Embed Size (px)
Citation preview

HEALTH CARE DELIVERY SCIENCE AND THE FUTURE OF MEDICAL
LEADERSHIP
HONG KONG HOSPITAL AUTHORITY CONVENTION 2013 ALBERT MULLEY, MD, MPP
MEMBER, INSTITUTE OF MEDICINE, NATIONAL ACADEMY OF SCIENCES DIRECTOR, THE DARTMOUTH CENTER FOR HEALTH CARE DELIVERY SCIENCE
HONG KONG MAY 15, 2013
The World’s Most Enduring Institutions • Dartmouth: 1769
• 1 of 8 in the Ivy League • #1 in US for Teaching • Top-10 university in America • Among the highest endowments
• Geisel School of Medicine: 1796 • 4th oldest in US
• Tuck School of Business: 1900 • Oldest in US • #1 in US (Wall Street Journal, 2007)
• #1 in the world (The Economist, 2011)
• Thayer School of Engineering: 1867 • Among the oldest in the US
2
Dartmouth’s Commitment to Serve Health Care Reform
Dartmouth College
Tuck School of Business at Dartmouth
Thayer School of Engineering at Dartmouth
Geisel School of Medicine at Dartmouth
The Dartmouth Institute for Health Policy & Clinical Practice
Dartmouth-Hitchcock Medical Center 3
Jim Yong Kim 12th President of the World Bank, 2012 Nominated by President Obama
4

Dartmouth’s Commitment to Serve Health Care Reform in China
A Five-Year Agreement Between Dartmouth and Ministry of Health Signed in Beijing, October 17, 2011 5
Why Dartmouth?
First-in-the-world Shared Decision Making Center The Dartmouth Atlas
Global Reach and Impact Dartmouth-Hitchcock Medical Center
Health Care Delivery Science e-Learning
Geisel School of Medicine at Dartmouth
6
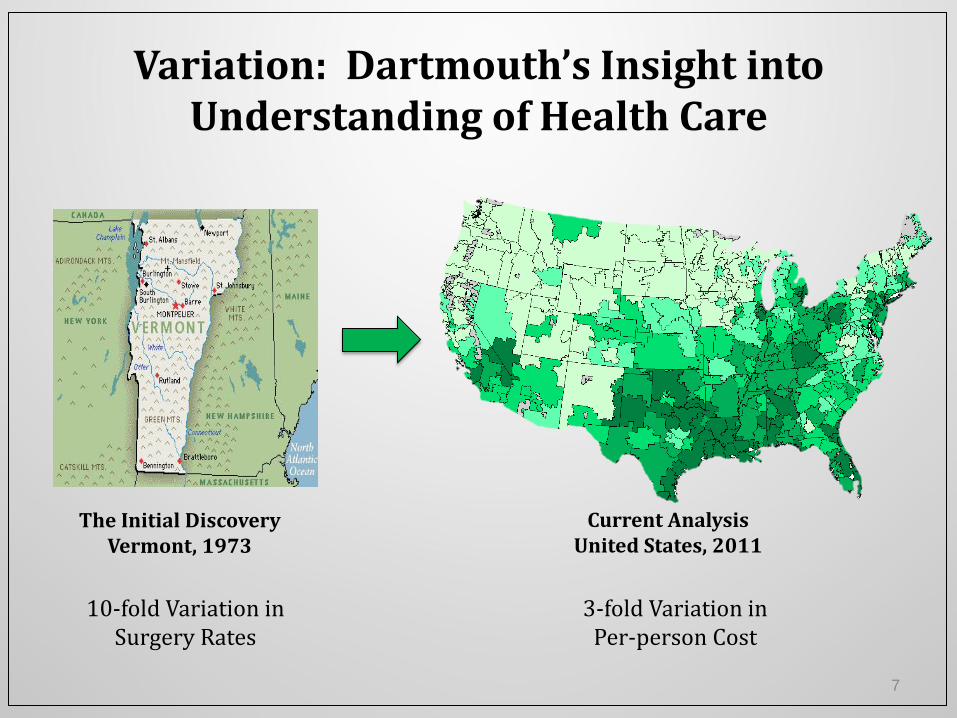
Variation: Dartmouth’s Insight into Understanding of Health Care
The Initial Discovery Vermont, 1973
Current Analysis United States, 2011
10-fold Variation in Surgery Rates
3-fold Variation in Per-person Cost
7
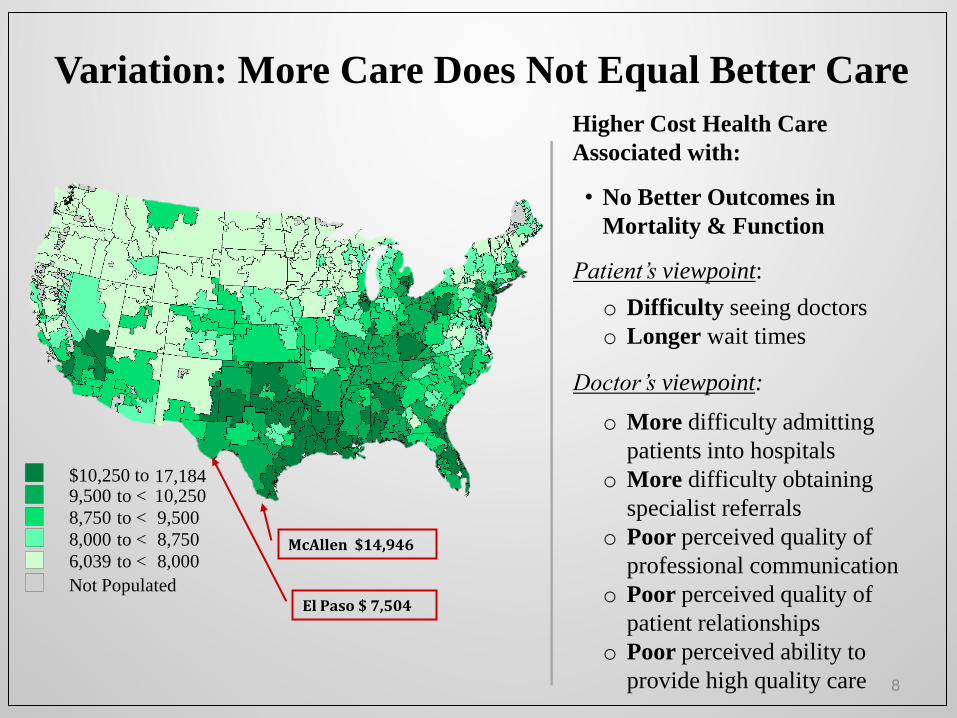
$10,250 to 17,184 9,500 to < 10,250
8,750 to < 9,500
8,000 to < 8,750
6,039 to < 8,000
Not Populated
McAllen $14,946
El Paso $ 7,504
Higher Cost Health Care
Associated with:
• No Better Outcomes in
Mortality & Function
Patient’s viewpoint:
o Difficulty seeing doctors
o Longer wait times
Doctor’s viewpoint:
o More difficulty admitting
patients into hospitals
o More difficulty obtaining
specialist referrals
o Poor perceived quality of
professional communication
o Poor perceived quality of
patient relationships
o Poor perceived ability to
provide high quality care
Variation: More Care Does Not Equal Better Care
8
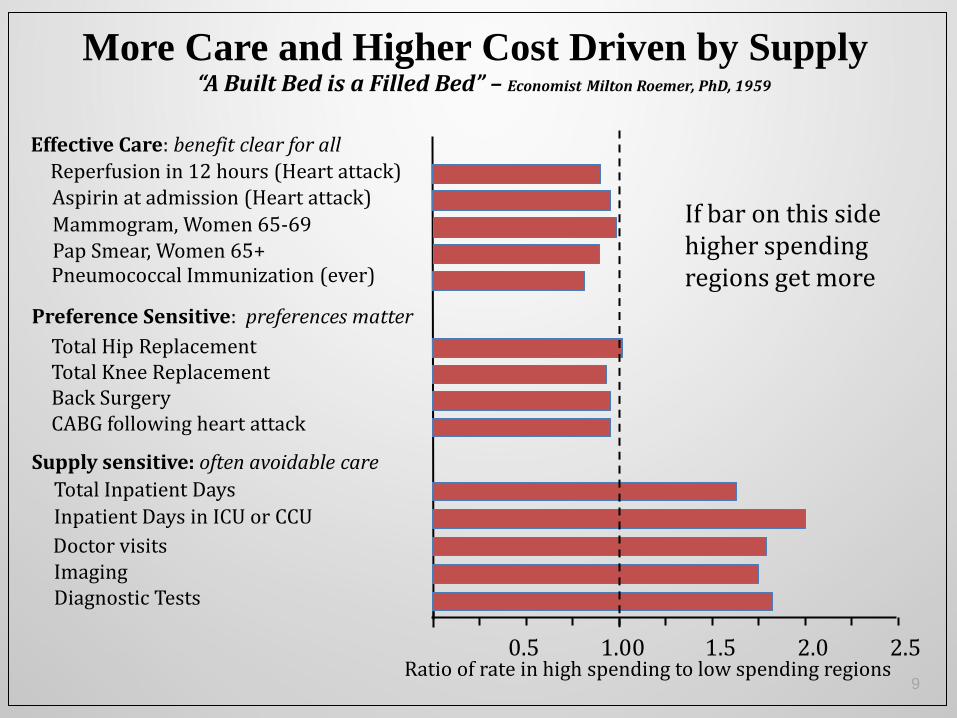
1.00 1.5 2.0 0.5 2.5 Ratio of rate in high spending to low spending regions
Supply sensitive: often avoidable care
Doctor visits Imaging Diagnostic Tests
Inpatient Days in ICU or CCU
Total Inpatient Days
Preference Sensitive: preferences matter
Total Hip Replacement Total Knee Replacement Back Surgery CABG following heart attack
Reperfusion in 12 hours (Heart attack)
Effective Care: benefit clear for all
Aspirin at admission (Heart attack)
Mammogram, Women 65-69 Pap Smear, Women 65+ Pneumococcal Immunization (ever)
If bar on this side higher spending regions get more
More Care and Higher Cost Driven by Supply “A Built Bed is a Filled Bed” – Economist Milton Roemer, PhD, 1959
9

10
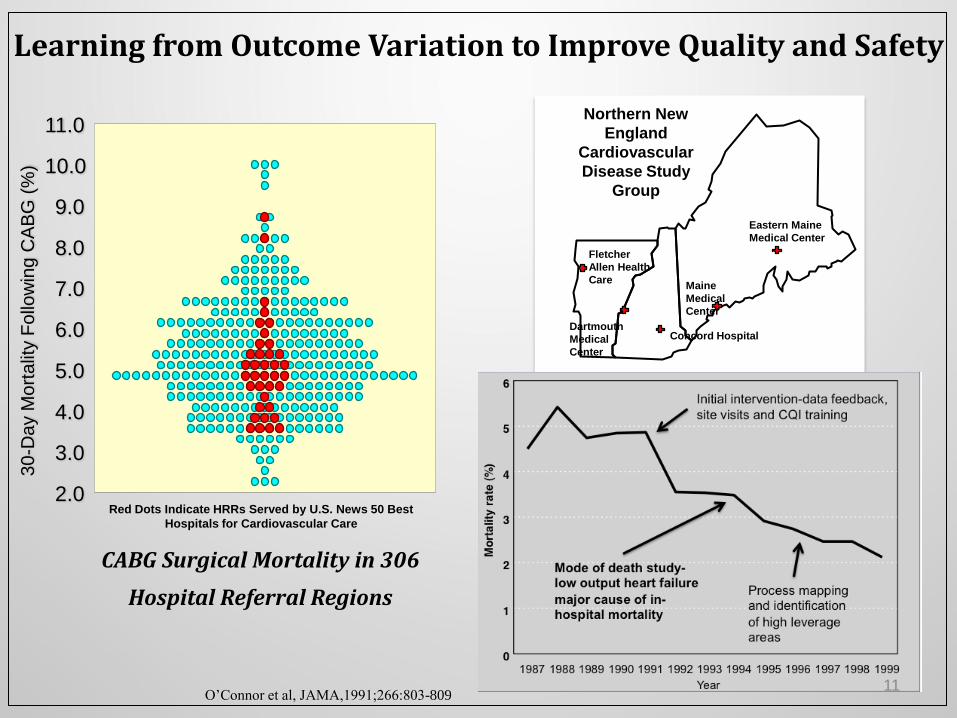
Learning from Outcome Variation to Improve Quality and Safety
CABG Surgical Mortality in 306
Hospital Referral Regions
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
11.0
30
-Da
y M
ort
alit
y F
ollo
win
g C
AB
G (
%)
Red Dots Indicate HRRs Served by U.S. News 50 Best
Hospitals for Cardiovascular Care
Fletcher
Allen Health
Care
Eastern Maine
Medical Center
Maine
Medical
Center
Dartmouth
Medical
Center
Concord Hospital
Northern New
England
Cardiovascular
Disease Study
Group
O’Connor et al, JAMA,1991;266:803-809 11
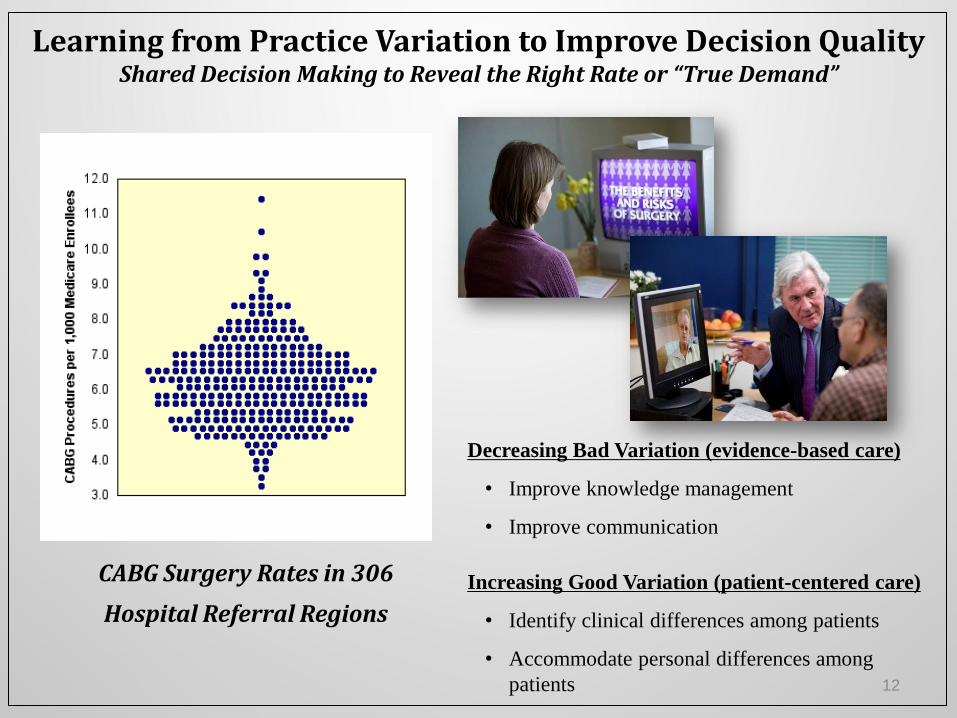
Learning from Practice Variation to Improve Decision Quality Shared Decision Making to Reveal the Right Rate or “True Demand”
CABG Surgery Rates in 306
Hospital Referral Regions
Decreasing Bad Variation (evidence-based care)
• Improve knowledge management
• Improve communication
Increasing Good Variation (patient-centered care)
• Identify clinical differences among patients
• Accommodate personal differences among
patients 12
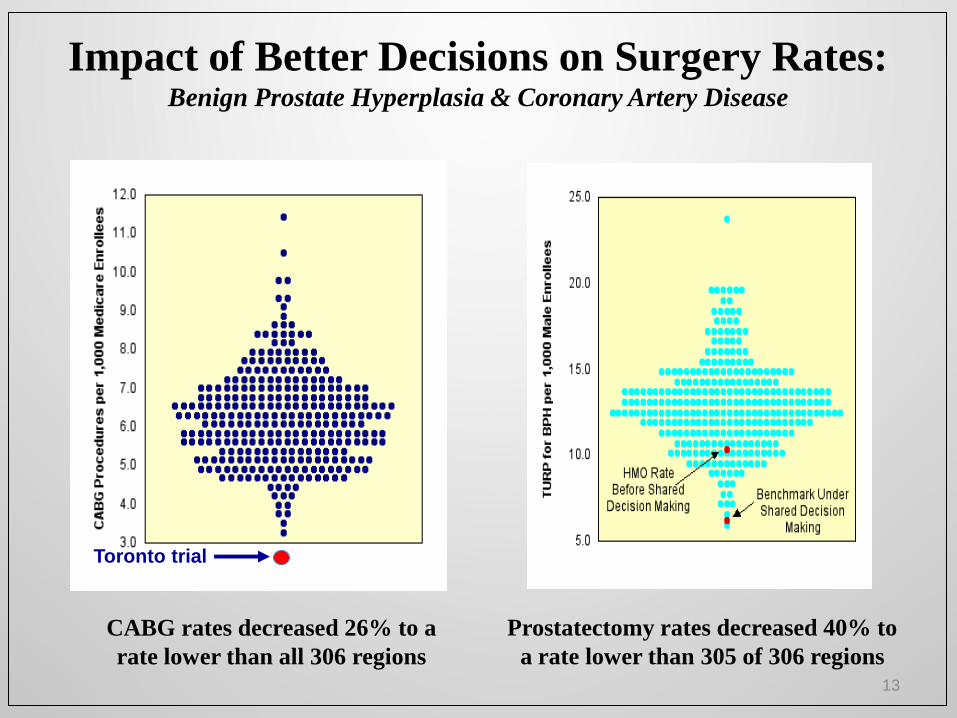
Prostatectomy rates decreased 40% to
a rate lower than 305 of 306 regions
Toronto trial
CABG rates decreased 26% to a
rate lower than all 306 regions
Impact of Better Decisions on Surgery Rates: Benign Prostate Hyperplasia & Coronary Artery Disease
13
High Value Healthcare Collaborative
• Commitment to transparency and knowledge exchange
• Commitment to learn from outcome variation to improve quality and safety
• Commitment to learn from process variation to lower cost
• Commitment to learn from treatment variation to improve decision quality with shared decision making
• First conditions include:
Total Knee Replacement Spine Surgery Diabetes Asthma Heart Failure
• Now includes 18 top hospital systems caring for more than 50 million patients
Founding Members
14
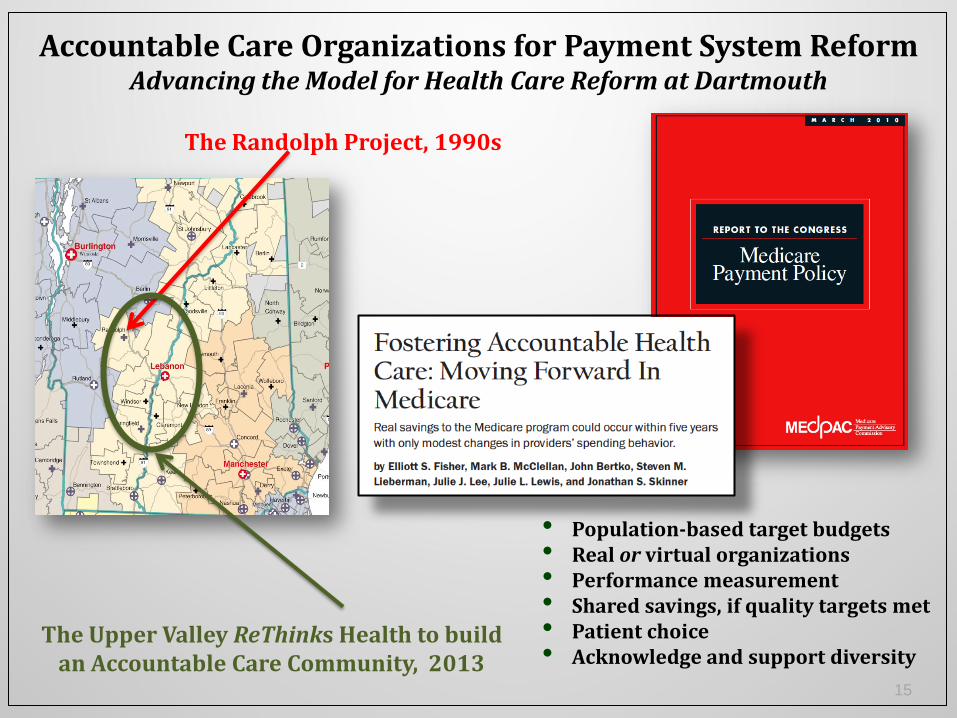
The Randolph Project, 1990s
• Population-based target budgets • Real or virtual organizations • Performance measurement • Shared savings, if quality targets met • Patient choice • Acknowledge and support diversity
Accountable Care Organizations for Payment System Reform Advancing the Model for Health Care Reform at Dartmouth
The Upper Valley ReThinks Health to build an Accountable Care Community, 2013
15
“It’s about the relationship between us and our patients.”
~ Rushika Fernandopulle, MD CEO, Iora Health
Primary Care as the Entry to High Value Health Care Doctors and Patients Co-Creating Value in a Knowledge Intensive Service Industry
16 16
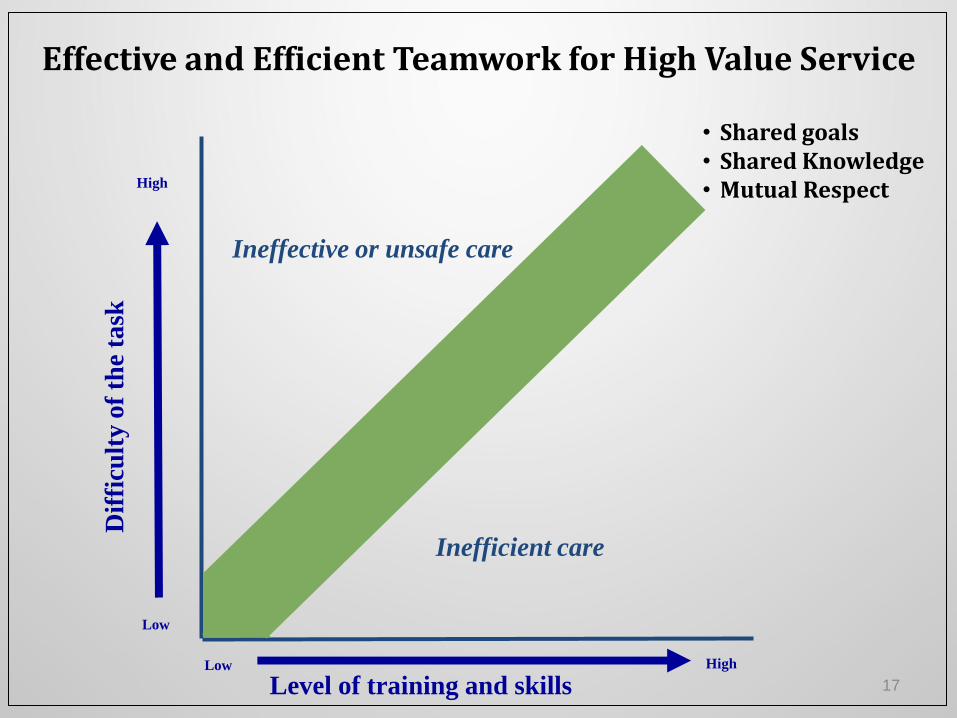
Level of training and skills
Dif
ficu
lty
of
the
task
High
High
Low
Low
Inefficient care
Ineffective or unsafe care
Effective and Efficient Teamwork for High Value Service
• Shared goals • Shared Knowledge • Mutual Respect
17
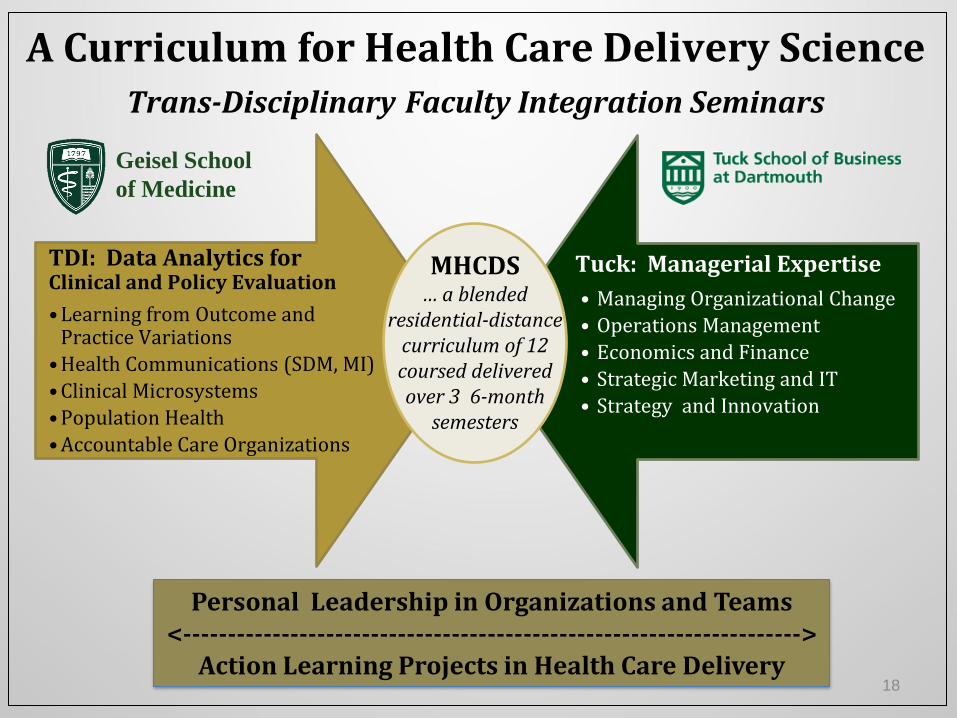
A Curriculum for Health Care Delivery Science Trans-Disciplinary Faculty Integration Seminars
TDI: Data Analytics for Clinical and Policy Evaluation
• Learning from Outcome and Practice Variations
• Health Communications (SDM, MI)
• Clinical Microsystems
• Population Health
• Accountable Care Organizations
Tuck: Managerial Expertise
• Managing Organizational Change
• Operations Management
• Economics and Finance
• Strategic Marketing and IT
• Strategy and Innovation
MHCDS … a blended
residential-distance curriculum of 12 coursed delivered over 3 6-month
semesters
Geisel School
of Medicine
Personal Leadership in Organizations and Teams <--------------------------------------------------------------------->
Action Learning Projects in Health Care Delivery 18
Learning in the Dartmouth Classroom Bringing Leaders and Future Leaders Together from Across Contexts and Nations
19
Learning in the Distance Classroom Bringing Leaders and Future Leaders Together from Across Contexts and Nations
20
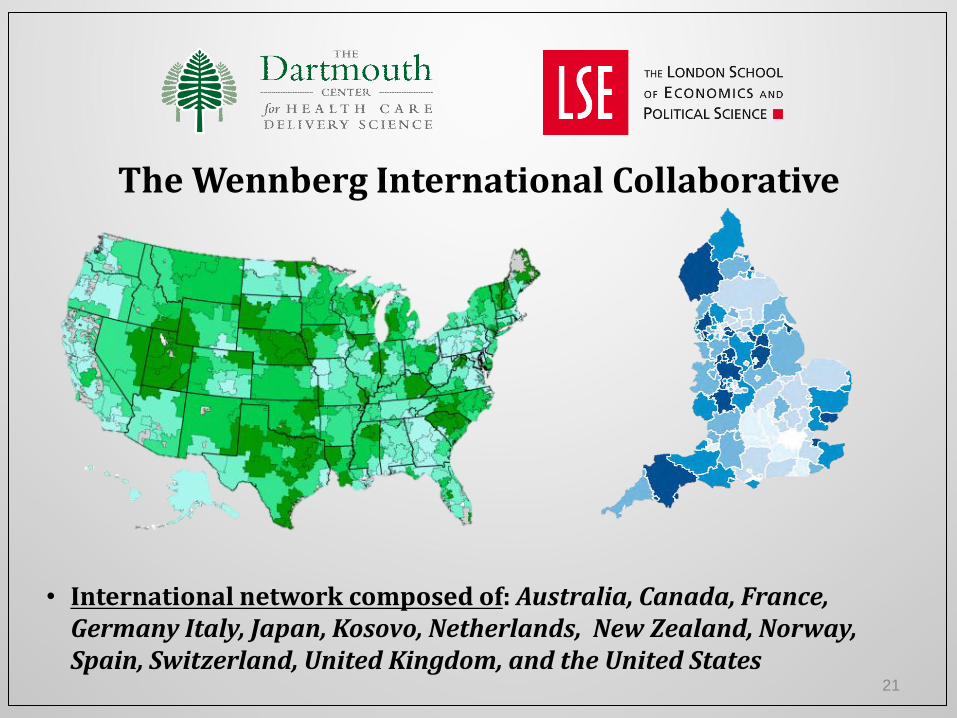
• International network composed of: Australia, Canada, France, Germany Italy, Japan, Kosovo, Netherlands, New Zealand, Norway, Spain, Switzerland, United Kingdom, and the United States
The Wennberg International Collaborative
21
A Journey toward Health Care Reform in China First Steps in Adapting Dartmouth’s Approaches to Serve China
• Regional Dartmouth Atlases of Health Care to Guide Investments in Reform
• A National Dartmouth Atlas of Health Care to Guide Learning from Across China
• A High Value Health Care Collaborative – Learning from Variation to Improve Quality and Decrease Costs of Care
• Integrated Care Networks Built by Leading Hospitals together with Community Health Care Centers in Research and Education as well as Care of both Patients and Populations
• New Models of Primary Care designed for Doctors and Patients Co-Creating Value in a Knowledge-Intensive Service Industry
• Accountable Care Organizations to Align the Incentives of Hospitals, Community Health Centers, and Doctors to Serve the People
• Leadership Training Programs to Align Knowledge and Understanding with the Goals of Health Care Reform
22
23
“This report estimates that from 20% to 40% of all
health spending is currently wasted through inefficiency, and points to 10 specific areas where
better policies and practices could increase the impact of expenditures, sometimes dramatically. Investing these resources more wisely can help
countries move much closer to universal coverage without increasing spending.”
Margaret Chan, WHO
2010
24

Dartmouth-Salzburg Global Health Care Seminars September 2011 + November 2012 with the World Bank + December 2013
September 2011 – Sixty Health Care Leaders from 27 Countries 25
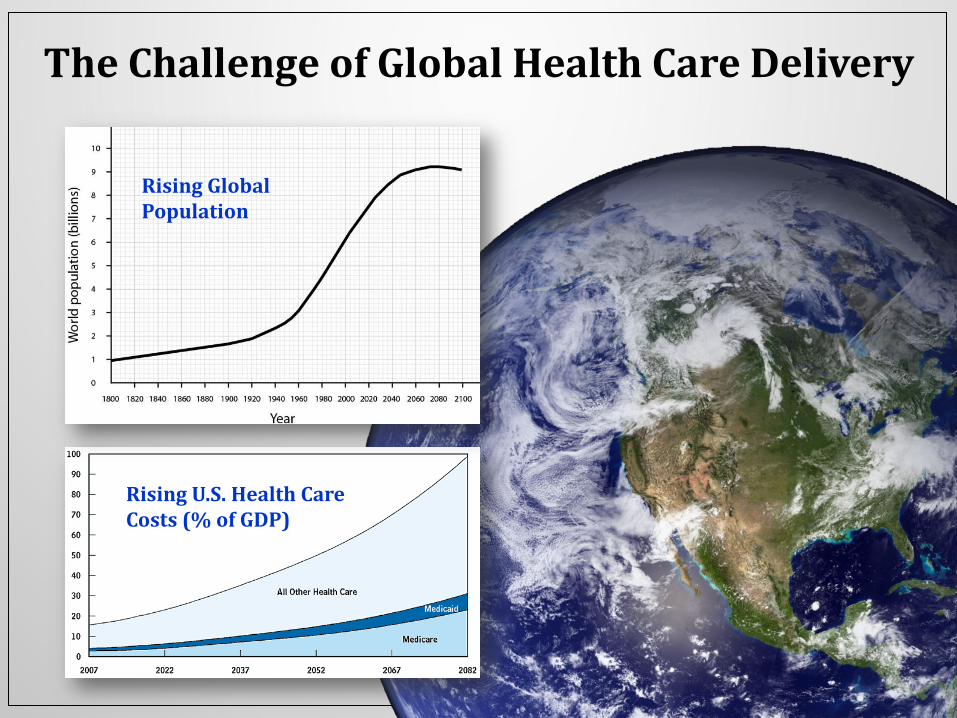
The Challenge of Global Health Care Delivery
26
Rising U.S. Health Care Costs (% of GDP)
Rising Global Population
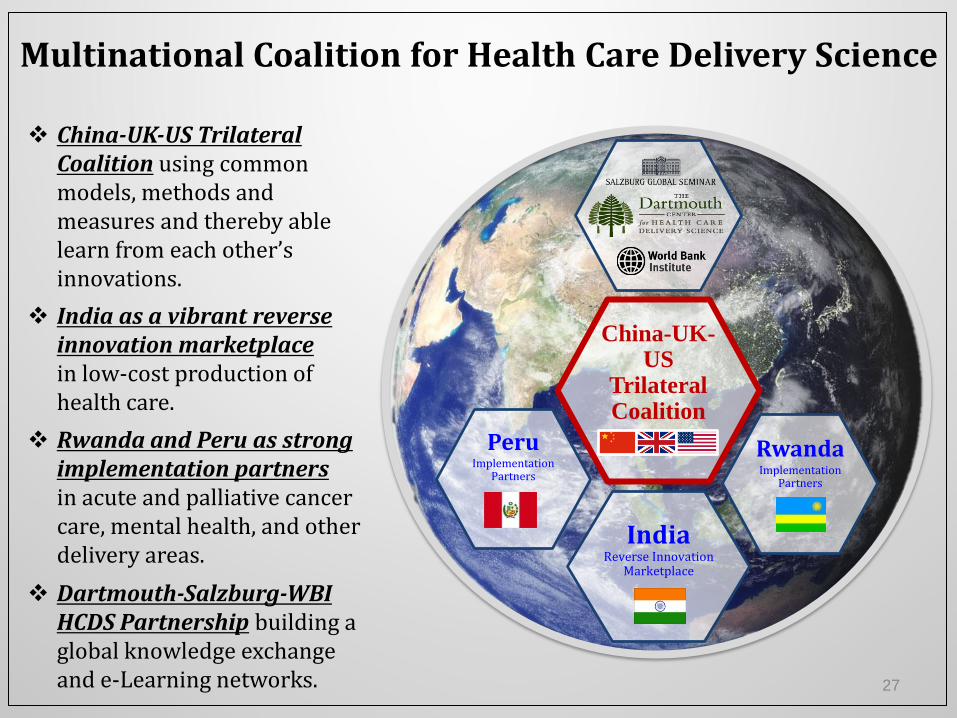
Multinational Coalition for Health Care Delivery Science
China-UK-US
Trilateral Coalition
Rwanda
Implementation Partners
Peru
Implementation Partners
China-UK-US Trilateral Coalition using common models, methods and measures and thereby able learn from each other’s innovations.
Dartmouth-Salzburg-WBI HCDS Partnership building a global knowledge exchange and e-Learning networks.
India as a vibrant reverse innovation marketplace in low-cost production of health care.
Rwanda and Peru as strong implementation partners in acute and palliative cancer care, mental health, and other delivery areas.
India Reverse Innovation
Marketplace
27