Embed Size (px)
Citation preview

Health Care Reform in the States
Government Research AssociationAnnual Conference
July 27, 2009Washington, D.C.
Enrique Martinez-VidalVice President, AcademyHealthDirector, State Coverage Initiatives

State Coverage Initiatives (SCI)
An Initiative of the Robert Wood Johnson Foundation
Community of State OfficialsConvening state officials
Resources and InformationWeb site: www.statecoverage.orgState ProfilesPublications/State of the States
Direct technical assistance to statesState-specific help, research on state policymakers’
questions Grant funding/Coverage Institute

Overview of Presentation
• Background• State Reform Strategies• Specific State Examples• Lessons Learned from State Reforms• Conclusion

14.9 17.7
The Non-Elderly as a Share of the Population and by Poverty Level, 2007
11%
29%

Drivers of State Health Reform Efforts
Uninsured still high Employer-sponsored insurance down Costs/premiums increasingly
unaffordable – Indiv; Families; Govt Coverage needed for effective and
efficient health care system Lack of national consensus – future? Greater political will at state level

Key Policy and Design Issues Different Populations Require Different Solutions Subsidies and Financing: Who will pay? Who will
benefit? Should Health Insurance Coverage Be Required? What is Affordable Coverage? What is the Most Appropriate Benefit Design? Do Insurance Markets Need to be
Reformed/Reorganized? Best Mechanisms for Cost Containment/Systems
Improvement
2008 State of the States(www.statecoverage.org)

What are States Doing to Reform the Health Care
System?

Key Elements of State Reform Strategies
Insurance market reforms
Public program reforms
Benefit design
Decrease insurance costs
Cost containment/system improvement
8

Insurance Market Reforms States use insurance market rules to try to lower premiums,
expand choice of plans/products, and increase efficiencies
Examples Require minimum insurance medical loss ratios: CA, NJ, CO Change definition of “dependents” and extend coverage
beyond the age of 18 for students/non-students: Many states Guaranteed issue: CA No Pre-ex limitations when moving between policies
(including non-group): IA Rating factors/Bands Must offer non-group policies to offer small group policies: NJ Transparency of broker fees/commissions Merge small group and individual markets: MA Purchasing mechanism (Connector): MA, WA High risk pools
9

Public Program Expansions
Increase eligibility levels Buy-in programs (esp. disabled) – sliding scale
premiums Longer eligibility periods (i.e., change from 6
mo. to 12 mo.) Outreach to eligible but not enrolled Streamline/simplify enrollment processes/auto-
enrollment strategies Waivers to support premiums for small
employers
10

Benefit Design Services included/excluded; cost-sharing; structure of access to
providers
Not just cost of coverage but value of the benefit plan – what set of services are purchased for specific amount of money
Before – limit benefits; raise cost-sharing; limit networks (value issue – not worth it)
Levers within benefit design: reduce premiums encourage efficient/appropriate consumer behavior change carrier and provider behavior
Evidence-based benefit design? MN
Consumer-driven health plans? IN
First-dollar benefits? TN
Direct consumer behavior change? RI, MD, NH, FL
11

Decreasing Insurance Costs
Direct and Indirect Subsidies Reinsurance Premium assistance Tax credits
Structural Changes to Lower Premium Costs Section 125 plans: MA, RI, CT, MO Administrative simplification/standardization: MN
12

Cost Containment and Quality Improvement Prioritized by States
2009 State of the States – pp. 54-59 (www.statecoverage.org)
Prevention/primary care/wellness Chronic care management and coordination Public health initiatives Value-based purchasing/payment reforms Medical error reduction/patient safety Health-acquired infection reduction Price and quality transparency Heath information technology and exchange Administrative and regulatory efficiencies

Specific State Examples

Strategies for Comprehensive Reform
Maine Massachusetts Vermont
Individual Mandate
No Yes NoWill consider if
coverage targets not met
Purchasing Mechanism
DirigoChoice Health Insurance Connector
Catamount Health
Subsidies for Low-Income
Up to 300% FPL Up to 300% FPL Up to 300% FPL
Public Program Expansion
Parents <200% FPL
Childless Adults <125% FPL
Adults <100% FPL
Children <300% FPL
Builds upon previous expansions
Children <300%
Parents <185%
Childless Adults <150% FPL
Employer Requirements
VoluntaryParticipating employers must
pay 60% of premium
$295/employee fee for non-offering.
Must offer §125 Plan
$365/FTE fee for non-offering

Massachusetts Pillars of the Reform
Employer Responsibilities Section 125 Plan Requirement Offer Coverage or Be Assessed
Personal Responsibility/Individual Mandate
Expansion of Publicly-subsidized Programs
Major Changes to Insurance Market Merged Small Group and Individual Markets Raising age of dependents – up to 25 Connector – Purchasing Mechanism NOT a Risk Pool

Current State of the Commonwealth
More than 439,000 newly-insured between June 2006 and March 31, 2008
191,000 more in private coverage (no public $$) – more than 40% of all newly covered have no subsidies
Employer-sponsored insurance remains predominant source of coverage (82% of non-elderly): no crowd-out
Non-group premiums are down over 40% and membership has grown over 50%
Approximately 1-2% of the MA population or 60,000 persons may be exempted from the mandate

Oregon: HB 2116 – Expanding Coverage
Children: “Healthy Kids” Access to comprehensive health care coverage for uninsured
Oregon children up to age 19 Options for families at all income levels Simplified application and enrollment processes Enhanced outreach to children in under-served communities Covers 80,000 currently uninsured children
Low-income adults: OHP Standard Covers approximately 60,000 uninsured, low-income adults Provides limited coverage, including medical, emergency dental,
mental health, prescription drug and chemical dependency services
Financing Restructures and renews provider taxes to replace those that
sunset October 1, 2009. Funded by 1% assessment on most health insurance premiums &
2.8% hospital tax on net revenues - combined with matching federal funds.

Oregon: HB 2009 – Setting Reform in Motion I
Streamlines State Health Functions Oregon Health Authority
– Consolidates state health purchasing and aligns programs to maximize efficiencies (including Public Employers Benefits/Oregon Educators/Medicaid/High Risk Pool and Premium subsidy (FHIAP)/Public Health/Mental Health and Addictions)
Oregon Health Policy Board– Guides the Health Authority as it implements reforms to gain value and reduce costs
Insurance Market Pieces Insurance Reform
– Implement value-based small business product– Improve oversight of small group, individual, and portability premium rates– Develop uniform standards for health insurers– Enhance data submitted by Insurers and TPAs
Business Plan for a Health Insurance Exchange due for next legislature’s approval

Oregon: HB 2009 – Setting Reform in Motion II
Gaining Value and Cost Savings Care Coordination:
– Statewide registry of physician orders for life sustaining treatment orders (POLST)
– Implement uniform quality standards and payment reform, starting with primary care and chronic disease
– Uniform use of Evidence-based health care guidelines and comparative effectiveness standards
– Health Information Technology Oversight Council (HITOC) Improved Transparency
– All-claims, all payer database– Public reporting on proposed hospital and ambulatory surgical
center capital projects – Healthcare workforce database and coordinated policy

Colorado Reforms – HB1293 (2009)Provides coverage to more than 100,000 Coloradans through Medicaid/CHIP using a hospital fee
• Generates about $600 million a year. State will receive about the same in federal matching funds.
– Children and pregnant women from 205 to 250 percent FPL – Parents from 60 to 100 percent FPL– Disabled adults and children with incomes up to 450 FPL will
be able to buy into the Medicaid program – Childless adults with incomes up to 100 percent FPL will be
eligible for a new medical assistance program
• Also raises reimbursement for inpatient and outpatient services up to Medicaid’s maximum allowable rate.
• 20 other states have similar fee to collect money for health programs and obtain federal matching funds.

Iowa Reforms – 2008/2009
Coverage for children up to 300% of FPL (with a sliding scale premium between 200-300% FPL) + one-year continuous eligibility
Creates Legislative Health Care Coverage Commission to develop Iowa Health Care Reform Strategic Plan – Final report by 10/11
A Medicaid buy-in option for those with disabilities Modify tax forms to ask if dependent children have insurance Implementation of Medicaid/CHIP performance bonus criteria
(express lane eligibility, paperless renewal verification, etc) Dependent coverage up to 25 years old can stay on parent’s
policy Health Care Workforce Support Initiative Transparency: Create MOU to use IA Hospital Assoc as state’s
intermediary to collect, maintain and disseminate hospital inpatient, outpatient and ambulatory information
A Medical Homes Initiative Healthy Communities Initiative, Quality improvement council,
electronic health plan to be developed

Vermont Blueprint Integrated Pilot Summary1. Financial reform (2 major components - includes MCAID/commercial insurers)
- Payment to practices based on NCQA PCMH score- Shared costs for Community Care Teams
2. Multidisciplinary care support teams (CCT Teams)- Local care support & population management
3. Health Information Technology- Web based clinical tracking system (DocSite)- Visit planners & population reports
- Electronic prescribing- Updated EMRs to match program goals and clinical measures in DocSite - Health information exchange network
4. Community Activation & Prevention - Prevention specialist as part of CCT - Community profiles & risk assessments
- Evidence based interventions
5. Evaluation- NCQA PCMH score (process quality)- Clinical process measures- Health status measures- Multi payer claims data base- Population Indicators

Health IT Framework
Global Information Framework
Evaluation Framework
Operations
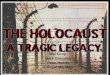
Blueprint Integrated Pilots Coordinated Health System
PCMH
PCMH
PCMH
PCMHHospitals
Public Health Prevention
Community Care TeamNurse Coordinator
Social WorkersDieticians
Community Health WorkersOVHA Care Coordinators
Public Health Prevention Specialist
Mental Health & Substance
Use Disorders
Source: Presentation by Craig Jones, State Coverage Initiatives-Sponsored site visit to
Vermont, June 8-10, 2009

Vermont: Prevention Strategies for Obesity
Menu labeling
Built environment (rail trails)
Community gardens
Changes in school cafeteria
selections (Farm to School)
Running/bike/hiking clubs
Weight control programs
Increased awareness
Health care provider recommendation
Source: Presentation by Craig Jones, State Coverage Initiatives-Sponsored site visit to
Vermont, June 8-10, 2009

Vermont Health Technology Fund
A dedicated fund to support ‘medical health care IT initiatives’ such as
Building health information exchange infrastructure Blueprint for Health IT initiatives Electronic Medical Records for primary care providers Technical assistance to providers in selection, installation and effective use
of IT Funds raised by 0.2% ‘investment fee’ on all medical claims paid
by insurers and TPA’s for 7 years Total 7 year funding of $33 million
2/3 for EMR’s 1/3 for health information exchange and technical assistance

State Medical Home Initiatives
• 31 states have engaged in efforts to implement programs to advance Medical Homes in Medicaid/CHIP
• States working across payers on Medical Homes Programs include Colorado, Louisiana, Maine, New Hampshire, Pennsylvania, Rhode Island, and Vermont
• States with model Medical Homes programs include Vermont, North Carolina, Rhode Island and Pennsylvania
• Medical Home Design Issues: Practice Redesign Consumer Engagement Beyond Primary Care Setting Incentive Alignment Evaluation

Community Care of North Carolina
Source: D. McCarthy and K. Mueller, “Community Care of North Carolina: Building Community Systems of Care Through State and Local
Partnerships,” Case Study, Organized Health Care Delivery System. The Commonwealth Fund. Jan. 2009
14 networks, > 1,300 primary care practices, 3,500-4,000 physicians
$3 PMPM to each network for nurse case management
Hire case managers/medical management staff
$2.50 PMPM to each PCP to serve as medical home and population-management activities
Care improvement: asthma, diabetes, prescription advantage list, nursing home poly-pharmacy initiative
Medical Home: providing acute and preventive services and facilitating patient access to care through referrals and after-hours coverage
Mental Health Integration: 4 CCNC networks have integrated mental health care into routine medical care
HealthNet Collaborative: integrated networks of care for uninsured adults; states provide technical assistance and funding to support 16 networks to serve uninsured adults up to 200% FPL
Studies conducted by Mercer documented that CCNC saved the state up to $314m in FY2006

Pennsylvania Chronic Care Initiative Created by Gov. Rendell, May 2007 to improve chronic care
delivery 45 Commission members, with 5 subcommittees: practice redesign, incentive
alignment, performance measurement, pooled claims database, consumer engagement
Model incorporates features of the Chronic Care Model and the Patient-Centered Medical Home
Four planned regional rollouts Southeast (5/08), South Central (2/09); Southwest and Northeast forthcoming
PCP practices must: attend “learning collaborative” meetings; work with practice coaches; use a patient registry and report data; achieve Level 1 NCQA PPC-PCMH Recognition within 12 months; reinvest funds into the site
Payers must: give a 3yr commitment; payment to IPIP for practice coaches; payment to PCP to offset costs
Source: Richard Snyder ”Pennsylvania’s Chronic Care Management, Reimbursement and Cost Reduction Commission,” presentation February 10-
11, 2009 and Michael Bailit “Overview of Medical Home Projects and Demonstrations to Date,” presentation March 2, 2009

Lessons Learned in State Reform Efforts
2009 State of the States – pp. 20-25(www.statecoverage.org)

Comprehensive Reform is Possible: Massachusetts Shows the Way
Massachusetts’ passage of universal reform in 2006, demonstrated bi-partisan support for broad reform is possible
Massachusetts public-private plan represents compromise between single payer and strict market-based approaches.
This approach has been broadly accepted and incorporated into other comprehensive reform proposals.

Compromise and Consensus Building Though consensus on the necessity of reform is
growing, significant political hurdles still hinder reform in many states.
There are a number of lessons learned from the states related to building stakeholder support:
Leadership is essential Be inclusive Build relationships early Find supporters wherever possible Get supporters on the record Keep your eyes on the prize(s): big picture & perfect vs good
States have established a consensus-building process for many reasons
Consensus building is not a magic bullet

No Free Solutions: Who Will Pay? Who Will Benefit?
Shared responsibility – Who helps cover the costs? Individuals; Employers; Federal government; State government;
Health plans/insurers; Providers Potential downside: “shared responsibility” means “shared pain”
Enough money in current system? If yes, then – Redistribution (Who will pay? Who will get paid?) States have attempted to recoup savings from the system:
• Maine and the Savings Offset Payment (SOP)• Minnesota’s 2008 health reform law
If not, then need new forms of revenue: Sin taxes; Sodas; Provider taxes; Payroll taxes; Lease lottery; Slots revenues; Gross Receipts Tax

Sustained Effort Needed
Health reform takes sustained effort/built on previous efforts, financing mechanisms Massachusetts New Jersey, Iowa, and Wisconsin Oregon, Colorado, and New Mexico
Sustained effort during implementation of reform is especially critical. To ensure success of reform: Outreach and education are crucial Strong evaluation mechanisms which allow reform
to be adapted as it moves forward

A Sense of Urgency Creates Opportunity
Massachusetts reforms propelled by potential to lose federal funds
Other states seek way to create similar sense of urgency
Comprehensive reform will remain difficult without a sense of urgency or a sense of inevitability as many stakeholders are invested in status quo

Individual Mandate Voluntary strategies will not result in universal
coverage - some states are beginning to recognize the need for mandatory participation - Massachusetts
Unenforceable? Impingement on individual freedom? Money for subsidies?
Those pursuing individual mandate must consider: Affordability of mandate Richness of benefits package How to enforce mandate
Though there are significant policy challenges, there are also notable benefits:
Distribution of risk Fairness “System-ness”

Relationship Btw Reducing Costs, Improving Quality & Expanding Coverage Little success so far in addressing underlying cost of
health care but a new focus on chronic care management/preventive care holds potential
Massachusetts leads on health coverage reform, while Minnesota is at the forefront of cost containment
The trend in states is to address access, systems improvement, cost containment simultaneously—concern about long-term sustainability of coverage programs and improved population health
Concerns about rising costs are an impetus for reform, but cost cutting is likely to raise opposition from various stakeholders.

Conclusion: States Can Advance Reform Initiatives But Need Federal Support
States face growing pressures for reform Uninsurance continues to rise as ESI declines Cost increases threaten state budgets and capacity to sustain
Medicaid/SCHIP
States play critical role in moving the conversations about coverage expansions Testing new ideas (politically and practically) Creating momentum for national policy solution
States cannot achieve universal coverage without a federal framework and funding BUT remember variation
State and National: Comprehensive reforms need sequencing Sequential = incremental with a vision
38