Embed Size (px)
Citation preview

Health and the Spiritual Dimension: Relationships and Implications for Professional
Preparation Programs Rebecca Banks
INTRODUCTION The concept of the spiritual dimension is not new to
health education or humankind. When attempting to answer questions dealing with meaning of life, the central core of an individual is often directed toward an infinite and all-powerful force which may be referred to as the “Ultimate Meaning,”1(p277) or “Ultimate Concern,”6(~~66-6~) or “Cosmic Force,” or “God.” According to many,*J the spiritual dimension is an integral part of one’s well-being. Yet, glaring deficiencies in the research and philosophical writing in health education have been reported by Hoyman (personal interview March 21 , 1978), Oberteuffer (personal interview May 23, 1978) and Vaux.’ Thus, the focus of the study was to investigate perceptions of select groups of health educators regarding the spiritual dimension of health and the extent to which the spiritual dimension ought to be incorporated in health education professional preparation programs. Data generated by this study will identify the perceptions of health educators about the spiritual dimension and serve as an indicator of the impact which this dimension may have in future professional preparation programs for health educators.
METHODS The study surveyed health educators using an
adaptation of the Delphi Technique. Using this technique, three rounds of data collection were employed. They consisted of three questionnaires: one as a brainstorming device, another as a rating instrument, and a third as a device to identify consensus.
The target population for this study was present and future experts in the field of health education. Two groups of health educators made up the sample.
The first sample consisted of six experts in the field of health education who represented divergent views on the spiritual dimension. All were located in the Midwest region of the United States and were accessible to the
researcher for personal interviews. There were two retired experts and four active experts in the group, and the same ratio existed between females and males. These individuals were selected on the basis of leadership in professional associations, publications and academic positions as chairpersons of health education departments at the college level.
The second sample, participating in the second and third rounds of the study, consisted of three subgroups: retired experts in health education, present experts in health education and doctoral candidates who were graduate teaching associates in health education during the 1977-78 school year. Twenty-five active experts, 25 graduate teaching associates and 20 retired experts were included in this second sample.
Doctoral candidates were selected because they will theoretically be leaders in the field in the next 25 years. Members of this subgroup were randomly selected irom a list of doctoral candidates who were graduate teaching associates in health education during the 1977-1978 school year at the 23 universities in the United States which offer a doctoral program in health education. Schools of public health were not included.
With advice from the expert panel, the following criteria was used in selecting the sample for active and retired experts: (1) retired experts were selected on the basis of their past leadership role in professional associations and upon their publications; (2) present experts were selected from prominent authors in the field, college department chairpersons in health education and officers in the two professional associations considered to be applicable to the study, ie, the Association for the Advancement of Health Education and the American School Health Associa- tion.
The rate of return for the first round of the study was 100%. In the second and third rounds, 88% of the graduate teaching associates and 80% of the active health education experts completed both question- naires; 50% of the retired health education experts
APRIL 1980 THE JOURNAL OF SCHOOL HEALTH 195

completed both. Round I: Identifying Components and Possible Future Efforts
The first phase of the study consisted of interviewing the six health education experts. The following questions were asked of the experts:
1. Is there a spiritual dimension of health? 2. What are the underlying characteristics or
components of the spiritual dimension? 3. What ramifications need to be considered if the
spiritual dimension is to be included in the professional preparation program for health educators?
4. To what extent and how should the spiritual dimension be incorporated into the health education professional preparation program?
5 . What will be the role of the spiritual dimension of health in the next 25 years?
6. What will be the role of the spiritual dimension in health education professional preparation programs in the next 25 years?
Analysis of the data for questions 2 , 3 and 4 consisted of three processes: (1) collation of similar responses, (2) synthesis of similar responses into an inclusive, representative statement and (3) reducing the number of synthesized statements to a number manageable in round two of the study. Presented below are statements from the expert panel in random order:
Question 2: Components of the Spiritual Dimension a. perceptions of what it is that causes the universe to work the way it does; b. something that is perceived as being unknown or hazily known; something for which there isn’t any easy answer and so it becomes a matter of faith; c. something for which there is no rational explanation; recognition of powers beyond the natural and rational; d. a set of principles or ethics to live by; e. something which gives meaning or purpose to life; f. the sense of selflessness and a feeling for others; a willingness to do for others more than for yourself; g. commitment to God/an Ultimate Concern/Cosmic Force; h. involves a survival issue i. the most pleasure-producing quality of humans.
Question 3: Things to be Considered in Order to Teach the Spiritual Dimension of Health Effectively a. recognize the diversity of student backgrounds and recognize that the spiritual dimension may mean different things for different people; b. recognize the diversity of spiritual belief structures; c. recognize the separation of Church and State; d. recognize that the inclusion should initiate respect for others and their views; e. recognize respect for the individual’s present convictions; f. recognize that the spiritual dimension may be a greater or lesser part of any person’s perceptions of health.
Question 4: Methodologies to be Used in Teaching About the Spiritual Dimension a. comparative approach which simply lays out different kinds of belief structures and different patterns of explanation of health and illness; b. holistic approach;
196 THE JOURNAL OF SCHOOL HEALTH
c. international or cross-cultural health course; d. use of problem-solving/valuing/judgement situations; e. study of group dynamics and interpersonal relationships; f. use of a comparative religion course as part of the general studies component; g. use of a philosophy course as part of the general studies component; h. a seminar experience which investigates the influence of various religions on health behaviors.
Round 11: Rating the Importance of Components and Future Efforts
Round two consisted of 70 health educators rating 27 items produced from the data from round one. These items were accompanied by a ten-position rating scale on which the respondents were asked to rate the relative importance of each item. A reminder letter, a second questionnaire and a telephone contact were used to maximize the response rate.
The analysis of the data from the second round of the study included calculating mean scores for each of the 27 items included on the questionnaire. These mean scores were then used to rank-order the components of the spiritual dimension and the ways to effectively teach about the spiritual dimension. In addition, item mean scores and, where appropriate, rank-ordered lists were computed for each of the subgroups (graduate teaching associates, active health education experts and retired health education experts). General priority categories were developed to aid in the interpretation of the mean scores; the following show these major groups: 1 .OO - 2.49 not important 2.50 - 4.49 relatively unimportant 4.50 - 6.49 important 6.50 - 8.49 very important 8.50 - 10.00 of critical importance
Sixty-three, or 90% of the people contacted, returned the questionnaire. However only 56, or 80070, were suitable for data analysis. Table 1 presents the rates of response of the questionnaire.
TABLE 1 Questionnaire Returns
Responses Usable Mailed Received Responses
t Retired: 20 18 12
Active: 25 21 20
T.A.: 25 24 24
Total: 70 63 (90’70) 56 (80%)
Rank-ordered lists dealing with the three major questions follows:
Ranking of the Components of the Spiritual Dimension Very Important:
1. Something which gives meaning or purpose to life 2. Set of principles or ethics to live by 3. The sense of selflessness and a feeling for others, a
APRIL 1980

willingness to do more for others than for yourself Important:
4. Commitment to God; an Ultimate Concern 5 . Perception of what it is that causes the universe to
work the way it does 6. Something for which there is no rational
explanation; recognition of powers beyond the natural and rational
7. Something that is perceived as being unknown or hazily known; something for which there isn’t any easy explanation and so it becomes a matter of faith
because it’s so hard to grasp Ranking of the Ways to Effectively Teach About the
Spiritual Dimension Very Important:
1. Recognize the diversity of student backgrounds and recognize that the spiritual dimension may mean different things for different people
2. Recognize that the inclusion should initiate respect
8. Involves a survival issue 9. The most pleasure-producing quality of humans
for others and their opinions 3. Recognize the diversity of spiritual belief
structures 4. Recognize respect for the individual’s present
views 5 . Recognize that the spiritual dimension may be a
greater or lesser part of any person’s perceptions of health Important:
6. Recognize the separation of Church and State Ranking of Methodologies and Approaches
Very Important:
tions 1. Use of problem-solving/valuing/judgement situa-
2. Holistic approach 3. Study of group dynamics and interpersonal
relationships Important:
influence of various religions on health behaviors 4. A seminar experience which investigates the
TABLE 2 Rating of the Components of the Spiritual Dimension by Subgroups
Not Relatively Very Of Critical Important Unimportant Important Important Importance
Perception of what it is that causes the universe to work the way it does;
Something that is perceived as being unknown or hazily known; something for which there isn’t any explanation and so it becomes a matter of faith;
Something for which there is no rational explana- tion; recognition of powers beyond the natural and rational;
A set of principles or ethics to live by;
Something which gives meaning or purpose to life;
The sense of selflessness and a feeling for others; a willingness to do for others more than for yourself;
Commitment to God; an ultimate concern;
Involves a survival issue:
The most pleasure-producing quality of humans because it is so hard to grasp.
TA A R
TA A R
TA A R
A
A
TA A R
A TA R
TA A R
A TA R
TA R
TA R
TA =graduate teaching associate; A =active health education experts; R =retired health education experts
APRIL 1980 THE JOURNAL OF SCHOOL HEALTH 197

5 . International or cross-cultural health course 6. Comparative approach which simply lays out
different kinds of belief structures and different patterns of explanation of health and illness
7. Use of a philosophy course as part of the general studies component Relatively Unimportant:
8. Use of a comparative religion course as part of the general studies component
Tables 2, 3, and 4 show the rating of the same three questions, (two, four and five) shown above for the three subgroups: graduate teaching associates, active health education experts and retired health education experts.
Responses on the last questionnaire indicated that a consensus was reached on each item. For the majority of the items, the degree of consensus ranged from 64% to 78%. Only five items did not fall within this range of consensus; two items had an extremely high degree of consensus (92% and 82%), and the remaining three had relatively low rates of consensus (6lV0, 59% and 53%).
On the item concerning the components of the spiritual dimension, the least amount of consensus was reached on the component having to do with a commit- ment to God/Ultimate Concern; 59% agreed with the mean score of 6.47 with the remaining 41% being almost equally divided between those wishing to raise
the rating and those believing the rating should be lowered. The highest degree of consensus on the components of the spiritual dimension was on the item ranked last, the most pleasure-producing quality of humans; 82% of the respondents agreed that this was the least important of the identified components. The degree of consensus on the three major components of the spiritual dimension (meaning in life, a set of principles to live by and a sense of selflessness) ranged from 72% to 76%.
Question four dealing with “ways to effectively teach about the spiritual dimension” contained the items with the greatest and the least amount of consensus. Approximately 92% of the respondents indicated that they agreed it is very important to recognize the diversity of student backgrounds and recognize that the spiritual dimension may mean different things for different people. This item was ranked number one on the first questionnaire. The least amount of consensus was reached on the issue of separation of Church and State; 53% of the respondents agreed that this is an important consideration. Approximately 27% of the respondents indicated that the rating position for this item should be “relatively unimportant.” This item was ranked last on the first questionnaire.
Question five involving the appropriate methodolo- gies and approaches to use when teaching about the spiritual dimension had moderate degrees of consensus
TABLE 3 Rating of Ways to Effectively Teach About
the Spiritual Dimension by Subgroups
Not Relatively Very Of Critical Important Unimportant Important Important Importance
By recognizing the diversity of student back- grounds and recognizing that the spiritual dimension may mean different things for different people;
By recognizing the diversity of spiritual belief structures;
By recognizing the separation of church and state;
By recognizing that the inclusion should initiate respect for others and their views;
By recognizing respect for each individual’s present convictions and not become an attempt to change them;
By recognizing that the spiritual dimension might be a greater or lesser part of any person’s perceptions of health.
TA A R
TA A R
TA A R
TA A R
TA A R
T A A R
TA = graduate teaching associate; A = active health education experts; R =retired health education experts
198 THE JOURNAL OF SCHOOL HEALTH APRIL 1980

TABLE 4 Rating of Methodologies and Approaches By Subgroups
Not Relatively Very Of Critical Important Unimportant Important Important Importance
1 Holistic approach;
Comparative approach which simply lays out different kinds of belief structures and different patterns of explanation of health and illness;
1 International or cross-cultural health course;
C I Responses Usable
Mailed Received Responses
Retired: 12 10 10
Active: 20 20 20
T.A.: 24 22 22
Total: 56 52 (93%) 52
Use of problem-solving/valuing/judgment situa- tions;
Study of group dynamics and interpersonal relationships;
Have a comparative religion course as part of the general studies component;
Have a philosophy course as part of the general studies component;
Develop a seminar to look into the influence of various religions on health behaviors.
TA A R
A
TA A R
TA A R
TA A R
R
R
TA R
TA A
TA A
A TA R
on all items; the range was from 61% to 73%. This question showed the most differences among the various generations of health educators on the first questionnaire.
The Delphi Technique utilizes a futuristic approach, and questions six and seven on the questionnaire were of this nature. These futuristic questions dealt with what the health educators perceived would be the significance of the spiritual dimension in regard to health in the next 25 years and what would be the significance of the spiritual dimension in health education professional preparation programs in the next 25 years. On the first questionnaire, 61% of the respondents agreed with the mean score of 6.56 concerning the significance of the spiritual dimension of individuals; 21 070 indicated the item should be rated “of critical importance”; and 67% agreed that the spiritual dimension should be an important factor in the professional preparation program in the next 25 years.
Round 111: Identifying the Degree of Consensus The third round of the study asked the respondents to
reconsider their rating in relation to the overall mean score for each of the 27 items. This was an attempt to identify the degree of consensus on the issues, “What are the components of the spiritual dimension?” and “TO what extent should the spiritual dimension be included in the health education professional
TA =graduate teaching associate; A = active health education experts; R =retired health education experts
~~~ ~~
IMPLICATIONS Data from this study indicated that the majority of
the health educators surveyed believe there is a spiritual dimension of health and that this dimension should be included in the health education professional preparation program. Based on the data collected, the researcher developed a definition of the spiritual dimension of health based on four aspects: a unifying force within individuals; meaning in life; a common
APRIL 1980 THE JOURNAL OF SCHOOL HEALTH 199

TABLE 6 Individual Item Analysis
for the Second Questionnaire
A: B: C:
Statement should be r a i s e d more than two p o s i t i o n s Statement i s w i t h i n two p o s i t i o n s above o r below t h e p o s i t i o n you b e l i e v e i s most app rop r ia te Statement should be lowered more than two p o s i t i o n s
T.A. ACTIVE
A(%): 25.00 15.00 B ( % ) : 60.00 70.00 C(%) : 15.00 15.00
A(%) : B(%) : C(%) :
A( %) :
A( %) : B(%) : C(%) :
A( %) : B ( % ) : C( %) :
A(%) :
C(% :
A( %) : B(%): C( %) :
C( %) :
A(%) : B(%) : C(%) :
C(%) :
A( %) :
16.66 5.55 83.33 77.77
0 16.66
11.11 5.36 72.22 78.95 16.66 15.79
27.77 10.52 55.55 73.68 16.66 15.79
22.22 31.57 72.22 63.16 5.55 5.26
11.11 31.58 83.33 68.42
5.55 0
23.52 10.52 64.70 73.68 11.76 15.79
27.77 10.52 55.55 68.42 16.66 21.05
25.00 16.66 75.00 61.11
0 22.22
5.55 11.76 77.77 76.47 16.66 11.76
21.05 20.00 63.16 60.00 15.79 20.00
A ( % ) : 0 10.00 B(%): 95.24 85.00 C(%): 4.76 5.00
33.33 15.00 $~~~ 52.44 75.00 C(%): 14.33 10.00
200
RETIRED
20 * 00 80.00
0
11.11 66.66 22.22
12.50 75.00 12.50
25.00 62.50 12.50
10.00 90.00
0
11.11 77.77 11.11
11.11 88.88
0
33.33 44.44 22 0 22
11 -11 77.77 11.11
0 100.00
0
22.22 66.66 11.11
0 100.00
0
0 75.00 25.00
OVERALL
20.00 68.00 12.00
11.11 77.78 11.11
8.89 75.55 15.55
20.00 64.44 15.55
23.40 72.34
4.25
19.56 76.09
4.53
15.55 73.33 11.11
21.74 58.69 19.56
18.60 69.77 11.63
6.81 81.82 11.36
20.83 62.50 16.66
4.08 91.84
4.08
20.41 65.31 14.28
QUEST ION
1. To what e x t e n t do you pe rce i ve t h e s p i r i t u a l dimension as being a v i t a l f a c t o r i n your h e a l t h ? (6.47)
2. I f you r a t e d I t em One as r e l a t i v e l y un impor tant o r h ighe r , t o what e x t e n t a re t h e f o l l o w i n g considered t o be under- l y i n g components o f you r s p i r i t u a l d imension?
a. pe rcep t ion o f what i t i s t h a t causes the universe t o work the way i t does; (5.93)
b. something t h a t i s perce ived as being unknown o r h a z i l y known o r something f o r which t h e r e i s n ' t any easy exp lana t ion and so i t becomes a ma t te r o f f a i t h ; (5.30)
something f o r which t h e r e i s no r a t i o n a l explanat ion; r e c o g n i t i o n o f powers beyond t h e n a t u r a l and r a t i o n a l ;
a s e t o f p r i n c i p l e s o r e t h i c s t o l i v e by; (7.61)
c.
(5.47)
d.
e. something which g i ves meaning o r purpose t o l i f e ; (8.22)
f. the sense o f se l f l essness and a f e e l i n g f o r o the rs ; a w i l l i n g n e s s t o do f o r o the rs more than f o r y o u r s e l f ; (6.93)
g. commitment t o God, an U l t ima te Concern, e t cetera; (6.47)
h. i nvo l ves a s u r v i v a l issue; (4.97)
i. t h e most pleasure-producing q u a l i t y o f humans because i t ' s so hard t o grasp. (4.66)
3. To what e x t e n t do you perce ive t h e s p i r i t u a l dimension o f h e a l t h should be i nc luded i n the h e a l t h educat ion p ro fes - s i o n a l p repara t i on program? (6.16)
I f you r a t e d I t em Three as r e l a t i v e l y unimportant o r h igher , how do you t h i n k t h e s p i r i t u a l dimension o f h e a l t h cou ld be taugh t most e f f e c t i v e l y ?
a. by recogn iz ing t h e d i v e r s i t y o f s tudent backgrounds and recogn iz ing t h a t t h e s p i r i t u a l dimension may mean d i f f e r e n t t h i n g s f o r d i f f e r e n t people; (8.14)
b. by recogn iz ing t h e d i v e r s i t y o f s p i r i t u a l b e l i e f s t ruc tu res ; (7.62)
4.
THE JOURNAL OF SCHOOL HEALTH APRIL 1980
T.A. ACTIVE RETIRE0 OVERALL QUESTION
A( %) : B(%) : C(%) :
A( %) :
C(%) :
A( %) :
C( %) :
B( %) :
B(%) :
I[:{ i C( %) :
A( %) : B(%) : C( %) :
i C( %) :
B(% :
A(%) : B(%): C(%) :
A(%) : B(%): C(%):
C(%) :
C(%) :
B(% : C( %) :
A( %) :
A(%) :
20.00 20.00 50.00 55.00 30.00 25.00
25.00 10.00 70.00 85.00 5.00 5.00
9.52 20.00 85.71 70.00
4.77 10.00
14.28 20.00 80.95 75.00 4.77 5.00
23.81 27.78 66.66 66.66
9.52 5.55
23.81 10.53 76.19 73.68
0 15.79
19.05 15.00 80.95 65.00
0 20.00
33.33 25.00 66.66 70.00
0 5.00
28.57 25.00 71.43 65.00
0 10.00
9.52 0 80.95 75.00
9.52 25.00
23.81 20.00 71.43 65.00 4.76 15.00
38.09 10.00 61.90 75.00
0 15.00
18.18 15.00 59.09 70.00 22.73 15.00
13.64 10.53 63.64 73.68 22.72 15.79
22 0 22 55.55 22.22
12.50 87.50
0
25.00 62.50 12.50
37.50 62.50
0
22 * 22 55.55 22.22
33.33 66.66
0
0 71.43 28.57
12.50 75.00 12.50
12.50 50.00 37.50
22.22 44.44 33.33
0 62.50 37.50
12.50 75.00 12.50
44.44 44 * 44 11.11
37.50 62.50
0
20.41 53.06 26.53
16.66 79.17 4.17
16.33 75.51
8.16
20.41 75.51 4.08
25.00 64.58 10.42
20.41 73.47 6.12
14.58 72.92 12.50
26.53 69.39 4.08
24.49 65.31 10.20
8.00 73.00 20.00
18.37 67.35 14.28
22.45 69.39
8.16
21.57 60.78 17.65
16.33 67.34 16.33
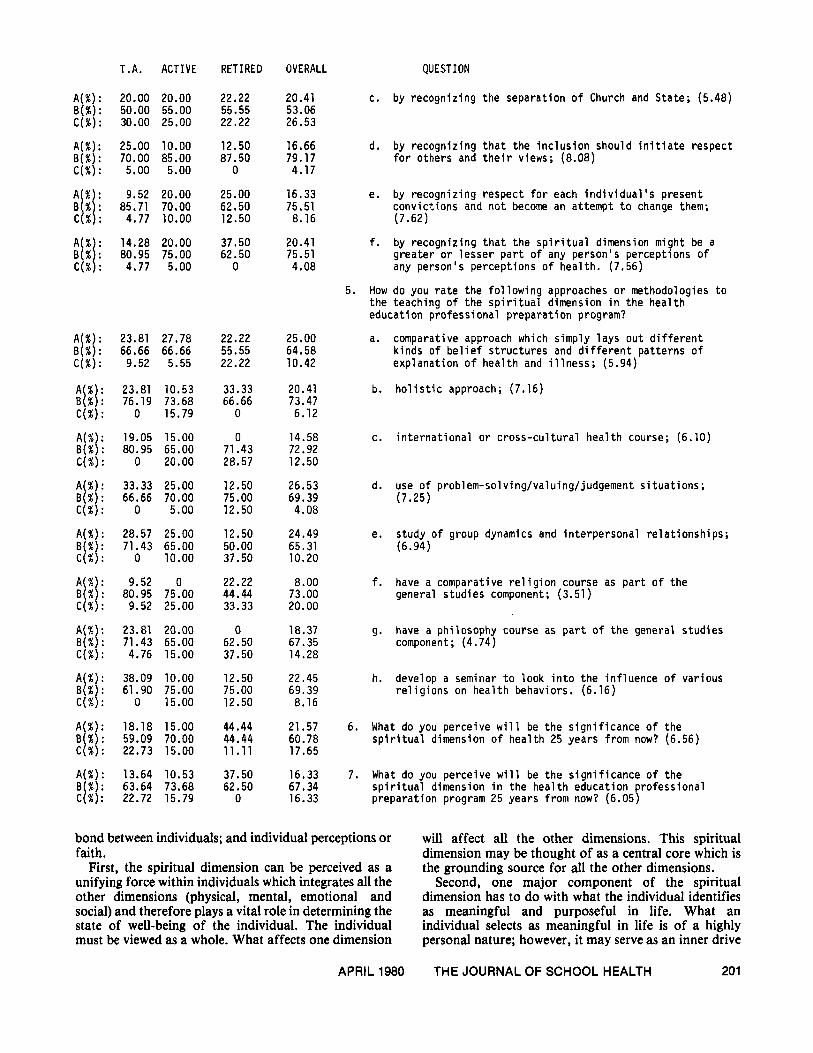
c. by recogniz ing the separat ion o f Church and State; (5.48)
d. by recogniz ing t h a t t h e i n c l u s i o n should i n i t i a t e respect f o r o thers and t h e i r views; (8.08)
e. by recogniz ing respec t f o r each i n d i v i d u a l ' s present conv i c t i ons and ncjt become an at tempt t o change them; (7.62)
g rea te r o r l esse r p a r t o f any person 's percept ions o f any person 's percept ions o f hea l th . (7.56)
How do you r a t e the f o l l o w i n g approaches o r methodologies t o t h e teaching o f t h e s p i r i t u a l dimension i n t h e h e a l t h educat ion p ro fess iona l p repara t i on program?
f. by recogn iz ing t h a t t h e s p i r i t u a l dimension might be a
5.
a.
b.
C.
d.
e.
f.
9.
h.
comparative approach which s imply l a y s ou t d i f f e r e n t k inds o f b e l i e f s t r u c t u r e s and d i f f e r e n t pa t te rns o f explanat ion o f h e a l t h and i l l n e s s ; (5.94)
h o l i s t i c approach; (7.16)
i n t e r n a t i o n a l o r c r o s s - c u l t u r a l h e a l t h course; (6.10)
use o f problem-solving/valuing/judgement s i t u a t i o n s ; (7.25)
study o f group dynamics and in te rpe rsona l re la t i onsh ips ; (6.94)
have a comparative r e l i g i o n course as p a r t o f t h e general s tud ies component; (3.51)
have a phi losophy course as p a r t o f t h e general s tud ies component; (4.74)
develop a seminar t o look i n t o t h e i n f l uence o f var ious r e l i g i o n s on h e a l t h behaviors. (6.16)
6. What do you perce ive w i l l be t h e s i g n i f i c a n c e o f t h e s p i r i t u a l dimension o f h e a l t h 25 years f rom now? (6.56)
7. What do you perce ive w i l l be t h e s i g n i f i c a n c e o f t h e s p i r i t u a l dimension i n t h e hea l th educat ion ro fess iona l preparat ion program 25 years f rom now? (6.05p
bond between individuals; and individual perceptions or faith.
First, the spiritual dimension can be perceived as a unifying force within individuals which integrates all the other dimensions (physical, mental, emotional and social) and therefore plays a vital role in determining the state of well-being of the individual. The individual must be viewed as a whole. What affects one dimension
APRIL 1980
will affect all the other dimensions. This spiritual dimension may be thought of as a central core which is the grounding source for all the other dimensions.
Second, one major component of the spiritual dimension has to do with what the individual identifies as meaningful and purposeful in life. What an individual selects as meaningful in life is of a highly personal nature; however, it may serve as an inner drive
THE JOURNAL OF SCHOOL HEALTH 201

for that individual’s life accomplishments. The basic needs or wants of individuals usually include the “want to live,’’ and this could be considered part of this aspect.
Third, this spiritual dimension is somewhat different from most of the other known dimensions of humans (physical, mental and emotional) in that it transcends the individual, thus it has the capacity to be a common bond between individuals. Components which could be placed in this aspect of the spiritual dimension would include: commitment to God/Ultimate Concern/ Cosmic Force; the sense of selflessness and a feeling for others; and a set of principles or ethics which govern our conduct. This common bonding aspect can be described as a force which begins in the individual and then goes beyond that individual to share warmth/love/compas- sion with another. This could be perceived as the “caring center” within individuals.
Finally, because this dimension of humans is the least obvious and measurable of the known dimensions, it is based upon individual perceptions and faith. Included in this part of the spiritual dimension would be components having to do with perceptions of what it is that causes the universe to work the way it does;
recognition of powers beyond the natural and rational; survival; and pleasure. Just as each individual is a unique biological creation, each individual is also unique in the sense of hidher own perception of the cosmos because it is dependent upon the inner and outer experiences of that individual. Religious beliefs, if any, could be placed in any or all of the above identified aspects of the spiritual dimension.
REFERENCES
1. Bulka RP: Logotherapy and Talmudic Judism. J Religion and Health 14(4):277-283, 1975.
2. Frank1 VE: Man’s Search for Meaning. New York, Pocket Books, 1963.
3. Smith BJ: Selected writings and their relationship to an ontology of health: an analytical study. Doctoral dissertation, University of Illinois at Champaign-Urbana, 1976.
4. Tillich P: My Search for Absolutes. New York, Simon and Schuster, 1967.
5. Vaux K: Religion and health. Preven Med 5522-536, 1976.
Rebecca Banks, PhD, Assistant Professor & Co- ordinator of Health Education Programs, University of Minnesota-Duluth, Duluth, MN 55812.
PROFESSIONAL REFERRAL SERVICE
The PROFESSIONAL REFERRAL SERVICE (PRS) is available to all health professionals and t o organizations employing health professionals.
Advertisers compose their own classified ads and may request their identities be withheld from publication. Ad- vertisers receive a box number and all replies are forwarded promptly.
INQUIRIES: All inquiries concerning advertisers with box numbers should include the box number and be ad- dressed t o Professional Referral Service, ASHA, Kent, Ohio 44240.
ADVERTISING RATES: Placement of an ad by an in- dividual seeking employment is $15 for up t o 10 lines, each line averaging six words. Each line after the tenth line is $1.50 per line. Placement by an organization seeking an employee is $30 for up to 10 lines, each line averaging six words. Each line after the tenth line is $3 per line.
MULTIPLE INSERTION DISCOUNT: An ad printed in two consecutive issues will receive a 19% discount; five con- secutive issues, 15%; 10 consecutive issues, 20%.
ASSISTANT PROFESSOR - Doctoral degree in an appropriate field; skills in research design and statistics; experience in public school and/or college levels; with
some expertise in community organization. Teach undergraduate and graduate courses. Available Sept. 1980; nine-month appointment; tenure track. Salary open depending upon qualifications. Send vitae to: Miriam L. Tuck, Chairperson, Department of Health Education, Russell Sage College, Troy, NY 12180. An Equal Opportunity/Affirmative Action Employer.
HEALTH EDUCATION POSITION. The Health education program at the University of New Mexico is seeking one associate professor and one assistant professor. These are full time, tenure track positions. The associate position is for coordinator of the program and teaching graduate programs. The assistant professor position will include teaching community and/or school health education courses at the graduate - undergraduate level. A doctorate in health education is required for both positions. Detailed position descriptions available. To apply, send letter of application, a vitae, three letters or more of references and transcripts to: Dr. Paul B. Dearth, Health Education Program, Department HPER, University of New Mexico, Albuquerque NM 87 13 1. Application deadline April 15, 1980.
202 THE JOURNAL OF SCHOOL HEALTH APRIL 1980