Embed Size (px)
Citation preview

© 2001 by the American Society for Dermatologic Surgery, Inc. • Published by Blackwell Science, Inc.ISSN: 1076-0512/01/$15.00/0 • Dermatol Surg 2001;27:915–919
Healing of Venous Ulcers of Long Duration with a Bilayered Living Skin Substitute: Results from a General Surgery and Dermatology Department
Harold Brem, MD,* Jeroen Balledux, MD,* Troy Sukkarieh, BS,* Polly Carson,
‡
and Vincent Falanga, MD
‡
*Department of Surgery, Mount Sinai Medical Center, New York, New York, and
‡
Boston University School of
Medicine, Departments of Dermatology and Biochemistry, Boston, Massachusetts
background.
A laboratory-grown bilayered living skin substi-tute (LSS) has been shown to accelerate the healing of venousulcers. However, issues related to optimal wound bed prepara-tion prior to the application of LSS have not been addressed.
objective.
When combined with standard compression ther-apy and near elimination of wound exudate, bioengineered skincan achieve complete closure of venous ulcers which have beenpresent for more than a year and which are difficult to heal.
methods.
In the general surgery (center A) and dermatology(center B) departments at two separate medical centers, LSSwas used to treat venous ulcers of more than 1 year’s durationand which had been unresponsive to conventional therapy.
Wound bed preparation at both centers had as common goalsthe removal of necrotic tissue, optimal formation of granula-tion tissue, and elimination of wound exudate.
results.
There was great comparability between the twocenters in the patients being treated, wound size and duration,and number of LSS applications. Both centers achieved a fre-quency of complete wound closure of greater than 70% within6 months.
conclusion.
At two separate clinical and specialty sites hav-ing a common goal of optimal wound preparation, treatmentwith LSS was associated with a high rate of complete closure ofhard to heal venous ulcers.
MORE THAN 1 million individuals have venous legulcers in the United States, and the economic impactof caring for these wounds runs into billions of dol-lars. Compression bandages, either inelastic or elasticand multilayered, represent the standard of care for
the treatment of venous ulcers.
1
Although anecdotal
experience and retrospective studies suggest that venousulcers are easy to heal, the reality is different. An increas-ing body of evidence suggests that only about 50–60%of patients with venous ulcers will heal within 6 monthswith standard compression therapy alone.
2–4
There isa need for more effective treatments, especially for pa-tients with ulcers of long duration, which are notoriouslydifficult to heal.
A number of important advances are presently be-ing made in the development and testing of bioengi-
neered skin products. A bilayered living skin substitute(LSS; Graftskin, Organogenesis, Inc., Canton, MA) iscommercially available (as Apligraf) through NovartisPharmaceuticals (East Hanover, NJ) in the United States
and is approved for the treatment of venous and dia-betic ulcers. In a large prospective randomized studyof 293 patients (240 evaluable) with venous ulcers,LSS was shown to be more effective than compressionalone in both the frequency of complete wound clo-sure and in the time required to achieve healing.
2
LSSis most effective in venous ulcers of long duration thathave been difficult to heal. Thus for a group of 120patients who had venous ulcers for more than 1 year,LSS combined with compression therapy proved al-
most three times more effective by 24 weeks (46% ver-
sus 19%,
P
�
.002) than compression treatment alone.
5
The reasons why LSS should specifically prove more ef-fective for ulcers that are difficult to heal are unclear,but it’s possible that the stimulation of wound repairinduced by LSS occurs mainly in ulcers that have beenparticularly recalcitrant to conventional therapy.
As LSS is more widely used in the treatment ofvenous ulcers and other approved indications (diabeticulcers), it is becoming increasingly clear that optimalresults with this therapy require a great deal of atten-tion to proper wound bed preparation and other woundcare parameters. In this article we describe our experi-ence in a group of patients with venous ulcers presentfor more than 1 year. Our results indicate that LSS iscapable of achieving high rates of complete woundclosure in this difficult to heal population. The two ac-
This work was supported in part by National Institutes of Healthgrant AR46557 to VF, the Eastern Paralyzed Veterans Association, andthe Wound Biotechnology Foundation.Address correspondence and reprint requests to: Vincent Falanga, MD,Boston University, Department of Dermatology, 609 Albany Street,Boston, MA 02118, or e-mail: [email protected].

916
brem et al.: skin substitute heals venous ulcers
Dermatol Surg 27:11:November 2001
ademic centers in this article, a general surgery and a der-matology department, developed a protocol of woundbed preparation having as a common goal the removalof necrotic tissue, optimal formation of granulation tis-sue, and near elimination of wound exudate.
Patients and Methods
A total of 33 patients with 50 venous ulcers of more than 1year in duration were treated with LSS at two academicmedical centers, the Department of Surgery at Mount SinaiMedical Center (New York City, NY) and the Departmentof Dermatology at Roger Williams Medical Center (Provi-dence, RI). All of the patients had venous ulcers in the ab-sence of significant arterial insufficiency, as demonstratedby plethysmography, normal ankle to brachial index (ABI;
�
0.08), and clinical criteria of hyperpigmentation, lipoder-matosclerosis, and location on the leg. All of the patientshad ulcers which had been present for more than 1 year andhad been unresponsive to compression therapy alone.
All patients who had cellulitis associated with theirwounds were treated with systemic antibiotics. The protocolat the two centers focused on optimizing the granulation tis-sue and overall appearance of the wound bed and eliminat-ing or greatly reducing wound exudate. The method ofwound debridement was different at the two centers. CenterA (Mount Sinai Medical Center), a general surgery depart-ment, utilized surgical excision of the wound in the operat-ing room and topical therapies for a moist wound healingenvironment. At this center, the wound base was excised
and the wound edges extended to 2–3 mm beyond the origi-nal margins. LSS was applied to the ulcer within 1 week ofsurgical debridement in 100% of the patients. Center B(Roger Williams Medical Center), a Boston University pro-gram in dermatology heavily focused on wound healing,achieved wound bed optimization gradually in the outpa-tient setting. This was done by treating the wounds for 2–4
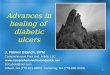
Figure 1. Preparation of bilayered LSS prior toapplication to the wound. A) LSS being liftedfrom its transwell. B) Fenestration of the LSSwith a scalpel as a method for allowing the es-cape of wound fluid. C) Meshing of the LSS asan alternative method for allowing wound fluidescape as well as a way to expand the con-struct. D) Meshed LSS. E) Application of meshedLSS to a venous ulcer. Copyright V. Falanga, 2000.
Table 1.
Clinical Characteristics and Outcome in Patients with Venous Ulcers Treated with a Bilayered Living Skin Substitute at Two Different Centers
Center A Center B
No. of patients 16 17Age of patients (years), mean
�
SD 67
�
13 65
�
21Number of ulcers 32 18Wound size (cm
2
)Mean
�
SD 39
�
68 25
�
42Median 12 9
Wound duration (years)Mean
�
SD 8.2
�
9.4 7.6
�
7.1Median 5 4.2
Number of applicationsMean
�
SD 2
�
1 1.7
�
0.5Median 2 2
Ulcers completely healed 25 (78%) 13 (72%)Time to heal (days)
Mean
�
SD 61
�
12 55
�
14Median 55 31
Center A is a general surgery department. Center B is a dermatology department.

Dermatol Surg 27:11:November 2001
brem et al.: skin substitute heals venous ulcers
917
weeks with a slow-release iodine preparation capable of re-ducing the bacterial burden and removing exudate (cadex-omer iodine). The cadexomer iodine was applied directly tothe wound as a primary dressing at every change of the com-pression bandage, which varied from two to three times aweek to once a week.
6,7
The secondary dressing consisted ofnonadherent gauze or foam dressing. Treatment with cadex-omer iodine was discontinued once the exudate was undercontrol.
8
At this time, provided that the wound bed alsoshowed optimal granulation tissue, patients were treatedwith LSS. Compression therapy was used in all patients im-mediately after LSS application. Elastic compression con-sisted of a four-layer bandaging system.
At both centers, LSS was applied after being fenestratedwith a scalpel or meshed at a ratio of 1.5:1 to allow for theescape of excessive wound fluid (Figure 1). LSS was immo-bilized over the wound with either 5-0 interrupted sutures(center A) or by a bolster and wound dressings alone (centerB). The primary wound dressing consisted of a petrolatum-impregnated gauze or a nylon dressing. At center B, whichdid not use sutures, this primary dressing was followed by
foam strips and an additional layer of the primary dressing.Patients were followed in the outpatient setting and follow-up at both centers occurred within the first week. At 1 weekafter application of the skin substitute, only the secondarydressings were generally removed, to allow for inspection ofsurrounding skin and to help ensure that there was no infec-tion. The primary dressing was generally left intact untilweek 2, at which time the wound was inspected. Extremecare was used in removing the primary dressing so as to notdisrupt the LSS. Follow-up thereafter was done weekly.
7
Results
This was a study of 33 patients with a total of 54venous ulcers. The demographic characteristics of pa-tients treated at centers A and B were quite compara-ble, as were wound size, wound duration, and numberof LSS applications required (Table 1). However, somedifferences in the patient cohorts were present betweenthe two centers. Patients at center A were more likely
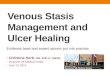
Figure 2. Application of bilayered LSS to a venous ulcer after surgical debridement. A) Venous ulcer debrided down to fascia. LSS was ap-plied immediately after debridement (not shown). B) Healing of the venous ulcer from the inferior edge by 6 weeks, shown here right af-ter repeated surgical debridement. C) Application of meshed LSS to the venous ulcer 7 days after the second surgical debridement shownin (C). D) Complete wound closure of the venous ulcer after 20 weeks. Copyright V. Falanga, 2001.

918
brem et al.: skin substitute heals venous ulcers
Dermatol Surg 27:11:November 2001
to have multiple ulcers. In general, wound size and du-ration were greater at center A, but this difference wasnot statistically significant (
P
�
.05). The frequency ofcomplete wound closure was comparable between thetwo centers, with a combined mean of 74%. This levelof efficacy in these ulcers of long duration was achievedwith a median of two applications of LSS. The meantime to heal was 61
�
12 and 55
�
14 days for centerA and B, respectively. However, this difference was notstatistically significant (
P
�
.05). Figures 2 and 3 arerepresentative examples of venous ulcers treated atcenter A and B, respectively. These examples illustratesome of the differences in the preparation of thewound bed and LSS application. Thus Figure 2 showsextensive surgical debridement, down to fascia, in apatient from center A with a venous ulcer that hadbeen unresponsive to treatment for many years. Asshown in Figure 2, extensive surgical debridement was
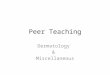
indeed followed by evidence of healing from the ulcer’sinferior margin, while the rest of the ulcer remainedunchanged. Repeated surgical debridement and treat-ment with LSS after 7 days accelerated the process ofhealing. On the other hand, Figure 3 illustrates the useof a slow-release iodine preparation (cadexomer io-dine) to reduce exudate and prepare the wound bed.The ulcer in Figure 3 had been unresponsive to treat-ment and was heavily colonized. The slow-release io-dine preparation was able to optimize the wound bed,thus allowing better outcome with the use of LSS.
Discussion
This report is from two medical centers and two de-partments, general surgery and dermatology, with acommon interest in chronic wounds and the use ofbioengineered skin. We describe our experience over a
Figure 3. Wound bed preparation and application of bilayered LSS to a venous ulcer. A) Venous ulcer with heavy bacterial colonization andcopious amounts of exudate. B) Ulcer being treated with cadexomer iodine, which is being removed with a cotton applicator. C) Appear-ance of ulcer during treatment with cadexomer iodine, showing improvement in the wound bed after 2 weeks. D) Optimal wound bedpreparation achieved in the outpatient setting after 5 weeks of treatment with cadexomer iodine. E) Ulcer treated with LSS. F) Appearanceof the ulcer 2 weeks after LSS application. G) Close-up of the ulcer’s margin, showing activation of the edge at week 1. H) Almost completewound closure at week 4. I) Complete wound closure at week 6. Copyright V. Falanga, 2001.

Dermatol Surg 27:11:November 2001
brem et al.: skin substitute heals venous ulcers
919
12-month period with the use of a bilayered LSS in thetreatment of venous ulcers present for more than 1year and unresponsive to conventional compressiontherapy. Both centers had as a common goal optimiza-tion of the wound bed and elimination of wound exu-date prior to the use of LSS.
8
Center A, a general sur-gery department, utilized surgical debridement in theoperating room as well as topical antiseptic prepara-tion. Center B, a dermatology department, used dress-ings and a slow-release antiseptic preparation. In spiteof these differences in the approach to wound bedpreparation, the results were similar at both centers.We show that optimization of the wound bed and theuse of LSS can lead to complete closure of hard to heal,long-standing venous ulcers in 70% of the time. Actu-ally this level of success with the use of LSS is superiorto the frequency of complete wound closure (57%) re-ported in the pivotal trial of LSS for venous ulcers, sug-gesting that we can greatly improve the results obtainedwith LSS by paying closer attention to preparing thewound prior to the application of the skin substitute.
5
The availability of advanced technological products,such as growth factors and bioengineered skin, is lead-ing us to consider and evaluate conventional woundcare more critically. Specifically, optimal wound bedpreparation is becoming an essential component of ul-cer care so as to maximize the effectiveness of ad-vanced products. It should be emphasized that woundbed preparation implies a global approach to the pa-tient and not to wound-specific characteristics alone.
8
For example, wound bed preparation would includeattention to treatment of congestive heart failure (caus-ing edema and circulatory failure).
While the appearance of the wound bed has gener-ally received the greatest attention in the past (ie, re-moving necrotic tissue, improving granulation tissue),the deleterious effect on healing of excessive woundexudate has not been properly emphasized. In this ar-ticle we highlight the importance of both wound bedappearance and removal of wound exudate in order toachieve optimal results with the use of bioengineeredskin. It has been shown that the exudate from venous
ulcers and other chronic wounds decreases both themigratory and proliferative potential of fibroblastsand keratinocytes. Wound fluid also contains a num-ber of proteases which can degrade extracellular ma-trix proteins and growth factors. Therefore we believethat much of our success in the treatment of venousulcers with LSS is due to elimination of wound exu-date.
8
Surgical debridement, as performed mostly atcenter A, removes the necrotic and inflammatory com-ponent of ulcers and decreases the bacterial burden.These steps, in turn, can lead to a decrease in thewound exudate. Similarly, prolonged outpatient treat-ment that emphasizes appropriate compression, removalof edema, decreased bacterial burden, and wound ex-udate with cadexomer iodine can greatly improve theeffectiveness of bioengineered skin.
In summary, this study of long-standing venous ul-cers suggests that the use of advanced therapeuticproducts, such as bioengineered skin, can lead to muchbetter results when proper attention is paid to woundbed preparation. As shown here, the means to achievean optimal wound bed with little exudation can varydepending on the clinical setting and specialty, but theclinical outcome appears to be comparable.
References
1. Sibbald RG. An approach to leg and foot ulcers: a brief overview.Ostomy Wound Manag 1998;44:28–32.
2. Falanga V, Margolis D, Alvarez O, et al. Healing of venous ulcersand lack of clinical rejection with an allogeneic cultured human skinequivalent. Arch Dermatol 1998;134:293–300.
3. Phillips TJ, Machado F, Trout R, et al. Prognostic indicators invenous ulcers. J Am Acad Dermatol 2000;43:627–30.
4. Phillips TJ. Successful methods of treating leg ulcers: the tried andtrue, plus the novel and new. Postgrad Med 1999;105:159–79.
5. Falanga V, Sabolinski M. A bilayered living skin construct (Apligraf)accelerates complete closure of hard-to-heal venous ulcers. WoundRep Reg 1999;7:201–7.
6. Holloway GA, Johansen KH, Barnes RW, Pierce GE. Multicentertrail of cadexomer iodine to treat venous stasis ulcers. West J Med1989;151:35–8.
7. Falanga V. How to use Apligraf to treat venous ulcers. Skin Aging1999;7:30–36.
8. Falanga V. Classifications for wound preparation and stimulation ofchronic wounds. Wound Rep Reg 2000;8:347–52.