-
Health care disparities Stereotyping and unconscious biasHarry
PomeranzMercy CollegeOctober 2008
-
Do you think the average African American is better off, worse
off, or just about as well off as the average white person in terms
of access to health care?
-
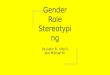
Black and White Differences in Specialty Procedure Utilization
Among Medicare Beneficiaries Age 65 and Older, 1993
-
Black
White
Black-to-
White Ratio
Angioplasty
(procedures per 1,000 beneficiaries per year)
2.5
5.4
0.46
Coronary Artery Bypass Graft Surgery
(procedures per 1,000 beneficiaries per year)
1.9
4.8
0.40
Mammography
(procedures per 100 women per year)
17.1
26.0
0.66
Hip Fracture Repair
(procedures per 100 women per year)
2.9
7.0
0.42
Amputation of All or Part of Limb
(procedures per 1,000 beneficiaries per year)
6.7
1.9
3.64
Bilateral Orchiectomy
(procedures per 1,000 beneficiaries per year)
2.0
0.8
2.45
Source: Gornick et al., 1996
-
What are potential sources of disparities in care?Health
systems-level factors financing, structure of care; cultural and
linguistic barriersPatient-level factors including patient
preferences, refusal of treatment, poor adherence, biological
differencesDisparities arising from the clinical encounter
-
Potential Sources of Racial and Ethnic Healthcare Disparities
Healthcare Systems-level Factors
Lack of stable relationships with primary care providers --
minority patients, even when insured at the same level as whites,
are more likely to receive care in emergency rooms and have less
access to private physicians
-
Disparities in the Clinical Encounter: The Core ParadoxHow could
well-meaning and highly educated health professionals, working in
their usual circumstances with diverse populations of patients,
create a pattern of care that appears to be discriminatory?
-
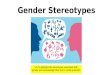
Perceptions of Disparities in Health CareWhat their race or
ethnic background isHow well they speak EnglishWhether they are
male or femaleWhether or not they have
insurance27%15%47%29%58%43%70%72%Generally speaking, how often do
you think our health care system treats people unfairly based
onDoctorsThe PublicPercent Saying Very/Somewhat OftenSource: Kaiser
Family Foundation, National Survey of Physicians, March 2002
(conducted March-October 2001); Survey of Race, Ethnicity and
Medical Care: Public Perceptions and Experiences, October 1999
(Conducted July Sept., 1999)Figure 18
-
Disparities in the Clinical Encounter: The Core Paradox
Uncertainty a plausible hypothesis, particularly when providers
treat patients that are dissimilar in cultural or linguistic
background
-
Disparities in the Clinical Encounter: The Core
ParadoxStereotyping evidence suggests that physicians, like
everyone else, use these cognitive shortcuts
-
Stereotyping: A DefinitionStereotyping can be defined as the
process by which people use social categories (e.g. race, sex) in
acquiring, processing, and recalling information about others.
-
Stereotyping: A Definition
Stereotyping beliefs may serve important functions - organizing
and simplifying complex situations and giving people greater
confidence in their ability to understand, predict, and potentially
control situations and people.
-
Stereotyping: RisksCan exert powerful effects on thinking and
actions at an implicit, unconscious level, even among well-meaning,
well-educated persons who are not overtly biased.Can influence how
information is processed and recalled.
-
Stereotyping: RisksCan exert self-fulfilling effects, as
patients behavior may be affected by providers overt or subtle
attitudes and behaviors.
-
Stereotyping: When Is It in Action?Situations characterized by
time pressure, resource constraints, and high cognitive demand
promote stereotyping due to the need for cognitive shortcuts and
lack of full information.
-
What is the Evidence that Physician Biases and Stereotypes May
Influence the Clinical Encounter? study conducted in actual
clinical settings found that doctors are more likely to ascribe
negative racial stereotypes to their minority patients. These
stereotypes were ascribed to patients even when differences in
minority and non-minority patients education, income, and
personality characteristics were considered.van Ryn and Burke
(2000)
-
What is the Evidence that Physician Biases and Stereotypes may
Influence the Clinical Encounter?medical students were more likely
to evaluate a white male patient with symptoms of cardiac disease
as having definite or probable angina, relative to a black female
patient with objectively similar symptoms. Rathore et al.
(2000)
-
What is the Evidence that Physician Biases and Stereotypes may
Influence the Clinical Encounter?mental health professionals and
trainees were more likely to evaluate a hypothetical patient more
negatively after being primed with words associated with African
American stereotypes. Abreu (1999)
-
The Elimination of Health Care Disparities
In 2002, the Institute of Medicine (IOM) published Unequal
Treatment: Confronting Racial and Ethnic Disparities in Health
Care, it reported that racial and ethnic minorities experience a
lower quality of health care than non-minorities, even when the
patient's insurance status and income are controlled.
-
The Elimination of Health Care DisparitiesThe study committee
also found evidence that stereotyping, biases, and uncertainty on
the part of health care providers contribute to unequal
treatment.
-
The Elimination of Health Care DisparitiesClinicians may order
fewer tests for racial and ethnic minorities if they do not
understand the patient's description of symptoms.
-
The Elimination of Health Care DisparitiesAlternatively,
clinicians may order more diagnostic tests to compensate for not
understanding what their patients are saying.
-
Race was noted in 16 of 18 case presentations by residents, but
only 19 of 36 cases involving white patients. Race was mentioned in
10 of 10 cases when the resident described black patient's
unflattering characteristics, but only four of nine cases where the
resident described unflattering characteristics in white
patients.
-
African American patients were viewed by physicians as less
intelligent, less educated, less likely to comply with their advice
and more likely to have problems with alcohol and drugs. Physicians
also rated African American patients as less likely to be the kind
of person whom the physician could have as a friend.
-
Using pain-management vignettes in patients who differed only in
race, male physicians prescribed higher doses of hydrocodone to
whites than to blacks, while female physicians did the opposite
-
Implicit Bias and Unconscious StereotypingResearch indicates:
Implicit biases are pervasive.People are often unaware of their
implicit biasesOrdinary people harbor negative associations in
relation to various groups
-
Implicit Bias and Unconscious Stereotyping
Implicit biases predict behavior People differ in levels of
implicit bias
-
Implicit Bias and Clinical Outcomes
Physicians reported no explicit preference for white versus
black patients
Implicit Association Test (IAT) revealed implicit preference
favoring white Americans
-
Implicit Bias and Clinical OutcomesIAT revealed implicit
stereotypes of black Americans as less cooperative with medical
procedures and less cooperative generally
As physicians pro-white implicit bias increased, so did their
likelihood of treating white patients and not treating black
patients with thrombolysis
-
Dual Process Stereotyping Two distinct methods of
stereotyping:
Automatic stereotyping
Goal modified stereotypingBurgess and van Ryn: Understanding the
provider contribution to race/ethnicity disparities in pain
treatment; Pain Med. 2006
-
Automatic Stereotypingoccurs when stereotypes are automatically
activated and influence judgments/behaviors outside of
consciousness
Occur regardless of their relevance to the perceivers
goalsBurgess and van Ryn: Understanding the provider contribution
to race/ethnicity disparities in pain treatment; Pain Med. 2006
-
Goal Modified StereotypingMore conscious process, done when
specific needs of clinician arise (time constraints, filling in
gaps in information needed to make complex decisionsBurgess and van
Ryn: Understanding the provider contribution to race/ethnicity
disparities in pain treatment; Pain Med. 2006
-
Function of StereotypingProviders are likely to apply
information contained in racial/ethnic stereotypes to interpret
symptoms and make decisions
Stereotypes likely to be used when stereotypic information is
perceived as clinically relevant, and the decision is complex
Burgess and van Ryn: Understanding the provider contribution to
race/ethnicity disparities in pain treatment; Pain Med. 2006
-
Web and Other ResourcesHeads Up! Website:
http://www.stop-disparities.org/RESOURCES.html
-
Web and Other Resources Implicit Association Test:
https://implicit.harvard.edu/implicit/ Project Implicit Information
Page: http://projectimplicit.net/ (Recommended Tests: Race,
Arab-Muslim, Gender, Sexuality)
"The Police Officer's Dilemma"
http://home.uchicago.edu/~jcorrell/TPOD.html and then click on the
very bottom link
http://backhand.uchicago.edu/Center/ShooterEffect/
Voiceover:
Another reason addressing disparities is challenging is related
to the relatively low level of awareness or acknowledgement of the
problem.When physicians and the public were asked about the
existence of disparities in health care, there was considerable
agreement that the health care system treats people unfairly based
on whether they have insurance coverage.However, despite evidence
of racial/ethnic disparities in care, less than a third (29%) of
physicians and less than half (47%) of the public believe that our
health care system treats people unfairly based on
race/ethnicity.Though compelling evidence of health care
disparities exists, it is not well known. Until there is greater
awareness of health care disparities, it will be difficult to
motivate providers, policymakers or the health care system to seek
out solutions to eliminate them.