Embed Size (px)
Citation preview

Health Care Capital Expenditures in Minnesota- A Data Short Take -
Health Economics Program
March | 2019

Background on Health Care Capital Expenditures
• Hospitals, clinics, and other health care providers commonlyspend money in the following ways:
• Updating, leasing, or building new facilities• Replacing or adding medical equipment• Installing or modernizing electronic health records systems
• These expenses contribute to what some call a ‘medical armsrace’1 where providers invest in costly technology2 or buildingprojects to attract patients away from competitors.
• Health care capital expenditures have been found to add about 5percent in overall spending3 nationally as providers must pay forthese investments by borrowing, using revenue exceedingexpenses, or other assets such as charitable foundations.
2

Capital Expenditure Monitoring in Minnesota
• Under Minnesota law, all major spending commitments (over$1 million) by health care providers must be reported to MDH4
• MDH started comprehensively collecting these major spending commitments in 2007
• There is likely additional spending on health care projects beyond what is reported, as the following types of projects over $1 million are exempt:
• Medical education or medical research
• Building maintenance or projects not directly related to patient care (e.g., parking lot or elevators)
• Certain changes in ownership or control (e.g., mergers or acquisitions)
3

General Trends in Health Care Capital Expenditures

5
Amount of Health Care Dollars Devoted to Capital Expenditures in Minnesota
In 2016, health care providers committed $645.4 million to major projects
This amounted to $2.12 spent
on major capital projects for every $100
spent health care in 2016
Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section 62J.17 and data collected to estimate health care spending in Minnesota. US10dollorbill-Series 2004A (2018, July 22). Wikimedia Commons, the free media repository. Retrieved, August 30, 2018 from https://commons.wikimedia.org/w/index.php?title=File:US10dollarbill-Series_2004A.jpg&oldid=312119332.

Three-year Rolling Average Total Capital Expenditure Spending with Maximum and Minimum, 2007 to 2016
6Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section. 62J.17. The year shown is the midpoint of the three-year average and the upper and lower bound are the maximum and minimum for each three year period.
$0
$200
$400
$600
$800
$1,000
$1,200
$1,400
$1,600
$1,800
2008 2010 2012 2014 2016
Mill
ions
of D
olla
rs
Maximum of Three-Years
Average of Three-Years
Minimum of Three-Years
Total capital expenditure spending varied substantially by year, but there was a reduction in spending following the
recession of 2008

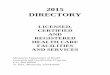
Minnesota Health Care Capital Expenditures by Size of Major Spending Commitment
7Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section 62J.17.
While most commitments
were less than $5 million, half of all
spending was over $20 million and nearly one
quarter was devoted to just 12 projects over
$100 million from 2007 to 2016
10.2%
17.4%
11.6% 10.8%
26.4%
23.6%614
482
141
66 68
120
100
200
300
400
500
600
700
Less than$2 million
$2 to $5Million
$5 to $10Million
$10 to $20Million
$20 to $100Million
Over $100million
0%
5%
10%
15%
20%
25%
30%
Num
ber o
f Maj
or C
omm
itmen
ts
Percent of Spending by Project Size
Percent of Spending Number of Major Commitments

Percent of Capital Expenditures by Health Care System, 2007 to 2016
8Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section 62J.17 for 2007 to 2016.
More than half of spending is invested by large health care systems
Mayo Clinic, 18%
Fairview Health Services, 17%
Allina Health System, 11%
Park Nicollet Health Services, 8%
CentraCare Health System, 5%
Children's Hospitals and
Clinics, 5%
HealthPartners, Inc., 4%
HealthEast Care System, 3%
Essentia Health, 2%
North Memorial Health Care, 2%
Sanford Health, 2%Lakeview Health
System, 1%
University of Minnesota Physicians,
1%
No Affiliation, 16%
Other Affiliated Providers, 6%
Other, 30%

Types of Capital Expenditure Projects

Capital Expenditures by Type of Provider
Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section 62J.17 for 2007 to 2016.
$125.7
$236.4
$1,974.8
$5,956.8
$0.0 $1,000.0 $2,000.0 $3,000.0 $4,000.0 $5,000.0 $6,000.0 $7,000.0
Surgery Centers
Diagnostic Imaging Centers
Health Care Systems or Clinics
Hospitals
Millions of Dollars
Hospitals are the leading source of health care capital expenditures in
Minnesota comprising 72% of all spending between 2007 and 2016
10

Capital Expenditures by Type of Provider and Project Type, 2007 to 2016
Building andSpace
MedicalEquipment
HealthInformationTechnology
OtherExpense
Hospitals $4,301 $1,026 $369 $260Health Care Systems and Clinics $512 $200 $609 $147Diagnostic Imaging Centers $108 $119 $4 $5Surgery Centers $65 $55 $0 $6
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
Nearly two-thirds of health care capital
spending are devoted to building and space
64% of all projects
18% of all projects13% of all projects
5% of all projects
11Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section 62J.17 for 2007 to 2016.

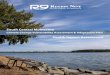
Capital Expenditures, by Type of Project and Year, 2007 to 2016
12Note: Major spending commitments can span several years and are monitored by commitment date such as board authorization.Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section 62J.17.
$0
$200
$400
$600
$800
$1,000
$1,200
$1,400
$1,600
$1,800
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Mill
ions
of D
olla
rs
Building and Space Medical Equipment Health Information Technology Other Expense
In 2007, several hospitals had major building and space projects including one of the largest from 2007-2015
In 2010, the Mayo Clinic boosted medical equipment spending with its $200 million proton beam radiation oncology project
In 2009, the US Congress enacted the Health Information Technology for Economic and Clinical Health Act
In 2015, the Mayo Clinic began a $237 million health information technology investment that totaled $1.5 billion in subsequent years
While large projects can span multiple years, certain projects explain variation across years

Single Capital Expenditure Projects Over $100 Million, 2007 to 2016
13Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section 62J.17 from 2007 to 2016.
$201.2 million
$102 million
$126.4 million
$127 million
$170 million
$175 million
$215 million
$281.8 million
$103.8 million
$134 million
$172 million
$175.5 million
$0 $50 $100 $150 $200 $250 $300
Mayo Clinic Hospital - Rochester, 2010
Mercy Hospital, 2015
Maple Grove Hospital, 2010
U of M Medical Center - Fairview, 2012
Park Nicollet Methodist Hospital, 2014
U of M Medical Center - Fairview, 2007
St. Cloud Hospital, 2007
Children's Hospital, Minneapolis, 2007
HealthEast Care System, 2013
Mayo Clinic Hospital - Rochester, 2015
Mayo Clinic, 2015
Fairview Health Services, 2009
Hosp
ital
HIT
Millions of Dollars
Hospital Construction
or Renovation
Health Information Technology
Proton Beam Facility

Proportion of Hospital Construction Expenditures by Setting Type, 2014 to 2016
Inpatient Only30.0%
Both Inpatient and Outpatient
49.1%
Outpatient Only20.9%
Less than one-third of hospital capital expenditures are devoted to inpatient services alone
Examples of combined inpatient and outpatient hospital capital expenditures include facility renovation or replacement of existing facility housing inpatient and outpatient services
14Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section 62J.17 from 2014 to 2016.

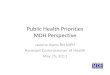
Proportion of Capital Expenditures on Medical Equipment
15‘Other Imaging’ includes a variety of equipment types such as angiography, single photon emission computed tomography, x-ray, and other modalities.Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section. 62J.17 for 2007 to 2016
MRI Equipment16.8%
CT or PET Equipment9.7%
Other Imaging Equipment
11.2%
Surgical Equipment14.6%
Radiation Oncology Equipment
13.2%
Other Medical Equipment
34.5%
More than one third of major spending commitments was devoted to diagnostic imaging equipment including magnetic resonance imaging (MRI), computed tomography (CT), and other imaging modalities from 2007 to 2016

Geographic Location of Capital Expenditure Projects

Location of Minnesota Health Care Capital Expenditures by Project Size, 2007 to 2016
17
The volume of spending isdependent on the location of major health careproviders

Distribution of Minnesota Health Care Capital Expenditures in Urban and Rural Areas, 2007 to 2016
18
82.3%
6.7%
7.1%3.9%
Percent of Health Care Capital Expenditures
Urban Areas had 82% of
state health care capital
expenditures and 74% of
the state population
Urban Areas also had 79%
of available hospital
beds

Minnesota Hospital Capital Expenditures by Type of Service, 2014 to 2016 by Urban or Rural Status
19
Buidling and Space Only, 25.1%
Buidling and Space Only, 52.0%
Building and Space & Medical Equipment,
46.5%
Building and Space & Medical Equipment,
44.2%
Medical Equipment Only, 9.3%
Medical Equipment Only, 1.2%
Health Information Technology, 16.3%
Health Information Technology, 2.3%
Non patient care, 2.7% Non patient care, 0.4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Urban Rural
Source: MDH, Health Economics Program analysis of major spending commitments submitted under Minnesota Statutes, Section 62J.17.

References
1 Devers, K. J., Brewster, L. R., & Casalino, L. P. (2003). Changes in Hospital Competitive Strategy: A New Medical Arms Race?. Health Services Research, 38(1p2), 447-469.
2 Smith S. et al., “Income, Insurance, and Technology: Why Does Health Spending Outpace Economic Growth?” Health Affairs, 28, no. 5 (September/October 2009): 1276-1284. A prior analysis estimated technology was responsible for 38-65 percent of spending growth: Robert Wood Johnson Foundation. “High and Rising Health Care Costs: Demystifying U.S. Health Care Spending.” Research Synthesis Report, No. 16. October 2008.
3 Glied, S., Ma, S., & Solis-Roman, C. (2016). Where The Money Goes: The Evolving Expenses Of The US Health Care System. Health Affairs, 35(7), 1197-1203.
4 Minnesota Statues, Section 62J.17 requires all providers of health care services (with the exception of nursing homes) to report major commitments to the Minnesota Department of Health (MDH). The threshold was $500,000 from 1992 through 2002 and is currently $1 million. The information in this presentation only includes spending officially reported to MDH; however, we routinely track health care capital expenditure information reported elsewhere.
3/8/2019 20

Contact and Other Information
Health Economics [email protected]
651-201-3550
___________________
HEP Home Page: www.health.state.mn.us/healtheconomics
Health Care Market Statistics: http://www.health.state.mn.us/data/economics/chartbook