Embed Size (px)
Citation preview

Health and Social Care Data Integration and Intelligence Project
Readiness Sessions

Making the Possible Happen
HSCDIIP – Readiness Sessions
• Welcome and Introductions
• Policy Context
• Background to HSCDIIP
• Information to Support Integration
• State of Readiness – What we’ve been doing
• Helping you get there – What you need to do
• Timelines and Future Phases
• Close

Policy Context

Integrating Health and Social Care in Scotland
Alison TaylorHead of Strategy and Delivery
Integration of Health and Social Care

Why integrate?
• People should be supported to live well at home or in the community for as much time as they can
• People should have a positive experience of health and social care when they need it

1) A guiding principle:
“. . . effective services must be designed with and for people and communities – not delivered ‘top down’ for administrative convenience”
The Christie Commission Report Commission on the future delivery of public services, June 2011
2) A single commissioner and budget for health and social care
3) Legislation:– The Public Bodies (Joint Working) (Scotland) Act 2014
Building blocks for integration

• Principles for integrated health and social care
• Nationally agreed outcomes for health and wellbeing
• Integrated governance arrangements for health and social care: delegation to a body corporate or lead agency
• Integrated budgets for health and social care
• Integrated oversight of delivery
• Strategic planning
• Localities
Public Bodies (Joint Working) (Scotland) Act (2014)

Integrated Resources: approximate scale
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
£b
n
Hospital Community Health FHS & Prescribing Social Work
Scotland Total=£12.3bn
Minimum to be delegated to Integration Authorities
=£7.7bn

Strategic planning andperformance reporting (slide 1)
Partnerships will need information to:•Map existing care pathways by geography, care group etc.
•Link outcomes to resources
•Measure effectiveness of new interventions
•Review and report on performance

Strategic planning andperformance reporting (slide 2)
Partnerships will need support for:•Analysis
•Modelling future pathways and financial impact of strategic needs assessment
•Financial planning

A&E Outpatients
InpatientsDay cases
Deaths
Prescribing
Age/gender
CHI
Linked File
SPARRA
Social Care
SIMDLinked Health and Social care file at
an individual service user level (Activity & Costs)
Partnership
Access
Via secure
platform
Data for integration

http://blogs.scotland.gov.uk/health-and-social-care-integration

Background to HSCDIIP

Information to Support Integration

A&E Outpatients
InpatientsDay cases
Deaths
Prescribing
Age/gender
CHI
Linked File
SPARRA
Social Care
SIMDLinked Health and Social care file at
an individual service user level (Activity & Costs)
Partnership
Access
Via secure
platform
Data for integration

• Resource Utilisation - mapped total spend (£)
• Health based activity information
• Disease specific groups (diabetes / dementia)
• Profiling service users– Delayed Discharges– High Resource Individuals
• Partnership Variation
• Basic Pathway Analysis
Information to Support Integration – What we Have Now

Information: What we have now
£11.7bn
£11.7bn

All Partnerships (All Ages) per weighted capita
Understand Variation in Spend

Dash Board 1 - Partnership Resource Mapping

Trends: Community prescribing costs, per weighted capita by GP practice,
2010/11 - 2012/13

Variation: H&SC weighted expenditure by GP practice
Dashboard 2 - Partnership & Practice Resource and Activity

Delayed Discharges
• Delayed Discharge Information available by;
• Partnership
• Number of delays
• Delay type (standard / code 9)
• Bed days occupied
• Resource consumption (£)
• All ages / 75+
• Rates (partnership & Scotland) per head population

• What do you think the average cost of a delay (per day)? £188 per day (standard)
• Example of Partnership X
• During 2013/14 cost of delay = £4.6m
• Bed days lost during year = 19,200
• Equivalent to 54 beds (2 wards?)
• How much do you think is lost to delays across Scotland? Approx £102m
All Delayed Discharges :2013/14
£205 per day (code 9s)Bed Days
• Standard: 421,157
• Code 9: 111,342

Dashboard 3 – Delayed Discharges
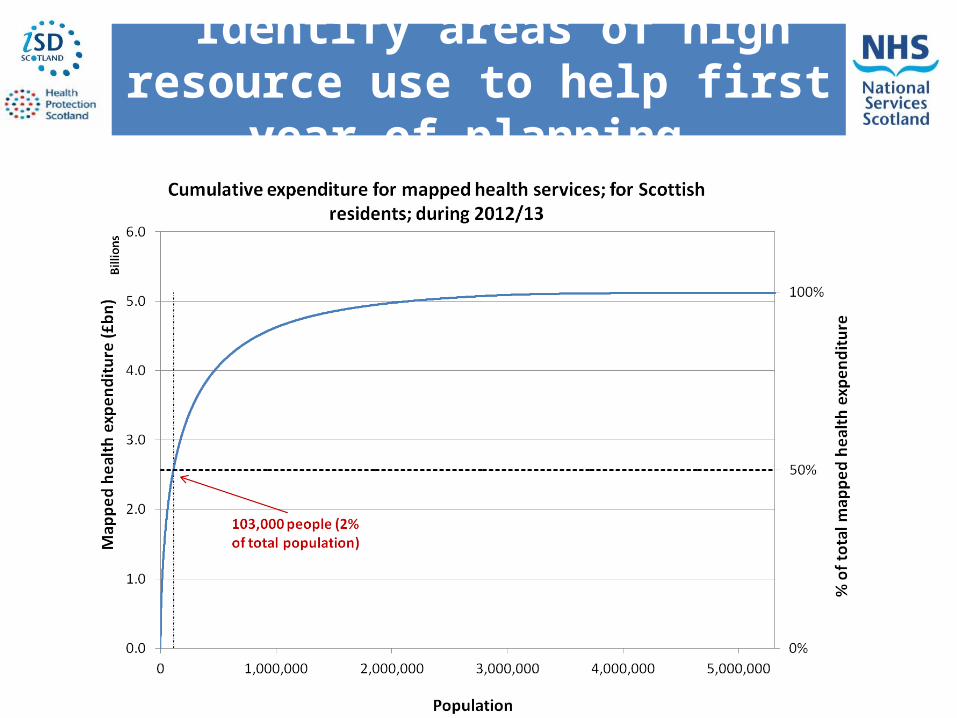
Identify areas of high resource use to help first year of planning

Identify areas of high resource use to help first year of planning
Hospital & GP prescribing resources 2012/13
102,628
£2.6bn
4,322,546
£2.6bn
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%

• Across Scotland 2% of the population utilise 50% of health resource
• Spend on HRIs £24,700/year vs average £1,200• Most extra cost is due to emergency hospital
admissionso Almost 4.5m
emergency bed days• HRIs account for around
half of all geriatric, psychiatric and GP beds
High Resource Individuals (HRIs)

Dashboard 4 – HRIs
Example Developments

Breakout Session
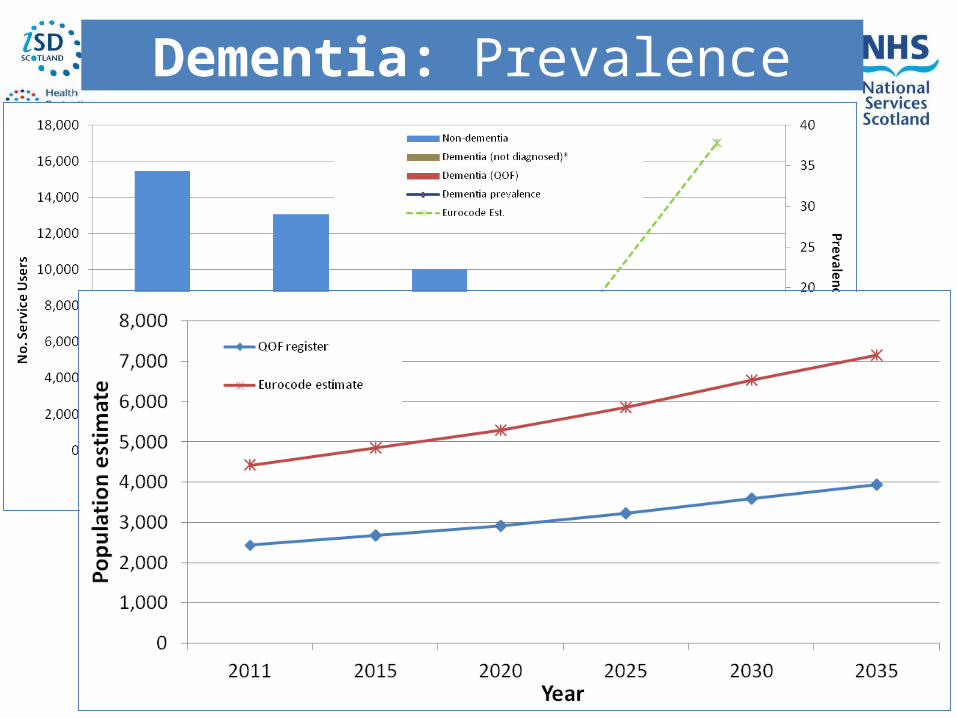
Dementia: Prevalence

Dementia: Costs

Dementia: Further analysis

Last six months of life: Hospital utilisation

• Future Analytical ‘Tools’
Impact analysis (evaluation)
Cost Benefit analysis
Predictive Analysis
Scenario Planning
• Pathway Analysis
Where we are heading

Predictive Analytics/Scenario Planning
Better model?
Naive model
J F M A M J J A S O N D
Em admission(gen med; 3 days;
£1,323)
Diagnosed CHD
Em admission(resp med; procedure; 4 days; £1721)
Em admission(gen med; 24 days; £8,042)
Delayed Discharge (Home)
A&E (£103)
Invest in ACPs?

Future Planned Developments
• Standard Reports via HSCDIIP Dashboard High level annual mapping (£) – 2010/11 to 2013/14 IP/DC detailed annual mapping – 2013/14 HRIs (Partnership level) – 2013/14 Delayed Discharges – 2012/13 to 2013/14
• Financial Information for Hospital Planning Existing acute financial/activity mapping by hospital Above, with addition of month up to Mar 2014 (activity for
Apr-Dec 2014)

Future Planned Developments
• Standard Reports via HSCDIIP Dashboard Development IP/DC detailed mapping (time trend) - 2010/11 to 2013/14 - HRI (Time Trend & Individual Level) Locality Level information GP Practice level Information Social Care Activity & Costs Community Health Activity & Costs Detailed Annual Mapping for:
o A&Eo Outpatiento Prescribing

Future Planned Developments
• Care Group Developments Multi-morbidity Last Six Months of Life Waste Indicators
• Other Planned Care Group Developments Falls Drug and Alcohol Cancer
• Pathway Analysis Delayed Discharges High Resource Individuals Visualisation
• *data dependant

Q&A

State of Readiness – What we’ve been doing
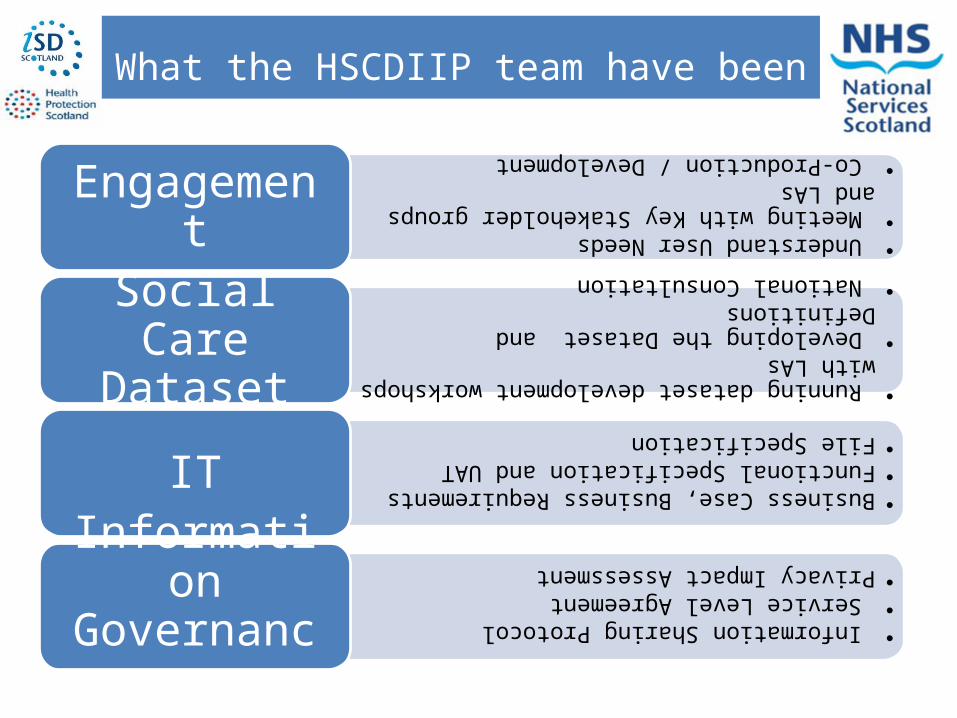
What the HSCDIIP team have been doing
• Understand User Needs
• Meeting with Key Stakeholder groups and LAs
• Co-Production / Development
Engagement
• Running dataset development workshops with LAs
• Developing the Dataset and Definitions
• National Consultation
Social Care Dataset
•Business Case, Business Requirements
•Functional Specification and UAT
•File Specification
IT
• Information Sharing Protocol
• Service Level Agreement
•Privacy Impact Assessment
Information Governance

Social Care Dataset and Data Submission

Dataset Submissions and File Spec
• Social care dataset and definitions ratified by Project Board in December 2014
• Dataset split into 10 sections; demographics must be returned with every submission
• Data to be submitted on a quarterly basis; except SDS
• Each file should be submitted as a separate .csv file (transferred through SFTP)
• Each file must contain client/service user Social Care ID
• Basic validation built into submission process
• Data walkthroughs

Secure File Transfer
Social Care Data submissions
Anticipated to be sent via Globalscape • Support for Set up and use• Authorised Users• Security Statement

Access Levels and Authorisation

Access to OutputsLevel Data Accessed Example
Scotland This allows the user to only see aggregated data for Scotland. The information is not broken down to Region, Partnership level, etc.
Partnership - Aggregate This allows the user to see aggregated data at Scotland level, labelled data for their own Partnership and the Region within which that Partnership is located. They will also see unlabelled data for all other Partnerships in Scotland.
Partnership – Detail This allows the user to see data at Scotland level, labelled data for their own Partnership and the Region within which that Partnership is located. They will also see labelled data for every General Practice in their Partnership area. Note: GP level is the geographic location which GP surgeries cover and is not GP data
Unnamed LA Unnamed LA Unnamed LA Unnamed LA
Scotland Av.
GP Prac1 GP Prac2 GP Prac3 GP Prac4 GP Prac5 GP Prac6
Partnership Av

• Users will apply for access using the User Access System
• Access can only be approved by your designated authoriser, and should mirror local practice.
• Following authorisation, ISD will provide the user with an individual user name and password to allow them to securely access Tableau at the agreed level
• Renewals are automatically sent out every 6 months.
Access

Information Governance

Underpins the whole health and social care integration project• SASPI template used• Data Sharing Agreement in place to support original
IRF type work• Data Processing Agreement in place for CHI seeding
(where required)• Alignment with the Scottish Government
Information Sharing Framework• Privacy Impact Assessment• Privacy Advisory committee (PAC)• CHI Advisory Group (CHIAG)
Information Governance

Information Governance
The Information Sharing Protocol (ISP) • Developed specifically for HSCDIIP• Allows Councils to send their data to NSS ISD for linkage
with existing health datasets• Supports the details and specific purposes for
sharing with NSS ISD• Includes the personal information being shared as well
as the required operational procedures and legal justification
• Will specify signatories from all parties• Highlights the proposed analytical outputs• Fit-For-Purpose• Will be reviewed in 15/16 to take account of new /
changing partnership requirements
Information Governance
Stakeholder Engagement Includes:• Caldicott Forum• CHIAG• Local Authority Legal Teams• Information Commissioner• Society of Local Authority
Solicitors and Administrators (SOLAR)
• LA and HB Chief Executives• Senior Solicitor, Central Legal
Office (NHS)• Information Sharing Board
(ISB) & Interoperability Working Group (IWG)
• Directors of Public Health• Data Protection and Freedom
of Information Officers Group • NHS IG Forum• Chief Officers• Partnerships, Health Boards
and Local Authorities• Local Information Security
Teams• Local Joint Information
Groups

Information Governance
Service Level Agreement• A Service Level Agreement (SLA) accompanies the ISP and
sets out the services NSS ISD will provide to Partnerships
The SLA also• Describes the available Access Levels• Captures the names of those agreed locally as those able
to authorise access within each partnership area (in accordance with local practice)
• Sets out the quarterly submission details and agreed dates to send data to NSS ISD

Information Governance
For consideration• Who is responsible for signing-off your ISP?
- Who should we be sending the document to i.e. Chief Exec, Chief Officer, Caldicott Guardian, all 3?
- Is there someone locally who would be responsible for co-ordinating partnership sign-off?
• What are your local processes for agreeing who should get access to what information as part of the SLA?- Do different staff need different access levels?- Who within your area would know which staff need access to which data?- Who / How will this be co-ordinated within your partnership?
• Who will your named contact be for ISD discussions on the ISP and SLA?
Information Governance
To discuss your requirements or for further information on the ISP or SLA, please contact
Margaret Parsons
Or telephone 0131 275 6528

Q & A

Helping you get there – What do you need to do

What happens after today?
What you need to do• Contact us to arrange dates for face-to-face walkthroughs with your
partnership• Identify those responsible for signing-off a) the ISP b) the SLA
SLA sign-off requires you to– Identify local authorisers who will approve which staff get access to
what information– Agree the sections of the Social Care dataset to be submitted to ISD
routinely– Identify who will be submitting data through the SFTP
• Once authorised individual staff need to apply for their Tableau logins & passwords

Helping you get there – What do you need to do
Other available support?
• Scottish Government funded initiative
• Piloted to date in 3 Local Authorities/Partnerships
• Complement existing teams
• Initial focus to provide analytical resource based within Partnerships
• Complements and supports the HSCDIIP project, helping to transform data into evidence for action
Local Intelligence Support Team (LIST)

Where we are at…
• All Chief Officers of H&SC Partnerships contacted offering support.
• Initial meetings taking place with Partnerships:Assess needs and prioritiesStrategic plans Information Framework
• Recruitment of staff
Local Intelligence Support Team (LIST)
Further information will be made available via ISD website www.isdscotland.org Or email: [email protected]

Future Phases
• Business as Usual
• Social Care data set evolution
• Addressing the Data Gaps
• Personal Outcomes
• Links to other areas (Third Sector)
• Digital Technology
• Evidence in to Action (WhatWorksScotland)
• Wider community planning
Future Phases

Close – Thank You!