Embed Size (px)
DESCRIPTION
health law to tackle vague diseases
Citation preview

154 lsjm 30 november 2009 volume 01

155lsjm 30 november 2009 volume 01
You are warmly welcomed to the Health Law & Ethics section of The LSJM’s second edition. We address a crucial component of medical disciplines across the board, tackling the ethics and policies behind controversial issues that affect all healthcare professionals and the public that we serve. In a society where the delivery of healthcare is inseparable from the complex world of politics, it is essential for us to question medical practice, from the point of our personal morality through to national legislation. We may find our traditional philosophies and the relevance of the Hippocratic Oath challenged in the growing face of medical innovation and technology. The issue of medical confidentiality is one that has received prominent attention and confrontation in recent times, but which has a longstanding and variable course through history that has largely not been looked at. An apparent progression has been seen from the paternalistic, physician-centred doctor’s oath, to a focus on the autonomy and rights of the individual. Nevertheless, the importance of respecting patient confidentiality was established at the very birth of modern medicine, with Hippocrates’ pledge “whatsoever I shall see or hear in the course of my profession, as well as outside my profession in my intercourse with men, if it be what should not be published abroad, I will never divulge, holding such things to be holy secrets”. 1 While he championed acting in the patient’s best interests, “never with a view to injury and wrongdoing”, there were no clear boundaries as to what would legally constitute a violation of the oath. It was a decision almost solely attributed to the individual physician, and concerns about negative gossip affecting patient confidence were part of the consideration. Similar versions of the oath were published throughout Europe in following centuries. In the 1700’s, John Gregory, a professor at Edinburgh University, published a paper, stating his concerns of the power that doctors had over their patients, the lack of professionalism and regularity in the profession, and that the protection and rights of patients were not of primary importance. He took a sympathetic view of the plights of patients, advocating women in particular and was to become influential in the reform of medical ethics at the time.2 In 1803, Thomas Percival was to become another influential figure in modern medical ethics, with a publication designed to guide the conduct of new physicians who had signed up at a Manchester Hospital during a taxing outbreak of typhus fever. He endorsed consulting with patients “in a tone of voice which cannot be overheard”, strictly observing “secrecy”, and using the knowledge gained in such consultations “with discretion... and the most scrupulous regard to fidelity and honour”. A similar policy was then incorporated into the first American Medical Association’s ethical code in 1846.2 Furthermore, a century later in 1948, the World Medical Association’s Declaration of Geneva published that “A doctor owes to his patient absolute secrecy on all which has been confided to him or which he knows because of the confidence entrusted to him”. 3 Here we start to see the disparity between recent changes to confidentiality laws, where the duty of the physician to a wider population has shifted to largely eclipse the absolute duty of physician to patient. A landmark case in 1971 saw a British physician, Dr. Robert Browne, appear before a disciplinary hearing of the General Medical Council for charges of serious professional misconduct, due to breaching patient confidentiality by informing a 16 year old girl’s parents that their daughter was taking the oral contraceptive pill.1 His defence centred on his belief that his decision had considered the possible adverse emotional impacts on the patient, the hazards of the drug, his belief that her parents -with whom he was familiar - would be most able to counsel her in this situation, and that in the spirit of Hippocrates’ Oath, his only interest was in what he believed was best for her. He was contentiously ruled as not guilty, due to a recognition that cases must be judged individually, and that it must considered that in some situations the disclosing of confidence may benefit the patient. In light of the case, the British Medical Association’s 1959 Code of Ethics was amended from, “It is a practitioner’s obligation to observe the rule of professional secrecy by refraining from describing voluntarily without the consent of the patient (save with statutory sanction) to any third party, information which he has learnt in his professional relationship with the patient”, to include that, “If in the opinion of the doctor, disclosure of information to a third party seems to be in the best medical interest of the patient, it is the doctor’s duty to make every effort to allow the information to be given to the third party, but where the patient refuses, that refusal must be respected”.1 The complexity of 21st century medical systems, which require and involve communication between physicians and multiple health disciplines, the availability to appropriate staff of medical records, issues of valid consent, and the need to address social issues, has realised the obsoleteness of some of the traditional views. Flexibility has particularly been required with at-risk or vulnerable groups, involving situations of abuse, sexual health and communicable diseases. A recent change in the GMC guidelines has sanctioned the release of certain information to the police regarding knife crime (see HLE News), and not solely gun crime as was previously the case, anticipating that increased statistics of the when and where’s of violent crime will aid police work and be in the interests of the safety of the public at large.4 What’s at stake here is a compromising of the fundamental bond of trust between doctor and patient. It will be a matter of treading that fine line between the physician’s duty to warn and duty to protect. Sandra Sadoo Section Editor Health Law & Ethics
ReferencesThe Genuine Works of Hippocrates. Trans. Francis Adams (1886). Vol. 2, 344-51. Rachel McAdams and Mark Skippen. The Eleventh Wellcome Trust Regional Forum for the History of Medicine in Scotland. Available from: 2. http://www.gla.ac.uk/departments/historymedicine/conferencesandpublications/eleventhwellcometrustregionalforumDeclaration of Geneva (1948). Adopted by the General Assembly of World Medical Association at Geneva 3. Switzerland, September 1948. Available from: http://www.cirp.org/library/ethics/genevaDoctors must report knife crime’. (2009) BBC News. Available from: http://news.bbc.co.uk/1/hi/uk/8276609.stm4.
EDITORIAL
Illu
stra
tion
: Ella
Bee
se

156 lsjm 30 november 2009 volume 01
NEWS
Statistics on late abortions (performed after 24 weeks gestation) held by the Department of Health (DoH) may soon be made public, as ruled by the Information Commissioner. The legal and ethical battle was sparked again as the Pro Life Alliance requested the data under the Freedom of Information Act and was originally turned down.
Since the Jepson case six years ago over the abortion of a child with a cleft lip and palate, the DoH have ceased publishing full statistical information on late stage abortions due to foetal abnormality, as this case led to the doctor being identified and pursued.
Under the 1967 Abortion Act, abortions after 24 weeks may be terminated up until birth, if there is evidence of a serious mental or physical risk to the mother or foetus. However, anti-abortion groups have argued that a cleft-lip, club foot, and other such malformations do not constitute “serious” abnormalities.
The DoH lawyers are concerned about releasing such information deeming it “sensitive, personal, and private”. Julie Bentley, CEO of the Family Planning Association released a joint statement with Brook stating that they were “dismayed” by the decision of the Information Commissioner, adding that the potential for individual women and doctors who carry out the procedure to be identified is worrying and unethical.
Although the Information tribunal has said that it is very unlikely for patients and doctors to be identified from the statistics alone, an internal review conducted by the DoH showed that the numbers were very small, and since such abortions are rare, the information should not be released to protect identities. Pro Life Alliance barrister Paul Diamond maintains that statistics do not constitute personal data, and that transparency is necessary to satisfy public interest in this controversial medical practice.
There are fears that the availability of such information will move Britain towards the US-style targeting of doctors who carry out abortions, and give anti-abortion campaigners ammunition to put pressure on individual women and doctors. The DoH will consider the implications of this judgment and may lodge an appeal with the High Court. Whether or not the release of such information will prevent future “unlawful killings”, or violate the privacy individual doctors and families, remains to be seen, as the issue of late abortion continues to tread a fine legal and ethical line.
ReferencesThe UK Statute Law Database. Abortion Act 1967 (c. 87). 1. Westminster: Office of Public Sector Information. [cited 2009 Oct 24]. Available from: http://www.statutelaw.gov.uk/content.aspx?activeTextDocId=1181037Dreaper, J. Late abortions data to be public. (2009) BBC News. 2. Available from: http://news.bbc.co.uk/1/hi/health/8309432.stmBoseley, S. Confidentiality fear over late abortion data. (2009) 3. The Guardian. Available from: http://www.guardian.co.uk/society/2009/oct/16/pro-life-alliance-abortion-jepson-case
MPs have approved an amendment to the Health Bill, meaning that England, Wales and Northern Ireland are all one step closer to sanctioning the removal of cigarettes from public display, including the outlawing of cigarette vending machines. Scotland is considering a similar ban. The amendment will now go before the House of Lords, before being initiated between 2011 and 2013 if passed.1, 2
The move has been defended by supporters who say that the banning of vending machines will cut off a major route by which underage children gain access to cigarettes, stopping younger generations from taking up and becoming addicted to smoking in the first place.3, 4
Some fear that this is yet more proof of the nanny state culture gone too far, further criminalising smoking and diminishing the individual’s right to choice and responsibility. In addition, the removal of tobacco products from public display will have the biggest impact on newsagents, for whom the sale of cigarettes contributes a large proportion of their income.5
Will the banning of such products from public places really reduce the number of people buying cigarettes? Won’t determined children find a way around such a ban? Only time will tell.
ReferencesBBC News. MPs approve cigarette vending ban. 2009 1. [cited 2009 Oct 13]. Available from: http://news.bbc.co.uk/1/hi/uk_politics/8303975.stmGriffiths P. Cigarette vending machines may be banned. 2009 [cited 2. 2009 Oct 13]. Available from: http://uk.reuters.com/article/idUKTRE59C14320091013?pageNumber=2&virtualBrandChannel=11564Mccartney I. McCartney wins support for cigarette vending ban. 3. 2009 [cited 2009 Oct 25]. Available from: http://www.ianmccartney.com/mccartney-wins-support-for-cigarette-vending-banBritish Heart Foundation. Sending vending machines to the 4. scrapheap will save lives. 2009 [cited 2009 Oct 13]. Available from: http://www.bhf.org.uk/news-and-campaigning/press-office/latest-news--views/cigarette-vending-machines.aspxBBC News. Newsagents warn Labour over ban. 2009 [cited 2009 5. Oct 11]. Available from: http://news.bbc.co.uk/1/hi/uk/8301195.stm
Late Abortions: A confidential or public matter?Maria KnoebelYear 3 Biomedical Sciences, Imperial College [email protected]
MPs move to ban public display of cigarettesJenifer SalmonsYear 5 Medicine, Imperial College [email protected]
Sour
ce: W
ellc
ome
Imag
es

157lsjm 30 november 2009 volume 01
Introduction“Scientists to create ‘frankenbunny’ in big research leap” 1 was just one of the many sensational headlines to greet attempts by two research groups in 2006 to gain licences for the creation of the first cytoplasmic hybrid (‘cybrid’) embryos in the UK. In contrast, charities supporting diseases identified as potential targets for such research, rushed forward to defend and promote the methods proposed by the two teams. These responses typified the extreme and varied emotional reactions of the British population to the prospective creation of these novel interspecies embryos. What are the ethical issues underlying these public objections to cybrid research? In light of recent advances in non-embryonic stem cell technology, are the possible advantages of cybrid research sufficient for these objections to be ignored? And do these ethical issues have any relevance to medical students?
For many years, stem cell technology has promised huge hopes in the field of medical research. Adult stem cells have been successfully used for transplantation in a number of diseases2, and human Embryonic Stem (hES) cells - with their ability to be isolated and genetically manipulated in pluripotent stem cell lines - seem to offer even greater hopes for studying genetic disease and
exploring pharmacological therapeutic interventions3. Despite this promise, new evidence has shown that in order to create a single successful cloned hES cell line thousands of oocytes are required4. Unwanted gametes from IVF patients are currently the main source of oocytes for hES cell research but these cannot satisfy the required volume. The use of animal oocytes has been suggested as a practical solution to this shortage; cloning technology would then be used to transplant a human nucleus into the enucleated animal oocyte. Traditionally, a significant ethical hurdle associated with oocyte-harvesting for research has been the associated risk of physical and emotional harm to female donors. The procedure is complicated and painful and often financial incentives are offered in exchange for eggs, leaving women vulnerable to the risk of exploitation, especially in resource poor settings. Using animal oocytes and a human nucleus (that could come from any somatic cell in a male or female donor of any age) would remove the need and resultant ethical issues of using human eggs in stem cell research. However this makes it straight forward to access cellular material for experiments. Some would argue it is too easy since it would be possible to get a cell sample for cloning purposes without even the donor’s knowledge.
A Cybrid Cul-De-Sac in Stem Cell Research?Katherine AdlingtonYear 3 (GEP) Medicine, King’s College London [email protected]:10.4201/lsjm.hle.005
Image: A stained 13 day old embryonic chick
Sour
ce: W
ellc
ome
Imag
es
ARTICLE

158 lsjm 30 november 2009 volume 01
The resulting part-human, part-animal embryo is termed a human-animal cytoplasmic hybrid embryo. This ‘cybrid’ would be over 99% genetically identical to the human donor of the nucleus, with just 0.1% of the embryo’s genetic material derived from the animal oocyte’s mitochondrial DNA5. Animal-animal cybrid embryos have previously been created and have even resulted in live offspring, when involving closely related animals6. This technology was used by conservation biologists to successfully clone a wild endangered sheep species using oocytes collected from a closely related, domesticated species, with the hope of preserving these endangered mammals. There are currently no rules to prevent the creation and full gestation of animal-animal cybrid embryos. The first successful example of a human-animal cybrid was reported in 2003, when Chinese scientists obtained well-characterised hES cell lines using a rabbit oocyte donor7. In this experiment, the Chinese research team classified the cybrids as human embryos and thus it was performed in accordance with international guidelines on human stem cell research (The Human Fertilisation and Embryology Act 1990 in the UK), such that human embryos should not be kept beyond 14 days and should not be introduced into the uterus of any species. Day 14 cut-off is used for two reasons; first, it appears to be the limit after which twinning does not occur so before this it is hard to consider an embryo as a distinct individual; and second, it signals the development of the primitive streak, which eventually develops into the embryonic neural system. Thus, it is considered that the early embryo before 14 days of development is not the equivalent of a foetus or person. These regulations remove the potentiality of such embryos to develop into living individuals, therefore, the classification of cybrid embryos as human can immediately quash any ‘frankenbunny’ fears.
In November 2006, two research teams in the UK applied to the Human Fertilisation and Embryology Authority (HFEA) for licences to create cybrid embryos with the aim of conducting research into the genetic reprogramming of cells and the genetic basis of neurodegenerative disorders8, 9. The Human Fertilisation
and Embryology Act 1990 had prohibited the mixing of human and animal gametes but had made no specific mention to the creation or classification of cybrid embryos and thus there existed no formal guidance in the UK as to whether the Chinese research team were justified in treating their cybrid embryos as human10. Whereas, the mixing of human and animal gametes would create a true hybrid embryo with equal genetic contribution from both gamete donors, a cybrid embryo is almost entirely genetically identical to the nucleus donor, with a minimal genetic contribution from the oocyte donor. A huge question hangs over the relative importance of the genetic and environmental contribution of the ooctye to the resulting embryo. A number of government consultations occurring since 1990 had reached conflicting conclusions as to how to classify cybrid embryos – human or otherwise – and whether such research was acceptable, resulting in no regulatory consensus or framework11, 12. This uncertainty was not reserved to regulatory groups. These research applications also generated a firestorm of controversy in the media and a very sudden, emotive reaction from the public, which prompted the UK Government to propose that the creation of hybrid and chimeric embryos in vitro should be banned once and for all13. Instead, the HFEA embarked upon a public consultation to explore the emotive and extreme reactions surrounding this issue and try to reach a consensus about how to classify and regulate cybrid research.
Ethical objections or knee-jerk reactions? The highly emotive response from the media and a proportion of the public that greeted the emergence of details of cybrid research appeared to stem from an instinctive, visceral reaction against it. Such reactions are often referred to as the ‘yuck factor’ and involve an insistence that the thing they are reacting to is inherently wrong without being able to suggest a logical explanation14. This notion of intuitive awareness forms part of the wider philosophical theory of ethical intuitionism, which states that instinctive moral reactions are the expression of an underlying and universal moral code15. Anthropologists such as Mary Douglas claim that this ‘yuck factor’ is a response to the violation of cultural taboos, which have evolved in all societies as a result of the innate human need to categorise the world around them16. Such reactions, however, are dangerous since projective emotions of disgust have been used in the past to wrongly justify group subordination in many societies, for example to drive racism or sexism7. John Harris highlighted the fact that there is no necessary connection between things that disgust us and cases where there are good reasons for judging as unethical18. Yet knee-jerk reactions are often unavoidable and perhaps, one could argue, even a necessary emotional starting point, without which we would be left with indifference.
Interestingly, in a series of public workshops about issues surrounding stem cell research, organised by the Medical Research Council in 2008, initial negative views of cybrids were largely overcome in response to education about the precise nature of the research19. Instinctive moral reactions are not always permanent nor can be relied upon exclusively because they may arise from ignorance of facts. Such ignorance is often fuelled rather than enlightened by the media. Reports frequently incorrectly refer to cybrid embryos as ‘chimeras’ or simply as ‘hybrids’: neither of these are biologically accurate definitions for cybrids20. These misnomers could have significant repercussions, for example, causing the public to associate cybrid technology with pre-existing images of mythological monsters, such as Homer’s fire-breathing chimera or the aforementioned ‘frankenbunny’.
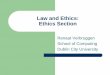
Image: Colour-enhanced electron microscope image of a human embryo at the blastocyst stage opened to reveal the inner cell mass. These cells go on to form the embryo and can be harvested and cultured to give rise to embryonic stem cells.
Sour
ce: W
ellc
ome
Imag
esARTICLE

159lsjm 30 november 2009 volume 01
Unnatural? A significant objection to the creation of cybrid embryos, especially amongst religious opponents, is the belief that it causes a violation of natural species boundaries. Yet there does not seem to exist one universal biological definition of species - in total there are between nine and twenty-two definitions in biological literature and none have received unanimous support 21. Similarly, the great hope that modern genomic technology would provide us with a unique blue print of the human genome to categorically define Homo sapiens has been ruined by the revelation that much of ‘our’ DNA is shared with a large number of apparently distantly related animals, such as yeast and worms, and we differ genomically from chimpanzees by as little as 1.2%22. Aspects of human cognitive capacity have also been used to distinguish Homo sapiens from other animals, such as language, intelligence or emotional complexity. However, any attempt to define features of human beings will either include non-human animals within their scope (dolphins are intelligent, sentient, emotionally-complex animals too) or exclude many patently human individuals (for example, those who are comatose, infants or even illiterate). Hence, it seems that no accepted identifiable species boundaries exist that cybrid research could be said to violate, nor is there any clear species definition that can be used to categorise a cybrid embryo.
Although there appears to be no consensus for biologically demarcating human beings, the public consultation showed that people felt reassured by the revelation that cybrid embryos would be almost entirely genetically-related to their human nuclear donor19. DNA continues to be recognised by the public at least as a significant part of what makes us human. However, this is not an exact science, we may ask at what genetic percentage would this embryo no longer be classified as human?
It is important to consider not only the amount of genetic contribution of the animal donor to the resulting cybrid embryo but also the precise effect this genetic material has on its development. Although initially many of the cellular proteins and RNA in the embryo are animal-derived, by day 14 when the embryo is currently destroyed, the only genetic contribution from the animal would come from the oocyte’s mitochondrial DNA(mtDNA)23. Evidence from animal-animal cybrid embryos that have survived (invariably animals that are closely related) suggests that this mtDNA does have an impact on the resulting embryo’s energy production ability. It would be extremely reductionist to state that a molecular change in the cellular control of ATP production changes the overall identity and classification of an individual. However, it is a change that is pervasive, occurring in every cell of the resulting embryo, and one for which we cannot predict the potential developmental impact. Xenotransplantation (such as the frequent use of pig heart valves in human cardiac surgery) is another form of interspecies manipulation. We can see that it is far easier to biologically classify a transplant recipient as human because there is an observable and measurable change to a discrete region of an already developed human body. On the other hand, cybrid embryos threaten our biological notion of humanness at the most basic level of all cells - at the very beginning of life.
Moral status?Membership in the human community has always depended on far more than DNA and an individual’s moral status exists apart from biological classifications. Immanuel Kant believed a universal
moral boundary exists separating humans from all other non-human animals based on the unique human quality of rationality 24. Membership in the human community is dependent on the innate possession of dignity by rational beings, which therefore bestows on humans alone an innate right to respect and ethical treatment. Cybrid research presents a dilemma for the concept of human dignity. On the one hand, it is the respect for the dignity of human beings that supports medical research to prevent human suffering38. On the other hand, the admixing of human and animal material in the creation of cybrids crosses the moral barrier between dignified human beings and undignified animals, violating human dignity in the process. According to this theory, not only would the dignity of the essentially human embryo be denigrated but also the dignity of the nucleus donor (as it is their DNA material that is being affected) and the future recipient of any resulting stem cell transplant. However, using rationality as a prerequisite for moral consideration presents the same problems as those previously encountered when trying to define human nature – it causes the exclusion of many marginal members of the human race. Even if we expand this definition to include the potential to become rational, we face further problems since; a) under current regulations, the cybrid embryo has no potentiality beyond 14 days, and b) even if it did, this is a novel being and we can only make predictions as to its future capacities for rationality.
Many people object to the human dignity theory because it denies the possession of dignity or moral status to any non-human animal. Whilst few claim that all living organisms should have equal moral status to humans25, there have been many attempts to define certain animals as worthy of moral consideration26. According to Peter Singer, these arguments are just as unacceptable as the human dignity theory: they all justify discrimination on the grounds of species or group membership27. Singer condemned such discrimination as ‘species-ism’ and branded it as indefensible as racism or sexism. However, whether ethically justifiable or not, humans have historically behaved as if they have a right to own animals and be in charge of their fate. This means there is a possibility for conflict and confusion in our moral obligations to cybrid embryos as part-animal, part-human beings.
Slippery slope?Overall, one of the main fears for the public is science would lead to the generation of live interspecies individuals from interspecies embryos. The stigma and moral confusion over our obligation to such individuals, as well as the uncertainty surrounding their successful biological development, would be great. The threat of such individual psychological harm is almost sufficient to motivate a complete ban on cybrid embryos, at least until such a time that social attitudes change and the moral status of animals has been addressed.
Conclusion Ethical objections to cybrid research could largely be silenced by careful regulation that ensures embryos are classified as human and therefore not kept beyond 14 days’ development. Development beyond this time would not be in the best interests of the potential individual or society due to the confusion that would surround classification and obligations of society to the cybrid person. This confusion partly explains the instinctive public reaction against this research. However, the high cost, risk for disease and lack of real promise all make cybrid research seem like an expensive, practically
ARTICLE

160 lsjm 30 november 2009 volume 01
unjustifiable cul-de-sac in the field of stem cell research. With the recent development of Induced Pluripotent Stem (iPS) cell technology, it would seem wrong to pursue such an ethically controversial and divisive research when an alternative is available. This is reflected by the fact that although the cybrid research was licensed by the HFEA and the HFE Act was amended to allow cybrid research in 200833, both research teams have failed to make progress, citing a lack of funding as a major reason34.
It is important for medical students to be aware of the different types of ongoing stem cell research since it is possible that some of these technologies and treatments will become vital clinical interventions in their future medical careers. However, it is important to distinguish the controversial media hype surrounding the experiments from the real clinical hope. Practitioners will not only be expected to understand the intricacies of the technology behind their treatments but also the complex ethical objections they might face from their patients, particularly those that have been negatively influenced by poorly informed media reports. Similarly, it is important to consider the use of animal materials for interventions in different areas of medicine and how each procedure has its own unique ethical nuances.
Whilst the future of stem cell research in this country seems to lie in iPS cell technology, it is interesting to note that huge funds are being directed into all areas of stem cell research in China, where the government believe the solution to a rapidly ageing population is investment in regenerative medicine. The first cybrid embryo was created in Beijing and scientists there are not only benefiting from the increase in funding but also a cultural environment where there seem to be fewer moral objections to the use of embryonic stem cells, perhaps partly due to a different religious and political tradition35. This limitless financial, public and governmental support offers an ideal environment for the advancement of cybrid embryo research, but it leaves us with the question, are the same ethical objections being debated in the UK universally relevant? And should regulations be universally binding?
Image: Undifferentiated embryonic stem cells Image: Heart muscle differentiated from embryonic stem cells
ReferencesDaily Mail. Scientists to create ‘frankenbunny’ in big 1.
research leap [Online] October 5 2006. Available from: http://www.dailymail.co.uk/news/article-408692/Scientists-create-frankenbunny-big-research-leap.html [Accessed 30th September 2006)Mimeault, M., Hauke, R. and Batra, S.K. Stem Cells: A 2.
Revolution in Therapeutics – Recent Advances in Stem Cell Biology and Their Therapeutic Applications in Regenerative Medicine and Cancer Therapies. Clinical Pharmacology & Therapeutics 2007; 82: pp. 252-264.Braude, P., Minger, S. and Warwick, R. Stem cell therapy: 3.
hope or hype? BMJ 2005; 330: pp. 1159-1160.Hall, V.J., Compton, D., Stojkovic, P., Nesbitt, M., Herbert, 4.
M., Murdoch, A. and Stojkovic, M. Developmental competence of human in vitro aged oocytes as host cells for nuclear transfer. Hum. Reprod 2007; 22(1): pp. 52-62.Human Fertilisation and Embryology Authority (ed.). 5.
Hybrids and Chimeras: A Consultation on the ethical and social implications of creating human/ animal embryos in research. London: HFEA; 2007 Loi, P., Ptak, G., Barboni, B., Cappai, P. & M. Clinton. 6.
Genetic rescue of an endangered mammal by cross-species nuclear transfer using post-mortem somatic cells. Nature Biotechnology 2001;19(10): 962-964 Chen, Y., He, Z.X., Liu, A. et al. (2003) Embryonic stem 7.
cells generated by nuclear transfer of human somatic nuclei into rabbit oocytes. Cell Res.2003; 13: pp. 251-263Tilgner, K., Atkinson, S.P., Golebiewska, A., Stojkovi, 8.
M., Lako, M. and Armstrong, L. Isolation of Primordial Germ Cells from Differentiating Human Embryonic Stem Cells. Stem Cells 2008; 26(12): pp. 3075-3085Minger, S. Interspecies SCNT-dervied human 9.
embryos- a new way forward for regenerative medicine. Regenerative Medicine 2007; 2(2): pp. 103-106Department of Health. Human Fertilisation and 10.
Embryology Act 1990. London: DoH: 1990
ARTICLE

161lsjm 30 november 2009 volume 01
Image: Heart muscle differentiated from embryonic stem cells
PERSPECTIVE
Dementia: Is honesty the best policy? Elizabeth PreciousYear 4, Imperial College [email protected]:10.4201/lsjm.hle.008
Dementia is an umbrella term for a number of clinical symptoms common to a wide range of pathological processes1.
The ‘normal’ natural decline in cognitive performance with increasing age may hinder its diagnosis. Indeed, the prevalence of dementia increases with age. In today’s society the major demographic shift concerning the expansion of the over fifties population is a recognised phenomenon; with the greatest rate of increase evident in the higher-risk age cohorts. Consequently health professionals are increasingly coming into contact with the clinical symptoms. The primary carers of those with dementia are usually family members. Dementia care raises moral issues and challenges for all participants due to the nature and distress associated with the condition. In clinical decision-making it is important to address the four principles: autonomy, beneficence, non-maleficence and justice as defined by Beauchamp and Childress. These are principles, not ordered rules. Today, physicians are commonly torn between respecting autonomy, doing good and avoiding paternalism.
Ethical dilemmas occur in dementing disorders, as patients are unable to practise the decisional and/or executional elements of autonomy. In cases where the patient is not competent some physicians believe it is morally just to act paternalistically4. Competence is the clinical term for the legal concept of capacity.
At present clinicians lack an accepted definition of what constitutes deceptive practice regarding dementia care2, 3. Deception encompasses a number of strategies from being ‘economical with the truth’ to outright lying; all involve intentionally making others believe what we do not. Decision-making concerning dementia needs to be addressed in order to alleviate the ethical unease currently experienced. This review will explore the tensions that exist due to the obligations to avoid harm and respect autonomy.
The current situationInterest and knowledge with regards to dementia has escalated in recent times, perhaps shifting public opinions and clinicians’ practices. Research has shown that family members are reluctant to have patients learn the truth, but would want to know if they developed the condition. Controversially, recent studies of those undergoing assessment for memory impairment, show that their desire to be informed is relatively high5-7. Currently, less than half of dementia patients are told their diagnosis; physicians find it easier to convey the diagnosis to relatives. The range of opinions revealed by studies shows the huge potential for disagreement.
DISCUSSION
In favour of disclosurePhysicians are required to employ the professional standards set out by the GMC; these guidelines are considered to be ethically correct and have weight in court. ( Table 1)
Virtue ethics incorporates the importance of these duties: a virtuous person is one who exercises principles of moral conduct. Choosing to withhold the diagnosis undermines the trust in the doctor-patient relationship, which could sway the patient’s compliance. The National Service Framework for Older People 2001 and the Canadian Alzheimer’s Society Guidelines concur that explaining the diagnosis to patients and carers is always a part of dementia care. The truth is always important to know despite how painful it may be4. Withholding information is a form of disrespect; it is patronising to permit them to live in a false reality. Article 3 of the Human Rights Act 1998 (HRA), which came into force in October 2000, states that no one will be subjected to degrading treatment. If a physician does not act on the test results, the diagnostic procedure is arbitrary and may be seen as abuse. Not telling the patient could be perceived as using their disability to manipulate them: both constitute exploiting the position of a doctor2. For some patients the news will trigger immediate sadness and fear, but this is usually neither significant nor irreversible6. As the disease progresses depression is less likely, because patients become less aware of their deficits. Depression is less likely to develop in patients with a well established care support network.
Duty-based ethics considers the nature of the action, independent of the anticipated outcomes. In dementia care, lies are often used with the best intentions8; however, there is a strong moral presumption against all forms of deceit. Deceitful practices may tarnish the reputation of the health services. It is important for physicians to take heed of their responsibility to the community.
Sour
ce: W
ellc
ome
Imag
es
Table 1: The Duties of a Doctor: relevant statements.Respect patients’ dignity and privacy• Respect the right of patients to be fully involved in decisions about their care• Be honest and trustworthy• Make sure that your personal beliefs do not prejudice your patients’ care• Avoid abusing your position as a doctor•
Work with colleagues in the ways that best serve your patients’ interests•

162 lsjm 30 november 2009 volume 01
The majority of family members act paternalistically to protect the patient from the harsh reality. Studies show that relatives are reluctant to deal with the patient’s grief and deceptive practice is often for the carer’s benefit2. Physicians’ decisions should not depend upon the opinions of the family, but their views should be taken into consideration. A study reported that only 58% of people would trust their spouses to make decisions on their behalf if they became incompetent9.
British Law does not give patients’ families authority to make decisions on behalf of those aged 18 years and above. The Mental Capacity Act 2005, which commenced in October 2007 states that an adult may appoint a Lasting Power of Attorney who is entitled to make decisions regarding their health and welfare as well as financial affairs. Clinicians should presume all adults to be competent in decision-making; capacity is decision and time specific. If the patient is incompetent at the time of diagnosis physicians should attempt to facilitate the patient’s abilities to enable them to participate as fully as possible in the proceedings. This is as much a part of respecting the patient’s autonomy, as allowing them to make their own decision. Physicians may be liable for negligence if they do not provide appropriate information. Gaining consent is a process, not a one-off event. Valid consent requires that the patient be: informed, competent and not coerced. Inflicting unwanted treatment on someone undermines their personhood and could lead to cases of perceived battery. Alternatives include acting in the patient’s best interests, referring to any advance directives, making substituted judgements or proxy decision-making.
Article 5 of the HRA states that everyone has the right to liberty and security. Without a diagnosis the patient is unable to exercise this right. This is also true of articles 9 and 10: the right of freedom of thought, conscience and religion, and freedom of expression, respectively.
In the early stages of the disease, patients are capable of undertaking decisions and should not be treated differently from others7. The deterioration, typically seen, can be slowed in those who remain mentally and socially active. Facilities can be implemented to allow the individual an extended period of independence. If a patient’s dignity is respected, their well-being can be enhanced. People with a mental illness deserve the same respect and equality as others; the stigma of the diagnosis is not a
reason to withhold the information. Discrimination is widespread. However, this is against article 14 of the HRA. Table 2 summarises the support for disclosure.
It is interesting to note the evolution of disclosure of cancer diagnosis: between 1961 and 1977 the number of doctors in favour of informing the patient increased from 10% to 97%10. The explanations against disclosing were similar to those currently given for dementia.
In support for more deceptive strategiesAs dementia patients withdraw into their own world, they lose their capacity to distinguish between true and false. Truth is a privilege available to those who can understand it and cope with its’ burden: theoretically it becomes impossible to lie. Treatment options are limited, and there is no cure for dementia. People receiving this diagnosis require resources. Currently time constraints are problematic11.
An abnormal level of cognitive performance is hard to assess and determine. Revealing a false diagnosis of dementia is unethical and uncertainty deters physicians from disclosing the diagnosis. The GMC states that clinicians need to recognise their professional limits. Therefore, in cases of significant doubt it is better to withhold the information. However, health professionals should always work with their colleagues in a way that best serves the patient and should seek the medical opinions of their colleagues. The vast majority of physicians have never received dementia training. In the absence of a specialist clinical framework there is nationwide variation in dementia care. Instruction and supervision need to be accessible in order to improve the quality of care. Utilitarianism is often used to describe the best outcomes as those which maximise happiness. The response to the disclosure is an individual process; some patients lose their self-esteem and withdraw from social activities. If the revelation of the diagnosis is likely to cause such suffering, the physician stands at risk of not practising non-maleficence. In this instance, where well-being is considered to be synonymous with happiness, the physician is giving hope, sparing pain and preserving self-respect by not disclosing the information, and therefore promoting the well-being of the patient. A physician should not let their personal beliefs affect the assessment of the situation; if deceptive practice will benefit the patient, a physician morally against dishonesty should still consider the strategy4.
Article 3, the only absolute right in the HRA forbids torture; this may support keeping the diagnosis from those patients who are susceptible to suicide and other depressive behaviours. Although the risk of suicide is relatively small, it is something that physicians need to be aware of. A study undertaken in 2002 asked family members of dementia patients about the disclosure of the diagnosis: half thought the informed patient reacted poorly to the diagnosis, and two-thirds felt that the disclosure was unhelpful to the patient12. Family members commonly disagree with the decision to disclose the diagnosis13.
It is important to differentiate between a psychological reaction and a psychopathological complication; the latter gives deceiving a moral justification. Depression is likely to occur especially in the early stages, and may hasten the patient’s decline. Distinguishing between the negative consequences of disclosure and the natural
Table 2: Reasons supporting disclosure.Reasons to inform
Reduce distress and improve psychological adjustment• Patients have a right to information about their condition• Patient is aware that they are ill – diagnosis explains the symptoms• Patients more likely to accept help and support• Patient is then responsible for informing necessary services e.g. DVLA• Can provide a sense of relief e.g. that the cause of abnormal cognitive performance is not • malignantPatient can consider treatment options and participate in research if willing• Patient can attain information on and be referred to community-based services • Patients can make plans and sort financial affairs• Promotes trust in doctor-patient relationship• Enables family to anticipate care needs, plan for the future and prepare for change• Family members can assess their own risk for dementia•
PERSPECTIVE

163lsjm 30 november 2009 volume 01
course of the disease is difficult. If the physician believes the patient does not have the ability to cope with the information the virtuous action is to withhold such a diagnosis.
The ethical duty to be honest is not absolute3; physicians need to be aware of the difference between the world of pure practical reason and that in which we live. Deceptive strategies are potentially beneficial for both carer and patient. The Data Protection Act 1998 states that although a patient has a right to their medical records, if a health professional believes that the knowledge is likely to cause serious harm to the physical or mental health of the patient or any other person they are justified to withhold the information. The GMC, however, highlights that upsetting the patient is not synonymous with ‘serious harm’.
If the assessment of the patient occurs in the latter stages of the disease process, the decline in the individual’s competence would render the disclosure procedure futile. The severity of dementia and the physician’s perception of the patient’s comprehension are key factors when deciding whether to disclose. Doctors must always be prepared to justify their actions. Table 3 highlights the factors that defend withholding the diagnosis.
In conclusionGood decisions consider all the relevant ethical principles, laws and current practice, and address truth-telling, confidentiality and dignity. The deontological approach recognises the importance of an individual’s rights and thus supports disclosure. Deciding which right predominates is not simple: any act that is not wrong is a possible right act. The consequentialist perspective offers a more person-centred approach, considering the impact on the patient. In light of the evidence I believe this theory supports the disclosure of the diagnosis.
There are many rational reasons for non-disclosure, but there is a lack of evidence supporting that it is more beneficial. The difficulty in diagnosing dementia must be differentiated from the difficulty in telling people an unwanted diagnosis. The negative outcomes anticipated by physicians and carers alike are worse than the reality. Literature supporting the disclosure of diagnosis is building. If possible disclosure should occur in the early stages of the disease process. Physicians need to be flexible: patients require an individual approach. The rights of those who do not wish to know should be respected.
Basic principles demand physicians to be truthful, so that patients can implement their moral and legal rights to decide whilst still competent. Nevertheless, blunt honesty is inappropriate; the truth should be eased across with compassion, to avoid hurting the patient. The final decision involves a complex balance between the clinical findings, the patients’ preferences, and their social context. I believe deceptive practice should not be completely disregarded; it may be appropriate if the patient is emotionally, psychologically or intellectually unable to cope with the diagnosis.
Further empirical research is needed to establish best practice. Paired interviews are needed to gain the physicians and family members’ views on the same experience. Future questions might include: Should patients and carers be informed simultaneously?
Info boxDiagnosing DementiaThe Abbreviated Mental Test (AMT) and the Mini Mental State Examination (MMSE) are used extensively to screen older people for cognitive impairment. The AMT consists of 10 questions, with a score of 6 or less suggesting impaired cognition.
The MMSE is the gold standard; it covers orientation, calculation, language, registration and recall. The examination involves 19 items; a score of less than 25 out of a possible maximum of 30 is suggestive of dementia. Tester variability makes the MMSE unreliable, and so the key is a thorough history. It is considered good practice to ask relatives and friends about progressive decline in function and memory. This exercise requires care, as relatives may be in denial about changes in their loved ones behaviour.
Ascertaining a diagnosis of dementia is not easy; not only is the list of differentials inexhaustible, but the range of cognitive processes affected, and the severity of their presentation can vary both within and between dementing disorders. This article makes no distinction between the classifications of dementia, which may be of importance as new treatments are unveiled.
Table 3: . Reasons against disclosing the diagnosis of dementiaReasons not to inform
Patient may become upset e.g. because their family role is altered • Patient may suffer psychological distress e.g. depression, suicide• The prognosis may frighten them and they may feel burdened by the inevitable future• Patient has a dread of developing dementia• Patient not cognitively/emotionally equipped to understand/retain the information• No benefit in knowing as no curative treatment available• Patient does not wish to be aware of any illness• To maintain/give hope• Stigma associated with dementia • Family may not be able to cope with patient’s reaction•
What level of information needs to be provided? The question is no longer if we should disclose the diagnosis, but when and how.
ReferencesJagger C, Lindesay J. The epidemiology of senile dementia. 1. In: Alistair Burns. Ageing and Dementia: A methodological approach. London: Edward Arnold, 1993:41-57.Wood-Mitchell A. Can a lie ever be therapeutic? The debate 2. continues. The Journal of Dementia Care 2007; 15(2):24-28. Sokol DK. Can deceiving patients be morally 3. acceptable? BMJ 2007; 334:984-986.Schermer M. Nothing but the truth? On truth and deception 4. in dementia care. Bioethics 2007; 21(1):13-22. Turnbull Q, Wolf A, Holroyd S. Attitudes of Elderly Subjects 5. toward “Truth Telling” for the Diagnosis of Alzheimer’s Disease. Journal of geriatric psychiatry and neurology 2003; 16:90-93. Pinner 6. G, Bouman WP. Attitudes of patients with mild dementia and their carers towards disclosure of the diagnosis. International psychogeriatrics 2003; 15(3):279-88. Elson P. The diagnosis of dementia: who wants to know? 7. The Journal of Dementia Care 2006; 14(5):36-38. Wood-Mitchell A, Waterworth A, Stephenson M, James 8. I. Lying to people with dementia: sparking the debate. The Journal of dementia Care 2006; 14(6):30-31. Jones RG. Ethical and legal issues in the care of those with 9. dementia. Reviews in Clinical Gerontology 2001; 11:245–268.Maguire CP, Kirby M, Coen R, Coakley D, Lawlor BA, O’Neill 10. D. Family members’ attitudes toward telling the patient with
Alzheimer’s disease their diagnosis. BMJ 1996; 313(7056):529.
AcknowledgementsI would like to thank Dr. Ian
Davidson for his encouragement and guidance with this work
PERSPECTIVE

164 lsjm 30 november 2009 volume 01
Childhood Obesity as a Form of Parental NeglectIt is estimated that 4% of children are obese and 15.4% of children are overweight1. Worryingly, these children already have important risk factors for developing coronary heart disease, which are unlikely to resolve as they are at an increased risk of remaining obese as adults1.
In 2007, Dr. Matthew Capehorn proposed to the BMA that extreme cases of childhood obesity should be regarded as cases of parental neglect. Although this motion was not accepted, Dr. Capehorn makes a valid argument for the case; “If you are faced with a child who is severely under-nourished, alarm bells would be ringing, and social services, doctors and other authorities would be involved. But the same approach is not taken when faced by a child who is obese.”
If a doctor fears that a child is being neglected, it is their legal duty to inform social services despite patient confidentiality. The issue to consider here is whether or not severe childhood obesity is a form of neglect, and if referral to social services is in the best interests of the child. From the perspective of the Royal College of Paediatrics and Child Health, “Obesity is a public health problem, not a child protection issue. There may be a few families who give cause for concern where there are other matters of neglect or emotional harm, and this is where a paediatrician might have discussions with social services”. This is an important argument, as according to reported cases, obesity has only formed part of child protection cases rather than being the sole cause of them. If parents are suspected of neglect due to the over-feeding of their child, it is important for them to first of all understand what the correct sized portions are for a child, through education by dieticians. However, a child who is morbidly obese with a number
of co-morbidities that affect their quality life may find that adhering to dietary guidance as well as exercise advice does not lead to successful attempts at losing weight. It is therefore an ethical grey area to solely and confidently attribute blame to the parents.2 Children with co-morbidities are less likely to be physically fit or have the motivation to exercise, thus despite the parent’s best attempts to encourage them, the child may be unable to lose weight. In particular, older children have increased autonomy and so parental control is less likely to be effective.3
However, it has to be considered that the removal of a child from their family and their home due to neglect, could cause significant emotional distress to them and other parties. Such situations need to be considered carefully to ensure that all that is done is in the child’s best interests, taking into account both emotional and physical factors as they may consider their home to be a happy and loving environment,
It is of course difficult to assess what the child’s best interests are; social factors needed to be considered as well as the attitude of the parents and the child, in deciding if severe obesity in a child is a case of medical neglect. More thorough guidelines to doctors and other health professionals on when to refer a child to social services for medical neglect would be beneficial in such cases.
ReferencesSusan A Jebb, Kirsten L Rennie and Tim J Cole. Prevalence 1. of overweight and obesity among young people in Great Britain. Public Health Nutrition, 2004 7: 461-465Collier D, Perkin R, Zanga J. Obesity as Medical 2. Neglect: Should Doctors Report? American Medical Association Journal of Ethics 2003 Volume 5, Issue 2Varness, Todd, Allen, David B., Carrel, Aaron L., 3. Fost, Norman. Childhood Obesity and Medical Neglect Pediatrics 2009 123: 399-406
Feature Series on ObesitySheena Sabherwal
Year 5 Medicine, Imperial College [email protected]
doi:10.4201/lsjm.hle.006

165lsjm 30 november 2009 volume 01
£Obesity is a health burden, which is showing no signs of regressing and in fact is rapidly progressing. It is estimated that by 2050, 90% of the adult population will be obese1. Within the UK, obesity-associated morbidity mounts enormous pressure on NHS resources, costing £4.2 billion every year1. Obesity and poor diet are associated with the development of serious morbidities, including ischaemic heart disease, type 2 diabetes and cancer, and accounts for 10% of all disability-adjusted life years lost2. These can result in doctors and health professionals dedicating more time to deal with these preventable problems, drawing away resources and time from other important health issues. A ‘Fat Tax’ is one proposed way of preventing the progression of obesity and encouraging healthier eating. In basic terms, it means that high calorie, high sugar and high fat foods or drinks will have a considerable tax added onto their selling price, in an attempt to deter their purchase. It is a system which has been implemented in a number of North American states and is a proposal which has previously been discussed by the UK government. However, how ethical is the Fat Tax proposal, and how will its implementation affect the associated burdens of disease?
An important ethical issue to consider is the effect of the inflation of food prices on the poor. Those with lower incomes will naturally spend a greater proportion of their household expenditure on food than the wealthy. Fat Tax may be effective in deterring the purchase of unhealthy foods in those with lower incomes, but such foods tend to be more calorific and cheaper than healthier foods, and so overall, food expenditure for the poor will increase3. This will unfairly reduce the money available for this group of the population to spend on other necessities such as rent, with possible subsequent economic problems. Alternatively, it may decrease expenditure on food, potentially leading to malnourishment. A method of overcoming this problem could be to subsidise healthier foods with the increased revenue from the Fat Tax. One study has shown that such an initiative will overcome differences in the effect of Fat Tax on the different income groups, and also anticipates that such a situation would be associated with a reduction of 6400 deaths due to cardiovascular and cancer-related causes.4
A problem with implementing Fat Tax is deciding which foods the policy should affect. Many studies have suggested that those high in saturated fats should be taxed. In theory, this is a worthy idea as high saturated fat consumption increases cholesterol levels, thereby increasing cardiovascular risk. However, it is suggested that this will also decrease the consumption of monounsaturated and polyunsaturated fats, as well as increase salt intake2. All of these dietary changes would be associated with a decrease in the consumption of unsaturated fats and an increase in blood pressure, outweighing the benefits of the decrease in saturated fat
consumption in terms of risk factors for associated morbidity. Bearing all of this in mind, it seems that deciding which foods to be taxed is a complex and contentious process, as one needs to take into account that all foods, even those classically seen as unhealthy, cannot be ruled solely as good or bad. For instance a food may be high in saturated fats but also high in calories, providing an important calorie intake to meet a person’s recommended daily allowance.
It could be argued that a Fat Tax would eliminate our autonomy and instead enhance paternalism whereby the government would have increasing control resulting in a population with reduced individual freedom. On the other hand, Fat Tax may simply reverse the powerful and negative implications of mass advertising by large multinational companies in promoting their unhealthy foods. It may also encourage manufacturers to make their food healthier by reducing saturated fat content and offering a wider range of healthy foods and snacks. A similar concept was adopted in the UK to reduce smoking by increasing tax on cigarettes; this has been shown overall to have had a successful outcome5. Therefore, a Fat Tax could simply be seen as an extension of this policy to promote good health within the community.
Upon reviewing the evidence, Fat Tax will inevitably have important consequences for the health of the population, particularly for lower income groups. This group is also known to have a greater prevalence of cardiovascular disease, so with careful implementation of the system, the obesity crisis as well as risk factors for morbidity should decline. This would reduce the burden on the NHS and the increased revenues from the Fat Tax could be used to fund campaigns promoting healthy eating and health education. As health professionals, it would be our responsibility to make sure that patients are aware of how to change their diets appropriately for optimal health in response to the effects of the Fat Tax.
ReferencesDepartment of health. Obesity [document available 1. on the internet] Department of health [Acessed: 21st October 2009]. Available from: http://www.dh.gov.uk/en/publichealth/healthimprovement/obesity/index.htmMytton, Oliver, Gray, Alastair, Rayner, Mike, Rutter, 2. Harry. Could targeted food taxes improve health? J Epidemiol Community Health 2007 61: 689-694 Marshall T. Exploring a fiscal food policy: the 3. case of diet and ischaemic heart disease. British Medical Journal 2000; 320(7230): 301–5.Kelechi E Nnoaham , Gary Sacks , Mike Rayner , Oliver Mytton 4. , and Alastair Gray. Modelling income group differences in the health and economic impacts of targeted food taxes and subsidies.Int. J. Epidemiol. 2009 38: 1324-1333.Joy Townsend, Price and consumption of 5. tobacco Br Med Bull 52: 132-142.
Fat Tax: More harm than good?
Illu
stra
tion
: Jon
atha
n H
yer

166 lsjm 30 november 2009 volume 01
Doctors Lead the Battle against
Drug Doping in Professional SportsJamal Omar, MEngYear 1 GEP Medicine, Barts and the [email protected]:10.4201/lsjm.hle.007“Nature cannot be tricked or cheated. She will give up to you the object of your struggles only after you have paid her price.” (Napoleon Hill, 1883-1970)
London 2012 is dawning. One need not look far to find athletes and instructors who assert a win-at-all-costs paradigm. They say that history has a funny way of repeating itself; if so, then the legacy of the next Olympics will doubtlessly be tainted by exclusions and withdrawal of honours, for the use of banned chemicals and procedures.
Newsflash: athletes cheat. For over 100 years, the modern Games have inspired a journey for supremacy, displaying awesome talent and proud nationalism, giving the world an ephemeral shared focus in the celebration of eternal champions. But triumph is no longer merely the product of hard work and natural ability. Scientifically motivated develop-ments in exercise regimens have had such a monumental influence on athletic performance that world records are now being broken more often than plates in a Greek restaurant. Yet, science is the academic backbone of doping and for methods aimed at dodging its discovery.
So why should healthcare professionals be aware of these issues? If elite athletes are allowed to cheat the rules of fair competition then the mainstream acceptance of these substances in the wider community - where the behaviour of victors is imitated - would have dire repercussions. Men, women, boys and girls the world over are submitting to the relentless onslaught of Adonis-like bodies staring out from magazines and movie screens, and are now demanding their piece of the ‘hormone cake’. Indeed, clandestine exploita-tion of performance-enhancing drugs amongst the general public is escalating10.
Athletes dope for several reasons: the perception that all their competitors are doing it, public expectation, financial reward, fame, desire to be the best, or to win private sponsorship. The fear of exposure and ignominy is a more potent disincentive than the possibility of self-injury. One study found that 50% of athletes interviewed would take a drug that guaranteed success, even if it resulted in death some years after the event1. Thus, the role of the
doctor, both in the research and clinical arenas, must be to develop methods for detection of prohibited drugs and to counsel those patients partaking in their abuse.
Which hormones are drugs of abuse, and which are fountains of youth? Anabolic steroids (AS), derivatives of testosterone, are manipulat-ed by athletes for their alleged anabolic benefits. Google ‘anabolic steroids’ and a plethora of flashing advertisements appear, selling dubious elixirs that promise ‘ripped abs’ and ‘a cut physique’, all endorsed by golden, perfectly-sculpted mortal engines.Modes of action of anabolic steroids include binding of androgen receptors which results in positive nitrogen balance in muscle, and favours anabolism. However, in ‘normal’ men, endogenous testosterone predominantly saturates the androgen receptors, so this result has limited significance6. Thus it follows that steroids must antagonise catabolism of muscle tissue. At saturation point, exogenous steroids competitively impede the binding of catabolic glucocorticoids to androgen receptors, thereby conserving lean muscle mass. Finally, steroids may bestow increased psychotropic stimulation resulting in greater motivation and reduced exhaustion4. Scientists and physicians have often doubted athletes’ conten-tions that steroids actually work. But scientists have been one step behind, as the literature indicates that suprapharmacological quantities of steroids may be anabolic in eugonadal men; however, the mechanistic pathways underlying these effects are unclear5. In any case, steroids have both anabolic and androgenic proper-ties, which explain the side effects involved. These include risk of developing coronary heart disease, liver cancer, severe acne and gynaecomastia. Is it really worth it?
Evidently, steroids are not the panacea. So, where do athletes turn to next?Growth hormone (GH) also appears in the catalogue of sports pharmacopoeia forbidden by WADA (World Anti-Doping Agency). GH is particularly difficult to identify in the laboratory, so preva-lence data is often anecdotal.
Nonetheless, nobody disputes that GH is widely abused. Its ef-fects, mediated by IGF-I, comprise amplified total body protein turnover and skeletal muscle synthesis in athletes and GH-deficient adults1. GH may also boost fatty acid availability and moderate oxi-dative protein loss in athletes to reduce fat deposits7. Furthermore, this response is affected by age, gender, individual fitness and by
ARTICLE

167lsjm 30 november 2009 volume 01
exercise routines8. It seems unlikely that this will better athletic performance, but athletes are desperate to maintain an edge. Current technology is accelerating, and genetic engineering of the GH/IGF axis has arrived. In vivo upregulation of anabolic molecules can be achieved via transfer of an athletically superior genotype to the host, inducing specificity that is virtually undetectable in the lab6 – illustrating the level of daring sophistication that doctors and scientists must face.
The risks involved in taking GH are many. Cadaver-derived pituitary GH harbours the threat of infection with CJD. Even using recom-binant human GH, adverse effects include various forms of cancer, because IGF-I biochemical cascades play a role in carcinogenesis4. This author believes that researchers and doctors have a duty to publicise these risks. They must learn from athletes and bodybuild-ers, victims of the slippery slope, who inject substantial doses of an unknown cocktail of drugs in a trial-and-error fashion, and end up with terminal illness. Let us not forget the acute dangers involved: people can be become so obsessed that they unintentionally over-dose and kill themselves. Healthcare professionals must adhere to the principle of ‘patients come first’, which is enshrined in all ethical and legal codes of medical practice.
Introducing – the final member of the doping repertoire – Erythropoietin. Time to shift gears again. Picture this: is there anything more physi-cally and mentally devastating than being overtaken by an opponent in a race? Your legs are screaming, your chest is on fire; you rasp and wheeze for precious air to stay abreast of the leader. You know that if you let him leave the pack, your will to continue shall ebb away. You quash the blazing panic rising in your stomach, and say a silent prayer as you bend over the handlebars and push for all you are worth. But it is all in vain.
By the top of the hill, he is a tiny blip in the distance. What could you have done, aside from choose better parents? Do you accept genetic limitations, or suspect foul play? Erythropoietin (EPO) burst onto the professional cycling scene in the early 1990s, and has infiltrated elite sport across the board, with organised doping strategies now commonplace in international teams3. Availability of EPO boomed with the advent of recombinant DNA technology. EPO stimulates the bone marrow to secrete more red blood cells into the circulation. Sportsmen abuse it to increase the oxygen carrying capacity of blood to improve stamina, but the subsequent increase in blood viscosity increases the risk of stroke and MI. Too many athletes have paid the ultimate price. This all begs the question…what are researchers and doctors doing about it?
We will take the example of GH. The numerous difficulties for lab-based GH quantification include the identical amino acid sequences of endogenous GH and rhGH, their short systemic half-life, pulsatile discharge behaviour and post-exercise elevation. Urine testing is not viable for rhGH detection because neither GH nor its biomarkers are excreted in adequate concentrations10. Sci-entists have devised a two-pronged method to expose GH abuse. A combination of these approaches satisfies WADA’s stipulation for two separate assays to charge an athlete. This formed the thrust of the international collaborative research project ‘GH-2000’. The consortium was led by the clinical endocrinologist Prof. Sönksen at St. George’s Hospital, London. Briefly, GH actions result in
production of various proteins, whose plasma levels may be utilised to identify exogenous GH. Numerous skeletal and soft tissue indi-cators also fluctuate due to GH dispensation (e.g. P-III-P, PICP and ICTP). It was concluded that IGF-I and P-III-P impart the optimum sensitivity and specificity1. Separate from GH-2000, researchers led by Dr. Strasburger in Munich have developed a direct test for rhGH. Pituitary GH exists as a 22 kDa isoform (constituting 75% of total), and others labelled non–22 kDa (20- and 17 kDa isoforms). rhGH possesses only the 22-kDa isoform, and external rhGH leads to a striking reduction in the natural pituitary-derived non–22- kDa isoforms by negative feedback. Hence, a high ratio of 22- to non-22 kDa isoforms is being trialled as a means of discovering GH abuse3. However, the ‘window of opportunity’ is fleeting – 36 hours maximum. The GH-2000 project was hugely successful, bringing together sci-entists and physicians across Europe to get one step ahead of rogue athletes, and adding flesh to the bones of this emerging medical specialty. These endeavours are critical not just to uphold respect for international sport, but also to prevent the wrong message from sifting through to the impressionable young. Conservative estimates of adolescent hormone abuse range from 3% to 7%, with users starting as young as nine10.
This author echoes the mindset of many others out there, who argue that blanket prohibition is a flawed strategy in a climate of reward3. Those who stand to gain from deception will inevitably be more imaginative than those implementing the regulatory policies, until the deceivers are progressively pushed into a corner and dare to take more desperate and perilous actions. Alternatives to this zero-tolerance approach must be sought, and users should be referred by their doctor to harm minimisation groups for supervision of injections in order to prevent needle sharing and overdose. In this way, the concept of doping will lose its underground appeal, and we can leave behind those who call themselves elite athletes, but are merely entertainers.
ReferencesMcHugh C.M., Park R.T., Sӧnksen P.H., Holt R.I.G. Challenges in 1. Detecting the Abuse of Growth Hormone in Sport. Clin. Chem., 51(9): 1587-1593 (2005) doi:10.1373/clinchem.2005.047845 Nelson, C. J. Howe, T. V. Nguyen, K.C. Leung, G. J. Trout, M. J. 2. Seibel, R. C. Baxter, D. J. Handelsman, R. Kazlauskas, and K. K. Ho, A. E. Influence of Demographic Factors and Sport Type on Growth Hormone-Responsive Markers in Elite Athletes. J. Clin. Endocrin. Metab., 91(11): 4424-4432 (2006) doi:10.1210/jc.2006-0612R T Dawson. Hormones and Sport (Drugs in sport – the role of the 3. physician). J. Endocrin., 170: 55–61(2001) doi:10.1677/joe.0.1700055Drugs and Therapeutics Bulletin (dtb). Medical 4. Aspects of Drug Use in the Gym. Independent review from the Consumer’s Association, 42(1) (2004)Bhasin S., Storer T.W., Berman N., Callegari C., Clevenger 5. B., Phillips J., Bunnell T.J., Tricker R., Shirazi A., Casaburi R. The effects of supraphysiologic doses of testosterone on muscle size and strength in normal men. NEJM, 335: 1-7 (1996) doi:10.1056/NEJM199607043350101Tokish J.M., Kocher M.S., Hawkins R.J. Ergogenic Aids: 6. A review of basic science, performance, side effects and status in sports. Am. J. Sports Med., 32(6): 1543-1556 (2004) doi:10.1177/0363546504268041Gibney J., Healy M.L., Sӧnksen P.H. The growth hormone/7. Insulin-like growth hormone axis in exercise and sport. Endocrine Rev., 28(6): 603-624 (2007) doi:10.1210/er.2006-0052Saugy M., Robinson N., Saudan C., Baume N., Avois L., Mangin 8. P. Human growth hormone doping in sport. Br. J. Sports Med., 40(suppl 1): i35-i39 (2006) doi:10.1136/bjsm.2006.027573Sönksen P.H. Hormones and Sport (Insulin, Growth Hormone and 9. Sport). J. Endocrin., 170: 13-25 (2001) doi:10.1677/joe.0.1700013Il
lust
rati
ons:
Yas
min
Jaff
er
ARTICLE
For the full list of references see thelsjm.co.uk.