Embed Size (px)
Citation preview

Health and social services department / The winning formula to beat malaria / April 2010 //
1
Advocacy report – 2nd edition updated with new data and case studies
The winning formula to beat malaria
© M
.Ha
lla
Ha
n/S
uM
ito
Mo
CH
eM
iCa
l-o
lyS
et
ne
t
Health and social services department / April 2010 //
2
nd e
dit
ion

Health and social services department / The winning formula to beat malaria / April 2010 //
2
There is growing scientific evidence to demon-strate that combining mosquito net distribution with follow-on “hang up” campaigns, carried out by trained volunteers in their own communities, increases net usage rates and significantly re-duces incidence of malaria.
Combining net distribution with follow-on sup-port and training at household level is crucial to reach the most vulnerable groups (such as those living in remote areas, refugees, people affected by stigma and discrimination) with limited or no access to government health services.
Trained volunteers who live in the same commu-nity as the beneficiary population and speak the same local language are ideally placed to help families overcome social or cultural barriers that could prevent the correct hanging and nightly use of nets.
Since 2002, as a direct result of net distributions carried out by National Red Cross and Red Cres-cent Societies — supported by the International Federation of Red Cross and Red Crescent Soci-eties (IFRC) — more than 300,000 malaria deaths have been averted, while 18.2 million people have been protected against malaria.
Significant progress has been made towards uni-versal coverage (providing nets to every house-hold to protect all persons at risk of malaria) and innovative new techniques are showing promis-ing results (such as home management of ma-laria in Kenya), but sustainable funding needs to be available to carry the success forward, to strengthen community involvement.
There is a need to expand operational research to determine the most effective and cost effective prevention and treatment packages.
Since 2002, the distribution of long-lasting in-secticide-treated mosquito nets (LLINs)1 has in-creased exponentially in sub-Saharan Africa. This
has been made possible due to the leadership of coun-tries with a malaria burden and thanks to the mobiliza-tion of international organizations and donors, who have united to stop malaria once and for all. Despite the many successes, malaria is still killing nearly 1 million people every year, mostly children under five years old, even though the disease is 100 per cent preventable and treatable.
In Africa malaria-carrying mosquitoes bite from dusk to dawn, so nightly use of nets provides the most cost effec-tive protection against malaria.
Red Cross Red Crescent supported pilot efforts in Ghana, Zambia and Togo between 2002 and 2004 helped demonstrate to the world’s public health com-munity that free distribution of nets combined with vaccination campaigns was one of the most effective and efficient ways to rapidly increase net coverage and nightly use. These large-scale efforts were logistically possible, in part through the coordinated support of thousands of volunteers mobilized by National Red Cross and Red Crescent Societies working in partner-ship with their ministries of health, national malaria control programmes and in-country partners. With the shift in 2008 from targeted coverage of the most vulnerable populations (children under five and preg-
nant women) to the objective of universal coverage (covering all populations at risk), the Red Cross Red Crescent has continued to work towards meeting the Roll Back Malaria 2010 targets and Millennium De-velopment Goals through the actions of community-based volunteers.
ObjectiveMalaria programmes being implemented by National Red Cross and Red Crescent Societies will contribute to achieving the Roll Back Malaria 2010 targets and the UN Secretary General’s call for “universal coverage of all populations at risk from malaria by the end of 2010.” Red Cross Red Crescent malaria programmes also con-tribute to the attainment of the Millennium Develop-ment Goals, especially Goal 4 (reduce child mortality), Goal 5 (improve maternal health) and Goal 6 (combat HIV/AIDS, malaria and other diseases). These goals are interlinked. MDG 4 and 5 will not be achieved if there is no targeted support for Goal 6.
Countries that have achieved high coverage of their pop-ulations with mosquito nets, as well as improved access to effective diagnostics and treatment, have shown enor-mous progress in the fight against malaria. Countries such as Eritrea, Rwanda, Zambia, Tanzania, and Sao Tome and Principe have seen reductions in malaria cases and deaths of up to 50 per cent, demonstrating that the MDG targets can be achieved.
Main findings
1. To make reading easier, we are using the word « nets » instead of LLINs all across this report, meaning “ insecticide-treated mosquito nets”.

Health and social services department / The winning formula to beat malaria / April 2010 //
3
Skilled volunteers, not just workforceVolunteers have played, and will continue to play, a valu-able role during mass distribution campaigns. They un-dertake a number of key activities to complement the distribution of nets: promoting a better understanding of the danger signs and risks of malaria, providing informa-tion on how to effectively prevent the disease and identi-fying where to access treatment within 24 hours of the onset of symptoms. Crucially, volunteers also carry out the personal follow-up household hang up visits. This clearly indicates that volunteers are, above all, trained community resource people with specific skills to give support and training, as well as enable communities to respond to malaria. Put simply, volunteers are the most effective means to inform, engage and empower commu-nities to protect them against malaria infection.
The “hang up” campaignsVolunteers are active in all phases of the campaign: be-fore, during and after the net distribution.
Before the distribution, Red Cross Red Crescent volun-teers make sure their local community is aware that the
distribution is taking place and they encourage families to go and get a free net. They ensure that families know where to go to receive nets, when the distribution will take place, the criteria for distribution (such as specific age groups or when vouchers are used to identify people at risk), how many nets the family will receive and the importance of using the nets every night to prevent ma-laria. If the campaign is multi-faceted (for instance com-bined with an immunization campaign for measles or polio), they also make sure families understand how es-sential it is to take their children to the vaccination post to be immunized.
The second action takes place during the campaign itself, with volunteers helping with the logistics and distribution of the nets. Volunteers organize and run hang up pavilions at each distribution site. These hang up pavilions show nets hanging correctly, and mes-sages from volunteers emphasize that all members of the family should sleep under their nets every night. The material used to demonstrate correct net hanging and use in hang up pavilions varies with the local con-text. In all cases, locally available hanging materials and beds will be used to ensure that beneficiaries see a demonstration of correct net hanging and usage in an environment that reflects their own situation. During
JeR
oe
n o
eR
leM
an
S

Health and social services department / The winning formula to beat malaria / April 2010 //
4
the campaign, volunteers continue to follow up with community members to ensure that they have benefit-ted from the interventions being offered by the minis-try of health.
The third action is the hang up campaign itself. Hang up activities take place immediately following net distribu-tions, and again just before the start of the rainy season. During house-to-house hang up visits, volunteers are as-signed a number of households that they are responsible for visiting. Volunteers make sure household members understand the danger signs of malaria and refer sick people to health facilities where they can be diagnosed and treated. During the household visit, they ensure the net is correctly installed and check that families and community members know how to use the net (for ex-ample, that the net should be tucked in under the sleep-ing mat to prevent entry of mosquitoes) and in different situations (for example, that the net can be used outside in situations where families sleep outdoors during the dry season, or planting, harvest season).
Red Cross Red Crescent volunteers pass the message that everyone should sleep under an insecticide treated net every night. In situations where households do not have enough nets to cover every sleeping space, messages are passed that the populations most vulnerable to malaria (children under five years of age, pregnant women, peo-ple that are living with HIV) should be given priority for sleeping under the nets available in the household.
In some cases, hang up campaigns lead into more com-prehensive multi-year communities fighting malaria pro-grammes (formerly called “keep up”). These programmes cover all malaria prevention and control options available at community level, and include activities to promote net ownership and usage, household spraying, access to ef-fective diagnosis and treatment at health facility or house-hold level, intermittent preventative treatment during pregnancy and infancy (according to ministry of health policy), as well as completion of the childhood routine vaccination series and attendance of pregnant women at antenatal care clinics.
Whether they are involved in hang up campaigns or communities fighting malaria programmes, the main ad-vantage that volunteers bring is that they live in the very same community that they serve, which means that they can talk to beneficiaries using the local language and with an understanding of the community context. They are also fully aware of local realities and customs that might prevent the hanging and nightly use of nets by the family members and are ideally placed to identify the most vulnerable members of the community.
The IFRC believes the formula to beat malaria will come through empowering communities to comprehensively respond to the disease. When community-based volun-teers provide knowledge, prevention and treatment op-tions, communities are genuinely empowered to be the most effective first responders to this ancient scourge.
JeR
oe
n o
eR
leM
an
S

Health and social services department / The winning formula to beat malaria / April 2010 //
5
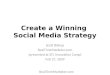
More Than 300,000 lives saved, 18.2 Million people proTecTed
Method of calculation for the number of lives saved:
Figure based on the Cochrane Review (Lengler study) that states for every 1,000 children sleeping under nets, 5.5 lives will be saved each year at 70 per cent net usage (Red Cross Red Crescent programmes achieve 70 per cent net usage).
Based on a total of 14 million nets distributed that are effective for three years, with an average of 1.3 people sleeping under a net, 300,300 lives saved over a three-year net lifespan.
Calculation: 3 year net [14,000,000 nets x 1.3 (average number of benefi-ciaries per net) / 1000] x 3 year net effectiveness x 5.5 lives saved per 1000 = 300,300
20
15
10
5
02002 2009
18.2 million
Millions of people protected since 2002
300,000250,000
200,000
150,000
100,000
50,0000
2002 2009
300,300
Number of lives saved since 2002
The IFRC will further step up its efforts by developing more hang up campaigns and will team up with partners to accelerate the delivery of nets to all malaria-en-demic areas.
In 2009, National Red Cross and Red Crescent Societies reached 3.7 million households or 14.8 mil-lion individuals through communi-ty-based activities to prevent ma-laria and ensure care providers are aware of malaria danger signs and the need to immediately access ef-fective treatment.
In 2010 National Red Cross and Red Crescent Societies will under-take malaria activities in the follow-ing countries: Haiti, Indonesia, India, Senegal, Mali, Burkina Faso, Ghana, Sierra Leone, Liberia, Cote d’Ivoire, Togo, Benin, Angola, Nigeria, Cam-eroon, Equatorial Guinea, Demo-cratic Republic of Congo, Malawi, Madagascar, Tanzania, Burundi, Rwanda, Kenya, Uganda, Sudan, Zimbabwe.
In addition to mass distribution and hang up campaigns, the IFRC also includes a malaria component in its emergency response activities when disasters take place in malaria en-demic areas or where epidemics are possible as a result of the disas-ter that has occurred.
As a result of mosquito net distributions supported by National Red Cross and Red Crescent Societies since 2002, more than 300,000 ma-laria deaths have been averted, while 18.2 million people have been protected.
Method of calculation for the number of people protected: 14 million nets distributed since 2002. On average 1.3 people sleep under the net or 14,000,000 x 1.3 = 18,200,000 people protected (see box explaining how we reached these numbers).

Health and social services department / The winning formula to beat malaria / April 2010 //
6
Measuring impactWhile measuring the coverage of net distributions in terms of household ownership has been relatively straightforward, measuring use has been more chal-lenging and even controversial. While it may be rela-tively easy to conduct surveys showing how many peo-ple received and retained a campaign net, it proves more difficult to know how many people slept under the net the previous night.
However, there are now a number of independent studies that show a clear trend. Results from the 2009 Togo na-tional net coverage and usage survey conducted by Health-Bridge show a 23 per cent increase in net usage following a single visit from a community based volunteer. Similar data was produced by the Centers for Disease Control and Prevention (CDC) survey on net coverage and usage in Sierra Leone (November 2007). In Sierra Leone, the data shows a 22 per cent increase in net utilization following a household visit by a community-based volunteer. The evi-dence is mounting to show the added value of community level actions that ensure nets are used every night.
Since 2004, a number of surveys have been published, all showing an increase in the use of mosquito nets where community-based volunteers are mobilized and encour-aged to visit households that have received nets.
The table below contains data from surveys conducted by CDC and HealthBridge showing the effect of household visits from a community-based volunteer in terms of the proportion of households using a mosquito net. Net us-age is typically between 10 and 23 percentage points higher in households that received a visit from a volun-teer than in households that did not receive a visit. This highlights the crucial importance of personal follow up and support to encourage behaviour change if malaria is to be prevented and the toll it takes on families and com-munities reduced.
Social and cultural differences“There are interesting differences in net usage between regions of Africa,” explains Jason Peat, the IFRC malaria programme manager.
“For instance, some countries in West and Central Africa tend to use the nets more widely, a culture of net use is already in place, and one of the principle challenges is ensuring there are enough nets in the household to en-sure every sleeping space is covered. In other countries, and due to regional differences within countries, a cul-ture of net use is still being developed and net use is much lower than expected.
Countries Without household visit % With household visit %
Togo (2009) 52 75
Togo (2006) 43 66
Niger 55 67
Sierra Leone 51 73
Madagascar (26 districts) 82 93
Mali 76 85
Togo Programme National de Lutte contre le Paludisme, Ministry of Health / Demographic Research Unit, University of Lomé / Togo 2009 and HealthBridge. Jenny Cervinskas
Togo CDC October 2005. Adam Wolkon, Jodi Vanden Eng, D.J. Terlouw
Niger CDC March 2006. Natasha Hochberg, Jodi Vanden Eng, James Eliades, Marcel Lama
Sierra Leone CDC November 2007. Manisha Kulkarni, Jodi Vanden Eng, Adam Wolkon
Madagascar HealthBridge / CDC Manisha Kulkarni, Rachelle Desrochers, Jim Goodson, Jo-Anne Mandy, Annett Cotte, Jenny Cervinskas, Jodi Vanden Eng
Mali Health Bridge / Jenny Cervinskas, Peter Berti, Rachelle Desrochers, Jo-Anne Mandy, Manisha Kulkarni

Health and social services department / The winning formula to beat malaria / April 2010 //
7
“In these countries, net distribution is followed up by in-tensive hang up campaigns to promote that high nightly usage rates are achieved and maintained.”
Focusing on the most vulnerableMalaria is preventable and curable. However, it is also a disease of poverty. People living in low-income coun-tries are more likely to suffer because of lack of money and limited access to healthcare, especially for those liv-ing in rural areas. However, people living in urban areas are also affected, especially those living on the edge of
cities, in slums that do not benefit from basic services such as access to water, garbage disposal and healthcare. Costs such as transport to health facilities, fees for con-sultation by medical personnel, malaria treatment, lost wages when a family member is ill with malaria or car-ing for a child with the disease, have severe consequenc-es on household resources. According to the Roll Back Malaria Partnership, malaria costs Africa at least 12 bil-lion US dollars in direct losses and much more in lost economic growth.
To be able to focus attention on the most vulnerable populations in a country, volunteers need to have a comprehensive knowledge of the community in which they work and live. In most cases, the most vulnerable populations (children under the age of five and preg-nant women, populations without access to health serv-ices, people living with HIV, stigmatized groups, refu-gees, migrants, people living in poorer areas of big cities) need a specially tailored programme since they are more likely to be negatively affected by malaria than other members of the community. The risks are higher for these groups due to their vulnerable status and be-cause they have limited access to health service and public information campaigns. When working with the most vulnerable populations, there is a need to commu-nicate the heightened risks associated with malaria and the danger signs so that people who are affected know they need to access treatment immediately upon onset of symptoms.
Cultural and social barriers can also prevent the correct use of the nets. According to a recent study from the Tulane University School of Public Health, there is evi-dence that some families who only own one net will have the head of the family sleep under it instead of the most vulnerable members of the household: children under the age of five and pregnant mothers. The Tulane study also shows that children often sleep in kitchens or a common room, which necessitates removing and re-hanging the net daily, something that does not neces-sarily happen every night. Yet, nightly use of the mos-quito net is critical as one mosquito bite can be enough to cause malaria.
All these reasons illustrate that whether the net usage is up by 10 per cent or 20 per cent depending on com-munities and countries, the action of community-based volunteers yet again proves essential to reduce malaria cases over the long term. The impact of ma-laria on communities and countries will not be re-duced until we can significantly reduce transmission of the disease and reduce mosquito populations. All affected communities need to be protected and have access to effective treatment.
10 KeY facTs aBoUT Malaria1. Malaria is a killer disease. It kills nearly 1 million
people a year.
2. 85 per cent of deaths are children under 5 years of age.
3. Nearly 250 million malaria cases are reported every year.
4. Malaria affects 40 per cent of the world’s population, putting 3.3 billion people at risk in 108 countries.
5. Children under the age of five and pregnant women are the most at risk from malaria
6. Malaria consumes as much as 40 per cent of public health expenditure in countries where it is endemic.
7. Malaria is a primary cause of poverty and puts additional burdens on health systems and families.
8. In Africa, mosquitoes that transmit malaria bite from dusk to dawn, so malaria nets provide effective protection.
9. There is currently no malaria vaccine approved for human use.
10. Since 2002, as a direct result of net distributions carried out by National Red Cross Red Crescent Societies supported by the IFRC, more than 300,000 malaria deaths have been averted, while 18.2 million people have been better protected against malaria.
Sources: 1-9: World Health Organization, Roll Back Malaria; 10: IFRC

Health and social services department / The winning formula to beat malaria / April 2010 //
8
Working with partnersBecause decreasing the burden of malaria is such a huge task, a coordinated effort is needed to expand the ownership and use of mosquito nets. The IFRC chairs the Alliance for Malaria Prevention (AMP)2, a part-nership of more than 40 organizations including gov-ernment, business, faith-based, and humanitarian or-ganizations. It is also a member of the Roll Back Malaria3 partnership.
At the country level, the ministry of health, representing the government of the country, leads the coordination of international and in-country partners, and is supported by National Red Cross and Red Crescent Societies, work-ing together towards malaria prevention and control.
Building more resilient communities
Whether through mass mosquito net distribution cam-paigns or house-to-house activities to ensure nets are cor-rectly hung and fever is immediately treated, the message the IFRC would like to deliver is still the same: empow-ering communities is essential to reach the most vulner-able individuals and households and reduce the malaria burden. The necessity of informing people about the threat of malaria and ensuring they know how to hang and use the net they have received is clear. Now, evidence confirms that this is the right way to go if we want to roll back malaria throughout the world.
2. http://www.allianceformalariaprevention.com/3. http://www.rollbackmalaria.org/

Health and social services department / The winning formula to beat malaria / April 2010 //
9
Here is a selection of web links where you can find out more information on malaria activities from National Red Cross and Red Crescent Societies around the world as well as other useful links on malaria.
IFRC.org malaria section http://www.ifrc.org/what/health/diseases/malaria/index.asp
IFRC.org World Malaria Day page http://www.ifrc.org/what/health/diseases/malaria/malariaday.asp
IFRC.org malaria toolkit page http://www.ifrc.org/what/health/diseases/malaria/toolkit.asp
Community Based Health and First Aid in action tools http://www.ifrc.org/what/health/firstaid/tools.asp
Roll Back Malaria Partnership http://www.rollbackmalaria.org/
World Malaria Day 2010 http://www.rollbackmalaria.org/worldmalariaday/index.html
Alliance for malaria prevention (AMP) website http://www.allianceformalariaprevention.com/
Malaria section of the WHO website http://www.who.int/topics/malaria/en/
Malaria section of the Centers for Diseases Control and Prevention (CDC) http://www.cdc.gov/malaria/
Malaria section of the Global Fund http://www.theglobalfund.org/en/malaria/
President’s Malaria Initiative website http://www.fightingmalaria.gov/
IFRC social media
Facebook: http://www.facebook.com/RedCrossRedCrescent
Twitter: http://twitter.com/Federation
Photos: http://www.flickr.com/ifrc
Videos: http://www.youtube.com/ifrc
Blog: http://ourworld-yourmove.org/blog-english/
online resoUrces
Be
n H
on
dik

Health and social services department / The winning formula to beat malaria / April 2010 //
10
in 2009, the Burkinabe Red Cross Society and the Ministry of Health piloted the first universal coverage
distribution in the country in the district of diébougou. in diebougou, every household was provided with suf-ficient long-lasting mosquito nets to cover all members of the household. the pilot distribution is being used to guide a national level distribution that will take place in 2010 throughout the country. the Burkina Faso Red Cross volunteers and staff played a major role in the pilot project and will continue to support the Ministry of Health with covering the rest of the country.
“Smile!” this is a good moment for a family portrait, as ihiri Justin Sonda and his extended family have just received nine insecticide-treated mosquito nets. they pose happily for a camera in front of their house in diébougou, in south-western Burkina Faso.
altogether 67,400 nets were distributed by Red Cross Red Crescent volunteers during the first week of July 2009 in Burkina Faso’s diébougou health district. the
campaign, primarily financed by the international Fed-eration of Red Cross and Red Crescent Societies (iFRC), was one of the first ever to apply new World Health organization (WHo) guidelines for universal coverage with nets, covering every sleeping space.
ihiri Justin Sonda, with 17 people in his household and nine sleeping spaces, was therefore entitled to nine mosquito nets. Before, they had two nets in the house, and malaria was common. the two nets al-ready in his possession were not long-lasting ones, which provide the most effective protection, and so they were replaced with better nets during the distri-bution.
high malaria prevalence
“Recently, i spent two days in the hospital because of malaria. during my convalescence, our seven-month-old baby was treated in intensive care, also for malaria.
Achieving universAl coverAge: The exaMple of BUrKina faso

Health and social services department / The winning formula to beat malaria / April 2010 //
11
two years ago, we lost a one-month-old baby girl be-cause of malaria. i hope these nets will improve health in our family,” ihiri Justin Sonda says.
Before the shift to universal coverage, mosquito net distributions targeted children under five and pregnant women. due to limited access to nets the maximum number of nets per family was often two.
With a population of around 110,000 people, dié-bougou is in one of the most malaria-prone regions of Burkina Faso. the environment is characterized by rich vegetation, several dams and poor sanitation fa-cilities, all factors that support a high-density mosqui-to population. Half of the consultations in local health centres are linked to malaria and child mortality due to malaria is high.
Jefferson Sié kam, a father of seven, is one of the vol-unteers helping with the diébougou distribution cam-paign. after having distributed more than 300 nets in his own village of Sorindigui, he visits his friends and neighbours to discuss the causes of malaria, how to use nets correctly and the need to immediately access health services when the danger signs of malaria are recognized.
Modern medicine “Sometimes it is hard to convince people who have symptoms of malaria to go to the health centre,” he says. “People have strong habits of using medicinal plants and traditional healers and some of them don’t believe in modern medicine. Fortunately, mosquito nets are widely accepted and people understand the importance to sleep under them.”
elyse kam, 21, listens to Jefferson attentively when he explains symptoms of severe malaria during a house visit. all this brings back painful memories from March this year when she lost her first child, aged only four months, because of malaria. She still finds it hard to talk about the death but has decided to share her experiences if she could that way help others.
“Here in Burkina Faso, people often say: ‘a long life is linked to the way we protect ourselves’. i would like to engage in the sensitization activities on malaria. When i watched the volunteers during the mosquito net dis-tribution, i realized that it’s an excellent way to help the community,” says elyse.
in addition to the iFRC, the Burkina Faso mosquito net distribution campaign was supported by uniCeF, WHo, national Malaria Control Programme, Plan and Japan international Cooperation agency. the Ministry of Health was involved in the training, census, distribu-tion, and supervision of all activities.
Text and photos: Noora Kero
a “winning forMUla” in BUrKina faso 99.7 per cent of households received a net during
the distribution.
98 per cent of these households received a hang up visit from a Red Cross volunteer.
Before the distribution net usage the night before was 15 per cent. Following the four day distribution and two weeks of hang up activities net usage the night before rose to 85 per cent (an increase of 70 per cent)
Lessons learned from the 2009 Diébougou distribution will be applied to the 2010 nation-wide universal coverage campaign.
Source: « Rapport technique, campagne de distribution de Diébougou, ministère de la Santé du Burkina Faso, juillet 2009.

12
WHile Bed netS HelP PRevent MalaRia, nets alone cannot prevent all cases of the dis-
ease. the kenya Red Cross Society – in partnership with the kenyan Ministry of Health, the World Health organization and with funding and technical sup-port from the Canadian Red Cross – is now leading the way in ensuring remote communities with poor access to health services can access effective ma-laria treatment through a home-based treatment project in kenya’s eastern coast.
Malaria often kills children soon after the onset of symptoms. While the most effective drugs are current-ly available in kenya, timely access to the medication is not always possible, especially in rural communities. a child can die from malaria in as little as 24 hours after the first symptoms appear, so accessibility to appro-priate and effective treatment is key. the project is currently underway in two districts on kenya’s east coast - lamu and Malindi - and will help determine if utilizing trained Red Cross Red Crescent volunteers is
KenYa: going beyond prevention with hoMe ManageMenT of Malaria
tHe togo Red CRoSS SoCiety conducted the first country-wide free distribution of mosquito
nets to children under five years of age in december 2004, with support of the iFRC and Canadian Red Cross. 905,000 nets were distributed during a one-week integrated child survival campaign that also in-cluded measles and polio vaccination and presump-tive treatment for intestinal worms.
the Red Cross Red Crescent’s commitment did not end there. Following the mass distribution a three year communities fighting malaria programme was started. it followed the three year effective lifespan of the nets and promoted net ownership, correct net hanging, nightly usage, recognition of the danger signs of ma-laria and the need for immediate treatment, the comple-tion of the routine childhood vaccination series, and at-tendance at antenatal care clinics by pregnant women.
in december 2008 with support from the Canadian Red Cross, the togo Red Cross supported a second country wide mass distribution of nets. the togo Red Cross provided 847,000 of the 1.2 million nets needed to cover the country. almost 3,800 Red Cross volun-teers were mobilized throughout the country in this massive life-saving campaign.
Since the 2004 distribution, the Canadian Red Cross and the iFRC have funded six years of communities fighting malaria activities, until 2011, to support the country in efforts to achieve the Roll Back Malaria 2010 targets and the 2015 Millennium development goals.
Results from the 2009 togo national net coverage and usage survey conducted by HealthBridge show a 23 per cent increase in net usage following a single visit from a community based volunteer1, confirming previ-ous figures showing a very significant contribution to reducing the burden of malaria in togo.
Togo: much more thAn A “one off”
1. The table on page 4 mentions figures showing improvements for net usage
Be
no
it M
aS
Hta
-Ca
RP
en
tie
R
Health and social services department / The winning formula to beat malaria / April 2010 //

13
an effective solution in the fight against malaria. na-tional Red Cross and Red Crescent Societies have a strong volunteer base rooted at the community level. this allows them to play a vital role in bridging the gap for those with little or no access to health services and information.
this is especially acute in remote communities with limited to no access to health services due to distance or the inability to pay for service. the kenya Red Cross project aims to determine the best, most effective strategies to ensure fast access to life-saving drugs so children who fall ill with malaria can be cured.
kenya Red Cross Society volunteers are trained to pro-vide life-saving artemisinin combination therapy (aCt) drugs to remote communities with poor access to health services, in line with the kenyan Ministry of Health poli-cy. this drug combination is the most effective treat-ment for those who have contracted malaria and the programme aims to reach individuals who may not ac-cess a health centre in time to receive treatment.
Key dataa baseline survey for this project was conducted be-tween november 2008 and January 2009. twelve months later (december 2009 to January 2010) an end line survey was conducted by the kenya Medical Re-search institute.
intervention results show use of community health workers improved access to aCts for fever manage-ment, increased the access and use of nets in the
population, improved uptake of intermittent preventive treatment among pregnant women in these communi-ties and improved early treatment-seeking behaviour among female care givers (including referral for cases of severe malaria).
Activity Baseline % Endline % Change + / -
Main source of advice on treatment – 2% 36% 34 increase RC volunteers / community health workers
Source of Artesunate Lumefantrine 0% 45% 45 increase treatment for children below 5 years
Increase in attendance at antenatal 62% 66% 4 increase care clinics by pregnant women
Treatment of children with ACTs 9% 30% 21 increase within 24 hours of the onset of fever
Children adhering to 3 day ACT 61% 70% 9 increase treatment course
Children slept under a net 56% 67% 11 increase the night before
WCCT knowledge of new antimalaria 25% 33% 8 increase being promoted by MoPHS
Kenyan Medical Research Institiute (KEMRI) March 2010
Sa
ltB
on
eS
, ol
av
a./
no
RW
eg
ian
Re
d C
Ro
SS
Health and social services department / The winning formula to beat malaria / April 2010 //

14
beyond AfricAMalaria in haiTi: turning trAgedy into opportunity
MalaRia iS not only a diSeaSe that affects sub-Saharan africa. large areas of asia and
the americas are also hit and, in some places, ma-laria prevalence rates are as high as those in africa.
in the first edition of this report, Haiti was highlighted as a case study for long-term community-based ma-laria programmes. However, this was before the mag-nitude 7 earthquake that hit the country on 12 January, 2010, leaving as many as 200,000 people dead and up to a million homeless. the Haitian national Red Cross
Society was also severely affected with many of its structures being either damaged or destroyed.
However, thanks to the support of volunteers and staff from national Red Cross and Red Crescent Societies from all over the world, the iFRC set up the biggest disaster relief operation in the recent history of the in-ternational Red Cross and Red Crescent Movement to respond to this tragedy.
the earthquake that struck in Haiti certainly further fu-els the risks of malaria spreading. overcrowding in camps housing displaced people, insufficient access to water and sanitation, overloaded medical facilities and ruptured sewer systems provide favourable condi-tions for the breeding of malaria vectors. the situation is further complicated by the rainy season starting in May, the lack of sufficient insecticide-treated mosquito nets and the difficulties faced for correct hanging of them in the camps, and the risk of flooding and de-struction associated with the hurricane season that hits Haiti almost on an annual basis.
all this comes on top of the extremely strained health system. the earthquake has left Haitian health facili-ties damaged or destroyed, and the system is incapa-ble of dealing with the high demand from suffering pa-tients. despite the massive support by the Red Cross Red Crescent and other actors, a drastic increase in malaria cases in the coming months can threaten much of what has been achieved.
the response to those malaria risks by the Red Cross Red Crescent is actually an integrated one, covering all aspects of water-related risks from diarrhoea, epi-demic diseases, and malaria. the immediate response lies with distributing mosquito nets together with other humanitarian partners. in the first few days following the earthquake, two mosquito nets were included in the relief item packages that were distributed by the iFRC to 80,000 families. More than 3 million nets are planned to be distributed in the coming year by many partners supporting the Haitian Ministry of Health.
But more needs to be done to make sure malaria is controlled in Haiti and a key aspect is relaunching ma-laria prevention programmes involving community-
int
eR
na
tio
na
l F
ed
eR
at
ion
We
nd
ell
PH
illi
PS
Health and social services department / The winning formula to beat malaria / April 2010 //

15
based volunteers. Because of the scale of the disaster, malaria prevention will be included in a broader ap-proach that includes epidemic control, disaster pre-paredness and integrated health programmes in com-munities, as defined in the iFRC community-based health and first aid in action approach. it also involves building back the capacities of the Haitian national Red Cross Society by providing training to volunteers who can then inform communities about the risks of malaria, identify households who are most at risk, pro-vide them with a net, teach them how to use it and make sure the most vulnerable populations pregnant as well as children under 5 sleep under it. Communi-cation is made easy given that the volunteers and the beneficiaries usually live in the same towns and speak the same language: Haitian Creole.
By building up the capacities of the Haitian national Red Cross Society, by training community-based vol-unteers locally, by stepping up malaria prevention campaigns over at least the next three years, and through effective partnerships, we would like to use this opportunity to make Haiti a safer country from the threat of malaria and other health-related risks so that the tragedy that hit the Haitian population becomes an opportunity for future generations.
For more information on the IFRC Haiti global operations: www.ifrc.org/haiti
BeaTing Malaria: The waY forward1. Make sure sustainable funding is available to
carry the success forward. Recent history in the elimination of other diseases has revealed that funding gaps lead to reduced efficiency which can lead to resurgence of diseases. Ma-laria can be prevented and cured.
2. Strengthen the civil society response. Malaria will be defeated by empowering communities with the knowledge and materials needed to prevent and treat this disease. Empowered communities can ensure sustained access to prevention and treatment materials from their ministry of health and local government.
3. We call for greater recognition, support and investment of community-based solutions and action. We need to ensure continued support at community level to protect gains already made in the battle against malaria.
4. Invest more in operational research. Medical re-search is necessary but more research is also needed to allow for data driven, efficient, and cost-effective malaria programmes on the ground.
JeR
oe
n o
eR
leM
an
S

Health and social services department / The winning formula to beat malaria / April 2010 //
16
the winning formula to beat malariaFor more information on the IFRC malaria programme, please contact:
In Geneva Jason Peat Senior health officer, malaria E-mail: [email protected]
Media and public relations contactsJean-Luc Martinage Communications and advocacy officer, global healthTel.: 41 79 217 3386E-mail: [email protected]
In BrusselsAude GalliEU malaria policy and advocacy managerRed Cross and Red Crescent European Union OfficeE-mail: [email protected]
194
50
0 0
4/2
010
e 4
,00
0
The International Federation of Red Cross and Red Crescent Societies promotes the humanitarian activities of National Societies among vulnerable people.
By coordinating international disaster relief and encouraging development support it seeks to prevent and alleviate human suffering.
The International Federation, the National Societies and the International Committee of the Red Cross together constitute the International Red Cross and Red Crescent Movement.
Our world is in a mess. It’s time to make your move. ourworld-yourmove.org