Embed Size (px)
Citation preview
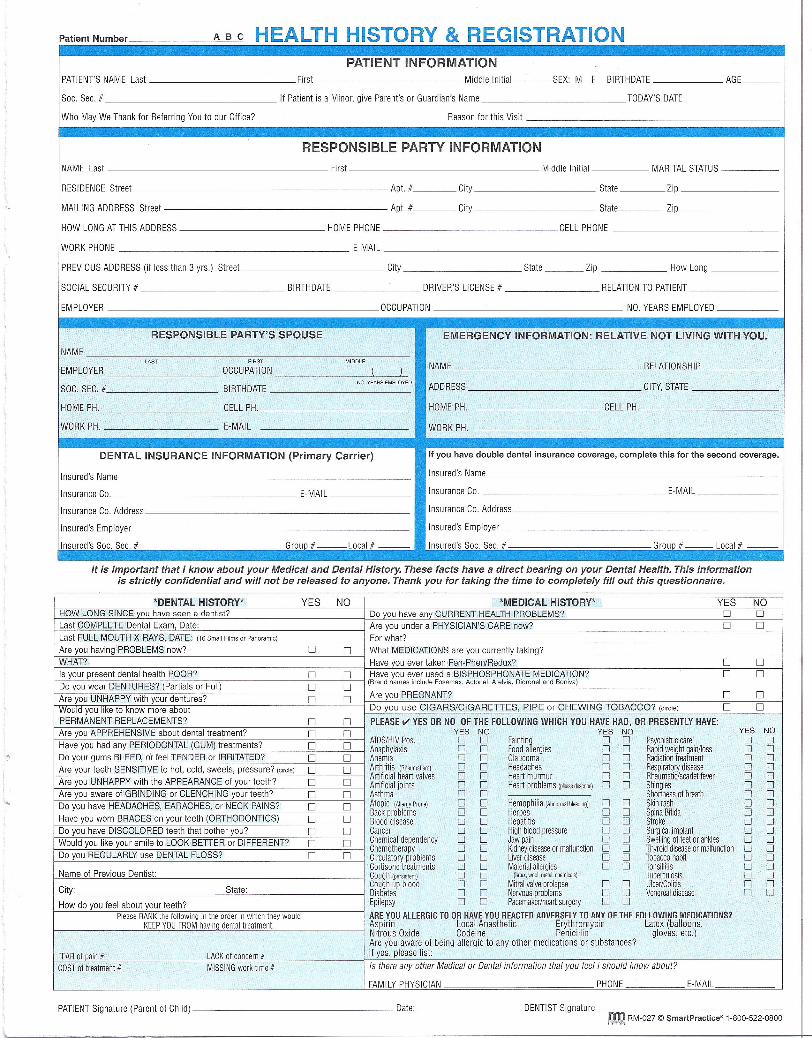
Patient Number ABC HEALTH HISTORY & REGISTRATIONPATIENT INFORMATION
PATIENT'S NAME Last First Middle Initial ___ SEX: M F BIRTHDATE AGE___
Soc. Sec. # If Patient is a Minor, give Parent's or Guardian's Name TODAY'S DATE
Who May We Thank for Referring You to our Office? Reason for this Visit
RESPONSIBLE PARTY INFORMATIONNAME Last First Middle Initial MARITAL STATUS
RESIDENCE Street Apt. # City State Zip
MAILING ADDRESS Street Apt. # City State Zip
HOW LONG AT THIS ADDRESS HOME PHONE CELL PHONE
WORK PHONE E-MAIL
PREVIOUS ADDRESS (if less than 3 yrs.) Street City State ___ Zip How Long
SOCIAL SECURITY # BIRTHDATE DRIVER'S LICENSE # RELATION TO PATIENT
EMPLOYER OCCUPATION NO. YEARS EMPLOYED
". • - ~~~~~~,,'lII'!!;~~~~L,,~RESPONSIBLE PARTY'S SPOUSE EMERGENCY INFORMATION: RELATIVE NOT LIVING WITH YOU.
NAMELAST FIRST MIDDLE NAME RELATIONSHIPEMPLOYER OCCUPATION ( )
NO. YEARS EMPLOYED ADDRESS CITY, STATESOC. SEC. # BIRTHDATE
HOME PH. CELL PH. HOME PH. CELL PH.
WORK PH. E-MAIL WORK PH.
DENTAL INSURANCE INFORMATION (Primary Carrier) If you have double dental insurance coverage, complete this for the second coverage.
Insured's Name Insured's Name
Insurance Co. E-MAIL Insurance Co. E-MAIL
Insurance Co. Address Insurance Co. Address
Insured's Employer Insured's Employer
Insured's Soc. Sec. # Group # Local # Insured's Soc. Sec. # Group # Local #J.
It is important that I know about your Medical and Dental History. These facts have a direct bearing on your Dental Health. This informationis strictly confidential and will not be released to anyone. Thank you for taking the time to completely fill out this questionnaire.
*DENTAL HISTORY* YES NO *MEDICAL HISTORY* YES NOHOW LONG SINCE vou have seen a dentist? Do you have any CURRENT HEALTH PROBLEMS? 0 0Last COMPLETE Dental Exam, Date: Are you under a PHYSICIAN'S CARE now? 0 0Last FULL MOUTH X-RAYS, DATE: (16 Small Films or Panoramic) For what?Are you having PROBLEMS now? 0 0 What MEDICATIONS are vou currentlv takino?WHAT? Have you ever taken Fen·Phen/Redux? 0 0Is your present dental health POOR? 0 0 Have you ever used a BISPHOSPHONATE MEDICATION? 0 0Do you wear DENTURES? (Partials or Full) 0 0
(Brand names include Fosamax, Actonel, Atelvia, Didronel and Boniva)
Are you UNHAPPY with your dentures? 0 0 Are you PREGNANT? 0 0Would you like to know more about Do you use CIGARS/CIGARETTES, PIPE or CHEWING TOBACCO? (circle) 0 0PERMANENT REPLACEMENTS? 0 0 PLEASE V YES OR NO OF THE FOLLOWING WHICH YOU HAVE HAD, OR PRESENTlY HAVE:Are you APPREHENSIVE about dental treatment? 0 0 YES NO YES NO YES NOHave you had any PERIODONTAL (GUM) treatments? 0 0 AIDS/HIVPos. 0 0 Fainting 0 0 Psychiatriccare 0 0
Anaphylaxis 0 0 Foodallergies 0 0 Rapidweightgain/loss 0 0Do your gums BLEED, or feel TENDER or IRRITATED? 0 0 Anemia 0 0 Glaucoma 0 0 Radiationtreatment 0 0Are your teeth SENSITIVE to hot, cold, sweets, pressure? (circle) 0 0 Arthritis (Rheumatism) 0 0 Headaches 0 0 Respiratorydisease 0 0Are you UNHAPPY with the APPEARANCE of your teeth? 0 0
Artificial heartvalves 0 0 Heartmurmur 0 0 Rheumatic/scarletfever 0 0Artificial joints 0 0 Heartproblems(p.,sedescnbe) 0 0 Shingles 0 0
Are you aware of GRINDING or CLENCHING your teeth? 0 0 Asthma 0 0 Shortnessof breath 0 0Do you have HEADACHES, EARACHES, or NECK PAINS? 0 0 Atopic (Allergy Prone) 0 0 Hemophilia(Abnormal bleeding) 0 0 Skinrash 0 0Have you worn BRACES on your teeth (ORTHODONTICS) Backproblems 0 0 Herpes 0 0 SpinaBifida 0 0
0 0 Blooddisease 0 0 Hepatitis 0 0 Stroke 0 0Do you have DISCOLORED teeth that bother you? 0 0 Cancer 0 0 Highbloodpressure 0 0 Surgicalimplant 0 0Would you like your smile to LOOK BEDER or DIFFERENT? 0 0 Chemicaldependency 0 0 Jawpain 0 0 Swellingof feetor ankles 0 0Do you REGULARLY use DENTAL FLOSS?
Chemotherapy 0 0 Kidneydiseaseor malfunction 0 0 Thyroiddiseaseor mafundion 0 00 0 Circulatoryproblems 0 0 Liverdisease 0 0 Tobaccohabit 0 0
Cortisonetreatments 0 0 Materialallergies 0 0 Tonsillitis 0 0Name of Previous Dentist: Cough(persistent) 0 0 (Ialex,wool,metal,chemicals) Tuberculosis 0 0City: State: Coughup blood 0 0 Mitralvalveprolapse 0 0 Ulcer/Colitis 0 0
Diabetes 0 0 Nervousproblems 0 0 Venerealdisease 0 0How do you feel about your teeth? Epilepsy 0 0 Pacemakeriheartsurgery 0 0
PleaseRANKthefollowing in the order in whichtheywould AREYOUALLERGICTO OR HAVEYOUREACTEDADVERSELYTO ANY OFTHEFOLLOWINGMEDICATIONS?KEEPYOUFROMhavinqdentaltreatment. Aspirin Local Anesthetic Erythromycin Latex (balloons,
Nitrous Oxide Codeine Penicillin gloves, etc.)Are you aware of being allergic to any other medications or substances?
FEARof pain# LACKof concern# If yes, please listCOSTof treatment# MISSINGwork time# Is there any other Medica/ or Dental information that you feel I should know about?
FAMILY PHYSICIAN PHONE E-MAIL
PATIENT Signature (Parent of Child) Date: -------- DENTIST Signature ------c=c--------------tal RM-027 © SmarlPractice" 1-800-522-0800
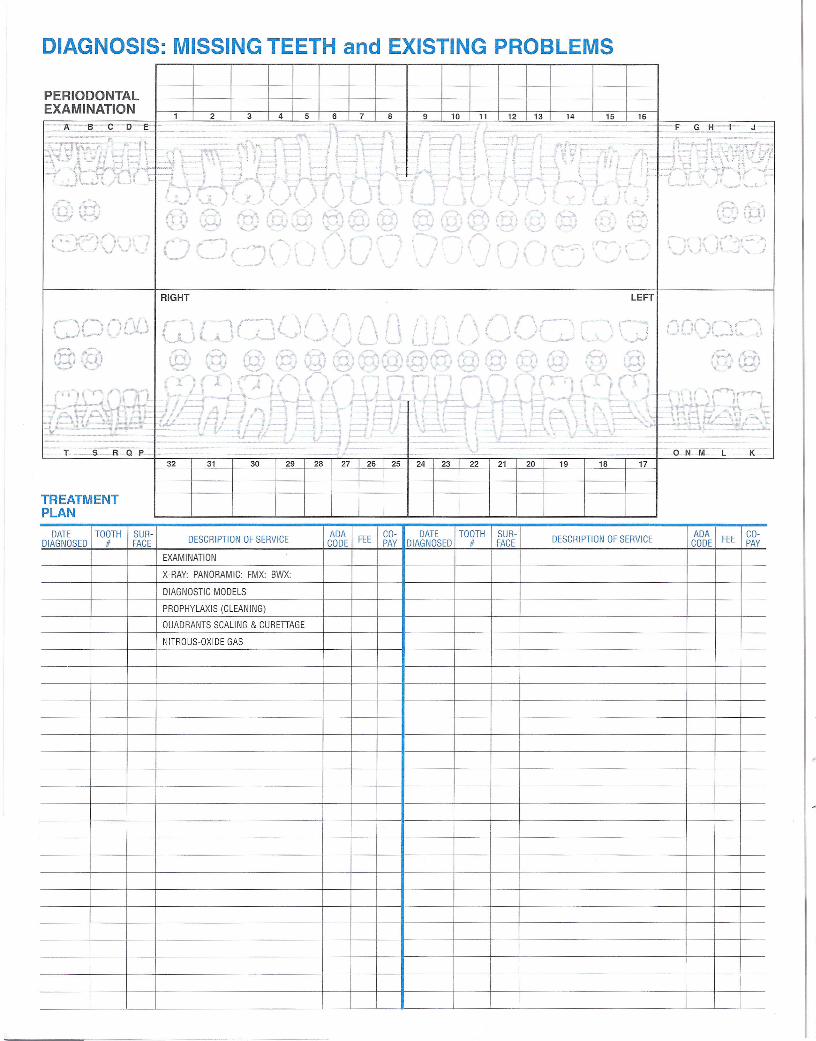
DIAGNOSIS: MISSING TEETH and EXISTING PROBLEMS
PERIODONTALEXAMINATION
162 43 6 7 8
.£LlL109 11 12 13 14 15
1- __J__
, ~_ "' .•..•. , /", . ~\ _-*.. I .' _t.. (
,- ~ /~. I t
'__ ' L..!',·...J
-
..•1 t -.-i t-
, 1
/, r.... ,. {'rY" ,, I ,
"--- -. r~'--' ( .
---'
RIGHT
- , .• : ,iII Ifi--l...<>' ,
,• \ I \
I I"---'- ,•. ~
,__ ~F
1 --I ( •1t, -.. ; L1 ••.'
I'
I ~\ ,
I I ,'-'-
, . {;.;. - .•,-
IJ
LEFT
,/ ;
i
,,, \ ,--- ...,, . I,-",,-'1-
I;
" ~\~:Y~ I<n. -I t I I
\ A.,.-'1 r =-.t:t ~ -1 t--- ,
T -S-R-Q P- - ---
TREATMENTPLAN
---
t f,
I,r
.\H •.••"." . 4'
I ("'f\V"-AI--'
32 31 29 28 26 25 24
----
23 22 21 20 19 18 17
DATE TOOTH SUR-DIAGNOSED If FACE
ADA CO-CODE FEE PAY
30 27
DESCRIPTION OF SERVICE I ADA CO- DATE TOOTH SUR-CODE FEE PAY DIAGNOSED If FACE
EXAMINATION
X-RAY: PANORAMIC: FMX: BWX:
DIAGNOSTIC MODELS
PROPHYLAXIS (CLEANING)
QUADRANTS SCALING & CURETIAGE
NITROUS-OXIDE GAS
DESCRIPTION OF SERVICE
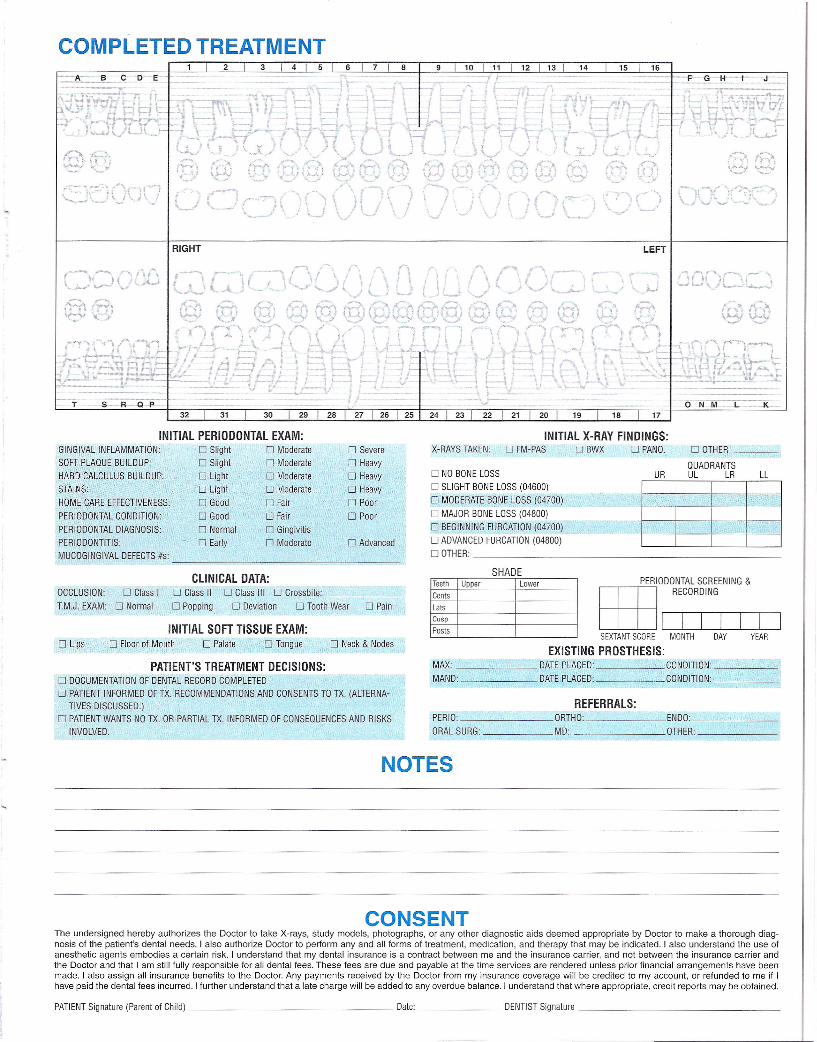
COMPLETED TREATMENT8 13 I 142 7
J3 4 5 6
_-A-- BCD -e- _=--==
- ,"/'
--. ~t' ,t
'f! I J"-'
11 12 1510 16
...- 1£--.( :~.,:'7::"":" ~\ ; .•......_-. -~..•
\ ,
RIGHT LEFT
(--"\ '-"1'.. )...; ,,-,- ~
--T- -S:-R~32
INITIAL PERIODONTAL EXAM:GINGIVAL INFLAMMATION: 0 SlightSOFT PLAQUE BUILDUP: 0 Slight
HARD CALCULUS BUILDUP: 0 LightSTAINS: 0 Light
HOME CARE EFFECTIVENESS: 0 Good
PERIODONTAL CONDITION: 0 GoodPERIODONTAL DIAGNOSIS: 0 NormalPERIODONTITIS: 0 EarlyMUCOGINGIVAL DEFECTS Is: ------------------------~----------
o Moderateo Moderateo Moderate
o Moderateo Fair
o Fairo Gingivitis
o Moderate
o Severeo Heavyo Heavyo Heavy
o Poor
o Poor
o Advanced
OCCLUSION: 0 Class I
IM.J. EXAM: 0 Normal
CLINICAL DATA:o Class II 0 Class III 0 Crossbite:
o Popping 0 Deviation 0 Tooth Wear o Pain
INITIAL SOFT TISSUE EXAM:o Lips o Floor of Mouth o Palate o Tongue o Neck & Nodes
PATIENT'S TREATMENT DECISIONS:o DOCUMENTATION OF DENTAL RECORD COMPLETEDo PATIENT INFORMED OF TX. RECOMMENDATIONS AND CONSENTS TO TX. (ALTERNA-
TIVES DISCUSSED.)o PATIENT WANTS NO TX. OR PARTIAL TX. INFORMED OF CONSEQUENCES AND RISKS
INVOLVED.
\ l, J
17
X-RAYS TAKEN:INITIAL X-RAY FINDINGS:
o FM-PAS 0 BWX 0 PANO. o OTHER
QUADRANTSUR UL LR LL
~
o NO BONE LOSSo SLIGHT BONE LOSS (04600)
o MODERATE BONE LOSS (04700)
o MAJOR BONE LOSS (04800)o BEGINNING FURCATION (04700)
o ADVANCED FURCATION (04800)o OTHER: _
SHADETeeth Upper LowerCentsLatscuspPosts
PERIODONTAL SCREENING &
EEJ~SEXTANT SCORE MONTH DAY YEAR
EXISTING PROSTHESIS:MAX: DATE PLACED: CONDITION: 1
MAND: DATE PLACED: CONDITION: ,
REFERRALS:PERIO: ORTHO: ENDO: ,
ORAL SURG: MD: OTHER: _
NOTES
CONSENTThe undersigned hereby authorizes the Doctor to take X-rays, study models, photographs, or any other diagnostic aids deemed appropriate by Doctor to make a thorough diag-nosis of the patient's dental needs. I also authorize Doctor to perform any and all forms of treatment, medication, and therapy that may be indicated. I also understand the use ofanesthetic agents embodies a certain risk. I understand that my dental insurance is a contract between me and the insurance carrier, and not between the insurance carrier andthe Doctor and that I am still fully responsible for all dental fees. These fees are due and payable at the time services are rendered unless prior financial arrangements have beenmade. I also assign all insurance benefits to the Doctor. Any payments received by the Doctor from my insurance coverage will be credited to my account, or refunded to me if Ihave paid the dental fees incurred. I further understand that a late charge will be added to any overdue balance. I understand that where appropriate, credit reports may be obtained.
PATIENT Signature (Parent of Child) Date: DENTIST Signature _
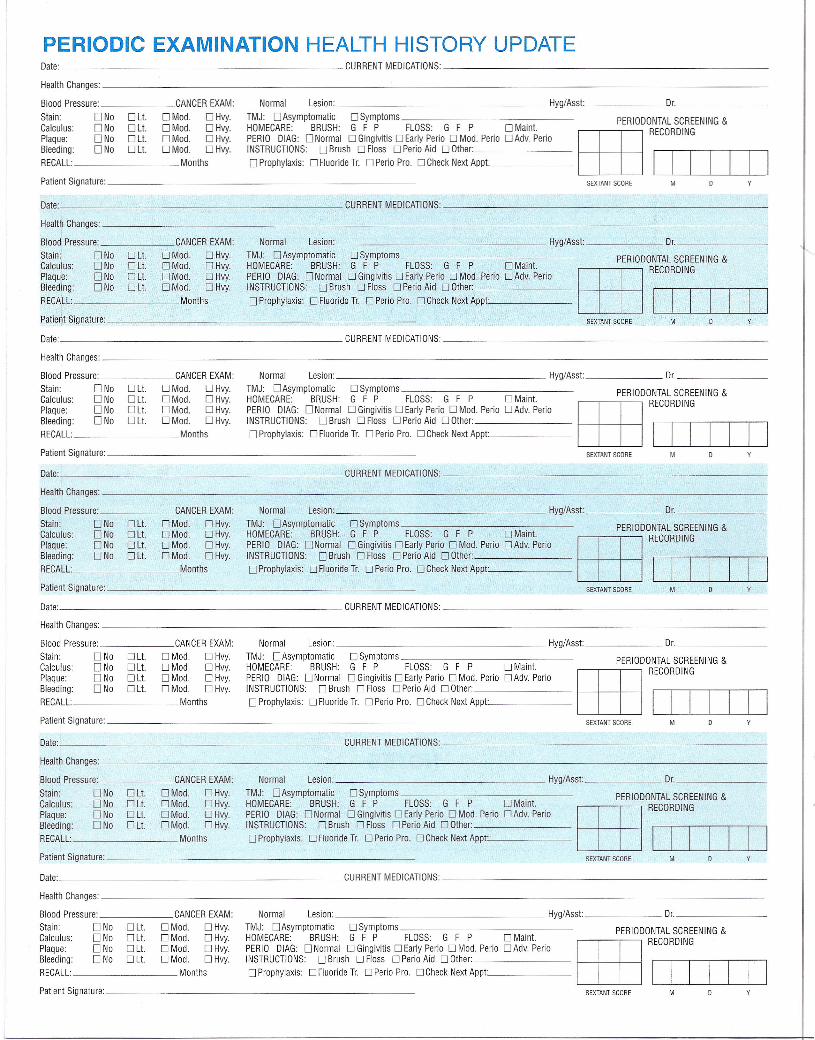
Normal Lesion: Hyg/Asst Dr. _
TMJ: DAsymptomatic DSymptoms_____________ PERIODONTALSCREENING&
HOMECARE: BRUSH: G F P FLOSS: G F P D Maint. EEB ROIIJIJECORDINGPERIO DIAG: D Normal D Gingivitis DEarly Perio D Mod. Perio D Adv. PerioINSTRUCTIONS: D Brush D Floss D Perio Aid D Other: _
D Prophylaxis: D Fluoride Tr. D Perio Pro. D Check Next Appt~· _
PERIODIC EXAMINATION HEALTH HISTORY UPDATEDate: CURRENTMEDICATIONS: _
Health Changes: _
Blood Pressure: CANCEREXAM:
Stain: D No D Lt. D Mod. D Hvy.Calculus: D No D Lt. D Mod. D Hvy.Plaque: D No D Lt. D Mod. D Hvy.Bleeding: D No D Lt. D Mod. D Hvy.
RECALL: Months
Patient Signature: _ SEXTANT SCORE M
Date: CURRENT MEDICATIONS: _
Health Changes: ------------------------
Blood Pressure: CANCEREXAM:
Stain: DNa D Lt. D Mod. D Hvy.Calculus: D No D Lt. D Mod. D Hvy.Plaque: D No D Lt. D Mod. D Hvy.Bleeding: D No D Lt. D Mod. D Hvy.
RECALL: Months
Normal Lesion: Hyg/Asst Dr. _
TMJ: DAsymptomatic DSymptoms______________ PERIODONTALSCREENING&
HOMECARE: BRUSH: G F P FLOSS: G F P D Maint. tm ROIIJIJECORDINGPERIO DIAG: DNormal DGingivitis DEarly Perio DMod. Perio DAdv. PerioINSTRUCTIONS: D Brush D Floss D Perio Aid D Other: _
D Prophylaxis: D Fluoride Tr. D Perio Pro. D Check Next Appt., _
Patient Signature:________________________ SEXTANT SCORE M
Date: CURRENT MEDICATIONS: _
Health Changes: _
Blood Pressure: CANCEREXAM:
Stain: D No D Lt. D Mod. D Hvy.Calculus: D No D Lt. D Mod. D Hvy.Plaque: D No D Lt. D Mod. D Hvy.Bleeding: D No D Lt. D Mod. D Hvy.
RECALL: Months
Normal Lesion: Hyg/Asst Dr. _
TMJ: DAsymptomatic DSymptoms______________ 0 0 SC EENING&HOMECARE: BRUSH: G F P FLOSS: G F P D Maint. PERI D NTAL Rtm ROIIJIJECORDINGPERIO DIAG: D Normal D Gingivitis DEarly Perio D Mod. Perio D Adv. PerioINSTRUCTIONS: D Brush D Floss D Perio Aid D Other: _
D Prophylaxis: D Fluoride Tr. D Perio Pro. D Check Next Appt., ------
Patient Signature: _ SEXTANT SCORE M
Date: CURRENTMEDICATIONS: _
Health Changes: _
Blood Pressure: CANCEREXAM:
Stain: D No D Lt. D Mod. D Hvy.Calculus: D No D Lt. D Mod. D Hvy.Plaque: D No D Lt. D Mod. D Hvy.Bleeding: D No D Lt. D Mod. D Hvy.
RECALL: Months
Normal Lesion: Hyg/Asst Dr. _
TMJ: DAsymptomatic DSymptoms______________ PERIODONTALSCREENING&
HOMECARE: BRUSH: G F P FLOSS: G F P D Maint. tm ROIIJIJECORDINGPERIO DIAG: DNormal DGingivitis DEarly Perio DMod. Perio DAdv. PerioINSTRUCTIONS: D Brush D Floss D Perio Aid D Other: _D Prophylaxis: D Fluoride Tr. D Perio Pro. D Check Next Appt: _
Patient Signature: _
Date: CURRENTMEDICATIONS: _
SEXTANT SCORE M
Health Changes: _
Blood Pressure: CANCEREXAM:
Stain: D No D Lt. D Mod. D Hvy.Calculus: D No D Lt. D Mod. D Hvy.Plaque: D No D Lt. D Mod. D Hvy.Bleeding: D No D Lt. D Mod. D Hvy.RECALL: Months
Normal Lesion: Hyg/Asst Dr. _
TMJ: DAsymptomatic DSymptoms______________ PERIODONTALSCREENING&
HOMECARE BRUSH: G F P FLOSS G F P D Maint. EEJ ROIIJIJECORDINGPERIO DIAG: D Normal D Gingivitis DEarly Perio D Mod. Perio D Adv. PerioINSTRUCTIONS: D Brush D Floss D Perio Aid D Other: _
D Prophylaxis: D Fluoride Tr. D Perio Pro. D Check Next Appt: _
Patient Signature: _ M
Date: CURRENTMEDICATIONS: _
Health Changes: _
Blood Pressure: CANCEREXAM:
Stain: D No D Lt. D Mod. D Hvy.Calculus: D No D Lt. D Mod. D Hvy.Plaque: D No D Lt. D Mod. D Hvy.Bleeding: D No D Lt. D Mod. D Hvy.RECALL: Months
SEXTANT SCORE
Normal Lesion: Hyg/Asst Dr. _
TMJ: DAsymptomatic DSymptoms_____________ PERIODONTALSCREENING&
HOMECARE: BRUSH: G F P FLOSS: G F P D Maint. tm ROIIJIJECORDINGPERIO DIAG: DNormal DGingivitis DEarly Perio DMod. Perio DAdv. PerioINSTRUCTIONS: D Brush D Floss D Perio Aid D Other: _
D Prophylaxis: D Fluoride Tr. D Perio Pro. D Check Next Appt.. ------
Patient Signature: _ MSEXTANT SCORE
Date: CURRENT MEDICATIONS: _
Health Changes: _
Blood Pressure: CANCEREXAM:
Stain: D No D Lt. D Mod. D Hvy.Calculus: D No D Lt. D Mod. D Hvy.Plaque: DNa D Lt. D Mod. D Hvy.Bleeding: D No D Lt. D Mod. D Hvy.RECALL: Months
Normal Lesion: Hyg/Asst Dr. _
TMJ: DAsymptomatic DSymptoms_____________ PERIODONTALSCREENING&
HOMECARE: BRUSH: G F P FLOSS: G F P D Maint. EEE ROIIJIJECORDING .PERIO DIAG: D Normal D Gingivitis DEarly Perio D Mod. Perio D Adv. PerioINSTRUCTIONS: D Brush D Floss D Perio Aid D Other: _D Prophylaxis: D Fluoride Tr. D Perio Pro. D Check Next Appt., _
Patient Signature: _ SEXTANT SCORE M



























![Welcome [sa1s3.patientpop.com]](https://img.pdfslide.us/doc/110x75/616ea213d147783a3d28f458/welcome-sa1s3-.jpg)

