Embed Size (px)
Citation preview

HEAD TRAUMAHEAD TRAUMA
WWW.FISIOKINESITERAPIA.BIZ

ObjectivesObjectivesDescribe the Describe the pathophysiologypathophysiology of traumatic of traumatic brain injurybrain injuryDiscuss the Discuss the scientific rationalescientific rationale for the for the therapeutic interventions used in the care therapeutic interventions used in the care of brain injured of brain injured Provide Provide research based recommendationsresearch based recommendationsfor the care of patient with traumatic brain for the care of patient with traumatic brain injuryinjury

Rhoads & Pflanzer (1996) Human Physiology p. 211

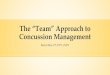
Layers of the Cranial Vault
Anatomy of the Brain www.neurosurgery.org/pubpgages/patres/anatofbrain.html#micro

Definition Definition –– Traumatic Brain Traumatic Brain InjuryInjury
Traumatic brain injury (TBI) is a nondegenerative, noncongenital insult to the
brain from an external mechanical force, possibly leading to permanent or temporary
impairments of cognitive, physical, and psychosocial functions with an associated
diminished or altered state of consciousness

Annually in the USAnnually in the US……1.5 million Americans sustain a TBI each year1.5 million Americans sustain a TBI each year80,000 people annually experience the onset of 80,000 people annually experience the onset of longlong--term disability following TBIterm disability following TBI50,000 people die every year as a result of TBI50,000 people die every year as a result of TBIIncidents of TBI outnumber Breast Cancer Incidents of TBI outnumber Breast Cancer (175,000), Spinal Cord Injury (11,000), HIV/AIDS (175,000), Spinal Cord Injury (11,000), HIV/AIDS (16,273), Multiple Sclerosis (10,400)(16,273), Multiple Sclerosis (10,400)5.3 million Americans live with TBI5.3 million Americans live with TBI--related related disabilitiesdisabilities

Cause of death in 25% of trauma patientsCause of death in 50% of MVCsSignificant long term disabilityPrompt recognition and treatment can improve outcomeAll patients with head or facial trauma have c-spine injury until proven otherwise!
Head InjuryHead Injury

Cost of TBICost of TBI
Survivor typically faces Survivor typically faces 55--10 years of intensive 10 years of intensive services services –– estimated estimated cost of $4 million/yearcost of $4 million/yearEconomic cost of TBI Economic cost of TBI in US estimated $48 in US estimated $48 billion/yearbillion/year

Types of Types of TBIsTBIsClosed Head InjuryClosed Head Injury
Acceleration/DecelerationAcceleration/DecelerationIf a moving object hits a movable If a moving object hits a movable head (e.g., head gets hit with a bat).head (e.g., head gets hit with a bat).If a moving head hits something If a moving head hits something stationary (e.g., if you have a car stationary (e.g., if you have a car wreck and your head hits the wreck and your head hits the dashboard).dashboard).Shaken type of movement (e.g., Shaken type of movement (e.g., Shaken Baby Syndrome when head Shaken Baby Syndrome when head rocks back and forth in skull).rocks back and forth in skull).Two types are:Two types are:
–– LinearLinear-- brain moves straight along brain moves straight along a linear path.a linear path.
–– AngularAngular-- Brain rotates at an angle, Brain rotates at an angle, twists, or rolls.twists, or rolls.
NonNon--AccelerationAcceleration–– Much more rare, referred to as a Much more rare, referred to as a
crushing injurycrushing injury–– If a moving object hits a head that is fixed If a moving object hits a head that is fixed
(e.g., car falls on head while you(e.g., car falls on head while you’’re re working under it).working under it).
((FerrandFerrand and Bloom, 111and Bloom, 111--112)112)

Types of Types of TBIsTBIsPenetrating/Closed Head InjuryPenetrating/Closed Head Injury
Low VelocityLow Velocity–– Skull is no longer in tact, part of Skull is no longer in tact, part of
skull or debri gets into the brain skull or debri gets into the brain ((FerrandFerrand and Bloom).and Bloom).
–– An example is if you get hit so An example is if you get hit so hard with a baseball that it hard with a baseball that it breaks skull and causes part of breaks skull and causes part of it to lay on the brain.it to lay on the brain.
High VelocityHigh Velocity–– Skull is no longer in tact, part of Skull is no longer in tact, part of
skull or debri gets into the brain skull or debri gets into the brain ((FerrandFerrand and Bloom).and Bloom).
–– An example is if during a gun An example is if during a gun shot wound the bullet shot wound the bullet penetrates the skull and goes penetrates the skull and goes into the brain matter.into the brain matter.
((FerrandFerrand and Bloom, 111and Bloom, 111--112)112)

MVAs are the leading cause of TBI in the general population, especially among whites in the United States (~50% of all TBIs)Falls are the second leading cause of TBI. Falls account for (~20-30% of all TBIs)
– In individuals aged 75 years and older, falls are the most common cause of TBI. The very young also commonly sustain TBI due to falls.
Firearms are the third leading cause of TBI (~12% of all TBIs) and are a leading cause of TBI among individuals aged 25-34 years
Mechanisms of Injury for Mechanisms of Injury for TBITBI

Brain injury results from:Brain injury results from:
––Direct injury to brain tissueDirect injury to brain tissue
––External forces applied to outside External forces applied to outside of skull transmitted to the brainof skull transmitted to the brain
––Movement of brain inside skullMovement of brain inside skull
Traumatic Brain Injury Traumatic Brain Injury (TBI)(TBI)

Traumatic Head Injury
ALL-NET Pediatric Critical Care Textbook Source: LifeART EM Pro (1998) Lippincott Williams & Wilkins. www.med.ub.es/All-Net/english/neuropage/trauma/head-8htm

Traumatic Brain InjuryTraumatic Brain Injury
Primary Brain InjuryPrimary Brain InjuryResults from what has Results from what has occurred to the brain at occurred to the brain at the time of the injurythe time of the injury
Secondary Brain InjurySecondary Brain InjuryPhysiologic and Physiologic and biochemical events biochemical events which follow the which follow the primary injuryprimary injury

HEAD INJURIES / BRAIN INJURIESHEAD INJURIES / HEAD INJURIES / BRAIN INJURIESBRAIN INJURIES
ConcussionConcussionDiffuse Axonal InjuryDiffuse Axonal InjuryEpidural HematomaEpidural HematomaSubdural HematomaSubdural HematomaCoup and Countercoup Coup and Countercoup InjuriesInjuries

ConcussionConcussionConcussion is caused by deformity of the Concussion is caused by deformity of the
deep structures of the brain, leading to deep structures of the brain, leading to widespread neurologic dysfunction that can widespread neurologic dysfunction that can result in impaired consciousness or comaresult in impaired consciousness or coma
Concussion is considered a mild form of Concussion is considered a mild form of diffuse axonal injurydiffuse axonal injury

Diffuse Axonal InjuryDiffuse Axonal InjuryDiffuse axonal injury is characterized by extensive generalized damage to the white
matter of the brainStrains during high-speed
acceleration/deceleration produced in lateral motions of the head may cause the injuries
Diffuse axonal injury also could occur as a result of ischemia

Epidural HematomaEpidural HematomaMost often occurs from impact loading to the skull with associated laceration of the dural arteries or veins, often by fractured bones and sometimes by diploic veins in the skull's marrow
More often, a tear in the middle meningeal artery causes this type of hematoma. – When hematoma occurs from laceration of
an artery, blood collection can cause rapid neurologic deterioration

Clinical Manifestation of Epidural Clinical Manifestation of Epidural HematomaHematoma
Brief loss of consciousness followed by a Brief loss of consciousness followed by a lucid period. The lucid period is followed by lucid period. The lucid period is followed by rapid decrease in level of consciousness. rapid decrease in level of consciousness. Complaints of severe, localized headache. Complaints of severe, localized headache. Decreased LOC.Decreased LOC.Fixed and dilated pupil on the same side as Fixed and dilated pupil on the same side as the injury. the injury.

Subdural HematomaSubdural Hematoma
Subdural hematoma tends to occur in patients with injuries to the cortical veins or pial artery in severe TBI
The associated mortality rate is high, approximately 60-80%.

Epidural and Subdural Hematoma
ALL-NET Pediatric Critical Care Textbook - Source: LifeART EM Pro (1998) Lippincott Williams & Wilkins. www.med.ub.es/All-Net/english/neuropage/trauma/head-8htm


Coup and Contrecoup Coup and Contrecoup ContusionsContusions
A combination of vascular and tissue damage leads to cerebral contusion
Coup contusions occur at the area of direct impact to the skull and occur because of the creation of negative pressure when the skull, distorted at the site of impact, returns to its normal shape
Contrecoup contusions are similar to coup contusions but are located opposite the site of direct impact

Coup and Contrecoup Coup and Contrecoup ContusionsContusions
The amount of energy dissipated at the site of direct impact determines whether the ensuing contusion is of the coup or contrecoup type
Most of the energy of impact from a small hard object tends to dissipate at the impact site, leading to a coup contusion
On the contrary, impact from a larger object causes less injury at the impact site since energy is dissipated at the beginning or end of the head motion, leading to a contrecoup contusion


The severity of TBI according to the GCS score (within 48 hrs.) is as follows:
– Severe TBI = 1-8
– Moderate TBI = 9-12
– Mild TBI = 13-15
Severity of TBI using the Severity of TBI using the Glasgow Coma Scale Glasgow Coma Scale
(GCS)(GCS)

GCSGCS
rispostarispostanessunanessuna11
rispostarispostanessunanessuna11decerebratadecerebrataflessioneflessione22
incomprensibiliincomprensibiliSuoni Suoni 22decorticatadecorticataflessioneflessione3311 No rispostaNo risposta
Parole Parole sconnessesconnesse
piangepiange33al doloreal doloreflessioneflessione4422 al doloreal dolore
DisorientatoDisorientatopiangepiange44doloredolorelocalizzalocalizza5533 al rumoreal rumore
parlaparlaconversaconversarideride55obbedisceobbediscenormalenormale6644 SpontaneaSpontanea
22--5 5 annianni
> 5 anni> 5 anni<2anni<2anni>1anno>1anno< 1anno< 1anno
VerbaleVerbaleRispostaRispostaMotoriaMotoriaRispostaRispostaApertura Apertura occhiocchi

ASSESSMENT RAPID TRAUMA SURVEY
ASSESSMENT ASSESSMENT RAPID TRAUMA SURVEYRAPID TRAUMA SURVEY
Note LOC (AVPU), secure airway and Note LOC (AVPU), secure airway and protect cprotect c--spinespineAssess breathingAssess breathing–– Do not allow the patient to become Do not allow the patient to become
hypoxichypoxicAssess circulationAssess circulation–– Control major bleedingControl major bleeding–– Prevent hypotensionPrevent hypotensionTransport decision and interventionsTransport decision and interventionsDo brief Do brief neuroneuro & GCS if altered LOC& GCS if altered LOC

ASSESSMENT DETAILED EXAMASSESSMENT ASSESSMENT DETAILED EXAMDETAILED EXAM
Vital signsVital signsSAMPLE historySAMPLE historyHeadHead--toto--toe exam, including toe exam, including neurological and GCS, fluid leak, neurological and GCS, fluid leak, battle signbattle signFurther bandaging and splintingFurther bandaging and splintingContinuous observationContinuous observation

MonroeMonroe-- Kellie PrincipleKellie Principle
Rogers (1996) Textbook of Pediatric Intensive Care p. 646

CBF
MAP(mmHg)
Normal 50 - 100 ml / min
Normal 60 - 150 mmHg
Cerebral Blood FlowRegulation of Cerebral Vascular Resistance
PaCo2 (mmHg)
Normal 30 - 50 mmHg

Management of Management of Traumatic Head InjuryTraumatic Head Injury
Maximize oxygenation and ventilationMaximize oxygenation and ventilation
Support circulation / maximize cerebral Support circulation / maximize cerebral
perfusion pressureperfusion pressure
Decrease intracranial pressureDecrease intracranial pressure
Decrease cerebral metabolic rateDecrease cerebral metabolic rate

Primary injury is immediate from bruising or penetrating objects
Secondary injury is from hypoxia or ↓ perfusion of the brain– Caused by swelling, hypoxia, or hypotension– May be prevented by good patient care– Hyperventilation decreases perfusion of the brain
tissue– Protect airway, give oxygen, maintain BP
Primary vs. SecondaryPrimary vs. SecondaryBrain InjuryBrain Injury

KillsKillsthe patient with ICPthe patient with ICP

MonitoringMonitoring
Serial neurologic examinationsSerial neurologic examinationsCirculation / RespirationCirculation / RespirationIntracranial PressureIntracranial PressureRadiologic Studies Radiologic Studies Laboratory StudiesLaboratory Studies
Scherer & Spangenberg (1998) Critical Care Medicine, 26(1)
Fibrinogen and platelets are significantly decreased in TBI patients

Respiratory Support: Maximize OxygenationRespiratory Support: Maximize Oxygenation
Hypoxemia is predictive of morbidityHypoxemia is predictive of morbidity–– Ong et al. (1996) Ong et al. (1996) Pediatric Neurosurgery, 24Pediatric Neurosurgery, 24(6)(6)
Neurogenic pulmonary edema / concurrent lung injuryNeurogenic pulmonary edema / concurrent lung injury
–– Positive End Expiratory PressurePositive End Expiratory PressureMay impair cerebral venous returnMay impair cerebral venous return
–– Cooper et al. (1985) Cooper et al. (1985) Journal of Neurosurgery, Journal of Neurosurgery, 6363
–– Feldman et al. (1997) Feldman et al. (1997) Journal of Neurosurgical Journal of Neurosurgical Anesthesiology, 9Anesthesiology, 9(2)(2)
PEEP > 10 cm H2O increases ICPPEEP > 10 cm H2O increases ICP

Respiratory Support: NormoventilationRespiratory Support: NormoventilationHyperventilation : Historical management more harm Hyperventilation : Historical management more harm
than good?than good?
ALL-NET Pediatric Critical Care Textbookwww.med.ub.es/All-Net/english/neuropage/\protect/vent-5htm
Originally adapted from Skippen et al. (1997) Critical Care Medicine, 25

IperventilazioneIperventilazione

HYPERVENTILATION IS NO LONGER
RECOMMENDED FOR TREATING HEAD
INJURY EXCEPT IN THE CASE OF HERNIATION SYNDROME
HYPERVENTILATION IS HYPERVENTILATION IS NONO LONGER LONGER
RECOMMENDED FOR RECOMMENDED FOR TREATING HEAD TREATING HEAD
INJURY EXCEPT IN INJURY EXCEPT IN THE CASE OF THE CASE OF HERNIATION HERNIATION SYNDROMESYNDROME

Evidence Supporting NormoventilationEvidence Supporting Normoventilation
Forbes et al. (1998) Forbes et al. (1998) Journal of Neurosurgery, 88Journal of Neurosurgery, 88(3)(3)
Marion et al. (1995) Marion et al. (1995) New Horizons, 3New Horizons, 3(3)(3)
McLaughlin & Marion (1996) McLaughlin & Marion (1996) Journal of Neurosurgery, Journal of Neurosurgery,
8585(5)(5)
Muizelaar et al. (1991) Muizelaar et al. (1991) Journal of Neurosurgery, 75Journal of Neurosurgery, 75(5)(5)
Newell et al. (1996) Newell et al. (1996) Neurosurgery, 39Neurosurgery, 39(1)(1)
Skippen et al. (1997) Skippen et al. (1997) Critical Care Medicine, 25Critical Care Medicine, 25(8)(8)
Yundt & Diringer (1997) Yundt & Diringer (1997) Critical Care Clinics, 13Critical Care Clinics, 13(1)(1)

Use of Hyperventilation ...Use of Hyperventilation ...
Management of very acute elevation of intracranial Management of very acute elevation of intracranial pressurepressure
Preemptive for activities known to increase Preemptive for activities known to increase intracranial pressureintracranial pressure
No lower than 32No lower than 32--35 cmH35 cmH2200--- Moderate and transient

Circulatory Support: Circulatory Support: Maintain Cerebral Perfusion PressureMaintain Cerebral Perfusion Pressure
0
1
2
3
4
5
6
Outcome
GoodModerateSevereVegetativeDead
Number of Hypotensive Episodes
Kokoska et al. (1998), Journal of Pediatric Surgery, 33(2)

Circulatory Support: Circulatory Support: Maintain Cerebral Perfusion PressureMaintain Cerebral Perfusion Pressure
Adelson et al. (1997) Adelson et al. (1997) Pediatric Neurosurgery, Pediatric Neurosurgery, 26(4)26(4)–– Children (particularly < 24 months old) are at Children (particularly < 24 months old) are at
increased risk of cerebral hypoperfusion after increased risk of cerebral hypoperfusion after TBITBI
–– Low CBF is predictive of morbidityLow CBF is predictive of morbidity
Rosner et al. (1995) Rosner et al. (1995) Journal of Neurosurgery, Journal of Neurosurgery, 8383(6)(6)–– Management aimed at maintaining CPP (70 Management aimed at maintaining CPP (70
mmHg) improves outcomesmmHg) improves outcomes
CPP = MAP - ICP

Altered Cerebral Altered Cerebral AutoregulationAutoregulation

ICP is usually low (<15mmHg)ICP is usually low (<15mmHg)Cerebral perfusion pressure (CPP) Cerebral perfusion pressure (CPP) depends upon BP and ICPdepends upon BP and ICPCPP = MAP CPP = MAP -- ICPICPIf the ICP goes up the BP must go If the ICP goes up the BP must go up to maintain the CPPup to maintain the CPP
Bottom line, need BP between 80Bottom line, need BP between 80--90 90 mmHg systolic to perfuse the brainmmHg systolic to perfuse the brain
Intracranial Pressure (ICP)Intracranial Pressure (ICP)

Lowering ICPLowering ICP
Evacuate hematomaEvacuate hematomaDrain CSFDrain CSF–– Intraventricular catheters use is limited by Intraventricular catheters use is limited by
degree of edema and ventricular effacementdegree of edema and ventricular effacementCraniotomyCraniotomy–– Permanence, risk of infection, questionable Permanence, risk of infection, questionable
benefitbenefitReduce edemaReduce edemaPromote venous returnPromote venous returnReduce cerebral metabolic rateReduce cerebral metabolic rateReduce activity associated with elevated ICPReduce activity associated with elevated ICP
Brain Blood
CSF MassBone

Hyperosmolar Therapy: Increase Blood Hyperosmolar Therapy: Increase Blood OsmolarityOsmolarity
Fluid
Osmosis: Fluid will move from area of lower osmolarity to an area of higher osmolarity
Movement of fluid out of cell reduces edema
Brain cell
Blood vessel

Diuretic TherapyDiuretic Therapy
Osmotic DiureticOsmotic DiureticMannitolMannitol ((0.250.25--1 gm / kg1 gm / kg) ) Increases osmolarityIncreases osmolarityVasoconstriction Vasoconstriction (adenosine) / less effect if (adenosine) / less effect if autoregulation is impaired autoregulation is impaired and if CPP is < 70and if CPP is < 70Initial increase in blood Initial increase in blood volume, BP and ICP volume, BP and ICP followed by decreasefollowed by decreaseQuestionable mechanism of Questionable mechanism of lowering ICP lowering ICP Rosner et al. (1987) Rosner et al. (1987) Neurosurgery, 21Neurosurgery, 21(2)(2)
Loop DiureticLoop DiureticFurosemideFurosemideDecreased CSF Decreased CSF formationformationDecreased systemic and Decreased systemic and cerebral blood volume cerebral blood volume (impairs sodium and (impairs sodium and water movement across water movement across blood brain barrier)blood brain barrier)May have best affect in May have best affect in conjunction with mannitolconjunction with mannitolPollay et al. (1983) Pollay et al. (1983) Journal Journal ofof Neurosurgery, 59Neurosurgery, 59 ; ; Wilkinson (1983) Wilkinson (1983) Neurosurgery,12Neurosurgery,12(4)(4)

Hypertonic Fluid Hypertonic Fluid AdministrationAdministration
Fisher et al. (1992) Fisher et al. (1992) Journal of Neurosurgical Journal of Neurosurgical Anesthesiology, 4Anesthesiology, 4–– Reduction in mean ICP in children 2 hours after Reduction in mean ICP in children 2 hours after
bolus administration of 3% salinebolus administration of 3% saline
Taylor et al. (1996) Taylor et al. (1996) Journal of Pediatric Surgery,31Journal of Pediatric Surgery,31(1)(1)–– ICP is lowered by resuscitation with hypertonic ICP is lowered by resuscitation with hypertonic
saline vs. lactated ringers solution in an animal modelsaline vs. lactated ringers solution in an animal model
Qureshi et al. (1998) Qureshi et al. (1998) Critical Care Medicine, 26Critical Care Medicine, 26(3)(3)–– Reduction in mean ICP within 12 hours of continuous Reduction in mean ICP within 12 hours of continuous
infusion of 3% saline acetate solutioninfusion of 3% saline acetate solution–– Little continued benefit after 72 hours of treatmentLittle continued benefit after 72 hours of treatment

Qureshi et al. (1998) Critical Care Medicine, 26(3)
Goal: Sodium 145-155
Hyperosmolar Therapy
Sodium: square
ICP: circle

Promote Venous DrainagePromote Venous DrainageKeep neck midKeep neck mid--line and elevate head of bed line and elevate head of bed ……. To . To
what degree?what degree?
Dicarlo in ALL-NET Pediatric Critical Care Textbookwww.med.ub.es/All-Net/english/neuropage/\protect/icp-tx-3.htm
Feldman et al. (1992) Journal of Neurosurgery, 76
March et al. (1990) Journal of Neuroscience Nursing, 22(6)
Parsons & Wilson (1984) Nursing Research, 33(2)

Reduction of Cerebral Metabolic RateReduction of Cerebral Metabolic Rate
Reduction in cerebral oxygen requirementReduction in cerebral oxygen requirement–– Anticonvulsants Anticonvulsants -- Prevent seizure activityPrevent seizure activity–– PentobarbitalPentobarbital
Adverse effects include hypotension and bone Adverse effects include hypotension and bone marrow dysfunctionmarrow dysfunctionUsed only after unsuccessful attempts to Used only after unsuccessful attempts to control ICP and maximize CPP with other control ICP and maximize CPP with other therapiestherapiesImproved outcome not fully supported by Improved outcome not fully supported by researchresearch
Traeger et al. (1983) Critical Care Medicine, 11Ward et al. (1985) Journal of Neurosurgery, 62(3)

Management of Pain & AgitationManagement of Pain & Agitation
OpiodsOpiodsBenzodiazepinesBenzodiazepines
Management of Movement
• Neuromuscular blockade
Difficult to assess neurologic exam
Monitor for hypotension
Short acting agents beneficial
ICP management continued...
Do opiods increase CBF?Increased ICP with concurrent decreased MAP and CPP has been documented. Elevation in ICP is transient and there is no resulting ischemia from decreased MAP / CPP.
Albanese et al. (1999) Critical Care Medicine, 27(2)

02468
101214161820
Before During After
TurningSuctioningBathing
Nursing Activities and ICP
Rising (1993) Journal of Neuroscience Nursing, 25(5)
ICP

Family Contact and ICP
Bruya (1981) Journal of Neuroscience Nursing, 13
Hendrickson (1987) Journal of Neuroscience Nursing, 19(1)
Mitchell (1985) Nursing Administration Quarterly, 9(4)
Treolar (1991) Journal of Neuroscience Nursing, 23(5)
Presence, touch and voice of family / significant others...
• Does not significantly increase ICP
• Has been demonstrated to decrease ICP

Traumatic Brain InjuryTraumatic Brain Injury

Factors that Effect Secondary Brain Factors that Effect Secondary Brain InjuriesInjuries
Blood PressureBlood PressureOxygenationOxygenationTemperatureTemperatureControl of Blood GlucoseControl of Blood GlucoseFluid Volume StatusFluid Volume StatusIncreased Intracranial PressureIncreased Intracranial Pressure

Treatment of Severe Head Injury
Refractory intracranial hypertension
Second tier therapies
Surgicaldecompression
Hypothermia
Barbituates
Hyperventilation
Corticosteroids

Blood GlucoseBlood Glucose
Stress responseStress responseHypoglycemiaHypoglycemiaCochran (2003)Cochran (2003)

HypothermiaHypothermia
Prevention and aggressive treatment of Prevention and aggressive treatment of feverfeverSignificant beneficial effect on Significant beneficial effect on neurologicneurologicoutcome with transient, mild hypothermia outcome with transient, mild hypothermia (32 (32 °° –– 34 34 °°C for 24 C for 24 ––48 hours)48 hours)Seizure incidence and ICP reducedSeizure incidence and ICP reducedHyperthermia produces deleterious effects Hyperthermia produces deleterious effects on neuronal recovery and BBB integrityon neuronal recovery and BBB integrity

GlucocorticoidsGlucocorticoids
Standards Standards -- not recommendednot recommendedGuidelines Guidelines -- nonenone

AntiAnti--seizure prophylaxisseizure prophylaxis
Standard Standard -- not not recrec for the prevention of late for the prevention of late PTSPTSGuidelines Guidelines -- nonenoneOptions Options -- may be used to treat early PTS in may be used to treat early PTS in high risk patientshigh risk patients

HyperventilationHyperventilation
Moderate hyperventilation (PaCOModerate hyperventilation (PaCO22 < 30 < 30 mmHg) may be associated with worse mmHg) may be associated with worse outcomeoutcome
Avoid even prophylactic hyperventilation in Avoid even prophylactic hyperventilation in first 24 h post TBI to prevent ischemiafirst 24 h post TBI to prevent ischemia

Summary of Recommended PracticesSummary of Recommended Practices
Maximize oxygenation (PEEP < 10)Maximize oxygenation (PEEP < 10)NormoventilateNormoventilateSuction only as needed, limit passes, preSuction only as needed, limit passes, pre--oxygenate, +/oxygenate, +/-- prepre--hyperventilate (not < hyperventilate (not < 30), use lidocaine when possible30), use lidocaine when possibleMaintain blood pressure and maintain CPP Maintain blood pressure and maintain CPP > 60> 60Evacuate intracranial bloodEvacuate intracranial bloodDrain CSF with ventriculostomy when Drain CSF with ventriculostomy when possiblepossible

Summary of Recommended PracticesSummary of Recommended Practices
Hyperosmolar therapyHyperosmolar therapyAvoid hyperthermia, +/Avoid hyperthermia, +/-- hypothermiahypothermiaPrevent seizuresPrevent seizuresReserve pentobarbital for refractory conditionsReserve pentobarbital for refractory conditionsMidMid--line neck, elevated head of bead, ? not > 30 line neck, elevated head of bead, ? not > 30 degreesdegreesTreat pain and agitation Treat pain and agitation -- consider preconsider pre--medication for medication for nursing activitiesnursing activitiesAvoid hyperglycemiaAvoid hyperglycemiaAllow family contactAllow family contact

Monitoring Brain MetabolismJugular Venous Catheter
Jugular Venous Oxygen Saturation (SJVO2)
Arteriojugular Venous Oxygen Difference (AJVO2)
Cerebral Metabolic Rate For Oxygen (CMRO2)
Possible better outcome in adults
Cruz (1998) Critical Care Medicine, 26(2)
Brain Sensors
Brain tissue pH, PaO2, PcO2, lactate
Kiening (1997) Neurology Research, 19(3)

Ernie CerebraliErnie Cerebrali

ERNIAZIONE CENTRALEERNIAZIONE CENTRALE I )I ) DiencefalicoDiencefalico
Respiro di Respiro di CheyeneCheyene -- StokesStokes. Pupille . Pupille miotiche reattivemiotiche reattive
II) II) MesencefalicoMesencefalicoTachipnea. Pupille mediane, Tachipnea. Pupille mediane, areattiveareattive, ,
movimenti movimenti disconiugatidisconiugati. Postura . Postura decorticatadecorticataIII) BulbareIII) Bulbare
Perdita di tutti i riflessi Perdita di tutti i riflessi troncoencefalicitroncoencefalici

Ernia Ernia UncaleUncale

HERNIATION SYNDROMEHERNIATION HERNIATION SYNDROMESYNDROME
Increased ICPIncreased ICPComaComaDilatation of Dilatation of ipsilateralipsilateral or both or both pupilspupilsContralateralContralateral hemiparesishemiparesisDecreasing respirationDecreasing respirationCushingCushing’’s Reflexs Reflex–– HypertensionHypertension–– BradycardiaBradycardia

E. E. TranstentorialeTranstentoriale e e SubfalcinaSubfalcina

ERNIAZIONE UNCALEERNIAZIONE UNCALECompressione asimmetricaCompressione asimmetrica
I FASE I FASE IperventilazioneIperventilazione,midriasi ,midriasi
omolateraleomolaterale,sguardo deviato in basso ed ,sguardo deviato in basso ed esternamenteesternamente
II FASEII FASE IperventilazioneIperventilazione, midriasi, risposta , midriasi, risposta
motoria asimmetrica, perdita della funzione motoria asimmetrica, perdita della funzione delldell’’oculomotore e dei riflessi cornealioculomotore e dei riflessi corneali

REATTIVITAREATTIVITA’’ PUPILLAREPUPILLARE

CAUSE DI MIOSICAUSE DI MIOSIClonidinaClonidina CCOppiacei Oppiacei OOFenotiazineFenotiazine PPSedativi, ipnoticiSedativi, ipnotici SS
ColinergiciColinergiciOrganofosforiciOrganofosforici
Emorragie del ponteEmorragie del ponteSonnoSonno

CAUSE DI MIDRIASICAUSE DI MIDRIASI
Anfetamine Anfetamine AnticolinergiciAnticolinergiciCocainaCocainaEfedrinaEfedrina
AntistaminiciAntistaminici
Alcool etilicoAlcool etilico
GlutetimideGlutetimide
Compressione III Compressione III paio nervi cranicipaio nervi cranici

Case 1Case 1Field TreatmentField Treatment––Position flat, spine Position flat, spine
immobilizationimmobilization––Hyperventilation with 100% Hyperventilation with 100%
oxygenoxygen––IV IV ––OnsceneOnscene time 9 minutestime 9 minutes

Case 1Case 1Trauma CenterTrauma Center–– UnresponsiveUnresponsive–– Unequal pupil, > on leftUnequal pupil, > on left–– Chest: normalChest: normal–– Abdomen: normalAbdomen: normal–– Pulse 44Pulse 44–– BP 260/140BP 260/140–– Respiration's 40, deepRespiration's 40, deep
––

Case 1Case 1Trauma CenterTrauma Center––XX--rayray
Spine: normalSpine: normalSkull: right linear fractureSkull: right linear fractureCT: right epidural hematoma, CT: right epidural hematoma, with midline shiftwith midline shift

Case 1Case 1Due to critical nature of patientDue to critical nature of patient’’s s condition it was decided to do a burr condition it was decided to do a burr hole right temporal areahole right temporal areaPatient almost immediately became Patient almost immediately became combativecombativeDecreased posturingDecreased posturingPules 88Pules 88BP 182/58BP 182/58RespirationRespiration’’s 20s 20

Case 1Case 1Patient tolerated surgery wellPatient tolerated surgery wellICP monitoredICP monitoredPlaced in medicated comaPlaced in medicated comaWoke up one week later, opened Woke up one week later, opened eyeseyesNever communicatedNever communicatedTransferred to rehabilitation unitTransferred to rehabilitation unitNever regained any additional Never regained any additional functionfunction

Case 2Case 2Called to the scene for a possible Called to the scene for a possible ““shootingshooting””49 year old female, found on the floor in a 49 year old female, found on the floor in a pool of blood pool of blood Large puncture wound on top of the head Large puncture wound on top of the head with bone fragments gray matter coming with bone fragments gray matter coming from the woundfrom the woundAlert, but disorientedAlert, but disorientedPupils equalPupils equalStrong radial pulseStrong radial pulsePulse 120, BP 148/70, respiration's 30 good Pulse 120, BP 148/70, respiration's 30 good TVTV

Case 2Case 2Placed on oxygenPlaced on oxygenSpinal immobilizationSpinal immobilizationDressing to head woundDressing to head woundIV establishedIV establishedSecond vitalsSecond vitals–– pulse 118pulse 118–– BP 130/palpBP 130/palp–– respirationrespiration’’s 28s 28
OnsceneOnscene time 12 minutestime 12 minutes

Case 2Case 2Arrive trauma centerArrive trauma center–– Alert, disorientedAlert, disoriented–– pupils left dilated, right normalpupils left dilated, right normal–– hemorrhage to left eyehemorrhage to left eye–– chest; normalchest; normal–– abdomen; normalabdomen; normal–– Pulse 90Pulse 90–– BP 146/80BP 146/80–– RespirationRespiration’’s 26s 26

Case 2Case 2Police arrive and state the patient Police arrive and state the patient was assaulted by her husband, and was assaulted by her husband, and was hit over the head with a was hit over the head with a hammerhammerXX--ray revealed multiple depressed ray revealed multiple depressed skull fractures, no evidence of skull fractures, no evidence of epiepior or subduralsubdural bleedbleed

Case 2Case 2Patient went to surgery to have the Patient went to surgery to have the wound wound debrideddebrided and have the chips and have the chips elevated.elevated.No evidence of brain injury during No evidence of brain injury during surgerysurgeryTwo days in ICUTwo days in ICUdischarged from the hospital two discharged from the hospital two weeks later, with no neurological weeks later, with no neurological damagedamage

Case 3Case 3Called to a high school stadium for a Called to a high school stadium for a football player that collapsed during the football player that collapsed during the game.game.According to the other players he was According to the other players he was hit in the head during the game.hit in the head during the game.He got up immediately and entered the He got up immediately and entered the huddle.huddle.Prior to the next play he appeared Prior to the next play he appeared confused and fell to the ground.confused and fell to the ground.Unresponsive to painUnresponsive to painPupils fixed and dilated Pupils fixed and dilated

Case 3Case 3RespirationRespiration’’s 38 deeps 38 deepSkin warm drySkin warm dryNo evidence of traumaNo evidence of traumaPulse 64Pulse 64BP 170/94BP 170/94

Case 3Case 3Helmet remained and he was Helmet remained and he was immobilized on a backboardimmobilized on a backboardOxygenOxygenHe had a grand mal seizure just He had a grand mal seizure just prior to arrival to hospitalprior to arrival to hospital

Case 3Case 3Arrived at the hospital, condition Arrived at the hospital, condition unchangedunchangedFamily arrived and stated he had a Family arrived and stated he had a head injury two days ago at football head injury two days ago at football practice, with a 60 second loss of practice, with a 60 second loss of consciousness.consciousness.Did not receive any medical attentionDid not receive any medical attentionLast night he felt sick to his stomach Last night he felt sick to his stomach and didnand didn’’t, and vomited a few times t, and vomited a few times during the night. during the night.

Case 3Case 3In the ED his pressure started In the ED his pressure started to drop.to drop.He was given fluids and He was given fluids and pressure agentspressure agentsHis extremities were flaccidHis extremities were flaccidPulse 66, BP 110/50, assisted Pulse 66, BP 110/50, assisted respirationrespiration’’ssCT revealed a large inoperable CT revealed a large inoperable subarachnoidsubarachnoid bleedbleed

Case 3Case 3IntubatedIntubatedTaken to the ICUTaken to the ICUA A ventriculostomyventriculostomy was placed to was placed to monitor ICPmonitor ICPTaken to radiology for arteriogram, Taken to radiology for arteriogram, showed that he had no carotid blood showed that he had no carotid blood flow, and little to no vertebral/basilar flow, and little to no vertebral/basilar artery flow artery flow Patient did not improve and one week Patient did not improve and one week later was taken off life supportlater was taken off life supportN h t dN h t d

Case 4Case 4Called to a city park for a 12 year Called to a city park for a 12 year female soccer player, that ran into a a female soccer player, that ran into a a player with her head.player with her head.Payers say she was unresponsive for a Payers say she was unresponsive for a minuteminuteShe is now conscious, appears orientedShe is now conscious, appears orientedHematoma on the top of her headHematoma on the top of her headNo fluid ears or noseNo fluid ears or noseNo other sign of traumaNo other sign of traumaPupils equal reactivePupils equal reactivePulse 100 BP 136/90 respirationPulse 100 BP 136/90 respiration’’s 24s 24

Case 4Case 4OxygenOxygenSpinal immobilizationSpinal immobilizationIV establishedIV establishedNo significant medical problems or No significant medical problems or complaintscomplaintsSecond vital Second vital –– pulse 80pulse 80–– BP120/80BP120/80–– respirationrespiration’’s 18s 18On scene time 18 minutesOn scene time 18 minutes

Case 4Case 4In the EDIn the ED–– Cranial nerves intactCranial nerves intact–– Ears clearEars clear–– Pupils equal reactivePupils equal reactive–– Chest; normalChest; normal–– Abdomen; normalAbdomen; normalVitals unchangedVitals unchangedXX--ray; nothing seenray; nothing seen

Case 4Case 4Removed from backboardRemoved from backboardObserved in the ED for six hours, Observed in the ED for six hours, constant constant neuroneuro and vital sign and vital sign checkschecksNo changes were noted No changes were noted Patient was discharged to the Patient was discharged to the family with instructions to observe family with instructions to observe for level of conscious, changes for level of conscious, changes ever 2ever 2--4 hours.4 hours.

ReferencesReferences
Dr. Baxter Larmon, Director of the UCLA CPC Dr. Baxter Larmon, Director of the UCLA CPC and Professor of Medicine, UCLA School of and Professor of Medicine, UCLA School of MedicineMedicine
UCLA EMT Lectures, Barry Jensen and EMT UCLA EMT Lectures, Barry Jensen and EMT Team, 2003Team, 2003
Brady / DOT paramedic lectures and Brady / DOT paramedic lectures and curriculumcurriculum
www.emedicine.comwww.emedicine.com