Embed Size (px)
Citation preview
HCCA 15th Annual Compliance Institute Conference 1
Health Care Compliance Association
15th Annual Compliance Institute
April 10-13, 2011
Lake Buena Vista, FL
Copyright 2011, Carolyn Zollar, J.D., AMRPA, Washington, DC, Tracey Nixon MS, Reliant, Addison, TX 1
Carolyn C. Zollar J.D. Tracey M. Nixon, MS
Vice President for Government Relations Vice President Gov’t Affairs/
and Policy Development Chief Compliance Officer
American Medical Rehabilitation Providers Assoc. Reliant Hospital Partners
888-346-4624 972-308-8567
[email protected] [email protected]
A Short RAC History
� 2005-2008 RAC Demonstration Program
� IRFs Most Frequent Vulnerability: Denials Due to Failure to Justify Medical Necessity
� Sec. 302 TRHCA 2006: Permanent RAC Program; Reach Back to 10/1/07
� To Date:
− Automatic Reviews in 2010 for IRF Outpatient Services
− Example: Timed and Untimed Codes
− Waiting for the Other Shoe to Drop: Medically Complex Reviews
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC
2
HCCA 15th Annual Compliance Institute Conference 2
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC3
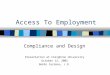
Medicare Compliance
Review Contractors
MIC
CERT MAC ZPIC
RAC
Medically Complex Reviews Will Focus on
IRF Medical Necessity Coverage Criteria
� Rewritten Effective 1/1/10
� Schizophrenia Is Advisable However
� Be Aware of Criteria Pre 1/1/10
� FY 2010 IRF PPS Rule, August 7, 2009 (74 F.R. 39762)
� See Handout for Citation of CMS Issuances
� Why Be Concerned About Old Regulations?
� Contractors Can Still Review Cases Pre 1/1/10 Esp. RACs, Although Unlikely
� LCDs Come Into Play Here Too
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC
4
HCCA 15th Annual Compliance Institute Conference 3
Three Key Criteria In Appeals for
Cases Pre Jan. 1, 2010
� Close medical supervision by qualified physicians
� 24/7 RN availability with specialized training or experience in rehabilitation
� Relatively intense level of rehab
� Focus on HCFA ruling 85-2 for appealing denials
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC5
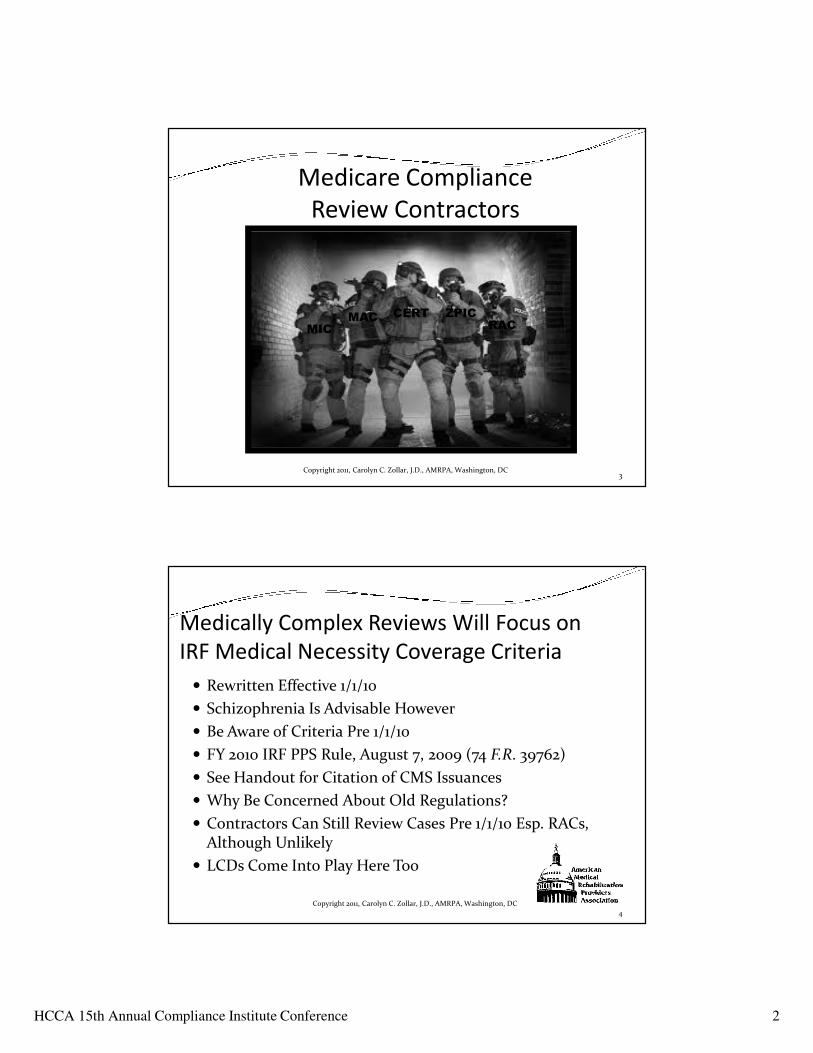
Medicare Medical Rehabilitation
Coverage Criteria Comparison
OLD - HCFAR 85-2 NEW - 42 CFR 412.622(a)(3)-(5)
A. General Deleted
B. Readmission Screening (a)(4)(i) – Rewritten completely and is now mandatory
C. Inpatient Assessment of Potential• 3-10 day evaluation
assessment• Will cover even when
deemed not to be a candidate
(a)(4)(i)(ii) and (iii)Assessment is a new requirement and is a specified part of the preadmission screening, post-admission evaluation and individualized plan of care3-10 day evaluation stay eliminated; admissions found not to be appropriate will be paid the short stay CMG (CMG 5001)
D. Inpatient Rehabilitation Care1. Close medical supervision by
a physician with training and experience in rehabilitation
42 CFR 412.622(a)(3)(iv)Close medical supervisionThis criteria is rewritten with more responsibility going to the rehab physicianMinimum of 3 face to face patient visits per week
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC6
HCCA 15th Annual Compliance Institute Conference 4
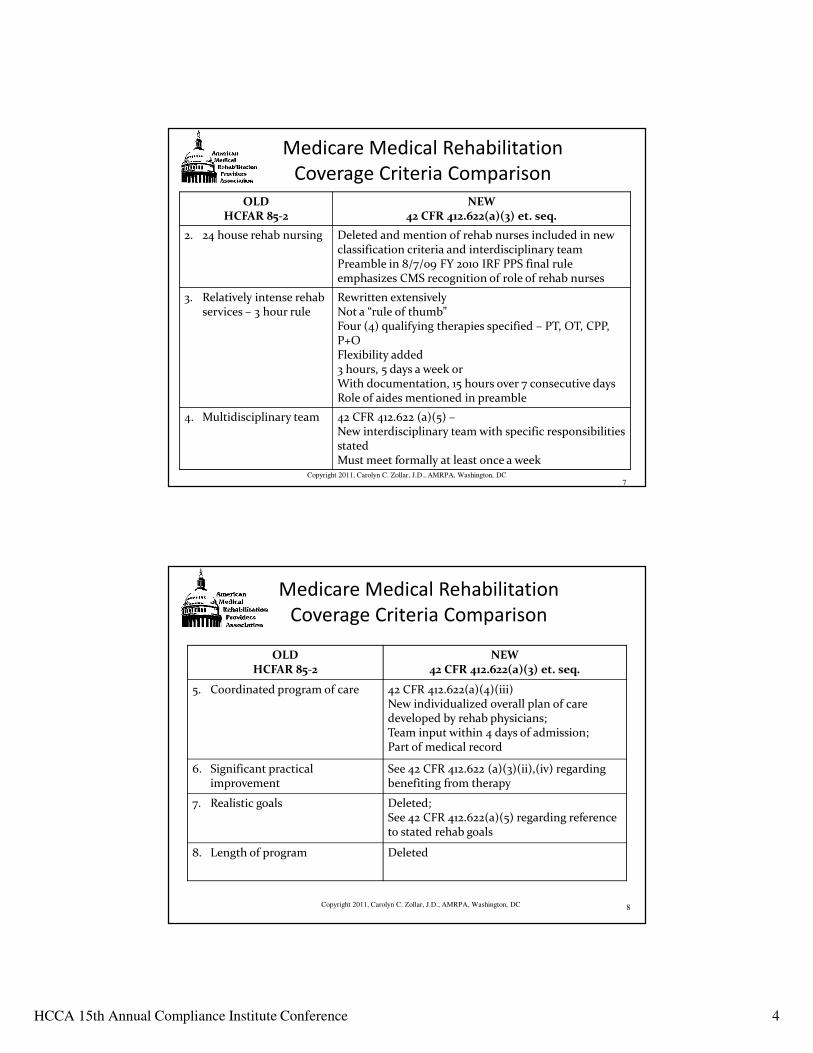
Medicare Medical Rehabilitation
Coverage Criteria Comparison
OLD HCFAR 85-2
NEW 42 CFR 412.622(a)(3) et. seq.
2. 24 house rehab nursing Deleted and mention of rehab nurses included in new classification criteria and interdisciplinary teamPreamble in 8/7/09 FY 2010 IRF PPS final rule emphasizes CMS recognition of role of rehab nurses
3. Relatively intense rehabservices – 3 hour rule
Rewritten extensivelyNot a “rule of thumb”Four (4) qualifying therapies specified – PT, OT, CPP, P+OFlexibility added3 hours, 5 days a week orWith documentation, 15 hours over 7 consecutive daysRole of aides mentioned in preamble
4. Multidisciplinary team 42 CFR 412.622 (a)(5) –New interdisciplinary team with specific responsibilities statedMust meet formally at least once a week
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC7
Medicare Medical Rehabilitation
Coverage Criteria Comparison
OLD HCFAR 85-2
NEW 42 CFR 412.622(a)(3) et. seq.
5. Coordinated program of care 42 CFR 412.622(a)(4)(iii)New individualized overall plan of care developed by rehab physicians;Team input within 4 days of admission;Part of medical record
6. Significant practical improvement
See 42 CFR 412.622 (a)(3)(ii),(iv) regarding benefiting from therapy
7. Realistic goals Deleted;See 42 CFR 412.622(a)(5) regarding reference to stated rehab goals
8. Length of program Deleted
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC 8
HCCA 15th Annual Compliance Institute Conference 5
CMS Focus on Four Criteria, Documentation,
Timing
� Four new criteria
1. Multiple therapeutic intervention
2. Intensity of rehab therapy
3. Sufficiently stable to actively participate
4. Need for physician supervision
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC
9
CMS Focus on Four Criteria, Documentation,
Timing
� Documentation of Specific Actions
− Preadmission Screening
� 48 hours before admission
− Post admission Evaluation
� Within 24 hours of admission
− Interdisciplinary Team Conference
� Within the first week
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC10

HCCA 15th Annual Compliance Institute Conference 6
CMS Focus on Four Criteria, Documentation,
Timing
� Documentation of specific actions
− Plan of Care
� End of 4th day following admission
− Start Therapy
� Within 36 hours from midnight of day of admission
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC11
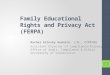
IRF NEW COVERAGE CRITERIA TIME LINE*
EFFECTIVE FOR DISCHARGES ON OR AFTER
JANUARY 1, 2010
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC 12
Time Action• 48 Hours Prior to Admission Preadmission Screening If Done 48 Hours
Before (Allows Flexibility For An Update)
• Within 24 Hours Of Admission Rehabilitation Physician To Conduct Post
Admission Evaluation
• By End Of The 4th Day Following
Admission
Individualized Plan Of Care Must Be
Completed By The End Of The Fourth Day
Following Admission To The IRF
• 1st Meeting Within A Week Of
Admission, Weekly Thereafter
Interdisciplinary Team Meeting
• 3 Times A Week Minimum Rehabilitation Physician To See Patient;
Reason Is To Reassess Patient
• Within 36 Hours From Midnight
Of Day Of Admission
Initial Therapy; Includes Evaluations
*However, read the preamble to the FY 2010 Final Rule for details as published in the Federal Register
dated August 7, 2009.
HCCA 15th Annual Compliance Institute Conference 7
Documentation Improvement
Challenges
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 13
TECHNICAL AND CLINICAL PERTINENCE
1. Incomplete and/or Contradictory Clinical Documentation
2. Incomplete specificity to support medical necessity of treatment rendered
3. Technical requirements not met
4. Inconsistent meeting of regulatory requirements
5. Incomplete documentation for facility reimbursement- severity and complexity of patient- Coding
6. Documentation to support FIM Accuracy
Documentation Improvement
Goals
14
GOALS
1. Secure medical record documentation that supports regulatory compliance requirements and medical necessity.
2. Improve facility reimbursement and case mix
3. Improve the accuracy of severity of illness through more accurate code assignments.
4. Accurately reflect quality outcomes5. Decrease reimbursement denials
6. Improve clinician/physician communication internally and to fiduciary reviewers
Copyright 2011, Tracey Nixon, Reliant, Addison, TX
HCCA 15th Annual Compliance Institute Conference 8
Improvement Plan
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 15
Audits
• Ongoing Concurrent and Closed Record Audits
Analysis of Data
• Determine baseline performance of Compliance % for: Nursing, Therapists, Physicians, Coders, Admission/Registration , CM
Improvement Plan
• Hire additional staff? Regional HIM/Coding Specialist, Auditor
• Improve Documentation: Templates, EMR
• Education /Resources/Tools
Ongoing Tracking
• Weekly /Monthly/Quarterly Reports
• MEC
• Performance Reviews
Audits
� Medical Necessity
� Coding
� IRF PPS Rule
� Discharge Coding
� IRF-PAI
� Billing
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 16
HCCA 15th Annual Compliance Institute Conference 9
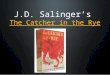
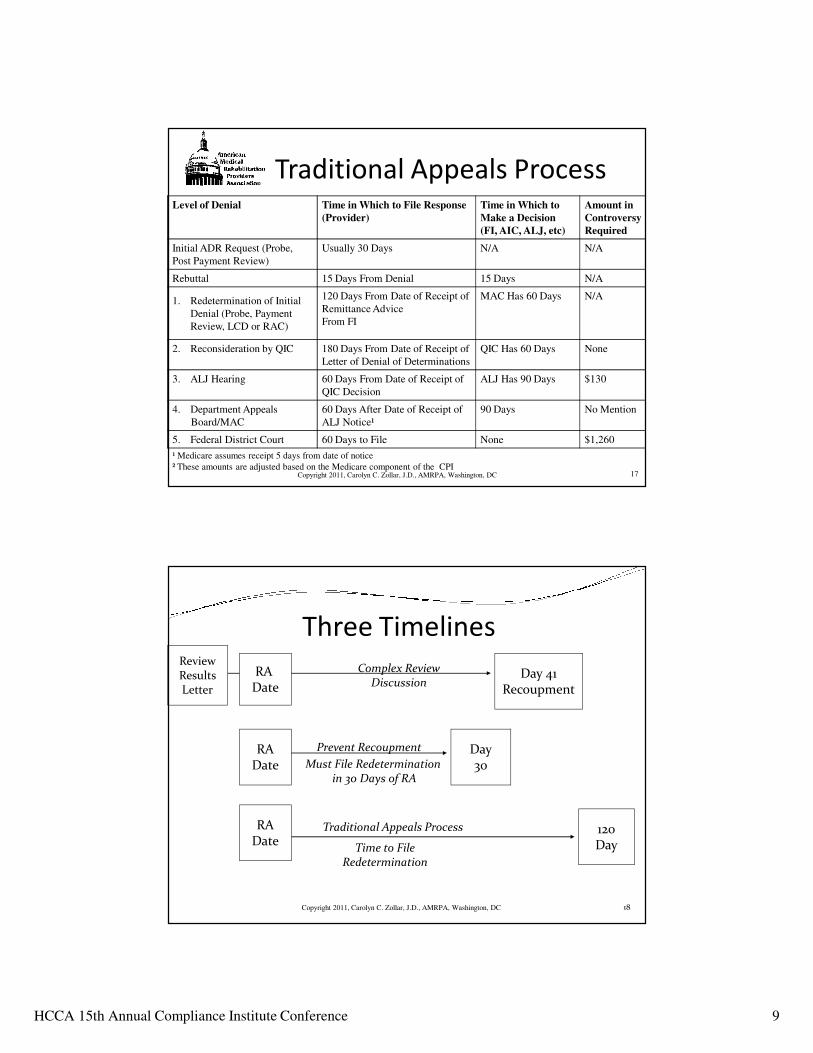
Level of Denial Time in Which to File Response
(Provider)
Time in Which to
Make a Decision
(FI, AIC, ALJ, etc)
Amount in
Controversy
Required
Initial ADR Request (Probe,
Post Payment Review)
Usually 30 Days N/A N/A
Rebuttal 15 Days From Denial 15 Days N/A
1. Redetermination of Initial
Denial (Probe, Payment
Review, LCD or RAC)
120 Days From Date of Receipt of
Remittance Advice
From FI
MAC Has 60 Days N/A
2. Reconsideration by QIC 180 Days From Date of Receipt of
Letter of Denial of Determinations
QIC Has 60 Days None
3. ALJ Hearing 60 Days From Date of Receipt of
QIC Decision
ALJ Has 90 Days $130
4. Department Appeals
Board/MAC
60 Days After Date of Receipt of
ALJ Notice¹
90 Days No Mention
5. Federal District Court 60 Days to File None $1,260
17
Traditional Appeals Process
¹ Medicare assumes receipt 5 days from date of notice
² These amounts are adjusted based on the Medicare component of the CPICopyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC
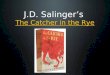
RADate
Traditional Appeals Process
Time to FileRedetermination
Prevent Recoupment
Must File Redeterminationin 30 Days of RA
Three Timelines
RA Date
Review Results Letter
Day 41Recoupment
120Day
Day30
RADate
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC 18
Complex ReviewDiscussion
HCCA 15th Annual Compliance Institute Conference 10
Timelines for RAC Review and Denials and
Traditional Appeals Have To Be Carefully
Managed� Note the Remittance Advice Date
� Note the Demand Letter Date
� Read RAC Demand Letter Carefully
� Note the RAC Discussion Dates
� Preventing Recoupment and Strategy Must Be Considered In Terms of Effect on Timelines, Finances, Quality of Grounds for Appeals
� Initial Determination Triggers Traditional Process for Appeals
� Definition of Initial Determination is Key
Copyright 2011, Carolyn C. Zollar, J.D., AMRPA, Washington, DC19
Best Defense is a Strong Offense
� Policy and Procedure
� Medical Records- Chart Prep
� Roles/Responsibilities
� Workflow/Timelines
� Appeals Team
� Checklist
� Tracking Tool
� Resources/Sample Letters
� Mock RAC Audit/Appeal
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 20
HCCA 15th Annual Compliance Institute Conference 11
Building an Appeal Defense
� Do you know what you would use to build an argument for payment?
� The object of appeal letter is to detail why the patient required rehab and putting the pieces together to form a narrative of patient’s stay.
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 21
Top 6 Hot Areas� Pre Admission Screening
� Physician’s Overall Plan of Care
� Date/Time Discrepancies
� Team Conference
� Post Admission Assessment
� 3 Hour Rule Compliance
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 22
HCCA 15th Annual Compliance Institute Conference 12
Physician Overall Plan of Care� Medical and functional goals, interventions, frequency and
duration and patient’s anticipated functional outcomes.
� Common error- late completion of overall plan of care by day four (4)
� Common error- not clearly identified in the record
� Common error- physician has not documented agreement with team goals, interventions, anticipated outcomes and frequency and duration of care by each discipline
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 23
Date/Time Discrepancies
� Pre-Admission Form
� Post Admission Evaluation
� Initiation of Therapy
� Plan of Care
� Physician Visits
� Team Conference
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 24
HCCA 15th Annual Compliance Institute Conference 13
Team Conference Documentation
� Must document how the treatment team addressed the plan of care and made appropriate adjustments
� Barriers to discharge and team goals
� Signatures from all team members
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 25
Post Admission Evaluation
� A struggle as it is often duplicative of information in H&P
� Includes: medical plan, co-morbidities, risks and potential complications, functional plan, anticipated outcomes, estimated length of stay, and expected discharge destination.
� Addressing risks and potential complications is vital to justifying close medical supervision.
� Can not be written by physician extender
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 26
HCCA 15th Annual Compliance Institute Conference 14
3- Hour Rule Compliance
� Day of admission counts as the first day of both the stay and 7 day period
� Weekend therapy
� Need tracking tool
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 27
Other Considerations
� Focus on Safety - Physical and Cognitive
� Cognition Problems
� Standardized Testing Results
� Patients with CMI < 1.0-
� Patient Discharge Planning Checklist
� Home Evaluation Checklist
Copyright 2011, Tracey Nixon, Reliant, Addison, TX 28