Embed Size (px)
Citation preview
Health Information Technology Issues in the 2015 Texas Legislative Session
Nora Belcher, Executive DirectorTexas e-Health Alliance
December 12, 2014
What is the Texas e-Health Alliance?• State’s leading advocate, from local communities
to the national level, for the use of health information technology to improve the health system for patients
• 501(c)6 non-profit started in 2009• Serves as a trade association for HIT companies
Slide 2
Background
This presentation will:• Provide an update on state level HIT activities,• Preview a number of HIT topics that will be
discussed during the 2015 session of the Texas Legislature, and
• Update attendees on the current state of the Sunset Commission review of Texas HHS system.
Slide 3
Overview
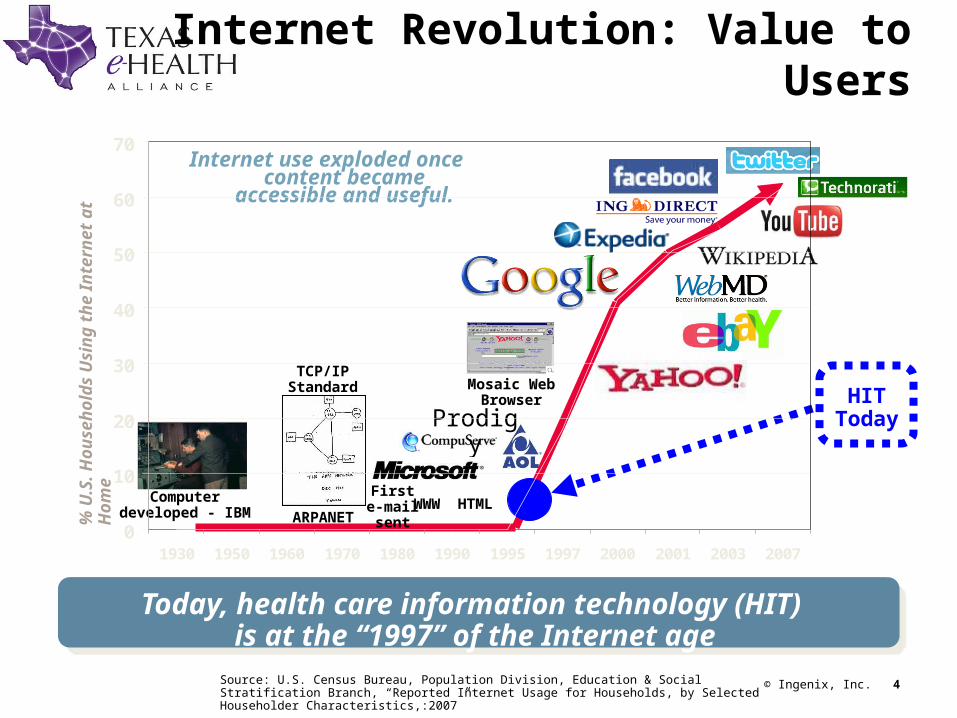
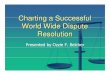
Internet Revolution: Value to Users
Internet use exploded once content became accessible
and useful.
0
10
20
30
40
50
60
70
1930 1950 1960 1970 1980 1990 1995 1997 2000 2001 2003 2007
© Ingenix, Inc. 4
Computer developed - IBM ARPANET
Mosaic Web Browser
Today, health care information technology (HIT) is at the “1997” of the Internet age
Prodigy
WWW HTML
TCP/IP Standard
Source: U.S. Census Bureau, Population Division, Education & Social Stratification Branch, “Reported Internet Usage for Households, by Selected Householder Characteristics,:2007”
% U
.S. H
ou
seh
old
s U
sin
g t
he
Inte
rnet
at
Ho
me
HIT Today
First e-mail sent
State Level Activities
• Electronic Health Record and Health Information Exchange Initiatives– HHSC administered EHR Incentive Program and local
HIE grant program (over $ 600 million)– Texas Health Services Authority and local HIEs moving
into implementation and interconnectivity
• Telemedicine, Telehealth and Home Monitoring– TMB adopted 2 models of telemedicine in Fall 2010– SB 293 (2011) expanded telemedicine and telehealth in
FFS Medicaid and set up a remote monitoring benefit– SB 7 (2013) encouraged the use of telemedicine in
nursing homes by managed care plans– TMB rule review fall 2014
Texas Legislature
• Before 2005 – 0 health IT bills filed• 2005 – 1 health IT bill filed• 2007 – 6 health IT bills filed• 2009 – 30 health IT bills filed• 2011- 3 health IT bills filed
– Electronic prescribing– Privacy– Telehealth/remote monitoring
• 2013 – 1 health IT specific bill filed– Driver’s license mag swipes
• THSA funding• DPS drug database access• Telemedicine in nursing homes
Page 6
Topics for 2015
Interoperability and use of standards in state agency IT systems
– HB 2939 filed in 2013 but did not pass– HHSC adopted policy in summer 2014
• Requires state agencies to develop interoperability plans and move towards using standards in IT systems
• Much work is needed to further define what data can be shared with who and when
• Long term view: the state should see improvements in data quality, provider reporting, and project management
Page 7
Topics for 2015
Access to public health registries for HIEs– Many of the governing statutes for public health registries
(immunization, lab reporting, etc) predate HIE– Legal concerns have been raised that providers cannot
delegate their required reporting to the state to their local HIE
– DSHS and THSA Sunset reports identify this as a barrier– Long term view: this will support a business case for HIEs
to do reporting, creating administrative simplification for the state and for providers, and improving the timeliness and accuracy of the data
Page 8
Topics for 2015
Medicaid/CHIP Health Information Exchange– Created by HB 1218 in 2009, before HITECH state grants
for HIE were public– Intended to create a function similar to the Foster Care
Passport, and provide claims data to Medicaid providers – Project implementation was delayed due to concerns
about consent and privacy; currently in pilot– Long term view: through Sunset, this project needs to be
reviewed and revised to better align with state HIE strategy.
Page 9
Topics for 2015
Remote monitoring– Medicaid remote monitoring benefit was created by SB
293 in 2011– Benefit was limited in scope and confined to certain
diagnoses and included a Sunset provision for the benefit unless recreated by the Legislature in 2015
– Long term view: The shift to managed care makes the Medicaid fee for service rule less important, but still necessary. Medicare penalties for readmission rates have strongly increased hospital interest in this benefit.
Page 10
Topics for 2015
Consumer telemedicine– Current Texas Medical Board rules require a face to face
visit or a referral before a patient can receive telemedicine services from a non-clinic location
– Tech companies and insurers are developing totally virtual clinic models in response to consumer demand and increasing sophistication of devices and peripherals
– Long term view: The legislature will have to weigh access and convenience for consumers and businesses vs. some risk that virtual visits may not present the physician with 100% of the needed data
Page 11
Topics for 2015
Provider/HIE “safe harbors”– Providers frequently cite the lack of legal precedents around
the use of HIEs as a barrier to HIE adoption– Concerns have been raised about who is liable if the
information in an HIE is incorrect and used in a treatment decision
– THSA through Sunset is pursuing clarification that providers and HIEs are responsible only for their own errors
– Long term view: as more and more data becomes available to providers, a standard of care will need to evolve that gives providers clear guidance as to their obligations regarding HIE
Page 12
Sunset Process
THSA, HHSC, DADS, DARS, DSHS, DFPS, and the Texas Health Care Information Council are all under review
– Self-evaluation reports are available for all agencies
– Sunset staff reports and commission decisions are available for DADS, DFPS, DARS, and DSHS
– THSA, THCIC, HHSC and HHS enterprise reports will be out in October/November
Page 13
What Does It Mean?
• Intense pressure on the state and on providers to show ROI for HIE
• Federated approach means localized data, so many providers will still juggle multiple interfaces
• Consumer demand will rise for:– curation and aggregation of their data. No one
wants 10 separate patient portals– online access to their doctor- or a doctor.
Page 14























![[Wendy Laura Belcher] Writing Your Journal Article](https://img.pdfslide.us/doc/110x75/577c7f921a28abe054a52463/wendy-laura-belcher-writing-your-journal-article.jpg)


