Embed Size (px)
Citation preview

SURGICAL ONCOLOGY AND RECONSTRUCTION
Sou
Sur
Aus
Aus
par
Head and Neck Cutaneous SquamousCell Carcinoma Metastatic to Cervical
Sublevel IIb Lymph Nodes Occurred FromPrimary Sites Involving the Auricle and
Adjacent Neck
*Reside
th Wal
yAssocigery, J
tralia;
tralia.
Addres
tment
Nigel Gordon Maher, BMed, BDSc, BSc,* and
Gary Russell Hoffman, MBBS, BDSc, MSc, PhDy
Purpose: Neck dissections that include sublevel IIb increase the risk of postoperative shoulder dysfunc-tion. The purpose of this investigation was to document the incidence of level IIb metastatic lymphaticspread in a group of patients undergoing neck dissection as part of the surgical management of cutaneous
squamous cell carcinoma of the head and neck.
Materials and Methods: A retrospective review of the pathology records taken from 1 surgeon from
June 2006 through June 2013 was carried out. The predictor variable was the primary tumor site. The out-
come variable was the metastatic nodal involvement according to neck level and sublevel. Secondary vari-
ables included T stage, pathologist, tumor depth, and the presence of perineural, perilymphatic, and
perivascular invasion. Data analyses were by descriptive statistics.
Results: Thirty-six patients with a total of 40 neck dissections met the inclusion criteria. The average
primary site tumor depth was 14.7 mm, and there were 16 cases of poorly differentiated squamous cell
carcinoma. Sublevel IIb was involved in 7.5% of cases, all of which occurred from lateralized primary sites
of the head and neck.
Conclusions: Cutaneous squamous cell carcinoma arising from the auricle and neck sites adjacent to sub-
level IIbmayhave increased risk ofmetastatic involvement of sublevel IIb nodes. Further studieswith larger
numbers are required to determine the risk of metastasis to sublevel IIb from midline sites of the face.
Crown Copyright � 2014 Published by Elsevier Inc on behalf of the American Association of Oral and
Maxillofacial Surgeons. All rights reserved
J Oral Maxillofac Surg 72:627-632, 2014
Cutaneous squamous cell carcinoma (cSCC) of the
head and neck is a common malignancy. It has the po-
tential to metastasize to the periparotid, intraparotid,
perifacial, and cervical lymph nodes. Such events sig-
nificantly alter the prognosis. The incidence of metas-
tases from cSCC of the head and neck varies from 0.5%
to 21%, but is most frequently reported at approxi-mately 5%.1-3
nt Medical Officer, Hunter New England Health, New
es, Australia.
ate Professor, Department of Oral and Maxillofacial
ohn Hunter Hospital, Newcastle, New South Wales,
University of Newcastle, Newcastle, New South Wales,
s correspondence and reprint requests to Dr Maher: De-
of Oral and Maxillofacial Surgery, John Hunter Hospital,
627
Depending on the clinical, pathologic, and radio-
graphic features of the primary site and surrounding
lymph node basin, a neck dissection (staging, thera-
peutic, or salvage) may be undertaken to clear the
neck of at-risk or involved lymphatic sites. An under-
standing of the pattern of lymphatic spread can help
guide the extent of neck dissections. Although meta-static spread of cSCC of the head and neck has been
Lookout Road, New Lambton, NSW 2305, Australia; e-mail:
Received July 17 2013
Accepted August 19 2013
Crown Copyright � 2014 Published by Elsevier Inc on behalf of the American
Association of Oral and Maxillofacial Surgeons. All rights reserved
0278-2391/13/01112-9$36.00/0
http://dx.doi.org/10.1016/j.joms.2013.08.024

628 CERVICAL SUBLEVEL IIb LYMPHATIC METASTASIS
well documented,4-7 sparse literature exists to
differentiate the cSCC metastatic involvement that
can occur within neck sublevels IIa and IIb.
Cervical level II is an anatomic region that contains
the lymph nodes surrounding the upper internal jugu-
lar vein and spinal accessory nerve (SAN). It is defined
by the skull base superiorly, hyoid bone inferiorly,
stylohyoid muscle medially, and posterior border ofthe sternocleidomastoid muscle posteriorly. The SAN
splits level II into sublevels IIa and IIb. IIa is anterior
to the SAN and IIb is the region posterior to the SAN.8
It is important to differentiate the metastatic involve-
ment of IIb nodes, because dissection of this sublevel
has been shown to increase the risk of postoperative
shoulder dysfunction.9 In a comparative study be-
tween neck dissections that spared and included sub-level IIb, patients who had IIb spared showed less of
a decrease in the motor action potential amplitude (av-
erage decrease, 4.55) 3 weeks postoperatively com-
pared with patients who had IIb included in the
dissection (average decrease, 12.03). In the patients
with sparing of IIb, there also was a lower incidence
of denervation shown by electromyography, and
quality-of-life scores were slightly higher.9 Long-termshoulder dysfunction can occur despite anatomically
preserving the SAN10 owing to the traction or devascu-
larization of the nerve during the dissection.10,11
Given the increasing emphasis on quality-of-life con-
siderations in cancer care, it is important to determine
the value of sublevel IIb dissection in head and neck
cancer. The purposes of this investigation were to 1)
document the lymphatic metastases of a group of pa-tients with head and neck cSCC with reference to sub-
level IIb and 2) review the literature to determine the
rate of sublevel IIb metastatic involvement in cSCC of
the head and neck. The hypothesis of the study was
that the rate of sublevel IIb metastatic involvement
would be lower in midline compared with lateralized
facial primary cSCC sites.
Materials and Methods
STUDY DESIGN AND SAMPLE
A retrospective study of the head and neck pathol-ogy records taken from 1 oral and maxillofacial sur-
geon from June 2006 through June 2013 was
conducted. In each case, the surgeon was the operator
or assistant for the neck dissection. This ensured that
the neck dissection was carried out in the same man-
ner on each occasion. After neck dissection, the
same surgeon pinned out the dissection specimen on
a corkboard and clearly labeled the relevant levelsand sublevels of the dissection.
Inclusion criteria were the resection of a primary or
recurrent cSCC in the head and neck region under-
taken in conjunction with a unilateral or bilateral
neck dissection. Exclusion criteria were undifferenti-
ated carcinomas, an unknown primary tumor site,
and lip tumors that involved the mucosal or vermillion
surfaces. This was because lip squamous cell carci-
noma has a different behavior and metastatic rate com-
pared with cSCC.12 Data also were excluded if they did
not distinguish between neck levels in general or be-
tween sublevels IIa and IIb specifically.
VARIABLES
The primary variables were categorical (tumor
site, neck levels and sublevels) and discrete (nodal
involvement). Other variables were continuous (tumor
depth) and categorical (tumor T stage, pathologist,andperineural, perilymphatic, or perivascular invasion).
DATA COLLECTION METHODS
The pathology reports were reviewed manually
and data were entered into a spreadsheet. Neck levels
and sublevels were divided into levels I, IIa, IIb, III, IV,and V. Distinction was not made when entering the
data for sublevel Ia, Ib, Va, or Vb. T staging was re-
corded according to the seventh edition of the Amer-
ican Joint Committee on Cancer staging system for
cSCC.13 This resulted in numerous cases staged as
T3 and T4, based on the sixth edition, being down-
staged owing to the changes in definitions with the
seventh edition.Cutaneous head and neck sites were divided into
the following categories:
� Ear and postauricular
� Temple
� Cheek and preauricular
� Periorbital
� Nose
� Chin
� Neck
Parotidectomy and parotid lymph node status also
were recorded.
DATA ANALYSIS
Analysis was by descriptive statistics. A c2 test wasconducted to determine whether there was any signif-
icant difference in IIb involvement between lateral and
midline primary sites. Midline sites were defined as
nose, chin, and periorbital sites; lateral sites were de-
fined by ear, postauricular, temple, cheek, and preau-
ricular sites.
ETHICS
Because of the retrospective nature of this study, it
was granted an exemption in writing by the Hunter

Table 1. PATIENT CHARACTERISTICS
MAHER AND HOFFMAN 629
New England Health ethics committee institutional re-
view board.
Gender, n (%)
Female 2 (6)
Male 34 (94)
Age (yr), mean (SD) 67.7 (10)
Tumor site, n (%)
Ear/postauricular 10 (28)
Cheek/preauricular 11 (31)
Temporal 4 (11)
Periorbit 5 (14)
Nose 2 (6)
Chin 2 (6)
Neck 2 (6)
T stage, n (%)
1 1 (3)
2 27 (75)
3 4 (11)
4 2 (6)
Not specified 2 (6)
Differentiation, n (%)
Well 5 (14)
Moderate 13 (36)
Poor 16 (44)
Results
One hundred ninety-eight records were screened.
Thirty-six patients matched the inclusion criteria of
the study. There were 40 neck dissections in total.
Table 1 presents their basic characteristics.
The average local (primary site) tumor depth was14.7 mm (range, 3.5 to 28 mm; median, 13.7 mm).
The clinical notes section in the pathology reports
showed that there were at least 8 cases of recurrent
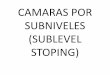
cSCC. Table 2 presents the metastatic involvement
for the group by level and site. In certain cases in
which there was a parotidectomy, no comment was
given for the lymph node count.
The c2 test to explore any difference in IIb involve-ment between midline and lateral sites lacked power
to generate a significant result.
Therewere 11 different reporting pathologists, with
2 of the pathologists reporting the majority of cases
(12 and 8 cases each).
Not specified 2 (6)
Histopathology, n (%)
Perineural invasion 16 (44)
Perilymphatic invasion 3 (8)
Perivascular invasion 4 (11)
Maher and Hoffman. Cervical Sublevel IIb LYMPHATIC METASTA-
SIS. J ORAL MAXILLOFAC SURG 2014.
Discussion
The purposes of this study were to 1) document the
cSCC lymphatic spread in a group of patients withhead and neck cancer with particular reference to sub-
level IIb and 2) review the literature to determine the
rate of sublevel IIb metastatic involvement in cSCC of
the head and neck. The hypothesis of the study was
that the rate of sublevel IIb metastatic involvement
would be lower in midline compared with lateralized
facial primary cSCC sites.
The present study found that sublevel IIb had met-astatic nodal involvement in 2 cases of ear cSCC and
in 1 case of a neck cSCC directly adjacent to the
same sublevel, with an overall average incidence of
7.5% per neck dissection. For these 3 cases, the per-
centages of sublevel IIb metastatic nodal involvement
from the overall nodes taken in each case from sub-
level IIb were 62.5% (5 of 8), 23.5% (4 of 17), and
50% (1 of 2). In terms of their characteristics, all 3cases were poorly differentiated: 1 had shown peri-
neural involvement, 2 were staged T2, and 1 was
staged T3. No tumor depths were recorded in the pa-
thology reports for these 3 cases. The clinical histo-
ries given did not indicate that any of these 3 cases
were recurrences.
The overall average of combined level II involve-
ment (ie, sublevels IIa and IIb) was 10% per neck dis-section. In relation to the authors’ hypothesis, no
periorbital, nose, or chin sites had IIb metastatic in-
volvement, which supports the hypothesis. However,
because this study had a small number of overall neck
dissections and a small number of sites from the mid-
line regions of the face, it is difficult to extrapolate
the significance of this finding. It also is acknowledged
that although periorbital primaries can be more later-ally located and drain to the parotid lymph nodes,
they were mentioned in the group of midline struc-
tures because the medial part of this region can in-
clude naso-orbital primaries, which was the case in
this study.
In comparison, a larger study of 151 elective and
therapeutic neck dissections showed that the inci-
dence of overall level II metastatic involvement forhead and neck cSCC was 37%.5 The present study
had a much lower overall level II involvement of
10%. Thismay be a result of the smaller sample, a differ-
ent ratio of therapeutic to elective neck dissections,
or differences in the clinicopathologic features of
the group. Nonetheless, the present population was
at a high risk for locoregional metastases given the
deep average tumor depth (14.7 mm) and prevalenceof recurrent disease, poorly differentiated tumors
(n = 16), and perineural invasion (n = 16). The pres-
ent study population was consistent with other stud-
ies that have shown a higher incidence of laterally
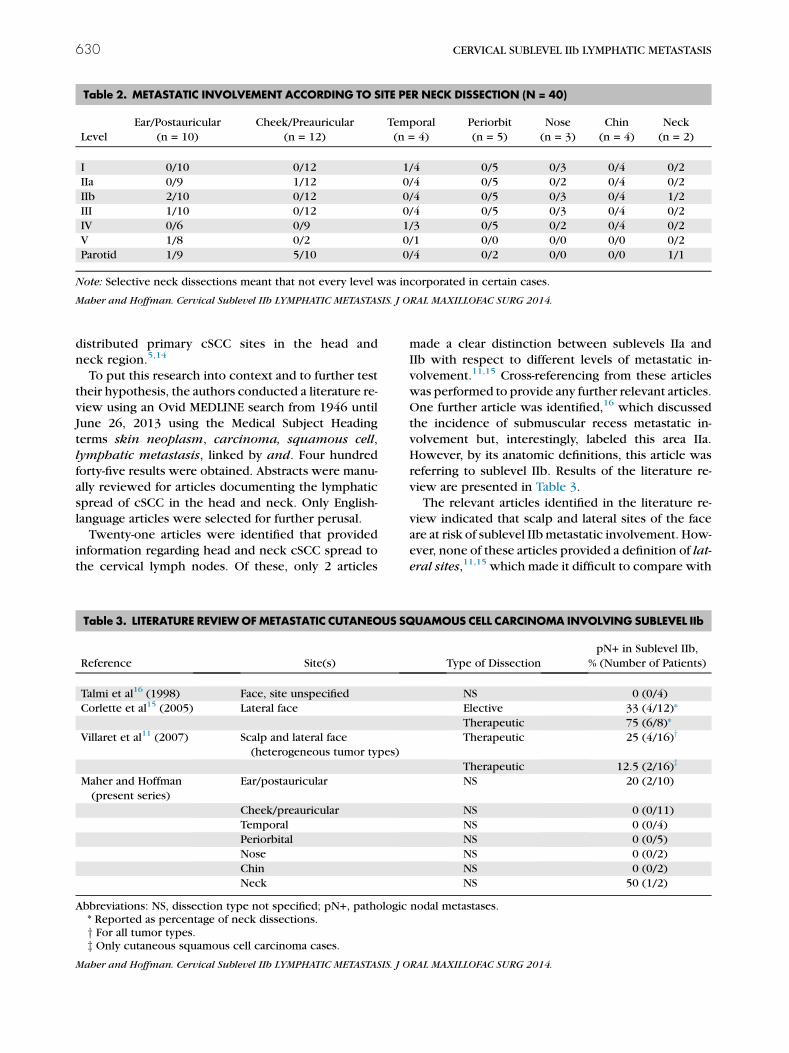
Table 2. METASTATIC INVOLVEMENT ACCORDING TO SITE PER NECK DISSECTION (N = 40)
Level
Ear/Postauricular
(n = 10)
Cheek/Preauricular
(n = 12)
Temporal
(n = 4)
Periorbit
(n = 5)
Nose
(n = 3)
Chin
(n = 4)
Neck
(n = 2)
I 0/10 0/12 1/4 0/5 0/3 0/4 0/2
IIa 0/9 1/12 0/4 0/5 0/2 0/4 0/2
IIb 2/10 0/12 0/4 0/5 0/3 0/4 1/2
III 1/10 0/12 0/4 0/5 0/3 0/4 0/2
IV 0/6 0/9 1/3 0/5 0/2 0/4 0/2
V 1/8 0/2 0/1 0/0 0/0 0/0 0/2
Parotid 1/9 5/10 0/4 0/2 0/0 0/0 1/1
Note: Selective neck dissections meant that not every level was incorporated in certain cases.
Maher and Hoffman. Cervical Sublevel IIb LYMPHATIC METASTASIS. J ORAL MAXILLOFAC SURG 2014.
630 CERVICAL SUBLEVEL IIb LYMPHATIC METASTASIS
distributed primary cSCC sites in the head and
neck region.5,14
To put this research into context and to further testtheir hypothesis, the authors conducted a literature re-
view using an Ovid MEDLINE search from 1946 until
June 26, 2013 using the Medical Subject Heading
terms skin neoplasm, carcinoma, squamous cell,
lymphatic metastasis, linked by and. Four hundred
forty-five results were obtained. Abstracts were manu-
ally reviewed for articles documenting the lymphatic
spread of cSCC in the head and neck. Only English-language articles were selected for further perusal.
Twenty-one articles were identified that provided
information regarding head and neck cSCC spread to
the cervical lymph nodes. Of these, only 2 articles
Table 3. LITERATURE REVIEWOFMETASTATIC CUTANEOUS SQ
Reference Site(s)
Talmi et al16 (1998) Face, site unspecified
Corlette et al15 (2005) Lateral face
Villaret et al11 (2007) Scalp and lateral face
(heterogeneous tumor types)
Maher and Hoffman
(present series)
Ear/postauricular
Cheek/preauricular
Temporal
Periorbital
Nose
Chin
Neck
Abbreviations: NS, dissection type not specified; pN+, pathologic* Reported as percentage of neck dissections.y For all tumor types.z Only cutaneous squamous cell carcinoma cases.
Maher and Hoffman. Cervical Sublevel IIb LYMPHATIC METASTASIS. J O
made a clear distinction between sublevels IIa and
IIb with respect to different levels of metastatic in-
volvement.11,15 Cross-referencing from these articleswas performed to provide any further relevant articles.
One further article was identified,16 which discussed
the incidence of submuscular recess metastatic in-
volvement but, interestingly, labeled this area IIa.
However, by its anatomic definitions, this article was
referring to sublevel IIb. Results of the literature re-
view are presented in Table 3.
The relevant articles identified in the literature re-view indicated that scalp and lateral sites of the face
are at risk of sublevel IIbmetastatic involvement. How-
ever, none of these articles provided a definition of lat-
eral sites,11,15 which made it difficult to compare with
UAMOUS CELL CARCINOMA INVOLVING SUBLEVEL IIb
Type of Dissection
pN+ in Sublevel IIb,
% (Number of Patients)
NS 0 (0/4)
Elective 33 (4/12)*
Therapeutic 75 (6/8)*
Therapeutic 25 (4/16)y
Therapeutic 12.5 (2/16)z
NS 20 (2/10)
NS 0 (0/11)
NS 0 (0/4)
NS 0 (0/5)
NS 0 (0/2)
NS 0 (0/2)
NS 50 (1/2)
nodal metastases.
RAL MAXILLOFAC SURG 2014.

MAHER AND HOFFMAN 631
the lateral site allocations in this study. The present
study indicates that sites involving the auricle and
neck (when adjacent to sublevel IIb) are at risk of
sublevel IIb metastatic involvement. Based on the
information of the literature review and this study,
the authors suggest that sublevel IIb always be
included in the neck dissection for primary sites
involving the scalp, lateral face, and neck (if it isadjacent to sublevel IIb). What is less clear is the
incidence of IIb involvement from the midline sites
of the face.
Other studies have shown that level II can be in-
volved with anterior or midline structures. Two of
10 neck dissections from a group of periorbital,
nose, and chin primary cSCC sites had level II meta-
static involvement in 1 study,5 and another studyshowed 4 of 10 patients had level II metastatic
involvement from cSCC of the nose and eyelid.17
Netterville et al18 showed that level II was not
involved in 5 patients with cSCC metastatic disease
involving the nose.
Although level II may be involved with metastatic
disease from midline cSCC primary sites, no other
studies have shown whether this involves IIa or IIbspecifically. Given that cSCC of the head and neck
has a predilection to lateral sites of the face, there
are often limited numbers of midline cases. This makes
finding strong evidence about IIb involvement from
these sites difficult.
Furthermore, there is no standardizedway of report-
ing the primary sites of the head and neck.5 Without
standardized information, cumulating patient informa-tion from different studies can be difficult.
The authors also acknowledge that there has been
limited literature thus far detailing the benefits of
IIb-sparing neck dissections in relation to shoulder
dysfunction and quality of life.9,19,20 Controlled trials
in patients undergoing superselective neck dissections
for laryngeal cancer should provide more answers.
Future studies also should aim to analyze thequality of life and yearly survival rates from neck
dissections incorporating or excluding sublevel IIb
for the management of cSCC of the head and neck.
Interestingly, a recent study found that for metastatic
cSCC to the cervical lymph nodes, the extent of
neck dissection did not have a statistically significant
influence on 5-year overall survival or 5-year disease-
free survival.21
The main strength of this study was that the same
surgeon was involved in each case and that demarca-
tion of the dissection specimen was consistent. This
study also is the largest to date to show sublevel IIb in-
volvement from cSCC of the head and neck.
Nevertheless, the main limitation of this study was
the small population. This meant the study was not
powered enough to generate a statistically significant
result when comparing midline with lateral sites.
Other limitations of the study were the retrospective
nature, no distinction between elective and therapeu-
tic neck dissections, and the variety of reporting pa-
thologists.
To the authors’ knowledge, this is the largest study
to date showing the rate of IIb metastatic involvement
in cSCC of the head and neck. The authors’ prelimi-nary study showed that metastatic involvement of sub-
level IIb occurred from auricular and adjacent neck
sites. It is difficult to accurately predict whether
more midline primary cSCCs have a lower incidence
of IIb involvement given the limited numbers from
this study and the literature review. However, the
present results indicate that this is a possibility. Fur-
ther studies are required that document the incidenceof IIb metastatic involvement from cSCC of the head
and neck. In addition, for comparison, it will be im-
portant to develop a standard guide for reporting
the different site categories of head and neck cutane-
ous cancers.
References
1. Moore B, Weber R, Prieto V, et al: Lymph node metastases fromcutaneous squamous cell carcinoma of the head and neck. La-ryngoscope 115:1561, 2005
2. Rowe D, Carroll R, Day CJ: Prognostic factors for local recur-rence, metastasis, and survival rates in squamous cell carcinomaof the skin, ear and lip. Implications for treatment modality se-lection. J Am Acad Dermatol 26:976, 1992
3. Lund H: How often does squamous cell carcinoma of the skinmetastasize? Arch Dermatol 92:635, 1965
4. O’Brien C, McNeil E, McMahon J, et al: Incidence of cervicalnode involvement in metastatic cutaneous malignancy involvingthe parotid gland. Head Neck 23:744, 2001
5. Vauterin T, Veness M, Morgan G, et al: Patterns of lymph nodespread of cutaneous squamous cell carcinoma of the head andneck. Head Neck 28:785, 2006
6. Veness M, Palme C, Morgan G: High-risk cutaneous squamouscell carcinoma of the head and neck: Results from 266 treatedpatients with metastatic lymph node disease. Cancer 106:2389, 2006
7. Ebrahimi A, Moncrieff M, Clark J, et al: Predicting the pattern ofregional metastases from cutaneous squamous cell carcinoma ofthe head and neck based on location of the primary. Head Neck32:1288, 2010
8. Robbins K, Clayman G, Levine P, et al: Neck dissection classifica-tion update: Revisions proposed by the American Head andNeck Society and the American Academy of Otolaryngology–Head and Neck Surgery. Arch Otolaryngol Head Neck Surg127:751, 2002
9. Giordano L, Sarandria D, Fabiano B, et al: Shoulder function afterselective and superselective neck dissections: Clinical and func-tional outcomes. Acta Otorhinolaryngol Ital 32:376, 2012
10. Goldstein D, Ringash J, Bissada E, et al: Scoping review of the lit-erature on shoulder impairments and disability after neck dissec-tion. Head Neck, 2013 (Epub)
11. Villaret A, Piazza C, Peretti G, et al: Multicentric prospectivestudy on the prevalence of sublevel IIb metastases in head andneck cancer. Arch Otolaryngol Head Neck Surg 133:897, 2007
12. Frierson HJ, Cooper P: Prognostic factors in squamous cell car-cinoma of the lower lip. Hum Pathol 17:346, 1986
13. Farasat S, Yu S, Neel V, et al: A newAmerican Joint Committee onCancer staging system for cutaneous squamous cell carcinoma:

632 CERVICAL SUBLEVEL IIb LYMPHATIC METASTASIS
Creation and rationale for inclusion of tumor (T) characteristics.J Am Acad Dermatol 64:1051, 2001
14. Mourouzis C, Boynton A, Grant J, et al: Cutaneous head and neckSCCs and risk of nodal metastasis—UKexperience. J Craniomax-illofac Surg 37:443, 2009
15. Corlette T, Cole I, Albsoul N, et al: Neck dissection of level IIb: Isit really necessary? Laryngoscope 115:1624, 2005
16. Talmi Y, Hoffman H, Horowitz Z, et al: Patterns of metastases tothe upper jugular lymph nodes (the ‘‘submuscular recess’’).Head Neck 20:682, 1998
17. Kraus D, Carew J, Harrison L: Regional lymph node metastasisfrom cutaneous squamous cell carcinoma. Arch OtolaryngolHead Neck Surg 124:582, 1998
18. Netterville J, Sinard R, Bryant GJ, et al: Delayed regional metasta-sis from midfacial squamous carcinomas. Head Neck 20:328,1998
19. Celik B, CoskunH, Kumas F, et al: Accessory nerve function afterlevel 2b-preserving selective neck dissection. Head Neck 31:1496, 2009
20. Koybasio�glu A, Bora Tokcaer A, Inal E, et al: Accessory nervefunction in lateral selective neck dissection with undissectedlevel IIb. ORL J Otorhinolaryngol Relat Spec 68:88, 2006
21. Wang J, Palme C, Wang A, et al: In patients with metastatic cuta-neous head and neck squamous cell carcinoma to cervicallymph nodes, the extent of neck dissection does not influenceoutcome. J Laryngol Otol 127(suppl 1):S2, 2013