-
8/3/2019 Health Economics- Lecture Ch06
1/42
The Production, Cost, and
Technology of Health Care
Dr. Katherine Sauer
Metropolitan State College of Denver
Health Economics
-
8/3/2019 Health Economics- Lecture Ch06
2/42
Recall from chapter 5 that health is the output goal.
Much attention is paid to the intermediate output,
health care.
Outline:
I. Degree of Substitutability in the Production Process
II. Costs
III. Efficiency
IV. Technology
-
8/3/2019 Health Economics- Lecture Ch06
3/42
I. Degree of Substitutability in the Production Process
Health practitioners often argue that there is basically one
way to treat a given illness. (monotechnic view).
Economists often note that there is more than one way to
skin a cat.
-
8/3/2019 Health Economics- Lecture Ch06
4/42
Suppose that when treating one case, it is not possible to
substitute any nurse hours for any physician hours:
Q=1
nurse hours
physicianhours
n1
p1
n2
Inputs are needed
in a fixed
combination of
p1/n1.
-
8/3/2019 Health Economics- Lecture Ch06
5/42
Suppose that there is some degree of substitutability for
nurse hours and physician hours when treating one case.
Q=1
nurse hours
physicianhours
n1
p1
n2
The rate of substitution
changes as we move
along the curve.
Even though
substitution is possible,
nurses and doctors are
not equivalent.p2
AB
-
8/3/2019 Health Economics- Lecture Ch06
6/42
What degree of substitution is possible?
The work done by economists suggests that substitution
possibilities could be substantial.
Depending on the number of physician hours employed,
one physician extender could substitute for 25 percent to
more than 50 percent of a physicians services.
(Brown,1988; Deb and Holmes, 1998; Liang and
Ogur, 1987; Okunade and Suraratdecha, 1998)
-
8/3/2019 Health Economics- Lecture Ch06
7/42
- look at elasticity of substitution (s )
- measures the responsiveness of a (cost-
minimizing) firm to changes in relative input prices
iceRatioFactor
tRatioFactorInpus
Pr%
%
(
(!I
The larger the value of , the greater the substitutability.
If a firm is a cost-minimizer, then it would respond to
changes in input prices. It would tend to shift from thecostlier
input to the relatively cheaper one.
-
8/3/2019 Health Economics- Lecture Ch06
8/42
Example:- Suppose in order to treat 75 cases, a hospital
employs
100 nurses and 100 physicians.
-The annual salary for a physician is $200,000 and is
$40,000 for a nurse.- Suppose that the elasticity of
substitution is 0.6.
If each physicians salary increases by $20,000, how willthe
hospital respond?
-
8/3/2019 Health Economics- Lecture Ch06
9/42
Q=75
nurses
physicians
100
100
n2
p2A
B
Intuitively we know that this hospitalwill substitute away from
physicians
and use more nurses.
-
8/3/2019 Health Economics- Lecture Ch06
10/42
To find the new number of nurses and doctors, we need
to calculate the %Factor Input Ratio.
We know = 0.60.
We can calculate the % Factor Price Ratio because we
have salary data.
initial factor price ratio = 200,000 / 40,000 = 5
new factor price ratio = 220,000 / 40,000 = 5.5
% factor price ratio = 5.5 5 x 100 = 10%5
-
8/3/2019 Health Economics- Lecture Ch06
11/42
0.60 = % factor input ratio
10%
6% = % factor input ratio
The initial factor input ratio = 100/100 = 1
The new factor input ratio = 1 (1)(0.06) = 0.94
So the ratio of physicians to nurses now = 0.94. If the
hospital uses one less doctor, what does that mean?
0.94 = 99
#N #N = 105
-
8/3/2019 Health Economics- Lecture Ch06
12/42
So, in response to the increase in physicians salaries, the
hospital can use 5 nurses to substitute for one physician.
Change in cost to the hospital from the substitution:save
$220,000 from not paying 1 physician
costs ($40,000 )(5) = $200,000 for the new nurses
net savings of $20,000
-
8/3/2019 Health Economics- Lecture Ch06
13/42
Q=75
nurses
physicians
100
100
105
99A
B
-
8/3/2019 Health Economics- Lecture Ch06
14/42
Empirical Evidence for Input Substitution in Hospitals
-
8/3/2019 Health Economics- Lecture Ch06
15/42
II. Costs
production function: relates inputs to output
cost function: relates costs to output
Theoretically speaking, the cost function is only validfor
cost-minimizing firms.
Do non-profits minimize costs?
Recall that the firms problem is to produce a certain
level of output at the minimum cost.
-
8/3/2019 Health Economics- Lecture Ch06
16/42
The expansion path C-F-G
shows the cost-minimizing
combinations of capital
and labor that can be usedto produce 100, 150 and
200 physician office visits,
respectively.
-
8/3/2019 Health Economics- Lecture Ch06
17/42
Suppose we are given the input prices
r = $1,200 and w = $1,000
The cost of producing 100, 150 and 200 physician visits
would be:
100: 20(1000) + 25(1200) =$50,000
150: 30(1000) + 40(1200) =
$78,000
150: 45(1000) + 50(1200) =
$105,000
-
8/3/2019 Health Economics- Lecture Ch06
18/42
-
8/3/2019 Health Economics- Lecture Ch06
19/42
This total cost curve leads to an average cost curve
like this one.
-
8/3/2019 Health Economics- Lecture Ch06
20/42
Economies of Scale: exist over the range of output
where a firms long run average costs are falling
(as a firm gets larger / produces more output, its averagecosts
fall)
LRAC
AC
($)
Q
AC1
AC3
AC2
Q1 Q2 Q3
How does
this relateto health
care?
-
8/3/2019 Health Economics- Lecture Ch06
21/42
Economies of Scope: exist when the joint production of twogoods
costs less than producing each good separately
- only possible for multi-product firms
ex: pediatric care and geriatric careQp = 100 Qg = 150
If the following is true, then economies of scope exist:
TC( Qp=100, Qg=150) < TC(Qp=100, Qg=0) + TC(Qp=0, Qg=150)
-
8/3/2019 Health Economics- Lecture Ch06
22/42
Issues in Hospital Cost Studies
a. Long Run vs Short Run
- clear in theory, what about in practice?
b. Structural vs Behavioral cost functions
- Structural functions are derived from economic theory.
(isoquant, isocost)
- Behavioral functions are an analysis of patterns in actual
cost data.
-
8/3/2019 Health Economics- Lecture Ch06
23/42
c. difficulties in all hospital studies
- What do hospitals produce?
(face very different case mixes)
LRAC for H3(very complicated)
LRAC for H2(somewhat complicated)
LRAC for H1(not complicated)
Q
AC
($)E
D
C
Estimated LRAC
-
8/3/2019 Health Economics- Lecture Ch06
24/42
- How to treat quality?
- Lacking in reliable measures of hospital input prices.
- Physician input prices are omitted.
-
8/3/2019 Health Economics- Lecture Ch06
25/42
Research Findings:
The most recent research supports claims thateconomies of scale
exist in hospitals.
Preya and Pink (2006) studied costs of Canadian
hospitals prior to a massive consolidation, findinglarge scale
unexploited gains to strategic
consolidation in the hospital sector.
Dranove and Lindrooth (2003) studied a large numberof hospital
consolidations, they found significant,
robust, and persistent savings for mergers, 2, 3, and 4
years after consolidation.
-
8/3/2019 Health Economics- Lecture Ch06
26/42
III. Efficiency
Technical Inefficiency: a producer is not achieving the
maximum output for a given input combination.
-production within a certain firm
-
8/3/2019 Health Economics- Lecture Ch06
27/42
Allocative Efficiency: requires the efficient allocation
ofinputs between firms, and between outputs.
Economic theory says that allocative efficiency will result
when:
- inputs are purchased in competitive markets
- firms are minimizing production cost
Each firm must respond optimally to changes in input
prices.
-
8/3/2019 Health Economics- Lecture Ch06
28/42
-
8/3/2019 Health Economics- Lecture Ch06
29/42
Empirical Techniques for evaluating efficiency:frontier and
non-frontier
Frontier: actual output or costs are compared to the best
possible situation
Non-Frontier: actual output or costs for two or more
groups of firms are compared, controlling for other
variables
We will focus only on frontier.
-
8/3/2019 Health Economics- Lecture Ch06
30/42
Frontier: Data Envelopment Analysis (DEA)
- the frontier for production is initially unknown
- it is revealed as firms are observed- linear programming is
used to construct the
outer shell of data points
Technicalinefficiency is
measured as the
distance from the
frontier.
-
8/3/2019 Health Economics- Lecture Ch06
31/42
Notable drawback: assumes all firms that are not on
the frontier are inefficient
Notable feature: do not need to make any assumptions
about the underlying distribution of inefficiency
non-parametric
-
8/3/2019 Health Economics- Lecture Ch06
32/42
Frontier: Stochastic Frontier Analysis (SFA)
- each firm is treated uniquely
- assume each firm will be affected by a shock
to its ability to provide care
- when a firm is randomly shocked (to alter its
production and cost), its best possible practice
(frontier) is randomly shifted
- when a frontier function is partially random,
it is a stochastic process
-
8/3/2019 Health Economics- Lecture Ch06
33/42
-
8/3/2019 Health Economics- Lecture Ch06
34/42
Notable drawback: need to guess in advance the
distribution of inefficiency
Notable feature: treats each firm uniquely
DEA andSFA areoftenusedascomplementarytools.
-
8/3/2019 Health Economics- Lecture Ch06
35/42
Results of Hospital Efficiency Studies:
Reported overall efficiency has been quite high.
The earliest DEA study (Valdmanis, 1990) reported
technical efficiency levels of about 90 percent, while
Magnussons DEA (1996) study reached similarly highlevels.
SFA studies have tended toward similar levels; early
SFA studies (Zuckerman, Hadley, and Iezzoni, 1994;and Folland
and Hofler, 2001) found the sum of
technical and allocative inefficiency to be only a little
more than 10 percent.
-
8/3/2019 Health Economics- Lecture Ch06
36/42
For-Profit vs Non-Profit Hospitals
In nearly all recent studies, nonprofit and for-profit
hospitals appear approximately equal in efficiency.
While the earliest studies (Valdmanis, 1990; and Ozcan
et al., 1992) found differences between samples of
public and for-profit hospitals, studies since then found
no significant differences (Sloan et al., 2001).
Burgess and Wilson (1998) concluded: We find no
evidence that differences in ownership affect technical
efficiency after controlling for other factors.
-
8/3/2019 Health Economics- Lecture Ch06
37/42
Inefficiency and Quality
Deily and McKay (2006) explain that hospitalinefficiency may
reduce the quality of care. -
inefficiency measure was a highly significant and
positive contributor to a measure of hospital
mortality rates.
Laine and colleagues (2005) attempted similar tests for
long-term care.
- no inefficiency effect on clinical quality,- inefficiency
contributes to the prevalence of
pressure ulcers, indicating poor quality of care
was associated with technical inefficiency.
-
8/3/2019 Health Economics- Lecture Ch06
38/42
IV. Technology
A. Technology and CostsDoes technological change increase or
decrease costs?
- if productivity is raised, then costs are lower
- if quality is improved, then costs can be higher
Holding quality constant, technological change means it
is less costly to produce a given level of output.
However, technology may change the mix of products or
services available, which may increase or decrease the
cost of treating a patient.
-
8/3/2019 Health Economics- Lecture Ch06
39/42
Measuring the cost of treatment can be difficult.
- treatments change over time
- effectiveness of treatment changes- quality changes
-
8/3/2019 Health Economics- Lecture Ch06
40/42
B. Who adopts new technology and why?
1. Profit principle: adopt if revenues are expected to
increase
2. Information channels: emphasizes the role of friends/
colleagues/journals/etc in decision making
3. Theory of innovation: adopt when PV of future profits
is greater than zero
- wait too long, miss out
- wait somewhat, gain from others experience
4. Managed care: flattening of incentives can decrease
interest in switching technologies
-
8/3/2019 Health Economics- Lecture Ch06
41/42
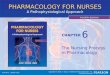
Classic Pattern of Adoption
(logistic function)
-
8/3/2019 Health Economics- Lecture Ch06
42/42
Summary:
The production function, which summarizes the
relationship of inputs and outputs, also embodies the
technology.
Technology that permits substitution between inputs
provides better flexibility to the manager.
Cost estimation describes the cost curves, which identify
the economies of scale and scope.
Health firms may differ in technology because the
adoption of new technologies differs among firms and is
never instantaneous