Embed Size (px)
Citation preview

MOPH
2012
Health Information
System Tools in
Afghanistan
M O P H _ H M I S D E P A R T M E N T

2
Table of Contents
Introduction………………………………………………………………………………………………………………………..4
Health Management Information System…………………………………………………….………………………5
Balanced Scorecard……………………………………………………………………………………………………………10
National Monitoring Checklist…………………………………………………………….……………………………..13
Diseases Early Warning System…………………………………………………………………………………………..14
Human Resources Database……………………………………………………………………………………………….15
CHW-HR Database…………..…………………………………………………………………………………………………16
Training Database………………………………………………………………………………………………………………18
Afghanistan Tuberculosis Information System (ATBIS)………………………………………………………..19
LQAS Database……………………………………………………………………………………………………………………20
Essential Drug List/License Drugs List…………………………………………………………………………………21
Health Related Studies/Special Studies Database………………………………………………………………..23
Grant Database……………………………………………………………………………………………………………………24
Standard Based Management & Recognition……………………………………………….……………………..24
Fully Function Service Delivery Point (FFSDP)……………………………………………………………………..24
Partnership Defined Quality……………………………………………………………………………………………….24
Healthcare Improvement (HCI)…………………………………………………………………………………………..25
Afghanistan Health Survey…………………………………………………………………………………………………26
National Risk and Vulnerability Survey………………………………………………………….……………………27
Afghanistan Multi Indicator Cluster Survey (AMICS)…………………….…………………….….……………28
Central Statistic Organization Population Estimation…………….…………………….………...…………..28
Lesson Learn from Past Experiences……………………………………………………………………..…………...29
Health Monitory & Evaluation Framework………………………………………………………….….…………..31

3
Introduction:
The Ministry of Public Health (MoPH) has adopted a Stewardship role in the health sector. The
Ministry is committed to enhancing evidence-based, bottom-up and participatory strategic
planning in all levels of the National Health Care System (NHCS). The Health Information System
(HIS) strives to ensure the availability, coordination, distribution and use of accurate, reliable,
and user-friendly health information in health service and program design, implementation,
Monitoring and Evaluation (M&E) and related activities. The MoPH uses a variety of sources
from which to gather information useful for health system management. Afghanistan’s Health
Information System (HIS) is primarily comprised of the following components:
1. Periodic Reports (Monthly, Quarterly, Semi-Annual, and Annual) to transmit data between
service levels. This component is the Health Management Information System (HMIS) 2. Results of periodic national and sub-national surveys and evaluations (e.g., household
surveys, facility assessments). this component is partly addressed by application of the National Monitoring Checklist and several periodic data collection exercises like the Third Party Evaluations.
3. Surveillance reports to communicate epidemic information about notifiable and newly emerging diseases that require immediate action. This component is called the Disease Early Warning System (DEWS)
4. Qualitative information collected from communities, health workers and program staff through both formal and informal channels.
5. Demographic data and vital statistics are obtained through the Central Statistics Office (CSO)
These systems have arisen with support of various partner agencies during the recovery and
reconstruction period, including WHO, the World Bank, the EC and USAID.

4
Health Management Information System
The HMIS is a system based on qualitative and quantitative indicators in which routine health
information is collected, processed, analyzed, interpreted, disseminated, and used to improve the
provision of health services according to the MoPH’s priorities and ultimately to improve the health
of the population. In addition, the information generated can be used for research and training
purposes. As part of a larger Health Information System (HIS), the HMIS proper mainly addresses the
periodic routine reports, including the data collection tools needed to compile the reports.
Purpose:
Afghanistan’s Health Management Information System is designed to:
1. Help health workers better manage their services and health facility supplies and resources;
2. Help health workers in their efforts to organize and monitor health development work in their communities;
3. Provide data to provincial MoPH and NGO managers for supervision and other supportive action;
4. Provide data to provincial and national program staff, and to donors for planning, monitoring and evaluation.
Existing HMIS forms
Pictorial Tally Sheet
Monthly Activity Report (Health Posts) - MAR
Monthly Aggregated Activity Report – MAAR
General Register – Facilities
Monthly Facility Tally Sheet
Monthly Integrated Activity Reports (Hospital OPD/CHC/BHC/SHC/MHT) – MIAR
Facility Status Report (CHC/BHC/SHC/MHT) – FSR
Catchment Area Annual Census (CATCHMENT AREA ANNUAL CENSUS (CAAC))
o Pictorial Data Collection Sheet
o CATCHMENT AREA ANNUAL CENSUS (CAAC) Report – Village Level/Facility Level
Hospital Monthly Inpatient Report (Hospitals and larger facilities with inpatient care) – HMIR
Hospital Monthly Tally Sheet
Hospital Status Report (Hospitals) – HSR
The previously included Notifiable Disease Report has been transferred to and incorporated into
DEWS.

5
HMIS functions by health system level
Health Post Level
Data collection Pictorial tally sheet Annual Census of catchment area population tally-sheet (CATCHMENT AREA ANNUAL
CENSUS (CAAC)) Data use
Analysis with assistance from HSC/BHC/CHC/DH during supervisory visits Planning of activities with assistance from HSC/BHC/CHC/DH Match performance (MAR) with coverage (CATCHMENT AREA ANNUAL CENSUS (CAAC))
Reports
Monthly Activity Report (MAR) with HSC/BHC/CHC/DH CATCHMENT AREA ANNUAL CENSUS (CAAC) – Health Post Level Report Feedback to Community Health Committees
Health Facility Level Data Collection
Data collection of activities in register(s) and patient card(s) Tally sheets Inventory records on essential drugs and supplies, equipment and staff Yearly census of households in catchment area ( CAAC)
Data Use
MIAR analysis – functioning of facility MAAR analysis – functioning of community based activities supervised by the facility HMIR analysis – functioning of inpatient departments Hospital Status Report analysis – availability & accessibility of care CATCHMENT AREA ANNUAL CENSUS (CAAC) analysis – cross check between activities and
coverage Facility Status Report analysis – availability & accessibility of care Investigation of notifiable diseases (through DEWS) – containment of epidemics Supervision of and feedback to Health Posts – improve performance of community-based
activities Feedback to community health committees Monthly, quarterly and annual activity planning
Reports
Monthly Integrated Activity Report (MIAR) Monthly Aggregated Activity Report of Health Posts (MAAR) Facility Status Report (FSR) Hospital Monthly Inpatient Report (HMIR) Hospital Status Report (HSR) Annual Census Report (CATCHMENT AREA ANNUAL CENSUS (CAAC) – Facility Level Summary
Report) Notifiable Diseases Report (through DEWS)

6
Provincial Level Data Storage
Status of facilities Staffing of facilities Service Statistics Grants Management Training data
Data Use
Aggregation and/or computerization of: - Monthly Integrated Activity Reports - Hospital Monthly Inpatient Reports - Monthly Aggregated Activity Reports - Catchment Area Annual Census - Facility and hospital status reports
Analysis and feedback to facilities - Supervision - 6 monthly or quarterly meetings - Written feedback reports
Provincial annual planning and progress monitoring Follow-up on Notifiable Diseases Report (DEWS)
Reports
Aggregated MIARs Aggregated HMIRs Aggregated MAARs Aggregated CATCHMENT AREA ANNUAL CENSUS (CAAC) Staffing changes Aggregated facility and hospital status reports Grants report Notifiable disease reports (through DEWS)
National Level Data Storage
Facility Codes and Database Staff Codes and Database Service Statistics Database Grants Management Database Training Database
Data Use
Analysis and calculation of national indicators Feedback to provinces:
- Supervision - Written reports - Annual planning meeting - Information on request
Follow-up on notifiable diseases reports

7
Reporting
Annual progress report on health status (BPHS indicators) Health information (e.g., Newsletters) Standard reports for use by other departments (HRD/GCMU/PLO)
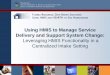
Provincial Public Health Directorate (PPHD) manages a hub:
Figure 1 - Computerization of HMIS: Ideal situation
MOPH
Master
PPHO
Hub
NGO
Replica
BHC/ CHC/
DH/ PH
Contracted
Out
Health Post Community
BHC/ CHC/
DH/ PH
Contracted
In

8
Health Posts and Community information (CATCHMENT AREA ANNUAL CENSUS (CAAC)) arrive at
facility level in paper format. The Facility sends paper reports to the NGO (for contracted-out
facilities) or to the PPHO (for contracted-in facilities). The NGO or the PPHO enters the received
information in a replica. The NGO sends a CD to the PPHO, where the replica is synchronized and
the NGO receives a new replica and analysis copy, both of which include the most recent data of the
NGO along with all data from other NGOs.
Health Posts and Community information arrive at the facility level in paper format. The Facility
sends paper reports to the NGO (for contracted-out facilities) or to the PPHO (for contracted-in
facilities). The NGO or the PPHO enter the received information in their respective replica. The NGO
and the PPHO send the replica to the MoPH, where it is synchronized with the Master hub. The
PPHO and the NGO receive a new replica (including an analysis copy), both of which include the
most recent data of the NGO along with all data from other NGOs.
Health Posts and Community information catchment area annual census S (CAAC)) arrive at facility
level in paper format. The Facility sends paper reports (including aggregated HP reports) to the NGO
(for contracted-out facilities) or to the NGO. The NGO enters the received information in a replica.
The NGO sends the replica to the MoPH, where it is synchronized with the Master hub. Both the
PPHO and the NGO get a new replica and analysis copy, both of which include the most recent data
of the NGO along with all data from other NGOs.

9
Balanced Scorecard BSC is a tool for assessment of performance as well as measurement of the quality of basic health care. Balanced scorecard provides a framework that not only provides performance measurements, but helps planners identify what should be done and measured. It enables executives to truly execute their strategies.
The purpose of the Afghanistan Health Sector Balanced Scorecard is to summarize
the performance of Afghanistan’s provinces in the delivery of the Basic Package of Health
Services (BPHS), and to provide policymakers, health managers and other decision makers
with evidence for areas of strength and weakness. The Balanced Scorecard (BSC) provides a
frame‐work to efficiently look at multiple areas of the health sector called domains,
which each contain an array of indicators. This allows the Ministry of Public Health (MoPH)
and other stakeholders in the health sector to visualize the performance of various provinces
as well as how the country is providing health services. The 2009/10 BSC can be compared to
the 2004, 2005, 2006, 2007 and 2008 BSCs, allowing for an assessment of the progress
made over the first six years of BPHS implementation in Afghanistan. The benchmarks
used in the 2005, 2006, 2007, 2008 and 2009/10 BSCs are based on the performance of
provinces documented in the 2004 BSC.
The BSC is not only a measurement tool; it is used by the MoPH to clarify its vision and
strategies, and to manage change. The BSC provides a framework to organize activities and
learn from experience. Six domains comprising of29 indicators were selected to summarize
health sector performance. This was determined through a participatory process that
involved the MoPH, NGOs and other development partners, and was facilitated by the
Third Party Evaluation team from the Johns Hopkins Bloomberg School of Public Health
(JHSPH) and the Indian Institute of Health Management Research (IIHMR). The BSC domain
summarizes the health sector from the following six perspectives:
1. Patients and Community
2. Staff
3. Capacity for Service Provision
4. Service Provision
5. Financial Systems
6. Overall Vision (MoPH Values)

10
How to Read the Balanced Scorecard
The BSC tables are color-coded to be easier to read. Numbers in green colored cells indicate that the result is above the upper benchmark (usually one of the top six provinces). Results shown in red cells indicate that it is in the bottom quintile (Bottom six provinces). All results in-between the top and bottom quintile are shown in yellow cells. The first 28 indicators are classified according to one of six domains. The first 26 of the indicators are measured as percentages. In some cases, the number shows what recent of the results in a province met a certain standard (e.g. Indicator 1 is the percent of patients that rated their satisfaction with health services as “highly satisfactory” on a 4-point scale; Indicator 5 shows the percent of staff salary payments that are up to date). In some cases, the percentage shows what percent of items in an index have been achieved (e.g. Indicator 6 shows the percent of expected equipment that is present and working). Two of the indicators are Concentration Indices, which is a measure of quality, where the results can range from -1 to 1. Each attribute (outpatient visits for Indicator 27 and satisfaction with services for Indicator 28) is analyzed according to how it is distributed among the population that is grouped according to their wealth. A result of -1 means that the most poor people in the province received the entire attribute (e.g. all outpatient visits or satisfaction). Result of +1 means that only the wealthiest people had the attribute. A “0” means that the attribute is equally distributed among the rich and poor. Detailed definitions for each of the indicators are described in the methods section of this report. The last two indicators in the BSC are composite indicators put at the bottom of the BSC. One is an indicator is called “The percent of upper benchmarks achieved”, and the other “the percent of lower benchmarks achieved”. The first is a composite indicator that demonstrates how well provinces have done in meeting the upper benchmarks across all of

11
the first 28 indicators. The second indicator measures how well provinces have done in meeting the lower level benchmarks across the first 28 indicators.
Current BSC:
During National Health Services Performance Assessment annual round 2004 – 2008, typically data
collection was performed during the summer months (July – September) all across the country. It
was suggested by various staked holders to plan the survey in such a manner so that the period of
data collection is not too predictable for the implementers. This will encourage the implementers to
ensure the delivery of high quality services across the year, instead of focusing just on a three
months window when the data collection was done earlier. It also takes into account the seasonal
variations in health service delivery.
Hence, for the 2009/10 round year round data collection approach was put into effect. A summary
of the period of data collection for each province is mentioned below in the table below.
National Sample 2004 - 2012
UNIT 2004 2005 2006 2007 2008 2010 2012
Number of Provinces 33 30 30 30 29 34 33
Number of Facilities 617 629 630 636 618 726 738
Number of Observations of Patient-Provider Interactions
5719 5856 5964 6089 5970 7979 6826
Number of Exit Interviews 5597 5862 5964 6087 5950 7979 6826
Number of Health Workers Interviewed
1553 1452 1723 1940 2233 2281 2393

12
National Monitoring Checklist (NMC) database
Purpose: The NMC is designed to monitor the implementation of the BPHS at provincial level by the
PHOs with the implementing partners. The purpose of National Monitoring Checklist (NMC)
database is to provide support to MoPH monitors, NGO managers, Provincial Health Office staff, and
central level MOPH staff to enter, maintain and analyze monitoring data. NMC database contains
detailed information on National Monitoring Checklist. All monitors and others who participate in
the monitoring process should enter the contents of NMC at the end of the mission to the database.
The database contains two modules. One module pertains to the monitoring of health facilities.
While the second component allows entry of monitoring results from health posts.
Data flow: Ideally, the NMC should be managed at provincial level by the PHOs with support by the
M&E Directorate. A copy of NMC database has been given to all provinces to enter, maintain and
analyze their provincial data.
Type of database: NMC database has to types 1) Data entry version and 2) Analysis version.
Data entry version is for entering the NMC data and contains provincial information only. This
version is kept by provinces and MoPH monitors.
The Analysis version is maintained by MoPH, M&E department and contains national data. This
version is shared with provinces and the central MoPH Department on quarterly basis for data
analysis.

13
Disease Early Warning System (DEWS)
Disease Early Warning System (DEWS) started its activity originally with eight Sentinel Sites (SS)
in eight regions of Afghanistan in the second half of December 2006. The main objectives of the
system was/ is to detect cases and collect information on 15 target diseases in early stage and
take necessary action to respond to the outbreaks and control the further spread of diseases, so
that contribute actively in reducing morbidity and mortality, especially among the vulnerable
groups of Afghan population. Later on the system extended its coverage in neighboring districts
and provinces gradually, so that currently (April 1, 2008) 129 Sentinel sites are functioning in 34
provinces of the country under the DEWS Surveillance System. All Sentinel Sites have to send
their reports on weekly basis to Afghan Public Health Institute, Ministry of Public Health. At
present, the verification, compilation and analysis of the received field reports take place
manually on weekly basis.
Database Specifications
1) The database can be linked with another database. 2) Is able to accept the field report entry and synchronize the received reports from sentinel
sites, so that the development of a hub-module will be needed. 3) Is able to check the received data for accuracy. 4) IS able to be linked with GIS-Mapping. 5) Usually, DEWS (Disease Early Warning System) receives reports from sentinel sites on
weekly bases in Excel sheets or MS Word format and it is expected that the DEWS database should be able to produce the following reports:
6) a- Disease occurrence by Week b- Disease events on monthly basis c- Provide reports on quarterly basis d- Produce Semi-annual reports and annual reports on all 15 DEWS Target Diseases. e- Provision reports on target diseases by province f- Provision reports on target diseases by district g- Provision reports on target diseases by health facility/sentinel sites h- Provision reports on target diseases by region and i- Provision reports on target diseases in country level. j- Produce of quality reports and charts according to needs. k- In case of adding new sentinel sites or reducing some, the application should be able
to accept the changes.

14
Human Resources (HR) Database
Since 2004 the MOPH has started registering all human resources working as MOPH employees, or
active in the contracted out facilities and services.
Data are being collected by the General Directorate of Human Resources in the HR database, linked
to HMIS, on current staff. This is a comprehensive database containing sufficient fields to satisfy the
needs for human resource information at all levels within the ministry and NGOs. It is maintained by
a team working in the Ministry of Public Health. It includes job descriptions, and qualifications. It
covers all Afghans employed by the ministry and by NGOs. Having been entered into this database
the employee receives one of four types of identity card: a blue MoPH Permanent Government
Employee ID card; a similar yellow one for temporary and contracted staff; a white National Health
Worker Registration ID; and a Student of IHS/CME Registration ID. Each card carries a photograph of
the individual and is signed on behalf of the Head of Personnel. Each individual also receives an HR
ID Number. The other data contained within these cards are the individuals’ dates of birth and the
dates of issue. Students retain the same number after graduation.
An Access-based modular database has been developed and contains presently the identification of
some 33,000 health workers. Upon registration all health workers have received a MOPH ID card,
confirming they are officially registered with the MOPH. This ID card does not signify employment as
civil servant. It does however contain the unique MOPH identification number of the health worker.
For each registered health worker, the database contains personal identification, present dwelling
place, present place of activity, educational and additional training history at the time of
registration, language skills, and (only for MOPH employees) disciplinary history.
The HR database relies on the facility and administrative units listings of the HMIS database.
At present the registration and inclusion in the database has been centralized by the MOPH in Kabul.
The decentralization of the updating process (using the hub model of the HMIS database) has been
started.

15
CHW-HR Database
Introduction The HR CHW Database allows storing the data on CHW information; this may include data on
Personal Information, Training and Language skills. It also helps easy analysis of the CHW
information at different levels by the built-in summary reports and graphs. In addition it allows
extracting of data at any level through the creation of customized queries. A Hub module was
developed to allow aggregating HR CHW Information from different locations where data is entered
in all provinces of Afghanistan .This HR CHW database is linked with other MOPH databases such as
HMIS and Human Resources, and shares common databases.
Data collection The base for the design of the CHW database is collecting of Community Health Worker data
collection form that captures specific information about the CHW, the . The collected data is then
entered into the computerized HR CHW Database for further data manipulation. Therefore, the
more completely and more accurately data is collected initially on the pre-defined forms, the more
accurate the data stored in the HR CHW Database will be, allowing, through analysis, the obtaining
of accurate information for decision making and Management issues .
The HR CHW data collection form in could one data collection forms. 1. HR CHW Registration,. Each
of the forms should be filled completely and accurately. Information Field should be filled by the
CHW. For detailed description about what data values required to be collected on each of the
format, please see HR CHW Registration guideline, .
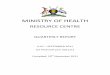
Data flow The data is collected from the CHW, then it is entered into the database and after that the database
(replica) is sent to MoPH HR CHW Hub where the database is synchronized to the Hub.
Any changes/updates like structural changes and adding new modules or reports to the database
will be brought to master copy of the HR CHW database and then replicated to hub and then to the
replica (Figure 1)

16
Figure 2: HR CHW Database Dataflow
Frequency and Method On quarterly (or more frequently if desired) basis MoPH Human Resource General Directorate that
uses the database will create a copy of their database back-end and send it to MoPH Human
Resource General Directorate through CD . MoPH will synchronize all of the HR CHW databases into
the Hub.

17
Training Database
The training database is developed in MS-ACCESS, with customized reports in MS-Excel pivot tables.
It allows storing the data on trainings, workshops and seminars provided by MoPH and partner
organizations. This may include data on pre-service and in service, initial or refresher trainings. It
also helps easy analysis of the training data at different levels by the built-in summary tables and
graphs. In addition it allows extracting of data at any level through the creation of customized
queries.
A Hub model (based on the HMIS model) was developed to allow aggregating training data from
different locations where data is entered.
The Training Database uses listings in the HR database and the HMIS database as lookup tables. The
linkage with the HMIS database allows spatial analysis of the data.
Over time the database will contain the training history of all registered health workers in
Afghanistan.

18
Afghanistan Tuberculosis Information System (BIS)
The TBIS database allows data entry of TB diagnosis, and TB treatment information collected at
health facilities/TB units on quarterly basis at province and/or NGO level. ATBIS database can
facilitate tracking the progress of TB information pertaining to individual facility, districts, and
provinces and at the country level or project/program level. The TBIS manual guides the user
through installation, data entry, and use of the software.
Data collection forms
The TBIS is designed upon the data flow of the data collection forms and is completed on a quarterly
basis by facilities TB services. The collected information on these forms is then entered into the
database. The TB information is collected through 4 main forms (TB Suspect Management, TB Case
Registration, TB SS Microscopy Conversion, TB treatment outcomes).The TB conversion form must
be completed with three months of retrospective data. For example, if you are filling this form at the
end of June, you must report the status of those patients who were registered during the month of
April, and the TB treatment outcomes form should be filled from 8 months back reporting status of
the patients who were registered eight months ago. For example, if you are filling the form at the
end of July 2009, the report should be from December 2008.

19
PMIS
PMIS as an information system that collects, integrates processes, analyzes, and reports on
pharmaceutical, logistics, and patient data. There are two main purposes when setting up a PMIS.
The first is to synthesize the large volume of data generated by pharmaceutical management
operations and process it into information for use in planning activities, estimating demand,
allocating resources, and monitoring and evaluating pharmaceutical management operations. The
second purpose is to create an audit trail for products as they enter or leave a pharmaceutical
supply system.
Several sub-modules of the overall PMIS have been identified, and for each either the existing
database module has been updated and improved, or the development of a new model has started.
Following are the modules that functioning:
1. EDL/LDL database
2. Pharmaceutical Registration Information System (PRIS
3. Pharmaceutical Logistics Information System (PLIS): in close collaboration with the
CPDS DIC, a database module will be developed to facilitate aggregation and
reporting of the pharmaceutical supply management information needed by the CPDS
Introduction to PRIS Database
The drug management information system (PRIS) is developed in MS-ACCESS. It is used to
enter information about drug manufacturing company, brand name registration, and also enter
information about items imported inside the country. The database also provides features to
extract information already existed in the database.
Essential Drugs List /License Drugs List Database
The Licensed Drug List contains all medicines that can be imported and sold in Afghanistan, under
their International Non-proprietary Name (INN), when it exists, otherwise the United States Adopted
Name (USAN) or the British Approved Name (BAN) is chosen.. The LDL contains all the drugs listed in
the Essential Drugs List, and hence contains all the drugs recommended for use in the BPH, EPHS and
the MoPH’s national programs. It also contains dispensary products and products used in dentistry.
It is used as guideline by the authorities granting import licenses for drugs used in the public and
private sector.
After considering several options, the Committee decided to adapt the An Atomo Therapeutical
Chemical (ATC) classification, promoted by the WHO Collaborating Centre for Drug Statistics
Methodology, which is itself adapted from classification system developed by the European
Pharmaceutical Market Research Association (EPhMRA) and the Pharmaceutical Business
Intelligence and Research Group (PBIRG).
The classification allows to group drugs in several categories, according to the organ or system on
which they act and their chemical, pharmacological and therapeutic properties. Five different levels
are used. The drugs are divided into fourteen main groups (1st level), with one
pharmacological/therapeutic subgroup (2nd level). The 3rd and 4th levels are

20
chemical/pharmacological/therapeutic subgroups and the 5th level is the chemical substance. The
2nd, 3rd and 4th levels are often used to identify pharmacological subgroups when that is
considered more appropriate than therapeutic or chemical subgroups.
Thus each chemical substance in the LDL has its 7-digit ATC code. This implies that the same
substance listed under different administrations forms or presentations will have the same ATC
code. The ATC code is not a unique identifier for each individual drug included in the LDL.
In addition, the recommended level of use in the BPHS and/or EPHS and/or vertical MOPH programs
for each drug is given.
The General Directorate of Pharmaceutical Affairs maintains and manages the updating of the
database. Detailed instructions for updating and including new products in the LDL or EDL are
included in the published LDL and EDL.
1.

21
Lot Quality Assurance Sapling (LQAS) database
Purpose: The purpose of Lot Quality Assurance Sapling (LQAS) database is to provide support to
MoPH or NGO managers to enter, maintain and analyze household (community based) survey data.
LQAS database contains detailed information on household survey questionnaire. Flexibilities: The
Household Survey (HHS) LQAS database allows the user to:
1. Define the Supervisory Area (SAs) and enter the sampling frame
2. Define the sample (select random numbers and sampling interval, and define household
numbers in each village of each SA to be interviewed)
3. Enter the collected data for each interview.
4. It simplifies the sampling protocol through an automated process and keeps track of villages
and households included in the sample for data entry of the results.
Information: The Lot Quality Assurance Sapling (LQAS) database contains and can give you
information at least about the following key indicators:
Main Indicators Specific Indicators Definition
Reproductive
Health
Contraceptive Prevalence
Rate
Proportion of currently married, not pregnant women
who are using (or whose partner is using) a modern
contraceptive method
Knowledge of two modern
contraceptive methods
Proportion of currently married, not pregnant women
who can name at least two modern contraceptive
methods
Safe
Motherhood
Births attended by a skilled
attendant
Proportion of mothers having a living child under 1 year
old whose latest delivery was attended by a doctor
,nurse, or trained midwife
Mothers attending one ANC
visit
Proportion of mothers having a living child under 1 year
old who made at least one antenatal care visit to a
doctor, nurse, or trained midwife during the latest
pregnancy
Mothers receiving PNC after
delivery
Proportion of mothers having a living child under 1 year
old whose latest delivery was followed by a visit to
doctor, nurse, or trained midwife
Pregnant woman receiving Proportion of mothers having a living child under 1 year

22
Main Indicators Specific Indicators Definition
TT2+ injections old who received at least two doses of tetanus toxoid
during their latest pregnancy
Child Health Children 1-2 fully immunized
against Diphtheria, Pertussis
and Tetanus (DPT3)
Proportion of children between 1 and 2 years old who
received at least three dose of DPT vaccine as recorded in
the child’s vaccination card
Children 1-2 received Vitamin
A therapy
Proportion of children between 1 and 2 years old who
received vitamin A drops during the previous six months
Children exclusively
breastfed during first 6
months
Proportion of children between 1 and 2 years old who
were exclusively breastfed in the past 24 hours before
the interview
Mothers with appropriate
care seeking behavior
Proportion of children under 2 years old with an episode
of either diarrhea, ARI, or fever during the past two
weeks whose mothers reported appropriate care-seeking
practice

23
Health Related Studies/Special Studies Database
1. Database Description
This searchable database contains various types of health related studies/ conducted in
Afghanistan. A user of this database enters key words to search for documents. The user will
be able to see an abstract of each available study/survey. Full documents of the studies can be
downloaded from the database. Hard copies are available for reference at the MOPH. This
database is accessible to all partners of the MOPH through the Research Department of APHI
and MoPH head site.
2. Purpose of the Database
The main purpose of this database is to provide a system for the collection of health related
studies/surveys at the MOPH and to make these studies available to the Ministry and its
partners. The Ministry and partners will thus be enabled to make evidence-based decisions
about ongoing activities as well as the need for future studies/surveys. Also, this database is a
useful tool for MoPH, NGOs and UN agencies and other health partners to disseminate their
study/survey results to a wider audience and to maximize the use of the information and is
also used as a tracking tool to avoid duplication of information that is already available on
particular area.
3. Areas of Information
To be considered for the Special Studies Database, all studies/surveys must comply with
established Database criteria as outlined below. Types of studies/surveys included in the
database are situation analyses, market surveys, surveillance studies, research, and evaluation
documents.
4. Data Collection
With the support of its various health partners, the MOPH distributes a Special Studies
Database Registration Form (copy attached). All the agencies that have conducted health
related studies/surveys are requested to complete and submit their research registration form
to the Research Department of the MOPH. Collected studies are processed and entered into
the database by the Research Department of MOPH.
5. Expectation for the Partners of MOPH
This database will be used by the Ministry as well as its partners working in the health sector
in Afghanistan. Strong partnership and cooperation of all the agencies are essential for the
system to work. For this reason, the Ministry kindly requests all the partners to complete the
registration form for all retrospective studies and surveys which are not already entered in the
Special Studies Database as well as any new results and submit the form to the Research
Department of Afghan Public Health Institute.

24
Grants Database
The Grants Database was initially developed in 2002 during the AHSEP Project and was subsequently
continued by the REACH project. The data base has continued to be used by the MoPH Grants and
Contract Management Unit (GCMU).
The Grants database is not a financial expenditure database however; it captures some information
about the amount of funds distributed to the grantees. This database provides information on the
number, timing of grants, the grants officer and the location and coverage by district of the
provincial grants.
Standard-Based Management and Recognition (SBMR) 2006 to 2011) The SBMR project was commenced in 17 Provinces in 2006. The main aim of the project was to
improve the performance of health providers and health facilities at the BPHS level using a quality
assurance methodology. This project defined standards for priority areas of basic health care
services. This project concluded in 2011.
The SBMR database is developed in MS-ACCESS, with customized reports in MS Excel. It allows
storing assessments of hospitals based standards.. It also allows creation of customized queries and
reports in ms access and ms excel. Currently, the database contains assessments from 5 USAID
supported provincial hospitals performed since inception in 2006. The database is now centralized.
Fully functional service delivery point (FFSDP)(2003 to 2005):
The FFSDP was a project initiated by USAID in 2003which was implemented in 13 provinces. The project aimed to: 1) improve the performance of the health service delivery system by encouraging behavior change in health providers 2) improve infrastructure, equipment functionality, availability of essential medicine, health facility management and community support. The FFSDP project introduced a set of standards and clinical staff and their supervisors were trained to evaluate their current performance (Ickx, 2006). The tool was used until 2005
Partnership defined quality (2007 to date):
This tool has been implemented in 18 provinces. The objective is to improve access and quality of healthcare through the involvement of the community. The project has been encouraging health workers and the community to look at the root cause of gaps in healthcare quality. It links quality initiatives with community mobilization. The project enables health staff to plan and design quality activities.
Health Care Improvement (HCI) (2008 to date): This tool was piloted six provinces in 2008. . The purpose of the project is to establish and implement quality standards in Primary health care facilities through the application of quality improvement methodologies. A baseline assessment was conducted by external assessors to identify the gaps. The health facilities' staff analyzed their own performance, identified solutions for problems and tested required changes. Additionally, the project aims to build a culture of quality improvement within the MoPH.

25
National Surveys:
Afghanistan Health Survey:
The 2006 Afghanistan Health Survey (AHS) is a population based survey designed to provide information on maternal and child health, child survival, family planning, health care utilization and related expenditures in rural Afghanistan. Other national surveys such as the Multiple Indicator Cluster Survey (MICS 2003) and the National Risk and Vulnerability Assessment (NRVA 2005) have both produced estimates on priority maternal and child health indicators. However, neither the MICS nor the NRVA provide information on what has occurred in Afghanistan’s heath sector following implementation of the Basic Package of Health Services (BPHS). The reference period for many of the indicators in the MICS and NRVA pre-dates implementation of the BPHS. The results from the AHS are instrumental in evaluating the level of progress made in the health sector in Afghanistan since the implementation of the BPHS began in late 2003 and 2004. The AHS is a multistage cluster survey that is representative of most of rural Afghanistan (excluding 6 major cities and provinces and districts that could not be covered due to insecurity). The sampling frame used to select villages for the survey was obtained from the Central Statistics Office (CSO) in July 2006. The sampling frame included over 45,000 enumeration units in rural and urban areas. The AHS included a total of 425 sampled clusters, of which 397 were completed. Twenty eight clusters were not completed due to security reasons. The final sample included 8,278 households. In each sampled household, all ever-married women between 10 and 49 years of age were interviewed, as well as primary caretakers of children 0-59 months of age whose mothers were either dead or no longer living in the household. Data collection started in mid-September and was completed by late December 2006. The AHS 2006 was conducted at the request of the Ministry of Public Health (MOPH). The Monitoring and Evaluation Department implemented the survey with technical assistance in all aspects of the survey from Johns Hopkins University (JHU) and the Indian Institute of Health Management Research (IIHMR). The main objective of this report is to provide estimates of priority health indicators for rural Afghanistan. The priority indicators to be measured include the following: • Proportion of births attended by a doctor/nurse/midwife; • Contraceptive prevalence rate; • Proportion of women receiving ante-natal care during pregnancy; • Proportion of pregnant women receiving tetanus injections; • Proportion of children 12-23 months of age having BCG immunization; • Proportion of children 12-23 months of age having OPV3 immunization; • Proportion of children 12-23 months of age having DPT3 immunization; • Proportion of children 12-23 months of age having measles immunization; • Proportion of children 12-23 months of age fully immunized; • Proportion of children 6-59 months of age receiving vitamin A Supplementation; • Proportion of children 0-5 months who were exclusively breastfed in the last 24 hours; • Proportion of children 6-9 months who received breast milk and appropriate complementary food for the last 24 hours; • Infant Mortality Rate; • Under-five Mortality Rate.

26
The National Risk and Vulnerability Assessment (NRVA) The National Risk and Vulnerability Assessment is a nationally representative multi-purpose survey. The main objectives of the survey are to provide up-to-date information for assessing the situation of the people of Afghanistan and to furnish data needed for monitoring progress toward development goals. The present 2007/8 NRVA is the third of three successive rounds of surveys, following NRVA 2003 and 2005. The NRVA 2003 survey was carried out with co-operation of the World Food Programme (WFP) and supported by the Vulnerability Analysis Unit (VAU) of the Ministry of Rural Rehabilitation and Development. The second NRVA survey was launched in 2005, with CSO and MRRD as the implementing agencies. This NRVA 2005 was a significant improvement in terms of sample design and coverage. As a follow-up to the first two surveys, the third NRVA survey was launched in 2007, jointly by MRRD and CSO, and with co-operation from the European Commission. The NRVA 2007/8 was based on a smaller sample of 20,576 households, but with further improvements in the questionnaire, sample design and coverage. It was designed to provide governments and other agencies with more robust and up-to-date socio-economic data. The aim of this tool is to provide key indicators of socio-economic development in Afghanistan, including 25 MDG indicators. These development indicators and additional information will support the Afghan PRSP (ANDS) and provide unique insights for policy makers, as well as for a broader audience. The gained understanding of poverty and vulnerability in the context of social change in Afghanistan should justify the tremendous survey efforts of the past two years. The subsequent Chapter 2 describes the main methodological characteristics of the NRVA 2007/8 survey, including brief descriptions of the sampling design, survey questionnaires, data collection and processing, data constraints, and comparison with the 2003 and 2005 NRVA surveys. Population structure and change are addressed in the first subject-matter chapter (Chapter 3), as these factors permeate into every development aspect of the remaining report sections. Afghanistan’s population composition by age and sex is analyzed, as well as the underlying dynamics of fertility, child mortality and migration. In addition, household and marriage patterns are examined. Chapter 4 provides an analysis of the structure of Afghanistan’s labor market and covers various labour force indicators, including employment, unemployment, working hours, vulnerable employment, and differentiation by age and sex. Special attention is also paid to working children and labour migration. Agriculture, as the predominant economic activity in Afghanistan, is one of the two subsequent core chapters of this report. Chapter 5 analyses the agricultural sector with a view on access to land, land area size, agricultural production, and type and amount of livestock owned, as well as on the particular constraints this sector is facing. In the key Chapter 6, development and vulnerability are condensed into indicators of poverty and food security. The twin Chapters 7 and 8 are dedicated to the social sectors of education and health, and to the changes occurring in these sectors. The former analyses literacy rates, school enrolment and educational attainment, whereas the latter covers access to health facilities, reproductive and child health, and disability. The housing situation is described in Chapter 9, with a view on house ownership, building characteristics and housing facilities, like electricity, drinking water and sanitation. Chapter 10 has a cross-cutting focus on the position of women and contains two main sections: one on the role of women in decision making (in the household and in the community) and one that largely summarizes the findings from all chapters, specifically from a women’s development perspective.

27
Household shocks and coping strategies, as well as community preferences for interventions are outlined and analysed in chapter 11. Chapter 12 formulates recommendations for development policy, and information needs.
Afghanistan Multi Indicator Cluster Survey:
Afghanistan Multiple Indicator Cluster Survey (AMICS), conducted in by the Central Statistics Organization (CSO). The survey provides valuable information on the situation of children and women in Afghanistan, and was based in large part on the needs to monitor progress towards goals and targets emanating from recent international agreements such as the Millennium Declaration, adopted by all 191 United Nations Member States in September 2000, and the Plan of Action of A World Fit For Children, adopted by 189 Member States at the United Nations Special Session on Children in May 2002. Both of these commitments build upon promises made by the international community at the 1990 World Summit for Children. In signing these international agreements, governments committed themselves to improving conditions for their children and to monitoring progress towards that end. UNICEF was assigned a supporting role in this task. The AMICS provides updated, complementary and comparative data to the NRVA, and is an additional data tool that will further help track progress towards the country’s development objectives, particularly those aimed at women and children. The AMICS was carried out by Afghanistan’s Central Statistics Organization (CSO), with the technical and financial assistance of UNICEF. The AMICS is a nationally representative sample of 13,468 selected households. The survey was designed to produce representative estimates of indicators for Afghanistan as a whole, for urban and rural areas, and for each of the country’s eight regions (Central, Central Highlands, East, North, North East, South, South East and West). A stratified two-stage cluster sample design was used in the AMICS. Questionnaires for the household, for women, and for children were administered in each sampled household. The methodology is described in further detail in Chapter Two. The results of the AMICS are presented in ten chapters: (3) characteristics of household and population, (4) child mortality, (5) nutrition, (6) child health, (7) water and sanitation, (8) reproductive health, (9) child development, (10) literacy and education, (11) child protection and (12) HIV and AIDS. The findings chapters share the data in table format, highlight key aspects of the results, and provide relevant methodological information that helps to further illuminate the data. This final report presents the results of the indicators and topics covered in the survey. As a report sharing the findings of a complex survey covering a multitude of indicators across several major sectors, the AMICS report has as its purpose to present the key findings resulting from the collection of data. It is beyond the scope of the report to analyze the findings or speculate on causes for survey results, though it is hoped that the data presented here will serve other stakeholders in better understanding the causes and consequences of these findings.
Central Statics Organization Population Estimation:
It has been no Population Census conducted in Afghanistan since1358 (1979). Over two decades of war threatened both the lives and livelihood of the people. In late 2001, there was an urgent need to tackle the problem of lack of statistics. Conduct of pre- population census head count was given priority for election in 2004-05. Presently, the population of Afghanistan is estimated (include nomadic and settled) based on pre census and population growth rate. The Annual growth rate of population is estimated to be 2.03%. The total fertility rate is estimated to be 6.3 which is highest in South Asia, (that of 3.3) the share of rural Population was 77%. The percentage of males was 51% and female was 49%. Over two decades war has caused more

28
than 3.3% of women to head the households . The high population growth rate, fertility and dependent population are major constraints for the net rate of economic growth. The total population of Afghanistan estimated 25.5 million in (2009-2010) it shows double increase from last census in (1979) Total Population in that year was 14.6 million. The high fertility rate 6.3% (Number of live birth per woman) is linked to several factors including the traditional preference for large families and children being seen as a source of family income.

29
Some lessons learned from the past experience
• No single measurement tool can address all aspects of health system performance
• No single tool can be relied on 100% • Performance data is only effective if only used systematically at micro and
macro management levels • Minimalism in information collection • Exhausting use of the existing tools before introducing a new tool Tools should be used to monitor trends. Arguing about methodology is counterproductive.

30
Monitoring and Evaluation
Terminology used What is Measured Available Data sources
Pro
gram
eva
luat
ion
i
Mo
nit
ori
ng
and
Eva
luat
ion
1
Fo
rmat
ive
ii Existing knowledge, beliefs, attitude and practices;
target groups and subgroups; barriers to action;
levels of access to services, information, social
support groups and a variety of resources channels
Existing epidemiologic and demographic
reports (CSO, MICS); special studies
using focus groups, in-depth interviews,
direct observation, etc… (Baseline
Household Survey; Mortality Survey,
Baseline BSC, CATCHMENT AREA
ANNUAL CENSUS (CAAC), ….)
Pro
gram
Per
form
ance
mo
nit
ori
ngiii
Pro
cess
eva
luat
ion
iv
Monitoring
inputsv
Inputs Funding, personnel, equipment, supplies,
infrastructure
ANHRA, HSR, FSR, FFSDP, HRD
Monitoring
outputsvi
Functional outputsvii (process
indicators).
Activities completed, units produced: number of
newly trained personnel, of personnel refresher
trained, of community meetings held, of
immunization campaigns
FSR, MIAR, BSC, FFSDP, Training
database
Service outputs relate to quality of
care and access of services
Quality of care, accessibility of services: number
BPHS facilities per 10000 people, number of BPHS
facilities with certified personnel, percentage of
BPHS facilities implementing DOTS, number of
trained CHWs per 1000 people ….
FSR, MIAR, MAAR, MIR, BSC
Sum
mat
ive
eval
uat
ion viii Utilization outputs Utilization of services: number of patients seen,
cases diagnosed, number of specific tests
performed, number of contraceptives
sold/distributed, number of ANC/PNC visits,
MIAR, MAAR, MIR, FFSDP, BSC

31
i“Program Evaluation” and “M&E” are terms commonly used to indicate the whole spectrum of evaluation activities. Sometimes it is said that
monitoring tracks outputs and outcomes and evaluation explains why change occurred, it is however unclear where monitoring ends and where
evaluation begins. ii“Formative evaluation” furnishes information that will guide program design. While often seen as the first step in solid programming, this type
of evaluation can also be used when a program has started to help steer the program or re-design parts of it. iii
“Program performance monitoring” monitors inputs, outputs and behavioral outcomes. It does not include the long-term outcomes that are
often determined by various outside factors like economic growth, women’s social status, ecological changes… iv
“Process evaluation” in its simplest form is also called implementation assessment. It allows evaluating whether the program is implemented as
planned, whether “things are on track”. Many stakeholders, in particular donor agencies, directors and evaluators often underutilize process
evaluation: there is more concern with what the project achieves (“did I make a difference”) than with what program activities are carried out.
number of deliveries by trained attendants
Monitoring
outcomesix
Initial Knowledge, attitude, beliefs FFSDP, BSC, Follow-on household
surveys
Intermediate Behavior and practice FFSDP, BSC, Follow-on Household
Surveys, CATCHMENT AREA ANNUAL
CENSUS (CAAC)
Long-term Health status: mortality, fertility, morbidity Mortality, fertility, morbidity studies
(MICS, DHS, AMS, NRVA, RAMOS,
Census)
Impactx
assessment
Causality/Probability/Plausibility Impact: did this intervention cause the observed
results? More and more abandoned for initial,
intermediate and long-term outcomes.
Statistically rigorously designed studies –
not applicable

32
However, once summative evaluation tells us that the program falls short of its objectives, only thorough process evaluation can help us
understand whether this was due to implementation failure (activities did not take place as planned) or program theory failure (activities took
place as planned, but the design was conceptually flawed). v“Inputs” encompass the human and financial resources, physical facilities, equipment, supplies, and operational policies that enable the
activities to be implemented. vi
“Output” measures results of the activities at the program level: number of activities performed (functional outputs), quality of care and access
of services (service outputs), level of service utilization (service utilization outputs). vii
For monitoring, there is no mention of “process indicators”. Instead, there are “functional outputs”, which quantify the activities that take
place and “service outputs” which measure quality of care and access to services viii
“Summative evaluation” measures the extent to which change occurs, consistent with the objectives of the program. I answers the question
“did it make a difference?” at different levels. Short term change often limits itself to change in knowledge and attitudes of the target groups,
intermediate change is reflected in change in practices and behavior related to the program objectives, long-term change can only be observed
after 5-10 years and concerns morbidity, mortality, fertility, … ix
“Outcomes” relate to measurement of indicators of the status of social and health conditions the activities are supposed to change. Outcomes
are often related to behavior that changes due to the program activities. This can be limited to program level (e.g. the number of FB+ patients
that are cured in a TB program), but is often larger and applied to the whole population (e.g. percent of all mothers that exclusively breastfeed
for six months). Many health programs use IEC as well as clinical activities, therefore we can discern three levels of outcomes:
i. Initial – knowledge, attitudes, beliefs, perceived risk
ii. Intermediate – behaviors (contraceptive use, breastfeeding, use of bed nets, appropriate care seeking for sick children)
iii. Long-term – mortality, morbidity, fertility
This classification prefers long-term outcomes over “impact”, since “outcomes” do not assume that the programmatic intervention causes the
change in behavior, it just assumes that it contributed (among other factors) to the change. x “Impact” carries different meanings for different people. Sometimes the simple perception that a program was well-liked, reached a large
audience, received positive comments from the press or celebrities is taken for “really having impact”. More commonly the following uses are
often seen:
1. “impact” referring to the long-term outcome of the ultimate program objective (i.e. morbidity, mortality and fertility)
2. “Impact” referring to the immediate short-term or intermediate effects of a health promotion program. One looks at variables available
within the timeframe of the evaluation, which provide some evidence of progress.
3. “Impact” referring to the cause-and-effect, assessed through studies with a methodologically sound study design and analytic technique.
From strongest to weakest these are:

33
i. Randomized controlled trials, the classic experimental model which establishes cause, is rarely applicable to large-scale health
programs
ii. Plausibility – observed change is associated with the program intervention
1. Quasi-experimental design: high external validity and feasible, but resource hungry and “what would have happened if no
program” -> propensity score analysis. Pretest-posttest separate sample design, pretest-posttest non-equivalent control
group design, time series
2. Post-test only cross-sectional design with dose-response analysis and regression analysis of level of exposure, or with
establishing propensity scores. However certain influencing factors are not readily measurable (e.g. motivation), and
reverse causation cannot be ruled out, even with endogeniety tests
iii. Adequate evidence: change occurred after the intervention. Often used when limited resources for evaluation: track the trends in
available statistics.