Embed Size (px)
Citation preview

Strengthening NICU Healthcare Professionals’ Knowledge
NICUCurrentsFebruary 2012 • Volume 3, Issue 1
Exploring the Neonatal Intensive Care Team7Nutrient Requirements
for Premature InfantsOnline post test - see page 5 for details.1
HeadlineBy Author
Nutrient Requirements for Premature Infants By Jackie Wessel, MEd, RD, CSP, CNSD, CLE
LearnIng ObjectIVesBy the end of this article, the reader should be able to:
• Identify two resources for nutrient requirements in preterm infants.
• Discuss that current multi-trace element packages may not provide appropriate trace elements.
• Identify that, in addition to providing trace elements, measuring the amount of elements may also be a problem.
A new dietitian entering the NICU asks for a nutrition assessment. “What are the nutrient require-
ments for these infants and where do I find a scientifically–based protocol for their feeding?” And I have to say truthfully that I use a cobbled-up set of references, gleaned mainly from talks by the leaders of the neonatal nutrition field that I have attended. I have their slides, book chapters, and many articles, all in an overflowing notebook. Not a neat or efficient way to assess and meet the requirements of these infants. The novice dietitian will inevitably ask, “Isn’t there just one set of recommen-dations that can be followed?”
In truth there are no up-to-date easily accessible national standards available. The situation is different in Europe where such standards can be found at the click of a mouse. A combined study group from the European Society of Paediatric Gastroen-terology, Hepatology and Nutrition and the European Society for Clinical Nutrition and Metabolism formulated evidence-based nutrition guidelines for the premature infant in 2009.1 These are published in English in the journal German Medical Science, with open access. The guidelines follow practi-cal categories: premature infants <1500 g, premature infants >1500 g, and ill full-term infants.1 It is a different approach to the
Earn free CE credits by reading the article and taking the online post test.
Literature Review10
2 | February 2012 NICU Currents
Feature: Nutrient Requirements for Premature Infants
neonatal population than we are used to. Late preterm infants are rarely distinguished here, and the category of sick full-term infants is hardly ever addressed. Full term infants make up a substantial percent of in-fants in the NICUs in children’s’ hospitals, but their needs are not the same as those of well, breastfed infants of the same age. In Europe, individual countries, such as the Netherlands, have implemented guidelines for neonatal nutrition care.2
In North America the latest guideline for neonatal nutrition care was published in Canada in 1995.3 The situation is even more dire in the United States. In a search of the American Academy of Pediatrics (AAP) web-site, the Committee of Nutrition (CON) section does not include a current clinical guideline for neonatal nutrition. There are nutrient requirements for the preterm infant in the Pediatric Nutrition Handbook published by the AAP, now in its 6th edition (2009).4 The data table for the requirements is taken from the Tsang, Uuay, Koletzko and Zlotkin book (2006).5 The Handbook has a chapter discussing preterm nutrition in a textbook style with references, but without grading of the literature. There is limited access to that information, too. The print edition can be purchased, but electronic ac-cess is only available through some hospital libraries that buy the e-book for the users of the library.6 Many recent articles still refer-ence the 1985 nutrition article in Pediatrics from AAP-CON.7
There are several excellent neonatal nu-trition texts. Adamkin (2009)8, Thureen and Hay (2006)9, and Tsang et al (2006)5 stand out. Thureen and Hay10 as well as Greer11 have excellent chapters on nutrient
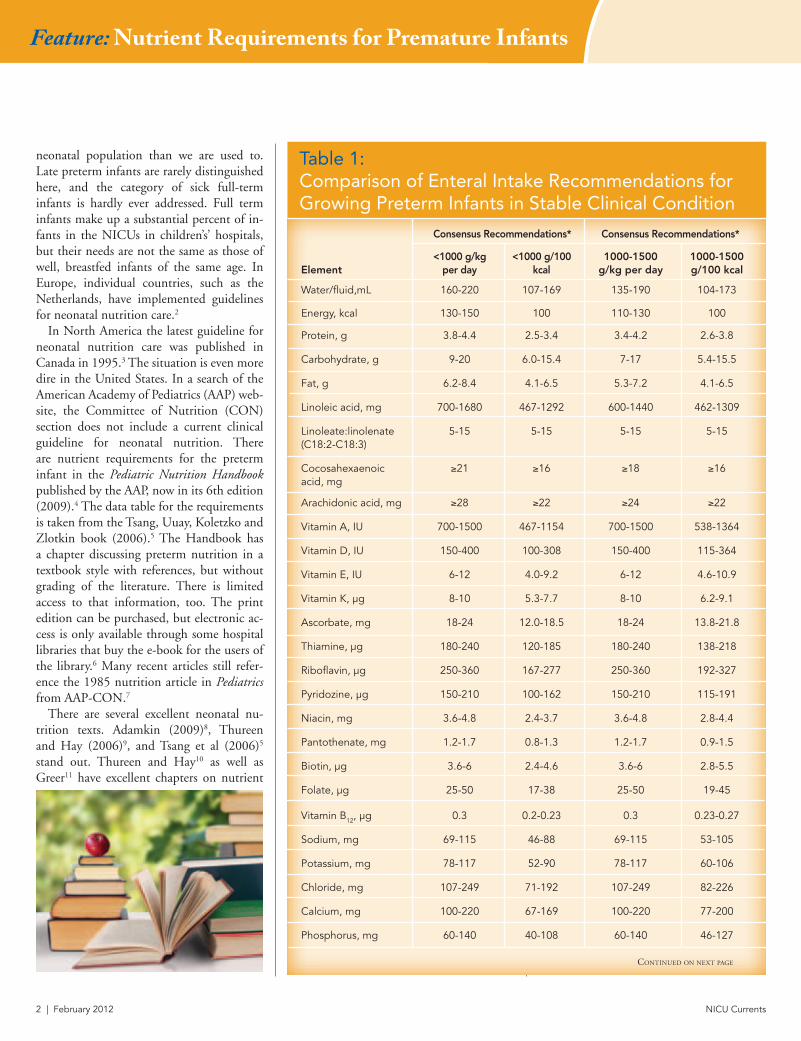
Table 1: Comparison of Enteral Intake Recommendations for Growing Preterm Infants in Stable Clinical Condition
consensus recommendations* consensus recommendations*
element<1000 g/kg
per day<1000 g/100
kcal1000-1500
g/kg per day1000-1500g/100 kcal
Water/fluid,mL 160-220 107-169 135-190 104-173
Energy, kcal 130-150 100 110-130 100
Protein, g 3.8-4.4 2.5-3.4 3.4-4.2 2.6-3.8
Carbohydrate, g 9-20 6.0-15.4 7-17 5.4-15.5
Fat, g 6.2-8.4 4.1-6.5 5.3-7.2 4.1-6.5
Linoleic acid, mg 700-1680 467-1292 600-1440 462-1309
Linoleate:linolenate (C18:2-C18:3)
5-15 5-15 5-15 5-15
Cocosahexaenoic acid, mg
≥21 ≥16 ≥18 ≥16
Arachidonic acid, mg ≥28 ≥22 ≥24 ≥22
Vitamin A, IU 700-1500 467-1154 700-1500 538-1364
Vitamin D, IU 150-400 100-308 150-400 115-364
Vitamin E, IU 6-12 4.0-9.2 6-12 4.6-10.9
Vitamin K, µg 8-10 5.3-7.7 8-10 6.2-9.1
Ascorbate, mg 18-24 12.0-18.5 18-24 13.8-21.8
Thiamine, µg 180-240 120-185 180-240 138-218
Riboflavin, µg 250-360 167-277 250-360 192-327
Pyridozine, µg 150-210 100-162 150-210 115-191
Niacin, mg 3.6-4.8 2.4-3.7 3.6-4.8 2.8-4.4
Pantothenate, mg 1.2-1.7 0.8-1.3 1.2-1.7 0.9-1.5
Biotin, µg 3.6-6 2.4-4.6 3.6-6 2.8-5.5
Folate, µg 25-50 17-38 25-50 19-45
Vitamin B12, µg 0.3 0.2-0.23 0.3 0.23-0.27
Sodium, mg 69-115 46-88 69-115 53-105
Potassium, mg 78-117 52-90 78-117 60-106
Chloride, mg 107-249 71-192 107-249 82-226
Calcium, mg 100-220 67-169 100-220 77-200
Phosphorus, mg 60-140 40-108 60-140 46-127
Continued on next page
NICU Currents February 2012 | 3
requirements in Gastroenterology and Nutri-tion: Neonatology Questions and Controversies (2008). Schanler and Anderson also have an excellent chapter on inpatient care of the low birth weight infant in Nutrition and Pediatrics by Duggan, Watkins, and Walker (2008).12 The nutrient guidelines listed in this chapter are also from Tsang et al.5 The American Dietetic Association (ADA) has a Pocket Guide to Neonatal Nutrition13 as well as a chapter in their Pediatric Nutrition Care Manual on Neonatal Care.14 Sadly, the Nutri-tional Care for High Risk Newborns 3rd edi-tion15 is out of print. The new publisher will not be publishing another edition despite numerous requests, but will not relinquish the copyright, so the future of that text is in limbo. The ADA pocket guide was meant to partially bridge that gap, but many feel that a full-size text is necessary to explain
the evidence and science behind the various recommendations.
The American Society for Parenteral and Enteral Nutrition (ASPEN) covers neonatal nutrition in the ASPEN Pediatric Nutrition Support Core Curriculum16 and Pediatric Nutrition Support Handbook.17 Neonatal nutrition is covered in many of their guide-lines and standards of care, the latest being the 2010 Nutrition Support of Neonates Supported with Extracorporeal Membrane Oxygenation.18 ASPEN also sponsored a
very important research workshop on Micro-nutrients in Parenteral Nutrition in 2009.19 Fourteen international leaders discussed individual micronutrients and a panel of clinicians, including pediatric and neonatal experts, discussed recommendations.19-33
However, it is shocking that the last set of recommendations for micronutrients in pe-diatrics was published in 1988,34 and it is of great concern that these recommendations were never mandated by the Food and Drug Administration and, therefore, never imple-mented.19 So, for example, the 1975 recom-mendations for increased vitamin A – made 36 years ago – are yet to be implemented in a parenteral vitamin product!
New data presented by the workshop and published in the 2009 supplement of Gastroenterology, raised concerns about the issue of contamination of parenteral nutrition with some trace elements.19 Also disturbing are the possibilities that the current multi-trace element packages may not provide the appropriate trace ele-ments. There may be too much of some (chromium and manganese) 22,23 not any of iodine,24 and perhaps inadequate boron, silicon, and molybdenum.26 Iodine was dis-cussed as a possible addition to parenteral nutrition because of the decline in the use of povidone-iodine solutions, which gave patients a dose of iodine. Now that these are not routinely used, iodine deficiency is a concern.19,24 Choline may be advisable as a new addition as well.32 Carnitine appears to be conditionally essential for the neonate, and new lower doses, 2-5 mg/kg, were dis-cussed.33 The difficulty in assessing micro-nutrient status was also covered. For many of the micronutrients, serum levels may not reflect total body levels. The difficulty in the technique of obtaining samples was also discussed. It is not known how long a patient can be without the specific nutrient
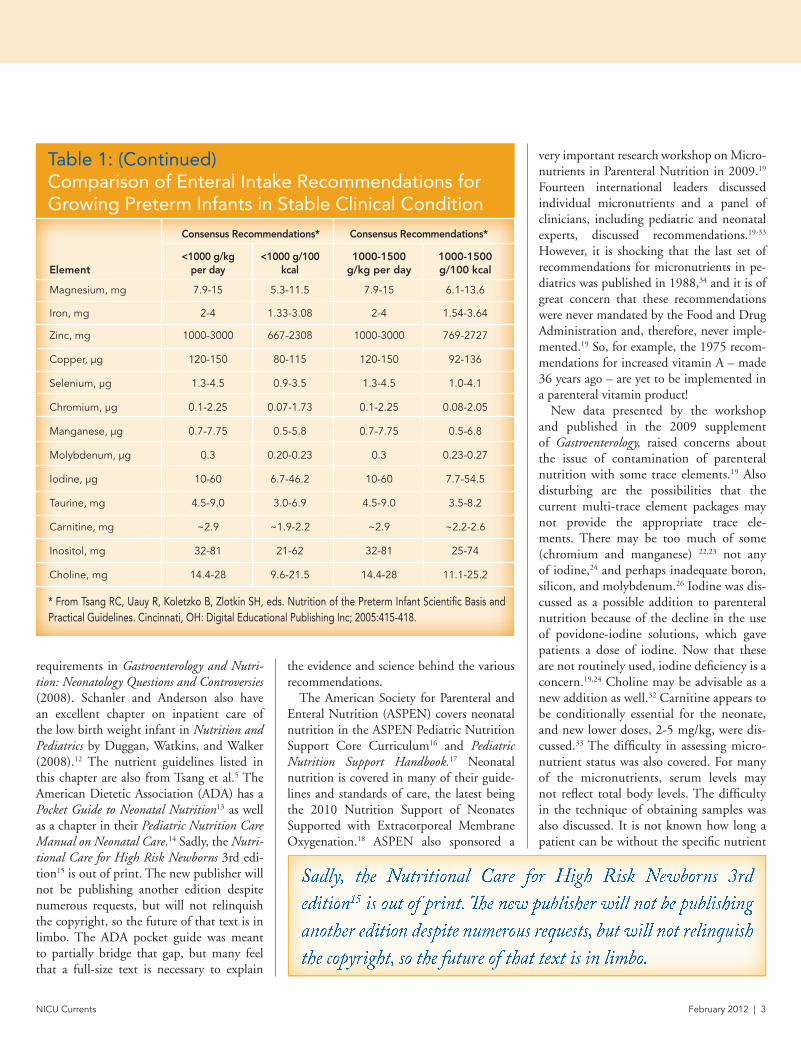
Table 1: (Continued) Comparison of Enteral Intake Recommendations for Growing Preterm Infants in Stable Clinical Condition
consensus recommendations* consensus recommendations*
element<1000 g/kg
per day<1000 g/100
kcal1000-1500
g/kg per day1000-1500g/100 kcal
Magnesium, mg 7.9-15 5.3-11.5 7.9-15 6.1-13.6
Iron, mg 2-4 1.33-3.08 2-4 1.54-3.64
Zinc, mg 1000-3000 667-2308 1000-3000 769-2727
Copper, µg 120-150 80-115 120-150 92-136
Selenium, µg 1.3-4.5 0.9-3.5 1.3-4.5 1.0-4.1
Chromium, µg 0.1-2.25 0.07-1.73 0.1-2.25 0.08-2.05
Manganese, µg 0.7-7.75 0.5-5.8 0.7-7.75 0.5-6.8
Molybdenum, µg 0.3 0.20-0.23 0.3 0.23-0.27
Iodine, µg 10-60 6.7-46.2 10-60 7.7-54.5
Taurine, mg 4.5-9.0 3.0-6.9 4.5-9.0 3.5-8.2
Carnitine, mg ~2.9 ~1.9-2.2 ~2.9 ~2.2-2.6
Inositol, mg 32-81 21-62 32-81 25-74
Choline, mg 14.4-28 9.6-21.5 14.4-28 11.1-25.2
* From Tsang RC, Uauy R, Koletzko B, Zlotkin SH, eds. Nutrition of the Preterm Infant Scientific Basis and Practical Guidelines. Cincinnati, OH: Digital Educational Publishing Inc; 2005:415-418.
Sadly, the Nutritional Care for High Risk Newborns 3rd edition15 is out of print. The new publisher will not be publishing another edition despite numerous requests, but will not relinquish the copyright, so the future of that text is in limbo.

4 | February 2012 NICU Currents
Feature: Nutrient Requirements for Premature Infants
that is being tested to get an accurate result. Without this information the test may only reflect the current micronutrient infusion.19
It is emphasized that meticulous handling is necessary to prevent contamination.
In neonatology, we tend not to use the Di-etary Reference Intakes (DRIs) from the Food and Nutrition Board, Institute of Medicine, National Academies. The DRI has a life-stage group for infants 0-6 months and 6 months to 1 year, but no category for premature infants. The DRIs are also not meant to be used to prescribe individual intakes.35
There are a couple of options to view when looking at the nutrient requirements of pre-mature infants. The nutrient requirements ac-companying this article by Tsang et al are the ones most often cited in the neonatal nutrition literature. When they are revised in the future, a wish list of contents would include:
a. Evidence-based recommendations;b. A guideline that is easily available online;c. Quantifying the amounts needed; d. Timing of administration; e. Optimal composition, such as that of
amino acids, or type of product to be used;
Table 2: Comparison of Parenteral Intake Recommendations for Growing Preterm Infants in Stable Clinical Condition
consensus recommendations* consensus recommendations*
element<1000 g/kg
per day<1000 g/100
kcal1000-1500
g/kg per day1000-1500g/100 kcal
Water/fluid,mL 140-180 122-171 120-160 120-178
Energy, kcal 105-115 100 90-100 100
Protein, g 3.5-4.0 3.0-3.8 3.2-3.8 3.2-4.2
Carbohydrate, g 13-17 11.3-16.2 9.7-15 9.7-16.7
Fat, g 3-4 2.6-3.8 3-4 3.0-4.4
Linoleic acid, mg 340-800 296-762 340-800
Linoleate:linolenate (C18:2-C18:3)
5-15 5-15 5-15 5-15
Vitamin A, IU 700-1500 609-1429 700-1500 700-1667
Vitamin D, IU 40-160 40-160
Vitamin E, IU 2.8-3.5 2.4-3.3 2.8-3.5 2.8-3.9
Vitamin K, µg 10 8.7-9.5 10 10.0-11.1
Ascorbate, mg 15-25 13.0-23.8 15-25 15.0-27.8
Thiamine, µg 200-350 174-333 200-350 200-389
Riboflavin, µg 150-200 130-190 150-200 150-222
Pyridozine, µg 150-200 130-190 150-200 150-222
Niacin, mg 4-6.8 3.5-6.5 4-6.8 4.0-7.6
Pantothenate, mg 1-2 0.9-1.9 1.2 1.0-2.2
Biotin, µg 5-8 1.3-7.6 5-8 5.0-8.9
Folate, µg 56 49-53 56 56-62
Vitamin B12, µg 0.3 0.26-0.29 0.3 0.30-0.33
Sodium, mg 69-115 60-110 69-115 69-128
Potassium, mg 78-117 68-111 78-117 78-130
Chloride, mg 107-249 93-237 107-249 107-277
Calcium, mg 60-80 52-76 60-80 60-89
Phosphorus, mg 45-60 39-57 45-60 45-67
Magnesium, mg 4.3-7.2 3.7-6.9 4.3-7.2 4.3-8.0
Iron, mg 100-200 87-190 100-200 100-222
Zinc, mg 400 348-381 400 400-444Continued on next page

NICU Currents February 2012 | 5
f. Special categories addressing the needs of infants who are sick and stressed, or have large wounds;
g. Categories broken down into weeks of gestation, including a category for the late preterm infant; and
h. A calendar for revising the standards, such as every 5 years.
This last item is important, as neonatal nutrition knowledge advances rapidly. For example, we now feel that there is an optimum time to deliver amino ac-ids in the first IV. Simply viewing a chart would not indicate when to give the needed protein.36-43
Revising the guidelines will be a daunting task, but one that is vitally needed for the optimal care of premature and sick infants.
About the Author Jacqueline J. Wessel, MEd, RD, CNSD, CSP, CLE is a Neonatal Nutritionist in the Regional Center for Neonatal Intensive Care at Cincin-nati Children’s Hospital. The author was com-pensated by Abbott Nutrition l
Complete the quiz on line at www.anhi.org at no charge. Please note online questions or answers are randomized and may not appear in the same sequence below. Do not assume that the “letter” preceding the correct response will be identical to the online version.
Post-Test: Nutrition and the Late Preterm Infant
abbott nutrition Health Institute, is an approved provider of continuing nursing education by the california board of registered nursing Provider #ceP 11213.
credit: 1 contact
hour
True/False:1. There are no up-to-date, easily accessible
national standards for nutrient require-ments in preterm infants in the US.
a. True b. False
2. The European Society of Paediatric Gas-troenterology, Hepatology, and Nutrition have formulated a set of easily accessible evidence-based nutrition guidelines for pre-term infants.
a. True b. False
3. In North America the latest guideline for neonatal nutrition care was pub-lished in Canada in 1995.
a. True b. False
4. The Committee on Nutrition of the AAP has a section on the current clinical guide-line for neonatal nutrition.
a. True b. False
5. Nutrient requirements for preterm infants are available in the AAP’s Pediatric Nutri-tion Handbook, but not online.
a. True b. False
Table 2: (Continued) Comparison of Parenteral Intake Recommendations for Growing Preterm Infants in Stable Clinical Condition
consensus recommendations* consensus recommendations*
element<1000 g/kg
per day<1000 g/100
kcal1000-1500
g/kg per day1000-1500g/100 kcal
Copper, µg 20 17-19 20 20-22
Selenium, µg 1.5-4.5 1.3-4.3 1.5-4.5 1.5-5.0
Chromium, µg 0.05-0.3 0.04-0.29 0.05-0.3 0.05-0.3
Manganese, µg 1 0.87-0.95 1 1.00-1.11
Molybdenum, µg 0.25 0.22-0.24 0.25 0.25-0.28
Iodine, µg 1 0.87-0.95 1 1.00-1.11
Taurine, mg 1.88-3.75 1.6-3.6 1.88-3.75 1.9-4.2
Carnitine, mg ~2.9 ~2.5-2.8 ~2.9 ~2.9-3.2
Inositol, mg 54 47-51 54 54-60
Choline, mg 14.4-28 12.5-26.7 14.4-28 14.4-31.1
* From Tsang RC, Uauy R, Koletzko B, Zlotkin SH, eds. Nutrition of the Preterm Infant Scientific Basis and Practical Guidelines. Cincinnati, OH: Digital Educational Publishing Inc; 2005:415-418.

6 | February 2012 NICU Currents
Feature: Nutrient Requirements for Premature Infants
REFERENCES1. Fusch C, Bauer K, Boehles HJ, et al: Neonatal/
Paediatric Guidelines Chapter 13 Ger Med Sci 20097 Doc 15.
2. Elsstgeest LE, Martens SE, Lopriore E, et al: Does parenteral nutrition influence electro-lytes and fluid balance in preterm infants in the first few days after birth? pLoS One 2010; 5:e9033.
3. Nutrition Commmittee, Canadian Paediatric Society, Nutrient needs and feeding of prema-ture infants. CMAJ 1995, 152:1765-1785.
4. Kleinman RE, ed: Pediatric Nutriton Hand-book, Elk Grove Village: American Association of Pediatrics, 2009.
5. Tsang R, Uuay R, Koletzko B, Zlotkin S: Nutri-ton of the preterm infant: Scientific basis and practical applications. 2nd ed. Cincinnati: Dig-ital Education Publications, 2006.
6. Kleinman RE, ed: Pediatric Nutrition Hand-book, Elk Grove Village: American Association of Pediatrics, 2009 e-book.
7. American Academy of Pediatrics Committee on Nutrition: Nutritional needs of low birth weight infants Pediatrics 1985; 76:976-986.
8. Adamkin D: Nutritional Strategies for the Low Birth Weight Infant. Cambridge: Cambridge University Press, 2009.
9. Thureen PJ, Hay WW Jr, eds: Neonatal Nutri-tion and Metabolism. Cambridge: Cambridge University Press, 2009.
10. Thureen PJ, Hay WW: Nutritional Require-ments of the Very Low Birth Weight Infant. In Neu J and Polin RA, eds: Gastroenterology and Nutrition: Neonatology Questions and Controversies. Philadelphia: Saunders, 2008. Pages 208-223.
11. Greer F: Macro and Micronutrients. In Neu J and Polin RA, eds: Gastroenterology and Nu-trition: Neonatology Questions and Contro-versies. Philadelphia: Saunders, 2008. Pages 224-252.
12. Schanler RJ, Anderson D: The Low Birthweight Infant: Inpatient Care. In Duggan C, Watkains JB, Walker WA, eds: Nutrition in Pediatrics 4: Basic Science Clinical Applications. Hamilton: BC Decker, 2008. Pages 377-394.
13. Groh-Wargo S, Thompson M, Cox JH: PNPG, ADA Pocket Guide to Neonatal Nutrition, Chi-cago: American Dietetic Association, 2009.
14. Pediatric Nutrition Care Manual (online). Chi-cago: American Dietetic Association, 2010.
15. Groh-Wargo S, Thompson M, Cox JH: Nutri-tional Care for High Risk Newborns. Chicago: Precept Press, 2000.
16. Corkins, MR, ed: Pediatric Nutrition Support Handbook. Silver Spring, MD: ASPEN, 2011.
17. ASPEN Pediatric Nutrition Support Core Cur-riculum. Silver Spring: ASPEN, 2010.
18. Jaksic T, Hull MT, Modi BP, et al: A.S.P.E.N. Clinical Guidelines: Nutrition Support of Ne-onates Supported with Extracorporeal Mem-brane Oxygenation J Parenter Enteral Nutr 2010; 34:247.
19. Buchman AL, Howard LJ, Guenter P, et al.. Micronutrients in parenteral nutrition: Too little or too much? Gastroenterol 2009 137: S1-6.
20. Jeejeebhoy K: Zinc: an essential trace ele-ment for parenteral nutrition Gastroenterol 2009; 137:S7-12.
21. Shike M: Copper in parenteral nutrition Gas-troenterol 2009; 137:S13-17.
22. Mourkarzel A: Chromium in parenteral nutri-tion: Too little or too much? Gastroenterol 2009; 137:S18-28.
23. Hardy G: Manganese in parenteral nutrition: Who, what, and why should we supplement? Gastroenterol 2009; 137:S29-35.
24. Zimmerman MB: Iodine: It’s important to pa-tients that require parenteral nutrition. Gas-troenterol 2009; 137:536
25. Forbes A: Iron and parenteral nutrition Gas-troenterol 2009: 137:S47-54.
26. Nielsen FA: Micronutrients in parenteral nu-trition: Boron, Silicon, and Fluoride Gastroen-terol 2009; 137:S55-60.
27. Shenkin A: Selenium in intravenous nutrition Gastroenterol 2009: 137:S61-69.
28. Berger MM: Vitamin C requirements in parenteral nutrition Gastroenterol 2009; 137:S70-78.
29. DeLuca H: Vitamin D and the parenteral nutri-tion patient Gastroenterol 2009; 137:S79-91.
30. Biesalki HK: Vitamin E requirements in paren-teral nutrition Gastroenterol 2009; 137:S92-104. Gastroenterol 2009, 137:S105-118.
31. Shearer MA: Vitamin K in parenteral nutrition Gastroenterol 2009; 137:S105-118.
32. Buchman AL: The addition of choline to parenteral nutrition Gastroenterol 2009; 137:S119-128.
33. Boum PR: Carnitine in parenteral nutrition Gastroenterol 2009; 137:S129-134.
34. Greene HL, Hambridge KM Schanler R, et al: Guidelines for the use of vitamins, trace ele-ments, calcium, magnesium, phosphorus in infants and children receiving total parenteral nutrition. Report of the subcommittee on Pe-diatric Parenteral Nutrient Requirements from the Committee on Clinical Practice Issues of the American Society for Clinical Nutrition Am J Clin Nutr 1988; 48:1324.
35. Aggett PJ, Bresson J, Haschke F, Hernell O, Ko-letzko B, Lafeber HN, Michaelsen KF, Micheli J, Ormisson A, Rey J, de Sousa JS, Weaver L: Rec-ommended Dietary Allowances (RDAs), Recom-mended Dietary Intakes (RDIs), Recommended Nutrient Intakes (RNIs), and Population Refer-ence Intakes (PRIs) are not “recommended intakes” J Pediatr Gastroenterol Nutr 1997; 25(2):236-41.
36. Stephens BE, Walden RV, Gargus RA, et al: First week protein and energy intakes are associ-ated with 18 month developmental outcomes in extremely low birth weight infants Pediatrics 2009; 123:1337-1343.
37. Te Braake FW, van der Akker CH, Wattimena DJ, et al. Amino acid administration in prema-ture infants directly after birth J Pediatr 2005; 147:457-461.
38. Thureen PJ, Anderson AH, Baron KA, et al: Pro-tein balance in the first week of life in ventilated infants receiving parenteral nutrition Am J Clin Nutr 1998; 68:1128-1135.
39. Thureen PJ, Hay WW Jr: Early aggressive nutri-tion in preterm infants Semin Neonatol 2001; 6:405-415.
40. Thureen PJ, Melara D, Fennesy PV, et al: Effect of low versus high intravenous amino acid in-take on very low birth weight infants in the early neonatal period Pediatr Res 2003; 53:24-32.
41. Valentine CJ, Fernandez S, Rogers LK, et al: Early amino acid administration improves preterm infant weight J Perinatol 2009; 29:428-432.
42. Van Goudoever JB, Colen T, Wattimena JL, et al: Immediate commencement of amino acid supplementation in preterm infants: effect on serum amino acid concentrations and protein kinetics on the first day of life J Pediatr 1995; 127:458-465.
43. Vlaardingerbroek H, van Houdoevr JB, van den Akker CHP: Initial nutritional management of the preterm infant Early Human Dev 2009; 85:691-695.

NICU Currents February 2012 | 7
Feature: Exploring the Neonatal Intensive Care Team
Speech-Language Pathologists (SLP), Occupational Therapists (OT) and Physical Therapists (PT) are vital mem-
bers of the interdisciplinary treatment team in the neonatal intensive care unit (NICU). Therapists assist parents and nursing/medical
Exploring the Neonatal Intensive Care Team: Specialization by Speech-Language Pathology, Occupational Therapy and Physical Therapy By Bridget Kaminski, MA, CCC-SLP and Julie McCoy, MOT, OTR/L
staff to understand and participate in the nor-mal developmental path of growth and matu-ration for neonates. This article discusses the importance of both the separate roles of SLPs, OTs and PTs, as well as the cross-over that in-herently happens between these disciplines. As
members of the medical team, these therapists address specific neonatal developmental needs when requested by a neonatologist and/or an advanced practice nurse.
Review of current literature reveals what could be construed as a struggle among SLPs, OTs and PTs in defining their explicit roles in the NICU. The American Speech-Language Hearing Association (ASHA) purports that the SLP is specifically appropriate for NICU work because of their “holistic competence in feeding and swallowing disorders, early com-munication development and caregiver-child interaction.”1 The American Occupational Therapy Association maintains that the OT’s ability to perform analysis of activities with adaptation to reach specific functional goals gives OTs a unique perspective for treatment of neonates in the NICU. Because discrepancies exist between the NICU environment, parental expectations and the infant’s capabilities, OTs provide education to achieve a “goodness of fit – the match between the infant’s capabilities and the physical and social environment.”2 Swee-ney et al3 suggest that the PT’s comprehensive
This article discusses the im-portance of both the separate roles of SLPs, OTs and PTs, as well as the cross-over that inherently happens between these disciplines.

8 | February 2012 NICU Currents
Feature: Exploring the Neonatal Intensive Care Team
knowledge of neurodevelopmental and muscu-loskeletal systems enables them to perform as equal partners on the neonatal team for evalu-ation of physiologically unstable infants. Early motor experiences provided by PT have a direct effect on central nervous system maturation and overall motor development.4 All three dis-ciplines require mutually advanced and special-ized training (beyond classroom fundamentals) to prepare therapists to work with neonates and their families in the NICU.2,3,5
Perhaps the biggest cross-over of roles occurs between SLP and OT in the assessment and treatment of neonatal feeding skills. Both SLPs and OTs pursue special training in infant swal-lowing and feeding to include: (a) normal feed-ing milestones, (b) normative versus premature reflexes, (c) infant feeding readiness cues and (d) the infant’s endurance capabilities. Therapists addressing feeding issues in the NICU must also be proficient in judging the infant’s latch, non-nutritive suck abilities, coordination of suck-swallow-breathe patterns, medical con-
cerns related to feeding (such as reflux and/or aspiration), oral hypersensitivities, feeding aver-sions and overall stability in vital signs.6
Therapists must also understand the necessity of feeding milestones including the time frame during which the acquisition of independent swallowing ability occurs. In addition, the im-pact of the individual neonate’s medical condi-tion influences his ability to acquire these skills. Swallowing is present at 16 weeks gestation and is fully developed at full term birth (38-42 weeks). Neonates less than 28 weeks gestational age (GA) have significant feeding delays related to initiation and progression to total oral feed-ing, which results in prolonged length of stay in the NICU.7,8 Infants greater than 28 weeks GA acquire feeding milestones more quickly and successfully when compared to their younger
peers. After initial assessment by the SLP or OT to evaluate the neonate’s oral motor cues, feeding readiness, cardiorespiratory stability and gastrointestinal tolerance/function, oral feedings are initiated. Therapists also provide education to parents and staff to facilitate the infant’s abil-ity to achieve oral feedings, which can lead to a safer, quicker discharge to home.9
The role of the SLP differs from the OT in the NICU by the ability of the SLP to assess an infant’s swallowing by Modified Barium Swallow Studies (MBSS). Along with a radiologist, the SLP assesses the stages of an infant’s swallow using various feeding thicknesses, nipples and feeding positions while viewing x-ray images. Using the MBSS the SLP assesses the oral and pharyngeal phases of the swallow as well as the infant’s latch and suck-swallow-breathe coor-
Perhaps the biggest cross-over of roles occurs between SLP and OT in the assessment and treatment of neonatal feeding skills.

NICU Currents February 2012 | 9
dination. If reflux is considered a cause in the neonate’s swallowing difficulty, both a MBSS and upper GI study can be performed in con-junction with each other. Performing these two studies together not only minimizes the neo-nate’s x-ray exposure, but enables the radiologist and SLP to also assess the esophageal phase of the infant’s swallow.
The OT’s role in the NICU also differs from the SLP’s role because the OT focuses on the overall effect of the environment on the infant. OTs provide modification and adaptation of the neonate’s sensory experiences to promote matu-ration and progressive developmental growth.2 Specific skills the OT brings to the NICU environment include: positioning/handling techniques for feeding and play tasks, visual stimulation, sensory activities, assessment of car seat position for respiratory stability and splint-ing for maintenance of joint integrity.
The PT’s distinct role in the NICU includes a focus on the maturation and organization of
emerging reflexes and physiologic stability. Spe-cific skills that the PT brings to the NICU in-clude observation/assessment of joint alignment, posture, muscle tone/strength and the infant’s ability to achieve transitional movements.10 PTs play an integral role for infants with any type of musculoskeletal disorder or deformity.
Utilizing a multidisciplinary therapeutic approach in the NICU optimizes care for all neonates because each discipline brings a unique perspective to solving problems. Per-haps the most important common ground among SLPs, OTs and PTs is their comprehen-sive approach to education — teaming with and coaching parents and other caregivers to achieve the best developmental outcomes for these fragile infants.
REFERENCES1. Therapy Times-SLP/OT Supplement: Learning
the basics of feeding, January 2011.2. Vergara E, Anzalone M, Bigsby R, et al: Spe-
cialized knowledge and skills for occupational therapy practice in the neonatal intensive care unit. American Journal of Occupational Therapy 2006; 60:659.
3. Sweeney, JK, Heriza CB, Blanchard Y: Part I: Clinical competencies and neonatal intensive care unit clinical training models Neonatal Phys-ical Therapy 2009; 21:296.
4. Sweeney JK, Heriza CB, Blanchard Y, Dusing SC: Part II: Practice frameworks and evidence-based practice guidelines. Neonatal Physical Therapy 2010; 22:2.
5. ASHA Practice Policy: “Roles of Speech-Lan-guage Pathologists in the NICU: Position State-ment 2004”
6. Thoyre, SM, Shaker, CS, Pridham, KF: The Early Feeding Skills Assessment for Preterm Infants. Neonatal Netw. 2005; 24(3):7-16.
7. Drenckpohl D, Dudas R, Justice S, et al: Out-comes from an oral feeding protocol imple-mented in the NICU Infant Child and Nutrition 2009; 1:1.
8. Jadcherla SR, Wang M, Vijayapal AS, Leuth-ner SR: Impact of prematurity and co-mor-bidities on feeding milestones in neonates: A retrospective study Journal of Perinatology 2010; 30:201.
9. Caretto V, Topolski KF, Linkous CM, et al: Cur-rent parent education on infant feeding in the neonatal intensive care unit: The role of the occupational therapist American Journal of Occupational Therapy 2000; 54:59.
10. Mahoney MC, Cohen MI: Effectiveness of developmental intervention in the neonatal intensive care unit: Implications for neonatal physical therapy Pediatr Phys Therapy 2005; 17:194.
ABOUT THE AUTHORS:bridget Kaminski, Ma, ccc-sLP graduated from Louisiana State University in Baton Rouge, Louisiana in 1992 and 1994 with both her Bachelors of Commu-nication Disorders and Masters of Speech-Language Pathology, respectively. Ms. Kaminski has 17 years experience in the areas of neonatal, pediatric, adult and geriatric populations with head/neck cancers, traumatic brain injuries including stroke, spinal cord injuries, progressive degenerative disorders, congeni-tal anomalies and prematurity of birth. Since 1994, Ms. Kaminski has been a member of the American Hear-ing and Speech Association. She also holds special certifications in her profession and has received nu-merous awards. She and Ms. McCoy co-authored and presented at the Neonatal Intensive Care Specialists Conference in Houston, Texas on the topics of Prader-Willi Syndrome and Therapeutic Feeding in the NICU. She would like to dedicate this publication to her two beautiful children, Catherine and Connor.
julie Mccoy, MOt, Otr/L graduated with honors from the University of Southern Mississippi with a Bachelor’s degree in Social and Rehabilitation Services in 1993. Ms. McCoy graduated magna cum laude from Texas Woman’s University in 1995 with a Master’s De-gree in Occupational Therapy. Ms. McCoy is an Occu-pational Therapist with 13 years experience. She and Ms. Kaminski co-authored and presented at the Neo-natal Intensive Care Specialists Conference in Hous-ton, Texas on the topics of Prader-Willi Syndrome and Therapeutic Feeding in the NICU. Currently, she is the Director of Therapy and Rehabilitation Services at Cy-press-Fairbanks Medical Center Hospital. Ms. McCoy continues with direct therapeutic care of the neona-tal, pediatric, adult and geriatric patient populations.
Specific skills the OT brings to the NICU environment include: positioning/handling techniques for feeding and play tasks, visual stimulation, sensory activities, assessment of car seat position for re-spiratory stability and splinting for maintenance of joint integrity.

10 | February 2012 NICU Currents
Literature ReviewLiterature Review
Leverson KT, Sommerfelt K, Ronnestad A, et al: Prediction of neurodevelop-mental and sensory outcome at 5 years in Norwegian children born extremely preterm Pediatrics 2011;127:e630.
From 1999 to 2000 all preterms in Norway with a gestational age (GA) between 22 and 27 weeks
and birthweights from 500-999 grams (n=638) were enrolled in a prospective observational study. Three hundred and six (82%) of these children were studied at a mean age of 5 years and 10 months
of age for the presence of cerebral palsy, blindness, deafness, and intelligence quo-tient (IQ).
Outcomes for the 306 children assessed included neurodevelopmental (ND) dis-ability rates of: (1) severe: 6% (n=18), (2) moderate: 9% (n=29), (3) mild: 41% (n=124), and (4) none: 44% (n=135). However, stratified by GA, outcomes were poorer for those children born at <25 weeks when compared to those born be-tween 26 and 27 weeks GA. Those extreme preterms born at 23-25 weeks GA with no neurodevelopmental disability accounted for 25% of the survivors while 51% of pre-terms born between 26 and 27 weeks GA had no ND. When stillbirths and deaths were included, survival without severe or moderate disability was 33% (born at 23-25 weeks GA) and 72% for those born at 26-27 weeks GA. For preterm survivors without CP, blindness or deafness GA has a limited association with cognitive and motor function. Higher cognitive and motor scores were associated with higher maternal education, normal intrauterine growth pattern, lack of severe retinopathy of prematurity and being a girl.
Luu TM, Ment L, Allan W, et al: Ex-ecutive and memory function in ado-lescents born very preterm Pediatrics 2011; 127:e639.
Seventy-seven percent (n=337) of 437 adolescents born between 1989 and 1992 in hospitals in Providence,
Rhode Island, Portland, Maine and New Haven, Connecticut with birthweights <1250 grams were studied at age 16 years. This cohort of adolescents (preterms at birth) was compared to 102 adolescent (born at full term) controls. Executive function, mental processes such as inhibi-tion, planning, sequencing, organization, cognitive flexibility and verbal fluency, that are necessary for learning and success in school were studied in both groups. Com-pared to the teens born at term the pre-
Editor’s NotE:
term-born adolescents showed significant deficits on tasks of verbal fluency, cognitive flexibility, planning/organization, inhibi-tion, and verbal, visuospatial and working memory. Even when the adolescents with significant disabilities (i.e., neurosensory and intelligence quotient <70) were ex-cluded, the significant group differences in executive function and memory persisted.
Predictors of performance of memory and executive function included severe brain injury and maternal education level. A neo-natal head ultrasound showing severe brain injury was highly predictive of lower scores on all measures of memory and executive function. Higher maternal education was associated with better results on adolescents’ executive function, and lower maternal edu-cation was associated with lower scores in these areas. Surprisingly, male gender, expo-
sure to indomethacin and antenatal steroids, being small for gestational age, birth weight and oxygen requirement at 28 days were not related to executive function or memory deficits during adolescence. So, even preterm infants who survive seemingly “intact” into adolescence still have school problems re-lated to their preterm birth throughout their academic life.

NICU Currents February 2012 | 11
Editor’s NotE:
McIntyre S, Badawi N, Brown C, Blair E: Population case-control study of cerebral palsy: Neonatal predictors for low-risk term singletons Pediatrics 2011;127:e667
This total population case-control study from the Western Australian Cerebral Palsy Register examined
term-born infants with cerebral palsy (CP) (n=442) with term-born controls (n=468). Because term infants account for the ma-jority of CP cases and the strongest predic-tor of subsequent CP in admission to the NICU with neonatal encephalopathy, this study examined: (1) term infants who did not receive NICU care, (2) compared CP
between this group and term infants who received NICU care and (3) identified neo-natal risk factors for CP in those infants not admitted to NICU.
In this study, 67% of the term infants (n=295) with CP were not admitted to the NICU at birth. In the affected infants all types of CP were represented, including 54% of those with the most severe deficits. In this group of term infants neonatal predictors of subsequent CP included: (1) abnormalities in tone, (2) temperature regulation, (3) consciousness, (4) fontanelles, (5) need for resuscitation at birth and (6) birth defects. Though the risk of CP increased with the number of risk factors, 39% of the infants who were not admitted to the NICU had none of the six risk factors.
Ligi I, Millet V, Sartor C, et al: Iatrogenic events in neonates: Beneficial effects of prevention strategies and continuous monitoring Pediatrics 2010; 126: e1461.
A 54-bed Level III neonatal center in France included all neonates born between January 1 and September
1, 2005 (the preintervention phase) and between January 1, 2008-2009 (the pos-tintervention phase). An anonymous, non-punitive, prospective, continuous incident reporting system was used to collect data about IE, defined by the researchers as “any event that occurred during hospitalization that compromised the safety of the patient, even if the patient was not harmed.” Events included as IEs were medication errors, ad-verse drug events, nosocomial infections,
severe and preventable IEs; “near-miss” events were not reported or collected.
A multidisciplinary care quality-improve-ment team analyzed data, performed root-cause analysis, and implemented corrective actions. Improvement opportunities were focused on 5 major areas: (1) reduction of central catheter infections, (2) limiting inva-sive procedures on low-birth-weight infants, (3) reducing unplanned (“accidental”) extuba-tions, (4) reducing 10-fold drug infusion rate errors and (5) minimizing cutaneous injuries.
Comparing the two time periods, the frequency of IEs was reduced after their in-terventions from 7.6 to 4.8/1000 patient days. The most fragile infants (<1250 grams) experienced significantly fewer severe IEs in 2008 than during 2005. Central catheter infections were significantly decreased from 2005 to 2008 and remained significantly decreased after adjustment for weight, gesta-tional age and catheter days. During the study periods, use of central catheters also decreased significantly from 359 to 239days/1000 pa-tient days. Ten-fold drug-dosing errors were significantly reduced with the interventions. No appreciable changes were found in the in-cidence of medication errors/100 admissions or in prescription errors. There was a trend toward reduction in the incidence of severe medication errors and a non-significant trend toward fewer cutaneous injuries (i.e., nasal ne-
crosis during nasal CPAP). During the study there was a surprisingly significant increase in the incidence of unplanned extubations from 4.9% in 2005 to 7% in 2008. Accidental tube displacement was ascribed most often to spontaneous movement and education, bilateral fixation and a novel weaning/ extuba-tion method was introduced to correct tube dislodgement. A change in hospital culture-—doctors viewing nurses as collaborators— assists in preventing medication errors.

Choose the most nutrition options
for the infantswho needthem most
©2012 Abbott Laboratories 80349.001/February 2012 LITHO IN USA www.abbottnutrition.com82783
Only Abbott Nutrition provides 27 different nutrition options for the NICU
For more information and patient support, visit us at: www.abbottnutrition.com
12 calorie options for human milk forti�cation 15 calorie options with the
Similac® Special Care® Liqui-Mix® System
Similac Expert Care® NeoSure® for the NICU to year 1
SIM974_80349_001_DialedUP_Ad_r01.indd 1 1/12/12 4:42 PM
Prolact+ H2MF® is manufactured by ProlactaBioscience, Monrovia, CA 91016