Embed Size (px)
Citation preview

CLINICAL GASTROENTEROLOGY
Healing of benign gastric and prepyloric ulcers: A prospective,
endoscopy--controlled, randolllized, double--blind, Canadian lllulticentre
study of omeprazole 20 and 40 mg daily and ranitidine 150 mg twice a day
PIERRE PARE, MD, ROBERT] BAILEY, MD, A NDRE P A RCIIAMBAULT, MD, H ENRI N A VERT, MD, C N OEL WILLIAMS, MD, ABR Tt IOMSON, MD, D EN IS L EVESQUE, MD, ALAIN FARLEY, MD
ABSTRACT: A double-blind, randomizeJ study was conducted in 118 patients with benign gastric or prepyloric ulcers to compare the efficacy of omeprazole 20 or40 mg da ily with raniticline 150 mg twice daily. The healing rates at four weeks were 67, 79 and 54% and at eight weeks increased to 90, 97 and 71 % for the omeprazole 20 and 40 mg groups and the ranitidine group, respectively (P<0.03 for the differences between each of the omeprazole groups anJ the ranitidine group at eight weeks). Multivariate analysis showed influence on healing rate for ulcer size but not for smoking status, sex or ulcer site. Symptomatic relief was excellent and similar in the three groups. Ulcer recurrence during the six month follow-up off treatment after initia l ulce r healing did not differ between the three groups. No serious adverse events could be attributed to the drugs. The authors conclude that treatment with omeprazole 20 or 40 mg daily for a period of four to eight weeks is safe and significantly more effective in ulcer healing than a ,tandard dose of ranitidine. Can J Gastroenterol 1990;4(1):7-12 (pour resume, t'Oirpage 8)
Key Words: Gastric ulcer, Omeprazole , Prepy/.oric ulcer, Ranitidine
Division of Gam oenr.emlogy, Hotel-Dieu de Quebec Hospiwl. Laval University, Quebec City, Quebec; lmernal Medicine, Royal Alexandra Ho~p,ral , Edmonton , Alberta; Centre de Ga.srro-encerologie et d' Endosco/1ie de Monrreal and Maisonneuve-Rosemum Hospiwl , Montreal , Quebec; Centre de Recl1erche en Physiu/>atholugie Digestive , University of Sherbruoke, Shabrooke, Quebec; Division of Gamoemerolo/!.)', Dalhousie Urnvmiry, Halifax, Nova Scoua, Oi11ision of Gastrocnterology, University of A lberti.I , Edmonton , Alberw
Correspondence and reprints: Dr Pierre Pare, Departmem of Medicine. I lotel-Dieu de Qw!bec Hospital, 11, Cote du Palais, Quehec City, Quebec G JR 2)6
Received for publication June 21 , 1989. Accepted November 13. 1989
CAN j 0 ASTROENTl:ROL VOL 4 No l j ANUARY/FE!>RUARY 1990
OMEPRAZOLE. A SUBSTITUTED
benzimiJ::izo le , is a gastric proton pump inhihitor producing potent inhibition of gasrric ac id secret ion ( 1,2). !rs efficacy in healing duoJenal ulcers has been shown in comparison to
c imetidine (3.4) anJ ranitiJine (5) . In patients with gastric ulcers, irs efficacy has also been evaluated with Joses of 20 and 30 mg (6,7). The efficacy of a drug regimen producing marked ac id suppression, as can be achieveJ with omcprazole 40 mg daily, was the objec t of this investigation.
Th b study compares two J oscs of omeprazole , 20 anJ 40 mg daily, produc ing Jiffcrent Jegrees of suppression of intragastric ac idity, with a srnndarJ dose of ranit iJine in the t reatmentofbenign gastric ulce r. The report deals with 118 patients enrolleJ by six Canadian centres accorJing to the protocol used in an internat ional multicentre randomized study, and is the only North American contribution to
7

PARE et al
La guerison des ulceres gastriques et prepyloriques benins: Une etude canadienne multicentrique prospective, randomisee, a double insu et controlee par l'endoscopie comparant l'omeprazole 20 et 40 mg par jour et la ranitidine 150 mg deux fois par jour
RESUME: Une etude randomisee a double msu a ete cffectucc :sur 11 8 patients atteims <l'ulccres gascriques ou prcpyloriques bcnins afin <le comparer l'efficacite de l'omeprazolc a 20 ou 40 mg par jour ct cellc de la ranitidinc administree a 150 mg deux fois par jour. Les taux de guerison a quacre semaines ccaient de 67, 79 ct 54% ct, a huit semaines, ils ont atteint 90, 97 et 71 % pour lcs groupcs traites par l'omcprazole (20 et 40 mg) ct la ranitidine, respcctivcment (P<0,03 pour les differences entrc chacun des groupcs trait cs par l'omeprazole et le groupe rccevant de la ranitidinc a huit semaincs). Unc analyse multifactorielle a revele une influence sur les taux de guerison en ce qui concerne le diamctre de l'ulcere, mais non pas pour le tabagisme, le sexe du patient ou le site de l'ulccre. Le soulagemcnt symptomaciquc fut excellent ct similai re clans Les trob groupcs. L'obscrvacion pendant six mo is apres la fin <lu traitement a dcmontre quc la rcc1dive ulccreusc n'etait pas difference entre Jes trois groupes. Aucun dfet secon<laire serieux n'a etc o bserve pendant l'ctudc. Les aULcurs conclucnt que le traitcment par l'omeprazole a 40 ou 20 mg par iour pendant unc pcrio<le de quatrc a huit semamcs est securicaire et significativement plus efficacc pour guerir l'ulcerc gasmque, qu'une J ose standard <le ranitidine.
the study. Earlier reports have implicated a difference in the healmg rates between North America r1n<l Europe (2,4 ).
PATIENTS AND METHODS Patients included 111 the study had
one or more active ulcers m the stomach with a greater ax is of at least 5 mm, verified by endoscopy within four days of bcgi1ming treatment with the study drug. Prepyloric. ulcers were included and classified as such to a llow separate analysis, but not stratified into the various treatment groups. Ulcers localized within 3 cm of the pyloric ring were defined prepyloric, an<l those localized mo re than 3 cm from the pylorus were considered gastric.
Patients were excluded from participation in the study for the following reasons: age below 18 or above 80 years; pregnant or breascfee<lmg; treatment with therapeutic doses of anti-ulcer drugs for more than three days during the 14 Jays preceding endoscopy; presence of erosive reflux esophagitis, pyloric stenosis, concurrent duodenal ulcer or bleeding ulcers; history of gastric surgery except for simple ulcer closure; other significant concurrent disease; and chronic alcoholism. Patients on treatment with non-
steroidal anti-inflammatory drugs (NSAIDs) were mcluded but advised not to change dose; these patients were classified but not stratified into the vario us treatment groups.
The study was conducted in accordance with the Declaration of Hclsmki and was approved by each inst itution's research and cthtCs review comnrntee. Written informed consent was obtained from all patient:,.
Six centres participated 111 the :study. The patients were randomly assigned to double-blind treatment with omeprazole 20 or 40 mg m the morning, or rani tidine 150 mg bid. A ll patients received the medicauon for four weeb. Paucnts whose ulcers had not healed after four weeks received a furrhcr four week treatment course. Ulcer healmg was assessed by endoscopy at four an<l, if necessary, eight weeks m patients with gastric ulcers and ar two and, if necessary, four and e ight weeks in patients with prepylonc ulcers. Complete rc-epithelialization of the ulcer site or sites was used as the criterion of ulcer healing. Gastric biopsies were taken from the ulcer area in order to
exclude malignancy. Refore treatment, the ulcer and
genera l medical histnnes were recorded for each patient, along with a history of
drug, tobacco and alcohol use. During t reatment, pmients were assessed after two an<l four weeks and if necessary after e ight weeks with an ulcer symptom severity rating, physical ex· amination, r1Jvcrse event evaluation, drug al.countabil ity, and lahoratori tests (hemoglobin, wh ite hloo<l cell count, plr1cclets, serum creatininc, electrolytes, bilirubin, a lkalme pho~ pharase, a lanme transaminase, aspar, tare transaminase, an<l urine protein and sugar).
After completion of the ulcer he~ling study phase, healed patients were fo llowed for a pencxl of six month,. Patients were reviewed at three r1nd six months and an endoscopy performed at s ix months o r earlier if ulcer symptoms recurred.
The healing data were analyzed with standard x2 tests and confidence inter vab for the heal mg probabilities. In ,iJ. d ition, r1 multivariate analysis of treatment regimen, ulcer size and site, smoking status, sex and NSAID use, was conducted to adjust for possible 11n balances in one or more of these factor, in the comparison between treatments. Unknown healing status was classificJ as 'not healed'. Safety analysis mcluJcJ data from a ll patients who received study drugs. The laboratory tests were performed in each individual centre, and thus varying units an<l reference ranges were used for vmiables.
RESULTS A total of 118 patients entered the
study. Table 1 shows the pre-entl) characteristics of the patients in the Lhrce groups. None of the differences observed between the treatment group, were statistically significant. Five patients were withdrawn <luring the study (Table 2).
The cumulative proportions of patients healed at four and eight weeks are shown in Tahle 3. The omeprazolc 20 mg regimen achieved significantly higher healing rates than ranitidine 150 mg hid afte r eight weeks of treatment ( P=0.03). With omeprazole 40 mg daily, the healing rates at four anJ eight weeks were significantly higher than the rates observed with raniti<linc (P=0.02 and P=0.001 ). Ana lysis of pm-
8 C-\N j GA::..'TROENTEROL VOL 4 No I JANUARY/FEBRUARY 1990

Healing of benign gastric and prepyloric ulcers
TABLE 1 Characteristics of patients
Omeprazole Omeprazole Ranitidine 20mJL 40m 150mg bid
Total number of patients 39 38 41 Age (years. mean±SD) 52.5±13.0 56.2±12.5 55±14.5 Male/female ratio 18/21 14/24 19/22 Smoker/nonsmoker ratio 21/18 19/19 24/17 Alcohol/no a lcohol ratio 20/19 12/26 15/26 Number taking NSAIDs 9 8 4 Duration of ulcer disease 8.7± 13.0 6.7±8.4 5.6±7.7 (years. mean±SD) Duration of c urrent episode 93.1±110.5 94.5±125.0 194.7±490.8 (days. mean±SD)
Patients with previous 3 5 2 ulcer complication
Number with gastric ulcer 28 24 28 Number with prepyloric ulcer 11 14 13 Ulcer size (mm. mean±SD) 11.7±6.0 10.7±5.0 12.5±8.9
TABLE 2 Patients withdrawn during study
Treatment rou Reason for withdrawal (time) Healing status
Unknown Unknown Healed
Omeprozole 40 mg
Ronitidine Ronitidine
Ronitidine
Ronitidine
TABLE 3
Worsening of symptoms (8 days)
Adverse events (9 days)
Adverse events ( 14 days)
Concurrent disease (16 days) Increase In ulcer size (29 days)
Not healed
Not healed
Cumulative healing rates (number and percentage of patients)
Treatment Four weeks 95%CI Eight weeks 95%CI
020 26/39(67%) 50to 81% 35/39(90%) 76 to 97%
O<IO 30/38(79%) 63 to90% 37 /38 (97%) 86to 100% R 22/41 (54%) 37 to69% 29/41 (7 1%) 54 to 84%
M0:1o-R) -8to 34% 2 to 36%
L\(040-R) 5to45% 11 to41%
L\(0,io-020) -8to 32% - 4 to 18%
Cl Confidence infeNol; 02() Omeprozole 20 mg doily; 040 Omeprozo/e 40 mg doily: R Ronitidine 150
mg twlee doily; A Difference
sible prognostic factors showed that ulcer site, smoking status and sex did not influence healing; ulcer s ize was the only prognostic factor of statistical significance (P=0.018). However, the logit analysis, taking into consideration the imbalance of more patients with large ulcers in the ranitidine group, did not change the statistical results (at eight weeks, omeprazole 20 mg group versus ranitid ine group, P=0.03 and
omeprazole 40 mg group versus ranitidine group, P=0.0 1). Differences in healing rates between the omeprazole 20 mg group and the omeprazole 40 mg group were not statistically significant.
In the small subgroup of patients taking NSAIDs, there was a significantly higher h ealing rate in omeprazole- versus ranitidine-treated patients; after eight weeks of treatment,
CAN J GASTROENTEROL VOL 4 N O I JANUARY/FEBRUARY 1990
six of nine, e ight of eight, and one of four patients were healed in the omeprazole 20 mg, omeprazole 40 mg and ranitidine groups, respectively (P=0.02). Healing rate~ afteTl wo weeb in prepyloric ulcer patients were six of l l, four of 14 and four of 13 in the omeprazole 20 mg, omeprazole 40 mg and rani tid ine groups, respectively ( not significant) .
A t pre-entry, a ll patients reported symptoms. After two weeb, the proportion of patients free from symptoms or mildl y symptom.:itic was 86% in the omeprazole 20 mg group, 83% in the omcprazole 40 mg group and 86% in the ranitidine group; after four weeks, the corresponding figures were 97, 9 1 and 94%, respectively.
Complaints during the study were reported by l O patients in the omeprazole 20 mg group, three patients in the omeprazole 40 mg group and 14 patients in the ranitidine group (Table 4) . None of the compla ints was cl inica lly important. However, the adverse events caused the withdrawal of two patients in the rani tidine grour (headache, sleepiness and unsteady gait in one patient who. e s ide effects disappeared completely on open treatment with the same drug; nausea and d izzi, ness which disappeared one Jay after stopping the trial medication in the ocher patient). In addition, one pmient in the ranitidinc group was wi thdrawn when a concurrent disease (pancreatic carc inoma) was clinica ll y diagnosed. During the study, there was no significant change in the mean values for the laboratory tests.
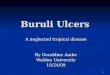
The cumulative proportions of the initially enrolled patients who were still in remission verified hy endoscopy, after the follow-up of six months, were 62% in the t)meprazole 20 mg group, 62% in the omeprazole 40 mg group and 4 7% in the ranitidine group (Figure l ); no statistically significant difference was observed between the three groups.
DISCUSSION Healing of benign gastric ulcers is a
slow process; indeed, on placebo, reported h ealing rates are in the range of 25 to 54% after observation for six to eight weeks (8- l 2). For the same period
9

PARE el al
TABLE 4 Complaints during the study (number of patients)
Complaint
Nausea . vomiting
Diarrhea Dizziness Headac he Tiredness Blurred vision Unsteady ga it Metallic taste Skin rash
0 20 3
2 3 1 2 0 0 0
0 40 0
1 0 0 1
0 0 0
R
2
3 1
2 0
1
2 0
Olo Omeprozole 20 mg doily.· O"° Omeprozole 40 mg doily: R Ron/tid1ne 150 mg twice doily
of treatment, clinica l trials using drugs acting to contro l gast ric acid report healing rates in the range of 67 LO 70% with antacids (8, I I ), 65 to 89'}-o with c ime tidine (6,8,9, 13, 14) 78 to 94%
P atie n ts in rem issio n ( %)
100
wiLh rani t id ine (13- 16) a nd 65 to 80% with famotidinc ( 12). However, comparisons of these results may noL be appropriaLc mce the ini t ia l ulcer size, a maior factor in determining the healing time course ( 17), was not taken into cons1derat ion . Furth ermore, t he st rong relation ship shown bcl\veen degree of acid suppression and healing rate in duodenal ulce rs ( l 8) b no t o bserved in clinical t ria ls of acid- inh ibiting d rugs in the treaunent of gastric ulcer ( 19).
T his study shows that treatment with omeprazole at a J ose of 40 mg tin ily, a very powerful ac1<l-suppressmg regimen , is more effec ti ve than a standard Jose of ran 1tidme in healing gaMric ulcers. O meprazole 20 mg da 1ly was nlso more effective than rani t i<line 150 mg t wice a J ay afte r e ight weeks of trentmenr. In comparison to c imeti<linc l g
da ily, omeprazole 30 mg da ily was shown to he more effective in healing ulcers located in the a nLrum of the stomach (6), while ran it idme 150 mg bid a nd omcprazole 20 mg daily in a previous study resulted m similar healmg rates (7) . The present results arc nor due to differences between the treatment groups in J e mographic J am, smoking status, ulcer locations or sex. In studying the tota l populmion of subjects e nrolled in the three groups, ulcer :,ize wa:. a progn osLic factor in the healing rate. However, the slightly smaller ulcer :.1ze in th e omeprazole grour1 could no t explain the differe nces in results since the log1t stallst1cal analysis that rhe authors used took into considerat ion rhc imba lance m ulcer size at t he hcgmnmg nf the study. It is
genera II y assumed that prcpylon c ul
···········-······----...
0
/
/
/
/ /
/ 60
40
20
2/ 0 Ul c e r hea l i n g atudy
- - I
I - - - I
'-···········: L ••••••••••• ,
··········-··········-.
'···········.
- ----- - -- --- ,
2
I
L-- - -- 1
3
'- - - I
I._ - - - - - - - -.
Omep r azole 20 mg
Omep r ezole 40 mg
_ ___ Ran lti d ln e
4 5 6
Follo w- up atu dy
Month s
Figure I ) Percent.ages of patien~ in renussion during six months following ulcer healing wiih omeprazole 20 mg daily, omcprazolc 40 mg daily and ranmdine I 50 mg twice daily
10 CAN J GM,TROENTEROL VOL 4 No I JANUARY/FEBRUARY 1990

Healing of benign gastric and prepyloric ulcers
cers behave physiologically similarly to
duodenal ulcers (20), for which omeprazole has been shown to be superiorto 150 mg ranicidine twice daily in its healing capacity (5). Although ,tudies of gastric acid secretion were not performed, the relative numbers of prepyloric over gascric ulce rs d id not differ between the three groups, and in each treatment group, about two-thirds of ulcers were gastric ulcers.
Even if Lhe pmhogenesis of gastric ulcers appears Lo be related more to
abnormalities in mucosa l defence mechanisms than to aggressive factors (21 ,22), this study nonetheless suggests that control of gastric ac id is likely to he very important in the he,1 ling of gastric ulcers. Adding placebo data to the analysis of the effect of H z receptor antagonists in the treatment of gastric ulcers, Howden ct al ( 19) found correlations between acid suppression antl ulcer hea ling stronger with suppression of total 24 h versus nocturnal acidi ty, contrasting with duodenal ulcers for which suppression of nocturnal acidity 1s the most relev<1nt c1cting factor with Hz receptor antagonists ( 18). In asymptomatic duodenal ulcer subjec ts,
ACKNOWLEDGEMENTS: The 11uthors ~re grateful to Mr Jan-Ake Westin , Senior Clinical Research Director, Astra C11naJa, for his support, anJ to Mrs R Simard for typing the manuscript. This study was supported and coorJinaLcd by AB Hiisslc, .i suhsidiary of Astra Canada.
REFERENCES [. Lind T, Cederberg C, Ekcnvcd G,
Haglund U, Olbc L. Effect of omeprazolc - a gastric proton pump inhibitor - on pcnragastric stimulateJ acid secretion in man. Gut 1983;24:270-6.
2. Clissold SP, Campoli-Richards OM. Omeprazolc. A preliminary review of its pharmacodynamic anJ pharmacokinetic properties, anJ therapeutic potential in peptic ulcer disease anJ Zollinger-Ellison syndrome. Drugs !986;32:15-47.
3. Lauritsen K, Rune SL, Bytzcr P, ct al. Effect of omcprazolc and cimct id inc on duodenal ulcer. N Engl J McJ 1985; 312:958-6 1.
4. Archambault AP, Part1 P, Bailey RJ ,
omeprazole 20 mg daily has been shown to result in a 90% suppression of mean 24 h intragastric acid ity (23), while ran itidine 150 mg twice daily reduced 24 h intragastric acidity by 63 to 69% (24-25 ). Repeated doses of omeprazole 40 mg daily have been reported to decrease 24 h median hydrogen ion activity by almost 100% in healthy volunteers (26) and 97% in tluodenal ulce r patients in symptomatic remission (23 ). The present clinical results in healing rates follow these gradual effects on 24 h intragastric acitli ty inc reasing from ranitidine 150 mg twice a day to omeprazole 20 mg daily and omeprazole 40 mg dai ly.
Even if acid is a permissive factor in the development of ulcers (and the amount need no t be excessive), perhaps almost complete suppression of acid over 24 h leaves the gastric mucosa under the predominant activity of the defensive mechanisms and turns off pathogenetic factors dependent on the presence of a minimum hydrogen ion concentrat ion such as tissue protein degradation. Total absence of acid might allow the action of natural healing mechanisms a t a faster pace than in
ct al. Omcprazolc (20 mg Jatly) versus cimctiJinc ( 1200 mg Jaily) in duodenal ulcer healing anJ pain relief. Gastrocntcrology 1988;94: 11 30-4.
5. Bardhan KO, Bianchi Porro G, Bose K, et al. A comparison of two different doses of omeprazole versus ranitiJinc in treatment of duodenal ulcers. J C lin Gastrocnrcrol l 986;8:408- L 3.
6. L'luritsen K, Rune SJ, Wulff HR, cc al. Effect of omeprazolc ,rnd cimctiJinc on prepyloric gastric ulcer: Double blind comparative tri11l. Gut I 988;29:249-5 3.
7. C lassen M, Dammann HG, Domschkc W, ct al. Omcprazole heals ducxlcnal, but not gastric ulcers more rapid ly than ranitiJine: Results of two German multicentrc trials. Hcpacogastrocntcmlogy l 985;32:243-5.
8. Isenberg JI. Peterson WL, Eh1shoff JD, ct al. Healing of benign gastric ulcer with low-dose antaciJ or cimetiJine. A Jouble-blind, randomized, placebocontrolled trial. N Engl J Med 1981;308: J 319-24.
9. Graham DY, AkJamar K, Dyck WP, et al. Healing of benign gastric ulcer: Comparison of cimctidinc .ind placebo in the Uni ted States. Ann lmem Med
CAN J GASTI~OENTEROL VOL 4 No I JANUARY/FEBRUARY l 990
circumstances of moderate acid inh ibition. Higher rates of ulcer healing achieved with omeprazole 20 antl 40 mg Jaily versus ranitidinc 150 mg twice daily a re consistent with the hypothesis that the degree of suppression of intragastric acitl is very important in the healing phase of gastric ulcers; there are furthermore no data suggesting that omeprazole has inherent cytoprotcctivc activity. However, pronounced inhibition of acid may abo promote liberation of gastrin and favour its trophic effect on the gastric mucosa.
The authors conclude that omeprazole 20 mg daily and omeprazole 40 mg tlaily resulted in a significantly more rapid healing rate than ranititline 150 mg twice daily in benign prepyloric and gastric ulcers. These results a rc similar to the data from the international study (27) and tlo not indicate a difference between North America and Europe in the reporting of healing rates. For a period of four co eight weeks, treatment with omeprazole was shown to be safe. Ulcer recurrence during the six month follow-up period was not different with e ither treatmenc usctl to heal the acute ulcer.
1985; [02:571-6. LO. Lam SK, Lau WY, Lai CL, ct al.
Efficacy of sucralfatc in corpus, prcpyloric, and Juodenal ulccr,1,snciatcd gasrric ulcers. A douhleblind , placcbo-contrnllcd study. Am J Med 1985;79:24-31.
11. Rydnmg A, Wchcrg R, Lange 0 , Bersrnd A. Healing of benign gastric ulcer with low-Jm,e antac1Js anJ fiber d icr. Gascroentcmlogy 1986;9 I : 56-61.
12. Si mon B, Mu ller P, Dammann HG. Famotidinc oncc-:1,dny in the therapy of acute, benign gastric ulcer: A worldwide experience. J Cl111 Gastrocntcrol 1987;9: 19-22.
I 3. Baron JH, Perrin VL, ct al. Gastric ulcer hc,1ling with ranitidine and cimctidinc. A multiccntre study. Scand J Gastrocntcrol 1983; 18:97 3-6.
14. The Belgian Peptic Ulcer Study Group. Single blinJ comparative stuJy of ranitidinc and cimctidinc in patients with gastric ulcer. Gut 1984;25:999-1002.
15. Lcrnux P, Farley A, Archambault A, ct al. Effect of ranitidint: tm healing of peptic ulcer: A 2-month study. Am J Ga,trocntcrol 1983;78:227-30.
11

PAR~er al
Summers K, WooJ JR. A smgle night time dose of raniridine in che acute treatment of gastric ulcer: A European multicentrc trial. Gut 1986;27:784-8.
17. Scheurer U, Witzel L, Halter F, Keller H-M, Huber R, Galcam R. Gastric and duodenal ulcer healing under placebo treatment. Gasrroenterology l 977;72:838-41.
18. Jones DB, Howden CW, Burget DW, Kerr GD, Hunt RI I. Acid suppression in dmxlenal ulcer: A mcrn-analys1s co define optimum dosmg with an tisecretory drugs. Gue 1987;28: 1 I 20-7.
19. Howden CW, Jones rm. Peace KE, Burget DW, I lunt RH. The trearment of gastric ulcer with antisecremry drugs. Relationship of pharmacological effect lO heal mg rates. Dig Dis Sn 1988;33:619-24.
20. Soll AH, Isenberg JI. Duodenal ulcer diseases. In: Sleiscnger Ml I, Fordtran JS, eds. Gascromtcstinal Disease. Phaladclphaa: WB Saunders, 1983:625-72.
21. Grossman Ml, Guth PH, Isenberg JI, er al. A new look ar peptic. ulcer. Ann Intern Med 1976;84:57-67.
22. Richardson CT. Gasmc ulcer. In: Slc1scngcr Ml I, Fordtrnn JS, eds. Gamointestinal Disease. Philadelphia: WB Saunder.,, 1983:672-93.
23. Sharma BK, Walt RP, PounJer RE, Gomes MdcFA, W1xxl EC, Logan LI I. Oprnnal Jose of oral omepramle for maximal 24 hour decrease of mtragastric arnlity. Gut I 984;25:957-64.
24. Walt RP, Male PJ, Hum RH, Rawlings J, M1lcon-Thomp,on GL, M1Mcw1czJJ. The effect of ran1t1dine and c1mctidinc
on the twenty four hour incrngascnc acidity profile and notturnal at1d secrr tion m duodenal ulcer pattenrs. ScanJ J Ga,rroenrerol 1981. I 9(Suppl)·B-7.
25. Gledhill T, I loward OM, Buck M, Paul A, Hunt RI I. Smgle notturnal dose of an 112 receptor antagonist for the rreacmenc of duodenal ulcer. Gut I 983;24:904-8.
26. Prichard PJ, Yeomans ND, Mihaly GW, ct al. Omeprazole: A srudy of it, mhih1rion of gastric pl I and oral pharmacokmer1cs after morning or even mg dosage. Gasrroentcrology 1985;88:64-9
27. Wa Ian A, Bader J-P, Classen M, er al. Effect of omcprazole and rnnit 1dmc on ulcer healing ,md rel.1p,e rnces m par,cncs w11h hcn1gn g.t\lrlC ulcer. N Engl J Med 1989; U0:69-7 5.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com