Embed Size (px)
Citation preview

1
STATE OF CONNECTICUT
OFFICE OF THE HEALTHCARE ADVOCATE
STATE INNOVATION MODEL PROGRAM MANAGEMENT OFFICE
REQUEST FOR PROPOSALS (RFP)
HEALTH ENHANCEMENT COMMUNITY CONSULTATION
The State Innovation Model (SIM) Program Management Office seeks consultation services to support
the State in planning for a new Health Enhancement Community initiative as part of Connecticutrsquos
broader SIM strategy The consultant(s) selected through this Request for Proposals (RFP) will provide
subject matter expertise strategic planning design development actuarial analysis and stakeholder
facilitation to support the creation of the HEC model and implementation approach The Health
Enhancement Community model will foster community-wide multi-sector collaboration and
accountability to promote healthier people better care smarter spending and health equity
This is a competitive procurement for one or more contracts of approximately seven months duration
Preference is given to proposals with a single point of accountability However the state welcomes
proposals from either a) a single bidder demonstrating the capacity to undertake all five objectives b)
a partnership between a principal bidder and subcontracted consultants or c) multiple bidders
responding to a subset of the objectives The anticipated combined maximum award is $12 million
The resulting contract may contain an option to renew at the Statersquos discretion to support additional
planning financial analysis or technical assistance
httpwwwbiznetctgovSCP_SearchBidResultsaspx
Applicable Dates
RFP Release Date 102017
Letter of Intent to Apply (optional) Due Date 11317
Application Due Date 120117 1pm Eastern Time
Anticipated Issuance of Notice of Award 121517
Anticipated Period of Performance 1118 ndash 73118
2
TABLE OF CONTENTS 1 EXECUTIVE SUMMARY 4
2 BACKGROUND INFORMATION 5
21 Connecticutrsquos State Innovation Model 5
22 Health Enhancement Community Initiative 7
3 REQUIRED SCOPE OF WORK AND QUALIFICATIONS 10
31 Scope of Work 10
32 Qualifications Error Bookmark not defined
33 Key Outputs And Timeline Error Bookmark not defined
4 AWARD INFORMATION Error Bookmark not defined
41 Award Amount Error Bookmark not defined
42 Eligibility Information Error Bookmark not defined
43 Period of Performance Error Bookmark not defined
44 Termination of Award Error Bookmark not defined
45 Issuing Office and Contract Administration Error Bookmark not defined
46 Official Contact Error Bookmark not defined
5 APPLICATION DETAILS Error Bookmark not defined
51 Submission Instructions Error Bookmark not defined
511 Letter of Intent to Apply Error Bookmark not defined
512 Respondentsrsquo Questions Error Bookmark not defined
513 Submission Requirements Error Bookmark not defined
514 Format Requirements Error Bookmark not defined
52 Application Content Error Bookmark not defined
6 EVALUATION AND SELECTION Error Bookmark not defined
61 Evaluation Criteria Error Bookmark not defined
62 Review and Selection Process Error Bookmark not defined
63 Procurement Process Error Bookmark not defined
631 Contract Execution Error Bookmark not defined
632 Acceptance of Content Error Bookmark not defined
633 Debriefing Error Bookmark not defined
634 Appeal Process Error Bookmark not defined
3
635 Contest of Solicitation of Award Error Bookmark not defined
636 Disposition of Responses- Rights Reserved Error Bookmark not defined
637 Qualification Preparation Expenses Error Bookmark not defined
638 Response Date and Time Error Bookmark not defined
639 Assurances and Acceptances Error Bookmark not defined
6310 Incurring Costs Error Bookmark not defined
6311 Statutory and Regulatory Compliance Error Bookmark not defined
6312 Key Personnel Error Bookmark not defined
6313 Other Error Bookmark not defined
7 DEFINITIONS AND ACRONYMS Error Bookmark not defined
Attachment A Proposal Face Sheet Error Bookmark not defined
Attachment B Procurement And Contractual Agreements Signatory AcceptanceError Bookmark not defined
4
1 EXECUTIVE SUMMARY The Health Enhancement Community (HEC) initiative is part of Connecticutrsquos comprehensive SIM strategy to promote healthier people better care smarter spending and health equity The consultant selected through this Request for Proposals (RFP) will provide subject matter expertise strategic planning design development actuarial analysis and stakeholder facilitation to support the creation of the HEC model and implementation approach
For the purpose of this RFP the state has established the following provisional definition
A Health Enhancement Community is accountable for health health equity and related costs for all
residents in a geographic area uses data community engagement and cross sector activities to identify
and address root causes and operates in an economic environment that sustainably funds and rewards
such activities by capturing the economic value of improved health
Any questions related to this grant program should be directed to
Faina Dookh
Fainadookhctgov
Applications must be submitted electronically on or before the date indicated below to
Fainadookhctgov
RFP Name Health Enhancement Community Consultation
RFP Release Date October 20 2017
Electronic Location of Request for Proposals httpwwwbiznetctgovSCP_SearchBidResultsaspx
Letter of Intent (optional) Due Date November 3 2017
Request for Proposals Application Due Date December 1 2017 at 1pm
Anticipated Notice of Award December 15 2017
Period of Award January 1 2018 ndash July 31 2018
Anticipated Total Available Funding $12 million
Anticipated Number of Awards One or two awards
Eligible Applicants
Consultants with expertise in operational and
strategic planning facilitation cross-sector
community health improvement stakeholder
engagement actuarial and health economic
modeling and payment reform
5
2 BACKGROUND INFORMATION
21 CONNECTICUTrsquoS STATE INNOVATION MODEL
The State Innovation Model (SIM) initiative is a Center for Medicare amp Medicaid Innovation (CMMI) effort to
support the development and implementation of state-led multi-payer healthcare payment and service
delivery model reforms that will promote
healthier people better care and smarter
spending in participating states In 2014
Connecticut received a $45 million State
Innovation Model (SIM) grant from CMMI to
implement a multi-faceted strategy to improve
the health outcomes and healthcare spending
trajectory of the state as well as to improve
the sizeable health disparities that continue to
persist Over a four-year period (2015-2019)
Connecticutrsquos SIM proposes to improve
Connecticutrsquos health system for the majority of
residents
We are investing in a transition away from
paying for a volume of healthcare services
towards paying based on whether people receive high quality care with lower growth in costs This includes
funding the design and launch of the statersquos first Medicaid Shared Savings Program (ldquoPCMH+rdquo) which rewards
healthcare providers for improved quality outcomes and better cost trends
We are providing technical assistance and supports to healthcare providers that want to succeed in these new
payment models so that they can connect individuals to community and behavioral supports deploy
community health workers use data to track and improve their performance and more Providers access these
resources through our Advanced Medical Home and Community amp Clinical Integration Programs
Simultaneously we engage consumers by promoting insurance plans that remove financial barriers to or
introduce rewards for preventive care medication adherence chronic disease management and high-quality
provider selection We promote these ldquoValue-Based Insurance Designsrdquo by convening employers and creating
easily adoptable templates and disseminating best-practices
Lastly we are developing and testing components of a Population Health Plan which is to be completed and
implemented before the end of the SIM test grant period This longer-term strategy will combine innovations
in clinical healthcare delivery payment reform and population health strategies to improve health as a
community approach rather than one focused solely on patient panels
6
Over the last year the population health planning efforts have focused on designing and launching the
Prevention Service Initiative (PSI) This initiative aims to increase the number of contracts between CBOs and
ACOs for diabetes and asthma self-management programs by providing technical assistance
The State is now turning its attention to developing and implementing the Health Enhancement Community
Initiative This initiative is our most ambitious project under this population health effort
Connecticutrsquos SIM moves Connecticutrsquos health care system along a path of transformation The HEC model is
intended to build on and extend many of the current SIM investments and aims See the diagram below which
aligns with Neal Halfonrsquos Transformation Framework1 particularly the highlighted sections which articulate
much of what we are seeking to solve for in the HEC planning process The next section provides the context
for the HEC initiative
Please also note the following regarding Connecticut-specific public health and community related information
Community Health Collaborative scan 2017 Population Health Council Environmental Scan CT Prevention
Programs NCD Policy Scan CT Community Health Needs Assessments
1 See highlighted sections of Halfon (2014) report
7
22 HEALTH ENHANCEMENT COMMUNITY INITIATIVE Connecticutrsquos State Innovation Model is implementing a range of care delivery and payment reforms to
improve health care and slow the growth of healthcare spending However taken alone these are not
enough to make Connecticut a place where preventable deaths diseases and health disparities are
eliminated and every person enjoys the best health possible To achieve these ambitious goals
Connecticutrsquos SIM will partner with communities to design a Health Enhancement Community initiative
that moves beyond treating illness to address root causes behavior and social determinants of health
Connecticut is proposing to create the conditions that promote and sustain cross-sector community-led
strategies focused on prevention A provisional definition to begin the planning process was developed
A Health Enhancement Community is accountable for health health equity and related costs for
all residents in a geographic area uses data community engagement and cross sector activities
to identify and address root causes and operates in an economic environment that sustainably
funds and rewards such activities by capturing the economic value of improved health
Many components of the HEC definition are intentionally undefined in order to accommodate a
thoughtful community-driven planning process
More Needs to be Done to Shift the Focus to Prevention
More than half of all Americans suffer from one or more chronic diseases and obesity a precursor to
many chronic diseases is contributing to lower life expectancy Health disparities around chronic
conditions also persistmdashpeople of color face higher rates of diabetes obesity stroke heart disease and
cancer A study by the Milken Institute calculated that seven chronic conditions are costing the US
economy more than $1 trillion per year In fact chronic conditions drive 96 of Medicare costs and 83
of Medicaid costs and are responsible for two thirds of the rise in overall healthcare costs since 1980
Despite the fact that 40 of cancer 80 of heart disease and 80 of type 2 diabetes are preventable
the rates and costs of chronic conditions are predicted to continue to rise significantly over the coming
years
Bringing Everyone to the Table
Preventing chronic disease is beyond the reach of any one
sector of the community Inadequate healthcare for example
contributes about 10 to a personrsquos chances of dying
prematurely Moreover prevention in healthcare is difficult in
the current ldquosick carerdquo system Even in the most advanced
alternative payment models preventing chronic disease is not
rewarded
Health behaviors such as smoking and diet and exercise are the
most important determinants contributing 40 to the risk of
Proportional Contribution to Premature Death
8
premature death Improving health also depends heavily on addressing the non-behavioral determinants
of healthndash the conditions in which people are born grow work live and age
Working together the business municipal educational social service public health and healthcare
sectors can influence both behavior and the social determinants of health Local organizations and
community members themselves know best what the challenges are of their communities and how to
approach them
Research validates that preventable deaths have been reduced when comprehensive multi-sector
networks undertake health improvement initiatives National efforts have also emphasized cross-sector
initiatives For example Accountable Communities for Health (ACH) (eg CHCS report NASHP report) are
coming to the forefront in many states National efforts such as REACH have been shown to make an
impact on health equity In Connecticut important local collective efforts are occurring that are forming
the foundation for planning HECs including multi-sector collaboratives to identify and prioritize the most
pressing health needs in a community2
Why Setting the Table is Not Enough
Despite increased awareness of health disparities and a broad range of societal efforts to improve the
health of populations little progress has been made in reducing social gaps in health3 In fact current
Accountable Communities for Health (ACH) models often do not focus on upstream prevention that can
lead to broad improvements in health and health equity Several of the biggest challenges to ACH models
around the country include data and measurement infrastructure clear governance schemes and the
lack of long term financial sustainability
The State can play a critical role in supporting communities and facilitating solutions to these challenges
Bringing stakeholders together without addressing such barriers that prevent communities from fully
enacting and sustaining a prevention strategy is not likely to curb the rising rates of chronic disease For
example the State can 1) assist communities to establish a framework for measurement and
accountability 2) support the development of local multi-stakeholder alignments and locally tailored
governance structures and 3) solve for financial sustainability by defining demonstrating and capturing
the value of improved health due to prevention and create conditions that attract investments and
innovations in prevention4 Financial sustainability solutions may include but are not limited to market-
oriented-solutions public-private partnerships in financing or development of wellness trusts
2 Community Solutions initiative in N Hartford The Vita Health and Wellness District in Stamford Healthier Greater New Haven Partnership Primary Care Action Group in Bridgeport coalitions to complete Community Health Needs Assessments and others 3 Williams DR Costa MV Odunlami AO and Mohammed SA Moving Upstream How Interventions that Address the Social Determinants of Health can Improve Health and Reduce Disparities J Public Health Manag Pract 2008 14(Suppl)S8-17 4 See Appendix 1 page 51 httpswwwsurgeongeneralgovprioritiespreventionstrategyreportpdf
9
SIM Governance
The planning and execution of the HEC initiative will be done through extensive engagement with a broad
array of people and sectors inside and outside of government and in communities The Lieutenant
Governor provides overall leadership and oversight for SIM The SIM initiative is executed in collaboration
with multiple agencies and organizations including the Department of Public Health the Department of
Social Services the Office of the State Comptroller Access Health CT UConn Health and others The SIM
PMO within the Office of the Healthcare Advocate is leading the implementation of SIM The PMO
coordinates activities across work streams engages stakeholders manages vendors executes care
delivery reform initiatives and communicates progress to the public
The PMO engages more than 150 stakeholders through a number of advisory councils that focus on
particular components of SIM such as quality measurement practice transformation value-based
insurance design and population health These councils are comprised of consumers employers
healthcare providers community organizations and subject matter experts The Population Health
Council will play a key advisory role for the HEC initiative and will be engaged throughout the planning
and implementation process Over the past year the Population Health Council has advised on the
development of the Prevention Service Initiative It will now change its focus to advise primarily on the
HEC initiative Councils make their recommendations to the Healthcare Innovation Steering Committee
(HISC) which provides key guidance on the direction of SIM The HISC will also be actively engaged as part
of the HEC initiative
The HEC initiative and planning efforts are being jointly administered by both the PMO and DPH The two
parties will also jointly direct the contract(s) resulting from this procurement
10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative
2
TABLE OF CONTENTS 1 EXECUTIVE SUMMARY 4
2 BACKGROUND INFORMATION 5
21 Connecticutrsquos State Innovation Model 5
22 Health Enhancement Community Initiative 7
3 REQUIRED SCOPE OF WORK AND QUALIFICATIONS 10
31 Scope of Work 10
32 Qualifications Error Bookmark not defined
33 Key Outputs And Timeline Error Bookmark not defined
4 AWARD INFORMATION Error Bookmark not defined
41 Award Amount Error Bookmark not defined
42 Eligibility Information Error Bookmark not defined
43 Period of Performance Error Bookmark not defined
44 Termination of Award Error Bookmark not defined
45 Issuing Office and Contract Administration Error Bookmark not defined
46 Official Contact Error Bookmark not defined
5 APPLICATION DETAILS Error Bookmark not defined
51 Submission Instructions Error Bookmark not defined
511 Letter of Intent to Apply Error Bookmark not defined
512 Respondentsrsquo Questions Error Bookmark not defined
513 Submission Requirements Error Bookmark not defined
514 Format Requirements Error Bookmark not defined
52 Application Content Error Bookmark not defined
6 EVALUATION AND SELECTION Error Bookmark not defined
61 Evaluation Criteria Error Bookmark not defined
62 Review and Selection Process Error Bookmark not defined
63 Procurement Process Error Bookmark not defined
631 Contract Execution Error Bookmark not defined
632 Acceptance of Content Error Bookmark not defined
633 Debriefing Error Bookmark not defined
634 Appeal Process Error Bookmark not defined
3
635 Contest of Solicitation of Award Error Bookmark not defined
636 Disposition of Responses- Rights Reserved Error Bookmark not defined
637 Qualification Preparation Expenses Error Bookmark not defined
638 Response Date and Time Error Bookmark not defined
639 Assurances and Acceptances Error Bookmark not defined
6310 Incurring Costs Error Bookmark not defined
6311 Statutory and Regulatory Compliance Error Bookmark not defined
6312 Key Personnel Error Bookmark not defined
6313 Other Error Bookmark not defined
7 DEFINITIONS AND ACRONYMS Error Bookmark not defined
Attachment A Proposal Face Sheet Error Bookmark not defined
Attachment B Procurement And Contractual Agreements Signatory AcceptanceError Bookmark not defined
4
1 EXECUTIVE SUMMARY The Health Enhancement Community (HEC) initiative is part of Connecticutrsquos comprehensive SIM strategy to promote healthier people better care smarter spending and health equity The consultant selected through this Request for Proposals (RFP) will provide subject matter expertise strategic planning design development actuarial analysis and stakeholder facilitation to support the creation of the HEC model and implementation approach
For the purpose of this RFP the state has established the following provisional definition
A Health Enhancement Community is accountable for health health equity and related costs for all
residents in a geographic area uses data community engagement and cross sector activities to identify
and address root causes and operates in an economic environment that sustainably funds and rewards
such activities by capturing the economic value of improved health
Any questions related to this grant program should be directed to
Faina Dookh
Fainadookhctgov
Applications must be submitted electronically on or before the date indicated below to
Fainadookhctgov
RFP Name Health Enhancement Community Consultation
RFP Release Date October 20 2017
Electronic Location of Request for Proposals httpwwwbiznetctgovSCP_SearchBidResultsaspx
Letter of Intent (optional) Due Date November 3 2017
Request for Proposals Application Due Date December 1 2017 at 1pm
Anticipated Notice of Award December 15 2017
Period of Award January 1 2018 ndash July 31 2018
Anticipated Total Available Funding $12 million
Anticipated Number of Awards One or two awards
Eligible Applicants
Consultants with expertise in operational and
strategic planning facilitation cross-sector
community health improvement stakeholder
engagement actuarial and health economic
modeling and payment reform
5
2 BACKGROUND INFORMATION
21 CONNECTICUTrsquoS STATE INNOVATION MODEL
The State Innovation Model (SIM) initiative is a Center for Medicare amp Medicaid Innovation (CMMI) effort to
support the development and implementation of state-led multi-payer healthcare payment and service
delivery model reforms that will promote
healthier people better care and smarter
spending in participating states In 2014
Connecticut received a $45 million State
Innovation Model (SIM) grant from CMMI to
implement a multi-faceted strategy to improve
the health outcomes and healthcare spending
trajectory of the state as well as to improve
the sizeable health disparities that continue to
persist Over a four-year period (2015-2019)
Connecticutrsquos SIM proposes to improve
Connecticutrsquos health system for the majority of
residents
We are investing in a transition away from
paying for a volume of healthcare services
towards paying based on whether people receive high quality care with lower growth in costs This includes
funding the design and launch of the statersquos first Medicaid Shared Savings Program (ldquoPCMH+rdquo) which rewards
healthcare providers for improved quality outcomes and better cost trends
We are providing technical assistance and supports to healthcare providers that want to succeed in these new
payment models so that they can connect individuals to community and behavioral supports deploy
community health workers use data to track and improve their performance and more Providers access these
resources through our Advanced Medical Home and Community amp Clinical Integration Programs
Simultaneously we engage consumers by promoting insurance plans that remove financial barriers to or
introduce rewards for preventive care medication adherence chronic disease management and high-quality
provider selection We promote these ldquoValue-Based Insurance Designsrdquo by convening employers and creating
easily adoptable templates and disseminating best-practices
Lastly we are developing and testing components of a Population Health Plan which is to be completed and
implemented before the end of the SIM test grant period This longer-term strategy will combine innovations
in clinical healthcare delivery payment reform and population health strategies to improve health as a
community approach rather than one focused solely on patient panels
6
Over the last year the population health planning efforts have focused on designing and launching the
Prevention Service Initiative (PSI) This initiative aims to increase the number of contracts between CBOs and
ACOs for diabetes and asthma self-management programs by providing technical assistance
The State is now turning its attention to developing and implementing the Health Enhancement Community
Initiative This initiative is our most ambitious project under this population health effort
Connecticutrsquos SIM moves Connecticutrsquos health care system along a path of transformation The HEC model is
intended to build on and extend many of the current SIM investments and aims See the diagram below which
aligns with Neal Halfonrsquos Transformation Framework1 particularly the highlighted sections which articulate
much of what we are seeking to solve for in the HEC planning process The next section provides the context
for the HEC initiative
Please also note the following regarding Connecticut-specific public health and community related information
Community Health Collaborative scan 2017 Population Health Council Environmental Scan CT Prevention
Programs NCD Policy Scan CT Community Health Needs Assessments
1 See highlighted sections of Halfon (2014) report
7
22 HEALTH ENHANCEMENT COMMUNITY INITIATIVE Connecticutrsquos State Innovation Model is implementing a range of care delivery and payment reforms to
improve health care and slow the growth of healthcare spending However taken alone these are not
enough to make Connecticut a place where preventable deaths diseases and health disparities are
eliminated and every person enjoys the best health possible To achieve these ambitious goals
Connecticutrsquos SIM will partner with communities to design a Health Enhancement Community initiative
that moves beyond treating illness to address root causes behavior and social determinants of health
Connecticut is proposing to create the conditions that promote and sustain cross-sector community-led
strategies focused on prevention A provisional definition to begin the planning process was developed
A Health Enhancement Community is accountable for health health equity and related costs for
all residents in a geographic area uses data community engagement and cross sector activities
to identify and address root causes and operates in an economic environment that sustainably
funds and rewards such activities by capturing the economic value of improved health
Many components of the HEC definition are intentionally undefined in order to accommodate a
thoughtful community-driven planning process
More Needs to be Done to Shift the Focus to Prevention
More than half of all Americans suffer from one or more chronic diseases and obesity a precursor to
many chronic diseases is contributing to lower life expectancy Health disparities around chronic
conditions also persistmdashpeople of color face higher rates of diabetes obesity stroke heart disease and
cancer A study by the Milken Institute calculated that seven chronic conditions are costing the US
economy more than $1 trillion per year In fact chronic conditions drive 96 of Medicare costs and 83
of Medicaid costs and are responsible for two thirds of the rise in overall healthcare costs since 1980
Despite the fact that 40 of cancer 80 of heart disease and 80 of type 2 diabetes are preventable
the rates and costs of chronic conditions are predicted to continue to rise significantly over the coming
years
Bringing Everyone to the Table
Preventing chronic disease is beyond the reach of any one
sector of the community Inadequate healthcare for example
contributes about 10 to a personrsquos chances of dying
prematurely Moreover prevention in healthcare is difficult in
the current ldquosick carerdquo system Even in the most advanced
alternative payment models preventing chronic disease is not
rewarded
Health behaviors such as smoking and diet and exercise are the
most important determinants contributing 40 to the risk of
Proportional Contribution to Premature Death
8
premature death Improving health also depends heavily on addressing the non-behavioral determinants
of healthndash the conditions in which people are born grow work live and age
Working together the business municipal educational social service public health and healthcare
sectors can influence both behavior and the social determinants of health Local organizations and
community members themselves know best what the challenges are of their communities and how to
approach them
Research validates that preventable deaths have been reduced when comprehensive multi-sector
networks undertake health improvement initiatives National efforts have also emphasized cross-sector
initiatives For example Accountable Communities for Health (ACH) (eg CHCS report NASHP report) are
coming to the forefront in many states National efforts such as REACH have been shown to make an
impact on health equity In Connecticut important local collective efforts are occurring that are forming
the foundation for planning HECs including multi-sector collaboratives to identify and prioritize the most
pressing health needs in a community2
Why Setting the Table is Not Enough
Despite increased awareness of health disparities and a broad range of societal efforts to improve the
health of populations little progress has been made in reducing social gaps in health3 In fact current
Accountable Communities for Health (ACH) models often do not focus on upstream prevention that can
lead to broad improvements in health and health equity Several of the biggest challenges to ACH models
around the country include data and measurement infrastructure clear governance schemes and the
lack of long term financial sustainability
The State can play a critical role in supporting communities and facilitating solutions to these challenges
Bringing stakeholders together without addressing such barriers that prevent communities from fully
enacting and sustaining a prevention strategy is not likely to curb the rising rates of chronic disease For
example the State can 1) assist communities to establish a framework for measurement and
accountability 2) support the development of local multi-stakeholder alignments and locally tailored
governance structures and 3) solve for financial sustainability by defining demonstrating and capturing
the value of improved health due to prevention and create conditions that attract investments and
innovations in prevention4 Financial sustainability solutions may include but are not limited to market-
oriented-solutions public-private partnerships in financing or development of wellness trusts
2 Community Solutions initiative in N Hartford The Vita Health and Wellness District in Stamford Healthier Greater New Haven Partnership Primary Care Action Group in Bridgeport coalitions to complete Community Health Needs Assessments and others 3 Williams DR Costa MV Odunlami AO and Mohammed SA Moving Upstream How Interventions that Address the Social Determinants of Health can Improve Health and Reduce Disparities J Public Health Manag Pract 2008 14(Suppl)S8-17 4 See Appendix 1 page 51 httpswwwsurgeongeneralgovprioritiespreventionstrategyreportpdf
9
SIM Governance
The planning and execution of the HEC initiative will be done through extensive engagement with a broad
array of people and sectors inside and outside of government and in communities The Lieutenant
Governor provides overall leadership and oversight for SIM The SIM initiative is executed in collaboration
with multiple agencies and organizations including the Department of Public Health the Department of
Social Services the Office of the State Comptroller Access Health CT UConn Health and others The SIM
PMO within the Office of the Healthcare Advocate is leading the implementation of SIM The PMO
coordinates activities across work streams engages stakeholders manages vendors executes care
delivery reform initiatives and communicates progress to the public
The PMO engages more than 150 stakeholders through a number of advisory councils that focus on
particular components of SIM such as quality measurement practice transformation value-based
insurance design and population health These councils are comprised of consumers employers
healthcare providers community organizations and subject matter experts The Population Health
Council will play a key advisory role for the HEC initiative and will be engaged throughout the planning
and implementation process Over the past year the Population Health Council has advised on the
development of the Prevention Service Initiative It will now change its focus to advise primarily on the
HEC initiative Councils make their recommendations to the Healthcare Innovation Steering Committee
(HISC) which provides key guidance on the direction of SIM The HISC will also be actively engaged as part
of the HEC initiative
The HEC initiative and planning efforts are being jointly administered by both the PMO and DPH The two
parties will also jointly direct the contract(s) resulting from this procurement
10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative

3
635 Contest of Solicitation of Award Error Bookmark not defined
636 Disposition of Responses- Rights Reserved Error Bookmark not defined
637 Qualification Preparation Expenses Error Bookmark not defined
638 Response Date and Time Error Bookmark not defined
639 Assurances and Acceptances Error Bookmark not defined
6310 Incurring Costs Error Bookmark not defined
6311 Statutory and Regulatory Compliance Error Bookmark not defined
6312 Key Personnel Error Bookmark not defined
6313 Other Error Bookmark not defined
7 DEFINITIONS AND ACRONYMS Error Bookmark not defined
Attachment A Proposal Face Sheet Error Bookmark not defined
Attachment B Procurement And Contractual Agreements Signatory AcceptanceError Bookmark not defined
4
1 EXECUTIVE SUMMARY The Health Enhancement Community (HEC) initiative is part of Connecticutrsquos comprehensive SIM strategy to promote healthier people better care smarter spending and health equity The consultant selected through this Request for Proposals (RFP) will provide subject matter expertise strategic planning design development actuarial analysis and stakeholder facilitation to support the creation of the HEC model and implementation approach
For the purpose of this RFP the state has established the following provisional definition
A Health Enhancement Community is accountable for health health equity and related costs for all
residents in a geographic area uses data community engagement and cross sector activities to identify
and address root causes and operates in an economic environment that sustainably funds and rewards
such activities by capturing the economic value of improved health
Any questions related to this grant program should be directed to
Faina Dookh
Fainadookhctgov
Applications must be submitted electronically on or before the date indicated below to
Fainadookhctgov
RFP Name Health Enhancement Community Consultation
RFP Release Date October 20 2017
Electronic Location of Request for Proposals httpwwwbiznetctgovSCP_SearchBidResultsaspx
Letter of Intent (optional) Due Date November 3 2017
Request for Proposals Application Due Date December 1 2017 at 1pm
Anticipated Notice of Award December 15 2017
Period of Award January 1 2018 ndash July 31 2018
Anticipated Total Available Funding $12 million
Anticipated Number of Awards One or two awards
Eligible Applicants
Consultants with expertise in operational and
strategic planning facilitation cross-sector
community health improvement stakeholder
engagement actuarial and health economic
modeling and payment reform
5
2 BACKGROUND INFORMATION
21 CONNECTICUTrsquoS STATE INNOVATION MODEL
The State Innovation Model (SIM) initiative is a Center for Medicare amp Medicaid Innovation (CMMI) effort to
support the development and implementation of state-led multi-payer healthcare payment and service
delivery model reforms that will promote
healthier people better care and smarter
spending in participating states In 2014
Connecticut received a $45 million State
Innovation Model (SIM) grant from CMMI to
implement a multi-faceted strategy to improve
the health outcomes and healthcare spending
trajectory of the state as well as to improve
the sizeable health disparities that continue to
persist Over a four-year period (2015-2019)
Connecticutrsquos SIM proposes to improve
Connecticutrsquos health system for the majority of
residents
We are investing in a transition away from
paying for a volume of healthcare services
towards paying based on whether people receive high quality care with lower growth in costs This includes
funding the design and launch of the statersquos first Medicaid Shared Savings Program (ldquoPCMH+rdquo) which rewards
healthcare providers for improved quality outcomes and better cost trends
We are providing technical assistance and supports to healthcare providers that want to succeed in these new
payment models so that they can connect individuals to community and behavioral supports deploy
community health workers use data to track and improve their performance and more Providers access these
resources through our Advanced Medical Home and Community amp Clinical Integration Programs
Simultaneously we engage consumers by promoting insurance plans that remove financial barriers to or
introduce rewards for preventive care medication adherence chronic disease management and high-quality
provider selection We promote these ldquoValue-Based Insurance Designsrdquo by convening employers and creating
easily adoptable templates and disseminating best-practices
Lastly we are developing and testing components of a Population Health Plan which is to be completed and
implemented before the end of the SIM test grant period This longer-term strategy will combine innovations
in clinical healthcare delivery payment reform and population health strategies to improve health as a
community approach rather than one focused solely on patient panels
6
Over the last year the population health planning efforts have focused on designing and launching the
Prevention Service Initiative (PSI) This initiative aims to increase the number of contracts between CBOs and
ACOs for diabetes and asthma self-management programs by providing technical assistance
The State is now turning its attention to developing and implementing the Health Enhancement Community
Initiative This initiative is our most ambitious project under this population health effort
Connecticutrsquos SIM moves Connecticutrsquos health care system along a path of transformation The HEC model is
intended to build on and extend many of the current SIM investments and aims See the diagram below which
aligns with Neal Halfonrsquos Transformation Framework1 particularly the highlighted sections which articulate
much of what we are seeking to solve for in the HEC planning process The next section provides the context
for the HEC initiative
Please also note the following regarding Connecticut-specific public health and community related information
Community Health Collaborative scan 2017 Population Health Council Environmental Scan CT Prevention
Programs NCD Policy Scan CT Community Health Needs Assessments
1 See highlighted sections of Halfon (2014) report
7
22 HEALTH ENHANCEMENT COMMUNITY INITIATIVE Connecticutrsquos State Innovation Model is implementing a range of care delivery and payment reforms to
improve health care and slow the growth of healthcare spending However taken alone these are not
enough to make Connecticut a place where preventable deaths diseases and health disparities are
eliminated and every person enjoys the best health possible To achieve these ambitious goals
Connecticutrsquos SIM will partner with communities to design a Health Enhancement Community initiative
that moves beyond treating illness to address root causes behavior and social determinants of health
Connecticut is proposing to create the conditions that promote and sustain cross-sector community-led
strategies focused on prevention A provisional definition to begin the planning process was developed
A Health Enhancement Community is accountable for health health equity and related costs for
all residents in a geographic area uses data community engagement and cross sector activities
to identify and address root causes and operates in an economic environment that sustainably
funds and rewards such activities by capturing the economic value of improved health
Many components of the HEC definition are intentionally undefined in order to accommodate a
thoughtful community-driven planning process
More Needs to be Done to Shift the Focus to Prevention
More than half of all Americans suffer from one or more chronic diseases and obesity a precursor to
many chronic diseases is contributing to lower life expectancy Health disparities around chronic
conditions also persistmdashpeople of color face higher rates of diabetes obesity stroke heart disease and
cancer A study by the Milken Institute calculated that seven chronic conditions are costing the US
economy more than $1 trillion per year In fact chronic conditions drive 96 of Medicare costs and 83
of Medicaid costs and are responsible for two thirds of the rise in overall healthcare costs since 1980
Despite the fact that 40 of cancer 80 of heart disease and 80 of type 2 diabetes are preventable
the rates and costs of chronic conditions are predicted to continue to rise significantly over the coming
years
Bringing Everyone to the Table
Preventing chronic disease is beyond the reach of any one
sector of the community Inadequate healthcare for example
contributes about 10 to a personrsquos chances of dying
prematurely Moreover prevention in healthcare is difficult in
the current ldquosick carerdquo system Even in the most advanced
alternative payment models preventing chronic disease is not
rewarded
Health behaviors such as smoking and diet and exercise are the
most important determinants contributing 40 to the risk of
Proportional Contribution to Premature Death
8
premature death Improving health also depends heavily on addressing the non-behavioral determinants
of healthndash the conditions in which people are born grow work live and age
Working together the business municipal educational social service public health and healthcare
sectors can influence both behavior and the social determinants of health Local organizations and
community members themselves know best what the challenges are of their communities and how to
approach them
Research validates that preventable deaths have been reduced when comprehensive multi-sector
networks undertake health improvement initiatives National efforts have also emphasized cross-sector
initiatives For example Accountable Communities for Health (ACH) (eg CHCS report NASHP report) are
coming to the forefront in many states National efforts such as REACH have been shown to make an
impact on health equity In Connecticut important local collective efforts are occurring that are forming
the foundation for planning HECs including multi-sector collaboratives to identify and prioritize the most
pressing health needs in a community2
Why Setting the Table is Not Enough
Despite increased awareness of health disparities and a broad range of societal efforts to improve the
health of populations little progress has been made in reducing social gaps in health3 In fact current
Accountable Communities for Health (ACH) models often do not focus on upstream prevention that can
lead to broad improvements in health and health equity Several of the biggest challenges to ACH models
around the country include data and measurement infrastructure clear governance schemes and the
lack of long term financial sustainability
The State can play a critical role in supporting communities and facilitating solutions to these challenges
Bringing stakeholders together without addressing such barriers that prevent communities from fully
enacting and sustaining a prevention strategy is not likely to curb the rising rates of chronic disease For
example the State can 1) assist communities to establish a framework for measurement and
accountability 2) support the development of local multi-stakeholder alignments and locally tailored
governance structures and 3) solve for financial sustainability by defining demonstrating and capturing
the value of improved health due to prevention and create conditions that attract investments and
innovations in prevention4 Financial sustainability solutions may include but are not limited to market-
oriented-solutions public-private partnerships in financing or development of wellness trusts
2 Community Solutions initiative in N Hartford The Vita Health and Wellness District in Stamford Healthier Greater New Haven Partnership Primary Care Action Group in Bridgeport coalitions to complete Community Health Needs Assessments and others 3 Williams DR Costa MV Odunlami AO and Mohammed SA Moving Upstream How Interventions that Address the Social Determinants of Health can Improve Health and Reduce Disparities J Public Health Manag Pract 2008 14(Suppl)S8-17 4 See Appendix 1 page 51 httpswwwsurgeongeneralgovprioritiespreventionstrategyreportpdf
9
SIM Governance
The planning and execution of the HEC initiative will be done through extensive engagement with a broad
array of people and sectors inside and outside of government and in communities The Lieutenant
Governor provides overall leadership and oversight for SIM The SIM initiative is executed in collaboration
with multiple agencies and organizations including the Department of Public Health the Department of
Social Services the Office of the State Comptroller Access Health CT UConn Health and others The SIM
PMO within the Office of the Healthcare Advocate is leading the implementation of SIM The PMO
coordinates activities across work streams engages stakeholders manages vendors executes care
delivery reform initiatives and communicates progress to the public
The PMO engages more than 150 stakeholders through a number of advisory councils that focus on
particular components of SIM such as quality measurement practice transformation value-based
insurance design and population health These councils are comprised of consumers employers
healthcare providers community organizations and subject matter experts The Population Health
Council will play a key advisory role for the HEC initiative and will be engaged throughout the planning
and implementation process Over the past year the Population Health Council has advised on the
development of the Prevention Service Initiative It will now change its focus to advise primarily on the
HEC initiative Councils make their recommendations to the Healthcare Innovation Steering Committee
(HISC) which provides key guidance on the direction of SIM The HISC will also be actively engaged as part
of the HEC initiative
The HEC initiative and planning efforts are being jointly administered by both the PMO and DPH The two
parties will also jointly direct the contract(s) resulting from this procurement
10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative

4
1 EXECUTIVE SUMMARY The Health Enhancement Community (HEC) initiative is part of Connecticutrsquos comprehensive SIM strategy to promote healthier people better care smarter spending and health equity The consultant selected through this Request for Proposals (RFP) will provide subject matter expertise strategic planning design development actuarial analysis and stakeholder facilitation to support the creation of the HEC model and implementation approach
For the purpose of this RFP the state has established the following provisional definition
A Health Enhancement Community is accountable for health health equity and related costs for all
residents in a geographic area uses data community engagement and cross sector activities to identify
and address root causes and operates in an economic environment that sustainably funds and rewards
such activities by capturing the economic value of improved health
Any questions related to this grant program should be directed to
Faina Dookh
Fainadookhctgov
Applications must be submitted electronically on or before the date indicated below to
Fainadookhctgov
RFP Name Health Enhancement Community Consultation
RFP Release Date October 20 2017
Electronic Location of Request for Proposals httpwwwbiznetctgovSCP_SearchBidResultsaspx
Letter of Intent (optional) Due Date November 3 2017
Request for Proposals Application Due Date December 1 2017 at 1pm
Anticipated Notice of Award December 15 2017
Period of Award January 1 2018 ndash July 31 2018
Anticipated Total Available Funding $12 million
Anticipated Number of Awards One or two awards
Eligible Applicants
Consultants with expertise in operational and
strategic planning facilitation cross-sector
community health improvement stakeholder
engagement actuarial and health economic
modeling and payment reform
5
2 BACKGROUND INFORMATION
21 CONNECTICUTrsquoS STATE INNOVATION MODEL
The State Innovation Model (SIM) initiative is a Center for Medicare amp Medicaid Innovation (CMMI) effort to
support the development and implementation of state-led multi-payer healthcare payment and service
delivery model reforms that will promote
healthier people better care and smarter
spending in participating states In 2014
Connecticut received a $45 million State
Innovation Model (SIM) grant from CMMI to
implement a multi-faceted strategy to improve
the health outcomes and healthcare spending
trajectory of the state as well as to improve
the sizeable health disparities that continue to
persist Over a four-year period (2015-2019)
Connecticutrsquos SIM proposes to improve
Connecticutrsquos health system for the majority of
residents
We are investing in a transition away from
paying for a volume of healthcare services
towards paying based on whether people receive high quality care with lower growth in costs This includes
funding the design and launch of the statersquos first Medicaid Shared Savings Program (ldquoPCMH+rdquo) which rewards
healthcare providers for improved quality outcomes and better cost trends
We are providing technical assistance and supports to healthcare providers that want to succeed in these new
payment models so that they can connect individuals to community and behavioral supports deploy
community health workers use data to track and improve their performance and more Providers access these
resources through our Advanced Medical Home and Community amp Clinical Integration Programs
Simultaneously we engage consumers by promoting insurance plans that remove financial barriers to or
introduce rewards for preventive care medication adherence chronic disease management and high-quality
provider selection We promote these ldquoValue-Based Insurance Designsrdquo by convening employers and creating
easily adoptable templates and disseminating best-practices
Lastly we are developing and testing components of a Population Health Plan which is to be completed and
implemented before the end of the SIM test grant period This longer-term strategy will combine innovations
in clinical healthcare delivery payment reform and population health strategies to improve health as a
community approach rather than one focused solely on patient panels
6
Over the last year the population health planning efforts have focused on designing and launching the
Prevention Service Initiative (PSI) This initiative aims to increase the number of contracts between CBOs and
ACOs for diabetes and asthma self-management programs by providing technical assistance
The State is now turning its attention to developing and implementing the Health Enhancement Community
Initiative This initiative is our most ambitious project under this population health effort
Connecticutrsquos SIM moves Connecticutrsquos health care system along a path of transformation The HEC model is
intended to build on and extend many of the current SIM investments and aims See the diagram below which
aligns with Neal Halfonrsquos Transformation Framework1 particularly the highlighted sections which articulate
much of what we are seeking to solve for in the HEC planning process The next section provides the context
for the HEC initiative
Please also note the following regarding Connecticut-specific public health and community related information
Community Health Collaborative scan 2017 Population Health Council Environmental Scan CT Prevention
Programs NCD Policy Scan CT Community Health Needs Assessments
1 See highlighted sections of Halfon (2014) report
7
22 HEALTH ENHANCEMENT COMMUNITY INITIATIVE Connecticutrsquos State Innovation Model is implementing a range of care delivery and payment reforms to
improve health care and slow the growth of healthcare spending However taken alone these are not
enough to make Connecticut a place where preventable deaths diseases and health disparities are
eliminated and every person enjoys the best health possible To achieve these ambitious goals
Connecticutrsquos SIM will partner with communities to design a Health Enhancement Community initiative
that moves beyond treating illness to address root causes behavior and social determinants of health
Connecticut is proposing to create the conditions that promote and sustain cross-sector community-led
strategies focused on prevention A provisional definition to begin the planning process was developed
A Health Enhancement Community is accountable for health health equity and related costs for
all residents in a geographic area uses data community engagement and cross sector activities
to identify and address root causes and operates in an economic environment that sustainably
funds and rewards such activities by capturing the economic value of improved health
Many components of the HEC definition are intentionally undefined in order to accommodate a
thoughtful community-driven planning process
More Needs to be Done to Shift the Focus to Prevention
More than half of all Americans suffer from one or more chronic diseases and obesity a precursor to
many chronic diseases is contributing to lower life expectancy Health disparities around chronic
conditions also persistmdashpeople of color face higher rates of diabetes obesity stroke heart disease and
cancer A study by the Milken Institute calculated that seven chronic conditions are costing the US
economy more than $1 trillion per year In fact chronic conditions drive 96 of Medicare costs and 83
of Medicaid costs and are responsible for two thirds of the rise in overall healthcare costs since 1980
Despite the fact that 40 of cancer 80 of heart disease and 80 of type 2 diabetes are preventable
the rates and costs of chronic conditions are predicted to continue to rise significantly over the coming
years
Bringing Everyone to the Table
Preventing chronic disease is beyond the reach of any one
sector of the community Inadequate healthcare for example
contributes about 10 to a personrsquos chances of dying
prematurely Moreover prevention in healthcare is difficult in
the current ldquosick carerdquo system Even in the most advanced
alternative payment models preventing chronic disease is not
rewarded
Health behaviors such as smoking and diet and exercise are the
most important determinants contributing 40 to the risk of
Proportional Contribution to Premature Death
8
premature death Improving health also depends heavily on addressing the non-behavioral determinants
of healthndash the conditions in which people are born grow work live and age
Working together the business municipal educational social service public health and healthcare
sectors can influence both behavior and the social determinants of health Local organizations and
community members themselves know best what the challenges are of their communities and how to
approach them
Research validates that preventable deaths have been reduced when comprehensive multi-sector
networks undertake health improvement initiatives National efforts have also emphasized cross-sector
initiatives For example Accountable Communities for Health (ACH) (eg CHCS report NASHP report) are
coming to the forefront in many states National efforts such as REACH have been shown to make an
impact on health equity In Connecticut important local collective efforts are occurring that are forming
the foundation for planning HECs including multi-sector collaboratives to identify and prioritize the most
pressing health needs in a community2
Why Setting the Table is Not Enough
Despite increased awareness of health disparities and a broad range of societal efforts to improve the
health of populations little progress has been made in reducing social gaps in health3 In fact current
Accountable Communities for Health (ACH) models often do not focus on upstream prevention that can
lead to broad improvements in health and health equity Several of the biggest challenges to ACH models
around the country include data and measurement infrastructure clear governance schemes and the
lack of long term financial sustainability
The State can play a critical role in supporting communities and facilitating solutions to these challenges
Bringing stakeholders together without addressing such barriers that prevent communities from fully
enacting and sustaining a prevention strategy is not likely to curb the rising rates of chronic disease For
example the State can 1) assist communities to establish a framework for measurement and
accountability 2) support the development of local multi-stakeholder alignments and locally tailored
governance structures and 3) solve for financial sustainability by defining demonstrating and capturing
the value of improved health due to prevention and create conditions that attract investments and
innovations in prevention4 Financial sustainability solutions may include but are not limited to market-
oriented-solutions public-private partnerships in financing or development of wellness trusts
2 Community Solutions initiative in N Hartford The Vita Health and Wellness District in Stamford Healthier Greater New Haven Partnership Primary Care Action Group in Bridgeport coalitions to complete Community Health Needs Assessments and others 3 Williams DR Costa MV Odunlami AO and Mohammed SA Moving Upstream How Interventions that Address the Social Determinants of Health can Improve Health and Reduce Disparities J Public Health Manag Pract 2008 14(Suppl)S8-17 4 See Appendix 1 page 51 httpswwwsurgeongeneralgovprioritiespreventionstrategyreportpdf
9
SIM Governance
The planning and execution of the HEC initiative will be done through extensive engagement with a broad
array of people and sectors inside and outside of government and in communities The Lieutenant
Governor provides overall leadership and oversight for SIM The SIM initiative is executed in collaboration
with multiple agencies and organizations including the Department of Public Health the Department of
Social Services the Office of the State Comptroller Access Health CT UConn Health and others The SIM
PMO within the Office of the Healthcare Advocate is leading the implementation of SIM The PMO
coordinates activities across work streams engages stakeholders manages vendors executes care
delivery reform initiatives and communicates progress to the public
The PMO engages more than 150 stakeholders through a number of advisory councils that focus on
particular components of SIM such as quality measurement practice transformation value-based
insurance design and population health These councils are comprised of consumers employers
healthcare providers community organizations and subject matter experts The Population Health
Council will play a key advisory role for the HEC initiative and will be engaged throughout the planning
and implementation process Over the past year the Population Health Council has advised on the
development of the Prevention Service Initiative It will now change its focus to advise primarily on the
HEC initiative Councils make their recommendations to the Healthcare Innovation Steering Committee
(HISC) which provides key guidance on the direction of SIM The HISC will also be actively engaged as part
of the HEC initiative
The HEC initiative and planning efforts are being jointly administered by both the PMO and DPH The two
parties will also jointly direct the contract(s) resulting from this procurement
10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative
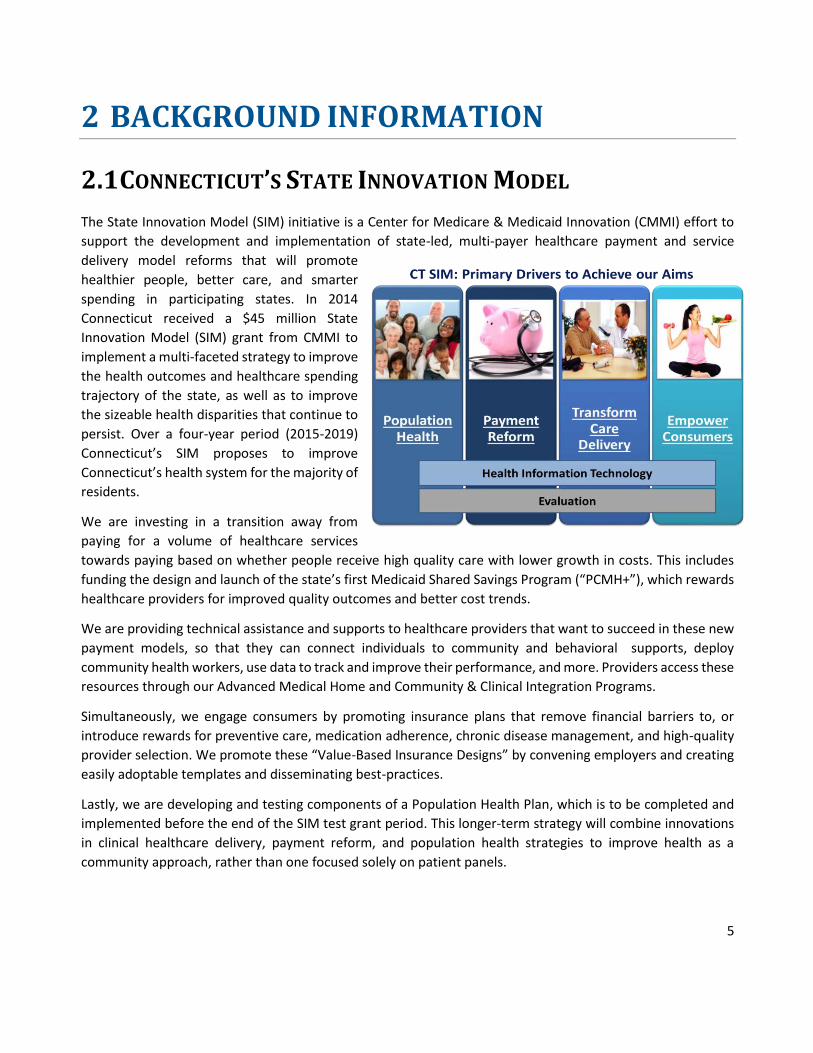
5
2 BACKGROUND INFORMATION
21 CONNECTICUTrsquoS STATE INNOVATION MODEL
The State Innovation Model (SIM) initiative is a Center for Medicare amp Medicaid Innovation (CMMI) effort to
support the development and implementation of state-led multi-payer healthcare payment and service
delivery model reforms that will promote
healthier people better care and smarter
spending in participating states In 2014
Connecticut received a $45 million State
Innovation Model (SIM) grant from CMMI to
implement a multi-faceted strategy to improve
the health outcomes and healthcare spending
trajectory of the state as well as to improve
the sizeable health disparities that continue to
persist Over a four-year period (2015-2019)
Connecticutrsquos SIM proposes to improve
Connecticutrsquos health system for the majority of
residents
We are investing in a transition away from
paying for a volume of healthcare services
towards paying based on whether people receive high quality care with lower growth in costs This includes
funding the design and launch of the statersquos first Medicaid Shared Savings Program (ldquoPCMH+rdquo) which rewards
healthcare providers for improved quality outcomes and better cost trends
We are providing technical assistance and supports to healthcare providers that want to succeed in these new
payment models so that they can connect individuals to community and behavioral supports deploy
community health workers use data to track and improve their performance and more Providers access these
resources through our Advanced Medical Home and Community amp Clinical Integration Programs
Simultaneously we engage consumers by promoting insurance plans that remove financial barriers to or
introduce rewards for preventive care medication adherence chronic disease management and high-quality
provider selection We promote these ldquoValue-Based Insurance Designsrdquo by convening employers and creating
easily adoptable templates and disseminating best-practices
Lastly we are developing and testing components of a Population Health Plan which is to be completed and
implemented before the end of the SIM test grant period This longer-term strategy will combine innovations
in clinical healthcare delivery payment reform and population health strategies to improve health as a
community approach rather than one focused solely on patient panels
6
Over the last year the population health planning efforts have focused on designing and launching the
Prevention Service Initiative (PSI) This initiative aims to increase the number of contracts between CBOs and
ACOs for diabetes and asthma self-management programs by providing technical assistance
The State is now turning its attention to developing and implementing the Health Enhancement Community
Initiative This initiative is our most ambitious project under this population health effort
Connecticutrsquos SIM moves Connecticutrsquos health care system along a path of transformation The HEC model is
intended to build on and extend many of the current SIM investments and aims See the diagram below which
aligns with Neal Halfonrsquos Transformation Framework1 particularly the highlighted sections which articulate
much of what we are seeking to solve for in the HEC planning process The next section provides the context
for the HEC initiative
Please also note the following regarding Connecticut-specific public health and community related information
Community Health Collaborative scan 2017 Population Health Council Environmental Scan CT Prevention
Programs NCD Policy Scan CT Community Health Needs Assessments
1 See highlighted sections of Halfon (2014) report
7
22 HEALTH ENHANCEMENT COMMUNITY INITIATIVE Connecticutrsquos State Innovation Model is implementing a range of care delivery and payment reforms to
improve health care and slow the growth of healthcare spending However taken alone these are not
enough to make Connecticut a place where preventable deaths diseases and health disparities are
eliminated and every person enjoys the best health possible To achieve these ambitious goals
Connecticutrsquos SIM will partner with communities to design a Health Enhancement Community initiative
that moves beyond treating illness to address root causes behavior and social determinants of health
Connecticut is proposing to create the conditions that promote and sustain cross-sector community-led
strategies focused on prevention A provisional definition to begin the planning process was developed
A Health Enhancement Community is accountable for health health equity and related costs for
all residents in a geographic area uses data community engagement and cross sector activities
to identify and address root causes and operates in an economic environment that sustainably
funds and rewards such activities by capturing the economic value of improved health
Many components of the HEC definition are intentionally undefined in order to accommodate a
thoughtful community-driven planning process
More Needs to be Done to Shift the Focus to Prevention
More than half of all Americans suffer from one or more chronic diseases and obesity a precursor to
many chronic diseases is contributing to lower life expectancy Health disparities around chronic
conditions also persistmdashpeople of color face higher rates of diabetes obesity stroke heart disease and
cancer A study by the Milken Institute calculated that seven chronic conditions are costing the US
economy more than $1 trillion per year In fact chronic conditions drive 96 of Medicare costs and 83
of Medicaid costs and are responsible for two thirds of the rise in overall healthcare costs since 1980
Despite the fact that 40 of cancer 80 of heart disease and 80 of type 2 diabetes are preventable
the rates and costs of chronic conditions are predicted to continue to rise significantly over the coming
years
Bringing Everyone to the Table
Preventing chronic disease is beyond the reach of any one
sector of the community Inadequate healthcare for example
contributes about 10 to a personrsquos chances of dying
prematurely Moreover prevention in healthcare is difficult in
the current ldquosick carerdquo system Even in the most advanced
alternative payment models preventing chronic disease is not
rewarded
Health behaviors such as smoking and diet and exercise are the
most important determinants contributing 40 to the risk of
Proportional Contribution to Premature Death
8
premature death Improving health also depends heavily on addressing the non-behavioral determinants
of healthndash the conditions in which people are born grow work live and age
Working together the business municipal educational social service public health and healthcare
sectors can influence both behavior and the social determinants of health Local organizations and
community members themselves know best what the challenges are of their communities and how to
approach them
Research validates that preventable deaths have been reduced when comprehensive multi-sector
networks undertake health improvement initiatives National efforts have also emphasized cross-sector
initiatives For example Accountable Communities for Health (ACH) (eg CHCS report NASHP report) are
coming to the forefront in many states National efforts such as REACH have been shown to make an
impact on health equity In Connecticut important local collective efforts are occurring that are forming
the foundation for planning HECs including multi-sector collaboratives to identify and prioritize the most
pressing health needs in a community2
Why Setting the Table is Not Enough
Despite increased awareness of health disparities and a broad range of societal efforts to improve the
health of populations little progress has been made in reducing social gaps in health3 In fact current
Accountable Communities for Health (ACH) models often do not focus on upstream prevention that can
lead to broad improvements in health and health equity Several of the biggest challenges to ACH models
around the country include data and measurement infrastructure clear governance schemes and the
lack of long term financial sustainability
The State can play a critical role in supporting communities and facilitating solutions to these challenges
Bringing stakeholders together without addressing such barriers that prevent communities from fully
enacting and sustaining a prevention strategy is not likely to curb the rising rates of chronic disease For
example the State can 1) assist communities to establish a framework for measurement and
accountability 2) support the development of local multi-stakeholder alignments and locally tailored
governance structures and 3) solve for financial sustainability by defining demonstrating and capturing
the value of improved health due to prevention and create conditions that attract investments and
innovations in prevention4 Financial sustainability solutions may include but are not limited to market-
oriented-solutions public-private partnerships in financing or development of wellness trusts
2 Community Solutions initiative in N Hartford The Vita Health and Wellness District in Stamford Healthier Greater New Haven Partnership Primary Care Action Group in Bridgeport coalitions to complete Community Health Needs Assessments and others 3 Williams DR Costa MV Odunlami AO and Mohammed SA Moving Upstream How Interventions that Address the Social Determinants of Health can Improve Health and Reduce Disparities J Public Health Manag Pract 2008 14(Suppl)S8-17 4 See Appendix 1 page 51 httpswwwsurgeongeneralgovprioritiespreventionstrategyreportpdf
9
SIM Governance
The planning and execution of the HEC initiative will be done through extensive engagement with a broad
array of people and sectors inside and outside of government and in communities The Lieutenant
Governor provides overall leadership and oversight for SIM The SIM initiative is executed in collaboration
with multiple agencies and organizations including the Department of Public Health the Department of
Social Services the Office of the State Comptroller Access Health CT UConn Health and others The SIM
PMO within the Office of the Healthcare Advocate is leading the implementation of SIM The PMO
coordinates activities across work streams engages stakeholders manages vendors executes care
delivery reform initiatives and communicates progress to the public
The PMO engages more than 150 stakeholders through a number of advisory councils that focus on
particular components of SIM such as quality measurement practice transformation value-based
insurance design and population health These councils are comprised of consumers employers
healthcare providers community organizations and subject matter experts The Population Health
Council will play a key advisory role for the HEC initiative and will be engaged throughout the planning
and implementation process Over the past year the Population Health Council has advised on the
development of the Prevention Service Initiative It will now change its focus to advise primarily on the
HEC initiative Councils make their recommendations to the Healthcare Innovation Steering Committee
(HISC) which provides key guidance on the direction of SIM The HISC will also be actively engaged as part
of the HEC initiative
The HEC initiative and planning efforts are being jointly administered by both the PMO and DPH The two
parties will also jointly direct the contract(s) resulting from this procurement
10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative

6
Over the last year the population health planning efforts have focused on designing and launching the
Prevention Service Initiative (PSI) This initiative aims to increase the number of contracts between CBOs and
ACOs for diabetes and asthma self-management programs by providing technical assistance
The State is now turning its attention to developing and implementing the Health Enhancement Community
Initiative This initiative is our most ambitious project under this population health effort
Connecticutrsquos SIM moves Connecticutrsquos health care system along a path of transformation The HEC model is
intended to build on and extend many of the current SIM investments and aims See the diagram below which
aligns with Neal Halfonrsquos Transformation Framework1 particularly the highlighted sections which articulate
much of what we are seeking to solve for in the HEC planning process The next section provides the context
for the HEC initiative
Please also note the following regarding Connecticut-specific public health and community related information
Community Health Collaborative scan 2017 Population Health Council Environmental Scan CT Prevention
Programs NCD Policy Scan CT Community Health Needs Assessments
1 See highlighted sections of Halfon (2014) report
7
22 HEALTH ENHANCEMENT COMMUNITY INITIATIVE Connecticutrsquos State Innovation Model is implementing a range of care delivery and payment reforms to
improve health care and slow the growth of healthcare spending However taken alone these are not
enough to make Connecticut a place where preventable deaths diseases and health disparities are
eliminated and every person enjoys the best health possible To achieve these ambitious goals
Connecticutrsquos SIM will partner with communities to design a Health Enhancement Community initiative
that moves beyond treating illness to address root causes behavior and social determinants of health
Connecticut is proposing to create the conditions that promote and sustain cross-sector community-led
strategies focused on prevention A provisional definition to begin the planning process was developed
A Health Enhancement Community is accountable for health health equity and related costs for
all residents in a geographic area uses data community engagement and cross sector activities
to identify and address root causes and operates in an economic environment that sustainably
funds and rewards such activities by capturing the economic value of improved health
Many components of the HEC definition are intentionally undefined in order to accommodate a
thoughtful community-driven planning process
More Needs to be Done to Shift the Focus to Prevention
More than half of all Americans suffer from one or more chronic diseases and obesity a precursor to
many chronic diseases is contributing to lower life expectancy Health disparities around chronic
conditions also persistmdashpeople of color face higher rates of diabetes obesity stroke heart disease and
cancer A study by the Milken Institute calculated that seven chronic conditions are costing the US
economy more than $1 trillion per year In fact chronic conditions drive 96 of Medicare costs and 83
of Medicaid costs and are responsible for two thirds of the rise in overall healthcare costs since 1980
Despite the fact that 40 of cancer 80 of heart disease and 80 of type 2 diabetes are preventable
the rates and costs of chronic conditions are predicted to continue to rise significantly over the coming
years
Bringing Everyone to the Table
Preventing chronic disease is beyond the reach of any one
sector of the community Inadequate healthcare for example
contributes about 10 to a personrsquos chances of dying
prematurely Moreover prevention in healthcare is difficult in
the current ldquosick carerdquo system Even in the most advanced
alternative payment models preventing chronic disease is not
rewarded
Health behaviors such as smoking and diet and exercise are the
most important determinants contributing 40 to the risk of
Proportional Contribution to Premature Death
8
premature death Improving health also depends heavily on addressing the non-behavioral determinants
of healthndash the conditions in which people are born grow work live and age
Working together the business municipal educational social service public health and healthcare
sectors can influence both behavior and the social determinants of health Local organizations and
community members themselves know best what the challenges are of their communities and how to
approach them
Research validates that preventable deaths have been reduced when comprehensive multi-sector
networks undertake health improvement initiatives National efforts have also emphasized cross-sector
initiatives For example Accountable Communities for Health (ACH) (eg CHCS report NASHP report) are
coming to the forefront in many states National efforts such as REACH have been shown to make an
impact on health equity In Connecticut important local collective efforts are occurring that are forming
the foundation for planning HECs including multi-sector collaboratives to identify and prioritize the most
pressing health needs in a community2
Why Setting the Table is Not Enough
Despite increased awareness of health disparities and a broad range of societal efforts to improve the
health of populations little progress has been made in reducing social gaps in health3 In fact current
Accountable Communities for Health (ACH) models often do not focus on upstream prevention that can
lead to broad improvements in health and health equity Several of the biggest challenges to ACH models
around the country include data and measurement infrastructure clear governance schemes and the
lack of long term financial sustainability
The State can play a critical role in supporting communities and facilitating solutions to these challenges
Bringing stakeholders together without addressing such barriers that prevent communities from fully
enacting and sustaining a prevention strategy is not likely to curb the rising rates of chronic disease For
example the State can 1) assist communities to establish a framework for measurement and
accountability 2) support the development of local multi-stakeholder alignments and locally tailored
governance structures and 3) solve for financial sustainability by defining demonstrating and capturing
the value of improved health due to prevention and create conditions that attract investments and
innovations in prevention4 Financial sustainability solutions may include but are not limited to market-
oriented-solutions public-private partnerships in financing or development of wellness trusts
2 Community Solutions initiative in N Hartford The Vita Health and Wellness District in Stamford Healthier Greater New Haven Partnership Primary Care Action Group in Bridgeport coalitions to complete Community Health Needs Assessments and others 3 Williams DR Costa MV Odunlami AO and Mohammed SA Moving Upstream How Interventions that Address the Social Determinants of Health can Improve Health and Reduce Disparities J Public Health Manag Pract 2008 14(Suppl)S8-17 4 See Appendix 1 page 51 httpswwwsurgeongeneralgovprioritiespreventionstrategyreportpdf
9
SIM Governance
The planning and execution of the HEC initiative will be done through extensive engagement with a broad
array of people and sectors inside and outside of government and in communities The Lieutenant
Governor provides overall leadership and oversight for SIM The SIM initiative is executed in collaboration
with multiple agencies and organizations including the Department of Public Health the Department of
Social Services the Office of the State Comptroller Access Health CT UConn Health and others The SIM
PMO within the Office of the Healthcare Advocate is leading the implementation of SIM The PMO
coordinates activities across work streams engages stakeholders manages vendors executes care
delivery reform initiatives and communicates progress to the public
The PMO engages more than 150 stakeholders through a number of advisory councils that focus on
particular components of SIM such as quality measurement practice transformation value-based
insurance design and population health These councils are comprised of consumers employers
healthcare providers community organizations and subject matter experts The Population Health
Council will play a key advisory role for the HEC initiative and will be engaged throughout the planning
and implementation process Over the past year the Population Health Council has advised on the
development of the Prevention Service Initiative It will now change its focus to advise primarily on the
HEC initiative Councils make their recommendations to the Healthcare Innovation Steering Committee
(HISC) which provides key guidance on the direction of SIM The HISC will also be actively engaged as part
of the HEC initiative
The HEC initiative and planning efforts are being jointly administered by both the PMO and DPH The two
parties will also jointly direct the contract(s) resulting from this procurement
10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative

7
22 HEALTH ENHANCEMENT COMMUNITY INITIATIVE Connecticutrsquos State Innovation Model is implementing a range of care delivery and payment reforms to
improve health care and slow the growth of healthcare spending However taken alone these are not
enough to make Connecticut a place where preventable deaths diseases and health disparities are
eliminated and every person enjoys the best health possible To achieve these ambitious goals
Connecticutrsquos SIM will partner with communities to design a Health Enhancement Community initiative
that moves beyond treating illness to address root causes behavior and social determinants of health
Connecticut is proposing to create the conditions that promote and sustain cross-sector community-led
strategies focused on prevention A provisional definition to begin the planning process was developed
A Health Enhancement Community is accountable for health health equity and related costs for
all residents in a geographic area uses data community engagement and cross sector activities
to identify and address root causes and operates in an economic environment that sustainably
funds and rewards such activities by capturing the economic value of improved health
Many components of the HEC definition are intentionally undefined in order to accommodate a
thoughtful community-driven planning process
More Needs to be Done to Shift the Focus to Prevention
More than half of all Americans suffer from one or more chronic diseases and obesity a precursor to
many chronic diseases is contributing to lower life expectancy Health disparities around chronic
conditions also persistmdashpeople of color face higher rates of diabetes obesity stroke heart disease and
cancer A study by the Milken Institute calculated that seven chronic conditions are costing the US
economy more than $1 trillion per year In fact chronic conditions drive 96 of Medicare costs and 83
of Medicaid costs and are responsible for two thirds of the rise in overall healthcare costs since 1980
Despite the fact that 40 of cancer 80 of heart disease and 80 of type 2 diabetes are preventable
the rates and costs of chronic conditions are predicted to continue to rise significantly over the coming
years
Bringing Everyone to the Table
Preventing chronic disease is beyond the reach of any one
sector of the community Inadequate healthcare for example
contributes about 10 to a personrsquos chances of dying
prematurely Moreover prevention in healthcare is difficult in
the current ldquosick carerdquo system Even in the most advanced
alternative payment models preventing chronic disease is not
rewarded
Health behaviors such as smoking and diet and exercise are the
most important determinants contributing 40 to the risk of
Proportional Contribution to Premature Death
8
premature death Improving health also depends heavily on addressing the non-behavioral determinants
of healthndash the conditions in which people are born grow work live and age
Working together the business municipal educational social service public health and healthcare
sectors can influence both behavior and the social determinants of health Local organizations and
community members themselves know best what the challenges are of their communities and how to
approach them
Research validates that preventable deaths have been reduced when comprehensive multi-sector
networks undertake health improvement initiatives National efforts have also emphasized cross-sector
initiatives For example Accountable Communities for Health (ACH) (eg CHCS report NASHP report) are
coming to the forefront in many states National efforts such as REACH have been shown to make an
impact on health equity In Connecticut important local collective efforts are occurring that are forming
the foundation for planning HECs including multi-sector collaboratives to identify and prioritize the most
pressing health needs in a community2
Why Setting the Table is Not Enough
Despite increased awareness of health disparities and a broad range of societal efforts to improve the
health of populations little progress has been made in reducing social gaps in health3 In fact current
Accountable Communities for Health (ACH) models often do not focus on upstream prevention that can
lead to broad improvements in health and health equity Several of the biggest challenges to ACH models
around the country include data and measurement infrastructure clear governance schemes and the
lack of long term financial sustainability
The State can play a critical role in supporting communities and facilitating solutions to these challenges
Bringing stakeholders together without addressing such barriers that prevent communities from fully
enacting and sustaining a prevention strategy is not likely to curb the rising rates of chronic disease For
example the State can 1) assist communities to establish a framework for measurement and
accountability 2) support the development of local multi-stakeholder alignments and locally tailored
governance structures and 3) solve for financial sustainability by defining demonstrating and capturing
the value of improved health due to prevention and create conditions that attract investments and
innovations in prevention4 Financial sustainability solutions may include but are not limited to market-
oriented-solutions public-private partnerships in financing or development of wellness trusts
2 Community Solutions initiative in N Hartford The Vita Health and Wellness District in Stamford Healthier Greater New Haven Partnership Primary Care Action Group in Bridgeport coalitions to complete Community Health Needs Assessments and others 3 Williams DR Costa MV Odunlami AO and Mohammed SA Moving Upstream How Interventions that Address the Social Determinants of Health can Improve Health and Reduce Disparities J Public Health Manag Pract 2008 14(Suppl)S8-17 4 See Appendix 1 page 51 httpswwwsurgeongeneralgovprioritiespreventionstrategyreportpdf
9
SIM Governance
The planning and execution of the HEC initiative will be done through extensive engagement with a broad
array of people and sectors inside and outside of government and in communities The Lieutenant
Governor provides overall leadership and oversight for SIM The SIM initiative is executed in collaboration
with multiple agencies and organizations including the Department of Public Health the Department of
Social Services the Office of the State Comptroller Access Health CT UConn Health and others The SIM
PMO within the Office of the Healthcare Advocate is leading the implementation of SIM The PMO
coordinates activities across work streams engages stakeholders manages vendors executes care
delivery reform initiatives and communicates progress to the public
The PMO engages more than 150 stakeholders through a number of advisory councils that focus on
particular components of SIM such as quality measurement practice transformation value-based
insurance design and population health These councils are comprised of consumers employers
healthcare providers community organizations and subject matter experts The Population Health
Council will play a key advisory role for the HEC initiative and will be engaged throughout the planning
and implementation process Over the past year the Population Health Council has advised on the
development of the Prevention Service Initiative It will now change its focus to advise primarily on the
HEC initiative Councils make their recommendations to the Healthcare Innovation Steering Committee
(HISC) which provides key guidance on the direction of SIM The HISC will also be actively engaged as part
of the HEC initiative
The HEC initiative and planning efforts are being jointly administered by both the PMO and DPH The two
parties will also jointly direct the contract(s) resulting from this procurement
10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative

8
premature death Improving health also depends heavily on addressing the non-behavioral determinants
of healthndash the conditions in which people are born grow work live and age
Working together the business municipal educational social service public health and healthcare
sectors can influence both behavior and the social determinants of health Local organizations and
community members themselves know best what the challenges are of their communities and how to
approach them
Research validates that preventable deaths have been reduced when comprehensive multi-sector
networks undertake health improvement initiatives National efforts have also emphasized cross-sector
initiatives For example Accountable Communities for Health (ACH) (eg CHCS report NASHP report) are
coming to the forefront in many states National efforts such as REACH have been shown to make an
impact on health equity In Connecticut important local collective efforts are occurring that are forming
the foundation for planning HECs including multi-sector collaboratives to identify and prioritize the most
pressing health needs in a community2
Why Setting the Table is Not Enough
Despite increased awareness of health disparities and a broad range of societal efforts to improve the
health of populations little progress has been made in reducing social gaps in health3 In fact current
Accountable Communities for Health (ACH) models often do not focus on upstream prevention that can
lead to broad improvements in health and health equity Several of the biggest challenges to ACH models
around the country include data and measurement infrastructure clear governance schemes and the
lack of long term financial sustainability
The State can play a critical role in supporting communities and facilitating solutions to these challenges
Bringing stakeholders together without addressing such barriers that prevent communities from fully
enacting and sustaining a prevention strategy is not likely to curb the rising rates of chronic disease For
example the State can 1) assist communities to establish a framework for measurement and
accountability 2) support the development of local multi-stakeholder alignments and locally tailored
governance structures and 3) solve for financial sustainability by defining demonstrating and capturing
the value of improved health due to prevention and create conditions that attract investments and
innovations in prevention4 Financial sustainability solutions may include but are not limited to market-
oriented-solutions public-private partnerships in financing or development of wellness trusts
2 Community Solutions initiative in N Hartford The Vita Health and Wellness District in Stamford Healthier Greater New Haven Partnership Primary Care Action Group in Bridgeport coalitions to complete Community Health Needs Assessments and others 3 Williams DR Costa MV Odunlami AO and Mohammed SA Moving Upstream How Interventions that Address the Social Determinants of Health can Improve Health and Reduce Disparities J Public Health Manag Pract 2008 14(Suppl)S8-17 4 See Appendix 1 page 51 httpswwwsurgeongeneralgovprioritiespreventionstrategyreportpdf
9
SIM Governance
The planning and execution of the HEC initiative will be done through extensive engagement with a broad
array of people and sectors inside and outside of government and in communities The Lieutenant
Governor provides overall leadership and oversight for SIM The SIM initiative is executed in collaboration
with multiple agencies and organizations including the Department of Public Health the Department of
Social Services the Office of the State Comptroller Access Health CT UConn Health and others The SIM
PMO within the Office of the Healthcare Advocate is leading the implementation of SIM The PMO
coordinates activities across work streams engages stakeholders manages vendors executes care
delivery reform initiatives and communicates progress to the public
The PMO engages more than 150 stakeholders through a number of advisory councils that focus on
particular components of SIM such as quality measurement practice transformation value-based
insurance design and population health These councils are comprised of consumers employers
healthcare providers community organizations and subject matter experts The Population Health
Council will play a key advisory role for the HEC initiative and will be engaged throughout the planning
and implementation process Over the past year the Population Health Council has advised on the
development of the Prevention Service Initiative It will now change its focus to advise primarily on the
HEC initiative Councils make their recommendations to the Healthcare Innovation Steering Committee
(HISC) which provides key guidance on the direction of SIM The HISC will also be actively engaged as part
of the HEC initiative
The HEC initiative and planning efforts are being jointly administered by both the PMO and DPH The two
parties will also jointly direct the contract(s) resulting from this procurement
10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative

9
SIM Governance
The planning and execution of the HEC initiative will be done through extensive engagement with a broad
array of people and sectors inside and outside of government and in communities The Lieutenant
Governor provides overall leadership and oversight for SIM The SIM initiative is executed in collaboration
with multiple agencies and organizations including the Department of Public Health the Department of
Social Services the Office of the State Comptroller Access Health CT UConn Health and others The SIM
PMO within the Office of the Healthcare Advocate is leading the implementation of SIM The PMO
coordinates activities across work streams engages stakeholders manages vendors executes care
delivery reform initiatives and communicates progress to the public
The PMO engages more than 150 stakeholders through a number of advisory councils that focus on
particular components of SIM such as quality measurement practice transformation value-based
insurance design and population health These councils are comprised of consumers employers
healthcare providers community organizations and subject matter experts The Population Health
Council will play a key advisory role for the HEC initiative and will be engaged throughout the planning
and implementation process Over the past year the Population Health Council has advised on the
development of the Prevention Service Initiative It will now change its focus to advise primarily on the
HEC initiative Councils make their recommendations to the Healthcare Innovation Steering Committee
(HISC) which provides key guidance on the direction of SIM The HISC will also be actively engaged as part
of the HEC initiative
The HEC initiative and planning efforts are being jointly administered by both the PMO and DPH The two
parties will also jointly direct the contract(s) resulting from this procurement
10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative

10
3 REQUIRED SCOPE OF WORK AND
QUALIFICATIONS
31 SCOPE OF WORK Below we outline five high-level objectives of the HEC initiative We also inventory the activities that the
resultant consultant will undertake to support the State in meeting these objectives These activities are not
meant to be comprehensive and may evolve as the planning work unfolds The State welcomes the
incorporation of the Respondentrsquos ideas in their response
We recognize that this scope of work requires a wide range of capabilities While the State prefers a single
contract and point of accountability the state welcomes proposals from a) a single bidder demonstrating the
capacity to undertake all five objectives b) a partnership between a principal bidder and subcontracted
consultants or c) multiple bidders responding to a subset of the objectives
OBJECTIVE 1 There is an innovative logical clear and actionable strategy to support and enable HECs in
Connecticutrsquos communities
1 Synthesize the Connecticut-specific problems the initiative addresses and what success looks like
2 Recommend the role of key sectors in enabling HECs to succeed including potential governance
structures sources of infrastructure support management resources fiduciary functions and coordinating
activities This includes identifying the respective role and functions of the State and participating
communities
3 Recommend community-wide process and outcome measures and methods for producing such measures
as a means to monitor HEC performance such measures must be sufficiently reliable and valid to serve as
the basis for accountability agreements and the distribution of financial rewards The recommendation
should include a solution for community-wide attribution (ie the population with regard to which the
HEC performance will be measured)
4 Recommend one or more financial models and a plan for implementing such models that would provide
financial resources up-front to plan and implement cross-sector activities and sustain such activities
ongoing Such models should at a minimum
a Enable near term investments in infrastructure and cross-sector activities
b Rely primarily on public and private sector investments and contributions rather than grants
c Provide rewards to HECs and other contributorsinvestors
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative
11
proportionate to the economic value of health improved considering the tangible and
intangible value produced in the healthcare sector as well as other sectors such as private
and public sector employers municipalities and state agencies such as corrections and child
welfare
taking into consideration the extended return on investment timeframes characteristic of
root cause preventive interventions
5 In support of 4 above consider promising options for financing root cause solutions such as those
identified in the RWJF report and CDC report The examination shall at a minimum include but not limited
to the following
Capture and reinvest Low-income housing tax credits
Blending and braiding federal state and local funds New Markets Tax Credit
Community benefit financial institutions Pay for SuccessSocial Impact Bonds
Hospital Community Benefit
Prevention escrow account
Wellness Trust
Captive insurance
6 Identify and review the range of existing value-based payment models with special attention to existing
Connecticut models and recommend adjustments to such models that would promote investments in
prevention
7 Recommend statutory and regulatory levers and various federal authorities (eg Medicare or Medicaid
waivers) that would be required to implement the solutions recommended in 4 5 and 6 above
8 Recommend health information technology enablers that would enable the success of HECs and federal
opportunities to finance such enablers in consultation with the Statersquos Health Information Technology
Officer (HITO)
9 Recommend levers regarding workforce
OBJECTIVE 2 The HEC strategy is designed using a community-driven process that is relevant to and has
strong buy-in from a diverse set of stakeholders
1 Implement an ongoing stakeholder engagement and communication strategy This strategy should at a
minimum
a Allow for community members existing collaboratives healthcare providers employers
community organizations municipal government representatives and others to be active
participants and co-creators of the ultimate HEC approach
b Special emphasis should be placed on garnering the input and engagement of individuals and
organizations that represent or serve populations with demonstrated health disparities
c Engage state experts in insurance and health economics and private and public universities
d Engage federal officials such as at CMS CMMI and HRSA as needed
12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative

12
e Communicate progress on a periodic basis translating complex ideas into simple clear
messages for broad dissemination
f Propose a feedback process where HEC components and recommendations are continuously
vetted and adjusted as part of the stakeholder input process
2 Support the State in engaging state agencies and statewide organizations (eg foundations) in the
planning process This may include preparing background materials organizing meetings preparing
summaries and serving as subject matter experts
3 Work with a cohort of no less than three reference community health collaboratives that meet a minimum
state of readiness in order to engage in a problem-solving partnership for designing the HEC strategy and
to illustrate how the recommendations from Objective 1 might be realized in a Connecticut-specific
community Jointly with the reference communities as planning partners the planning should examine
barriers and opportunities related to governance management infrastructure data measurement and
financing with respect to cross-sector health and prevention activities The planning partners should
examine existing sources of funds that are currently used to subsidize such activities or that could be
leveraged as part of a braided or blended funding solution The planning partners should also examine
potential sources of investment capital that may be accessible to members of these communities
OBJECTIVE 3 The State can quantify the magnitude of the economic opportunity associated with health
improvements that may be undertaken by HECs
1 Propose and conduct financial modeling using Medicare data contained in the Connecticut All Payer Claims
Database to project the potential savings associated with various health improvement scenarios over a 2
5 10 15 and 20-year timeframe The analysis should focus primarily on the economic benefits of health
problems avoided (ie a reduction in the incidence and prevalence of acute and chronic illness and injury)
as a result of primary and upstream secondary prevention The analysis should examine non-disease
specific approaches to quantifying value creation such as impact on population risk trend as reflected in
HCC risk scoring The analysis should not focus on savings that accrue from improvements in clinical
management as is typical of most value-based payment models
2 Produce a flexible financial modeling tool using Medicare data that enables state planners to modify
assumptions and assess associated economic impact
3 Recommend companion analyses that may be undertaken by the State and its private partner payers with
respect to Medicaid state employees and commercially insured populations in order to produce a
complete statewide view of the potential economic value of health improved
4 Propose and conduct analyses with respect to other state agency service expenditures to which health
improvement benefits would likely accrue in corrections juvenile justice education housing and child
welfare
13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative

13
5 Work with 2-3 employers to model the potential value of prevention efforts as it relates to productivity
(eg presenteeism amp absenteeism)
OBJECTIVE 4 Input from the Population Health Council and the Health Care Innovation Steering Committee
(HISC) is incorporated into the HEC initiative and there is adequate buy-in from members
1 Engage the HISC and Population Health Council in the formulation of an HEC vision and associated
Population Health Council charter which will serve as a frame for the advisory process
2 Facilitate in-person monthly Population Health Council meetings including the following
a Preparing meeting agendas presentation materials and background materials facilitating the
discussion conducting presentations creating a structured and logically sequenced timetable
b Arranging for presentations andor illustrating local experiences that feature related work in
Connecticut and in other states
3 Provide periodic presentations to and solicit input from the HISC
Note well The consultant(s) should plan to facilitate 7-10 meetings of the Population Health Council which
is expected to meet no less than monthly during this intensive planning process The consultant(s) should
plan to address the HISC on three to four occasions through the conclusion of the planning process The HISC
usually requires two meetings to review and approve a final plan including a period of public comment
OBJECTIVE 5 Summary Report and Plan
1 Produce a concise and clear report including at a minimum background key findings and recommended
HEC initiative strategy consistent with the advice of the Population Health Council and HISC
2 The report should contain a summary of the community engagement status including an illustration of a
hypothetical future state The future state should provide an applied view of the proposed strategy if it
were implemented and fully realized in these reference communities
3 Propose a detailed plan with timelines milestones etc that operationalize key components of the HEC
initiative





























