Embed Size (px)
Citation preview

www.npjournal.org The Journal for Nurse Practitioners - JNP 123
Health literacy has been identified by theInstitute of Medicine (IOM),1 World HealthOrganization (WHO),2 the Joint Com -
mission, and the Agency for Healthcare Research andQuality (AHRQ)3 as a significant problem impactinghealth outcomes. Health literacy is defined as “the degreeto which individuals have the capacity to obtain, process,and understand basic health information and servicesneeded to make appropriate health decisions.”4 Risk fac-tors for limited health literacy (LHL) include age, genet-ics, ethnic and racial minority, language, educationalstatus, socioeconomic status, and environment, whichincludes rural location and underserved areas.1
However, all segments of the population may experi-ence some health literacy challenges when trying to nav-igate the ever-increasing complex healthcare system. TheAgency for Healthcare Research and Quality (AHRQ)has released a toolkit to help make positive changes toimprove health literacy at the practice level. While thetopic of health literacy is not new, sadly, nursing’s contri-bution to the health literacy literature has been limited,
even though patient education and advocacy are a corefocus of nursing practice.
Nurses can play an instrumental role in promotingbetter understanding of health information and advocatefor interventions to promote health literacy and improvehealth outcomes. This article reviews the problem ofLHL and provides suggestions for evidence-based qualityimprovement that incorporates recommendations fromthe AHRQ toolkit.
Healthy People 2010 and the Healthy People 2020draft objectives5 provide a road map for the nation toachieve the goals of health promotion and disease pre-vention. The two comprehensive goals outlined in thedocument are to increase quality and years of healthy lifeand eliminate health disparities.6 Although still in draftform, Healthy People 20205 initiatives mirror concernfor provider and patient communication clarity, as well ascall for research to improve health communication. Toachieve the goals of reducing health disparities andextending the quality and quantity of life, changes inhealth behavior are often necessary. Health literacy has
ABSTRACTAlthough millions of Americans are able to navigate city streets, bus routes, andmalls, many do not have the skills to manage their health and negotiate our health-care system. Low formal education levels, older age, ethnic and racial minorities,rural location, and poverty are some factors associated with increased rates of limitedhealth literacy. Limited literacy impacts health behaviors, decisions, and, ultimately,outcomes. This article reviews health literacy research and discusses practical ways toimprove health literacy in practice, including the Agency for Healthcare Researchand Quality’s toolkit for health literacy.
Keywords: health literacy, health outcomes, patient education, providercommunication© 2011 American College of Nurse Practitioners
Health Literacy: The Road toImproved HealthOutcomesLaurie Anne Ferguson, DNP, APRN, ANP-BC, FNP-C, CPNP, and Roberta Pawlak, MS, PhD(c), RN

124 The Journal for Nurse Practitioners - JNP Volume 7, Issue 2, February 2011
been described as the “currency” for improving the qual-ity of US health, healthcare, and health outcomes.7 TheIOM has made the use of understandable health infor-mation one of its priorities.1
Today’s healthcare environment is complex and requiresincreased patient responsibility to navigate various systems,make health decisions, and follow therapeutic plans. Evenpeople who have above-average literacy may find navigationoverwhelming. Most health materials are written at higherlevels than most adults can understand. Low formal educa-tion levels, older age, ethnic minorities, rural location, andpoverty are associated with increased rates of LHL.7 This isboth an individual and population problem, therefore, inter-ventions must address both.
EPIDEMIOLOGYHealth literacy improvement is central in achieving the sixcomponents of high-quality healthcare outlined in theIOM’s report “Crossing the Quality Chasm”: safety, effec-tiveness, efficiency, timeliness, patient centeredness, andequitable treatment.8 Illiteracy, or the inability to read, con-tributes to LHL. However, health literacy includes thebroader definition of being able to manage personal health.It is estimated that only 12% of the 228 million US adultshave the skills to manage their own healthcare adequately.9
LHL is associated with lower use of preventive services,increased hospitalizations, and poorer health outcomes.10-12
Health disparities are exacerbated by a complex healthcaresystem, aging populations, low health literacy rates, andincreasing rates of chronic diseases.13
Several system-level factors contribute to the problemof limited literacy. Contributory factors include medica-tion complexity, short office visits, increased self-caredemands, care fragmentation, and insurance paperwork.14
Today’s healthcare system requires patients to takeincreasingly more responsibility for managing theirhealth. The challenges increase as treatment decisions aremore and more complex. Within the framework of com-plexity, LHL has been found to relate to delayed diag-noses, poor adherence to treatment regimens, andincreased morbidity and mortality.15,16 Treatment regi-mens require more time and explanation and are oftendifficult in busy primary care practices. Dischargeinstructions and patient education materials may be diffi-cult for patients to understand. Treatment adherence andpatient follow-up, which are often inadequate, areimpacted by LHL.
Primary providers are often charged with the role ofgatekeeper to direct and coordinate an individual’s care.However, patients may see numerous specialists. Plans ofcare may not be effectively communicated between spe-cialists and generalists, thus contributing to duplicateservices and medication errors. Patient/provider commu-nication breakdown is compounded when the patient hasLHL skills, as the patient often relays informationbetween providers. For example, the patient may notunderstand the reason or necessity for referral, and there-fore a comprehensive evaluation does not occur or,worse, misinterpretation causes errors to ensue.
Patient access to care may also be hampered by com-plicated insurance application, referral, and reimburse-ment forms. Consent forms developed for provider legalprotection may not readable and understandable by thepatient. Therefore, consent forms may not truly provideinformed consent.
Providers frequently make broad assumptions abouttheir patient’s ability to comprehend information.Graduating from high school, for example, does not guar-antee a patient can read at a 12th-grade level. A 5th- to6th-grade reading level is recommended for most patient-education materials.17 Cotugna, Vickery, and Carpenter-Haefele18 found that half of health-education materialsreviewed were written above the 8th-grade level.Healthcare providers often use medical jargon, which is aforeign language to people outside of health services. Inaddition, the fast pace of busy primary care practices doesnot allow adequate time to assess and improve patients’understanding. LHL is also confounded by cultural andlanguage differences in the US. Furthermore, manyproviders have not been educated in ways to enhancepatients’ understanding.
However, health literacy is not just about written mate-rials; health literacy is also about accessing healthcare andpreventive services, understanding diagnoses and treatmentregimens, and possessing the ability to act on health infor-mation to improve overall health (Figure 1).19,20
IMPACT OF LHLThe consequences of LHL result in declines in ournation’s health status. LHL is associated with increasedrates of hospitalization and poorer health outcomes.21
According to the IOM’s report, “Health Literacy: aPrescription to End Confusion,”1(p. 81) LHL consequencesinclude increased economic costs in health services,

www.npjournal.org The Journal for Nurse Practitioners - JNP 125
higher societal costs, and increased burden of human suf-fering and disease. In addition, LHL may increase stressfrom the shame and stigma of illiteracy, which decreasesself-efficacy and increases psychological burden.
LHL is associated with limited health knowledge,higher rates of chronic disease, and decreased use of pre-ventive services.21 A higher risk of death is related toLHL.12 From an epidemiological perspective, the risk ofincreased mortality from limited literacy is the same asthe impact of chronic disease.22 The risk is further com-pounded when individuals have chronic health problems,leading to greater burden of illness on individuals andtheir families. LHL is associated with lower use of pre-ventive services, such as immunizations and cancerscreenings. Individuals may lack knowledge of signs andsymptoms of disease or delay seeking evaluation becauseof no insurance or a distrust of healthcare providers.23-25
In addition, people with LHL may have difficulty findingtheir way in healthcare facilities or simply not have accessto transportation.15
LHL negatively impacts a parent’s ability to correctlycomplete insurance forms, understand over-the-countermedication labels, and administer medications correctly.26
Parents with LHL are more likely to have children whoare not covered by health insurance.23 Improving healthliteracy increases child health promotion by positivelyimpacting modifiable risk factors, such as injury preven-tion, nutrition and obesity, tobacco use, and maternalmental health.27
Medication adherence is known to positively impacthealth outcomes. Misinterpretation of medicationinstructions, however, is common with individuals withlow health literacy and leads to poor adherence. Bailey etal28 found LHL was associated with incorrect medicationdosing or administration errors in over 28% of subjectssurveyed. The most frequent mistakes were with dosagemeasurement and the frequency of medication adminis-tration. Pictograms for medication counseling may bevery effective in reducing medication errors and improv-ing medication adherence among an LHL population.29
Communication in patient encounters is a providerresponsibility. Patient health literacy capabilities are linkedto health outcomes. The use of medical jargon often resultsin decreased patient understanding.30 Unfortunately,providers often overlook communication needs and rarelyassess patient recall or comprehension.31
Health literacy can be considered a determinant ofhealth because it influences patient access, communication,decisions, and treatment adherence.32 Health disparity pat-terns tend to parallel rates of limited health literacy.33 Theproblem of LHL is costly for society.22 Improvement inindividual health literacy decreases health disparities andimproves the health of the overall population.
IMPACTING HEALTH OUTCOMESImproving health literacy requires interventions toimprove patients’ understanding and behavior, providercommunication, and the skills required to navigate
Figure 1. Determinants of health literacy: a determinant of population health (adapted15,19,20,32).
PersonalFactors
Age
Genetics
Language
Race &Ethnicity
Education
SES
SystemFactors
Medications
Time
Self-care
Fragmentationof Care
Insurance
Paperwork
AccessibleHealthcare
AppropriateHealthcare
UniversalPrecautions
EnhancedProviderCommunications
InformedConsumer
TreatmentAdherence
HealthLiteracy
ReducedHealth
Disparities
IMPROVEDPOPULATION
HEALTH

126 The Journal for Nurse Practitioners - JNP Volume 7, Issue 2, February 2011
complex healthcare systems. All patients should be pre-sumed to have LHL, and a “universal precautions”approach should be followed, as suggested by Paasche-Orlow and Wolf (Figure 1).15 Applying universal pre-cautions for this population places the burden on theclinician to routinely assume there is LHL. Universalprecautions means that patient-education needs to be acentral priority in every patient encounter.
Sadly, the healthcare provider has few incentives tospend time educating patients when insurance plans reim-burse based upon procedures and diagnoses. The “medical-ization” of health status problems assumes the solutions areincreased “medical care” when the solution may be inimproving patient education and health literacy. Healthcareneeds to shift from an exclusively medical focus on healthstatus problems to include social and economic causes ofpoor health status and health disparities.34
Improved patient knowledge improves health literacy.Printed material should be written in a clear, culturallysensitive manner at the 5th-grade level or lower.17 Theuse of technology can convey complicated ideas by pic-tures, video, and multimedia, which transcend the spokenand written word and provide opportunities to bridgethe divide of limited health literacy.35,36
CLINICAL INTERVENTIONSTwo interventions for promoting better understanding inpatients with low literacy are Ask Me 3™37and the Teach-Back Method.38 Ask Me 3, which is endorsed by theAmerican Medical Association Foundation, is a tooldesigned to promote better communication. The tool,which is also available in Spanish, encourages patients toask the following three questions of their provider:39
• What is my main problem?• What do I need to do? • Why is it important for me to do this? The Teach-Back Method, also called closing the loop
or show me, is a method to assess patients’ understandingof their illness and its treatment. Illiterate patients may relyheavily on spoken instructions, demonstration, and pic-tures. Using everyday language, the healthcare providerprovides information and has the patient repeat back ordemonstrate what has been taught.38
It is interesting to note that nurses have long used ateach-back approach that they call return demonstration.Strategies for improving communication with patientswith LHL include asking open-ended questions and
using pictures and demonstrations. Culturally sensitiveand easy-to-understand language is critical to enhancingpatient understanding. Providers should assess the qualityof the educational materials they provide for clarity andunderstandability, not simply legal compliance. Whileassessing literacy is a basic requirement, health literacyneeds are more comprehensive and require not onlyreading comprehension but understanding how to applythat knowledge to managing one’s healthcare.
Ironically, medications are approved by the US Foodand Drug Administration only after extensive research,yet written materials do not have a similar evaluationprocess for approval and use.40 Assessing whether educa-tional materials have a clear, concise message and usesimple terms may be additionally enhanced by the use ofpictures and other media, such as videos or DVDs. Manypatients do not have the skills or ready access to websitesand electronic media, but providers can increase access bydownloading simplified materials for distribution.
Other techniques for improving health literacy in theclinical setting include limiting the number of items ortopics discussed at one encounter to improve compre-hension.41 The use of one- to two-syllable words tocommunicate information, along with avoiding medicaljargon, is necessary to improve understanding and subse-quently adherence. Reviewing key points using variousmodes improves communication and understanding.Educational pamphlets with lots of pictures combinedwith a short video/DVD can improve comprehension ofcomplicated topics.
A simple strategy of casually handing patients printedmaterials that are upside down can reveal those who cannotread without causing embarrassment. Instructions on pre-scriptions should include the reason for taking the medica-tion and how often to take it in specific terms. Expertssuggest avoiding the usage of terms like BID or TID. A spe-cific time for medication to be taken should be written onthe prescription (instead of morning, afternoon, and night).For instance writing 8 a.m. and 8 p.m. or 8 a.m., 2 p.m., and10 p.m. make directions less ambiguous.
Effective education materials must also be culturallysensitive. One size does not fit all; effective patient educa-tion materials in one setting may not be understood inanother (see Figure 2 for examples).
At the population level, effective approaches forimproving health literacy need to be interdisciplinary andoccur in many settings, including venues outside healthcare.

www.npjournal.org The Journal for Nurse Practitioners - JNP 127
Health programs need to incorporate instruction on healthpromotion and disease prevention along with teaching skillson how to navigate the healthcare system and improvedecisions about personal health.
The 2010 AHRQ publication, “Health LiteracyUniversal Precautions Toolkit,”42 outlines specific stepsfor assessing practice and suggestions for tools to beimplemented to improve health literacy for all patients.The toolkit contains background information on healthliteracy, tools to assess a practice’s current health literacysensitivity, and resources that can be easily downloadedand implemented into practice. Four focus areas areaddressed to improve health literacy in practice: improvedspoken communication, improved written communica-tion, improved self-management and empowerment, andimproved supportive systems.
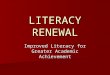
To improve health outcomes, practices need a structuredapproach to assess and make positive changes. The toolkitdiscusses access, knowledge, and behavior as specific factorsto improve health outcomes and the tools to assist withimplementing it in practice (Figure 3). Specifically, thetoolkit provides suggestions for evaluating a practice andincorporating specific interventions, including choosing sig-nage, navigating the system, reinforcing medication regi-mens, and incorporating video/DVD technology as anintervention for patient education.
The task of assessing a practice can seem over-whelming, but the toolkit advocates implementingone or two strategies at a time. For instance, one fairly
simple strategy is to give every patient a brown paperor zipper-top plastic bag with instructions to bring itto every visit filled with all their current over-the-counter and prescribed medications. Reviewing anychanges in medications between visits often providessurprising insight. A specific ICD-9 code (V58.69)found in the AHRQ toolkit to bill for medicationreview provides incentive for practices to incorporatethis simple intervention.
Another strategy that’s easy to implement is to pro-vide maps or directions to the office of specialists towhom patients are commonly referred. These maps canreduce confusion and improve navigation of the health-care system. Specific tools for assessing health literacy, aswell as resources to assess the quality of written educa-tional materials, can be found in Figure 4.
Figure 2. Features of a good handout. Adapted from Doak
CC, Doak LG, Root JH. Teaching patients with low
literacy skills. 2nd ed. Philadelphia: J.B. Lippincott,
1996.
• Use pictures
• Focus on a central message
• Emphasize key points by highlighting, coloring, orunderlining text
• Use lots of white space
• Use fonts sized 12 or larger
Figure 3. Health Literacy Universal Precautions Toolkit.42
Access Knowledge Behavior
Transportation
Insurance
Scheduling
Support Systems
Medical Information
Communication
Understanding
Language/Culture
Tools to Improve
Supportive
Systems
Self-efficacy
Adherence
Self-care
Social Reinforcement
Tools to Improve
Spoken and Written
Communication
Tools to Improve
Self-management
and Empowerment
Improved
Health
Outcomes

Figure 4. Tools to Help Healthcare Providers Identify and Address Patients with Low Health Literacy
Identify Health Literacy Issues Address Health Literacy Issues
Address practice patterns and reduce barriers • Don’t assume anything!
• Ask the patients about their understanding, how they best learn,and then apply the given input
• Investigate alternative practice patterns to allow more time toreinforce teaching (perhaps lower level provider, once educationprovided by APN)
• Have admissions or clerical personnel explain and help completeforms
• Consider application of interdisciplinary team, case management,or medical home models (share and coordinate information)
• Apply advocacy skills
• Provide simple maps for navigation
• Match delivery of message to patient’s means, ability, and culture
Assess communication with patients • Determine resources need to reduce language and culturalbarriers
• Use everyday language, and not medical jargon
• Reinforce risks and benefits of treatment adherence
• Ask open-ended questions when possible
• Assign specific times to medications and treatments (avoid TID,BID, etc.)
• Limit amount of information given in one encounter
• Design materials with a clear, concise message
• Apply multiple means to convey information: verbal, written,demonstrations, pictograms, videos, multi-media, computersoftware, story-telling
Assess patient comprehension, recall, and ability Confirm understanding of information and patient ability by usingAsk Me 3™ and Teach-Back Methods
Return explanations
Return demonstrations
Additional resources
• AHRQ Health Literacy Universal PrecautionsToolkithttp://www.ahrq.gov/qual/literacy/
• Healthfinder.govhttp://nifl.gov/mailman/listinfo/healthliteracy
• US Department of Health & Human Serviceshttp://www.healthfinder.gov
• Online course in health literacywww.hrsa.gov/healthliteracy/training.htm
• Health literacy listserv http://nifl.gov/mailman/listinfo/healthliteracy
• Plain language thesauruswww.nphic.org/files/editor/file/thesaurus_1007.pdf
Additional resources
• Ask Me 3™http://www.npsf.org/askme3/
• Teach-Back Methodhttp://www.nchealthliteracy.org/toolkit/tool5.pdf
• Guide for developing print materialswww.nci.nih.gov/aboutnci/oc/clear-and-simple/page1
• Online readability calculatorwww.wordscount.info
• Health Literacy Translations Toolkithttp://www.hablamosjuntos.org/mtw/default.toolkit.asp
128 The Journal for Nurse Practitioners - JNP Volume 7, Issue 2, February 2011

CONCLUSIONLHL impacts the most vulnerable segments of the popu-lation. While some populations are at increased risk, allindividuals at one time or another may be affected byLHL. The stress of a new diagnosis and information over-load can contribute to limitations in health literacy andlead to poor health outcomes. Improving health literacyis a critical goal in improving health outcomes.Healthcare providers can make a positive impact inimproving health outcomes by critically assessing clinicalpractice and working to improve communication, knowl-edge, behavior, and access.
References
1. Nielsen-Bohlman L, Panzer AM, Kindig DA, eds. Health literacy: a prescription toend confusion. Washington DC: National Academies Press; 2004.
2. World Health Organization. Health literacy and health behavior. http://www.who.int/healthpromotion/conferences/7gchp/track2/en/. Accessed December 9, 2010.
3. Agency for Healthcare Research and Quality. 2007 National HealthcareDisparities Report. Rockville MD: The Agency; 2008.
4. Ratzan SC, Parker R. Introduction. In: Selden CR, Zorn M, Ratzan SC, ParkerRM, eds. National Library of Medicine Current Bibliographies in Medicine:Health Literacy. Bethesda MD: National Institutes of Health; 2000.
5. U.S. Department of Health and Human Services. Healthy People 2009 DraftObjectives. http://www.healthypeople.gov/. Updated 2009. Accessed October10, 2010.
6. U.S. Department of Health and Human Services. Healthy People 2010.Washington DC: U.S. Government Printing Office; 2000.http://www.healthypeople.gov/Document/pdf/uih/2010uih.pdf. UpdatedNovember 2000. Accessed April 1, 2010.
7. Paasche-Orlow MK, Parker RM, Gazmararian JA, Nielsen-Bohlman LT, RuddRR. The Prevalence of Limited Health Literacy. JGIM. 2005;20(2):175-184.
8. Abrams MA, Klass P, Dreyer BP. Health literacy and children: Recommendationsfor action. Pediatrics. 2009;124:S327-S331.
9. Agency for Healthcare Research and Quality. 2007 National HealthcareDisparities Report. http://www.ahrq.gov/qual/nhdr07/nhdr07.pdf. UpdatedNovember 2008. Accessed April 1, 2010.
10. Baker DW, Wolf MS, Feinglass J, Thompson JA, Gazmararian JA, Huang J.Health literacy and mortality among elderly persons. Arch Intern Med.2007;167(14):1503-1509.
11. DeWalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy andhealth outcomes. JGIM. 2004;19(12):1228-1239.
12. Sudore RL, Yaffe K, Satter Field S, et al. Limited literacy and mortality inthe elderly the health, aging, and body composition study. JGIM.2006;21(8):806-812.
13. Parker RM, Ratzan SC, Lurie N. Health literacy: a policy challenge foradvancing high-quality health care. Health Aff. 2003;22(4):147-153.
14. Weiss BD, Mays MZ, Martz W, et al. Quick assessment of literacy in primarycare: the newest vital sign. Ann Fam Med. 2005;3(6):514-522.
15. Paasche-Orlow MK, Wolf MS. The causal pathways linking health literacy tohealth outcomes. Am J Health Behav. 2007;31:S19-26.
16. Wolf MS, Davis TC, Shrank W, et al. To err is human: Patient misinter -pretations of prescription drug label instructions. Patient Educ Counseling.2007;67(3):293-300.
17. Communicating with patients who have limited literacy skills: report of theNational Work Group on Literacy and Health. J Fam Pract. 1998;46(2):168.
18. Cotugna N, Vickery CE, Carpenter-Haefele KM. Evaluation of literacy level ofpatient education pages in health-related journals. J Comm Health.2005;30(3):213-219.
19. Evans RG, Stoddart GL. Consuming research, producing policy? Am J PublicHealth. 2003;93(3):371-379.
20. Evans RG, Stoddart GL. Producing health, consuming health care. Soc SciMed. 1990;31(12):1347-1363.
21. Berkman ND, Chen J, Soroui JS, White S. Literacy and health outcomes.Summary, Evidence Report/Technology Assessment No. 87 AHRQ.http://www.ahrq.gov/clinic/epcsums/litsum.pdf. Updated January 2004.Accessed April 1, 2010.
22. Volandes AE, Paasche-Orlow MK. Health literacy, health inequality and a justhealthcare system. Am J Bioethics. 2007;7(11):5-10.
23. Bennett I, Chen J, Soroui JS, White S. The contribution of health literacy todisparities in self-related health status and preventative health behaviors inolder adults. Ann Fam Med. 2009;7:204-211.
24. Herman AD, Mayer GG. Reducing the Use of emergency medical resourcesamong Head Start families: a pilot study. J Comm Health. 2004;29(3):197-208.
25. Herman AD, Young KD, Espita, D et al. Impact of a health literacyintervention on pediatric emergency department use. Pediatr Emerg Care.2009;25:434-438.
26. Yin HS, Johnson M, Mendelsohn AL, Abrams MA, Sanders LM, Dreyer BP.The health literacy of parents in the United States: a nationallyrepresentative study. Pediatrics. 2009;124(Supplement_3):S289-298.
27. Sanders LM, Shaw JS, Guez G, Baur C, Rudd R. Health literacy and childhealth promotion: implications for research, clinical care, and public policy.Pediatrics. 2009 2009;124(Supplement_3):S306-314.
28. Bailey SC, Pandit AU, Yin, S et al. Predictors of misunderstanding pediatricliquid medication instructions. Fam Med. 2009;41:715-721.
29. Yin HS, Dreyer BP, van Schaick L, Foltin GL, Dinglas C, Mendelsohn AL.Randomized controlled trial of a pictogram-based intervention to reduceliquid medication dosing errors and improve adherence among caregiversof young children. Arch Pediatr Adolesc Med. 2008;162(9):814-822.
30. Castro CM, Wilson C, Wang F, Schillinger D. Babel babble: physicians’ use ofunclarified medical jargon with patients. Am J Health Behav. 2007;31:S85-95.
31. Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physiciancommunication with diabetic patients who have low health literacy. ArchIntern Med. 2003;163(1):83-90.
32. Pawlak R. Economic considerations of health literacy. Nurs Econ.2005;23(4):173-180.
33. Bodie GD, Dutta MJ. Understanding health literacy for strategic healthmarketing: eHealth literacy, health disparities, and the digital divide. HealthMarketing Q. 2008;25:175-203.
34. Lantz PM, Lichtenstein RL, Pollack HA. Health policy approaches to populationhealth: the limits of medicalization. Health Aff. 2007;26(5):1253-1257.
35. Barry MJ. Health decision aids to facilitate shared decision making in officepractice. Ann Intern Med. 2002;136(2):127-135.
36. Woolf SH, Chan ECY, Harris R, et al. Promoting informed choice:transforming health care to dispense knowledge for decision making. AnnIntern Med. 2005;143(4):293-300.
37. Partnership for Clear Health Communication at the National Patient SafetyFoundation. 2008. http://www.npsf.org/askme3/PCHC/. Accessed October 15,2010.
38. Wilson FL, Baker LM, Nordstrom CK, Legwand C. Using the teach-back andOrem’s self-care deficit nursing theory to increase childhood immunizationcommunication among low-income mothers. Issues Comprehen PediatrNurs. 2008;31(1):7-22.
39. Cassey MZ. Building a case for using technology: health literacy and patienteducation. Nurs Econ. 2007;25(3):186-188.
40. Panel 1: Health literacy, literacy, and health outcomes. Washington, DC:Surgeon General’s Workshop on improving health literacy; 2006.http://www.surgeongeneral.gov/topics/healthliteracy/panel1.htm. AccessedDecember 9, 2010.
41. Hironaka LK, Paasche-Orlow MK. The implications of health literacy onpatient-provider communication. Arch Dis Childhood. 2008;93(5):428-432.
42. Health Literacy Universal Precautions Toolkit. Rockville, MD: Agency forHealthcare Research and Quality. http://www.ahrq.gov/qual/literacy/.Updated April, 2010. Accessed October 15, 2010.
Laurie Anne Ferguson, DNP, APRN, ANP-BC, FNP-C,CPNP, is an associate professor at Loyola University in NewOrleans and practices as a family nurse practitioner in ruralLouisiana. She can be reached at [email protected]. RobertaPawlak, PhD-C, RN, a doctoral candidate at the University ofWisconsin-Madison studying nursing and population health sci-ences, is an assistant professor and graduate program director atEdgewood College in Madison, WI. In compliance with nationalethical guidelines, the authors report no relationships with businessor industry that would pose a conflict of interest.
1555-4155/11/$ see front matter© 2011 American College of Nurse Practitionersdoi:10.1016/j.nurpra.2010.11.020
www.npjournal.org The Journal for Nurse Practitioners - JNP 129