunizations• Online health information portals
Screening Services• Infant hearing screening
• Self-navigation tools
Assessment &
Diagnostic Services • Prenatal and post-partum and new born services
• Midwifery services
• Annual health check-up
• Pharmacy services
• Clinical case management and service coordination
services (tools, health information, referrals, etc)
• Core-hospital based services including:
• Inpatient and ambulatory core hospital services including
obstetrics, eating disorders, paediatric services, mental
health
• Follow-up on inpatient / ambulatory care for individuals
who receive services in other hospitals(i.e. large
community, tertiary centres)
• Psychology
• Asthma services
• Service coordination and clinical case
management for specialized/complex
cases (eligibility placements, care
plans, coping techniques, decision-
making guidance etc)
• Core hospital-based and specialty
services including:
• Obstetrics and gynaecology services
• Neonatal Level 1 and 2, Obstetrics
level 1 and 2, Level 2 paediatrics
• Follow-up inpatient / ambulatory care
for individuals who receive services
in other hospitals (i.e. tertiary)
• Pschiatric services (paediatric mental
health)
• Tertiary care
• Services may include: Paediatric
surgical and medical sub-speciality
services (oncology, neurology,
etc), Neonatal Level 3, High-risk
pregnancy and obstetrics model,
Adult eating disorder clinics, Rare
genetics model, Cystic fibrosis
services, Cleft lip/palate
specialized services, Paediatric
trauma acute services
• Education, research, and clinical
trials
• Specialized clinical case management
(personal coaching, care plans, coping
techniques, intensive case
management, etc)
• Telehealth, telemedicine, and
telehomecare
Treatment Services
Pre/post treatment care,
supportive care
• Breast-feeding support services
• Healing services
• Home-based Rehabilitation services (OT, PT, SLP)
• Recreation therapy
• In-home community support services
• Peer support services
• Service coordination services
• Transition services
• Respite care for caregivers/families
• Inpatient rehabilitation services
• Supportive housing services for child
and youth with specialized needs
• Enhanced caregiver support
• Residential hospice services
• Respite services
• Alternative medicine services
• Abuse services
• Post partum services
Cura
tive
Rehabilitative &
Support
ive
Pre
ventive a
nd
Pro
motive
Primary and secondary prevention
Public health services
Integrated screening services
31 Health System Design: Blueprint Initiative Phase 2
Implications of Women’s Health & Paediatric services model of care
• Enabling “true self-management”, will require
individuals to have easy access to evidence-
based health information and inventory of health
services
• Develop effective working relationships with
navigators and proactively coordinate
information across health and social agencies
(i.e. communication of child behavior within
schools to primary care physician for „wholistic‟
assessment)
• Referrals by “active linking” and development of
integrated care plans will require stronger relationships
among stakeholders across health and social agencies
• Shift to local resources will require increased capacity of
front-line resources within community with regards to:
• Knowledge and understanding of all health
services across the continuum
• Understanding of person‟s health care history and
social considerations
• Develop trust and accountability with relationships
beyond traditional boundaries (i.e. health and non-health
ministries)
• Consistent interpretation and application of privacy laws
to enable information sharing across health sectors,
social agencies, non-traditional providers, and ministries
• Changes in funding model will require enhanced
collaboration between ministries of education, child youth
services, and health and long term care
Providers Individuals/Families
32 Health System Design: Blueprint Initiative Phase 2
Long Term Care
Services & Complex
Continuing Care

33 Health System Design: Blueprint Initiative Phase 2
The model of care has been developed upon the guiding vision
elements and principles
Vision
Elements
• Person-centered
• Sustainable
• Quality
• Accessible
• Timely
• Proactive
• Preventative
• Community-based services
Principles
• Connected for Life
• Diverse
• Promotes Independence
• Collaborative
• Simple
• Equity for All
• Sustainable
• Shared Accountability
• Engaging
• Evidence/best practice
• Maintain home “whereever home is”
• Ethical
• Relationships
• Sensitivity to language differences
34 Health System Design: Blueprint Initiative Phase 2
• Focus on maintaining independence for
individuals within their homes
• Community hubs, centered around
individual/caregivers for support, will
facilitate access to all long term care
services (i.e. LTCH, CCC beds)
• Personal care teams to maintain continuity
for individuals as they access services
across the health system
Model of care uses community hubs to manage and facilitate local
access to all long term care and complex continuing care services
How is this model different from
today’s service delivery model?
Providers
• Appropriate use
of complex
continuing care
and long term
care capacity
• Early
identification and
intervention of
health needs
What are the benefits of the
Model of Care?
Individuals/ Families
• Case management is provided
in settings that optimize care
delivery
• Empowerment of
individual/family members in
managing their own care –
Individual is part of health
team
• Care provided closer to home
allows individuals to have
increased access to personal
support network
• Individuals are connected to
health system through their
journey – “connected for life”
35 Health System Design: Blueprint Initiative Phase 2
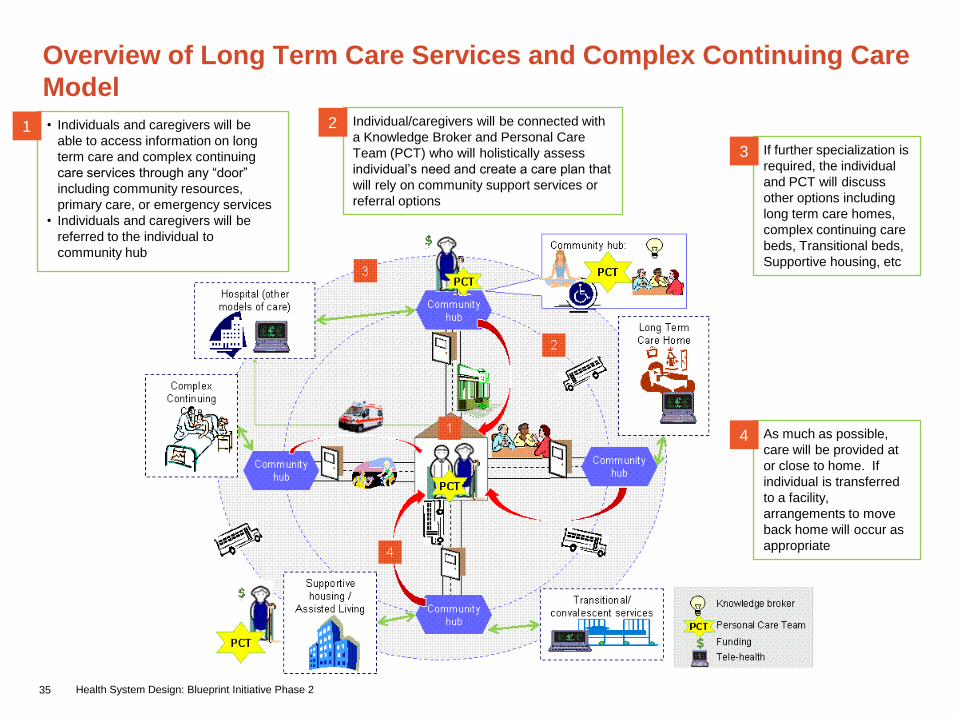
Overview of Long Term Care Services and Complex Continuing Care
Model
• Individuals and caregivers will be
able to access information on long
term care and complex continuing
care services through any “door”
including community resources,
primary care, or emergency services
• Individuals and caregivers will be
referred to the individual to
community hub
1 Individual/caregivers will be connected with
a Knowledge Broker and Personal Care
Team (PCT) who will holistically assess
individual‟s need and create a care plan that
will rely on community support services or
referral options
2
If further specialization is
required, the individual
and PCT will discuss
other options including
long term care homes,
complex continuing care
beds, Transitional beds,
Supportive housing, etc
3
As much as possible,
care will be provided at
or close to home. If
individual is transferred
to a facility,
arrangements to move
back home will occur as
appropriate
4
36 Health System Design: Blueprint Initiative Phase 2
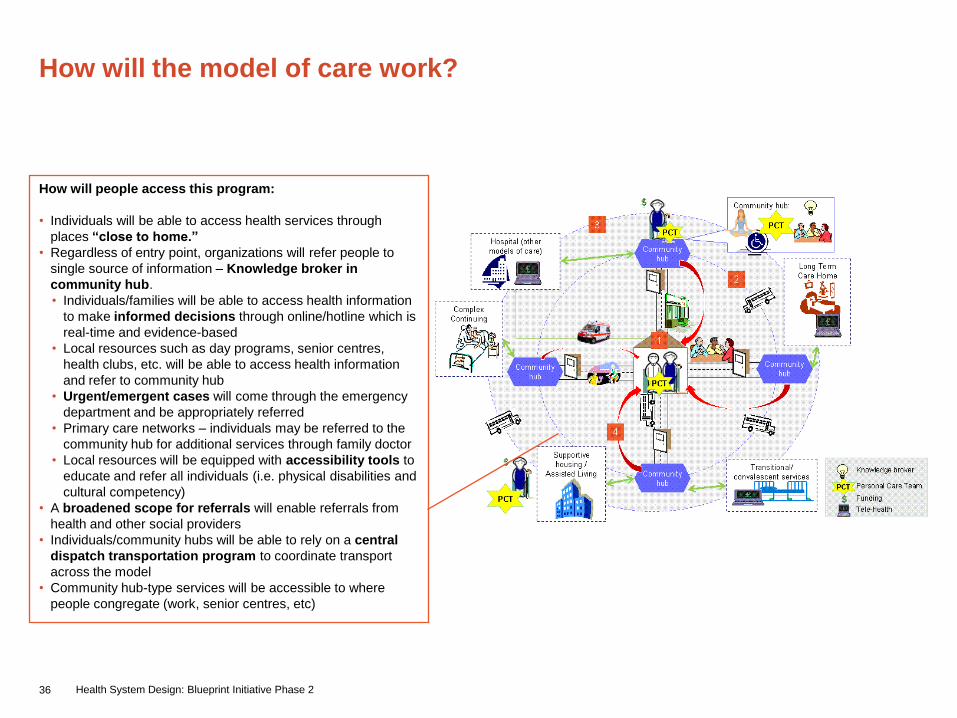
How will the model of care work?
How will people access this program:
• Individuals will be able to access health services through
places “close to home.”
• Regardless of entry point, organizations will refer people to
single source of information – Knowledge broker in
community hub.
• Individuals/families will be able to access health information
to make informed decisions through online/hotline which is
real-time and evidence-based
• Local resources such as day programs, senior centres,
health clubs, etc. will be able to access health information
and refer to community hub
• Urgent/emergent cases will come through the emergency
department and be appropriately referred
• Primary care networks – individuals may be referred to the
community hub for additional services through family doctor
• Local resources will be equipped with accessibility tools to
educate and refer all individuals (i.e. physical disabilities and
cultural competency)
• A broadened scope for referrals will enable referrals from
health and other social providers
• Individuals/community hubs will be able to rely on a central
dispatch transportation program to coordinate transport
across the model
• Community hub-type services will be accessible to where
people congregate (work, senior centres, etc)
37 Health System Design: Blueprint Initiative Phase 2
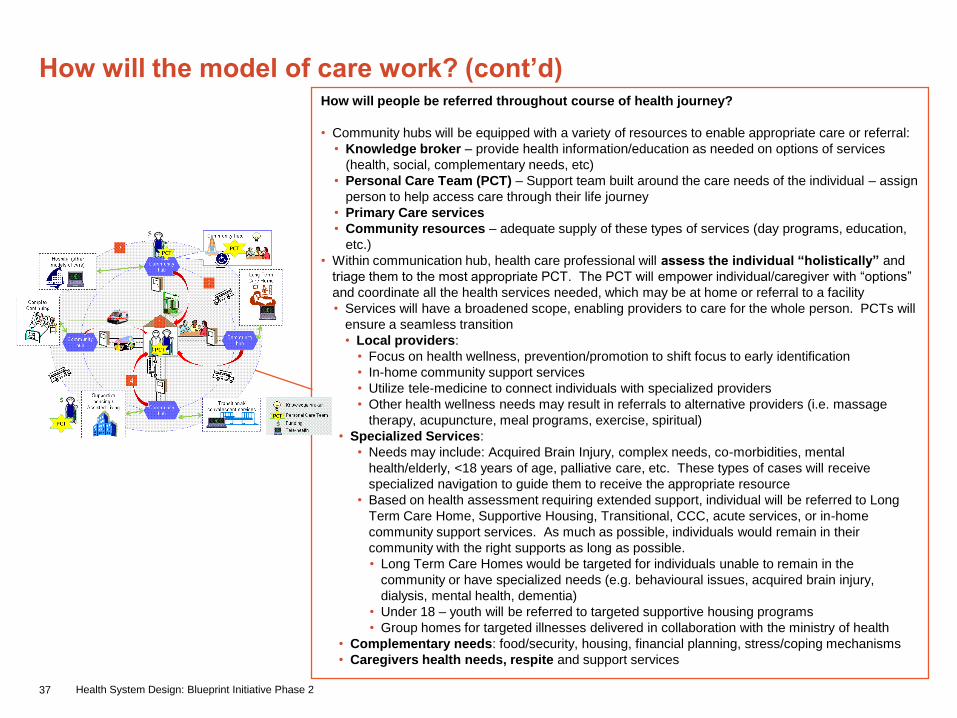
How will the model of care work? (cont’d)How will people be referred throughout course of health journey?
• Community hubs will be equipped with a variety of resources to enable appropriate care or referral:
• Knowledge broker – provide health information/education as needed on options of services
(health, social, complementary needs, etc)
• Personal Care Team (PCT) – Support team built around the care needs of the individual – assign
person to help access care through their life journey
• Primary Care services
• Community resources – adequate supply of these types of services (day programs, education,
etc.)
• Within communication hub, health care professional will assess the individual “holistically” and
triage them to the most appropriate PCT. The PCT will empower individual/caregiver with “options”
and coordinate all the health services needed, which may be at home or referral to a facility
• Services will have a broadened scope, enabling providers to care for the whole person. PCTs will
ensure a seamless transition
• Local providers:
• Focus on health wellness, prevention/promotion to shift focus to early identification
• In-home community support services
• Utilize tele-medicine to connect individuals with specialized providers
• Other health wellness needs may result in referrals to alternative providers (i.e. massage
therapy, acupuncture, meal programs, exercise, spiritual)
• Specialized Services:
• Needs may include: Acquired Brain Injury, complex needs, co-morbidities, mental
health/elderly, <18 years of age, palliative care, etc. These types of cases will receive
specialized navigation to guide them to receive the appropriate resource
• Based on health assessment requiring extended support, individual will be referred to Long
Term Care Home, Supportive Housing, Transitional, CCC, acute services, or in-home
community support services. As much as possible, individuals would remain in their
community with the right supports as long as possible.
• Long Term Care Homes would be targeted for individuals unable to remain in the
community or have specialized needs (e.g. behavioural issues, acquired brain injury,
dialysis, mental health, dementia)
• Under 18 – youth will be referred to targeted supportive housing programs
• Group homes for targeted illnesses delivered in collaboration with the ministry of health
• Complementary needs: food/security, housing, financial planning, stress/coping mechanisms
• Caregivers health needs, respite and support services
38 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
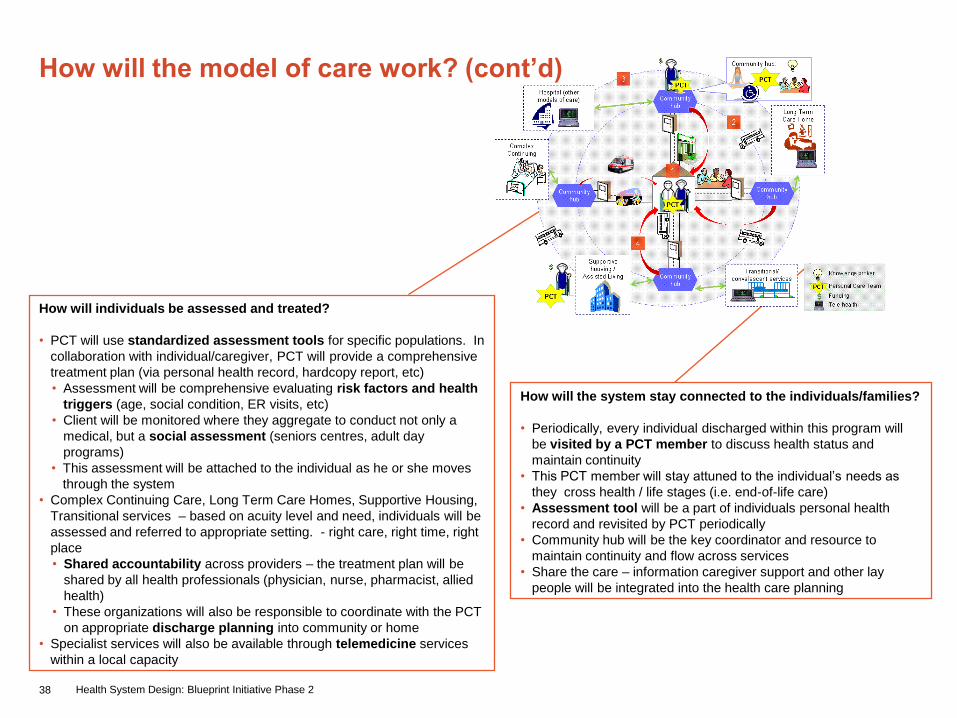
How will individuals be assessed and treated?
• PCT will use standardized assessment tools for specific populations. In
collaboration with individual/caregiver, PCT will provide a comprehensive
treatment plan (via personal health record, hardcopy report, etc)
• Assessment will be comprehensive evaluating risk factors and health
triggers (age, social condition, ER visits, etc)
• Client will be monitored where they aggregate to conduct not only a
medical, but a social assessment (seniors centres, adult day
programs)
• This assessment will be attached to the individual as he or she moves
through the system
• Complex Continuing Care, Long Term Care Homes, Supportive Housing,
Transitional services – based on acuity level and need, individuals will be
assessed and referred to appropriate setting. - right care, right time, right
place
• Shared accountability across providers – the treatment plan will be
shared by all health professionals (physician, nurse, pharmacist, allied
health)
• These organizations will also be responsible to coordinate with the PCT
on appropriate discharge planning into community or home
• Specialist services will also be available through telemedicine services
within a local capacity
How will the system stay connected to the individuals/families?
• Periodically, every individual discharged within this program will
be visited by a PCT member to discuss health status and
maintain continuity
• This PCT member will stay attuned to the individual‟s needs as
they cross health / life stages (i.e. end-of-life care)
• Assessment tool will be a part of individuals personal health
record and revisited by PCT periodically
• Community hub will be the key coordinator and resource to
maintain continuity and flow across services
• Share the care – information caregiver support and other lay
people will be integrated into the health care planning
39 Health System Design: Blueprint Initiative Phase 2
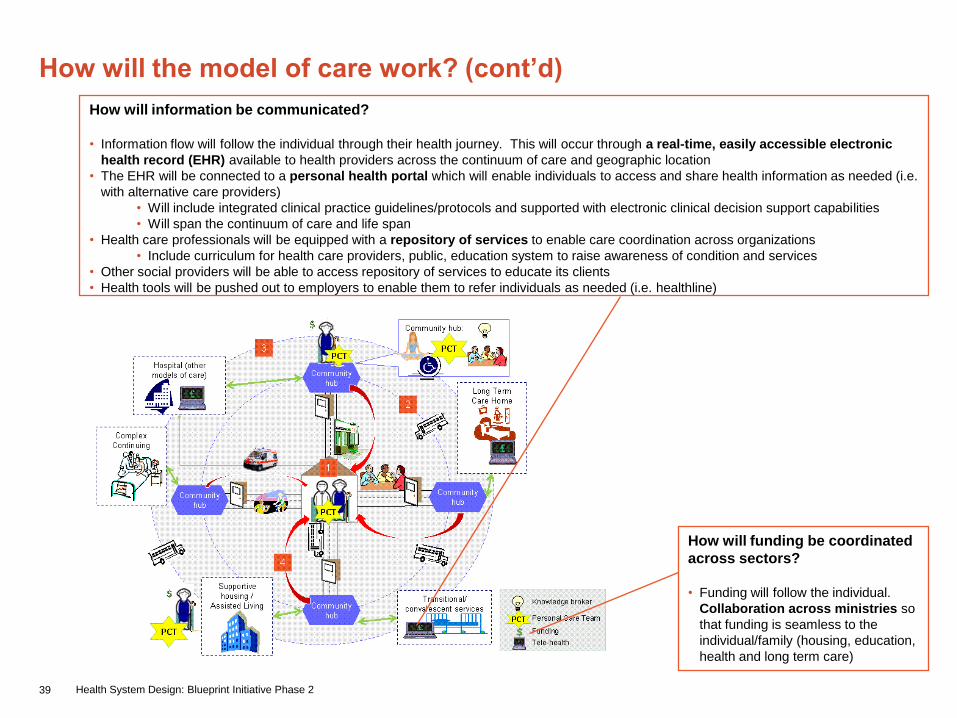
How will information be communicated?
• Information flow will follow the individual through their health journey. This will occur through a real-time, easily accessible electronic
health record (EHR) available to health providers across the continuum of care and geographic location
• The EHR will be connected to a personal health portal which will enable individuals to access and share health information as needed (i.e.
with alternative care providers)
• Will include integrated clinical practice guidelines/protocols and supported with electronic clinical decision support capabilities
• Will span the continuum of care and life span
• Health care professionals will be equipped with a repository of services to enable care coordination across organizations
• Include curriculum for health care providers, public, education system to raise awareness of condition and services
• Other social providers will be able to access repository of services to educate its clients
• Health tools will be pushed out to employers to enable them to refer individuals as needed (i.e. healthline)
How will the model of care work? (cont’d)
How will funding be coordinated
across sectors?
• Funding will follow the individual.
Collaboration across ministries so
that funding is seamless to the
individual/family (housing, education,
health and long term care)
40 Health System Design: Blueprint Initiative Phase 2
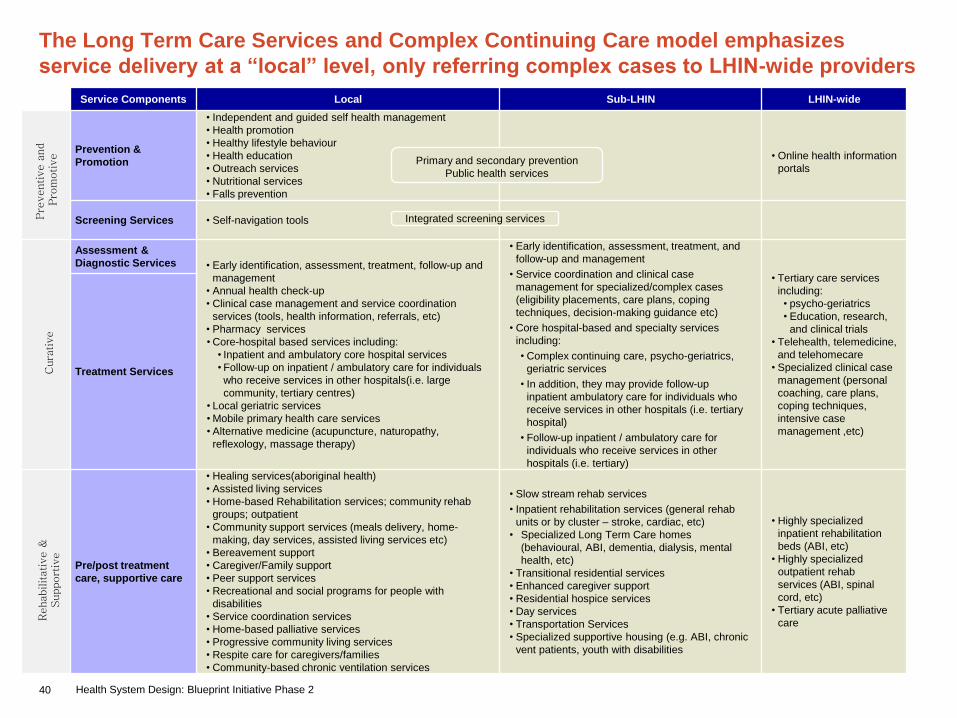
The Long Term Care Services and Complex Continuing Care model emphasizes
service delivery at a “local” level, only referring complex cases to LHIN-wide providers
Service Components Local Sub-LHIN LHIN-wide
Prevention &
Promotion
• Independent and guided self health management
• Health promotion
• Healthy lifestyle behaviour
• Health education
• Outreach services
• Nutritional services
• Falls prevention
• Online health information
portals
Screening Services • Self-navigation tools
Assessment &
Diagnostic Services • Early identification, assessment, treatment, follow-up and
management
• Annual health check-up
• Clinical case management and service coordination
services (tools, health information, referrals, etc)
• Pharmacy services
• Core-hospital based services including:
• Inpatient and ambulatory core hospital services
• Follow-up on inpatient / ambulatory care for individuals
who receive services in other hospitals(i.e. large
community, tertiary centres)
• Local geriatric services
• Mobile primary health care services
• Alternative medicine (acupuncture, naturopathy,
reflexology, massage therapy)
• Early identification, assessment, treatment, and
follow-up and management
• Service coordination and clinical case
management for specialized/complex cases
(eligibility placements, care plans, coping
techniques, decision-making guidance etc)
• Core hospital-based and specialty services
including:
• Complex continuing care, psycho-geriatrics,
geriatric services
• In addition, they may provide follow-up
inpatient ambulatory care for individuals who
receive services in other hospitals (i.e. tertiary
hospital)
• Follow-up inpatient / ambulatory care for
individuals who receive services in other
hospitals (i.e. tertiary)
• Tertiary care services
including:
• psycho-geriatrics
• Education, research,
and clinical trials
• Telehealth, telemedicine,
and telehomecare
• Specialized clinical case
management (personal
coaching, care plans,
coping techniques,
intensive case
management ,etc)
Treatment Services
Pre/post treatment
care, supportive care
• Healing services(aboriginal health)
• Assisted living services
• Home-based Rehabilitation services; community rehab
groups; outpatient
• Community support services (meals delivery, home-
making, day services, assisted living services etc)
• Bereavement support
• Caregiver/Family support
• Peer support services
• Recreational and social programs for people with
disabilities
• Service coordination services
• Home-based palliative services
• Progressive community living services
• Respite care for caregivers/families
• Community-based chronic ventilation services
• Slow stream rehab services
• Inpatient rehabilitation services (general rehab
units or by cluster – stroke, cardiac, etc)
• Specialized Long Term Care homes
(behavioural, ABI, dementia, dialysis, mental
health, etc)
• Transitional residential services
• Enhanced caregiver support
• Residential hospice services
• Day services
• Transportation Services
• Specialized supportive housing (e.g. ABI, chronic
vent patients, youth with disabilities
• Highly specialized
inpatient rehabilitation
beds (ABI, etc)
• Highly specialized
outpatient rehab
services (ABI, spinal
cord, etc)
• Tertiary acute palliative
care
Cura
tive
Rehabilitative &
Support
ive
Pre
ventive a
nd
Pro
motive
Integrated screening services
Primary and secondary prevention
Public health services
41 Health System Design: Blueprint Initiative Phase 2
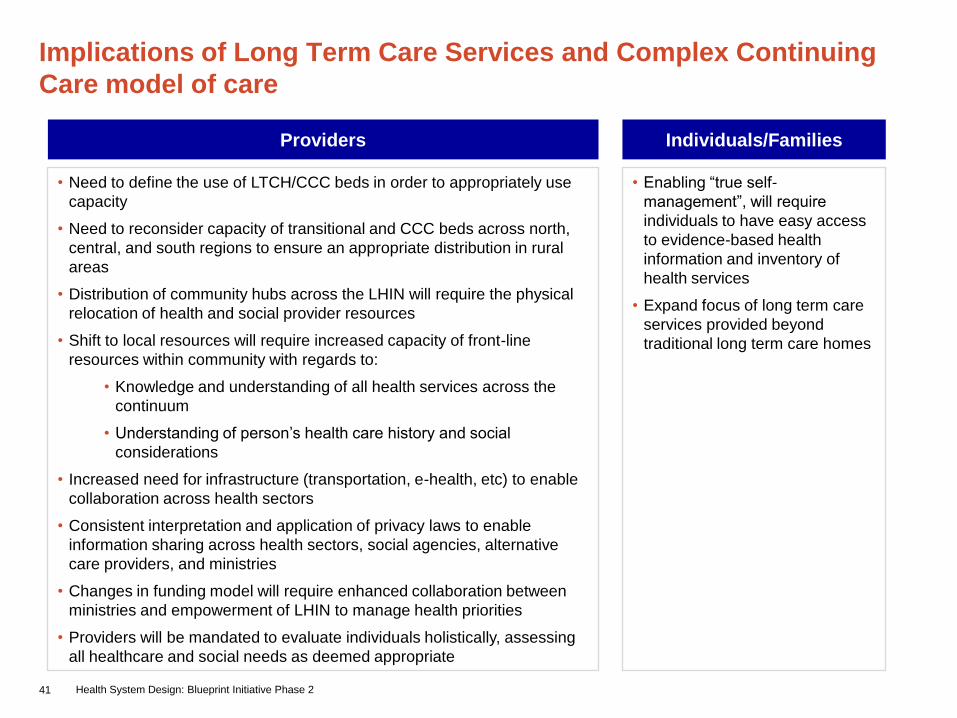
Implications of Long Term Care Services and Complex Continuing
Care model of care
• Enabling “true self-
management”, will require
individuals to have easy access
to evidence-based health
information and inventory of
health services
• Expand focus of long term care
services provided beyond
traditional long term care homes
• Need to define the use of LTCH/CCC beds in order to appropriately use
capacity
• Need to reconsider capacity of transitional and CCC beds across north,
central, and south regions to ensure an appropriate distribution in rural
areas
• Distribution of community hubs across the LHIN will require the physical
relocation of health and social provider resources
• Shift to local resources will require increased capacity of front-line
resources within community with regards to:
• Knowledge and understanding of all health services across the
continuum
• Understanding of person‟s health care history and social
considerations
• Increased need for infrastructure (transportation, e-health, etc) to enable
collaboration across health sectors
• Consistent interpretation and application of privacy laws to enable
information sharing across health sectors, social agencies, alternative
care providers, and ministries
• Changes in funding model will require enhanced collaboration between
ministries and empowerment of LHIN to manage health priorities
• Providers will be mandated to evaluate individuals holistically, assessing
all healthcare and social needs as deemed appropriate
Providers Individuals/Families

42 Health System Design: Blueprint Initiative Phase 2
Emergency Services
43 Health System Design: Blueprint Initiative Phase 2
The model of care has been developed upon the guiding vision
elements and principles
Vision
Elements
• 24/7 available emergency services within overall system with timely, accessible
levels of care using the right provider, providing the right care
• Individual and family centered care
• Culturally competent care
Principles
• Available and appropriate time to care
• Ensuring individual/families and staff safety
• Evidence-based care: LHIN-wide ED medical directives supported LHIN-wide,
clinical pathway, pre-printed orders
• Collaborative, inter-professional team working to their full scope of practice
• Access to adequate back-up support from other programs
• Access to timely diagnostics
44 Health System Design: Blueprint Initiative Phase 2
• GPS-type care coordination system to
enable emergency services to book
follow-up appointments across health
sectors
• Expansion of provider roles across
the continuum to optimize care
delivery
• Integrated collaboration across health
sectors to enable seamless referrals
Model of care focuses on expanding access to emergency services
beyond emergency departments
How is this model different from
today’s service delivery model?
Providers
• Enables the right
practitioners to
provide the right
care in the right
place
• Strengthened
relationship
between partners
across health
sectors
What are the benefits of the
Model of Care?
Individuals/ Families
• Care is coordinated
for individual and
family before leaving
the provider

45 Health System Design: Blueprint Initiative Phase 2
Overview of Emergency Services Model
• Individuals/ families will access
emergency services through any door
– “right ride to the right place”
• Once care is provided within the
provider setting, the individual will be
discharged to community resources for
any follow-up care – “right follow-up”
• Once the individual enters the
system, they will be holistically
evaluated and treated and/or referred
to the appropriate care – “right care
by right provider”
1 3
Triage
Assessment /
Reassurance
Treatment
Care Coordination
Education / Self
Care: Referral
to primary care
Consults with
specialists
Inpatient Care –
Facility Transfers
GPS – Booking of all
follow-up appointments
Culturally sensitive care
for homeless and other
specialized populations
2
telehealth
Health
Information
Community Support
ServicesUrgent
Care
Centre
Emergency
Department
Primary
Care
(FHT/FHN/C
HC/GP/NP
Clinic)
“Right ride to the
right place”
EMS
1
2
3
Release
Assess and
transport (if
necessary)
46 Health System Design: Blueprint Initiative Phase 2
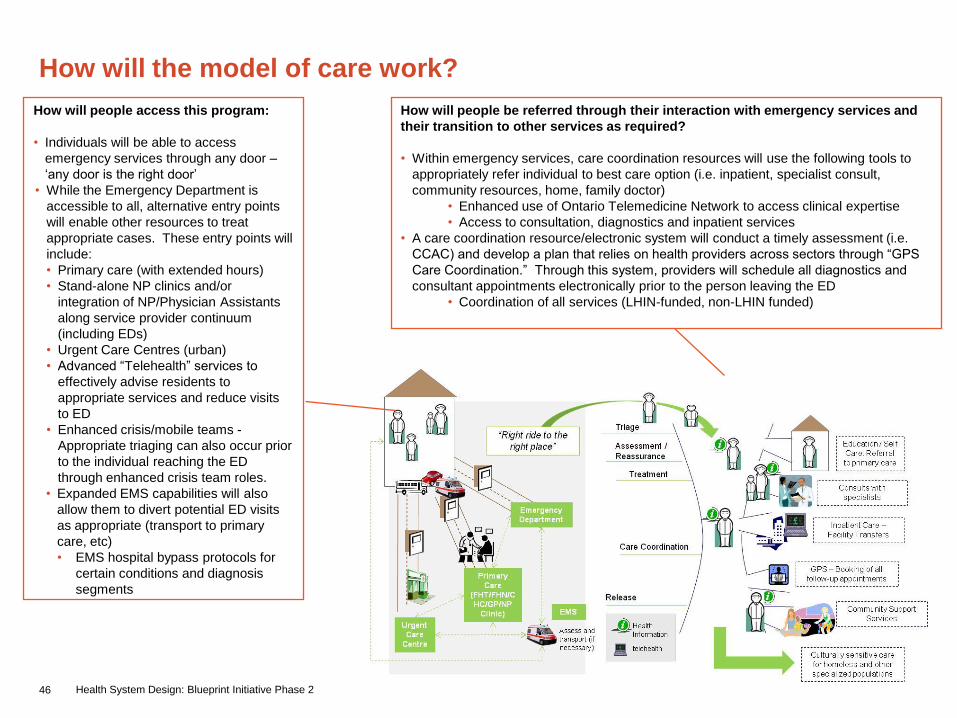
How will the model of care work?
How will people access this program:
• Individuals will be able to access
emergency services through any door –
„any door is the right door‟
• While the Emergency Department is
accessible to all, alternative entry points
will enable other resources to treat
appropriate cases. These entry points will
include:
• Primary care (with extended hours)
• Stand-alone NP clinics and/or
integration of NP/Physician Assistants
along service provider continuum
(including EDs)
• Urgent Care Centres (urban)
• Advanced “Telehealth” services to
effectively advise residents to
appropriate services and reduce visits
to ED
• Enhanced crisis/mobile teams -
Appropriate triaging can also occur prior
to the individual reaching the ED
through enhanced crisis team roles.
• Expanded EMS capabilities will also
allow them to divert potential ED visits
as appropriate (transport to primary
care, etc)
• EMS hospital bypass protocols for
certain conditions and diagnosis
segments
How will people be referred through their interaction with emergency services and
their transition to other services as required?
• Within emergency services, care coordination resources will use the following tools to
appropriately refer individual to best care option (i.e. inpatient, specialist consult,
community resources, home, family doctor)
• Enhanced use of Ontario Telemedicine Network to access clinical expertise
• Access to consultation, diagnostics and inpatient services
• A care coordination resource/electronic system will conduct a timely assessment (i.e.
CCAC) and develop a plan that relies on health providers across sectors through “GPS
Care Coordination.” Through this system, providers will schedule all diagnostics and
consultant appointments electronically prior to the person leaving the ED
• Coordination of all services (LHIN-funded, non-LHIN funded)
47 Health System Design: Blueprint Initiative Phase 2
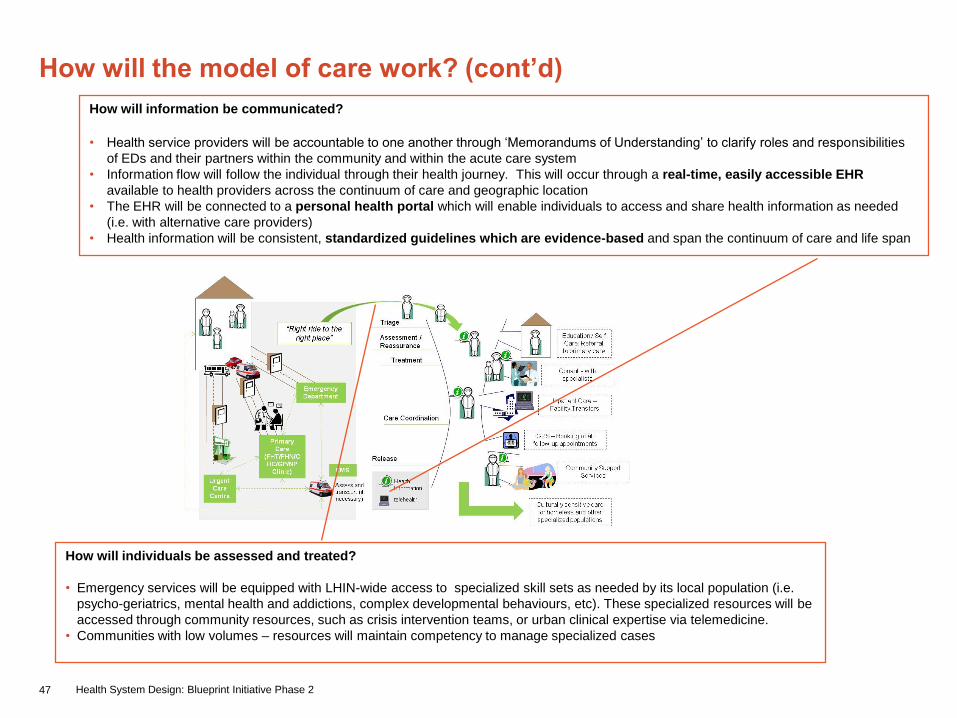
How will the model of care work? (cont’d)
How will individuals be assessed and treated?
• Emergency services will be equipped with LHIN-wide access to specialized skill sets as needed by its local population (i.e.
psycho-geriatrics, mental health and addictions, complex developmental behaviours, etc). These specialized resources will be
accessed through community resources, such as crisis intervention teams, or urban clinical expertise via telemedicine.
• Communities with low volumes – resources will maintain competency to manage specialized cases
How will information be communicated?
• Health service providers will be accountable to one another through „Memorandums of Understanding‟ to clarify roles and responsibilities
of EDs and their partners within the community and within the acute care system
• Information flow will follow the individual through their health journey. This will occur through a real-time, easily accessible EHR
available to health providers across the continuum of care and geographic location
• The EHR will be connected to a personal health portal which will enable individuals to access and share health information as needed
(i.e. with alternative care providers)
• Health information will be consistent, standardized guidelines which are evidence-based and span the continuum of care and life span
48 Health System Design: Blueprint Initiative Phase 2
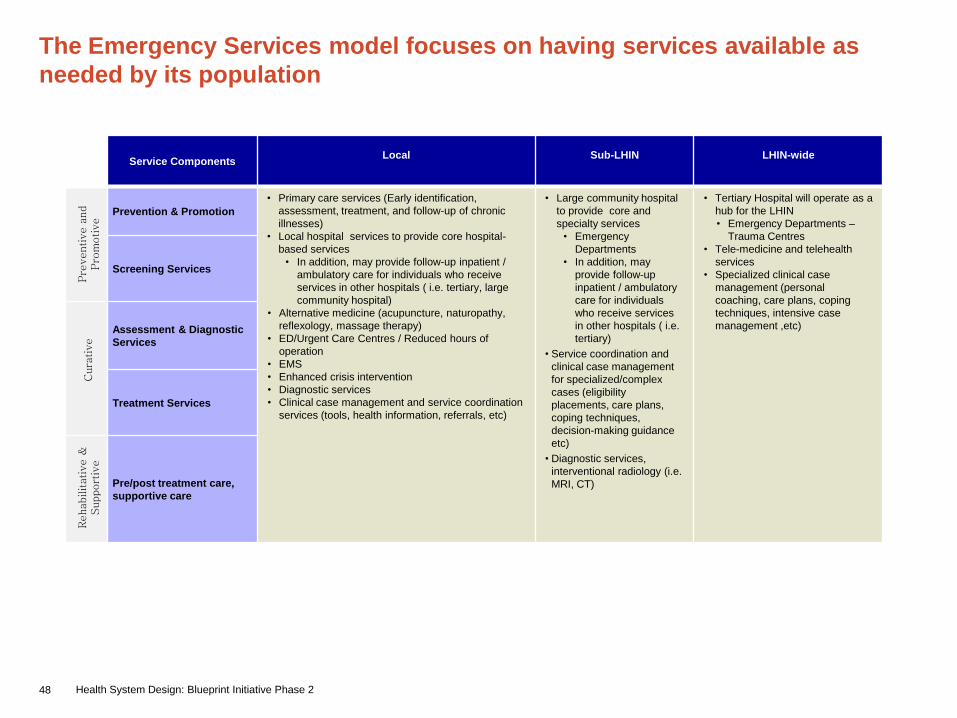
The Emergency Services model focuses on having services available as
needed by its population
Service ComponentsLocal Sub-LHIN LHIN-wide
Prevention & Promotion
• Primary care services (Early identification,
assessment, treatment, and follow-up of chronic
illnesses)
• Local hospital services to provide core hospital-
based services
• In addition, may provide follow-up inpatient /
ambulatory care for individuals who receive
services in other hospitals ( i.e. tertiary, large
community hospital)
• Alternative medicine (acupuncture, naturopathy,
reflexology, massage therapy)
• ED/Urgent Care Centres / Reduced hours of
operation
• EMS
• Enhanced crisis intervention
• Diagnostic services
• Clinical case management and service coordination
services (tools, health information, referrals, etc)
• Large community hospital
to provide core and
specialty services
• Emergency
Departments
• In addition, may
provide follow-up
inpatient / ambulatory
care for individuals
who receive services
in other hospitals ( i.e.
tertiary)
• Service coordination and
clinical case management
for specialized/complex
cases (eligibility
placements, care plans,
coping techniques,
decision-making guidance
etc)
• Diagnostic services,
interventional radiology (i.e.
MRI, CT)
• Tertiary Hospital will operate as a
hub for the LHIN
• Emergency Departments –
Trauma Centres
• Tele-medicine and telehealth
services
• Specialized clinical case
management (personal
coaching, care plans, coping
techniques, intensive case
management ,etc)
Screening Services
Assessment & Diagnostic
Services
Treatment Services
Pre/post treatment care,
supportive care
Cura
tive
Rehabilitative &
Support
ive
Pre
ventive a
nd
Pro
motive

49 Health System Design: Blueprint Initiative Phase 2
Implications of Emergency Services model of care
• Expand focus on accessing emergency
services beyond the emergency
department. Increase reliance on non-
ED resources for health needs (i.e.
PCP, urgent care, NP clinic, etc)
• Future service model is driven by ensuring quality service delivery
via all access points in the system, not as a cost-containment
strategy. This is particularly important when planning for access to
emergency services within HHR limitations
• Further research to be conducted to determine appropriate time to
care in rural and urban areas – what is considered acceptable travel
time in South West LHIN in relation to these areas. Implication: Both
sessions understand rationalization of resources is a consequence
of this definition
• Clarification of policy on “Hospital” designation, if ED operates on
reduced hours
• Seamless referral system will require stronger relationships and
accountability among stakeholders across health and social
agencies
• Need to evaluate the impact of reduced hour EDs on nearby
services, as well as to other areas of the hospital (i.e. inpatient
units)
• Increased workload to EMS and RNs for escorting patients during
transfers
• Changes in physician workload and reimbursement systems
• Consistent interpretation and application of privacy laws to enable
information sharing across health sectors, social agencies,
alternative care providers, and ministries
Providers Individuals/Families

50 Health System Design: Blueprint Initiative Phase 2
Enablers for Emergency Services model of care
• LHIN-wide HHR strategy for recruitment and retention for physicians and RNs providing
emergency services, in particular, targeted towards rural and remote communities
• Appropriate physician remuneration models to reflect the work and hours required in
delivering care 24/7
• Effective back-up/specialist clinician support practitioners in managing acute and/or
complex cases
• A LHIN wide bed management system to facilitate admissions from ED.
• LHIN wide non-ambulance patient transportation delivery model and algorithm. Cost of
non-ambulance patient transportation needs to be recognized in the funding for institutions.
• MOHLTC legislative adjustments to enable expanded role of EMS
51 Health System Design: Blueprint Initiative Phase 2
Medicine
Medicine model of care refers to the
delivery of internal medicine services
and medical sub-specialties (e.g.
cardiology, nephrology,
endocrinology, etc)
52 Health System Design: Blueprint Initiative Phase 2
The model of care has been developed upon the guiding vision
elements and principles
Vision
Elements
• Access will be timely, person-focused, and evidence based
• Efficient use of care resources
• Individual‟s care experience is built on consistency, quality, and excellence
• Evidence based quality of care
• Integrated seamless model
Principles
• Transparent and accountable system
• Standardized communication and language
• Designed and tailored care at each point along an individuals care continuum
• Resources flow with the individual‟s care needs
• Enhance local capacity

53 Health System Design: Blueprint Initiative Phase 2
• A centralized system navigator in the
form of a coordinated primary care
network across the LHIN
• Care close to home balanced with
Centres of Excellence
• Information sharing portal for
individuals, providers, and families
• An „advanced‟ telemedicine service
will serve as a true option for
individuals/families and providers
• Standardized, consistent approach to
care provision
Model of care uses a centralized system navigator in the form of an
expanded primary care network to assess and triage individuals /
families based on level of complexity/intensity
How is this model different from
today’s service delivery model?What are the benefits of the
Model of Care?
Providers
• Capacity utilization
in the LHIN will
improve as a result
of precise
navigation to
appropriate health
facilities
• More dedicated
time for quality
care as a result of
advanced
telemedicine
support and easily
accessed online
education and self
management tools
What are the benefits of the
Model of Care?
Individuals/ Families
• Individuals and
families will have a
trusted point of first
contact for all
medical situations
• Individuals and
families will have
access to health
education and self-
management tools
through several
mediums
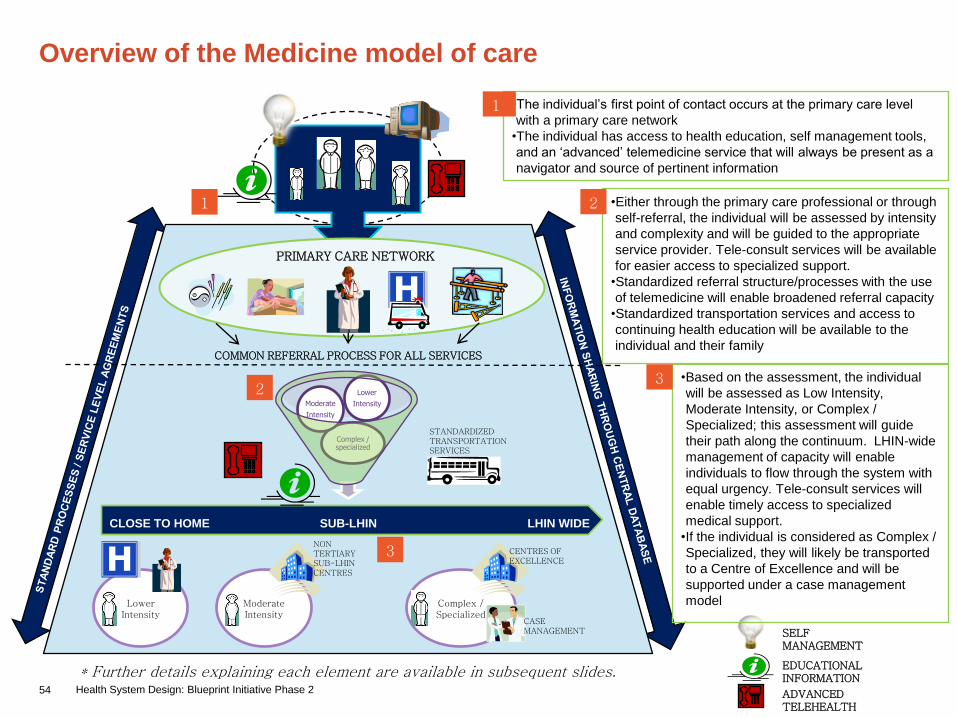
54 Health System Design: Blueprint Initiative Phase 2
Overview of the Medicine model of care
PRIMARY CARE NETWORK
COMMON REFERRAL PROCESS FOR ALL SERVICES
SELF MANAGEMENT
EDUCATIONAL INFORMATION
ADVANCED TELEHEALTH
Complex / specialized
Moderate
Intensity
Lower
Intensity
CLOSE TO HOME SUB-LHIN LHIN WIDE
LowerIntensity
Complex / Specialized
ModerateIntensity
CENTRES OF EXCELLENCE
NON TERTIARY SUB-LHIN CENTRES
CASE MANAGEMENT
STANDARDIZED TRANSPORTATION SERVICES
•The individual‟s first point of contact occurs at the primary care level
with a primary care network
•The individual has access to health education, self management tools,
and an „advanced‟ telemedicine service that will always be present as a
navigator and source of pertinent information
1
•Either through the primary care professional or through
self-referral, the individual will be assessed by intensity
and complexity and will be guided to the appropriate
service provider. Tele-consult services will be available
for easier access to specialized support.
•Standardized referral structure/processes with the use
of telemedicine will enable broadened referral capacity
•Standardized transportation services and access to
continuing health education will be available to the
individual and their family
2
•Based on the assessment, the individual
will be assessed as Low Intensity,
Moderate Intensity, or Complex /
Specialized; this assessment will guide
their path along the continuum. LHIN-wide
management of capacity will enable
individuals to flow through the system with
equal urgency. Tele-consult services will
enable timely access to specialized
medical support.
•If the individual is considered as Complex /
Specialized, they will likely be transported
to a Centre of Excellence and will be
supported under a case management
model
3
1
2
3
* Further details explaining each element are available in subsequent slides.

55 Health System Design: Blueprint Initiative Phase 2
How will the model of care work?
How will people access this program?
•Individuals and their families will be supported by an integrated
primary care network consisting of traditional providers such as
physicians and nurses but also consisting of allied health and
alternative care providers. They will have the ability to refer
individuals.
•Individuals and health care providers will have access to tele-consult
services to ensure timely access to specialized support
•Individuals will also have online health information and self
management tools to enable and promote responsible health
management and choices
•Individuals and their families will have 24 hour telephone access to
an advanced version of telemedicine, whereby they can choose to
receive basic consultation or be navigated to the appropriate resource
•Primary care networks will offer extended hours in each community in
order to offer flexible choices and access
•Centralized transportation dispatch system across the LHIN will
streamline access as needed
How will individuals be referred in this continuum?
•Upon their interaction with a primary care practitioner, they will
then be assessed for social, clinical, and geographic factors and
by level of complexity / intensity. Tele-consult services will be
used as required.
•Members of the primary care team (i.e. OT, PT, physician) will
triage the individual to the appropriate health provider upon
completion of the assessment. Both health providers and
individuals/families will be able to use a standardized referral
structure to seamlessly access specialty services

56 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
How will individuals be identified
and assessed?
• Online educational materials and self
management tools will help to enable
and promote responsibility of the
individual to self manage illness or
condition
• Individuals will be assessed by a team
of practitioners within a broader
primary care network
How will individuals and providers
access education and information?
•For the individual and their family, there will be
single point of access to education and
information available anywhere; examples
include, telemedicine, online self management
tools, information and education at community
centres and schools
•Online health information portal accessible
anywhere for individuals and families and
providers that can be easily understood
•Tele-consult services available for specialized
medical advice
•Electronic health record (EHR) available to both
individuals and providers. This information will
be communicated back to the primary care
network via the EHR
•Standardized tools, resources, and knowledge
exchanges for providers

57 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
What role will Medicine play in complementary care?
• Individuals and their families will be taken care of in a culturally
sensitive environment
• The primary health team will bring holistic approaches to health as
well as tailored care (i.e. aboriginal care, seniors care)
• There will be access to complementary services through online
support and telehealth (i.e. meals on wheels)
How will Medicine care for specialized needs?
• Individuals will have unique specialty services available to them in
key areas of the LHIN
• Individuals will receive case management support for highly
complex / specialized cases at tertiary hospitals and Centres of
Excellence located across the LHIN
58 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
How will Medicine support health research?
• Meaningful data will be collected at each
point of interaction within a common data
warehouse (i.e. person-provider, person-
website, provider-provider). This will be used
to prioritize funds for LHIN-initiated research
• Partnerships among traditional and
alternative care practitioners and academic
health centres will be strengthened
How will care be coordinated?
•For less complex individuals, case management support will be provided by the primary care
physician; for specialized / complex individuals, the CCAC will work together with primary care
networks to support more complex case management
•Standardized processes and operations will be instituted throughout the LHIN to support
screening, assessment, and discharge at all hospitals and facilities across the LHIN

59 Health System Design: Blueprint Initiative Phase 2
The Medicine model focuses on using the expertise of primary care practitioners to
appropriately assess and navigate individuals to the appropriate service facility
Service Components Local Sub-LHIN LHIN-wide
Prevention &
Promotion
• Independent and guided self health management
• Health promotion
• Healthy lifestyle behaviour
• Health education and advocacy
• Outreach services
• Nutritional services and dietary services
• Smoking cessation services
• Online health information portals
Screening Services • Self-navigation tools
Assessment &
Diagnostic Services• Early identification, assessment, treatment, follow-
up and management of chronic illnesses
• Annual health check-up
• Pharmacy services
• Clinical case management and service
coordination services (tools, health information,
referrals, etc)
• Core-hospital based services including:
• Inpatient and ambulatory, high volume/low acuity
general medicine and internal medicine services
• Follow-up on inpatient / ambulatory care for
individuals who receive services in other
hospitals(i.e. large community, tertiary centres)
• Diagnostic assessments
• Shared care services with specialists and
primary care
• Emergency services
• Alternative medicine (acupuncture, naturopathy,
reflexology, massage therapy)
• Early identification, assessment, treatment, follow-up
and management of chronic illnesses
• Service coordination and clinical case management for
specialized/complex cases (eligibility placements, care
plans, coping techniques, decision-making guidance
etc)
• Core hospital-based and specialty services including:
• Inpatient and ambulatory, moderate volume/acuity,
internal medicine physician (PCI, oncology, etc)
• Follow-up inpatient / ambulatory care for individuals
who receive services in other hospitals (i.e. tertiary)
• Diagnostic assessments – interventional radiology
(i.e. MR, CT)
• Pain and symptom management services (i.e.
chronic pain)
• Systemic and radiation therapy
• Tertiary /Quaternary care services
(low volume/high acuity):
• Sub-specialized inpatient and
ambulatory internal medicine
services (i.e. specialized thyroid
and parathyroid services, sub-
specialized respiratory services,
rheumotology)
• Specialized radiation and
systemic therapy
• Education, research, and clinical
trials
• Specialized clinical case
management (personal coaching,
care plans, coping techniques,
intensive case management ,etc)
• Complex multi-disease
management
• Telehealth, telemedicine, and
telehomecare
Treatment Services
Pre/post treatment
care, supportive
care
• Healing services
• Home-based Rehabilitation services
• In-home community support services
• Bereavement support
• Caregiver/Family support
• Peer support services
• Recreational and social programs for people with
disabilities
• Respite care for caregivers/families
• Service coordination services
• Supportive services to manage chronic illnesses
(Dialysis, stroke, diabetes, chiropody, weight
management)
• Home-based palliative services
• Chronic ventilation services
• Respite care for caregivers/families
• Inpatient rehabilitation services (general rehab units or
by cluster – stroke, cardiac, etc)
• Supportive housing services
• Long term care services
• Transitional residential services
• Enhanced caregiver support
• Residential hospice services
• Day services
• Palliative care services (end stage COPD)
• Highly specialized inpatient
rehabilitation beds (ABI, etc)
• Highly specialized outpatient
rehab services (ABI, spinal cord,
etc)
• Tertiary acute palliative care
Cura
tive
Rehabilitative &
Support
ive
Pre
ventive a
nd
Pro
motive
Integrated Screening (aneurysm, carotid disease, etc)
Primary and secondary prevention
Public health services
Patient, family, and caregiver education and information services

60 Health System Design: Blueprint Initiative Phase 2
Implications of the Medicine model of care
• Enabling “true self-management”, will
require individuals to have easy access
to evidence-based health information
and inventory of health services
• The primary care networks and primary health teams that will be
supporting individuals and their families throughout the LHIN will
require greater attention in terms of health human resources
recruitment and distribution.
• A clear delineation of each providers role, at all levels, within the
system.
• A commitment to building a world class, advanced Telemedicine
service will require a coordinated commitment by leaders in health
care to develop and institute 1) an inventory of available services at
each facility across the LHIN, 2) a common set of screening,
assessment, and discharge guidelines, and 3) a real time view of
capacity utilization across the LHIN.
• Implementing a case management approach for Complex /
Specialized individuals will require a common set of clinical
standards across the LHIN and all agencies and organizations; it
will also require increased coordination between hospitals /
organizations and physician offices in order to best translate
inpatient information into outpatient practice.
• A coordinated effort across the health care providers to collect and
contribute to an electronic health record database.
• Leverage purchasing power in coordinating a centralized
transportation system
Providers Individuals/Families
61 Health System Design: Blueprint Initiative Phase 2
Critical Care

62 Health System Design: Blueprint Initiative Phase 2
• Collaboration among all critical care units
across the LHIN to ensure that the right patient
is in the right place at the right time (consistent
admission criteria)
• Being respectful of family and patient by
consistently sharing information throughout the
process to enable decision making
• Development of the Electronic Health Record
will enable the seamless transition of care to
other services within the hospital, to their local
community or local hospital
• Development of regional critical care physician
on-call system and structure
Model of care focuses on LHIN-wide management of critical care
resources to enable appropriate use, ensure critical mass, and
maintain individual/family focused care
How is this model different from today’s service delivery model?
What are the benefits of the Model of Care?
Providers
• Maximizes utilization of
resources across the
entire LHIN
• With the regional on-call
system, all consults will
be directed to the on-call
physician. This
minimizes stress as
providers will no longer
have to provide both
patient care and on-call
consults concurrently
• Access to quicker advice
from critical care
physician
What are the benefits of the Model of Care?
Individuals/ Families
• Strengthens relationship
with patient, families and
providers
• Minimizes stress to patient
and families during
transition points in care

63 Health System Design: Blueprint Initiative Phase 2
Overview of Critical Care model of care
1
Patient / Family
Focus
• Care of critical care
patients will focus
on the needs of
patients and their
families.
Consistent
communication of
information
throughout the care
journey across
transition points is
needed to minimize
stress and optimize
recovery
Communication
• Communication between
the local, sub-LHIN and
LHIN wide referral centres
will be required to
optimize the utilization of
beds throughout the LHIN
• CritiCall will serve as
triage system to facilitate
communication to
consultant
Critical Mass
• Critical mass ensures
patients receive safe
and effective treatment.
2
4
Appropriateness
• Critical care beds will operate as
LHIN-wide beds to ensure the right
patient is in the right bed at the right
time.
• CritiCall will serve as an efficient
critical care triage system to ensure
patients are in the appropriate
bed by having real-time
access to information on the availability
of level 2 & 3
beds throughout the LHIN
• A referral will be made only
if the sending physician
consults with a critical
care physician.
Consultation to be
facilitated by CritiCall.
CritiCall
Sub-LHIN Hospital
Level 2 & 3
LHIN-Wide Referral
Hospital
Level 3
CritiC
all
Cri
tiC
all
CritiCall
Long Term Care Services / Complex
Continuing Care
Local Hospital Level 23
* Further details explaining
each element are available in
subsequent slides.

64 Health System Design: Blueprint Initiative Phase 2
How will the Critical Care model of care work?
Where will patients be referred throughout course of Critical
Care journey?
• Clear and consistent definition of Level 2 & Level 3 beds is required to
ensure that there is clarity and accountability managing the utilization of
beds across the LHIN
• Development of guidelines / protocols for “Resuscitation – Stabilization and
Transfer of the Critically Ill Patient” to promote a common understanding to
the appropriateness of referrals across the LHIN
• Development of hospital patient transfer criteria. These criteria will be
determined by each hospital‟s limitations to provide patient‟s needs. Local,
sub-LHIN and LHIN-wide referral hospitals will develop consistent
guidelines for assessments and transfers.
• Development of transfer partnerships between community hospitals and
LHIN-wide referral centre. These partnerships will be both within and
external to LHIN and will be focused on patient need.
• Development of Hospital Repatriation Policy – once the patient‟s care can
now be met by the local hospital, arrangements will be made to transfer
patients.
• Promotion of communication and support between local and LHIN-wide
referral centre using telemedicine, LHIN-wide teleconferences on topics
relevant to each hospital‟s needs or related to recent patient transfers.
How will Critical Care accommodate for specialized
needs?
• Patients requiring acute dialysis, burn, trauma, neurological
and cardiac surgical services will require referral to the
LHIN-wide Referral Hospital
• For Chronic Vent patients, services will require early and
proactive coordinated funding and services within and
external to the critical care setting (i.e. CCAC, LTC, respite
services etc.)
How will patients / families / providers access this program:
• Providers (i.e. EMS and physicians) will contact CritiCall to understand real
time critical care bed availability in the LHIN. CritiCall will determine the
most appropriate critical care bed for the patient based on the level of
acuity of illness, urgency and geography.
• A referral will be made only if the sending physician consults with a critical
care physician. These consultation to be facilitated by CritiCall.

65 Health System Design: Blueprint Initiative Phase 2
How will the Critical Care model of care work?(cont’d)
How will local, sub-LHIN and LHIN-wide referral centres support each other to optimize quality patient care?
• Critical Care Information System will provide up to date information on the utilization and level of acuity of patients
currently occupying critical care beds across the LHIN. As such, this information with CritiCall will support providers in
determining the appropriate occupancy of the patients and initiate transfers as needed to optimize capacity and
resource utilization of their beds
• Support from LHIN-wide referral centres to local sites for information, assessment and treatment via telemedicine and
transfers as required.
• To increase consistency, expertise and quality of critical care, LHIN-wide educational programs using protocols / care
bundles / benchmarks directed at enhancing patient care will be implemented

66 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
How will the system stay connected to the individual?
• Understand and document as early as possible the goals
of care by patient / families to optimize level and setting
of care provided. As care progresses, these goals will
require ongoing assessment and updates
• To minimize stress on patients and families, care
planning by involving patients/families through the care
journey and providing education to enable decision
making. This communication and information will also
ease transitions from critical care to different levels of
care (i.e. general medical units, different hospitals, LTC,
palliative care etc.) for patients/families
• Involvement and communication with other providers as
needed (i.e. End of Life, Palliative Care, CCAC,
respiratory services, LTC services)
How will information be communicated?
• Development of information to educate patients on the appropriateness of care in the various facilities. This will raise the awareness and
confidence in patients / families that the most appropriate care is being provided in the right setting
• Implementation of the Electronic Health Record (EHR) that supports broad provider access to accurate patient histories and current
interventions, will enable all providers to make care decisions in a timely manner. The EHR will also result in more seamless transitions of
care from hospital to in-patient unit (i.e. surgical, medical, etc.), between hospitals and hospital to community / home
• CritiCall will serve as triage system to facilitate communication among providers and critical care consultants
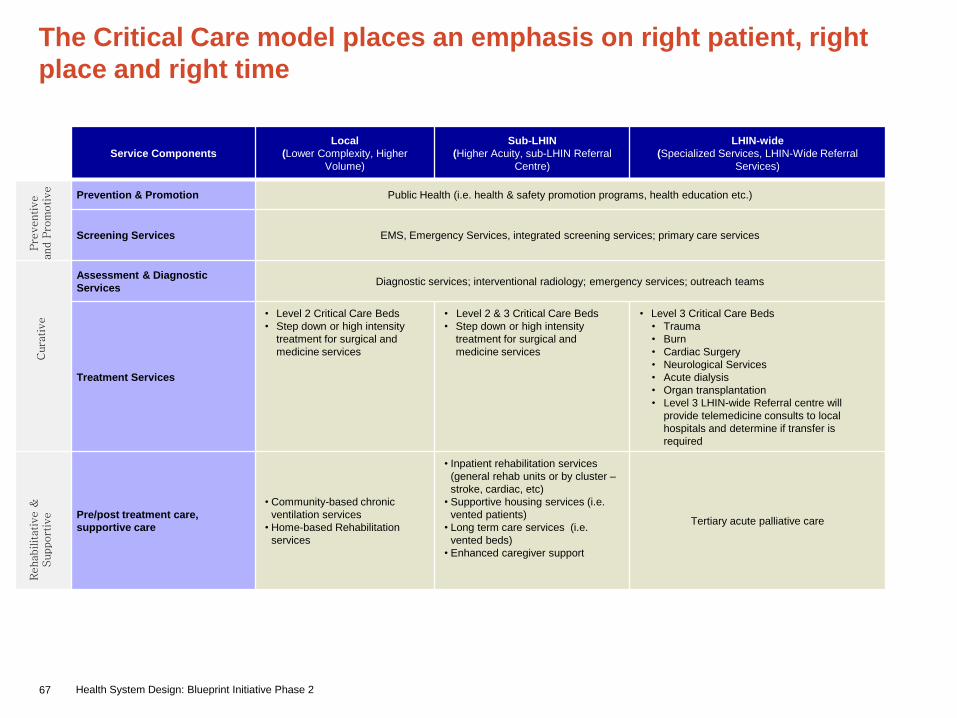
67 Health System Design: Blueprint Initiative Phase 2
The Critical Care model places an emphasis on right patient, right
place and right time
Service Components
Local
(Lower Complexity, Higher
Volume)
Sub-LHIN
(Higher Acuity, sub-LHIN Referral
Centre)
LHIN-wide
(Specialized Services, LHIN-Wide Referral
Services)
Prevention & Promotion Public Health (i.e. health & safety promotion programs, health education etc.)
Screening Services EMS, Emergency Services, integrated screening services; primary care services
Assessment & Diagnostic
ServicesDiagnostic services; interventional radiology; emergency services; outreach teams
Treatment Services
• Level 2 Critical Care Beds
• Step down or high intensity
treatment for surgical and
medicine services
• Level 2 & 3 Critical Care Beds
• Step down or high intensity
treatment for surgical and
medicine services
• Level 3 Critical Care Beds
• Trauma
• Burn
• Cardiac Surgery
• Neurological Services
• Acute dialysis
• Organ transplantation
• Level 3 LHIN-wide Referral centre will
provide telemedicine consults to local
hospitals and determine if transfer is
required
Pre/post treatment care,
supportive care
• Community-based chronic
ventilation services
• Home-based Rehabilitation
services
• Inpatient rehabilitation services
(general rehab units or by cluster –
stroke, cardiac, etc)
• Supportive housing services (i.e.
vented patients)
• Long term care services (i.e.
vented beds)
• Enhanced caregiver support
Tertiary acute palliative care
Cura
tive
Rehabilitative &
Support
ive
Pre
ventive
and P
rom
otive

68 Health System Design: Blueprint Initiative Phase 2
Implications of Critical Care services model of care
• A focus on patient / family preferences to determine
the appropriate use of critical care resources. The
community will be educated on the level of care
available at the local, sub-LHIN and LHIN-wide level
• A shift to LHIN-wide ownership of critical care beds
requiring collaboration, shared accountability and
transparency to ensure patients are in the right place
at the right time. This will require the development of
LHIN-wide definitions for beds, protocols for
stabilization & transport, and repatriation policies
• In making this shift, there will be a need to
balance the management of scarce resources
centrally while still enabling local access, i.e.
centrally managed pool for critical care beds.
Providers across the LHIN would need to have
visibility into these resources to not only
enable key processes such as scheduling and
monitoring availability, but manage locally to
provide access.
• Develop the Electronic Health Record to support
seamless transitions between hospitals, within
hospitals and from hospital to community
Providers Individuals/Families

69 Health System Design: Blueprint Initiative Phase 2
Surgical Services

70 Health System Design: Blueprint Initiative Phase 2
The model of care has been developed upon the guiding vision
elements and principles
Vision
Elements
• Maintain transparency and accountability
• Require patient/consumer accountability through empowerment and choice
• Deliver effective transitioning through the care continuum
• Provide equitable, appropriate access to care
• Enable the flow of the right information
• Provide evidence based, standardized care; „the right care, the right time‟
Principles
• Increase the patient‟s/consumer's ability to play an active role in the management
of their care
• Maximize the use of technology
• Ensure the efficient use of health human resources to increase the sustainability of
health human resources in the LHIN
• Equitable access regardless of geography
• Ensure that service capacity reflects population requirements
• Maximize utilization of the current system capacity
• Maintain an individual centered, high quality approach to care delivery
• Ensure critical volumes are maintained when distributing services in the LHIN

71 Health System Design: Blueprint Initiative Phase 2
• Single, unified point of access with
common referral standards / process
by specialty
• Consistent use of standardized care
pathway‟s across the LHIN
• Utilization of tertiary and non-tertiary
Centres of Excellence across the
LHIN to ensure that care is provided
closer to home when possible
Model of care emphasizes a centralized and coordinated point of
access to all surgical services across the LHIN
How is this model different from today’s service delivery model?
What are the benefits of the Model of Care?
Providers
• Improved capacity
utilization and
patient flow across
the LHIN
• Improved quality of
care through the
adoption of
standardized care
pathways from
screening,
assessment
through to
discharge
guidelines
What are the benefits of the Model of Care?
Individuals/ Families
•Improved equity,
timeliness and access
to care in the „right‟
place
•Increased choice for
individuals when it
comes to their care
delivery

72 Health System Design: Blueprint Initiative Phase 2
Overview of the Surgical Services model of care
BED CAPACITY AND AVAILABLE SERVICES DASHBOARD
ELECTRONIC HEALTH RECORD REPOSITORY
PATIENT / CAREGIVER INFORMATION AND EDUCATION
Capacity +
Patient C
hoic
e
PATIENT AND FAMILY
24 h
our
Local A
ssessm
ent
Navig
ation to P
ost-
Op C
are
•Information is collected at each
interaction point in the
continuum and entered into an
EHR repository
•Transportation infrastructure
and support is in place
throughout the continuum
4
4
The patient and their family‟s
first point of contact will be
local and available on a 24-
hour basis. This coordinated
centralized process will serve
to navigate the patient to the
right provider at the right
location.
1
1
CENTRES OF EXCELLENCE
LO
CA
LSub-LH
INLH
INPR
OV
INC
E
HIGHLY SPECIALIZED SURGICAL SERVICES
CORE, CRITICAL MASS SERVICES
HIGH VOLUME CORE SERVICES
The patient will be given the
information that is required to inform
them of the wait times and availability
of the required services across the
LHIN. The patient can balance factors
like wait times and location to make a
decision that works for them.
2
2
The patient will experience a
coordinated approach for
rehabilitation and supportive
service options, including health
promotion and prevention to
ensure smooth transition between
hospital and home/other HSP.
3
3
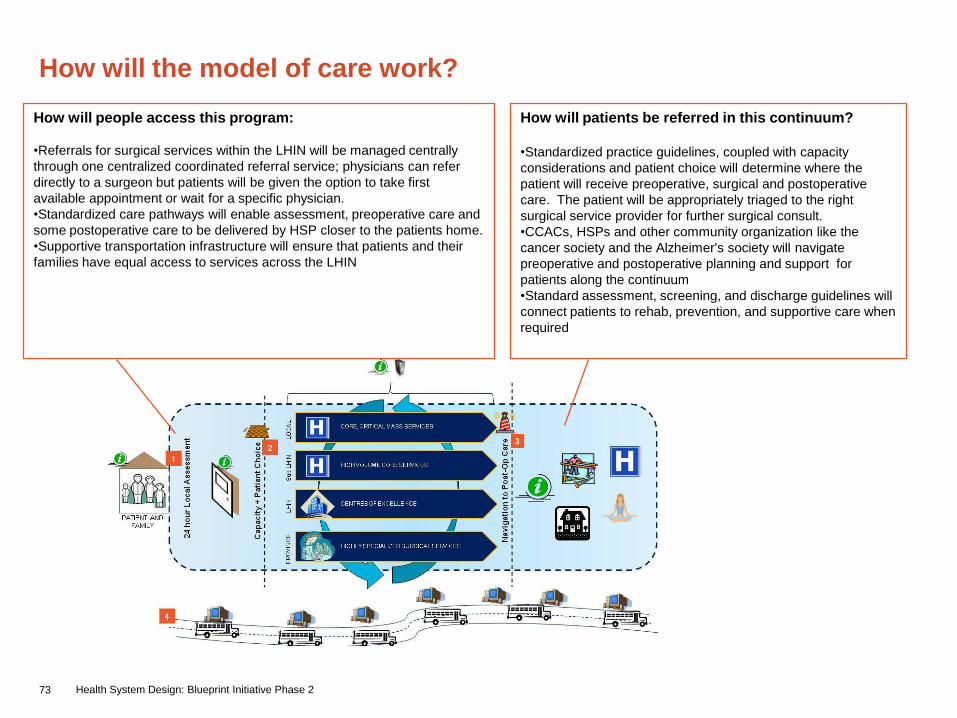
73 Health System Design: Blueprint Initiative Phase 2
How will the model of care work?
How will people access this program:
•Referrals for surgical services within the LHIN will be managed centrally
through one centralized coordinated referral service; physicians can refer
directly to a surgeon but patients will be given the option to take first
available appointment or wait for a specific physician.
•Standardized care pathways will enable assessment, preoperative care and
some postoperative care to be delivered by HSP closer to the patients home.
•Supportive transportation infrastructure will ensure that patients and their
families have equal access to services across the LHIN
How will patients be referred in this continuum?
•Standardized practice guidelines, coupled with capacity
considerations and patient choice will determine where the
patient will receive preoperative, surgical and postoperative
care. The patient will be appropriately triaged to the right
surgical service provider for further surgical consult.
•CCACs, HSPs and other community organization like the
cancer society and the Alzheimer's society will navigate
preoperative and postoperative planning and support for
patients along the continuum
•Standard assessment, screening, and discharge guidelines will
connect patients to rehab, prevention, and supportive care when
required
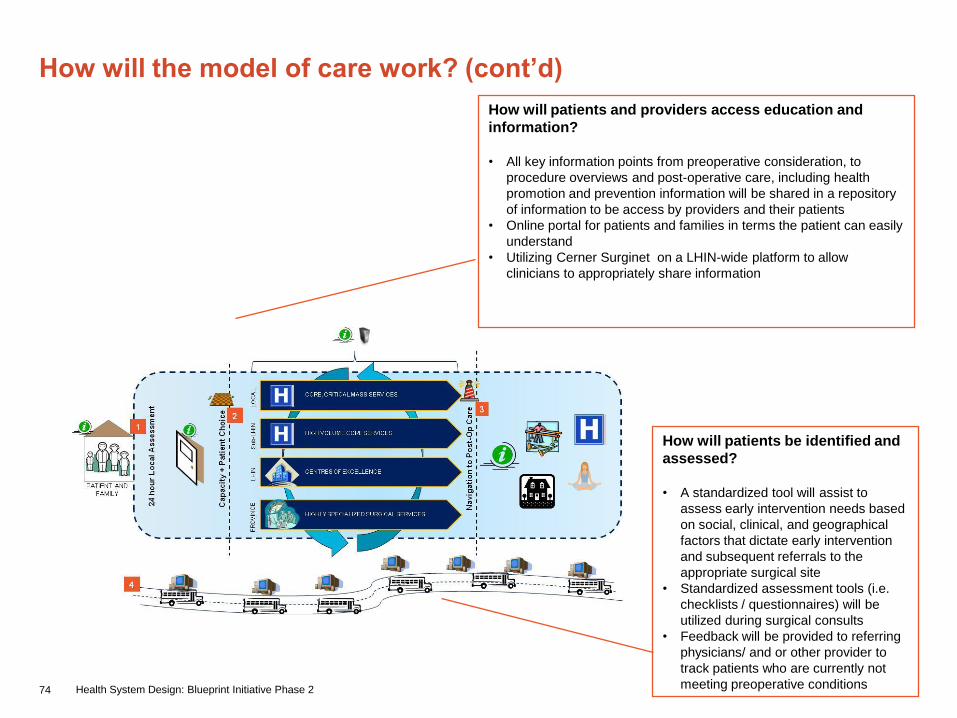
74 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
How will patients be identified and
assessed?
• A standardized tool will assist to
assess early intervention needs based
on social, clinical, and geographical
factors that dictate early intervention
and subsequent referrals to the
appropriate surgical site
• Standardized assessment tools (i.e.
checklists / questionnaires) will be
utilized during surgical consults
• Feedback will be provided to referring
physicians/ and or other provider to
track patients who are currently not
meeting preoperative conditions
How will patients and providers access education and
information?
• All key information points from preoperative consideration, to
procedure overviews and post-operative care, including health
promotion and prevention information will be shared in a repository
of information to be access by providers and their patients
• Online portal for patients and families in terms the patient can easily
understand
• Utilizing Cerner Surginet on a LHIN-wide platform to allow
clinicians to appropriately share information

75 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
What role will Surgical Services play in complementary care?
• Implement pre and postoperative guidelines as it relates to
complementary needs; including proactively engaging allied health
professionals (i.e. nutritional services) to support the elderly
population that require surgical intervention
• Ensure that there is consistent funding for and availability of
complementary care services based on population needs
How will Surgical Services care for specialized needs?
• Collaboration and coordination of case management resources
within the LHIN, the CCACs and other community support
organizations to better coordinate pre and postoperative care and
rehabilitation
• Health care professionals will work with patient support networks
where applicable to the patient‟s case
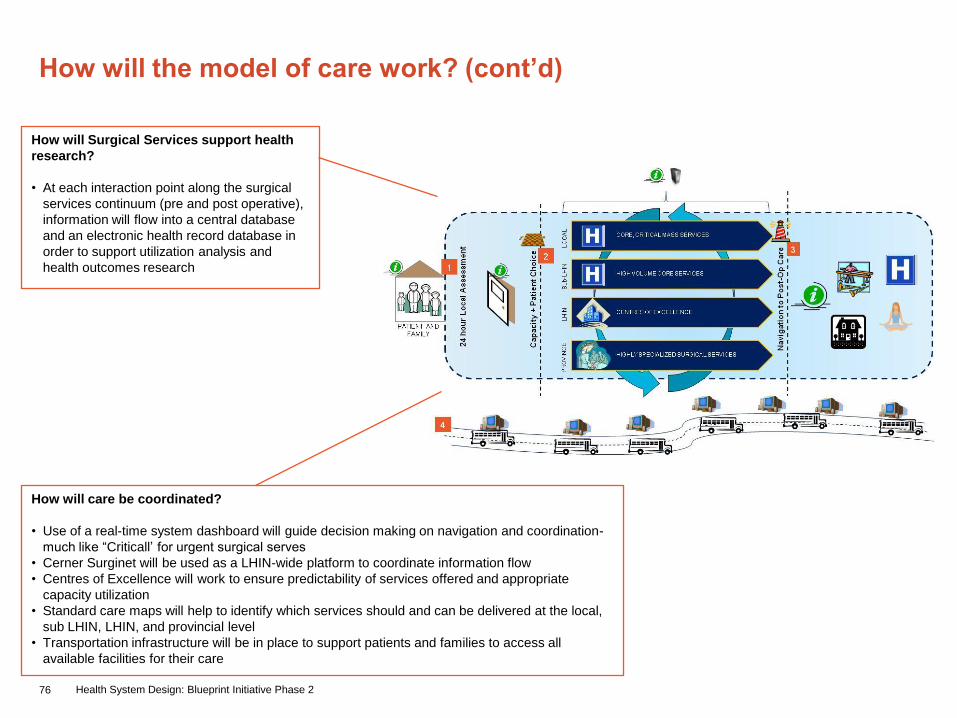
76 Health System Design: Blueprint Initiative Phase 2
How will the model of care work? (cont’d)
How will Surgical Services support health
research?
• At each interaction point along the surgical
services continuum (pre and post operative),
information will flow into a central database
and an electronic health record database in
order to support utilization analysis and
health outcomes research
How will care be coordinated?
• Use of a real-time system dashboard will guide decision making on navigation and coordination-
much like “Criticall‟ for urgent surgical serves
• Cerner Surginet will be used as a LHIN-wide platform to coordinate information flow
• Centres of Excellence will work to ensure predictability of services offered and appropriate
capacity utilization
• Standard care maps will help to identify which services should and can be delivered at the local,
sub LHIN, LHIN, and provincial level
• Transportation infrastructure will be in place to support patients and families to access all
available facilities for their care

77 Health System Design: Blueprint Initiative Phase 2
The Surgical Services model focuses on using tertiary and non-tertiary sites
to ensure timely, individualized, and appropriate care
Service Components Local Sub-LHIN LHIN-wide
Prevention &
Promotion
• Independent and guided
self health management
• Health promotion
• Online health information portals
Screening Services
• Self-navigation tools
• Outreach teams to encourage screening
(urologist teams, pre-cancer screening)
Assessment &
Diagnostic Services• Primary care services - Early identification, assessment,
treatment, and follow-up and management
• Pharmacy services
• Clinical case management services
• Decision-making support
• Core-hospital based services including:
• Inpatient and ambulatory, high volume/low acuity, surgical
services (i.e. General surgery, primary ortho surgery,
cataracts)
• Follow-up on inpatient / ambulatory care for individuals
who receive services in other hospitals(i.e. large
community, tertiary centres)
• Pain and symptom management services
• Shared care services with specialists and primary care
• Emergency services
• Early identification, assessment, treatment,
and follow-up and management
• Service coordination and clinical case
management for specialized/complex cases
(eligibility placements, care plans, coping
techniques, decision-making guidance etc)
• Core hospital-based and specialty services
including:
• Inpatient and ambulatory, moderate
volume/acuity, surgical services (i.e.
endoscopy, joint repairs, urology, vascular
surgery)
• Follow-up inpatient / ambulatory care for
individuals who receive services in other
hospitals (i.e. tertiary)
• Specialized diagnostic modalities not
available at the local level – interventional
radiology (i.e. MRI, CT)
• Tertiary and quaternary care (low
volume/high acuity) including:
• Burns, neurosurgery, thoracic
surgery, plastic, tertiary GI
services, organ transplantation, etc
• Education, research, and clinical
trials
• Telehealth and telemedicine services
• Specialized clinical case
management (personal coaching,
care plans, coping techniques,
intensive case management ,etc)
Treatment Services
Pre/post treatment
care, supportive
care
• Home-based Rehabilitation services
• In-home community support services
• Bereavement support
• Caregiver/Family support
• Peer support services
• Recreational and social programs for people with disabilities
• Service coordination services
• Home-based palliative services
• Respite care for caregivers/families
• Pre- and post- operative care
• Audiology services
• Inpatient rehabilitation services (general
rehab units or by cluster – stroke, cardiac,
etc)
• Supportive housing services
• Long term care services
• Enhanced caregiver support
• Highly specialized inpatient
rehabilitation beds (ABI,
neurosurgery, etc)
• Highly specialized outpatient rehab
services (ABI, spinal cord, etc)
• Tertiary acute palliative care
Cura
tive
Rehabilitative &
Support
ive
Pre
ventive a
nd
Pro
motive
Integrated Screening (colonoscopy, breast cancer,
etc)
Public health services
Primary and Secondary Prevention (eye health education
Patient and family /caregiver information and education

78 Health System Design: Blueprint Initiative Phase 2
Implications of Surgical Services model of care
• Increased surgical services capacity either at the
local or sub-LHIN level, reducing reliance on potential
need to travel and access London-based services
where appropriate
• Enabling “true self-management”, will require
individuals to have easy access to evidence-based
health information and inventory of health services
(i.e. online portal)
• A „Centres of Excellence‟ model for both tertiary and
non-tertiary services will require increased navigation
resources at each step in the care continuum and a
coordinated look at LHIN capacity
• Increased commitment to aligning rehabilitation and
support aspects of an individual‟s care will require the
development of practice guidelines specific to
surgical patients
• A single point of first access delivered locally to
individuals and their families will require 1) standard
guidelines for assessment and referral, and 2)
investment and development of a real time system
dashboard that tracks bed capacity and services
utilization.
• There will be a need to balance the management of
scarce resources centrally while still enabling local
access, i.e. centrally managed pool for surgical
services (beds and OR blocks). Providers across the
LHIN will need to have visibility into these resources
to enable key processes such as scheduling and
monitoring availability, but would be managed locally
to provide access.
Providers Individuals/Families