Embed Size (px)
Citation preview

Health in LondonAuthor(s): Sarah CurtisSource: Area, Vol. 33, No. 1 (Mar., 2001), pp. 84-92Published by: Wiley on behalf of The Royal Geographical Society (with the Institute of BritishGeographers)Stable URL: http://www.jstor.org/stable/20004129 .
Accessed: 15/06/2014 07:44
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
Wiley and The Royal Geographical Society (with the Institute of British Geographers) are collaborating withJSTOR to digitize, preserve and extend access to Area.
http://www.jstor.org
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions

84 Observations
and middle income affordability is a key element of housing sustainability for London (Campaign for Homes in Central London 1986).
References
Butler T 1 997 Gentrification and the middle classes Ashgate, Aldershot
Butler T and Hamnett C 1994 Gentrification, class and gender: some comments on Warde's 'Gentrification as consumption' Environment and Planning D 12 477-93
Campaign for Homes in Central London 1986 City life: a
future for central London ChiCL, London Dunn R, Forrest R and Murie A 1987 The geography of
council house sales in England, 1979-85 Urban Studies 24 47-59
Forrest R and Murie A 1988 Selling the Welfare State: the
privatisation of public housing Routledge, London Frost M and Spence N 1993 Global city characteristics and
central London's employment Urban Studies 30(3) 547-58
Graham D and Spence N 1995 Contemporary deindustri
alisation and tertiarisation in the London economy Urban
Studies 32(6) 885-91 1 Hamnett C 1987 A tale of two cities: socio-tenurial polar
isation in London and the South East, 1966-1981 Environment and Planning A 19 53 7-56
- 1 989 The social and spatial segmentation of the London
owner occupied housing market: an analysis of the flat
conversion sector in Breheny M and Congdon T eds Growth and change in a core region Pion, London
200-18 - 1996 Social polarisation, economic restructuring
and welfare state regimes Urban Studies 3 3(8) 1407-30
- 1999 Winners and losers: home ownership in modern
Britain UCL Press, London Hamnett C and Cross D 1998a Social polarisation and
inequality in London: the earnings evidence, 1979-95 Environment and Planning C 16 659-80
1 998b Social change, social polarisation and income inequality in London, 1979-93 Geojournal 46 39-50
HM Land Registry 2000 http://www.landreg.gov.uk/ppr/ interactiv
Malpass P and Murie A 1987 Housing policy and practice
2nd edition Macmillan, London McDowell L 1997 The new service class: housing, con
sumption and lifestyle among London bankers in the 1 990s Environment and Planning A 29 2061-78
Tindall G 1973 A street in London New Society
14 January Young K and Kramer J 1978 Strategy and conflict in
metropolitan housing Heinneman, London
Health in London
Sarah Curtis Department of Geography, Queen Mary and Westfield College, University of London, Mile End Road,
London El 4NS
Email: [email protected]
This manuscript was received 6 November 2000
This paper summarizes some geographical perspec tives on health inequality in London. The discussion focuses especially on the argument that London's role as a global city is significant for health differences in London's population.
Globalization
Theories of globalization are used in human geogra phy to understand how economic, social and politi cal events in one part of the world increasingly have
significance in very distant areas (e.g. Waters 1995). This arises from processes which include:
* time space compression; * increased global communication; * global circuits of capital; and * increased impact of cultural influences from
around the world.
In global cities, such as London, these trends are particularly apparent, although not all aspects of
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions

Observations 85
London are related to globalization. Key features of London's population, form and function that are associated with its global city role include:
* centres of financial/commercial control of the capitalist economy;
* international transport and communications; * significant numbers in the population who
are cosmopolitan, internationally mobile and ethnically diverse;
* comparatively high average incomes supporting many in wealthy lifestyles; and
* international centres for culture, arts and sciences, education and learning.
These are largely positive things for London as a whole, contributing to the city's wealth and prestige and making it a vibrant, fascinating place to live. However, commentators, and particularly geo graphers, also point to the spatial unevenness of globalization tendencies. Not all areas and people are affected by globalization to the same extent, or in the same ways. Within London we observe striking economic and social diversity.
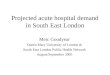
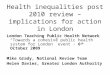
Figure 1 shows the geographical variation in an index of local conditions for 1998 disseminated by DETR. It combines information on factors such as unemployment, low income and housing conditions. The map shows inequality in living conditions across London, with outer London and the 'west end' relatively advantaged while areas of inner London, especially the 'east end' are on average more dis advantaged. Of course, this scale analysis masks the even greater variability that exists at the finer scale of enumeration districts. For example, within East London and City Health Authority in East London (which extends across Hackney, Tower Hamlets,
Newham and the City) data for enumeration districts show local concentrations of relatively wealthy populations close to concentrations of poverty (Figure 2).
Some geographers (e.g. Sassen 1991) have argued that this 'polarization' and diversity in economic terms is very typical of global cities. In simple terms, it reflects differences in economic status and oppor tunities between, on the one hand, an 'elite' group
who have core roles in London's global activities professional workers with relatively secure opportu nities for well-paid employment in multi-national organizations-and on the other hand those whose work is less valued in relation to London's global functions, working in low grade manual and service
jobs, which may be low paid, arduous, unsatisfying, short term and insecure.
Income and employment inequality in London goes together with other aspects of difference. There is a 'consumption cleavage' (Cater and Jones 1989)
or 'housing divide' between those in good quality owner-occupied or rented housing and those in poor quality housing either in run down council estates or in poorer parts of the privately rented or owner-occupied sectors. One factor in this housing divide is the demand among the 'elite' groups of workers for homes of a high standard within short commuting time of central London. This contributes to rising prices for good quality family homes in accessible London suburbs or in central locations, many of which have been gentrified by conversion of run down housing and industrial buildings to relatively expensive private sector homes. Housing in London becomes more expensive for everyone and poor people are obliged to move out of gentrifying areas where they can no longer afford to live. Several geographers have investigated the complex associ ations between changes in the housing market, changes in the labour force and trends in social and spatial polarization (Atkinson 2000; Lyons 1999;
McDowell 1997; Hamnett 1996; Forrest and Murie 1995).
Residential areas of London vary in terms of the quality of the services offered and the amount of pressure of demand for these services. This is acknowledged in a consultation paper recently pro duced by the government's social exclusion unit (Social Exclusion Unit 2000) which analyses the problems of deprived areas and refers to the impor tance of access to basic, 'mainstream', services such as healthcare. Furthermore, poorer populations are
more likely to live close to environmental nuisances or potential hazards such as major roads, airports and waste disposal sites (e.g. Dolk et al. 1 995).
The international mobility and cosmopolitan nature of the population also generates inequalities. London as a global city draws in many 'elite' workers from abroad, but it also attracts poorer migrants, some of whom have left their countries of origin as refugees. London's population therefore includes large ethnic minority populations, many of whom are
British-born descendants of older migrants. While some of these people are represented among 'elite' socio-economic groups in London, ethnic minority groups in general are disproportionately represented among the poorer paid and low grade jobs in the city.
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions
86 Observations
Uf) Rt W
CMN ? qT W
C%J ri a co LOr
mu,
coLOrrN
ci US~~~~~~~~~~~~~~~~~~
cc
0
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions

Observations 87
* III~~~~~~~~~~~~*
Eu
C
x O.~~~~~~~~~~ c
Eu
Eu
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions

88 Observations
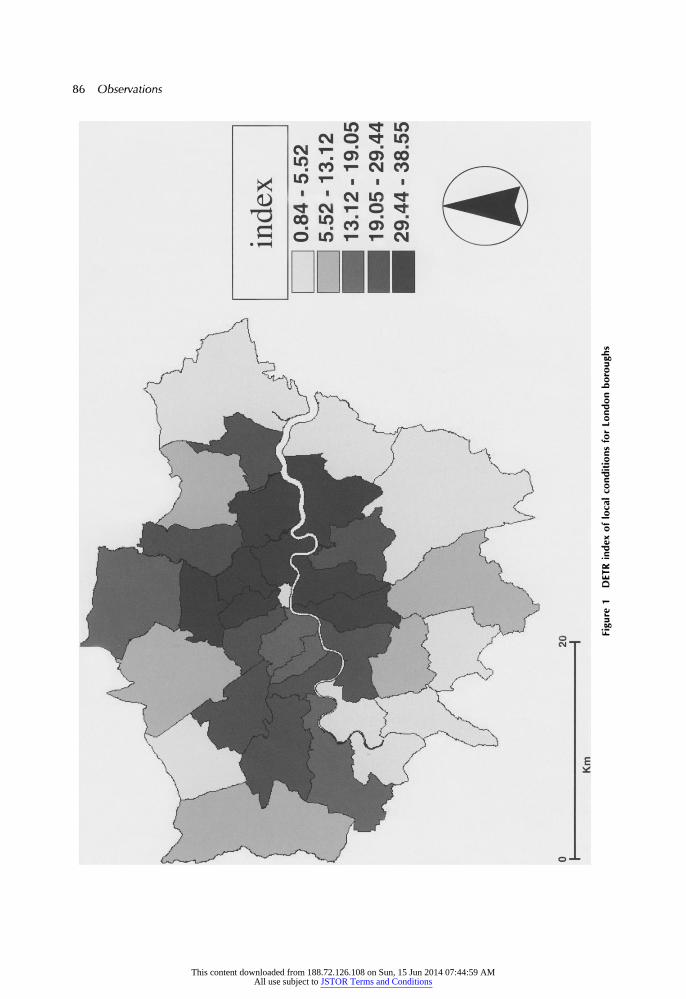
Structural Economic, Social and Political Factors
(including globalization of economies and societies)
Inequalities in the determinants of health
(including employment, housing, social position, welfare services, environmental hazards)
Inequalities in health
(including medical and lay people's views of physical and mental health)
Figure 3 The association between structural processes, determinants of health and health inequalities
So we have a population in London which is highly mobile, ethnically diverse and experiencing highly variable conditions of wealth and living and working conditions. These inequalities are also evident in other British cities, but London's global city role
contributes to these inequalities, heightening their
effect. In terms of social and economic sustainability, the situation raises some real questions about the negative as well as the positive aspects of this global city position.
Health difference
The potential implications for health difference in the
population are clear. Aspects of living conditions such as employment, housing, access to services and environment can be considered as determinants of
health. Inequalities in these determinants of health are key to understanding the inequalities in health which we observe within London (Figure 3).
A good deal of research in Geography and other disciplines has established the strength of these links
(Congdon et al. 1997; Shaw et al. 1999). Age and sex standardized indicators of self reported illness (Figure 4) and mortality (Figure 5) show geographical
patterns in London which closely match those of
the socio-economic indicators in Figure 1. Figure 6
illustrates that correlation at the finer scale of
wards. These measures indicate a 'health divide' between
the more affluent and more deprived areas in
London. Such associations do not of themselves prove that deprivation causes ill-health and early death, but detailed and careful analysis by geogra phers, social epidemiologists and other researchers has shown that these associations do arise to a large
extent because socio-economic inequality has material and psycho-social effects on health. The evidence is reviewed for example in the Independent Inquiry into Inequalities in Health Chaired by Sir
Donald Acheson (Department of Health 1998) and the Government's White Paper on public health (Department of Health 1999) acknowledges this evidence. (For reviews from a geographical perspec tive, see, for example, Curtis and Jones 1 998; Popay et al. 1998).
The Acheson report also highlighted the signifi cance for health difference of ethnic diversity in
Britain. Significant health differences can be observed between ethnic minority groups, some of which may be associated with cultural factors, though much of the variation can be explained in terms of the relative socio-economic disadvantage of
minority populations in Britain and by inequalities in health care (Nazroo 1997). Many of our key ser vices, like the National Health Service, social services and transport services depend heavily on workers from ethnic minority groups as employees. Ethnic
minority groups also make up a significant pro portion of patients using the NHS in areas like London. The NHS is required to provide services which are sensitive to the needs of our ethnically diverse population and competent to deal with these needs.
Health and regeneration
Significant efforts are made to reduce inequalities in the determinants of health in London. In East London alone there is currently a total investment of over ?380 million. Our analysis of these schemes showed that actions to improve education, training and
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions

Observations 89
C) m
0)0. CO CI I 0) rr
L 04
cm
w _ ?o~~~~~~~~~~~~~~ __ o~~~~~~~~~~~~~~ _ o~~~~~~~~~~~~~~~
0
r N |~~~~~~~~~~~~~~~ 7 ~ ~ ~~~ < L | E~~~~~~~~~~~~
_~~~~~~~~~~~~~~~~~~~~
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions

90 Observations
Or
CM0)rr
Ul~~~~~~~~~~~~~o 0)0)..~~~~~~~~~~~~
c
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~r_
C .0 E C
/ w___~~~~~~~~~~~~~~~~~~~
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions

Observations 91
250.00
200.00
s 150.00
c" 1 00.00
50.00
.00
.00 5.00 10.00 15.00 20.00
ILD
Figure 6 Correlation of indicators of local deprivation (ILD) and standardized Illness ratios (SIR) for wards in London
chances of employment, housing, and social ca pacity in communities were most commonly cited objectives. Increasingly those planning these projects are being encouraged to think about the health impacts of these initiatives. Health Impact Assess
ment (HIA) involves appraising what the likely health outcomes will be and whether they will reduce health inequalities (BMA 1998; Ison 2000). Geogra phers are among those involved in developing strategies for HIA (Cave et al. 2000).
Can such regeneration schemes help to reverse the chains of causation by which deprivation leads to poor health? Though some health improvements, might be expected in the long term, there are several reasons why health gains may be difficult to identify in the short term (Curtis et al. 2000). Limitations
of regeneration schemes in this respect are that they:
* address the symptoms of inequality, not the struc tural factors causing inequality;
* focus on certain aspects of deprivation, but health is affected by a wider range of factors;
* focus on certain areas and sometimes exclude the most disadvantaged groups; and
* may not raise people far enough out of poverty and insecurity to make a difference to health (some research suggests that deprivation quickly
damages health but reversing the damage is slow and difficult-e.g. Benzeval et al. 2000).
Conclusions
While strong inequalities in poverty and wealth persist in London, health for all Londoner's is not going to be achievable or sustainable. Work on health impact assessment suggests that we should not be complacent in thinking that current efforts at regeneration and urban renewal will be sufficient to reduce the health inequalities we observe in London. Effective measures to stop people falling into poverty in the first place would probably be more effective in the long run, and it is also important to provide good health services which are accessible to deprived populations in London, whose health is most likely to be undermined by the global city processes operating in London.
References
Atkinson R 2000 Professionalization and displacement in Greater London Area 32(3) 287-95
Benzeval M, Dilnot A, Judge K and Taylor J 2000 Income
and health over the life course: evidence and policy implications in Graham H Understanding health inequalities Milton Keynes, Open University Press
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions

92 Observations
British Medical Association 1998 Health and environ mental impact assessment: an integrated approach Earthscan, London
Cater I and Jones T 1989 Social geography: an introduction to contemporary issues Arnold, London
Cave B, Curtis S, Aviles M and Coutts A 2000 Health
impact assessment: a toolkit for regeneration schemes in east London Queen Mary, University of London, Health Research Group in Geography, London.
Congdon P, Shouls S and Curtis S 1997 A multi-level
perspective on small area health and mortality: a case
study of England and Wales International Journal of
Population Geography 3 243-63 Curtis S and Jones 11998 Is there a place for Geography in
the analysis of health inequality? Sociology of Health and Illness 20(5) Special Issue 645-72
Curtis S Aviles M and Cave B 2000 Urban regeneration,
health and geography Paper presented to 9th Inter national Symposium in Geography of Health Montreal 3-7 July Available from Health Research Group, Geogra
phy Department, Queen Mary, University of London, London El 4NS
Department of Health 1998 Independent inquiry into inequalities in health: report (Chair Sir Donald Acheson)
HMSO, London 1999 Saving lives: our healthier nation White Paper on
Public Health cm 4386 HMSO, London Dolk H, Mertens B, Kleinschmidt I, Walls P, Shaddick G
and Elliott P 1995 A standardization approach to the
control of socio-economic confounding in small area studies of environment and health Journal of Epidemi ology and Community Health 49 supplement 2 s9-sl 4
Forrest R and Murie A 1995 From privatization to commodification-tenure conversion and new zones of transition in the city International Journal of Urban and
Regional Research 19(3) 407 Hamnett C 1996 Social polarisation, economic restructur
ing and welfare state regimes Urban Studies 33(8) 1407-30
Ison E 2000 London's health: developing a vision together. Resource for health impact assessment 2000 London NHSE, London
Lyons M 1999 Professionalisation, feminisation, and sociospatial polarisation in London,1971-1991 Environ
ment and Planning A 31(3) 493-506
McDowell L M 1997 The new service class: housing,
consumption, and lifestyle among London bankers in the 1990s. Environment and Planning A 29(11) 2061-78
Nazroo J 1997 The health of Britain's ethnic minorities: findings from a national survey Policy Studies Institute, London
Popay J, Williams Thomas C and Gatrell A 1998 Theorising inequalities in health the place of lay knowledge in
Bartley M, Blane D and Davey-Smith G eds The sociol
ogy of health inequalities Blackwell, Oxford 59-84 Sassen S 1991 The global city Princetown University Press,
New York Shaw M, Dorling D, Gordon D and Davey-Smith G 1999
The widening gap: health inequalities and policy in Britain Policy Press, Bristol
Social Exclusion Unit 2000 National strategy for neighbour hood renewal: a framework for consultation Central Office of Information, London
Waters, M 1995 Globalization Routledge, London
London's transport-investing for sustainability
Martin Frost School of Geography, Birkbeck College, 7-1 5 Gresse Street, London WI P 2LL
Email: [email protected]
This manuscript was received 18 October 2000
Powerful forces are combining to make the next few
years a critical time in the evolution of London's transport system. There is now a national, integrated transport policy which sets the seal on several years of policy evolution, spelling out the advantages (both environmental and social) of shifting emphasis away from car travel and towards a better quality public transport system (DETR 1998). There are ten year spending plans which promise about f l8bn
of investment in London's transport system, accompanied by a further ?7bn of operating support by 2010 (DETR 2000). There is a new Mayor whose main area of power and responsibility is in running the city's transport system, coordinating the trans port plans of the individual boroughs and even breaking new ground with proposals for congestion charging (GLA 2000). There is a vibrant economy, at least in central London, and a thriving tourist industry
This content downloaded from 188.72.126.108 on Sun, 15 Jun 2014 07:44:59 AMAll use subject to JSTOR Terms and Conditions