-
4521 (9/17)
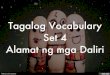
HEADER INFORMATION1. Type of Transaction (Check all applicable
boxes)
� Statement of Actual Services – OR – � Request for
Predetermination/Preauthorization
CARRIER NAME AND ADDRESS:2. Delta Dental of Illinois
P.O. Box 5402Lisle, IL 60532
(Please do not use for DeltaCare dental HMO)PRIMARY PAYER
INFORMATION3. Name, Address, City, State, Zip Code
PRIMARY SUBSCRIBER INFORMATION4. Name (Last, First, Middle
Initial, Suffix), Address, City, State, Zip Code
5. Date of Birth (MM/DD/CCYY) 6. Gender 7. Subscriber Identifier
(SSN or ID#)� M � F
8. Plan/Group Number 9. Employer Name
PATIENT INFORMATION10. Relationship to Primary Subscriber (Check
applicable box) 11. Student Status
� Self � Spouse � Dependent Child � Other � FTS � PTS
12. Name (Last, First, Middle Initial, Suffix), Address, City,
State, Zip Code
13. Date of Birth (MM/DD/CCYY) 14. Gender 15. Patient ID/Account
# (Assigned by Dentist)� M � F
OTHER COVERAGE
16. Other Dental or Medical Coverage? � No (Skip 17-23) � Yes
(Complete 16-23)
17. Subscriber Name (Last, First, Middle Initial, Suffix)
18. Date of Birth (MM/DD/CCYY) 19. Gender 20. Subscriber
Identifier (SSN or ID#)� M � F
21. Plan/Group Number 22. Relationship to Primary Subscriber
(Check applicable box)� Self � Spouse � Dependent � Other
23. Other Carrier Name, Address, City, State, Zip Code
RECORD OF SERVICES PROVIDED24. Procedure Date 25. Area 26. 27.
Tooth Number(s) 28. Tooth 29. Procedure 29a. Diag. Pointer
(MM/DD/CCYY) of Oral Tooth or Letter(s) Surface Code 30.
Description 31. FeeCavity System
1
2
3
4
5
6
7
8
9
10
MISSING TEETH INFORMATION Permanent Primary33. (Place an ‘X’ on
each missing tooth) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 A B C D
E F G H I J
32 31 30 29 28 27 26 25 24 23 22 21 20 19 18 17 T S R Q P O N M
L K
31a. OtherFee(s)
32. Total Fee
35. Remarks
AUTHORIZATIONS36. I have been informed of the treatment plan and
associated fees. I agree to be responsiblefor all charges for
dental services and materials not paid by my dental benefit plan,
unless pro-hibited by law, or the treating dentist or dental
practice has a contractual agreement with myplan prohibiting all or
a portion of such charges. To the extent permitted by law, I
consent toyour use and disclosure of my protected health
information to carry out payment activities inconnection with this
claim.X_________________________________________________________________________________________Patient/Guardian
signature Date
37. I hereby authorize and direct payment of the dental benefits
otherwise payable to me,directly to the below named dentist or
dental entity.
X_________________________________________________________________________________________Subscriber
signature Date
BILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or
dental entity is not submitting claim on behalf of the patient or
insured/subscriber)
48. Name, Address, City, State, Zip Code
49. Corporate Entity NPI (Type 2) 50. License Number 51. SSN or
TIN
ANCILLARY CLAIM/TREATMENT INFORMATION38. Place of Treatment
(Check applicable box) 39. Number of Enclosures (00 to 99)
� Provider’s Office � Hospital � ECF � OtherRadiograph(s) Oral
Image(s) Model(s)
40. Is Treatment for Orthodontics? 41. Date Appliance Placed
(MM/DD/CCYY)� No (Skip 41-42) � Yes (Complete 41-42)
42. Months of Treatment 43. Replacement of Prostheses? 44. Date
Prior Placement (MM/DD/CCYY)Remaining � No � Yes (Complete 44)
45. Treatment Resulting from (Check applicable box)�
Occupational illness/injury � Auto accident � Other accident
46. Date of Accident (MM/DD/CCYY) 47. Auto Accident State
TREATING DENTIST AND TREATMENT LOCATION INFORMATION53. I hereby
certify that the procedures as indicated by date are in progress
(for proceduresthat require multiple visits) or have been completed
and that the fees submitted are the actual fees I have charged and
intend to collect for those procedures.
X_________________________________________________________________________________________Signed
(Treating Dentist) Date
54. Individual NPI (Type 1) 55. License Number
56. Address, City, State, Zip Code 56a. Provider Specialty
Code
57. Phone Number ( ) – 58. Treating ProviderSpecialty
34. Diagnosis Code List Qualifier �� (ICD-9 = B, ICD-10 = AB)
34a. Diagnosis Code(s) A _______________ B ________________ C
_______________ D ________________(Primary diagnosis in “A”)
52. Phone Number ( ) – 52a. Additional Provider ID
-
Discrimination is Against the Law Delta Dental of Illinois
complies with all applicable Federal and State civil rights laws
and does not discriminate on the basis of race, color, national
origin, age, disability, gender, or gender identity. Delta Dental
of Illinois does not exclude people or treat them differently
because of race, color, national origin, age, disability, gender or
gender identity. Delta Dental of Illinois:
Provides free aids and services to people with disabilities to
communicate effectively with us, such as:
o Qualified sign language interpreters o Written information in
other formats (large print, audio, accessible electronic
formats,
etc.)
Provides free language services to people whose primary language
is not English, such as: o Qualified interpreters o Information
written in other languages
If you need these services, contact our Civil Rights
Coordinator: Stacey Bonn If you believe that Delta Dental of
Illinois has failed to provide these services or discriminated in
another way on the basis of race, color, national origin, age,
disability, gender, or gender identity, you can file a grievance
with: Director of Client Services Delta Dental of Illinois 111
Shuman Boulevard Naperville IL 60563 Phone: 800-323-1743 Email:
[email protected] You can file a grievance in person or by
mail, phone or email. If you need help filing a grievance, our
Director of Client Services is available to help you. You can also
file a civil rights complaint with the U.S. Department of Health
and Human Services, Office for Civil Rights, electronically through
the Office for Civil Rights Complaint Portal, available at
https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone
at: U.S. Department of Health and Human Services 200 Independence
Avenue, SW Room 509F, HHH Building Washington, D.C. 20201
1-800-368-1019, 800-537-7697 (TDD) Complaint forms are available at
http://hhs.gov/ocr/office/file/index.html
mailto:[email protected]://ocrportal.hhs.gov/ocr/portal/lobby.jsfhttp://hhs.gov/ocr/office/file/index.html
-
Arabic
ي عرب . ملحوظة: إذا كنت تتحدث اذكر اللغة، فإن خدمات المساعدة
اللغوية تتوافر لك بالمجان. اتصل برقم ةال
Chinese
繁體中文
注意:如果您使用繁體中文,您可以免費獲得語言援助服務。請致電 1-800-323-1743。
French
Français
ATTENTION : Si vous parlez français, des services d'aide
linguistique vous sont proposés gratuitement. Appelez le
1-800-323-1743. German
Deutsch
ACHTUNG: Wenn Sie Deutsch sprechen, stehen Ihnen kostenlos
sprachliche Hilfsdienstleistungen zur Verfügung.
Rufnummer: 1-800-323-1743. Greek
Ελληνικά ΠΡΟΣΟΧΗ: Αν μιλάτε ελληνικά, στη διάθεσή σας βρίσκονται
υπηρεσίες γλωσσικής υποστήριξης, οι οποίες παρέχονται
δωρεάν. Καλέστε 1-800-323-1743. Gujarati
ગજુરાતી
સુચના: જો તમે ગજુરાતી બોલતા હો, તો નન:શુલ્ક ભાષા સહાય સેવાઓ
તમારા માટે ઉપલબ્ધ છે. ફોન કરો 1-800-323-1743. Hindi
हिंदी
ध्यान दें: यदि आप हिंदी बोलते है ंतो आपके लिए मुफ्त में भाषा
सहायता सेवाएं उपलब्ध हैं। 1-800-323-1743 पर कॉल करंे। Italian
Italiano
ATTENZIONE: In caso la lingua parlata sia l'italiano, sono
disponibili servizi di assistenza linguistica gratuiti. Chiamare
il
numero 1-800-323-1743. Korean
한국어
주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 1-800-323-1743
번으로 전화해
주십시오.
Polski
Polski
UWAGA: Jeżeli mówisz po polsku, możesz skorzystać z bezpłatnej
pomocy językowej. Zadzwoń pod numer 1-800-323-1743. Russian
Русский
ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны
бесплатные услуги перевода. Звоните 1-800-323-1743. Spanish
Español
ATENCIÓN: Si habla español, tiene a su disposición servicios
gratuitos de asistencia lingüística. Llame al 1-800-323-1743.
Tagalog
Tagalog
PAUNAWA: Kung nagsasalita ka ng Tagalog, maaari kang gumamit ng
mga serbisyo ng tulong sa wika nang walang bayad.
Tumawag sa 1-800-323-1743. Urdu
وارد
خبردار: اگر آپ اردو بولتے ہیں، تو آپ کو زبان کی مدد کی خدمات مفت
میں دستیاب ہیں ۔ کال
کريں .1-800-323-1743 Vietnamese
Tiếng Việt
CHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ
miễn phí dành cho bạn. Gọi số 1-800-323-1743.
.1-800-323-1743
If you or someone you are helping has questions about Delta
Dental of Illinois,you have the right to get help and information
in your language at no cost.
1: Check Box1: Off Check Box2: Off
3: Primary Payer Name: Primary Payer Address:
4: Primary Subscriber Name and Address:
5: DOB:
6: Check Box1: Off Check Box2: Off
7: SSN:
8: Plan No:
9: Employer Name:
10: Check Box1: Off Check Box2: Off Check Box3: Off Check Box4:
Off
11: Check Box1: Off Check Box2: Off
12: Name and Address:
13: DOB:
14: Check Box1: Off Check Box2: Off
15: Patient ID:
Other Coverage: 16: Check Box1: Off Check Box2: Off
17: Subscriber Name:
18: DOB:
19: Check Box1: Off Check Box2: Off
20: SSN:
21: Plan/Group Number:
22: Check Box1: Off Check Box2: Off Check Box3: Off Check Box4:
Off
23: Other Carrier Name: Other Carrier Address:
24: Procedure Date1: Procedure Date2: Procedure Date3: Procedure
Date4: Procedure Date5: Procedure Date6: Procedure Date7: Procedure
Date8: Procedure Date9: Procedure Date10:
25: Area of Oral Cavity1: Area of Oral Cavity2: Area of Oral
Cavity3: Area of Oral Cavity4: Area of Oral Cavity5: Area of Oral
Cavity6: Area of Oral Cavity7: Area of Oral Cavity8: Area of Oral
Cavity9: Area of Oral Cavity10:
26: Tooth System1: Tooth System2: Tooth System3: Tooth System4:
Tooth System5: Tooth System6: Tooth System7: Tooth System8: Tooth
System9: Tooth System10:
27: Tooth Number1: Tooth Number2: Tooth Number3: Tooth Number4:
Tooth Number5: Tooth Number6: Tooth Number7: Tooth Number8: Tooth
Number9: Tooth Number10:
28: Tooth Surface1: Tooth Surface2: Tooth Surface3: Tooth
Surface4: Tooth Surface5: Tooth Surface6: Tooth Surface7: Tooth
Surface8: Tooth Surface9: Tooth Surface10:
29: Procedure Code1: Procedure Code2: Procedure Code3: Procedure
Code4: Procedure Code5: Procedure Code6: Procedure Code7: Procedure
Code8: Procedure Code9: Procedure Code10:
29a: Diag Pointer1: Diag Pointer2: Diag Pointer3: Diag Pointer4:
Diag Pointer5: Diag Pointer6: Diag Pointer7: Diag Pointer8: Diag
Pointer9: Diag Pointer10:
30 Description1: 31: Fee1000-1: Fee100-1: Fee10-1: Fee1000-2:
Fee100-2: Fee10-2: Fee1000-3: Fee100-3: Fee10-3: Fee1000-4:
Fee100-4: Fee10-4: Fee1000-5: Fee100-5: Fee10-5: Fee1000-6:
Fee100-6: Fee10-6: Fee1000-7: Fee100-7: Fee10-7: Fee1000-8:
Fee100-8: Fee10-8: Fee1000-9: Fee100-9: Fee10-9: Fee1000-10:
Fee100-10: Fee10-10:
30 Description2: 30 Description3: 30 Description4: 30
Description5: 30 Description6: 30 Description7: 30 Description8: 30
Description9: 30 Description10: 31a: Other Fees1000-1: Other
Fees100-1: Other Fees10-1:
32: Total Fee1000-1: Total Fee100-1: Total Fee10-1:
33: Missing Teeth1: Missing Teeth2: Missing Teeth3: Missing
Teeth4: Missing Teeth5: Missing Teeth6: Missing Teeth7: Missing
Teeth8: Missing Teeth9: Missing Teeth10: Missing Teeth11: Missing
Teeth12: Missing Teeth13: Missing Teeth14: Missing Teeth15: Missing
Teeth16: Missing Teeth17: Missing Teeth18: Missing Teeth19: Missing
Teeth20: Missing Teeth21: Missing Teeth22: Missing Teeth23: Missing
Teeth24: Missing Teeth25: Missing Teeth26: Missing Teeth27: Missing
Teeth28: Missing Teeth29: Missing Teeth30: Missing Teeth31: Missing
Teet32: Missing TeethA: Missing TeethB: Missing TeethC: Missing
TeethD: Missing TeethE: Missing TeethF: Missing TeethG: Missing
TeethH: Missing TeethI: Missing TeethJ: Missing TeethK: Missing
TeethL: Missing TeethM: Missing TeethN: Missing TeethO: Missing
TeethP: Missing TeethQ: Missing TeethR: Missing TeethS: Missing
TeethT:
34: Diag: Code1: Code2:
34a: Diag: CodeA: CodeB: CodeC: CodeD:
35: Remarks: Date:
37: Date:
38: Check Box1: Off Check Box2: Off Check Box3: Off Check Box4:
Off
39: Number of Enclosures1: Number of Enclosures2: Number of
Enclosures3:
40: Check Box1: Off Check Box2: Off
41: Date:
43: Check Box1: Off Check Box2: Off
44: Date:
45: Check Box1: Off Check Box2: Off Check Box3: Off
46: Date:
47: State:
48: Name: Address:
49: NPI:
50: License No:
51: SSN:
52: Area code: Ph No1: Ph No2:
52a: Additional Provider ID:
53: Date:
54: NPI:
55: License No:
56: Address: City, State Zip:
56a: Provider Specialty Code:
57: Area code: Ph No1: Ph No2:
58: Additional Provider ID: