Embed Size (px)
Citation preview

Headaches,Posture,
CervicalSpine& the
ShoulderGirdle

Firstthingsfirst!• Letusdoaquickposturalscanofeachother;with“quick”beingtheoperativeword!
• Wewillfocusontheorientationofthe:– Head– Neck– ShoulderGirdle– UpperThoracicSpine&associatedribs– withaquickpeekatthelow-backandhips.


QuickReviewofAnatomy
• Boneyandarticularstructures:-– Oftheshoulder-girdle andcervicalareas.
• Acommonpattern:- UpperXSyndrome– (meantasoneexampleofnumerousposturalpatternsfoundinHeadache&Migraineclients)
• Musculature:-


http://www.shoulderdoc.co.uk/images/uploaded/glenoid.jpg

http://www.shoulderdoc.co.uk/images/uploaded/glenoid.jpg

http://www.shoulderdoc.co.uk/images/uploaded/glenoid.jpg

http://www.shoulderdoc.co.uk/images/uploaded/glenoid.jpg

http://www.youtube.com/watch?v=VdaY775JGX4&feature=player_embedded
You-Tubevideo:MovementsoftheShoulder
https://youtu.be/BrItOoELlZg

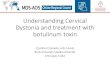
Observations&Inspection :UpperCrossSyndrome
TightmusculatureWeakmusculatureWeak TightDeepflexors Sub-occipitalsoftheneck UpperTrapezium&Levator
ScapulaeRhomboids SCM&ScalenesInfraspinatus TeresmajorandLatissimus&Teresminor DorsiMiddleand PectoralisMajor&MinorlowerTrapezium SerratusAnterior
N.B.TautversesTightandPalpation

Occiput is extended;The Upper Cervical Spine (the OA jt. & C2) are held in extension, while the lower cervical spine and upper thoracic are held Flexed.Chin moves forward
into protrusion.
Shoulder rolls forward, oris protracted. Kyphosis will begin
to exaggerate.Thoracic Kyphosis exaggerates and themusculature & posterior ligaments are stretched.
Resultsin:

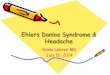
Traumassuchaswhiplashinjuriescanresultinother
posturaldeviations:


http://img.medscape.com/pi/features/slideshow-slide/c-spine/fig2.jpg

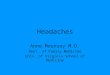
SomeConsequences:-I would like to suggest, for our purposes, that there are five major areas where postural & muscle balance issues “come home to roost” and precipitate the majority of headaches, migraines and just plain cervical pain experienced by so many of our clients. Each of these 5 have specific ways of being assessed and treated:• Head, Face & Jaw (TMJ)• Occipital-Atlanto-Axial joints (O-C1-C2)• The Cervical lordosis – C3-4-5• The Cervico-Thoracic area, C6 to T4/5• The Shoulder Girdle (the “base” for the 4 above)

ProgressionofTreatment.
Thesefiveareasarechosentohelporganizetheinformationgiventhroughoutthisworkshop.Thisisespeciallytruefortheprogressionoftreatment:• Startingwiththeshouldergirdleasour“general”– “peripheral”approach.
• Wewillthenprogressthroughthecervicothoracicarea,tomid-cervical,upintothespecializedsub-occipitalarea(O-C1-C2),andthenaddressthehead/cranium-face-jaw

Stop!Please!NoMore!!!

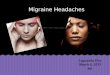
GeneralMusculatureinvolved:



http://www.shoulderdoc.co.uk/images/uploaded/interscapular_pain_2a.jpg
T4syndrome,ormoreaccurately“upperthoracicsyndrome”,isarareandperhapsunder-recognizedclinicalentitythatwarrantsattention.Upperthoracicsyndromeisbasedonthepremisethatdysfunctionofthejointsinthethoracicspine(includingtheintervertebral/zygaphophseal,costovertebralandcostotransvere joints)canreferpainandparaesthesiatotheupperlimbsandthehands.AssympatheticoutflowtotheupperlimbissuppliedbylevelsT2-5,thesympatheticnervoussystemcouldprovideapathwayforreferralfromthethoracicspinetotheupperlimb.Thissyndromeis3timesmorecommoninwomenthanmen

• Althoughthissyndromeispoorlydefinedintheliterature,theclusterofsymptomsreportedinT4/Upperthoracicsyndromeinclude:
• •Subjectivereportsofparasthesia,alteredandextremetemperatureperceptionand“puffiness”intheglovedistributionofbothhands
• •Ahistory,orcurrentcomplaintofintermittentposteriorthoracicpainorpainaroundthescapularegion
• •Symptomsworselastthingatnightorwithactivitiesinvolvingthoracicflexion/slumping(e.g sittingatacomputer/deskforlongperiods,layingwithpillowsunderyourhead)
• •Positionofmostcomforttendstobelayingcompletelyflat(supine)
• Objectiveassessmentfindingsinclude:• 1.Increasedcervicallordosisandcervico-thoracickyphosis• 2.Flattenedupperthoracicspine(T2-7)• 3.Minimalthoracicmovementduringsinglearmelevationtoeitherside• 4.Notablerestrictioninupperthoracicmovement• 5.Localtendernessandsymptomsreproducedwithmobilisationofthespine
anywherebetweenlevelsT2-7(historicallyincludingT4)• 6.Localhypomobility ofthevertebralsegmentassociatedwithsymptoms• 7.Positiveupperlimbtensiontests,oftenlimitedonbothsidesbypainacross
upperthoracicspine• 8.Positiveslumptest

• References• 1.Bialosky,J.E.,Bishop,M.D.,Price,D.D.,Robinson,M.E.,andGeorge,S.Z.(2009)The
mechanismsofmanualtherapyinthetreatmentofmusculoskeletalpain:acomprehensivemodel.ManualTherapy,Vol.14,pp.531-538
• 2.Bodduk,N.(2002)Innervationandpainpatternsofthethoracicspine.In:Physicaltherapyofthecervicalandthoracicspineed GrantR.ClinicsinPhysicalTherapy,Vol.17,3rded,ChurchillLivingstone,pp.73-81
• 3.Conroy,J.L.,andScneiders,A.G.(2005)TheT4syndrome.ManualTherapy,Vol 10,no.4,pp.292-296
• 4.Crawford,H.J.,andJull,G.A,(1993)Theinfluenceofthoracicpostureandmovementonrangeofarmelevation.Physiotherapy,Vol.9,pp.143-148
• 5.Edmondson,S.J.,andSinger,K.P.(1997)Thoracicspine:anatomicalandbiomechanicalconsiderationsformanualtherapy.ManualTherapy,Vol,2,no.3,pp.132-143
• 6.Evans,P.(1997)TheT4syndrome:somebasicscienceaspects.Physiotherapy,Vol.83,no.4,pp.187-189
• 7.Fruth,S.J.(2006)Differentialdiagnosisandtreatmentinapatientwithposteriorupperthoracicpain.PhysicalTherapy,Vol.86,no.2.,pp.254-268
• 8.Maitland,G.,Hengeveld,E.,Banks,K.andEngland,K.(2005)Maitland’svertebrall manipulation.7thed.Edinburgh:ButterworthHeinemann
• 9.Jowsey,P.,andPerry,J.(2010)SympatheticnervoussystemeffectsinthehandsfollowingagradeIIIposter-anteriorrotatorymobilisationtechniquetoT4:arandomisedcontroltrial.ManualTherapy,Vol.15,pp.248-253
• 10.Watson,L.A.,Pizzari,T.,andBalster.S.(2009)Thoracicoutletsyndromepart1:clinicalmanifestations,differentiationandtreatmentpathways.ManualTherapy,Vol.14,pp.586-595



http://www.backpain-guide.com/Chapter_Fig_folders/Ch05_Anatomy_Folder/Ch5_Images/05-3_C1_and_C2.jpg