Embed Size (px)
Citation preview

HEADACHESWESTERN CLINICAL SCIENCES
SIOM-SPRING 2012
Dr. Alex

HEADACHES:WHERE ARE WE GOING WITH
THIS TODAY?• We will discuss the most common types of
headaches, how to differentiate them, common clinical characteristics, what is believed to cause each type, and Western treatment options.
• We will review danger signs needing referral.• We will review some physical exam components
that are helpful in evaluating a patient with headache.
• We will briefly review commonly used pharmaceuticals and herbals used in treating and preventing headaches.

COMMON TYPES OF HEADACHES
• MIGRAINE• TENSION-TYPE• CLUSTER• MEDICATION OVERUSE
– (AKA REBOUND HEADACHE)
• POST-TRAUMATIC• SINUS

MIGRAINE HEADACHE
• 17% of women, 6% of men (3x more common in women)
• Classically, presents as episodic unilateral (70%) head pain with gradual onset, crescendo, pulsating, mod-severe pain, dull, deep, steady, aggravated by activity, associated with nausea, vomiting, photophobia, phonophobia, may have preceding aura, lasts 4-72 hrs.
• Migraine sufferers prefer to rest in a dark, quiet place.

MIGRAINE HEADACHE
• Migraine can be with aura, without aura, or migraine variants (ophthalmic, e.g.)
• What is an aura? A progressive neurologic deficit or disturbance with subsequent complete recovery typically before the onset of the headache. Most auras resolve in less than an hour. Usually the headache starts within an hour of the aura resolving.
• Common auras: visual (zig-zags in visual field, spots), loss of sensation in arm or face, speech slurring, focal motor weakness. Can be confused as a stroke or TIA.


MIGRAINE HEADACHE
• What causes migraines?• Used to believe it was a “vascular headache”,
but now we understand more.• Genetic component/threshold• Neuronal dysfunction that initiates an event in
the brainstem that is self-propagating wave of neuronal depolarization that spreads across the cerebral cortex, causing “neurogenic inflammation” of the meninges
• May involve serotonin as well as substance P and vasoactive peptides

MIGRAINE HEADACHE
• TREATMENT OPTIONS:– PREVENTIVE (LIFESTYLE)– ABORTIVE– PROPHYLACTIC

MIGRAINE HEADACHE• MIGRAINE TRIGGERS:
– DIET: alcohol, chocolate, aged cheeses, MSG, Nutrasweet, caffeine, nuts, nitrates, anything a person is allergic or sensitive to
– HORMONES: menses (due to declining estrogen), ovulation, progesterone (BCP)
– SENSORY STIMULI: strong light, odors, sounds, flickering lights
– STRESS: let-down periods, times of intense activity, loss or change (divorce, job change)
– ENVT CHANGE: weather, travel, seasons, altitude, sleep patterns, dieting, skipping meals, irreg physical activity, schedule changes

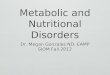
Headache diary
Reproduced with permission from Bristol-Myers Squibb Company. Copyright 2001 Bristol-Myers Squibb Company.

MIGRAINE HEADACHE
• PREVENTIVE TX:– Avoid triggers– Regular exercise– Relaxation– Biofeedback– Massage– Physical therapy– Acupuncture– Chiropractic/osteopathic manipulations– Hypnosis– TENS (transcutaneous electrical nerve stimulator)

MIGRAINE HEADACHE
• ABORTIVE TREATMENT– NSAIDs– Tylenol (caution: can cause rebound!)– Excedrin (Tylenol, aspirin, caffeine)– Triptans: (Imitrex, Maxalt, Amerge, Frova, Zomig)
migraine-specific medications that inhibit the release of vasoactive peptides, promote vasoconstriction, block pain pathways in the brainstem. Use early in HA. Not used in patients with CAD, CVA, pregnancy, uncontrolled HTN. Can cause chest pressure, flushing, dizziness, paresthesias, drowsiness/malaise). SC, PO, NS. $15-54/attack
– Anti-nausea meds– Combos

MIGRAINE HEADACHE
• PROPHYLACTIC TREATMENT– Calcium-channel blockers– Tricyclic antidepressants– Beta blockers– SSRIs– Anti-seizure medications: valproic acid (Dilantin),
topiramate (Topamax), gabapentin (Neurontin)– Bo-Tox injections– Magnesium 500mg/day

MIGRAINE HEADACHE
• OTHER PROPHYLACTIC POSSIBILITIES– Butterbur (75 mg/day): may cause GI upset– CoEnzymeQ10 (100mg 3x/day)– Feverfew– Riboflavin (400 mg/day)

TENSION-TYPE HEADACHE
• Most common type of headache• Pressure/tightness all over head bilaterally (vice-grip)• Waxes and wanes over time in intensity• Duration is variable• Usually does not have associated migraine features
(N/V/light and sound sens/aura)• We used to think this type of headache was due to
contraction/hypertonicity of muscles of head and skull. It is now viewed as a migraine variant and has similar pathophysiology to migraine but is more mild.

TENSION-TYPE HEADACHE
• Primary treatment includes stress management, psychotherapy and support, relaxation, biofeedback, Tylenol, aspirin, and NSAIDs.
• If they occur frequently, suspect medication overuse HA, discuss pain management and coping skills, and consider prophylactic meds (tricyclic antidepressants).

CLUSTER HEADACHE
• Repetitive headaches that occur for weeks to months at a time, followed by periods of remission.
• Not common: <1% of population• Men>Women• Age onset 25-50 yo

CLUSTER HEADACHE
• Clinical features:– Unilateral– Begins suddenly without warning and reaches max
intensity in a few minutes– Deep, excruciating, continuous, explosive– Usu begins in or around the eye or temple– Lasts 15 min-3 hours– Ipsilateral tearing, eye redness, runny nose,
sweating, pallor. N/V may occur, photophobia on affected side.
– Patient is usually pacing, restless due to pain

CLUSTER HEADACHE
• Episodic: 1-3 attacks/day over 6-12 weeks followed by 6-12 months of remission
• Usually begin between 9pm-9am and tend to recur at about the same time of day each day.
• >50% of patients report alcohol as trigger

CLUSTER HEADACHE
• What causes cluster headaches???• Vasodilation, extracerebral neuronal
dysfunction, hypothalamus, genetics, tobacco, alcohol…
• How do we treat cluster headaches???• 100% O2 (oxygen!), triptans can be used• Prophylactic meds: Calcium channel
blockers, Lithium, prednisone, seizure meds

MEDICATION OVERUSE HEADACHE
• 1% of population (women>men)• Most commonly involves Tylenol, Fiorinal
(butalbital-aspirin-caffeine), aspirin, but can also involve NSAIDs, narcotics
• Continuous analgesic exposure causes tolerance which results in mini-withdrawals
• Moral of the story: Acute medications should be limited to <10 days/month!

POST-TRAUMATIC HEADACHE
• Usually begins within 7 days after a head trauma
• Tension type headache character is the most common
• Beware of danger signs for a intracranial bleed (more to come on the danger signs)

SINUS HEADACHE
• Overdiagnosed!!! Migraine sufferers, cluster headache patients can have stuffy nose, sinus pressure/pain…
• Really need pussy discharge in nose to diagnose. Facial pain/congestion/fullness, nasal obstruction, fever, loss of smell to make the diagnosis of a sinusitis-related headache.
• A true sinus headache is treated with nasal irrigation, nasal sprays, antibiotics

SO HOW DO YOU TELL ONE TYPE OF HEADACHE FROM
ANOTHER?• 1. How often do you get severe/disabling
headaches? (sensitive for migraine)• 2. How often do you get other (milder)
headaches?• 3. How often do you take HA relievers or pain
pills? (med overuse? If uses meds>3 days/week &/or have daily headaches)
• 4. Has there been any recent change in your headaches? (ID pts with important secondary causes)

SO HOW DO YOU TELL ONE TYPE OF HEADACHE FROM
ANOTHER?• Historical clues: age at onset, aura?,
freq/intensity/duration, #HA days/mo, time and mode of onset, quality of pain, location of pain, radiation, associated symptoms, family history of migraine, things that make HA better and worse, effect of activity on HA, relationship with food/alcohol, response to any prior Tx, visual changes, recent trauma, recent changes in sleep/exercise/diet, change in work/lifestyle, change in meds/BCP, envtl factors, menses

OTHER CAUSES OF HEADACHES
• Stress/anxiety/depression• Cervical spine disease• Intracerebral mass (cancer, noncancerous mass,
abscess, blood)• Fever• Vascular lesion (aneurysm, AVM)• Acute hypertensive emergency• Infection-meningitis, encephalitits• Benign intracranial hypertension• Glaucoma• Metabolic disturbance (sugar, electrolytes)

HEADACHE DANGER SIGNS
• Sudden onset or severe persistent HA that reaches max intensity within a few seconds or minutes
• Absence of similar HAs in the past (“first” or “worst headache of my life”)
• Worsening pattern of HA (mass, med overuse, hematoma)
• Focal neurologic symptoms (mass, AVM)• Fever assoc with HA

HEADACHE DANGER SIGNS
• Any change in mental status, personality, fluctuation in level of consciousness.
• Rapid onset with strenuous exercise, esp after minor trauma
• New HA in pts <5 yo or >50 yo• New HA type in pt with cancer• New HA type in pt with HIV• HA during pregnancy

PHYSICAL EXAM
• BP/Pulse• Neuro exam: getting up from seated
position, toes/heels walk, gait, Romberg, motor, sensory, coordination, cranial nerves.
• Danger signs on exam: meningismus, focal neurologic signs, papilledema
• Almost all HA patients will have a normal neuro exam



IMAGING
• It is a clinical decision as to which HA patients a doctor will request a CT or MRI of the head.
• In general, if a patient has a significant change in the pattern, frequency, severity of HA, progressive worsening, focal neuro signs, HA causing awakening from sleep, onset of HA >50 years old, HA after trauma CT of head.

BEFORE THIS GIVES YOU A HEADACHE, LET’S TAKE A
BREAK

SEIZURE DISORDERSWESTERN CLINICAL SCIENCES
SIOM-SPRING 2012
Dr. Alex

WHAT’S IN STORE…
• WHAT ARE SEIZURES?• WHAT CAUSES SEIZURES?• TYPES OF SEIZURES• HISTORICAL CLUES• DIAGNOSIS• TREATMENT• WHAT TO DO WHEN SOMEONE HAS A
SEIZURE

WHAT ARE SEIZURES?
– Uncoordinated electrical discharges in the cerebral cortex
– Due to either the overactivity of excitatory neurotransmitters or the underactivity of inhibitor neurotransmitters
– Epilepsy is the term used to describe people who have recurrent seizures for any of a number of reasons. Over half of people with epilepsy, though, have no known cause.
– Seizures are depicted in prehistoric cave paintings, referred to by Hippocrates and in the Bible.
– 5-8/1000 people have seizure disorder

GENERAL SEIZURE TYPES
• Epileptic seizures have typical neurophysiological changes which can be identified on electroencephalogram (EEG).
• Then there are nonepileptic seizures that do not have these typical features and are more likely to be due to an acute metabolic change or hypoxemia.

EPILEPTIC SEIZURESCAUSES
• Genetics• Congenital brain
malformations• Inborn errors of
metabolism• High fevers• Head trauma• Brain tumors• Stroke
• Intracranial infection• Cerebral degeneration• Drug withdrawal• Drug reactions

NONEPILEPTIC PHYSIOLOGIC SEIZURESCAUSES
• Hyperthyroid• Hypoglycemia• Hyperglycemia• Hyponatremia• Hypoxia
– Resp/cardiac arrest– Carbon monoxide– Drowning– Anesthesia– Syncope/fainting
• Uremia• Transient ischemic
attack• Cardiac arrythmias

TYPES OF SEIZURES
• Partial (only part of the cortex disrupted)– Simple (consciousness not impaired)– Complex (with impairment of consciousness)
• Generalized (begins affecting the whole cortex at one time)– Nonconvulsive: Absence– Convulsive: Myoclonic, Clonic, Tonic, Tonic-
Clonic, Atonic

SIMPLE PARTIAL SEIZURES
• With motor symptoms– Focal motor– Phonatory
• With somatosensory symptoms– Visual– Auditory– Olfactory– Gustatory– Vertiginous
• With psychic symptoms– Dysphasic– Cognitive– Déjà vu– Affective (fear)– Hallucinations

COMPLEX PARTIAL SEIZURES
• Most common type of seizure among adult epileptics.
• Usually last < 3 minutes• Person appears awake but not responsive
and has no memory of the seizure at all.• Staring, grimacing, lip smacking, plucking
at clothes, gesturing, chewing, snapping fingers, walking, running, undressing

GENERALIZED SEIZURES
• Nonconvulsive– Absence: occurs almost exclusively in kids. Last 5-10
sec only. Staring and unresponsiveness, sometimes some repetitive behaviors.
• Convulsive– Myoclonic: sudden brief muscle contractions, singly
or in clusters. Frequently just the arms.– Clonic: Rhythmic jerking of muscles, frequently
affecting arms, neck, face.– Tonic: Muscle stiffening only– Atonic: “drop attacks” sudden loss of muscle tone of
the legs fall.– Tonic-Clonic: gets all the attention, dramatic

GENERALIZED TONIC-CLONIC SEIZURE
• Frequently preceeded by an aura, or technically a simple partial seizure, when the seizure begins and the person is still awake to notice smell, visual symptoms, feelings.
• Then the seizure begins with a tonic phase (10-20 sec): loss of consciousness, loss of posture, flex arms, eyes deviate up, extend back/neck/arms/legs, involuntary noises, shallow resp (cyanosis), tremors begin…
• Clonic phase (30-90 sec): brief violent generalized flexor contractions alternating with progressively longer muscle relaxation.

GENERALIZED TONIC-CLONIC SEIZURE
• During clonic phase, there may be cyanosis, cheek or tongue biting (no tongue swallowing!), salivation (may be bloody), loss of bladder or bowel control, and then ends with a deep inspiration and sustained muscle relaxation.
• After the seizure, there is a post-ictal period during which the person may be confused, have no memory, headache, muscles sore, fatigue/exhaustion, embarrassment, trouble talking, frustration or anger, weakness, fear, depression, lonliness, nausea, thirst…

WHEN TALKING TO SOMEONE ABOUT THEIR SEIZURES
• Most people know seizure triggers (lowers threshold): strong emotions, loud music, flashing lights, fever, menses, lack of sleep, stress, intense exercise.
• Most true seizures will have some post-ictal period.
• Medications• Past medical history (head injury, Alzheimer’s,
stroke, intracranial infection, substance abuse)• FamHx

SEIZURE DIAGNOSIS
• Made by history given by patient and witnesses.
• Blood work done to rule out physiologic causes
• EEG• MRI to rule out other causes

SEIZURE TREATMENT
• Antiseizure medications are begun when it is believed that the person is likely to continue to have seizures.
• Drugs block the sodium or calcium channels in the nerve cells to inhibit the electrical activity that stimulates the seizure. There are also medications used that affect GABA metabolism (an inhibitory neurotransmitter).

SEIZURE TREATMENT
• Seizure diary to discover triggers.• Psychosocial issues related to loss of
independence, employment, insurance, ability to drive, and self-esteem.
• In Washington state, you can drive if you have not had a seizure for 6 months. The doctor who makes the driving recommendation is liable.

WHAT TO DO WHEN SOMEONE HAS A SEIZURE
• It is very scary to see, but it is important to try to stay calm.
• Protect the person from injury by removing harmful objects from nearby
• Look for any ID/jewelry that identifies the person as an epileptic.
• Cushion the head• Aid in breathing by gently placing them on their sides
when seizure is done.• Reassure calmly and tell them what just happened and
where they are.• Stay with the person until the recovery is complete.

WHAT TO DO WHEN SOMEONE HAS A SEIZURE
• DON’T…• Restrain the person in any way• Put anything in their mouths• Try to move the person• Give them any food or drink until fully
recovered• Attempt to bring them around• Yell at them or get angry with them

WHAT TO DO WHEN SOMEONE HAS A SEIZURE
• CALL 911 IF….• You think it may be the person’s first
seizure• Seizure lasts more than 5 minutes• One seizure follows another without
regaining consciousness between.• The person is injured during the seizure.• (It is OK if the person turns blue during the
seizure)

PERIPHERAL NEUROPATHY

PERIPHERAL NERVOUS SYSTEM
• Everything except the brain and spinal cord
• Takes messages from the brain out into the body.
• Motor• Sensory• Autonomic (sweat glands, blood vesssels,
digestion, bowel and bladder, sexual function)

NEUROPATHY
• Nonspecific term meaning damage to nerves.
• Damage occurs due to lack of blood flow and therefore lack of oxygen supply
• In the PNS, symptoms can be due to damage of motor/sensory/autonomic nerves causing a variety of symptoms.
• Symptoms usually begin gradually over time

NEUROPATHY
• Pain
• Numbness
• Tingling
• Weakness
• Burning
• Loss of feeling
• Sensation that you are wearing socks or gloves
• Nausea/vomiting
• Diarrhea or constipation
• Sharp/jabbing pain• Electric pain• Incontinence of bladder or
bowel• Extreme sensitivity to light
touch• Lack of coordination• Sexual dysfunction• Low blood pressure• Sweating

NEUROPATHY-CAUSES
• Trauma/repetitive use (carpel tunnel)
• Diabetes (50%)• Alcoholism• Vitamin deficiency• HIV• Autoimmune disease• Hypothyroidism
• Medications (chemo, HIV meds)
• Toxins (heavy metals)• Genetics

NEUROPATHY-DIAGNOSIS
• Neurologic examination• Labs: vitamin levels, TSH• Nerve conduction study• Nerve biopsy

NEUROPATHY-TREATMENT
• Depends on the cause• Control sugars if from diabetes• Supplement vitamins if deficient• Treat autoimmune disease• Discontinue offending activity if due to
mechanical irritation• Discontinue offending med or toxic
exposure

NEUROPATHY-TREATMENT
• Tylenol/NSAIDs/Aspirin for pain• Anti-seizure medications (Neurontin,
carbamazapine, phenytoin) dizzy, drowsy• Lidocaine patch• Tricyclic antidepressants/SSRIs• Codeine/narcotics• TENS• Biofeedback• Acupuncture• Hypnosis• Relaxation Techniques

TENS

NEUROPATHY-COMPLICATIONS
• Foot ulcers/gangrene• N/V/bloating (gastroparesis)• Impotence• Incontinence of urine or stool• Hypotension• Sweating or lack of sweating


THAT’LL WRAP THIS UP!