Embed Size (px)
Citation preview

Health expenditure 2015

National Institute for Health Development
Department of Health Statistics
Estonian Health Care Expenditure in 2015
Tallinn 2017

2
Mission of the Department of Health Statistics:
Public Health and Welfare through Better Statistics and Information
Authors: Mare Ruuge, Marika Inno
Please note! As is normal for statistical analyses, slight adjustments of the data provided in this analysis are possible during a year. Please refer to the online versions (analysis at http://www.tai.ee/en/ and data at http://pxweb.tai.ee/PXWeb2015/index_en.html) when using the report and the data.

3
BRIEF SUMMARY
Estonian health expenditure made up 6.5% of the GDP.
Estonian health expenditure in 2015 was 1.3 billion euros.
During 2009–2015, health expenditure in current prices increased by 397 million euros, 98
million euros from that marks the increase in 2015.
In 2015, health expenditure in current prices increased by 7.8% when compared to the previous
year, in constant prices increase was 1.4%.
The average annual increase in health expenditure during 2009–2015 was 6.2% in current prices
and 1.6% in constant prices.
The expenditure of the Estonian Health Insurance Fund was 856 million euros and their share in
total health expenditure was 64.8%.
The central government expenditure was 122 million euros and its share was 9.2%.
The expenditure of households was 300 million euros and their share was 22.7%.
The Estonian health expenditure per person in 2015 was 1,006 euros, of which the public sector
share was 761 euros and the share of households was 229 euros.

4
CONTENTS
INTRODUCTION ....................................................................................................................................... 5
1. FINANCING OF ESTONIAN HEALTH EXPENDITURE .............................................................................. 6
1.1 Health expenditure and gross domestic product .......................................................................... 6
1.2 Health care financing sources ....................................................................................................... 9
1.3 Health care financing schemes .................................................................................................... 12
2. DIVISION OF HEALTH EXPENDITURE BY SERVICES AND SERVICE PROVIDERS ................................... 22
3. HEALTH EXPENDITURE PER CAPITA ................................................................................................... 27
4. ACCOUNTING METHODOLOGY OF HEALTH EXPENDITURE ............................................................... 30
REFERENCE MATERIAL ........................................................................................................................... 33

5
INTRODUCTION
This analysis, which is a part of the series “Health Expenditure in Estonia”, published by the National Institute for Health Development, gives an overview of health expenditure during 2009–2015.
The objective of the analysis is to provide information about the financing of health system through various financing sources, financing schemes, health services, and service providers, using the methodology for calculating national health accounts titled SHA20111 and developed by OECD (Organisation for Economic Cooperation and Development), WHO (World Health Organization), and Eurostat (Statistical office of the European Union). Internationally comparable health expenditure data is available on the OECD database in the health section: http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT
According to the methodology of SHA2011, health expenditure includes health services, such as curative care, rehabilitation, nursing care, ancillary health services, medical products, prevention, and the administration of health system. However, health expenditure does not include the expenditure of teaching, health research and development, environmental health and other services, where the main activity is not improvement of health. Capital investments have been excluded from expenditure and are examined separately.
The analysis covers expenditure on Estonian residents. This means that health expenditure does not reflect the cost of health services provided to foreigners and the cost of medical goods purchased by foreigners to the known extent.
The analysis presents the results of methodological work done with revision of the system of data collection conducted during the past three years, as well as data from previous years, recalculated on the basis of the new system. Further recalculations have been scheduled, in order to provide access to data users to time series from the year 2000 and onwards; however, the data that has currently been harmonized, published and transmitted to international databases is that of the years 2009–2015.
This publication is intended to be used by all institutions and persons interested in the field of health financing, and by the wider public.
The compilers would like to thank all who provided data and information and in doing so, contributed to the calculation of health expenditure.
1OECD’s methodology is used in more than 100 countries under the name of System of Health Accounts (SHA).
Another expression used is the National Health Accounts (NHA). http://ec.europa.eu/eurostat/documents/3859598/5916161/KS-30-11-270-EN.PDF/655cbab0-4f9d-4d41-82bb-d39b6fb3f397?version=1.0 or on the website of the National Institute for Health Development http://www.tai.ee/images/PDF/Metoodika/A_system_of_Health_Accounts_2011.pdf

6
1. FINANCING OF ESTONIAN HEALTH EXPENDITURE
1.1 Health expenditure and gross domestic product
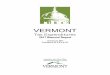
In 2015, the Estonian health expenditure in current prices was 1.321 billion euros. Health expenditure amounted to 6.5% of GDP (Figure 1.1.1).
Health expenditure is influenced by the system of financing and organizing health care, as well as
social and economic factors. There is a strong correlation between general income level and how
much the state spends on health care. The general level of health expenditure is measured by its
relationship to gross domestic product.
Figure 1.1.1. Health expenditure as a share of GDP, 2015
1. Includes investments. 2. OECD estimate.
Source: http://www.oecd.org/health/health-at-a-glance-europe-23056088.htm
Estonia is among those European countries where health expenditure makes up the smallest
percentage of GDP; Estonia is on the same level with other Baltic countries, Poland and Croatia. The
average percentage in the European Union (EU28) is 9.9%, the Estonian figure makes up 64% of the
average. On the one hand, this characterizes the operational efficiency of the Estonian health care
system, but on the other hand it shows that most other countries have a broader selection of
financed necessary health care services, and that services are also financed to a greater extent (see
the international comparison of health expenditure per person in Figure 3.3).
11
,1
11
,1
11
,0
10
,8
10
,6
10
,4
10
,4
9,9
9,8
9,6
9,6
9,4
9,1
9,0
8,9
8,4
8,3
8,2
7,5
7,2
7,0
7,0
6,8
6,6
6,5
6,5
6,3
5,6
5,0
11
,5
9,9
8,8
0
2
4
6
8
10
12
14
Private/voluntary Government/compulsory
%

7
Figure 1.1.2. EU28 and Estonian health expenditure as a share of GDP, 2005–2015
In the case of health expenditure percentage from the GDP, it is reasonable to monitor the general
level, not so much the decimal points. As it shows the relationship between two indicators, every
GDP change or change in health expenditure will somewhat change the result. One year’s result can
even be significantly influenced by a situation in which the GDP and health expenditure are changing
in opposite directions, or as was the case in Estonia in 2009, when the GDP dropped by 14% and
health expenditure decreased by 2% in comparison with the previous year (Figure 1.1.2). The
percentage of health expenditure from GDP increased during the economic crisis years of 2008–
2009, decreased during 2010–2011 and has been increasing again since 2013. If we take a look at the
corresponding changes in GDP and health expenditure (Figure 1.1.3), it is clear that the changes in
health expenditure reflect general economic changes with a certain reference period.
Figure 1.1.3. Changes in GDP and health expenditure, 2006–2015
8,7 8,7 8,7 8,9 9,7 9,6 9,5 9,6 9,9 10,0 9,9
5,0 4,9 5,0 5,7
6,5 6,3 5,8 5,8 6,0 6,1 6,5
0
2
4
6
8
10
12
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
%
EU28
Estonia
-20
-10
0
10
20
30
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Annual growth of HE
Annual growth of GDP
%

8
When comparing changes in Estonian health expenditure and in gross domestic product, it is clear
that in 2010 and 2011, the increase in GDP exceeded that of health expenditure; those indicators
were equal in 2012 (Figure 1.1.3) and since 2013 health expenditure has increased faster than GDP.
Figure 1.1.4. Percentage of health expenditure from GDP and health expenditure in current prices, 2009–2015 Even though health expenditure has continuously increased, from 924 million euros in 2009 to 1,324
million euros in 2015 (Figure 1.1.4), the share of expenditure in GDP has, due to changes in GDP,
moved in the opposite direction during 2010–2011. By 2015, the share of health expenditure in GDP
has returned to the same level as in 2009.
Figure 1.1.5. Growth and real growth of health expenditure, 2010–2015
0%
1%
2%
3%
4%
5%
6%
7%
0
200
400
600
800
1 000
1 200
1 400
2009 2010 2011 2012 2013 2014 2015
The
shar
e o
f G
DP
Hea
lth
exp
end
itu
re in
cu
rren
t p
rice
s,
mill
lion
eu
ros
Health expenditure
The share of GDP
-2
0
2
4
6
8
10
2010 2011 2012 2013 2014 2015
Health expenditure in current prices
Health expenditure in constant prices (reference year 2010)
%

9
The increase of health expenditure in current prices in 2015 was 7.8% compared to the previous
year, whereas real growth, on the basis of constant prices 2, was 1.4% (Figure 1.1.5). The average
annual growth rate of health expenditure during 2009–2015 was 6.1%, real growth rate was 1.6%.
The health expenditure in current prices was 43% higher in 2015 than it was 2009, the increase in
constant prices was 10%.
1.2 Health care financing sources
In order to finance Estonian health care, funds are collected from three main sources: social security
contributions (62% in 2015), other domestic revenues, such as revenue of households and private
companies (24%), and revenues of the state budget (14%). Social security contributions consist of the
health insurance part of social tax paid by the employer (13% of an employee’s wages). Other
domestic revenues include people’s out-of-pocket payments in health expenditure and companies’
expenditure on health care services (incl. occupational health). In Estonia, household out-of-pocket
payments make up the majority of other domestic revenue, i.e. 93–94%.
Figure 1.2.1 Health expenditure by financing source, 2015
External resources (both direct and those distributed by the state) make up a minimal share in health
financing sources. This shows that the Estonian health care system is relatively independent of
external resources when it comes to financing running costs. Private insurance financing schemes are
not common in Estonia either, nor do they influence the system.
2 Constant price – value of goods or services in a reference period (reference year used here: 2010) in average
prices. Current price of goods and services is deflated by the price index.
Transfers from government
domestic revenues (FS.1)
14%
Transfers distributed by
government from foreign origin
(FS.2) 0,2%
Social insurance contributions
(FS.3) 62%
Voluntary prepayment (FS.5)
0,3% Direct foreign
transfers (FS.7) 0,005%
..Other revenues from households
n.e.c. (FS.6.1) 23%
..Other revenues from corporations
n.e.c. (FS.6.2) 1%
Other domestic revenues
n.e.c. (FS.6) 24%

10
There have been no significant changes in the financing of the Estonian health care system during the
past seven years. All financing sources continue to contribute to growth more or less proportionally.
No new financing sources have been emerged during the aforementioned period.
The time series from 2009–2015 (Figure 1.2.2) depicts 2010 as an exceptional year, during which
state budget revenues and social security contributions decreased in current prices when compared
to the previous year, whereas other domestic revenues continued to increase. In 2014, state budget
revenues were used for health expenditure to a smaller extent than it was in 2013. The increase in
other domestic revenues remained moderate in 2011, the growth was 5 million euros, i.e. 2%. In
2013, domestic revenues increased by 14%, the growth remained a consistent 8% during other years.
Figure 1.2.2. Distribution of health expenditure by financing sources, 2009–2015
The share of other domestic revenues has increased in the structure of health expenditure financing
sources; this increase has stayed on the same level for the past three years (Figure 1.2.3). In terms of
state budget revenues, 2014 was an exceptional year when the share of other domestic revenues
was smaller than in previous years and in 2015. The share of social security contributions for that
period remained in the range of 60.9–63.2%, the lowest percentage was in 2010 and the highest in
2014.
578 567 592 651 701 773 816
203 219 224 241
275 296
318
137 125 136 145
156 148
180
0
200
400
600
800
1 000
1 200
1 400
2009 2010 2011 2012 2013 2014 2015
Mill
ion
eu
ros
Direct foreign transfers (FS.7)
Transfers distributed by government from foreign origin (FS.2) Voluntary prepayment (FS.5)
Transfers from government domestic revenues (FS.1)
Other domestic revenues n.e.c. (FS.6)

11
Figure 1.2.3. Structure of health expenditure by financing sources, 2009–2015
62,6 60,9 61,2 62,4 61,7 63,2 61,8
22,0 23,5 23,1 23,1 24,2 24,2 24,1
14,8 13,5 14,0 13,8 13,8 12,1 13,6
0%
20%
40%
60%
80%
100%
2009 2010 2011 2012 2013 2014 2015
Direct foreign transfers (FS.7)
Transfers distributed by government from foreign origin (FS.2)
Voluntary prepayment (FS.5)
Transfers from government domestic revenues (FS.1)
Other domestic revenues n.e.c. (FS.6)
Social insurance contributions (FS.3)

12
1.3 Health care financing schemes
The Estonian health care is financed through three main financing schemes. These are the national
health insurance i.e. the Estonian Health Insurance Fund, households and the government.
In 2015, the Estonian Health Insurance Fund (EHIF) financed 64.8%, household’s out-of-pocket
payments, i.e. people’s expenditure on health care services and goods made up 22.7% and the
central government financed 9.2%. Voluntary health financing schemes have a quite small share in
Estonian health expenditure, the corresponding indicator was 1.6% in 2015. Local government
financing was 1.7%. The share of external financing (rest of the world) is extremely small, since the
external financing of health sector predominantly takes place through the central government
schemes.
The structure of financing schemes has been consistent throughout the observed years, although the
expenditure in all schemes has increased year by year (excl. the EHIF decrease in 2010). The share of
local governments and central government has remained 10–11% during all years and the share of
voluntary financing models was 1.6–1.8% (Figure 1.3.1). The share of EHIF in health expenditure has
decreased slightly (it was 67% in 2009 and 65% in 2015). For the same extent has increased the share
of households (from 20% in 2009 to 23% in 2015).
Figure 1.3.1. Distribution of health expenditure by financing schemes, 2009–2015
During 2009–2015, health expenditure increased by 397 million euros, 98 million euros from that marks the increase in 2015 (Figure 1.3.2).
67,4 65,6 65,8 65,9 64,8 65,7 64,8
20,4 22,0 21,6 21,5 22,6 22,7 22,7
9,0 9,6 9,6 9,5 9,6 8,9 9,2
0%
20%
40%
60%
80%
100%
2009 2010 2011 2012 2013 2014 2015
Rest of the world (HF.4)
Local government (HF.1.1.2)
Voluntary schemes (HF.2)
Central government (HF.1.1.1)
Household out-of-pocket payment (HF.3)
Estonian Health Insurance Fund (HF.1.2.1)

13
Figure 1.3.2. Health expenditure by financing schemes, 2009–2015
As previously mentioned, the expenditure of nearly all providers of finance contributors increased in
current prices during 2009–2015 (Figure 1.3.3).
Figure 1.3.3. Annual growth in health expenditure by financing schemes, 2009–2015
The average annual growth in central government financing during the period was 7%, remaining in
the range of 7–10% during most years, this indicator was the lowest in 2011 and exceeded the 10%
limit in 2015. The growth of the Estonian Health Insurance Fund contribution has been more evenly
distributed over the years, the annual average growth was 6%, with the sole exception of the
decrease in 2010. The cost-sharing of households in health expenditure increased on average by 8% a
622 610 638 688 736 803 856
188 204 209 225
257 278
300
83 90 93 99
109 109
122
0
200
400
600
800
1 000
1 200
1 400
2009 2010 2011 2012 2013 2014 2015
Mill
ion
eu
ros
Rest of the world (HF.4)
Local government (HF.1.1.2)
Voluntary schemes (HF.2)
Central government (HF.1.1.1) Household out-of-pocket payment (HF.3) Estonian Health Insurance Fund (HF.1.2.1)
Total 924 930 969 1 044 1 136 1 223 1 321
-5% 0% 5% 10% 15% 20%
Voluntary schemes (HF.2)
Household out-of-pocket payment (HF.3)
Estonian Health Insurance Fund (HF.1.2.1)
Central government (HF.1.1.1) + Local government (HF.1.1.2)
2009/2010
2010/2011
2011/2012
2012/2013
2013/2014
2014/2015

14
year, the exceptions being in 2011 when the increase was about 2% and in 2013 when the increase
was 14% compared to the previous year.
Almost two-thirds of the total volume of health expenditure in Estonia is financed through the
Estonian National Health Insurance Fund, in the total sum of 856 million euros. In 2015, the health
expenditure of EHIF increased by 53 million euros, i.e. 6.6%, when compared to the previous year. In
2014, the growth was compared to the previous year 9.1%.
Revenue of the health insurance part of the social security tax has increased by 7% in 2015, and 8% in
20143. Service expenditure changed as follows:
in 2014 in 2015
General medical care
+8% +12%
Specialised medical care
+10% +6%
Nursing care +19% +16%
Dental care +4% +9%
Compensation of pharmaceuticals
+6% +3%
In absolute value, the largest share of health expenditure in 2015 formed inpatient care expenditure
– 294 million euros or 34% (281 million euros in 2014) (Figure 1.3.4). Outpatient general and
specialised medical care covered 28% or 237 million euros of the expenditure of the Estonian Health
Insurance Fund (219 million euros in 2014). The compensation on prescribed medicines amounted to
14% or 114 million euros from the health expenditure of the Estonian Health Insurance Fund (110
million euros in 2014).
Figure 1.3.4. Health expenditure of the Estonian Health Insurance Fund by service groups, 2009–
2015
3 Source: Estonian Health Insurance Fund Yearbook 2015
430 416 432 461 491 535 569
15 14 15 17
20 24
28
62 61 72 78
87 94
104
92 95 96
107 112
119 122
0
100
200
300
400
500
600
700
800
900
2009 2010 2011 2012 2013 2014 2015
Mill
ion
eu
ros
Health system administration (HC.7) Preventive care (HC.6)
Pharmaceuticals and medical goods (HC.5) Ancillary services (HC.4)
Long-term care (HC.3)
Rehabilitative care (HC.2)
Curative care (HC.1)

15
Over the reference years, the expenditure structure of the Estonian Health Insurance Fund has
remained stable and only minor changes have occurred. The task of the EHIF as the main health
contributor is to ensure the stability of financing of medical care at different levels and the
sustainability of health insurance. In addition to health care services, support has to be provided to
people for purchasing necessary pharmaceuticals and therapeutic appliances as well. On the basis of
the expenditure structure by main service groups in 2009–2015, the share of curative care has
decreased slightly (from 69% to 67%), the share of ancillary health services, such as imaging and
other diagnostic services, has increased (from 10% to 12%). The share of nursing care expenditure
has been 3% as of 2012, before that is was 2%. The share of medical goods in 2015 was 14%, 15%
during previous years and even 16% in 2010. A decrease has occurred in the expenditure of
prescribed medicines.
The second largest group in the expenditure of curative care services, after inpatient care, during
2009–2015, was family physician care, i.e. basic medical and diagnostic services, which made up 30%
(Figure 1.3.5). The share of inpatient care during the observed time period has decreased from 55%
to 52% and the share of day care has increased from four to six percent.
Figure 1.3.5. Distribution of health expenditure of the Estonian Health Insurance Fund in curative
care, 2009–2015
Expenditure incurred through the central government, which has a 9% share in Estonian health
expenditure, has been depicted in Figure 1.3.6. When in 2014, the expenditure incurred through the
central government remained on the same level as the previous year, then in 2015, it increased by
12%. The absolute value of health expenditure incurred by the central government in 2014 was 109
million euros and 122 million euros in 2015.
55 56 55 55 54 53 52
4 4 4 4 4 6 6
29 30 30 30 31 28 31
6 5 5 5 6 6 6
6 5 5 5 5 8 5
0%
20%
40%
60%
80%
100%
2009 2010 2011 2012 2013 2014 2015
Home-based care (HC.1.4)
Specialised outpatient care (HC.1.3.3)
Dental care (HC.1.3.2)
General outpatient care (HC.1.3.1)
Day care (HC.1.2)
Inpatient care (HC.1.1)

16
Figure 1.3.6. Health expenditure of the central government by service groups, 2009–2015
The largest section of health expenditure of the central government was made up of ancillary health
services expenditure, the majority of which is for financing of ambulance service. The expenditure of
these services increased by a fifth, i.e. 6.7 million euros, when compared to 2014. Therefore,
expenditure concerning ambulance service and transport of patients made up 29% of central
government health expenditure in 2015, in 2014 less – 26.5%. The second larger service group was
curative care, which made up 23% of central government health expenditure. With an increase of
only 0.9%, the financing of curative care remained almost on the same level as in 2014. With regard
to curative care services, the central government finances the inevitable care provided to uninsured
persons, the health services in prisons and the Defence Forces of Estonia, and HIV/AIDS treatment. In
2015, prevention (incl. HIV and tuberculosis programmes and immunization) became the third
largest group among services financed by the central government with 13%, thereby reaching on the
same level as nursing care. Even though rehabilitation care expenditure makes up only 1.7% of
central government expenditure, the increase of this group’s expenditure is noticeable despite
relatively large fluctuations. The central government expenditure on rehabilitation increased by 11%
in 2015.
Nearly 90% of central government health expenditure is financed through the Ministry of Social
Affairs. Expenditure incurred through the Ministry of Social Affairs during 2009–2015 amounted to
an average of 8.5% of health expenditure.
Household out-of-pocket payments are made up of people’s compulsory cost-sharing payments in
the case of health care services and goods reimbursed by the EHIF, and in the case of other services
that are not on the list of services and pharmaceuticals reimbursed by the EHIF, from the expenses
paid for those.
Household out-of-pocket payments amounted to 22.7% of health expenditure both in 2015 and
2014. The health expenditure of households made up 278 million euros in 2014, and 300 million
26 26 27 27 29 31 37
13 12 14 20 26 28
28
7 11 11 13
9 12
16
13 13 13
12 14
14
15
13 15 15
15
19 11
12
11 13 14
12
10 12
11
0
20
40
60
80
100
120
2009 2010 2011 2012 2013 2014 2015
Mill
lion
eu
ros
Rehabilitative care (HC.2)
Health system administration (HC.7) Pharmaceuticals and medical goods (HC.5) Long-term care (HC.3)
Preventive care (HC.6)
Curative care (HC.1)
Ancillary services (HC.4)

17
euros in 2015. The increase in expenditure when compared to the previous year was 8.2%, which is
0.4 percentage points larger than the general growth of health expenditure.
The current level of household out-of-pocket payments place Estonia in the warning and caution
zone according to both the OECD and WHO (15–30% of health expenditure). Using health care
services at such a level of out-of-pocket payments is expensive for low-income people and brings
about the risk of not receiving medical assistance on time or of a worsening financial situation in the
case of receiving care. However, the Estonian National Health Plan 2009–2020 has set the maximum
limit of out-of-pocket payments at 25%. In recent years, the percentage of out-of-pocket payments
has gradually increased, but it still remains in the set limits.
Services in the case of which the share of the public sector financing is smaller the share of out-of-
pocket payments is larger in households’ expenditure. Out-of-pocket payments are smallest in the
most expensive health care service, inpatient care service, however, inpatient care expenditure
makes up the largest share among all health care services. Similarly, the expenditure of family
physician service is not visible in households’ expenditure.
The largest part in people’s expenditure when observing health care services by service groups has,
through the years, gone to pharmaceuticals, medical goods and curative care services, which in the
case of households primarily include dental care and specialised outpatient medical care (Figure
1.3.7).
Figure 1.3.7. The household health expenditure by services, 2009–2015 * Other curative care – curative care services other than dental care, i.e. inpatient care, day care, family physician care,
specialised outpatient medical care and home-based curative care.
Dental care expenditure made up the largest share of curative care services (29% in 2015) when
observing household expenditure by separate services. Prescribed medicines made up 22% of
household health expenses and over-the-counter medicines made up 16%. A total of 8% of health
expenditure was spent on long-term care services, 12% on specialised outpatient medical care and
22 32 27 28 35 39 43
46 48 54 58
71 77 87 12
14 13 14
18 23
25 103
107 109 119
125 131
139
0
50
100
150
200
250
300
2009 2010 2011 2012 2013 2014 2015
Mill
lion
eu
ros
Pharmaceuticals and medical goods (HC.5)
Ancillary services (HC.4)
Long-term care (HC.3)
Rehabilitative care (HC.2)
Dental care (HC.1.3.2)
Other curative care* (HC.1)

18
8% on various therapeutic appliances (incl. glasses). The expenditure structure was very similar to
that of 2014.
Figure 1.3.8. Structure of household health expenditure by service groups, 2009–2015 * Other curative care – curative care services other than dental care, i.e. inpatient care, day care, family physician care,
specialised outpatient medical care and home-based curative care.
The share of pharmaceuticals and therapeutic appliances in the expenditure structure of households
has decreased during 2009–2015 (Figure 1.3.8). The first, slight decrease took place in 2010 and the
second, more significant decrease occurred in 2013; the decrease continued in 2014 and 2015 as
well. Whereas until 2009, the share of pharmaceuticals and therapeutic appliances was 55%, by 2015
that indicator has dropped to 46%. The biggest influence factors here have been the ever-increasing
use of generic pharmaceuticals and the additions made to the list of therapeutic appliances that are
compensated by the Estonian Health Insurance Fund. Along with the decreased share of expenditure
on medical goods – pharmaceuticals and therapeutic appliances, the share of services has increased
in the health expenditure of households, including the share of curative care services (from 36% to
43%) and that of nursing care (from 6% to 8%). There have been small fluctuations in the share of
rehabilitation expenditure (2–3%). Compared to 2014, in 2015, people’s expenses on rehabilitation
decreased by a third, the decrease occurred in the use of outpatient rehabilitation services.
12 15 13 13 14 14 14
24 23 26 26 28 28 29
6 7 6 6 7 8 8
55 52 52 53 49 47 46
0%
20%
40%
60%
80%
100%
2009 2010 2011 2012 2013 2014 2015
Pharmaceuticals and medical goods (HC.5)
Ancillary services (HC.4)
Long-term care (HC.3)
Rehabilitative care (HC.2)
Dental care (HC.1.3.2)
Other curative care* (HC.1)

19
Figure 1.3.9. Growth in household health expenditure by service groups, 2009–2015, 2009=0% * Other curative care – curative care services other than dental care, i.e. inpatient care, day care, family physician care,
specialised outpatient medical care and home-based curative care.
The fastest growth in the expenditure of households during 2009–2015 (Figure 1.3.9) occurred in
expenses on nursing care (2.1 times), on dental care and other curative care (1.9 times). The
expenditure of pharmaceuticals and other medical products increased 1.4 times. Increases in
rehabilitation expenditure have occurred with fluctuations.
Changes in expenditure can be compared to changes in the use of health care services. According to
statistics collected by the National Institute for Health Development, the number of dental care visits
has been steadily increasing after the decrease in 2010 (-4%), a little less than 1% per each year, with
the exception of 2014, when the increase was 2.4%. The change has occurred due to an increase in
the number of dental care visits by 15-year-olds and older people, as the number of visits of 14-year-
olds and younger children has decreased slightly. The reason here is not the decrease of children in
the population, as the rate for 1,000 children of the same age has also been constantly decreasing
since 2009.
The number of denture visits decreased in 2010 and 2011, increased up to 2014, when the number
of visits exceeded that of 2009, and decreased again in 2015 by 2%.
There was a bigger increase in orthodontic treatment of children up to 14 years old in 2011, but the
indicator has been decreasing ever since. However, the number of visits to orthodontists by 15-year-
olds and older people has, after the 10% fall in 2010, been increasing significantly – at least 9% per
year.
2010 was a year of decrease in the use of outpatient medical care, which was followed by a
compensating increase in 2011, after which annual changes have been small fluctuations. In 2010,
the number of visits to medical specialists decreased by 2% (4% in the case of children aged 0–14
years, 1% in the case of 15-year-olds and older) when compared to the previous year. In 2015, the
-20
0
20
40
60
80
100
120
2009 2010 2011 2012 2013 2014 2015
Total
Other curative care* (HC.1)
Dental care (HC.1.3.2)
Rehabilitative care (HC.2)
Long-term care (HC.3)
%

20
number of visits to medical specialists made up 99.5% of visits of adults and 92% of visits of children
made in 2009. The number of physicians’ home visits has decreased quite significantly: in 2015, the
number of family doctors home visits made up 30% of the home visits to children aged 0–14 years
and 47% of the home visits to 15-year-olds and older people made in 2009.
When it comes to the use of inpatient care, the number of hospital discharges per year decreased by
0.8% on average, with the exception of 2013, when the number of hospital discharges increased by
1.6% when compared to the previous year. The number of hospitalised patients in curative care (by
bed specialty) has also decreased; significant decreases when compared to the previous year
occurred in 2012 (3%), 2014 and 2015 (2%). In 2015, there were 7% less hospitalisations in curative
care when compared to 2009, but 31% more in inpatient nursing care. The number of
hospitalisations in inpatient nursing care has increased with nearly every year – the average annual
growth for the period is 5% per year, but there was no increase in 2011 and 2015 saw a 5% decrease
compared to the previous year. 2011 was an exceptional year in terms of using day care as the
number of discharges from day care increased by 13% when compared to the previous year; the
average increase for the period was 5.6% per year. The number of discharges from day care had
increased 38% by 2015, when compared to 2009.
Independent work of qualified nurses has increased during 2009–2015: outpatient consultations by
17% per year on average, home visits by 6% per year. When compared to 2009, the number of
outpatient consultations increased by 2.5 times by 2015, the number of home visits increased by
44%.
Figure 1.3.10. Distribution of health expenditure by financing schemes, 2014
Source: http://www.oecd.org/health/health-at-a-glance-europe-23056088.htm
7
84
12
83
8 5 4
79
15
37
4 11
31
76
10
62
3 9
3
65 69 67
10 9
65 60
28
9
44
74
52
19
78 72 74 76 76 64
42
75 66
45
66
13
73 62 68
5 2
57 58
1
31
44
1
11
29
47
13 14 13 16 11 12 18 15 20
15 7
18 18 22 23 19 17 22 13
25 15
29 31 28 28 39 35 46 50
14 17
27
1 2 1 5 6 4 5
14 4 5 1
3 8 4 15
5 13
2 1 3 5 1 4 4
0
10
20
30
40
50
60
70
80
90
100
%
Government schemes Compulsory health insurance Out-of-pocket Voluntary health insurance Other

21
When we compare Estonian health expenditure structure by financing schemes with those of other
member states, the distinction can be made is between the countries that have national health
insurance system just like Estonia, and countries that do not have a system like that or where it has
very little significance. The structure of health expenditure by financing schemes does not depend on
the countries’ wealth or population size, instead it characterises the financing organisation of
countries’ health care systems. In Figure 1.3.10, countries have been listed in descending order based
on the share of financing through the public sector. Based on this indicator, Estonia is rather close to
the average in EU28: 76% of Estonian health expenditure is financed through the government and
the health insurance fund; the average for EU28 is 79%. Financing through households is more
extensive in Estonia than the average indicator of EU countries – 23% in Estonia, 15% in EU28.
Voluntary health financing schemes (private insurance, private companies) have a relatively small
share (0.2%) in Estonian health expenditure; the average EU28 for this indicator is 5%.
The contribution of the central government and local governments to the Estonian health care
financing is on the average European level (Figure 1.3.11). However, place on the list depends on the
differences of health care systems in different countries (see Figure 1.3.10 as well).
Health care is in the third place in the government budget, right after social protection and
education. The government’s contribution to health care is one of the biggest, which in 2014 made
up 13.5% of the total of government expenditure; the share has been gradually increasing year by
year.
Figure 1.3.11. Share of government health expenditure from the total government expenditure,
2014
Source: http://apps.who.int/gho/data/view.main.HEALTHEXPRATIOSWE?lang=en
14,0% 13,5%
0%
5%
10%
15%
20%
25%

22
2. DIVISION OF HEALTH EXPENDITURE BY SERVICES
AND SERVICE PROVIDERS
If we divide Estonian health expenditure based on service providers (Figure 2.1), then nearly half of
the expenditure was incurred by hospitals (47%), the largest health care service providers, in the
absolute value of 623 million euros. Outpatient health care institutions, with a 22% share of
expenditure, are the next group of service providers in the list; their expenditure amounted 289
million euros. Retailers of medical goods, who exceeded the expenditure of outpatient health care
institutions in 2014, were the third largest group this year with a 21% share of health expenditure
among service providers; their expenditure made up 275 million euros. The majority of retailers of
medical goods are pharmacies.
Figure 2.1. Distribution of health expenditure by service providers, 2015
During 2009–2015, there were no major changes in the distribution of expenditure by service
providers, although the expenditure of all service provider groups has increased annually (Figure 2.2).
The share of hospitals has remained 47–48% throughout, 3–4% for nursing care and 21–22% for
outpatient health care providers. Nevertheless, two small steady changes have occurred: the share of
Residential long-term care facilities
4%
Providers of ambulatory health
care 22%
Providers of ancillary services
2%
Retailers and other providers
of medical goods 21%
Providers of preventive care
1%
Providers of health care system
administration and financing
2%
Rest of economy 0%
Rest of the world 1%
Regional Hospitals
24%
Central Hospitals
14%
General Hospitals
6%
Other Hospitals 3%
Hospitals 47%

23
ancillary health services has increased in 2014 and 2015, from one percentage to two percentages,
and the share of retailers of medical goods has decreased from 23% to 21%.
Figure 2.2. Health expenditure by service providers, 2009–2015
Figure 2.3 depicts how big the shares of different services in the health expenditure of 2015 are.
Curative care services (inpatient care, day care and outpatient care) make up the largest group of
health expenditure, a total of 56.1%. Medical goods for outpatient patients (pharmaceuticals,
medical non-durable goods, therapeutic appliances and other medical goods) make up the second
largest group, which formed 21% of health expenditure. The third main service group – ancillary
health services – incorporates laboratory and imaging services, ambulance services, and makes up
11% of health expenditure.
Outpatient care (29%) and inpatient care (23%) made up the largest sections in the curative care
service group (Figure 2.3). In the group of medical goods, the largest health expenditure section was
made up by prescribed medicines (14%), the share of over-the-counter medicines remained under
4% and the share of therapeutic appliances was under 3%. The share of various prevention activities
made up 3% of health expenditure.
445 442 459 495 541 586 623
28 29 30 31
42 47
51 199 197 210
227 246
255 289
13 13 13 13
15 20
23
210 218 222
242
257 262
275
0
200
400
600
800
1 000
1 200
1 400
2009 2010 2011 2012 2013 2014 2015
Mill
ion
eu
ros
Rest of the world (HP.9)
Rest of economy (HP.8)
Providers of health care system administration and financing (HP.7) Providers of preventive care (HP.6)
Retailers and other providers of medical goods (HP.5) Providers of ancillary services (HP.4) Providers of ambulatory health care (HP.3) Residential long-term care facilities (HP.2) Hospitals (HP.1)

24
Figure 2.3. Division of health expenditure by services, 2015
When observing health expenditure by service groups during 2009–2015 (Figure 2.4), it initially
appears that after the regression in 2010, the annual 8% growth, starting from 2012, has been
divided between different services relatively evenly. When compared to 2014, the expenditure of
nearly all services increased in 2015, only the expenditure on outpatient rehabilitation care
decreased by 7%. However, the service expenditure increase has been different across services. The
increase of inpatient care expenditure (by 5%) was smaller than the general increase, and with it
continued the decrease of the share of inpatient care. In 2015, expenditure on ancillary health
services (13%), nursing care (12%) and day care (11%) increased above average. When the
expenditure of outpatient care increased by 11%, it included an increase of basic medical and
diagnostic services, i.e. primarily family doctor services by 14%, dental care increased by 11%, and
specialised outpatient medical care increased by 5%.
In short, the most significant changes in the expenditure of health services over the past three years
have been the following:
in 2013, increase in expenditure of specialised outpatient medical care, dental care, day care,
rehabilitation care and nursing care, and decrease of rehabilitation activities;
in 2014, increase in expenditure of day care, nursing care, rehabilitation care and prevention
activities, and decrease of patient transportation and therapeutic appliances;
in 2015, increase in expenditure of family physician care, nursing care, day care and dental
care, ambulance and imaging services (from among ancillary health services), prevention
activities, and decrease of rehabilitation care.
Ambulatory care 29%
Inpatient curative care 23%
Day curative care 3%
Home-based curative care
0%
Long-term care 6%
Rehabilitative care 2%
Laboratory services 5%
Imaging services 3%
Patient transportation
3%
Prescribed medicines
13%
Over-the-counter medicines
4%
Therapeutic appliances
3%
Medical non-durable goods
1%
Preventive care 3%
Governance and Health system and financing
administration 2%

25
Figure 2.4. Health expenditure by service groups, 2009–2015
During 2009–2015, the share of curative care in health expenditure has remained 55–56%. Figure 2.5
illustrates the changes that took place in the structure of curative care expenditure by services during
2009–2015. The share of inpatient care in curative care has decreased significantly. In 2009, the
share of inpatient care in curative care was 48%, whereas in 2015 that indicator was considerably
lower – 42%. The share of specialised outpatient medical care increased from 9% to 11%, the share
of dental care increased from 14% to 16% and the share of day care increased from 4% to 5%.
Figure 2.5. Curative care expenditure by service groups, 2009–2015
518 513 532 574 628 683 740
44 45 45 49
57 66
75
88 88 98 106
116 126
142
210 218 222
242
257
262
275
28 32 32
36
34
37
42
0
200
400
600
800
1 000
1 200
1 400
2009 2010 2011 2012 2013 2014 2015
Mill
ion
eu
ros
Health system administration (HC.7)
Preventive care (HC.6)
Pharmaceuticals and medical goods (HC.5)
Ancillary services (HC.4)
Long-term care (HC.3)
Rehabilitative care (HC.2)
Curative care (HC.1)
48 47 47 46 44 43 42
4 4 4 4 4 5 5
25 25 26 25 25 23 25
14 14 14 14 16 16 16
9 10 9 10 11 13 11
0%
20%
40%
60%
80%
100%
2009 2010 2011 2012 2013 2014 2015
Home-based care (HC.1.4)
Specialised outpatient care (HC.1.3.3)
Dental care (HC.1.3.2)
General outpatient care (HC.1.3.1)
Day care (HC.1.2)
Inpatient curative care (HC.1.1)

26
When comparing Estonian health expenditure structure by services to that of other European
countries, there are countries in which the expenditure of inpatient care exceeds that of outpatient
care, as well as countries in which inpatient care and outpatient care make up equal parts in health
expenditure (Figure 2.6). In the European Union, on average, 30% of health expenditure goes to both
inpatient and outpatient care.
Figure 2.6. Division of health expenditure by services, 2014
1. Includes rehabilitation care at hospitals and day care at institutions
2. Includes home-based curative care and ancillary health services as well
Source: http://www.oecd.org/health/health-at-a-glance-europe-23056088.htm
Estonia is among the countries where the share of outpatient care exceeds that of inpatient care.
There are major difference between countries when it comes to the division of health expenditure
between long-term care and medical goods. Estonia stands out with the small share of long-term
care expenditure in health expenditure. We are closer to the EU average when it comes to medical
goods and inpatient care. There are relatively small differences between countries when we observe
collective services (prevention, administration of health care). Differences between countries are in
part caused by different organisation of health care systems, as well as different accounting or data
collection methods.
41 39 36 35 34 33 33 32 30 30 30 29 29 29 29 29 28 28 28 28 28 27 27 26 26 23 23 19 31 29 27
22 17
17
31 28 26 32
44
26 30 30 24 27 29 29 31
24 30 31
40 33 36 34
48 38
36 34 39
30 28 34
2
2
6 15 12
9
3
22 10 15 25
9 4 14
23
27 18 5
6
18 24 2
9
3
26 12
20 28 19
31 37 43
23 17
20 20
19 14
23 19 16
31 33 20
11 12 15
35
21 30
15 10
20 22
32
12
20
15 11 13
5 5 4 5 6 8 6 2 7 7 7 6 4 5 8 7 9 9 6 5 4 5 5 4 5 7 5 9
4 4 6
0
10
20
30
40
50
60
70
80
90
100
%
Inpatient care¹ Outpatient care² Long-term care Medical goods Collective services

27
3. HEALTH EXPENDITURE PER CAPITA
We can get a better overview of expenditure incurred during 2009–2015, if we do not focus on the
total sum, but expenditure per person in euros.
If we divide the health expenditure of all financing schemes with the number of inhabitants in
Estonia, we get the result that 1,006 euros was invested into the health per one person in Estonia in
2015; as that is the average sum, to the extent of which each person received health care services.
Every person used on average for inpatient care approximately 237 euros, for prescribed medicines
136 euros and for family physician services 143 euros (Figure 3.1).
Figure 3.1. Health expenditure per capita by services, 2009–2015, euros
By 2015, when compared to 2009, the expenditure on day care per person increased the most (1.8
times), expenditure on nursing care and dental care increased by 1.7 times. The smallest increase
185 183 187 200 209 225 237
105 109 110 119 123 130 136 99 96 103
110 119 117 143
66 66 74 80
88 96
108
51 53 53 61
73 95
93
53 53 58 62
75 81
90
33 34 34
37
43
50
57
0 €
100 €
200 €
300 €
400 €
500 €
600 €
700 €
800 €
900 €
1 000 €
2009 2010 2011 2012 2013 2014 2015
Inpatient curative care (HC.1.1) Prescribed medicines (HC.5.1.1)
General outpatient care (HC.1.3.1) Ancillary services (HC.4)
Day care (HC.1.2) and specialised outpatient care (HC.1.3.3)
Dental care (HC.1.3.2)
Long-term care (HC.3) Over-the-counter medicines (HC.5.1.2)
Other medical goods (other HC.5) Preventive care (HC.6)
Health system administration (HC.7) Rehabilitative care (HC.2)
Total 692€ 698€ 729€ 788€ 861€ 929€ 1 006€

28
occurred in inpatient care, prescribed medicines, over-the-counter medicines and in administration
of health care (1.3 times).
The average health expenditure per person is significantly higher than that of households, i.e. the
people’s own expenditure on health services. As previously mentioned, the services in the case of
which the share of the public sector is smaller in financing made up a larger share in households’
expenditure.
On average, every person spent 229 euros on various health services and goods in 2015. In 2014, that
figure was 211 euros. In 2015, the highest expenditure of households went to dental care (66 euros),
the next in line were prescribed medicines (49 euros) and over-the-counter medicines (37 euros), the
total for other services was 77 euros (Figure 3.2).
Figure 3.2. Households’ health expenditure per capita, 2009–2015, euros
Household expenditure per person had by 2015, when compared to 2009, increased the most in
nursing care, dental care and for other medical goods besides medicines (increased about 2 times);
the slowest expenditure increase occurred concerning rehabilitation care and medicines (1.2 times
and 1.3 times respectively).
One indicator for health expenditure level in different countries is health expenditure per person. As
countries have different wage and price levels, international comparisons of health expenditure
implement comparable price level per person on the basis of purchasing power parity (PPP). This is
35 36 40 44 54 58 66
38 41 41 44 45 46
49 27 27 28 31
33 35 37
17 24 20
21 27
29 33
11 12 13
15
17 18
20
9 10 10
11
13 17
19
0 €
50 €
100 €
150 €
200 €
250 €
2009 2010 2011 2012 2013 2014 2015
Dental care (HC.1.3.2) Prescribed medicines (HC.5.1.1)
Over-the-counter medicines (HC.5.1.2) Curative care excl. dental care (other HC.1)
Other medical goods (other HC.5) Long-term care (HC.3)
Rehabilitative care (HC.2) Ancillary services (HC.4)
Total 141€ 153€ 157€ 170€ 195€ 211€ 229€

29
why the Estonian numbers indicated in the comparison of countries differ from those included in the
previous figure. At figure 3.3 is used euro PPP, as European countries are compared. Estonia is
among the group of countries with the lowest expenditure, along with Hungary, Lithuania and
Poland. Therefore, the sum spent on health care per person in Estonia is 2.1 times smaller than the
average in the European Union. The comparability of health expenditure between countries may be
influenced by differences in the coverage of long-term care services and division into health and
social costs.
Figure 3.3. Health expenditure per person, 2015, EUR PPP
1. Includes investments.
2. OECD estimate.
3. In the case of Luxembourg, total population only includes permanent residents who have health insurance, so that
number is smaller than the actual total population.
Source: http://www.oecd.org/health/health-at-a-glance-europe-23056088.htm
Health expenditure characterises the health care system’s expenditure on health, yet this is an
investment into improving and maintaining people’s health. The goal of health systems performance
is not just in the provision of necessary health care services, but to provide these services in a way
that benefits health the most. Health expenses should be viewed alongside with achieved results in
health (better health, improved quality of life, higher satisfaction levels) and not evaluate the
performance based on the volume of services provided (i.e. quantity) only. Better health and a
healthier population are also the basis for economic growth.
6 0
23
4 0
03
3 9
83
3 9
37
3 9
22
3 7
89
3 7
73
3 4
81
3 3
42
3 0
84
2 9
88
2 7
81
2 4
76
2 4
49
2 3
66
1 9
83
1 9
67
1 8
50
1 6
63
1 5
76
1 5
39
1 3
71
1 3
64
1 3
48
1 2
59
1 1
09
1 1
08
1 0
30
81
6
5 3
54
4 6
81
3 1
26
0
1 000
2 000
3 000
4 000
5 000
6 000
Private/voluntary Government/compulsory
EUR

30
4. ACCOUNTING METHODOLOGY OF HEALTH
EXPENDITURE
Estonia has implemented the methodology of SHA2011 for calculating health expenditure since
2013.
This methodology is a common further development of OECD-WHO-Eurostat methodology of SHA1.0
implemented earlier and used for the data compilation of 2000–2012 health expenditure in Estonia.
This is an internationally standardised framework, which is used for systematic evaluation of national
health expenditure of countries in a comparable way.
The objective for the development of the new SHA2011 methodology was to make the data of
different countries more comparable. To the countries are provided more specific instructions for
classifying health expenses and the methodology is used by the member states of the corresponding
international organisations in calculating health expenditure. Classifications used for accounting –
health care providers (ICHA-HP), health care financing schemes (ICHA-HF), health care functions
(ICHA-HC), revenues of health care financing schemes (ICHA-FS), gross fixed capital formation in
health system by type of asset (ICHA-HK) and factors of health care provision (ICHA-FP) – have been
published together with explanations on the website of the National Institute for Health
Development in Estonian:
http://www.tai.ee/et/tegevused/tervisestatistika/metaandmed/klassifikaatorid.
The use of SHA2011 is mandatory for all EU Member States from the reference year of 2014, and the
submission of data takes place on the basis of the implementing regulation of the European
Commission 2015/359, available at: http://eur-lex.europa.eu/eli/reg/2015/359/oj
The main conceptual difference between the two methodologies is that gross fixed capital formation
in health is no longer part of health expenditure, and has been excluded from health expenditure.
Based on SHA1.0 capital investments was included into total health expenditure.
Another significant change took place in the classification of external financing. According to SHA1.0,
expenditure from foreign financing sources was always classified under the Rest of the world.
SHA2011 classifies expenditure, which is administered by national structural unit, under the financing
scheme of the corresponding structural unit. For example, externally financed projects of the
Ministry of Social Affairs, where the latter is responsible for the organisation of projects, are shown
under the financing schemes of public sector (HF.1). Only amounts directly from abroad received
financing to the service providers, without any intermediation from Estonia, will be shown inside the
rest of the world financing schemes (HF.4). In the new table of the revenues of health care financing
schemes (FS) shows income used for financing health expenditure according to their sources;
including direct receipts from abroad, in the subdivision FS.7.
All data necessary for the compilation of health expenditure has been collected generally through the
organisers of financing (Estonian Health Insurance Fund, state budget, ministries, private insurance
companies, etc.). The data are verified and if necessary, specified together with the data providers
and all made expenses are classified according to the function (purpose) for which the money was
spent.

31
During the work, it will be specified as much as possible through which service provider money was
spent for the corresponding purpose, and where final consumption took place. Since the objective is
to classify expenditure according to final consumption (and exclude intermediate consumption), then
the contributor is often not the one, which carries out the corresponding activity or where the
money is actually spent – therefore, the data obtained through organisers will be further classified
according to the corresponding service providers and activities. In practice, classification means
marking each amount spent according to all applicable classifications (financing source, health
function, service provider, and financing scheme). Expenditure where the primary proposes of the
activity is not health, or related to health and health care indirectly will be excluded. Therefore, the
labour and social field expenditure of the Ministry of Social Affairs is not included. Neither does
health expenditure include compensations for the temporary incapacity to work paid by the EHIF.
In the calculation of the household health expenditure, the main basis consist of the data of the
health service providers from the statistical reports of the National Institute for Health Development
on health statistics: on the volumes of the services provided and revenue received from persons
(individuals) payments. In case of medical goods (including pharmaceuticals), the data is based on
the statistics obtained from various sources. The methodology of calculation of household health
expenditure has been described in detail in the publication Health Expenditure 2014:
http://www.tai.ee/en/health-data/research-reports/download/366.
The data for the calculation of health expenditure has been derived from the following sources. The
data has been collected both on pre-determined standard forms and in a free-format. Additionally,
statistics on different services and expenses that have been made publicly available on websites have
also been used.
List of data sources:
1. Estonian Health Insurance Fund – expenditure on health insurance benefits (services and goods, prevention).
2. Ministry of Finance – 2015 annual statement on local government budget implementation. 3. Health expenditure on ministries and their divisions: Ministry of Education and Research,
Ministry of Justice, Ministry of Defence, Ministry of the Environment, Ministry of Economic Affairs and Communications, Ministry of Rural Affairs, Ministry of Finance, Ministry of the Interior, and Ministry of Foreign Affairs.
4. Data on health expenditure from insurance companies operating in Estonia. 5. State Agency of Medicines – turnover of pharmaceuticals in hospital and retail pharmacies. 6. Institutions of occupational health – statistics on mandatory medical examinations of employees. 7. Statistics Estonia – health expenses (incl. occupational health) of companies; population;
indicators of national accounts. 8. Estonian E-Health Foundation – expenditure on developing the e-solutions of the national health
system. 9. Data on health expenditure from the Health Board and the State Agency of Medicines. 10. Departments of the Ministry of Social Affairs:
a. Department of Finance and Asset Management – specified data on medical treatment
expenses of uninsured persons, foreign aid projects, foreign loans; health projects financed
through the Ministry of Finance from gambling tax; expenditure on purchased services,
infertility treatment expenditure. 2015 State Budget Execution Report is the source of data
on the health expenditure of the Ministry of Social Affairs administrative area.

32
b. Department of Analysis and Statistics – institutional reporting on social welfare. 11. National Institute for Health Development – health promotion projects and programmes and
statistical reports: a. Health care providers' economic activity b. Physicians’ consultations and home visits c. Day care d. Hospital beds and hospitalisation e. Dental care report
12. Estonian Red Cross – health expenses. 13. Annual reports of the Commercial (Business) Register – for clarifying information of health
service providers who are licensed by the Health Board. 14. SA Hille Tänavsuu Vähiravifond Kingitud Elu (The cancer treatment foundation "The Gift of Life")
– news about financing cancer treatment and data about the takeover by the Estonian Health Insurance Fund.

33
REFERENCE MATERIAL
Estonian Health Insurance Fund – website, annual report
https://www.haigekassa.ee/en/organisation
https://www.haigekassa.ee/en/annual-reports
Website of the Ministry of Social Affairs
https://www.sm.ee/en
State Agency of Medicines – sales statistics of pharmaceuticals
http://www.ravimiamet.ee/en/statistics-medicines
Database of Statistics Estonia – economy and population
http://pub.stat.ee/px-web.2001/I_Databas/Economy/databasetree.asp
http://pub.stat.ee/px-web.2001/I_Databas/Population/databasetree.asp
Health statistics and health research database of the National Institute for Health Development
http://pxweb.tai.ee/PXWeb2015/index_en.html
Website of the Department of Health Statistics of the National Institute for Health Development
http://www.tai.ee/en/r-and-d/health-statistics
Health expenditure methodology 2013 of the National Institute for Health Development, 2014
http://www.tai.ee/en/health-data/research-reports/download/339
Database of Eurostat (the statistical office of the European Union)
http://ec.europa.eu/eurostat/data/database
Database of the World Health Organization
http://www.euro.who.int/en/data-and-evidence/databases
Database of the Organisation for Economic Cooperation and Development (OECD)
http://www.oecd.org/health/health-data.htm

Health and health care statistics:
• Health statistics and health research databasehttp://www.tai.ee/tstua
• Website of Health Statistics Department of National Institute for Health Developmenthttp://www.tai.ee/en/r-and-d/health-statistics/activities
• Dataquery to National Institute for Health [email protected]
• Database of Statistics Estoniahttp://www.stat.ee/en
• Statistics of European Unionhttp://ec.europa.eu/eurostat
• European health for all database (HFA-DB)http://data.euro.who.int/hfadb/
• OECD’s statistical databases (OECD.Stat)http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT