Embed Size (px)
Citation preview

Laryngeal cancer

• 1% of new cancer diagnoses
• laryngeal cancer accounts for about one-fourth of head and neck cancer diagnosed annually.
• male-to-female ratio for larynx cancer is 4:1
• lower socioeconomic groups .

• The supraglottis has rich bilateral lymphatics Thus the strong tendency for supraglottic tumors to spread via lymphatics.
Supraglottic :

• There is a paucity of lymphatics and, compared with supraglottic primary neoplasms malignant glottic tumors have less a tendency for bilateral regional lymphatic spread and remain confined to the glottis for longer periods of time.

• Tobacco smoking, alcohol.
• HPV 16 / 18
• GERD implicated
• Occupational factors
• Radiation exposure
• Genetic factors
• Premalignant lesions

• Squamous cell carcinomas:
95% of all malignant laryngeal tumors

Supraglottic tumors
• asymptomatic until a relatively large tumor bulk is present . Nodal metastasis is often the initial complaint.
Glottic tumors
• tend to present early, with hoarseness as their chief complaint.
Subglottic tumors
rare and may present with stridor or hemoptysis .

Supraglottic cancer

Supraglottic cancer

Epiglottic tumor

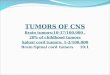
Glottic squamous cell carcinoma of the larynx. The tumor involves the anterior half of the left vocal cord.

Glottic Tumor

Glottic Tumor

Subglottic cancer

• Hoarsness • Dyspnea . • Dysphagia. • Ear pain. • Hemoptysis • Throat pain • Airway compromise • Aspiration • Neck mass

• complete head and neck examination should be performed.
• The quality of the voice is noted. A breathy voice may indicate a vocal cord paralysis and a muffled voice, a supraglottic lesion.
• Palpation : – cervical lymphadenopathy
– broadening of the laryngeal prominence
– Restricted laryngeal crepitus may be a sign of post cricoid or retropharyngeal invasion ( late stage )

• Laryngoscopy:
- mirror examination
- fiberoptic endoscope:
Malignant laryngeal lesions can appear to be fungating, friable, nodular, or ulcerative, or simply as changes in mucosal color

• Triple endoscopy and includes direct laryngoscopy, esophagoscopy, and bronchoscopy. – Assess the extent of the laryngeal tumor
– Assess the respiratory tract and upper digestive tract for synchronous primary tumors.
– To investigate cervical lymph node mets of unknown origin.
• DIRECT LARYNGOSCOPY :
Biopsies of suspected malignant sites
with cup forceps.

• CT Neck • MRI Neck • PET scan:
– Identifying occult nodal metastases,
– Distinguishing the recurrence of malignant growth from radionecrosis and other sequelae of prior treatment.
– Identifying the location of any unknown primary cancer.

Treatment
• Early : surgery or radiotherapy
• Advanced : surgery + radiotherapy

Prognosis
Early laryngeal cancer has a very good prognosis (greater than 95%) 5 year survival
Involvement of lymph nodes in the region is associated with a poorer prognosis.

Pharyngeal Cancer

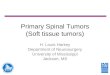
Nasopharynx The pharyngeal
recess (fossa of Rosenmüller) – most common site of NP tumour.

• The palatine tonsils are most common site of OP tumour

On either side of the
laryngeal orifice is a
recess, termed the
sinus pyriformis, which
is bounded medially
by the aryepiglottic
fold, laterally by the
thyroid cartilage and
hyothyroid membrane.
sinus pyriformis is the
most common site of hypopharyngeal CA.