Embed Size (px)
Citation preview

Policy Statement—Child Passenger Safety
abstractChild passenger safety has dramatically evolved over the past de-cade; however, motor vehicle crashes continue to be the leadingcause of death of children 4 years and older. This policy statementprovides 4 evidence-based recommendations for best practices inthe choice of a child restraint system to optimize safety in passen-ger vehicles for children from birth through adolescence: (1) rear-facing car safety seats for most infants up to 2 years of age; (2)forward-facing car safety seats for most children through 4 yearsof age; (3) belt-positioning booster seats for most children through8 years of age; and (4) lap-and-shoulder seat belts for all who haveoutgrown booster seats. In addition, a fifth evidence-based recom-mendation is for all children younger than 13 years to ride in therear seats of vehicles. It is important to note that every transition isassociated with some decrease in protection; therefore, parentsshould be encouraged to delay these transitions for as long aspossible. These recommendations are presented in the form of analgorithm that is intended to facilitate implementation of the rec-ommendations by pediatricians to their patients and families andshould cover most situations that pediatricians will encounter inpractice. The American Academy of Pediatrics urges all pediatri-cians to know and promote these recommendations as part of childpassenger safety anticipatory guidance at every health-supervisionvisit. Pediatrics 2011;127:788–793
Improved vehicle crashworthiness and greater use of child restraintsystems have significantly affected the safety of children in automo-biles. Major shifts in child restraint use, particularly the use of boosterseats among older children, have occurred in response to public edu-cation programs and enhancements to child restraint laws in nearlyevery state.1–3 In addition, there has been a substantial increase inscientific evidence on which to base recommendations for best prac-tices in child passenger safety. Current estimates of child restrainteffectiveness indicate that child safety seats reduce the risk of injuryby 71% to 82%4,5 and reduce the risk of death by 28% when comparedwith those for children of similar ages in seat belts.6 Booster seatsreduce the risk of nonfatal injury among 4- to 8-year-olds by 45%compared with seat belts.7 Despite this progress, approximately1500 children younger than 16 years die in motor vehicle crasheseach year in the United States, nearly half of whom were completelyunrestrained.8
The American Academy of Pediatrics (AAP) strongly supports optimalsafety for children and adolescents of all ages during all forms of travel.
COMMITTEE ON INJURY, VIOLENCE, AND POISON PREVENTION
KEY WORDSchild passenger safety, motor vehicle crash, child restraintsystem
ABBREVIATIONSAAP—American Academy of PediatricsCSS—car safety seat
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict of interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-0213
doi:10.1542/peds.2011-0213
All policy statements from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
Organizational Principles to Guide and Define the ChildHealth Care System and/or Improve the Health of all Children
788 FROM THE AMERICAN ACADEMY OF PEDIATRICS by guest on February 26, 2020www.aappublications.org/newsDownloaded from

This policy statement provides 5evidence-based recommendations forbest practices to optimize safety in pas-
senger vehicles for all children, frombirth through adolescence (a summaryof recommendations is listed in Table 1):
1. All infants and toddlers should ridein a rear-facing car safety seat(CSS) until they are 2 years of age
TABLE 1 Summary of Best-Practice Recommendations
Best-Practice Recommendation Complementary Information
All infants and toddlers should ride in a rear-facing car safety seat(CSS) until they are 2 y of age or until they reach the highestweight or height allowed by the manufacturer of their CSS.
Infant-only seats usually have a handle for carrying and can be snappedin and out of a base that is installed in the vehicle. They can only beused rear-facing. Convertible CSSs can be used either forward- orrear-facing and typically have higher rear-facing weight and heightlimits than infant-only seats.When children using infant-only seats reach the highest weight for theirseat, they should continue to ride rear-facing in a convertible seat foras long as possible. Most currently available convertible seats can beused rear-facing to at least 35 lb.
Combination CSSs are seats that can be used forward-facing with aharness system and then, when the child exceeds the height orweight limit for the harness, as a booster seat with the harnessremoved.
All children 2 y or older, or those younger than 2 y who have outgrownthe rear-facing weight or height limit for their CSS, should use aforward-facing CSS with a harness for as long as possible, up to thehighest weight or height allowed by the manufacturer of their CSS.
Several models of convertible and combination CSSs can accommodatechildren up to 65 or 80 lb when used forward-facing. The lowestmaximum weight limit for currently available forward-facing CSSs is40 lb.
All children whose weight or height is above the forward-facing limitfor their CSS should use a belt-positioning booster seat until thevehicle lap-and-shoulder seat belt fits properly, typically when theyhave reached 4 feet 9 inches in height and are between 8 and 12 yof age.
There is a safety advantage for young children to remain in CSSs with aharness for as long as possible before transitioning to booster seats.
When children are old enough and large enough to use the vehicleseat belt alone, they should always use lap-and-shoulder seat beltsfor optimal protection.
Booster seats function by positioning the child so that both the lap andshoulder portions of the vehicle seat belt fit properly; the lap portionof the belt should fit low across the hips and pelvis, and the shoulderportion should fit across the middle of the shoulder and chest. Theycome in both high-back (a seat back that extends up beyond thechild’s head) and backless models.The lap portion of the belt should fit low across the hips and pelvis, andthe shoulder portion should fit across the middle of the shoulder andchest when the child sits with his or her back against the vehicleseat back. If they do not, then the child is likely too small to use thevehicle seat belt alone and should continue to use a belt-positioningbooster seat.
CSSs should be installed tightly either with the vehicle seat belt or withthe LATCH system, if available. LATCH is a system of attaching a CSS tothe vehicle that does not use the seat belt. It was designed to easeinstallation of the CSS. Whether parents use LATCH or the seat belt, theyshould always ensure a tight installation of the CSS into the vehicle.
All children younger than 13 y should be restrained in the rear seatsof vehicles for optimal protection.
LATCH indicates lower anchors and tethers for children.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 127, Number 4, April 2011 789 by guest on February 26, 2020www.aappublications.org/newsDownloaded from

or until they reach the highestweight or height allowed by themanufacturer of their CSS.
2. All children 2 years or older, orthose younger than 2 years whohave outgrown the rear-facingweight or height limit for theirCSS, should use a forward-facingCSS with a harness for as long as
possible, up to the highest weightor height allowed by the manufac-turer of their CSS.
3. All childrenwhoseweight or height isabove the forward-facing limit fortheir CSS should use a belt-positioning booster seat until the ve-hicle lap-and-shoulder seat belt fitsproperly, typically when they have
reached 4 feet 9 inches in height andare between 8 and 12 years of age.
4. When children are old enough andlarge enough to use the vehicle seatbelt alone, they should always uselap-and-shoulder seat belts for opti-mal protection.
5. All children younger than 13 yearsshould be restrained in the rear
FIGURE 1Algorithm to guide the implementation of best-practice recommendations for optimal child passenger safety (see Table 1 for a summary of recommenda-tions and Table 2 for definitions and explanations).
790 FROM THE AMERICAN ACADEMY OF PEDIATRICS by guest on February 26, 2020www.aappublications.org/newsDownloaded from
seats of vehicles for optimalprotection.
It should be noted that the recom-mendation that all children youngerthan 2 years be restrained in aninfant-only or convertible CSS usedrear-facing represents a significantchange from previous AAP policy andis based on new data from the UnitedStates9 as well as extensive experi-
ence in Sweden.10,11 It is important tonote that most currently availableCSSs have weight limits for rear-facing use that can accommodatethe new recommendations.12
Certain considerations contained in thispolicy statement are relevant to com-mercial airline travel as well and arenoted in the accompanying technical re-port.13 Other AAP policy statements pro-
vide specific recommendations to opti-mize safety for preterm and low birthweight infants,14 children in schoolbuses,15 and children using other formsof travel and recreational vehicles.16–18 Inaddition, complementary AAP policystatements provide recommendationsfor teenaged drivers19 and the safetransport of newborn infants20 and chil-drenwith special health care needs.21,22
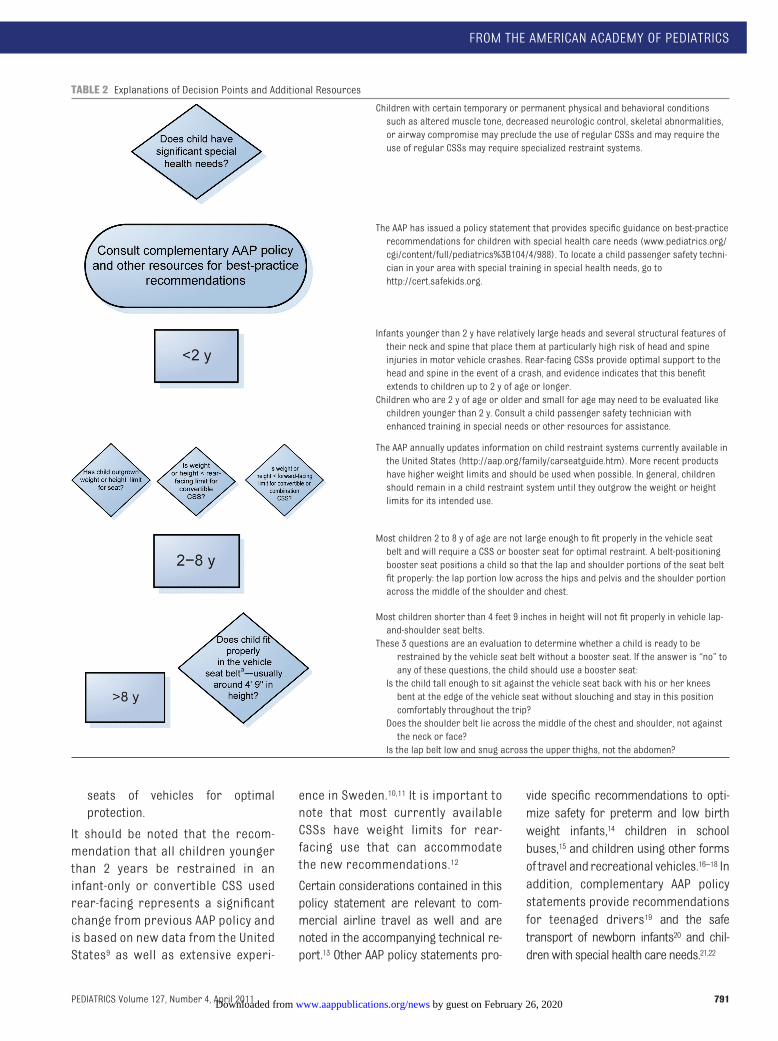
TABLE 2 Explanations of Decision Points and Additional Resources
Children with certain temporary or permanent physical and behavioral conditionssuch as altered muscle tone, decreased neurologic control, skeletal abnormalities,or airway compromise may preclude the use of regular CSSs and may require theuse of regular CSSs may require specialized restraint systems.
The AAP has issued a policy statement that provides specific guidance on best-practicerecommendations for children with special health care needs (www.pediatrics.org/cgi/content/full/pediatrics%3B104/4/988). To locate a child passenger safety techni-cian in your area with special training in special health needs, go tohttp://cert.safekids.org.
Infants younger than 2 y have relatively large heads and several structural features oftheir neck and spine that place them at particularly high risk of head and spineinjuries in motor vehicle crashes. Rear-facing CSSs provide optimal support to thehead and spine in the event of a crash, and evidence indicates that this benefitextends to children up to 2 y of age or longer.Children who are 2 y of age or older and small for age may need to be evaluated likechildren younger than 2 y. Consult a child passenger safety technician withenhanced training in special needs or other resources for assistance.
The AAP annually updates information on child restraint systems currently available inthe United States (http://aap.org/family/carseatguide.htm). More recent productshave higher weight limits and should be used when possible. In general, childrenshould remain in a child restraint system until they outgrow the weight or heightlimits for its intended use.
Most children 2 to 8 y of age are not large enough to fit properly in the vehicle seatbelt and will require a CSS or booster seat for optimal restraint. A belt-positioningbooster seat positions a child so that the lap and shoulder portions of the seat beltfit properly: the lap portion low across the hips and pelvis and the shoulder portionacross the middle of the shoulder and chest.
Most children shorter than 4 feet 9 inches in height will not fit properly in vehicle lap-and-shoulder seat belts.These 3 questions are an evaluation to determine whether a child is ready to berestrained by the vehicle seat belt without a booster seat. If the answer is “no” toany of these questions, the child should use a booster seat:Is the child tall enough to sit against the vehicle seat back with his or her kneesbent at the edge of the vehicle seat without slouching and stay in this positioncomfortably throughout the trip?Does the shoulder belt lie across the middle of the chest and shoulder, not againstthe neck or face?Is the lap belt low and snug across the upper thighs, not the abdomen?
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 127, Number 4, April 2011 791 by guest on February 26, 2020www.aappublications.org/newsDownloaded from

Pediatricians play a critical role in pro-moting child passenger safety. To facil-itate their widespread implementationin practice, evidence-based recom-mendations for optimal protection ofchildren of all ages in passenger vehi-cles are presented in the form of analgorithm (Fig 1) with an accompany-ing table of explanations and defini-tions (Table 2). A summary of theevidence in support of these recom-mendations is provided in the accom-panying technical report.13 Becausepediatricians are a trusted source ofinformation to parents, every pediatri-cian must maintain a basic level ofknowledge of these best-practice rec-ommendations and promote anddocument them at every health-supervision visit. Prevention of motorvehicle crash injury is unique in health-supervision topics, because it is theonly topic recommended at everyhealth-supervision visit by Bright Fu-tures.23 Pediatricians can also use thisinformation to promote child passen-ger safety public education, legisla-tion, and regulation at local, state, andnational levels through a variety of ad-vocacy activities, including ensuringthat their state’s child passengersafety law is in better alignment with
the best-practice recommendationspromoted in this policy statement.
Because motor vehicle safety for chil-dren is multifaceted and will continueto evolve, all pediatricians should fa-miliarize themselves with additionalresources to address unique situa-tions for their patients that may not becovered by the algorithm and to main-tain current knowledge. In particular,many communities have child passen-ger safety technicians who have com-pleted a standardized National High-way Traffic Safety Administration(NHTSA) course and who can providehands-on advice and guidance to fam-ilies. In most communities, child pas-senger safety technicians work at for-mal inspection stations; a list of thesestations is available at www.seat-check.org. If your community does nothave an inspection station, you canfind a child passenger safety techni-cian in your area on the National ChildPassenger Safety Certification Website (http://cert.safekids.org) or theNHTSA child safety seat inspectionstation locator (www.nhtsa.dot.gov/cps/cpsfitting/index.cfm). Car seatcheckup events are updated at www.safekidsweb.org/events/events.asp. Inaddition, additional resources for pedi-atricians and families can be found at
www.aap.org or www.healthychildren.org.
LEAD AUTHORDennis R. Durbin, MD, MSCE
COMMITTEE ON INJURY, VIOLENCE,AND POISON PREVENTION, 2008–2010H. Garry Gardner, MD, ChairpersonCarl R. Baum, MDM. Denise Dowd, MD, MPHDennis R. Durbin, MD, MSCEBeth E. Ebel, MDMichele Burns Ewald, MDRichard Lichenstein, MDMary Ann P. Limbos, MDJoseph O’Neil, MD, MPHElizabeth C. Powell, MDKyran P. Quinlan, MD, MPHSeth J. Scholer, MD, MPHRobert D. Sege, MD, PhDMichael S. Turner, MDJeffrey Weiss, MD
CONTRIBUTORStuart Weinberg, MD – Partnership for PolicyImplementation (PPI)
LIAISONSJulie Gilchrist, MD – Centers for DiseaseControl and PreventionLynne Janecek Haverkos, MD – Eunice KennedyShriver National Institute of Child Healthand Human DevelopmentJonathan D. Midgett, PhD – Consumer ProductSafety CommissionAlexander S. Sinclair – National HighwayTraffic Safety AdministrationNatalie L. Yanchar, MD – Canadian PaediatricSociety
STAFFBonnie [email protected]
REFERENCES
1. Durbin DR, Kallan MJ, Winston FK. Trends inbooster seat use among young children incrashes. Pediatrics. 2001;108(6). Availableat: www.pediatrics.org/cgi/content/full/108/6/e109
2. Winston FK, Chen IG, Elliott MR, Arbogast KB,Durbin DR. Recent trends in child restraintpractices in the United States. Pediatrics.2004;113(5). Available at: www.pediatrics.org/cgi/content/full/113/5/e458
3. Insurance Institute for Highway Safety.Child restraint/belt use laws. Available at:www.iihs.org/laws/restraintoverview.aspx.Accessed August 17, 2010
4. Arbogast KB, Durbin DR, Cornejo RA, KallanMJ, Winston FK. An evaluation of the effective-ness of forward facing child restraint sys-tems. Accid Anal Prev. 2004;36(4):585–589
5. Zaloshnja E, Miller TR, Hendrie D. Effective-ness of child safety seats vs safety belts forchildren aged 2 to 3 years. Arch PediatrAdolesc Med. 2007;161(1):65–68
6. Elliott MR, Kallan MJ, Durbin DR, Winston FK.Effectiveness of child safety seats vs seatbelts in reducing risk for death in childrenin passenger vehicle crashes [publishedcorrection appears in Arch Pediatr AdolescMed. 2006;160(9):952]. Arch Pediatr Ado-lesc Med. 2006;160(6):617–621
7. Arbogast KB, Jermakian JS, Kallan MJ,Durbin DR. Effectiveness of belt positioningbooster seats: an updated assessment. Pe-diatrics. 2009;124(5):1281–1286
8. National Highway Traffic Safety Administra-tion. FARS encyclopedia. Available at: www-fars.nhtsa.dot.gov. Accessed August 17, 2010
9. Henary B, Sherwood CP, Crandall JR, et al.Car safety seats for children: rear facing forbest protection. Inj Prev. 2007;13(6):398–402
10. Isaksson-Hellman I, Jakobsson L, Gustafs-son C, Norin HA. Trends and effects of childrestraint systems based on Volvo’s Swedishaccident database. In: Proceedings of ChildOccupant Protection 2nd Symposium. War-rendale, PA: Society of Automotive Engi-neers Inc; 1997:316
11. Jakobsson L, Isaksson-Hellman I, LundellB. Safety for the growing child: experi-ences from Swedish accident data [Abstr05-0330]. In: Proceedings: 19th Interna-tional Technical Conference on the En-hanced Safety of Vehicles. Washington,DC: National Highway Traffic SafetyAdministration; 2005
792 FROM THE AMERICAN ACADEMY OF PEDIATRICS by guest on February 26, 2020www.aappublications.org/newsDownloaded from

12. American Academy of Pediatrics. Car safetyseats: product listing for 2011. Available at:www.healthychildren.org/carseatlist. Ac-cessed January 7, 2011
13. Durbin DR; American Academy of Pediatrics,Committee on Injury, Violence, and PoisonPrevention. Technical report: child passen-ger safety. Pediatrics. 2011;127(4). Avail-able at: www.pediatrics.org/cgi/content/full/127/4/eXXX
14. Bull MJ, Engle WA; American Academy of Pe-diatrics, Committee on Injury, Violence, andPoison Prevention and Committee on Fetusand Newborn. Safe transportation of pre-term and low birth weight infants at hospi-tal discharge. Pediatrics. 2009;123(5):1424–1429
15. American Academy of Pediatrics, Commit-tee on Injury, Violence, and Poison Preven-tion, Council on School Health. School trans-
portation safety. Pediatrics. 2007;120(1):213–220
16. American Academy of Pediatrics, Commit-tee on Injury and Poison Prevention. All-terrain vehicle injury prevention: two-,three-, and four-wheeled unlicensed motorvehicles. Pediatrics. 2000;105(6):1352–1354
17. American Academy of Pediatrics, Commit-tee on Injury and Poison Prevention. Bicy-cle helmets. Pediatrics . 2001;108(4):1030–1032
18. American Academy of Pediatrics, Commit-tee on Injury and Poison Prevention. Per-sonal watercraft use by children and ado-lescents. Pediatrics. 2000;105(2):452–453
19. American Academy of Pediatrics, Commit-tee on Injury, Violence, and Poison Preven-tion and Committee on Adolescence. Theteen driver. Pediatrics . 2006;118(6):2570–2581
20. American Academy of Pediatrics, Commit-tee on Injury and Poison Prevention. Safetransportation of newborns at hospitaldischarge. Pediatrics . 1999;104(4) :986 –987
21. American Academy of Pediatrics, Commit-tee on Injury and Poison Prevention. Schoolbus transportation of children with specialhealth care needs. Pediatrics. 2001;108(2):516–518
22. American Academy of Pediatrics, Commit-tee on Injury and Poison Prevention.Transporting children with special healthcare needs. Pediatrics. 1999;104(4 pt 1):988 –992
23. American Academy of Pediatrics. BrightFutures: health care professionals toolsand resources Web site. Available at: http://brightfutures.aap.org. Accessed August 17,2010
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 127, Number 4, April 2011 793 by guest on February 26, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2011-0213 originally published online March 21, 2011; 2011;127;788Pediatrics
Committee on Injury, Violence, and Poison PreventionChild Passenger Safety
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/127/4/788including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/127/4/788#BIBLThis article cites 14 articles, 11 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/current_policyCurrent Policyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on February 26, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2011-0213 originally published online March 21, 2011; 2011;127;788Pediatrics
Committee on Injury, Violence, and Poison PreventionChild Passenger Safety
http://pediatrics.aappublications.org/content/127/4/788located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2011 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on February 26, 2020www.aappublications.org/newsDownloaded from