Embed Size (px)
Citation preview

Paul Y. Kwo, MD, FACG
Treatment of Patients with Decompensated Cirrhosis and Liver
Transplant Recipients
Paul Y. Kwo, MD, FACGProfessor of Medicine
Medical Director, Liver TransplantationGastroenterology/Hepatology DivisionIndiana University School of Medicine
975 W. Walnut, IB 327Indianapolis, IN 46202-5121
phone 317-274-3090fax 317-274-3106email [email protected]
HCV Management in Decompensated Cirrhosis:
Current Therapies
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 1 of 15

Paul Y. Kwo, MD, FACG
Dose Adjustments in Cirrhosis
Childs Class PEG IFN alfa 2a, μg/wkPEG IFN alfa 2b,
μg/kg/wkRibavirin Daily
A 180 1.5 1000-1200 mg/day
B No No 600 mg
C No No 600 mg
Childs Class Sofosbuvir SimeprevirLedipasvir/sofosbuvir
PTV/OMB/DSB Daclatasvir
A 400 mg 150 mg 90mg/400mg75/50/12.5 mg + 250
mg60 mg
B 400 mg No* 90mg/400mg No*60 mg
C 400 mg No 90mg/400mg No60 mg
LDV/SOF + RBV: Genotype 1 and 4 with Advanced Liver Disease
Week 0 Week 12 Week 36Week 24
LDV/SOF + RBV
LDV/SOF + RBV
SVR12
SVR12
SOLAR-1
• Treatment naïve or experienced
• CPT Class B
• CPT Class C
• Post liver transplantation
SOLAR-2: (greater G4 population)
• Treatment naïve or experienced
• CPT Class B
• CPT Class C
• Post liver transplantation
•Charlton M, et al. Gastroenterology, 2015 [epub ahead of print]•Reddy RT, et al. Presented at: AASLD; November 7-11, 2014; Boston, MA. Abstract 8.•Manns M, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract G02.
SOLAR-1 and SOLAR-2
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 2 of 15

Paul Y. Kwo, MD, FACG
LDV/SOF + RBV: SVR12 in Genotype 1 or 4 with Decompensated Cirrhosis
•1. Charlton M, et al. Gastroenterology, 2015 [epub ahead of print]•2. Flamm SL, et al. Presented at: AASLD; November 7-11, 2014; Boston, MA. Abstract 239. 3. Manns M, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract G02.
LDV/SOF + RBV 12 weeks LDV/SOF + RBV 24 weeks
SOLAR-1: GT 1 and 4[1.2]
100
80
60
40
20
0
SV
R12
(%
)
CTP B CTP C
87 89 86 90
26/ 30
24/ 27
19/ 22
18/ 20n/N =
100
80
60
40
20
0S
VR
12 (
%)
CTP B CTP C
8796
20/23
22/23
85
72
13/18
17/20n/N =
SOLAR-2: GT 1[3]
AE, adverse event; CTP, Child-Turcotte-Pugh; LDV, ledipasvir; RBV, ribavirin; SAE, serious adverse event; SOF, sofosbuvir.
Comparable efficacy between SOLAR-1 and SOLAR-2 studies
LDV/SOF + RBV: Safety in Advanced Liver Disease Pre OLT
Treatment-related serious adverse events (SAEs) mostly related to RBV
No deaths or D/C attributed to treatment with study drug (LDV/SOF)
•Samuel D, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Poster P0774.
SOLAR-1 and SOLAR-2
Safety Outcome, n (%) Pretransplant CPT B + C (n = 215)
Grade 3/4 AE 51 (24)
SAE 61 (28)
Serious treatment-related AE 5 (2)
AE leading to discontinuation of LDV/SOF >2 patients
HCCSepsis
9 (4)
2 (<1)2 (<1)
Death 10 (5)
Liver Transplantation 11 (5)
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 3 of 15

Paul Y. Kwo, MD, FACG
LDV/SOF + RBV: Change in MELD Score from Baseline to Follow-up Week 4 in CPT B or C Disease
•Manns M, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract G02.
*Missing FU-4: n = 24.
Pre/Post-Transplantation (CPT B and C; n = 136)*
Ch
ang
e in
ME
LD
Sco
re
4
2
0
-2
-4
-6
-8
-10(-11)
(-17)
n = 18
(8)
**
*
SOLAR-2
Real-World Efficacy of SOF/SMV ± RBV & SOF/RBV Regimens in Cirrhosis Pts With MELD >10
HCV-Target Network: North America, Germany, Israel
GT1 Naive GT 1Exp’d
MELD 10-15 MELD 16-21 MELD > 21
100
80
60
40
20
0
SV
R12
(%
)
3/7
31/40
6/10
8/14
21/26
37/67
67/92
19/28
5573 6860
5768
7843
5/8
7/10
2/3
63 7067
0/1
6/6
1/1
100 100
n/N =
SOF + RBV (n = 102) SOF + SMV (n = 117) SOF + SMV + RBV (n = 34)
48/67
72
8/14
48/67
13/19
81GT 2 GT 3
39
10/26
HCV TARGET•Reddy RK, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract O007.
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 4 of 15

Paul Y. Kwo, MD, FACG
HCV TARGET: SAEs, Death, Liver Transplantation
SOF/RBVN=88
SOF/SMVN=114
SOF/SMV/RBV N=32
Total N=234
Total patients with SAEs N (%) 27 (31) 8 (7) 9 (26) 44 (17)
Hepatic decompensation* 10 (11) 2 (2) 4 (12) 16 (6)
Infections 0 2 (2) 1 (3) 10 (4)
Death 0 2 (2) 1 (3) 3 (1)
Unspecified 0 0 1 (3) 1 (0.4)
Hepatic Failure 0 1 (1) 0 (0) 1 (0.4)
Shock 0 1 (1) 0 1 (0.4)
Underwent OLT on treatment 4 (5) 3 (3) 5 (16) 12 (5)
*Hepatic encephalopathy, variceal bleeding, hepatic failure, hepatic hydrothorax, bacterial peritonitis
Reddy RK, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract O007.
ALLY-1: SOF + DCV + RBV for 12 Weeks in Patients With Genotype 1 HCV and Cirrhosis
Child-Pugh score: A, B, or C
MELD scores 8-40
Hepatocellular carcinoma allowed•Poordad F, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract LO8.
SV
R12
, %
92 94
56
0
20
40
60
80
100
A B C
Child-Pugh class
All Genotypes
11/12 30/32 9/16
SV
R12
, %
ALLY-1
• Treatment naïve or treatment experienced adults with any HCV genotype
• DAA failures allowed, except NS5A
76100
80 83100
0
20
40
60
80
100
1a 1b 2 3 4Genotype
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 5 of 15

Paul Y. Kwo, MD, FACG
•11
92.0 94.0
56.0
0
20
40
60
80
100
A B C
•Child-Pugh class
91.3 95.7
78 76
90.983.7
89.297
75 75
56
100
73
No Yes No Yes >3.5 2.8
to
3.5
<2.8
SVR12 by Baseline Disease SeverityS
VR
12, %
<1.7 1.7
to
2.3
>2.3 <2.0 2.0
to
3.0
>3.0
Ascites HE Albumin, g/dL INR T bili, mg/dL
•
SVR12 by Child-Pugh Class
Advanced cirrhosis cohort, all genotypes
•HE = hepatic encephalopathy
Treatment of Decompensated HCV Cirrhosis in Patients with Diverse Genotypes: 12 weeks Sofosbuvir and NS5A inhibitors
With/Without Ribavirin Non-randomized observational cohort study of National Health Service of England (N = 467)
Patients received 12 weeks SOF + LDV or DCV ± RBV at treating MD discretion (non-randomized)
•Foster GR, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract O002.
12-wk SOF + LDV + RBV 12-wk SOF + LDV 12-wk SOF + DCV + RBV 12-wk SOF + DCV
N =
100
80
60
40
20
0All GT1 GT3
SV
R12
, % (
ITT
)
P<.05
59
43
70 71
252 28 172 15 164 21 45 5 61 7 114 7
80 71 74 73
86 81 82
60
DCV, daclatasvir; GT, genotype; HCV, hepatitis C virus; ITT, intent to treat.
Other GT
100
3
8589
27 13
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 6 of 15

Paul Y. Kwo, MD, FACG
European Compassionate Use Program (CUP): SOF + DCV ± RBV for 24 Weeks
Treatment naive or treatment experienced
– CP Category: 57% CP A; 36% CP B; 6% CP C
– MELD Scores: >50% had MELD Scores ≥ 9 and <15
DCV dose determined by country; inclusion of RBV based on physician discretion•Welzel TM, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract P0772.
n/N =
100
80
60
40
20
0A B C
SV
R12
, %
100 100 100
39/40
19/20
58/60
97 95 97 100 95 98
24/24
21/22
45/46
1/1 1/1 2/2
CP Score
24-wk DCV + SOF + RBV24-wk DCV + SOF All patients
Phase 2, nonrandomized, open-label study
30 patients with HCV G1 infection and CP-B cirrhosis
10 noncirrhotic patients with HCV G1 infection were enrolled for PK analyses
GZR and EBR administered as separate entities (FDC not used in C-SALT)
– GZR 50 mg utilized in C-SALT, modelled upon the exposure of GZR in non-HCV-infected CP-B patients
EFFICACY AND SAFETY OF GRAZOPREVIR AND ELBASVIR IN HEPATITIS C GENOTYPE 1 INFECTED PATIENTS WITH CHILD-PUGH CLASS B CIRRHOSIS
•Follow-up:
•Primary endpoint:
•SVR12• HCV RNA <15 IU/mL
•(COBAS TaqMan v2.0 [LLoQ 15 IU/mL])
•GZR 50 mg / EBR 50 mg
•GZR 100 mg / EBR 50 mg
•D1 •TW4 •TW8 •TW12 •FUW4 •FUW8 •FUW12
•n=30
•Child-Pugh B
•n=10
•Noncirrhotic
•CP=Child-Pugh; EBR=elbasvir; GZR=grazoprevir; LoQ=limit of quantification; PK=pharmacokinetic; SVR=sustained virologic response
•Jacobson Presented at EASL ; April 22-26, 2015; Vienna, Austria
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 7 of 15

Paul Y. Kwo, MD, FACG
SVR-12: C-SALT SAFETY RESULTS
Study DesignASTRAL-4 Childs B Cirrhosis
Open-label, randomized (1:1:1) US study
GT 1-6 treatment-naïve or -experienced patients with CPT B cirrhosis
Eligibility criteria: CrCL >50 mL/min, platelets >30,000 x 103/μL; no HCC or liver transplant
Weight-based RBV dosing (1000 or 1200 mg/day)
•Wk 0 •Wk 12 •Wk 24
SOF/VEL •SVR12
•Wk 36
SOF/VEL + RBV •SVR12
SOF/VEL •SVR12
n=75
n=75
n=75
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 8 of 15

Paul Y. Kwo, MD, FACG
Results: SVR12 in GT 1 PatientsASTRAL-4
8896 92
0
20
40
60
80
100
•SOF/VEL+ RBV
•12 week
•SOF/VEL
•24 week
•65/68 •65/71
•SOF/VEL
•12 week
•60/68
•5 relapse
•2 death
•1 LTFU
•1 relapse
•2 deaths
•3 relapse
•3 LTFU
SVR-12
Results: SVR12 in GT 3 PatientsASTRAL-4
50
85
50
0
20
40
60
80
100
SOF/VEL+ RBV
12 week
SOF/VEL
24 week
•11/13 •6/12
SOF/VEL
12 week
•7/14
•6 relapses
•1 death
•1 breakthrough
•1 relapse
•1 breakthrough
•4 relapse
•1 death
SVR
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 9 of 15

Paul Y. Kwo, MD, FACG
Post liver transplant treatment of HCV infection
Post transplant Drug interactions: DAAs as Culprits
•Dick TB, et al. Hepatology. 2015. [Epub ahead of print]
MedicationCyclosporine Tacrolimus Sirolimus Everolimus
Cmax AUC Cmax AUC Cmax AUC Cmax AUC
Ribavirin
Ledipasvir ND ND ND ND ND ND
Sofosbuvir 27% 9% ND ND ND ND
Simeprevir 16% 19% 24% 17% ND ND ND ND
Daclatasvir 4% 3% 5% ND ND ND ND
3D Regimen 1% 482% 299% 5613%Expected increase in both Cmax and
AUC.
Expected increase in both Cmax and
AUC.
•HCV infection inhibits cytochrome P450 through direct and indirect mechanisms. SVR leads to lower CNI levels
and risk of ACR.
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 10 of 15

Paul Y. Kwo, MD, FACG
Post transplant Drug interactions: DAAs as Victims
•Dick TB, et al. Hepatology. 2015. [Epub ahead of print]
(CYA and TAC affect DAA metabolism or transport)
MedicationDaclatasvir Ledipasvir Sofosbuvir Simeprevir
Cmax AUC Cmax AUC Cmax AUC Cmax AUC
Cyclosporine 4% 40% ND ND 154% 353% 374% 481%
Tacrolimus 7% 5% ND ND 3% 13% 79% 85%
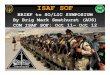
SOLAR-1: SVR12 Rates in OLT Patients Receiving LDV/SOF + RBV
In the 24-week arm, 8 patients with CPT B and 1 patient with CPT C have not reached the follow-up week 12 visit
MELD scores improved from baseline through follow-up Week 4 in 15/48 patients with CPT A and 8/41 patients with CPT B disease
Reddy RT, et al. Hepatology. 2014;60(suppl): Abstract 8.
100
80
60
40
20
0F0-F3 CPT A CPT B CPT C
12 wks LDV/SOF + RBV24 wks LDV/SOF + RBV
96 98 96 9683 60
6785
SV
R12
(%
)
53/55
55/56
25/26
24/25
22/26
15/18
3/5
2/3n/N =
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 11 of 15

Paul Y. Kwo, MD, FACG
Solar-2: LDV/SOF + RBV: SVR12* in Genotype 1 or 4
. Manns M, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract G02.
LDV/SOF + RBV 12 weeks LDV/SOF + RBV 24 weeks
SOLAR-2: GT 1
100
80
60
40
20
0
SV
R12
(%
)
F0-F3, CPT A CTP B&C
96 98 88 89
72/75
57/ 58
57/ 65
54/ 61n/N =
100
80
60
40
20
0S
VR
12 (
%)
CTP B&C
91100
10/11
7/7
57
86
6/74/7n/N =
SOLAR-2: GT 4
Comparable efficacy between 12 and 24 week durations
F0-F3, CPT A
-8
-6
-4
-2
0
2
4
Change in MELD ScoreSOLAR-1: LDV/SOF + RBV in Post Transplant
Missing FU-4: n=3 CTP A 12 wk; n=5 CTP B 12 wk; n=5 CTP B 24 wk
•Change from Baseline to Follow-Up Week 4
•CTP A Patients (n=48) •CTP B Patients (n=41)
•n=4 •n=1
-8
-6
-4
-2
0
2
4
•n=9 •n=4
•(-11)
•12 Wk (n=23) •24 Wk (n=25) •12 Wk (n=21) •24 Wk (n=20)
Reddy, AASLD, 2014, Oral #8
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 12 of 15

Paul Y. Kwo, MD, FACG
Ally-1: SOF +DCV+RBV 600 Post OLT
SVR12 by HCV Genotype
94.0 9790 91
100
0
20
40
60
80
100
10/11 1/1
SV
R12
, %
Overall 1a 1b
Genotype
3 6
N = 53
50/53 30/31 •9/10
•Poordad F, et al. Presented at: EASL; April 22-26, 2015; Vienna, Austria. Abstract LO8.
SOF +DCV+RBV 600 Post OLTInterim SVR12 Results
Post-transplant CohortDCV + SOF DCV + SOF + RBV All patients
89
100
89
100 10091 91
0
20
40
60
80
100
GT 1 GT 3 All GT
•SV
R 1
2, %
•11
•2528
•66
•3033
•11
•3134
•2427
•Relapse, n=1Deaths, n=2
■ NS5A sequencing (population-based) in relapse patient identified Y93S RAV
•HCV genotype
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 13 of 15

Paul Y. Kwo, MD, FACG
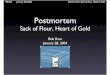
CORAL-1: GT1 Patients After Liver Transplantation (F0-F2)
PTV/OMB/DSB: co-formulated paritaprevir/r/ombitasvir, 150 mg/100 mg/25 mg QD; dasabuvir, 250 mg BID
RBV: dosing was managed at the discretion of the investigator and closely monitored per protocol
Tacrolimus 0.5 mg q 1-2 weeks, Cyclosporin reduced to 20% of daily dose
Day 0 Week 24
SVR12
To Week 72
PTV/OMB/DSB + RBV
(n=34)
Kwo PY, et al. N Engl J Med. 2014;371(25):2375-2382.
CORAL-1: SVR Rates in GT1 Liver Transplant Patients
No patient had breakthrough
One patient had a relapse (post-treatment day 3)
– At the time of relapse, this patient had R155K in NS3 protease, M28T+Q30R in NS5A, and G554S+G557R in NS5B, none of which were present at baseline
Study now including F3-F4, 12 week duration
100% 97% 97% 97%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
EOTR SVR4 SVR12 SVR24
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 14 of 15

Paul Y. Kwo, MD, FACG
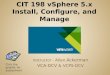
CirrhoticGenotype
1a 1b
MELD
<10 ≥ 10
Overall Tx
Experienced
Yes No
0
100
80
60
40
20
94/104
90%
52/60 42/44
87%95%
51/58
88%
27/28
96%
59/67 35/37
Yes
88%
No
19/21 8/10
HCV-TARGET – Post TransplantHCV RNA Outcomes for SOF+SMV±RBV:
Genotype 1 interim analysis
95% 90%80%
SV
R %
Summary
Patients with decompensated cirrhosis may be treated successfully across all genotypes
– SVR rates are good, lower than compensated cirrhosis
– SOF/RBV, SOF/LDV ± RBV 12-24 weeks, SOF/DCV ± RBV 12-24 weeks
– Carefully consider who to treat in transplant setting to avoid MELD purgatory
Post Liver Transplant
– No graft should fail due to recurrent HCV across all genotypes
– 12 weeks of SOF/LDV/RBV or SOF/DCV/RBV
– 24 weeks of SOF/LDV or SOF/DCV
– 24 weeks of PTV/OMB/DSV/RBV
ACG 2016 Midwest Hepatitis School Copyright 2016 American College of Gastroenterology
Page 15 of 15