-
8/9/2019 Health IT_Why Now_Health Disparities Summit
1/30
Health IT: Why Now?
Thomas Tsang, MD, MPH
Office of the National Coordinator for HITNew York REACH Health
Disparities SummitJune 3, 2010
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
2/30
Qualit context
HITECH goals M nin f l
Healthcare Reform
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
3/30
What we cant measure cannot bemanaged!
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
4/30
CDC- 100 000 ex ire from hos ital-ac uired
infections 2009 In 2000, the Institute of Medicine estimated
that up to 98,000 Americans die each year
from preventable medical errors.Medical errors are killing more
people per year, in the
U.S., than breast cancer, AIDS, or motor vehicleaccidents.
80 percent of errors were initiated bymiscommunication.
1 Kohn, L., J. Corrigan, and M. Donaldson. To Err Is Human:
Building a Safer Health System. Committee of Health Care in
America, Institute of Medicine. 2000.2 Institute of Medicine and
Centers for Disease Control and Prevention. National Center for
Health Statistics: Preliminary Data for 1998 and 1999. 2000.3Smith,
Peter, et. al. Missing Clinical Information During Primary Care
Visits, The Journal of the American Medical Association. February
2005.4&5 National Coalition on Health Care, Facts About Health
Care - http://www.nchc.org/facts/cost.shtml
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
5/30
National Health Quality Report 2009- Track
Survey data collected from populations (N=11) AHRQ, Medical
Expenditure Panel Survey (MEPS) - , CMS, Medicare Current
Beneficiary Survey (MCBS) SAMHSA, National Survey of Drug Use and
Health (NSDUH)
Data collected from samples of health care facilities (N=8)
American Cancer Societ -American Colle e of Sur eons National
Cancer Data Base NCDB CDC-NCHS, National Ambulatory Medical Care
Survey (NAMCS) CMS, End-Stage Renal Disease Clinical Performance
Measurement Program
Data extracted from data systems of health care organizations
(N=13) AHRQ, Healthcare Cost and Utilization Project State
Inpatient Databases (HCUP SID) CMS, Quality Improvement
Organization (QIO) program. Indian Health Service, National Patient
Information Reporting System (NPIRS) NIH, United States Renal Data
System (USRDS)
Data from surveillance and vital statistics systems (N=5)
- , , , CDC-NCHS, National Vital Statistics System (NVSS)
NIH-National Cancer Institute, Surveillance, Epidemiology, and End
Results (SEER) program
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
6/30
2009 NHQR Findings
ua ty simproving, but theace is slow
especially for
preventive care andchronic diseasemanagement.
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
7/30
2009 NHQR Findings
Health care quality needs to be improved
Private No insuranceMeasure insurance (%) (%) Difference
Women ages 40-64 who had a mammogram in the last 2years
74.2 38.3 35.9
Children a es 2-17 who had a dental visit in the calendar 59.6
27.9 31.7year
Adults ages 40-64 with diagnosed diabetes who received adilated
eye examination in the calendar year
64.1 35.4 28.7
Adults ages 50-64 who ever received a colonoscopy,sigmoidoscopy,
or proctoscopy
47.5 20.7 26.8
Adults with obesity who received advice from a provider
toexercise
61 41.2 19.8
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
8/30
Core Measures Getting Worse
Blacks Asians AI/ANs Hispanics
Adults age 50 and over who report * * * *
Cancer
they ever received a colonoscopy,
sigmoidoscopy, proctoscopy, orfecal occult blood test
ancer ea s per ,population per year for colorectalcancer
* *
Heartdisease
who received recommendedhospital care
Respiratorydiseases
Adults age 65 and over who everreceived pneumococcal
vaccination
Hospital patients with pneumonia
* * * *hospital care
National Healthcare Quality Report 2009 AHRQ
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
9/30
HITECH Vision Furnish tools to begin a major transformation
in
Provide best opportunity for each patient tov u w
information exchange
ress e mos press ng o s ac es o a op onand meaningful use of
electronic health records
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
10/30
HIT as a tool and foundation for deliverysystem mprovement
Im rovedQuality &Efficiency
CareDelivery Provider Payment
Innovations
Measurement
HIT FoundationMeaningful Use of EHRs
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
11/30
Sustainable Health Outcomes:
Quality, Efficiency Population Health
Innovative Care Delivery
Processes and Payment Reform
Electronic Health Records and
Information Exchange
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
12/30
HITECH goals
o a ou ec no ogy
Improving health and transforming health care throughmeanin ful
use of HIT
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
13/30
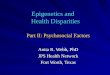
Getting to Meaningful UseTo Improve Health Health are
TECHNOLOGYADOPTION
REDESIGN
MEANINGFULMEANINGFULOUTCOMESBetter Health
HEALTH
USEUSE TransformedCare DeliveryReduce
CONSUMERINFORMATION
EXCHANGEHealthDisparities
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
14/30
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
15/30
Grass Meaningful Use of Grass
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
16/30
Framework: HIT Policy CommitteesRecommended Five Priorities
Improve quality, safety, efficiency and
reducehealthdisparities
Engage patients & families in their health care
mprove care coor na on
Improve population and public health
personal health information
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
17/30
Meaningful Use
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
18/30
Meaningful Use Proposed Stage 1bjectives for EPs Eligible
Hospitals
.
2. Implement drug-drug, drug-allergy, drug-formulary checks
3. Maintain an up-to-date problem list of current and active
diagnoses based on ICD-9-CM or SNOMED CT
4. Maintain active medication list
.
6.6. Record demographicsRecord demographics
7. Record and chart chan es in vital si ns
18
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
19/30
Meaningful Use Proposed Stage 1
8. Record smoking status for patients 13 years and older
9. Incorporate clinical lab-test results into EHR as structured
data
10. Generate lists of patients by specific conditions to use for
quality
, ,
11. Report ambulatory quality measures to CMS or the States
12. Implement 5 clinical decision support rules relevant to
specialtyor high clinical priority, including diagnostic test
ordering, along
with the ability to track compliance with those rules
.
payers
14. Submit claims electronically to public and private
payers
19
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
20/30
Meaningful Use Proposed Stage 1
Ob ectives for EPs & Eli ible Hos itals
15. Provide patients with an electronic copy of their healthn
orma on upon reques
16. Capability to electronically exchange key clinical
informationamong providers of care and patient-authorized
entities
. er orm me ca on reconc a on a re evan encoun ers aneach
transition of care
18. Provide summary care record for each transition of care
and
19. Capability to submit electronic data to immunization
registriesand actual submission where required and accepted
.public health agencies and actual transmission according
toapplicable law and practice
.the certified EHR technology through the implementation of
appropriate technical capabilities20
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
21/30
Additional Meaningful Use Proposed
1. Generate and transmit permissible prescriptions
age ec ves or s n y
electronically
2. Send reminders to patients per patient preference for-
3. Provide patients with timely electronic access to
their health information within 96 hours ofinformation being
available to EP
4. Provide clinical summaries for patients for each
21
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
22/30
Incentive Payment Timeline
Medicare
EPs may receive payments no sooner than January2011
Eligible hospitals & CAHs may receive payments no
Medicaid EPs
Can otentiall receive a ments as earl as 2010 forA/I/U and
hospitals as early as 2011
Medicare Advantage EPs
Will receive payments following determination thatthey are not
eligible for full incentive under MedicarePart Bantici ate
determination in s rin 2012
22
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
23/30
Regional Extension Centers
HITRC
Beacon Communities
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
24/30
Role of Regional Extension Centers (RECs)
Unbiased guidance on vendor selection andgroup purchasing
Reach out to providers of underservedcommunities
un n n y ninformation exchange
Privacy and security best practices
Everything involved in ensuring meaningfuluse of EHRs
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
25/30
15 Beacon Communities
Extend advanced health IT
and exchange infrastructure Demonstrate a vision ofthe future
where:
,patients are meaningful
users of health IT, and
Leverage data to informspecific delivery system andpayment
strategies
measurable & sustainableimprovements in healthcare quality,
safety,
efficiency, and populationhealth
25
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
26/30
HIT-enabled quality improvementExpectations regarding data
collection
E-specifications for quality measures
en er or e care e ca nnova onSuccess of value-based purchasing
demos & pilots
measured b HIT- enerated data
Re-admissions reimbursement
PQRI and RHQDAPU
Health-Associated Infections Evolution of the patient-centered
medical
home
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
27/30
Subtitle C-Creating Healthier Communities/Sec. 4201ommun ty rans
ormat on rants-grants to
promote individual and community health andprevent the incidence
of chronic disease
Sec. 4302 Understanding health disparities; datacollection and
analysis-
-workforce
Sec. 6301- Patient-Centered Outcomes Research
ec. ommun y- ase co a ora ve carenetworks.
Sec. 10334- Minorit Health- codifies OMH andelevates the NCMHHD
to an Institute
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
28/30
Dis arities tentativel June 4
Care coordination P l i n li h l h
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
29/30
Healthcare is local !
Challenge: The power to change the systemis in your hands.
-
8/9/2019 Health IT_Why Now_Health Disparities Summit
30/30
htt ://healthit.hhs. ov