Embed Size (px)
Citation preview

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
te
Assessment ofPrimary medical care
in The Universal Coverage Scheme
Thaworn Sakunphanit, Director, Health Insurance System Research Office (HISRO)
Health Systems Research Institute (HSRI).Ministry of Public Health
Ningxia, China8-9 May 2014

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
te
• Design• Accessibility
– Take up rate• Responsiveness of Health Care System
– Patient experiences• Clinical Output/Outcome
2

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
te
Risk
stra
tifica
tion Low
Medium
High Perio
dic
Scr e
e nin
gM
o di fy
risk
pro
g ra m
s
Acute care
Chronic careand
Terminal care
DiseaseManagement
Case Management
Source: Modified from Kongstvedt, Peter R (2001).The Managed Health Care Handbook.
Care Program
Design:Continuum of Care & Strategic Purchasing

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
teTake Up Rate of UCS:Equity in utilization
4
Note: CI range from -1 to + 1. Minus 1 (plus 1 ) means in favour of the poor (rich), or the poor (rich) disproportionately use more services than the rich (poor).
Health centre Community hosp Provincial hosp Private hosp Overall
2001 -0.294 -0.271 -0.037 0.431 -0.090
2003 -0.365 -0.315 -0.080 0.348 -0.139
2004 -0.345 -0.285 -0.119 0.389 -0.163
2005 -0.380 -0.300 -0.100 0.372 -0.177
-0.50
-0.40
-0.30
-0.20
-0.10
0.00
0.10
0.20
0.30
0.40
0.50
Concentration Index of OP service by type of health facilities: 2001 - 2005
Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
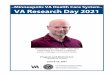
teProblem of Take Up Rate
Ambulatory Services In-patient Services
Perc
ent
Acu
te il
lnes
s
Acc
iden
tan
d In
jurie
s
Chr
onic
illn
ess
Illne
ss
Acc
iden
t
Chi
ld d
eliv
ery
Oth
ers
Prev
entio
n
Legally eligible, but do not claim for benefits
No eligibility
Don’t answer
Source: HISRO (2014) Analysis from Health Welfare Survey 2011 of the NSO
• Vary among different benefits• Still occur in low-income group
Legally eligible, and claim for benefits
Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
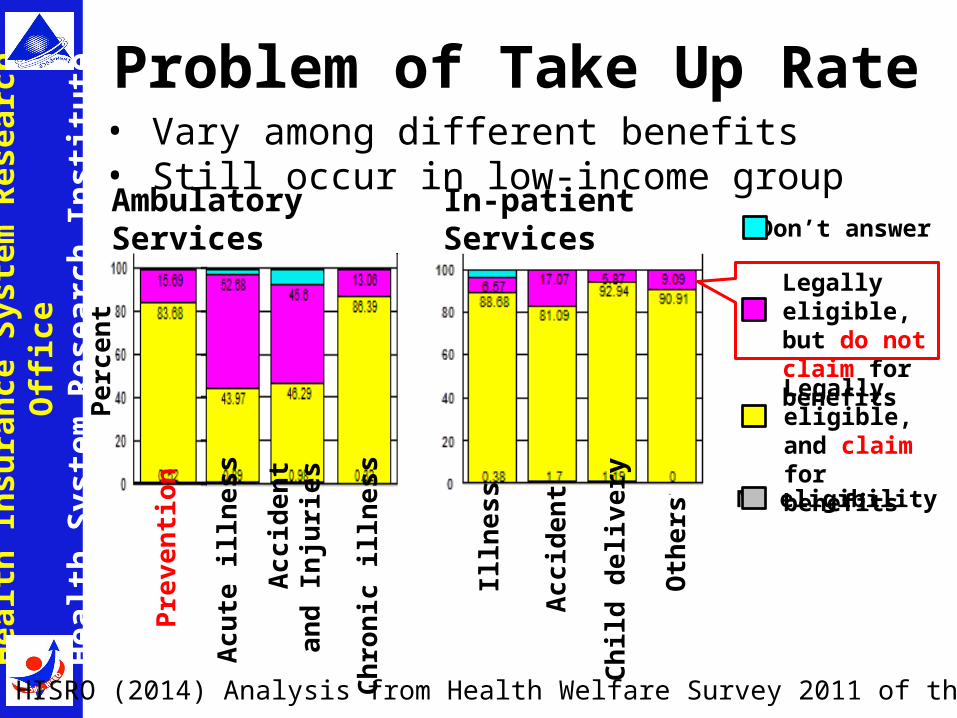
teTake Up Rate of the UCS:Risk screening in 2011
Source: NHSO

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
teTake Up Rate of the UCS:
Vaccines coverage in 2012
Source: NHSO

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
teTake Up Rate of the UCS:
Vulnerable Group• Qualitative study of take up benefits of the UCS in 2
urban areas showed 3 groups of legally eligible elders: Take-up, Temporary non-take-up and Non-take-up.
• Determinants of take-up decisions comprise cost, time of traveling, quality of care and quality of services
Source: Suwanrada (2010) In-depth study on utilization benefits of the Universal Health Coverage Scheme of urban elder

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
te
9
Responsiveness of Health Care System for Beneficiaries of UCS
02
46
810
excludes outside values
Dignity AutonomyConfidentiality CommunicationPrompt BasicAmenities
choice
Client orientationRespect for person
• Lower in high education groups• Higher in private health care facilities
Source: HISRO (2012) Study for Development of Responsiveness Tools.
Note: Exit survey of 7,500 beneficiaries from 43 facilities (hospitals) using Stratified three-stage sampling techniques
Dignity
Autonom
y
Confiden
tialit
y
Comm
unicatio
n
Prom
pt
Basic
Amen
ities
Choices
Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
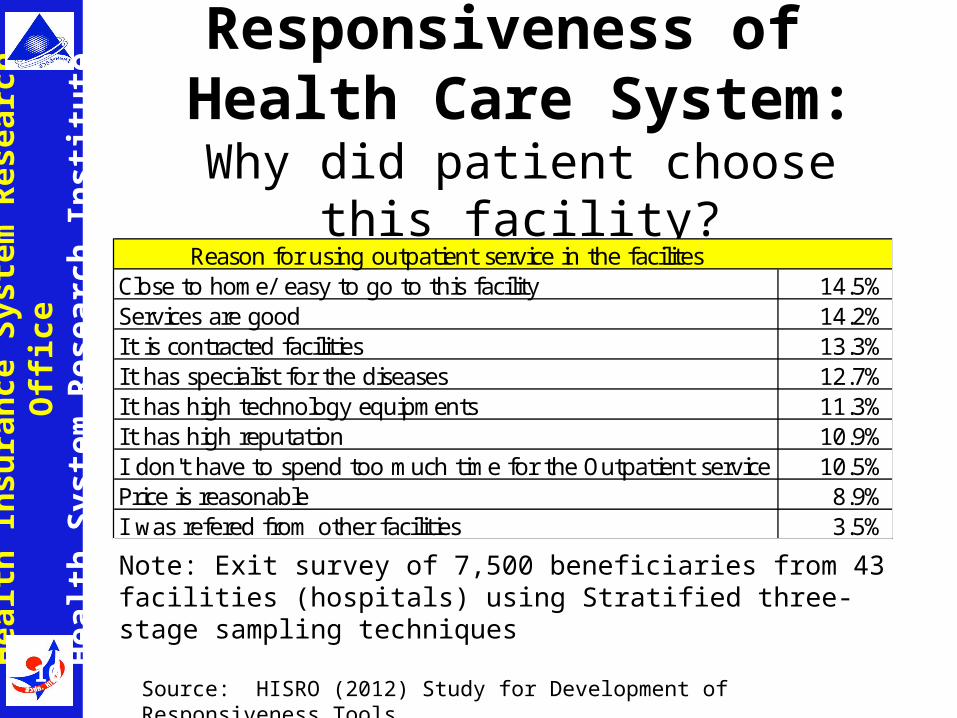
teResponsiveness of
Health Care System:Why did patient choose this facility?
10
Note: Exit survey of 7,500 beneficiaries from 43 facilities (hospitals) using Stratified three-stage sampling techniques
Source: HISRO (2012) Study for Development of Responsiveness Tools.
Reason for using outpatient service in the facilitesClose to home/ easy to go to this facility 14.5%Services are good 14.2%It is contracted facilities 13.3%It has specialist for the diseases 12.7%It has high technology equipments 11.3%It has high reputation 10.9%I don't have to spend too much time for the Outpatient service 10.5%Price is reasonable 8.9%I was refered from other facilities 3.5%

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
teAmbulatory Care Sensitive Conditions
(ACSC): Preventable Admission
Source: HISRO (2010);: Analysis of Inpatient Database of CSMBS, and UCS .

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
teCommunity Based National Survey
Distribution of Patients by Treatment Outcome
0%
20%
40%
60%
80%
100%
2003-4 2008-9 2003-4 2008-9 2003-4 2008-9
Hypertension Diabetic Hypercholesterol
No diag No trearment Uncontrol Control
Source: Aekplakorn (2010): Analysis of Health Exam Survey 2003-2004 and 2008-2009.

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
teMedical Record Reviewed of UCS:
Diabetic Miletus Type II
13 Source: Rangsin et al (2011, 2012 and 2013).
Note: Percentage of Controlled cases using Fasting Blood Sugar was a little bit higher than using HbA1c
Stratified cluster sampling from 600 facilities out of total 1013 CUPs (hospitals and clinics)

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
teChallenges
• Accessibility and quality of Primary medical care in The UCS has continuously improved
• However, low take up rate of Primary medical care is still challenge issue of the UCS
• Appropriate measures for different target groups to improve health literacy, self care and people participation
• More efficient “Chronic Care Model” is also needed for better quality and outcome of health care services.
14

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
teChallenges (Cont.)
• Increase role of Local governments in health care e.g. decentralization of Primary Medical Care to Local governments
• Mitigate and cope with Aging Society– Community-based Long Term Care, which need
harmonization of Primary Medical Care and Social care, will affect the design and implementation of Primary Medical Care.
• Economic growth, which creates more middle income group, will also create more pressure for better hospitality services and choices
15

Hea
lth In
sura
nce
Syst
em R
esea
rch
Offi
ceH
ealth
Sys
tem
Res
earc
h In
stitu
te
Thank You
16