Embed Size (px)
Citation preview

Haykowsky and Lee W. JonesJessica M. Scott, Susan Lakoski, John R. Mackey, Pamela S. Douglas, Mark J.
Molecularly Targeted Cancer TherapeuticsThe Potential Role of Aerobic Exercise to Modulate Cardiotoxicity of
doi: 10.1634/theoncologist.2012-0226 originally published online January 18, 20132013, 18:221-231.The Oncologist
http://theoncologist.alphamedpress.org/content/18/2/221located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

ABSTRACT
Molecularly targeted therapeutics (MTT) are the future ofcancer systemic therapy. Theyhavealreadymoved frompalli-ative therapy for advanced solidmalignancies into the settingof curative-intent treatment for early-stage disease. Cardio-toxicity isa frequentandpotentially seriousadversecomplica-tion of some targeted therapies, leading to a broad range ofpotentially life-threatening complications, therapy discontin-uation, and poor quality of life. Low-cost pleiotropic interven-tions are therefore urgently required to effectively preventand/or treat MTT-induced cardiotoxicity. Aerobic exercisetherapyhas theuniquecapacity tomodulate,without toxicity,
multiple gene expression pathways in several organ systems,including a plethora of cardiac-specificmolecular and cell-sig-nalingpathways implicated inMTT-inducedcardiac toxicity. Inthis review, we examine themolecular signaling of antiangio-genic andHER2-directed therapies thatmay underpin cardiactoxicity and the hypothesized molecular mechanisms under-lying the cardioprotective properties of aerobic exercise. It ishoped that this knowledge can be used to maximize the ben-efits of small molecule inhibitors, while minimizing cardiacdamage in patients with solid malignancies. The Oncologist2013;18:221–231
Implications for Practice: Cardiotoxicity, a frequent and devastating adverse complication of somemolecularly targeted thera-pies (MTTs), can lead to potentially life-threatening cardiovascular complications, therapy discontinuation, and poor quality oflife. In non-cancer patients with left ventricular dysfunction and heart failure, aerobic exercise is one of themainstay clinical in-terventions for the prevention and treatment of cardiovascular disease. However, few studies have investigated the efficacy ofaerobicexercise in thepreventionand/or treatmentofMTT-inducedcardiac injury. This topic isofparticular importancebecausecardiac function isa strongpredictorof cardiovascularandall-causemortality,qualityof life, and fatigue,andmaybeevencancer-specificmortality. Here,weprovide a comprehensive overviewof cardiacmolecular and cell-signaling pathways specific toMTT-induced cardiac toxicity. This review also outlines many pertinent aerobic exercise-induced molecular signaling pathways thatmayuniquelyprevent and/or treatMTTcardiac injury.Overall, informationpresented in this reviewprovides critical informationfor basic scientists, clinicians, and exercise oncology researchers who are investigating the application of exercise in cancer con-trol.
INTRODUCTION
The emergence of molecularly targeted therapeutics (MTTs)hasrevolutionizedthemanagementofsolidmalignancies.An-tiangiogenic and human epidermal growth factor receptor 2(HER2)-directedMTTsareapprovedby theU.S. FoodandDrugAdministration (FDA) for the treatment of several solidmalig-nancies, either as monotherapy or in combination with stan-dard chemotherapy [1, 2]. The biologic selectivities of thesedrugs were expected to substantially reduce off-target toxic-ity, although it is now apparent that MTTs cause adverse car-diovascular consequences, such as hypertension andprogressive left ventricular (LV) dysfunction, ultimately lead-ing to symptomatic heart failure.
Several excellent reviews have described the biologic andmolecular mechanisms underlying MTT-induced cardiotoxic-ity and risk for cardiotoxicity [1–8]; however, comparably lit-tleattentionhasbeen focusedonstrategies topreventand/ormitigate anticipated injury. MTTs target multiple cellularpathways including highly coordinated myocardial molecularsignaling. Pleiotropic interventions will therefore be requiredto effectively prevent and/or treat MTT-induced cardiotoxic-ity. Aerobic exercise therapy has the unique capacity tomod-ulate, without toxicity, multiple gene expression pathways inseveral organ systems, including aplethora of cardiac-specificmolecular and cell-signaling pathways implicated in MTT-in-
Correspondence: JessicaM. Scott, Ph.D., Exercise Physiology and Countermeasures, NASA Johnson Space Center, Universities Space ResearchAssociation, 2101 NASA Parkway, Houston, TX 77058, USA. Telephone: 281-483-8398; Fax: 281-483-4181; e-mail: [email protected] March 29, 2012; accepted for publication September 5, 2012; first published online in The Oncologist Express on January 18, 2013.©AlphaMed Press 1083-7159/2013/$20.00/0 http://dx.doi.org/10.1634/theoncologist.2012-0226
ThePotential RoleofAerobic Exercise toModulateCardiotoxicityofMolecularly TargetedCancerTherapeuticsJESSICAM. SCOTT,a SUSAN LAKOSKI,b JOHN R.MACKEY,c PAMELA S. DOUGLAS,dMARK J. HAYKOWSKY,c LEEW. JONESdaNASA Johnson Space Center, Universities Space Research Association, Houston, Texas, USA; bUniversity of Texas SouthwesternMedical Center, Dallas, Texas, USA; cUniversity of Alberta, Edmonton, Alberta, Canada; dDukeUniversityMedical Center, Durham,North Carolina, USADisclosures of potential conflicts of interestmay be found at the end of this article.
KeyWords. Exercise • Cardiotoxicity • Molecular therapeutics • Solidmalignancies
TheOncologist®
SymptomManagement and Supportive Care
TheOncologist2013;18:221–231 www.TheOncologist.com ©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

duced cardiac toxicity. Here we reviewmolecular signaling ofantiangiogenic and HER2-directed therapies that may under-pin cardiac toxicity and the hypothesized cardioprotectiveproperties of aerobic exercise.
THEBIOLOGY OF TYROSINEKINASESReceptor tyrosine kinases (RTKs) are enzymes that act as criti-calmediators of normal cellular signal transduction and regu-latediverse cellularprocesses including cell cycleprogression,metabolism, transcription, and apoptosis (reviewed exten-sively elsewhere [9, 10]). All RTKs are embedded in plasmamembranes and consist of an extracellular ligand-binding do-mainandan intracellular kinasedomain.RTKsarenotonly keyregulators of normal cellular processes, but they also are cen-tral to malignant transformation and tumor proliferationwhen constitutively activated via gene amplification, overex-pression, or mutations [11]. Strategies for the prevention orinterception of deregulated RTK signaling include the devel-opment of selective agents that target either the extracellularligand-binding domain or the intracellular tyrosine kinasebinding region [2, 4]. Monoclonal antibodies (mAbs) are de-signed to inhibit kinaseactivationbybinding to theextracellu-lar portion of RTKs or by binding to growth factor ligands thatactivate RTKs. Mechanistically, anti-RTK mAbs block the li-gand-receptor interaction, thus inhibiting activation of the ty-rosine kinase domain, and/or induce downregulation ofreceptor expression [12]. In contrast, small-molecule tyrosinekinase inhibitors (TKIs) bind to the intracellular portion ofRTKs, thereby inhibiting the phosphorylation of downstreamsubstrates.
MECHANISMS OFHER2-DIRECTEDTHERAPYCARDIAC INJURYOverexpression and/or gene amplification of the RTK HER2(also known as ErbB2) is present in approximately 20% ofwomenwith breast cancer [13], aswell as approximately 10%and 5%of patients with non-small cell lung cancer, [14] andgastric cancer, respectively [15]. Randomized trials demon-strate that HER2-directed agents cause significant im-provements in disease-free survival and overall survivalamong women with early [16, 17] and metastatic [18]HER2-positive breast cancer. However, trastuzumab (thefirst FDA-approvedHER2-directedmAb) andpertuzumab (anewer mAb in phase III testing) are associated with cardiactoxicity (Table 1).
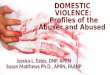
HER2-DIRECTEDTHERAPY INHIBITION OF CARDIACMOLECULAR SIGNALINGWe focus here on the putative role of ErbB2 and transforminggrowthfactor� (TGF�) signalingasmajorpathwaysmediatinganti-ErbB2 cardiotoxicity (Fig. 1).
ErbB2ErbB2belongstothefamilyofhumanepidermalgrowthfactor(EGF) receptorscomprisedof theEGFreceptor (ErbB1),ErbB2,ErbB3, and ErbB4 [19]. Hyperactivation of the ErbB2/ErbB3/PI3K complex in tumor cells leads to upregulation of the phos-phatidylinositol 3-kinase (PI3K)-Akt pathways resulting incellular proliferation [20], increased mitogen-activated pro-tein kinase (MAPK) activity causing protein hypertrophy [21],and reduced cytostasis via CCAAT/enhancer-binding protein
(C/EBP�) [22]. The antiproliferative activity of HER2-directedtherapy is therefore based on disruption of the ErbB2-ErbB3complex in tumor cells, thus reducing intracellular Akt activity[19, 23] and MAPK signaling [24]. Conversely, HER2-directedtherapy dramatically alters cardiomyocyte function and/orsurvival via inhibition of Nrg1/ErbB/Akt signaling.
The essential role of ErbB2 signaling for cardiomyocyteproliferation was first revealed through germline deletion ofErbB2 receptors inmice, which proved lethal inmid gestationwith failure of proper ventricle formation [25]. Transgenicmice with cardiac-specific deletion of ErbB2 after cardiac de-velopment survive embryogenesis [25] but develop progres-sive cardiomyopathy in adulthood [16]. In the healthy heart,neuregulin-1� (Nrg1) is released by endocardial and myocar-dial endothelialmicrovascular cells and binds to ErbB4on car-diomyocytes leading to activation of the ErbB2/ErbB4/PI3K/Akt complex. HER2-directed agents inhibit Nrg1release [26] and significantly decrease both total and phos-phorylated Akt in neonatal rat cardiomyocytes [27], thuspotentially limiting cell growth, glucose uptake, and pro-tein regulation [28–30] and ultimately triggering the pro-gression of heart failure [31].
TGF�During carcinogenesis, TGF� signaling initially preventsmalignant progression via the small mother against decap-entaplegic (Smad) pathway [32]. Eventually, malignantcells overexpressing ErbB2 circumvent the growth-sup-pressive effects of TGF� by downregulating TGF� receptorsoralteringdownstreampathways [22]. In theheart, TGF� reg-ulates ventricular remodeling (cardiomyocyte hypertrophy)via activation of the Smad/3 and4 complexes andmatrixmet-alloproteinases [33]. Inhibition of ErbB2 signalingwith trastu-zumab also activates TGF� and C/EBP� signaling in breastcancer cells [22]. Whether trastuzumab induces TGF� andC/EBP� signaling in cardiomyocytes is unknown; however, in-creased cardiac TGF� and C/EBP� expression results in path-ological remodeling [34].
AEROBIC EXERCISE-INDUCED CARDIOPROTECTION FROMHER2-DIRECTEDAGENTSFigure 2 outlines the modulation of ErbB and TGF� signalingthrough aerobic exercise. The cardioprotective properties ofincreasedNrg1/ErbB signaling arewell described [26, 29]. Forexample, drug-induced enhancement of myocardial Nrg1/ErbB signaling significantly improved both cardiac perfor-mance and survival in four different rodent models of LVfailure [31]and induceddifferentiatedcardiomyocytes topro-liferate [35]. In vitro studies in isolated cardiac endothelialcells (themain sourceofNrg1 in theheart) showthatmechan-ical strain increases endothelial Nrg1 synthesis and release[36],whereasNrg1 release is directly inhibited by angiotensinII and adrenergic agonists [37]. Aerobic exercise increases en-docardialmechanical strain [38]withaconcomitant reductioninangiotensin II [39]. Interestingly, Lebrasseuretal. [40] foundthat resistance or aerobic exercise increased proteolytic pro-cessing of mature Nrg1 transmembrane protein to solubleNrg1 in rat skeletal muscle. Thus, we contend that increasedNrg1synthesis in theventricle in responsetoexercise-inducedmechanical stress will evoke suppression of neurohormonalfactors, leading to cardioprotection.
222 Targeted Therapy, Cardiotoxicity, and Exercise
©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

Figure 1. Mechanisms underlying HER2-directed therapy cardiotoxicity. Inhibition of ErbB receptorswith HER2-directed therapies im-pacts numerous signaling pathways resulting in suppression of myofilament protein synthesis via the PI3K-Akt pathway (pathway A),suppression of protein hypertrophy via the MAPK pathway (pathway B), suppression of cell survival via Src/Fak pathway (pathway C),suppression of myofilament protein synthesis and upregulation of protein degradation via TGF-�1 and C/EBP� signaling (pathway D),and alterations in cardiac energymetabolism via downregulation of AMPK (pathway E).
Abbreviations: AMPK, AMP-activated protein kinase; C/EBP�, CCAAT/enhancer binding protein; Fak, focal adhesion kinase;MAPK,mitogen-activatedprotein kinase;Nrg1,Neuregulin-1�; PI3K, phosphatidylinositol 3-kinase; Smad, smallmotheragainstdecapentaple-gic; TGF�, transforming growth factor�.
Table 1. Incidence of cardiotoxicity in HER2-directed and angiogenesis inhibitor clinical trials
Agent Class Target Malignancy Heart failureSubclinical decline inejection fraction (≥ 10%)
Hypertension(≥ grade I)
HER2-directed
Trastuzumab mAb ErbB2 ErbB2� breast cancer,MGC (phase III)
1.7%–4% (early) �89, 908.3%–20% (advanced)�16, 91–95��
2.1%–14% (early) �89�16%–18% (advanced)�16, 92–96�
NA
Lapatinib TKI ErbB1, ErbB2 ErbB2� breast cancer,NSCLC (phase II)
0.2% (advanced) �97� 1.4%–5% (advanced)�97, 98�
4% (advanced) �99�
Pertuzumab mAb ErbB2 ErbB2� breast cancer(phase II)
9% (advanced) �100� 1.2%–54% (advanced)�91, 100–102�
NA
Angiogenesis inhibitors
Bevacizumab mAb VEGF RCC, NSCLC, glioblastoma,CRC, breast
2.2%–3% (advanced)�103, 104�
2%–14% (early) �105–1070.8%–23.5% (advanced)�103, 104, 108��
2%–12% (early) �106, 109�17.9%–35% (advanced)�103, 104, 110�
Ramucirumab mAb VEGFR RCC (phase II), breast(phase III)
NA NA 13.5% (advanced) �111�
Sunitinib TKI VEGFR 1–3, c-kit,PDGFR
RCC, GIST 2.7%–11% (advanced)�62, 112�
4%–47% (advanced)�62, 112�
5%–47% (advanced)�62, 113, 114�
Sorafenib TKI VEGFR 2, PDGFR,Raf1
RCC,melanoma NA 18.9% (advanced) �115� 7.2%–43% (advanced)�116–119�
Pazopanib TKI VEGFR, c-kit, PDGFR RCC, breast (phase II) NA NA 14%–40% (advanced )�120, 121�
Cediranib TKI VEGFR 1–3, c-kit RCC, breast, and liver (allphase II)
NA NA 21%–81% (advanced)�122–124�
Vandetanib TKI VEGFR, EGFR MTC, NSCLC (phase III),mHRPC (phase II)
NA NA 14%–29% (advanced)�125–127�
Motesanib TKI VEGFR, PDGFR, c-kit MBC (Phase II) NA 9% (advanced) �128� 12% (advanced) �128�
Axitinib TKI VEGFR, PDGFR, c-kit Pancreatic, (phase III),MBC (phase II)
NA 1.8% (advanced) �129� 7%–27.9% (advanced)�129, 130�
Abbreviations: CRC, colorectal cancer; GIST, gastrointestinal stromal tumor; HF, heart failure;mAb,monoclonal antibody;MBC,metastatic breastcancer;MGC,metastatic gastric cancer;mHRPC,metastatic hormone-refractory prostate cancer;MTC,metastaticmedullary thyroid cancer, NA,not available; NSCLC, non-small-cell lung cancer; RCC, renal cell carcinoma; TKI, tyrosine kinase inhibitor.
223Scott, Lakoski,Mackey et al.
www.TheOncologist.com ©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

Aerobic exercisemay alsomodulate a number ofmyocar-dial intracellular processes, thus overcoming HER2-inhibitorreceptor blockade.McMullen et al. [41, 42] elegantly demon-strated that exercise increases myocardial Akt, with subse-quent attenuation of pathologic LV remodeling, fibrosis, andprotein degradation. Whether similar processes occur dur-ing administration of targeted cancer therapeutics has notbeen investigated; however, exercise training increasesmyocardial PI3K activity [43] with an effective reduction ininfarct size and cardiomyocyte apoptosis in rats subjectedto myocardial ischemia reperfusion [44], as well as improveslifespan in mice with dilated cardiomyopathy [45]. These in-vestigations provide evidence for the protective effects ofPI3K/Akt signaling insettingsof targetedtherapy-inducedcar-diac stress.
Finally, aerobic exercise inhibits TGF� and C/EBP� signal-ing to effectively prevent and/or attenuate pathological car-diac hypertrophy in various mouse models. For instance,aerobicexerciseattenuates isoprenaline-induced increases inmyocardial levels of TGF� andC/EBP�mRNA,with parallel in-hibition of pathological myocardial hypertrophy [34]. Exer-cise-induced reduction of TGF� and C/EBP� expression, inturn, increases both cardiomyocyte size and cell division re-sulting in physiological hypertrophy [34]. Interestingly, exer-cise or experimental downregulation of C/EBP� expressionhas also been shown to upregulate GATA4, a regulator of car-diomyocyte proliferation during myocardial regeneration inzebrafish [46]. Thesedata indicate that aerobic exercise inhib-
its TGF-�1andC/EBP�expressionandupregulatesGATA4, ul-timately leading to modulation of protein degradation andupregulation of protein synthesis.
In the only human study examining MTTs and exercise todate, our group found that 16 weeks of supervised aerobictraining failed to attenuate trastuzumab-induced LV dilationand reduced ejection fraction in patients with HER2-positiveoperable breast cancer [47]. This observation is in contrast toworkbyusandothersdemonstrating thataerobic trainingcanreverseLVremodeling inpatientswithstableheart failure [48,49]. These discordant findings were likely due to the fact thatparticipants in the trastuzumab trial attended an insufficientnumber of training sessions anddid not receive a high enoughtraining stimulus to achieve beneficial adaptations.
MECHANISMS OFANGIOGENESIS INHIBITIONDIRECTEDTHERAPY-INDUCED CARDIAC INJURYAngiogenesis, the formation of new capillary blood vessels, ispredominantly regulated via vascular endothelial growth fac-tor (VEGF) and is fundamental for bothphysiologic andpatho-logic processes (reviewed extensively in references [50, 51]).VEGF inhibition, alone or in combination with conventionalchemotherapy, is now approved by the FDA as first-line ther-apy for abroad rangeof advancedsolidmalignancies [50]. Theincidence andmagnitude of cardiac injury withmultitargetedTKIs is particularly high, whereas treatment with monoclonalmAbs appears to cause comparably less injury (Table 1).
Figure 2. Mechanisms underlying modulation of HER2-directed therapy cardiotoxicity through aerobic exercise. Aerobic exercise in-duces cardioprotection via upregulation of Nrg1 synthesis and release, thus activating pathways A–C; inhibition of TGF-�1 and C/EBP�signaling and upregulation of GATA4 (pathway D); and activation of AMPK expression (pathway E).
Abbreviations: AMPK, AMP-activated protein kinase; C/EBP�, CCAAT/enhancer binding protein; Fak, focal adhesion kinase;MAPK,mitogen-activatedprotein kinase;Nrg1,Neuregulin-1�; PI3K, phosphatidylinositol 3-kinase; Smad, smallmotheragainstdecapentaple-gic; TGF�, transforming growth factor�.
224 Targeted Therapy, Cardiotoxicity, and Exercise
©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

Figure 3. Mechanismsunderlying anti-angiogenic therapy cardiotoxicity. InhibitionofVEGF signalingwith tyrosine kinase inhibitor-directedtherapies impacts numerous signaling pathways resulting in inhibition of angiogenesis, and protein synthesis and degradation via the PI3K-Akt-NO pathway; and inhibition of cell proliferation and differentiation via theMAPK-ERK pathway. Monoclonal inhibitors include bevaci-zumaband ramucirumab;multikinase inhibitors include sunitinib, axitinib, pazopanib,motesanib, vadetanib, and sorafenib.
Abbreviations:MAPK,mitogen-activated protein kinase; NO, nitric oxide; PI3K, phosphatidylinositol 3-kinase; VEGF, vascular endo-thelial growth factor.
Figure4. Mechanismsunderlying anti-angiogenic therapy cardiotoxicity throughaerobic exercise. Aerobic exercise induces cardiopro-tection via upregulation of VEGF expression; a nitric oxide-dependant increase in endothelial progenitor cells; and activation of STAT3resulting in erythropoietin secretion and binding to cardiac progenitor cells, causing differentiation into endothelial cells.
Abbreviations: CPC, cardiac progenitor cells; MAPK, mitogen-activated protein kinase; NO, nitric oxide; PI3K, phosphatidylinositol3-kinase; EC, endothelial cell; EPO, erythropoietin; VEGF, vascular endothelial growth factor.
225Scott, Lakoski,Mackey et al.
www.TheOncologist.com ©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

ANTIANGIOGENIC THERAPY INHIBITION OF CARDIAC ANDVASCULARMOLECULAR SIGNALINGPutative pathways underlying the cardiotoxic properties ofmonoclonal andmultitargetedagents are illustrated inFigure3.
Monoclonal InhibitionCirculatingVEGFbinds to its receptorsplateletderivedgrowthfactor receptor (PDGFR), VEGFR1 (also known as Flt-1), andVEGFR2 (also knownas Flk-1orKDR).Monoclonal therapeuticinhibition of the VEGF pathway is achieved via antibodies tar-geting a VEGF ligand (e.g., bevacizumab binding to VEGF), de-coy receptors for VEGF (e.g., aflibercept), or antibodiestargeting the extracellular domain of VEGFRs (e.g., ramuci-rumab binding to VEGFR2), thus limiting endothelial cellsprouting, migration, proliferation, and tube formation [52].Of importance, suppression of VEGF/VEGFR signaling causespathological alterations in cardiac and vascular tissues [53,54]. For instance, global VEGF knockout in rodents causes em-bryonic lethality [55],whereas postnatalmurine downregula-tion of myocardial VEGF expression initiates a cascade ofevents leading toprogressivediastolicandsystolic LVdysfunc-tion [43]. Cardiac-specific VEGF knockoutmice display abnor-malcardiacmusclecapillaritynumber [56]andclassic features
of cardiomyopathy (i.e., reduced cardiac output, fractionalshortening, decreased dP/dt) [57]. Physiologically, cardiomyo-cyte binding of VEGF activates Akt, initiating signaling pathwaysregulatingnitricoxide (NO)synthase,angiogenesis, andprogeni-tor cell differentiation into cardiomyocytes [58–60]. Anti-VEGFagents likely inhibit vascular NO release, thus promoting vaso-constriction, increased peripheral resistance, and increasedblood pressure, [53], as well as limiting endothelial progen-itor cell (EPC) [59] and cardiac progenitor cell (CPC) [61] de-velopment and ultimately restraining cardiomyocytedifferentiation.Unfortunately, limited clinical data andmech-anistic information are available to substantiate these poten-tial pathways.
Multitargeted InhibitionMultitargetedTKIsmay lead toagreater incidenceandmagni-tude of cardiotoxicity due to binding of multiple proteinsand/or downstream pathways (Table 1). For instance, Chu etal. [62]demonstrated that sunitinib,which targetsVEGFR1–3,c-kit, and PDGFR, leads to profound structural and functionalabnormalities in cardiomyocyte mitochondria, leading to adecrease in ATP production. In addition, blockade of VEGFR2with TKIs decreases endothelial nitric oxide synthase (eNOS)
Table 2. Potential future research directions to assessmodulation ofmolecularly targeted therapeutic cardiotoxicity with
aerobic exercise
Underlyingmechanisms ofMTT-related cardiotoxicity
• Elucidate the specific actions of HER2-inhibitors onmyocardial Nrg1 release and ErbB downstreampathways
• Examinewhether anti HER2 agents upregulatemyocardial TGF� and C/EBP� signaling and consequently downregulate GATA4signaling
• Determine the effects of anti-angiogenic agents onmyocardial and vascular VEGF expression and VEGFR signaling
• Examine the impact ofMTT on other tissues, such as skeletal muscle
• Delineate the longitudinal cardiac consequences in patients receivingMTTs
Underlyingmechanisms of aerobic exercise-induced cardioprotection
• Perform translational exercise-cardiotoxicity studies to elucidatewhether aerobic exercise:
• Upregulatesmyocardial Nrg1 and PGC1-� expression
• Decreasesmyocardial TGF� and C/EBP� signaling and increases GATA4 signaling
• Increasesmyocardial downstream effector signaling (e.g., endothelial progenitor cell, cardiac progenitor cell)
• Evaluate aerobic exercise intensity required to prevent/treat cardiotoxicity
• Establishmost effective timing (before, during, or following therapy) to perform aerobic exercise training
• Examinewhether integrating resistance and aerobic exercise can protect peripheral as well as central factors
• Monitor antineoplastic indices during aerobic exercise training to ensure antineoplastic goals ofMTTs aremet
Potential ResearchModels
• Neonatal rat ventricularmyocytes
Model should be used to examinemolecularmechanisms underlying cardiomyocyte hypertrophy, stress, and failure as a result ofMTT-induced toxicity
• Zebrafish
Ideal for cardiotoxicity-aerobic exercise studies given that the underlying cardiac development, patterning, genes, functions, anddisease characteristics are similar to humans, and has recently been established as novel exercisemodel
• Knockout/transgenic rodents
Genetically downregulated or upregulated pathways in rodents should be used to establish exercise-induced cardioprotectivesignaling pathways
• Patient populations
Adequately poweredmulticenter RCTswith appropriate cardiac endpoints are required to evaluate the relative efficacy ofaerobic exercise training to prevent/treat cardiotoxicity
Abbreviations:MTT,molecularly targeted therapeutic; RCT, randomized controlled trial.
226 Targeted Therapy, Cardiotoxicity, and Exercise
©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

activationandNOrelease,promotingvasoconstrictionand in-creased blood pressure [63]. Of significance, the combinedcardiac and vascular injury may enhance the severity of car-diac injury. Izumiya et al. [64] demonstrated that VEGF inhibi-tion contributed to progression from compensatory cardiachypertrophy to LV failure under hypertensive conditions.Chronic hypertension ultimately leads to a compensatory in-crease inmyocardial musclemass tomaintain normal cardiacoutput [65]. In both hypertensive and pre-hypertensivestates, there is slow but steady hypertrophy of the LV [66],leading to a decreased ability to relax initially during exerciseand subsequently at rest [67]. Whether concentric remodel-ing occurs in patients receiving antiangiogenic therapies hasnot been investigated.
AEROBIC EXERCISE-INDUCED CARDIOPROTECTION FROMANGIOGENESIS INHIBITIONAerobic exercise-induced increase in vascular andmyocardialVEGF/VEGFR signaling may prevent/treat antiangiogenesis-induced cardiotoxicity. These conceptual pathways are illus-trated in Figure 4. Upregulation of myocardial VEGF usingnaked DNA gene therapy enhances capillary density and de-creasesendothelial cell andcardiomyocyteapoptosis, leadingto improvements in cardiac function in a diabetic rat model[43]. Aerobic exercise augments the aging-induced [68] andinfarct-induced [69] decrease in VEGF mRNA and protein ex-pression in murine cardiac tissue. Increased VEGF expressionoccurs viaupstreamperoxisomeproliferator-activated recep-tor-� coactivator-1� (PGC-1�) through the transcription fac-tor estrogen-related receptor-� and is independent of
hypoxia-inducible factor 1�-induced VEGF expression [70].Aerobicexercise rapidlyupregulatesPGC-1�mRNAinskeletalmuscle,witha concomitant increase inmitochondrial contentleading to resistance to fatigue and a higher number of oxida-tive fibers [71]. Thus, because PGC-1� is obligatory for the ex-ercise-induced increase in VEGF expression, it is evident thatPGC-1� has a particularly prominent role in regulating train-ing-induced VEGF expression.
An additional putative cardioprotective mechanism is ex-ercise-induced augmentation in the production andmobiliza-tion of CPCs and EPCs via acute increases in interleukin-6 (IL-6), NO, and VEGF-dependent mechanisms [72–74]. Aerobic
exercise leads to an NO-dependent increase in circulatingEPCs inmice and humans [72], thus contributing to neovascu-larizationandvascular repair, leading to improvedendothelialfunction and myocardium recovery after ischemia [75–78].IL-6 also playsmultiple functions in angiogenesis and vascular
Aerobic exercise rapidly upregulates PGC-1� mRNAin skeletalmuscle,with a concomitant increase inmi-tochondrial content leading to resistance to fatigueand a higher number of oxidative fibers. Thus, be-cause PGC-1� is obligatory for the exercise-inducedincrease inVEGFexpression, it is evident that PGC-1�has a particularly prominent role in regulating train-ing-induced VEGF expression.
Table 3. Future challenges for research investigating the effects of and mechanisms of aerobic exercise in MTT-induced
cardiac toxicity
Preclinical studies
• Many of the availableMTTs are humanized agents. Thus, whether the cardiotoxicmechanistic action of these agents is the samein rodentmodels is questionable. Investigators should strive to test themurine versions of selected agents whenever possible.
• Within available rodentmodels, strains have inherently different exercise capacities whichmay also contribute to distinct cardiacadaptations to exercise training �131, 132�. These disparitiesmay account for discordant findings between investigations.
• Cardio-oncology investigations often use eithermale or female animals only. However, there are sexually dimorphiccardiovascular adaptations to exercise training in bothmice and rats �133–135�, which limitsmechanistic implications for eithermale or female patients.
• Mechanistic investigations are often conducted in animals that are young and otherwise healthy. In contrast, cancer patients aretypically older with the presence of concomitant comorbidities which exacerbate treatment-induced cardiotoxicity �136�.
• No threshold of exercise intensity for inducing observable cardiac adaptations has been identified in any clinical disease �137�.Most animal cardio-oncology exercise studies utilize continuous treadmill running characterized by fixed speed, inclination, andduration �138�. Elucidation of the dose-response relationship of exercise on cardiac function in rodents and how this translates tothe clinical setting are urgently required.
Clinical studies
• Overt cardiac events are relatively uncommon in cancer patients receivingMTTs; asymptomatic events aremore frequent.Nevertheless, given the current event ratewith standard detection techniques, large trials will be required to examine the effectof exercise on reducing the event rate. This issue could be somewhat addressed using biomarker enriched trials in which patientsonly at high-risk of events are recruited. Established biomarkers to identify such high-risk patients are not yet available butcurrently under investigation �8�.
• Cancer patients typically receiveMTTs in combinationwith other agents, particularly cytotoxic agents, possibly confounding theeffects of exercise onMTT-induced cardiotoxicity �139�, making interpretation challenging.
• Although numerous studies have demonstrated excellent adherence and safety profiles withmoderate intensity exercise �140�,no studies to date have examinedwhether patients receivingMTTs can successfully adhere or tolerate structured exercisetraining prescriptions incorporatingmoderate or high intensity training.
• The clinical impact of exercise on the antitumor efficacy ofMTTs in patients is unknown. Investigations determining theinteraction between exercise and tumor outcomes are critical in both rodent and human studies �141�.
Abbreviations:MTT,molecularly targeted therapeutic.
227Scott, Lakoski,Mackey et al.
www.TheOncologist.com ©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

remodeling and may stimulate EPC proliferation, migration,and tube formation following exercise [73, 79].
Importantly, this upregulation in EPCs and CPCs has beenimplicated in cardiomyocyte healing processes. Kolwicz et al.[80] found that exercise increased CPC proliferation by�200% and augmented the presence of KIT-positive cells (astem cell factor crucial for themobilization of progenitor cellsto sites of injury) in the heart. Togetherwith signal transducerand activator of transcription 3 (STAT3), this exercise-inducedincrease in CPC proliferationmay play a key role in cardiomy-ocyte proliferation, differentiation, and survival [81]. STAT3activation has been shown to mediate cardiac hypertrophyand protect cells in response to cardiomyopathy induced byischemiaordrug treatment [82–84]. Significantly, exercise in-creases STAT3 activation [85, 86], causing release of erythro-poietin into the cardiacmicroenvironment that, in turn, bindstoCPCs,causingdifferentiation intoendothelial cells [87].Pre-sumably, these endothelial cells can then be activated byVEGF to express matrix metalloproteinases, which degradethe vascular basement membrane to form new capillary net-works [88]. Collectively, we speculate that aerobic exercisemay increase PGC-1� and VEGF secretion and STAT3 activa-tion, with the resultant release, mobilization, and homing ofCPCs during angiogenesis inhibitor therapy.
CONCLUSIONMolecularly targeted therapeutics are the future of cancersystemic therapy; they have already moved from palliativetherapy for advanced solidmalignancies into the settingof cu-rative-intent treatment for early-stagedisease. Cardiotoxicityis a frequent and potentially serious adverse complication ofsome targeted therapies, leading to a broad range of poten-tially life-threatening complications, therapydiscontinuation,andpoorquality of life. Low-cost,multitargeted interventionsarethereforeurgently requiredtomitigatetheseadversecon-sequences. Evidence reviewed here indicates that aerobic ex-ercise is a nontoxic, pleiotropic therapy that affects diversecardiac signaling pathways implicated in the cardiotoxicity in-duced by anti-HER2 and antiangiogenic therapy. It is impor-tant to stress that the current evidence base is emergentwith
asmall numberof studies;manyareasofMTT-inducedcardio-toxicity remain tobedefinedandaddressed.A summaryof fu-ture investigations needed to define the nature andmagnitude of the cardioprotective effects of exercise in thesetting ofMTT is provided in Table 2. Future challenges for re-search investigating the effects of aerobic exercise in MTT-induced cardiac toxicity are provided in Table 3.
Although clinical and research interest in aerobic exercisehas increaseddramatically over the past decade, amore thor-ough understanding of themyocardial signaling pathways ac-tivated by exercise will be needed to improve cardiovascularoutcomes. Collectively, such researchwill lead tomechanisti-cally driven clinical trials. Importantly, adequately poweredmulticenter randomized controlled trials are required to eval-uate the relative efficacy of aerobic exercise training to pre-vent/treat cardiotoxicity. These investigations, in turn, willinform exercise prescription rehabilitation guidelines for pa-tientswith cancer,whereby themost effective exercise inten-sity and timing (before, during, or following therapy) areestablished.Weanticipate that exercisewill complementmo-lecularly targeted therapeutics to improve thehealth and lon-gevity of patients with solidmalignancies.
ACKNOWLEDGMENTSThiswork is supported inpartbygrants fromtheNationalCan-cer Institute (CA143254, CA142566, CA138634, CA133895,CA164751 to L.W.J.), funds from George and Susan Beischer(L.W.J.), and a Natural Sciences and Engineering ResearchCouncil postdoctoral fellowship (J.M.S.).
AUTHOR CONTRIBUTIONSConception/Design: JessicaM. Scott, LeeW. JonesManuscriptwriting: JessicaM.Scott, SusanLakoski, JohnR.Mackey, Pamela S.Douglas,Mark J. Haykowsky, LeeW. Jones
Final approval ofmanuscript: JessicaM. Scott, Susan Lakoski, JohnR.Mackey,Pamela S. Douglas,Mark J. Haykowsky, LeeW. Jones
DISCLOSURESJohnR.Mackey:RocheOncology;PamelaS.Douglas:Atritech/BostonScientific, Edwards Lifesciences (RF); CardioDX,UniversalOncology (OI).Theother authors indicatedno financial relationships.(C/A)Consulting/advisory relationship; (RF)Research funding; (E) Employment; (H)Honoraria
received; (OI)Ownership interests; (IP) Intellectual property rights/inventor/patentholder; (SAB)
Scientific advisoryboard
REFERENCES
1. Chen MH, Kerkela R, Force T. Mechanisms ofcardiac dysfunction associatedwith tyrosine kinaseinhibitor cancer therapeutics. Circulation 2008;118:84–95.
2. Force T, Krause DS, Van Etten RA. Molecularmechanisms of cardiotoxicity of tyrosine kinase in-hibition. Nat Rev Cancer 2007;7:332–344.
3. Yeh ET, Bickford CL. Cardiovascular complica-tions of cancer therapy: Incidence, pathogenesis,diagnosis,andmanagement. JAmCollCardiol2009;53:2231–2247.
4. Force T, Kerkela R. Cardiotoxicity of the newcancer therapeutics: Mechanisms of, and ap-proaches to, the problem. Drug Discov Today 2008;13:778–784.
5. Jones LW, Haykowsky MJ, Swartz JJ et al. Earlybreast cancer therapy and cardiovascular injury.J AmColl Cardiol 2007;50:1435–1441.
6. Cardinale D, SalvaticiM, SandriMT. Role of bio-markers in cardioncology.ClinChemLabMed2011;49:1937–1948.
7. Cardinale D, Sandri MT. Role of biomarkers inchemotherapy-inducedcardiotoxicity.ProgCardio-vasc Dis 2010;53:121–129.
8. Khouri M, Douglas P, Mackey J et al. Cancertherapy-inducedcardiac toxicity inearlybreast can-cer: Addressing the unresolved issues. Circulation2012 (in press).
9.Neet K, Hunter T. Vertebrate non-receptor pro-tein-tyrosine kinase families. Genes Cells 1996;1:147–169.
10. Schlessinger J. Cell signaling by receptor ty-rosine kinases. Cell 2000;103:211–225.
11. Kolibaba KS, Druker BJ. Protein tyrosine ki-nasesandcancer.BiochimBiophysActa1997;1333:F217–248.
12. Imai K, Takaoka A. Comparing antibody andsmall-molecule therapies for cancer. Nat Rev Can-cer 2006;6:714–727.
13. Slamon DJ, Clark GM, Wong SG et al. Humanbreast cancer: Correlation of relapse and survival
with amplification of the HER-2/neu oncogene. Sci-ence 1987;235:177–182.
14. Stephens P,Hunter C, Bignell G et al. Lung can-cer: Intragenic ERBB2 kinasemutations in tumours.Nature 2004;431:525–526.
15. Lee JW, Soung YH, Seo SH et al. Somaticmuta-tions of ERBB2 kinase domain in gastric, colorectal,and breast carcinomas. Clin Cancer Res 2006;12:57–61.
16. Piccart-GebhartMJ, ProcterM, Leyland-JonesB et al. Trastuzumab after adjuvant chemotherapyin HER2-positive breast cancer. N Engl J Med 2005;353:1659–1672.
17. Slamon D, Eiermann W, Robert N et al. Adju-vant trastuzumab in HER2-positive breast cancer.N Engl JMed 2011;365:1273–1283.
18.Geyer CE, Forster J, Lindquist D et al. Lapatinibplus capecitabine for HER2-positive advancedbreast cancer. N Engl JMed 2006;355:2733–2743.
19. Hynes NE, Lane HA. ERBB receptors and can-
228 Targeted Therapy, Cardiotoxicity, and Exercise
©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

cer: The complexity of targeted inhibitors. Nat RevCancer 2005;5:341–354.
20. Yarden Y, SliwkowskiMX. Untangling the ErbBsignalling network. Nat Rev Mol Cell Biol 2001;2:127–137.
21.Roberts PJ, Der CJ. Targeting the Raf-MEK-ERKmitogen-activated protein kinase cascade for thetreatment of cancer. Oncogene 2007;26:3291–3310.
22.Arnal-EstapeA, TarragonaM,MoralesMet al.HER2 silences tumor suppression in breast cancercells by switching expression of C/EBPss isoforms.Cancer Res 2010;70:9927–9936.
23.Mohsin SK,Weiss HL, GutierrezMC et al. Neo-adjuvant trastuzumab induces apoptosis in primarybreast cancers. J Clin Oncol 2005;23:2460–2468.
24.DaveB,Migliaccio I, GutierrezMCet al. Loss ofphosphatase and tensin homolog or phosphoinosi-tol-3kinaseactivationandresponsetotrastuzumabor lapatinib in human epidermal growth factor re-ceptor 2-overexpressing locally advanced breastcancers. J Clin Oncol 2011;29:166–173.
25. Crone SA, Zhao YY, Fan L et al. ErbB2 is essen-tial in the prevention of dilated cardiomyopathy.NatMed 2002;8:459–465.
26. Ky B, Kimmel SE, Safa RN et al. Neuregulin-1beta is associatedwithdisease severity andadverseoutcomes in chronic heart failure. Circulation 2009;120:310–317.
27.Gordon LI, BurkeMA, Singh AT et al. Blockadeof theerbB2 receptor induces cardiomyocytedeaththrough mitochondrial and reactive oxygen spe-cies-dependent pathways. J Biol Chem 2009;284:2080–2087.
28. Brero A, Ramella R, Fitou A et al. Neuregulin-1beta1 rapidlymodulates nitric oxide synthesis andcalciumhandling in rat cardiomyocytes. CardiovascRes 88:443–452.
29. Pentassuglia L, Sawyer DB. The role of Neu-regulin-1beta/ErbB signaling in the heart. Exp CellRes 2009;315:627–637.
30. Kuramochi Y, Guo X, Sawyer DB. Neuregulinactivates erbB2-dependent src/FAK signaling andcytoskeletal remodeling in isolatedadult rat cardiacmyocytes. JMol Cell Cardiol 2006;41:228–235.
31. Liu X, Gu X, Li Z et al. Neuregulin-1/erbB-acti-vation improves cardiac function and survival inmodels of ischemic, dilated, and viral cardiomyopa-thy. J AmColl Cardiol 2006;48:1438–1447.
32. Derynck R, Akhurst RJ, Balmain A. TGF-betasignaling in tumor suppression and cancer progres-sion. Nat Genet 2001;29:117–129.
33. Kakkar R, Lee RT. Intramyocardial fibroblastmyocytecommunication.CircRes2010;106:47–57.
34.BostromP,MannN,WuJetal. C/EBPbeta con-trols exercise-induced cardiac growth and protectsagainst pathological cardiac remodeling. Cell 2010;143:1072–1083.
35. Bersell K, Arab S, Haring B, Kuhn B. Neuregu-lin1/ErbB4 signaling induces cardiomyocyte prolif-eration and repair of heart injury. Cell 2009;138:257–270.
36. LemmensK,DoggenK,DeKeulenaerGW.Roleof neuregulin-1/ErbB signaling in cardiovascularphysiology and disease: Implications for therapy ofheart failure. Circulation 2007;116:954–960.
37. Lemmens K, Segers VF, Demolder M, De Keu-lenaer GW. Role of neuregulin-1/ErbB2 signaling inendothelium-cardiomyocyte cross-talk. J Biol Chem2006;281:19469–19477.
38. Esch BT, Scott JM, Warburton DE et al. Leftventricular torsion and untwisting during exercisein heart transplant recipients. J Physiol 2009;587:2375–2386.
39. FernandesT,HashimotoNY,MagalhaesFCetal.Aerobic exercise training-induced left ventricular hy-pertrophy involves regulatoryMicroRNAs, decreasedangiotensin-converting enzyme-angiotensin ii, andsynergistic regulation of angiotensin-converting en-zyme 2-angiotensin (1–7). Hypertension 2011;58:182–189.
40. LebrasseurNK, CoteGM,Miller TA et al. Regu-lation of neuregulin/ErbB signaling by contractileactivity in skeletal muscle. Am J Physiol Cell Physiol2003;284:C1149–1155.
41.McMullen JR, Shioi T, Zhang L et al. Phospho-inositide 3-kinase(p110alpha) plays a critical rolefor the inductionof physiological, but not patholog-ical, cardiac hypertrophy. Proc Natl Acad Sci U S A2003;100:12355–12360.
42. McMullen JR, Jennings GL. Differences be-tween pathological and physiological cardiac hy-pertrophy: Novel therapeutic strategies to treatheart failure. Clin Exp Pharmacol Physiol 2007;34:255–262.
43. Yoon YS, Uchida S, Masuo O et al. Progressiveattenuation of myocardial vascular endothelialgrowth factor expression is a seminal event in dia-betic cardiomyopathy: Restoration of microvascu-lar homeostasis and recovery of cardiac function indiabetic cardiomyopathy after replenishment of lo-cal vascular endothelial growth factor. Circulation2005;111:2073–2085.
44. Zhang KR, Liu HT, Zhang HF et al. Long-termaerobic exercise protects the heart against isch-emia/reperfusion injury via PI3 kinase-dependentand Akt-mediated mechanism. Apoptosis 2007;12:1579–1588.
45.McMullen JR, Amirahmadi F, Woodcock EA etal. Protective effects of exercise and phosphoinosi-tide 3-kinase(p110alpha) signaling in dilated andhypertrophic cardiomyopathy. Proc Natl Acad SciU S A 2007;104:612–617.
46. Kikuchi K, Holdway JE, Werdich AA et al. Pri-mary contribution to zebrafish heart regenerationby gata4(�) cardiomyocytes. Nature 2010;464:601–605.
47.HaykowskyMJ,Mackey JR, ThompsonRBetal.Adjuvant trastuzumab induces ventricular remod-eling despite aerobic exercise training. Clin CancerRes 2009;15:4963–4967.
48. Haykowsky MJ, Liang Y, Pechter D et al. Ameta-analysis of the effect of exercise training onleft ventricular remodeling in heart failurepatients:The benefit depends on the type of training per-formed. J AmColl Cardiol 2007;49:2329–2336.
49.Wisloff U, Stoylen A, Loennechen JP et al. Su-perior cardiovascular effect of aerobic intervaltraining versus moderate continuous training inheart failure patients: A randomized study. Circula-tion 2007;115:3086–3094.
50. Jain RK. Normalization of tumor vasculature:Anemergingconcept inantiangiogenic therapy.Sci-ence 2005;307:58–62.
51. Kerbel RS. Tumor angiogenesis. N Engl J Med2008;358:2039–2049.
52.Munoz-Chapuli R, Quesada AR, Angel MedinaM. Angiogenesis and signal transduction in endo-thelial cells. CellMol Life Sci 2004;61:2224–2243.
53. D’Adamo DR, Anderson SE, Albritton K et al.Phase II study of doxorubicin and bevacizumab for
patientswithmetastatic soft-tissue sarcomas. J ClinOncol 2005;23:7135–7142.
54. Choueiri TK, Mayer EL, Je Y et al. Congestiveheart failure risk in patients with breast cancertreated with bevacizumab. J Clin Oncol 29: 632–638.
55.GerberHP, Hillan KJ, RyanAMet al. VEGF is re-quired forgrowthandsurvival inneonatalmice.De-velopment 1999;126:1149–1159.
56. Olfert IM, Howlett RA, Tang K et al. Muscle-specific VEGF deficiency greatly reduces exerciseendurance inmice. J Physiol 2009;587:1755–1767.
57. Giordano FJ, Gerber HP, Williams SP et al. Acardiacmyocyte vascular endothelial growth factorparacrine pathway is required to maintain cardiacfunction. Proc Natl Acad Sci U S A 2001;98:5780–5785.
58. Lambrechts D, Carmeliet P. Genetics in ze-brafish, mice, and humans to dissect congenitalheart disease: Insights in the role of VEGF. Curr TopDev Biol 2004;62:189–224.
59.ChenK,BaiH,ArzigianMetal. Endothelial cellsregulate cardiomyocyte development from embry-onic stem cells. J Cell Biochem2010;111:29–39.
60. Dimmeler S, Fleming I, Fisslthaler B et al. Acti-vationofnitricoxide synthase inendothelial cellsbyAkt-dependent phosphorylation.Nature 1999;399:601–605.
61. Chen Y, Amende I, Hampton TG et al. Vascularendothelial growth factorpromotescardiomyocytedifferentiation of embryonic stem cells. Am JPhysiol Heart Circ Physiol 2006;291:H1653–1658.
62.ChuTF,RupnickMA,KerkelaRetal. Cardiotox-icity associated with tyrosine kinase inhibitorsunitinib. Lancet 2007;370:2011–2019.
63. Facemire CS, NixonAB, Griffiths R et al. Vascu-lar endothelial growth factor receptor 2 controlsblood pressure by regulating nitric oxide synthaseexpression. Hypertension 2009;54:652–658.
64. Izumiya Y, Shiojima I, Sato K et al. Vascular en-dothelial growth factor blockade promotes thetransition from compensatory cardiac hypertrophyto failure in response to pressure overload. Hyper-tension 2006;47:887–893.
65. Jain M, Townsend RR. Chemotherapy agentsand hypertension: A focus on angiogenesis block-ade. Curr Hypertens Rep 2007;9:320–328.
66. LevyD. Left ventricular hypertrophy. Epidemi-ological insights from the FraminghamHeart Study.Drugs 1988;35(suppl 5):1–5.
67. Brucks S, Little WC, Chao T et al. Contributionof left ventricular diastolic dysfunction to heart fail-ure regardless of ejection fraction. Am J Cardiol2005;95:603–606.
68. Iemitsu M, Maeda S, Jesmin S et al. Exercisetraining improvesaging-induceddownregulationofVEGF angiogenic signaling cascade in hearts. Am JPhysiol Heart Circ Physiol 2006;291:H1290–1298.
69.WuG, Rana JS,Wykrzykowska J et al. Exercise-induced expression of VEGF and salvation of myo-cardium in the early stage of myocardial infarction.Am J Physiol Heart Circ Physiol 2009;296:H389–395.
70. Arany Z, Foo SY, Ma Y et al. HIF-independentregulation of VEGF and angiogenesis by the tran-scriptional coactivator PGC-1alpha. Nature 2008;451:1008–1012.
71. Lin J, Wu H, Tarr PT et al. Transcriptional co-activator PGC-1 alpha drives the formation of slow-twitchmuscle fibres. Nature 2002;418:797–801.
229Scott, Lakoski,Mackey et al.
www.TheOncologist.com ©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

72. Laufs U, Werner N, Link A et al. Physical train-ing increases endothelial progenitor cells, inhibitsneointima formation, and enhances angiogenesis.Circulation 2004;109:220–226.
73.Mobius-Winkler S, Hilberg T, Menzel K et al.Time-dependent mobilization of circulating pro-genitorcellsduringstrenuousexercise inhealthy in-dividuals. J Appl Physiol 2009;107:1943–1950.
74.SchobersbergerW,Hobisch-HagenP, FriesDet al. Increase in immune activation, vascular en-dothelial growth factor and erythropoietin afteran ultramarathon run at moderate altitude. Im-munobiology 2000;201:611–620.
75.Takahashi T, KalkaC,MasudaHetal. Ischemia-and cytokine-induced mobilization of bone mar-row-derived endothelial progenitor cells for neo-vascularization. NatMed 1999;5:434–438.
76. Dimmeler S, Aicher A, VasaM et al. HMG-CoAreductase inhibitors (statins) increase endothelialprogenitor cells via the PI 3-kinase/Akt pathway.J Clin Invest 2001;108:391–397.
77.UrbichC,HeeschenC,AicherAetal. CathepsinL is required for endothelial progenitor cell-inducedneovascularization. NatMed 2005;11:206–213.
78. Asahara T, Murohara T, Sullivan A et al. Isola-tion of putative progenitor endothelial cells for an-giogenesis. Science 1997;275:964–967.
79. Fan Y, Ye J, Shen F et al. Interleukin-6 stimu-lates circulating blood-derived endothelial progen-itor cell angiogenesis in vitro. J Cereb Blood FlowMetab 2008;28:90–98.
80. Kolwicz SC,MacDonnell SM, Kendrick ZV et al.Voluntary wheel running and pacing-induced dys-function in hypertension. Clin Exp Hypertens 2008;30:565–573.
81.CohenT,Nahari D, CeremLWet al. Interleukin6 induces the expression of vascular endothelialgrowth factor. J Biol Chem1996;271:736–741.
82.KunisadaK,HirotaH, Fujio Yet al. ActivationofJAK-STAT and MAP kinases by leukemia inhibitoryfactor through gp130 in cardiac myocytes. Circula-tion 1996;94:2626–2632.
83.Hilfiker-KleinerD,Hilfiker A, FuchsMet al. Sig-nal transducer and activator of transcription 3 is re-quired for myocardial capillary growth, control ofinterstitial matrix deposition, and heart protectionfrom ischemic injury. Circ Res 2004;95:187–195.
84.KunisadaK,NegoroS,ToneEetal. Signal trans-ducer and activator of transcription 3 in the hearttransduces not only a hypertrophic signal but a pro-tective signal against doxorubicin-induced cardio-myopathy. Proc Natl Acad Sci U S A 2000;97:315–319.
85. Trenerry MK, Carey KA, Ward AC, Cameron-SmithD. STAT3 signaling is activated in human skel-etal muscle following acute resistance exercise.J Appl Physiol 2007;102:1483–1489.
86. Toth KG, McKay BR, De Lisio M et al. IL-6 in-duced STAT3 signalling is associatedwith the prolif-eration of human muscle satellite cells followingacutemuscle damage. PLoSOne 2011;6:e17392.
87.HochM, Fischer P, Stapel B et al. Erythropoie-tin preserves the endothelial differentiation capac-ity of cardiac progenitor cells and reduces heartfailure during anticancer therapies. Cell Stem Cell2011;9:131–143.
88.Westenbrink BD, Ruifrok WP, Voors AA et al.Vascular endothelial growth factor is crucial forerythropoietin-induced improvement of cardiacfunction in heart failure. Cardiovasc Res 2010;87:30–39.
89. Tan-Chiu E, Yothers G, Romond E et al. Assess-ment of cardiac dysfunction in a randomized trialcomparing doxorubicin and cyclophosphamide fol-lowedbypaclitaxel,withorwithout trastuzumabasadjuvant therapy in node-positive, human epider-mal growth factor receptor 2-overexpressingbreast cancer: NSABP B-31. J Clin Oncol 2005;23:7811–7819.
90. Bang YJ, Van Cutsem E, Feyereislova A et al.Trastuzumab in combination with chemotherapyversus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophagealjunction cancer (ToGA): A phase 3, open-label, ran-domised controlled trial. Lancet 2010;376:687–697.
91. Baselga J, Cortes J, Kim S, et al. Pertuzumabplus trastuzumab plus docetaxel for metastaticbreast cancer. N Engl JMed 2012;366:109–119.
92.SlamonDJ, Leyland-JonesB,ShakSetal.Useofchemotherapy plus a monoclonal antibody againstHER2 for metastatic breast cancer that overex-presses HER2. N Engl JMed 2001;344:783–792.
93. CobleighMA, Vogel CL, Tripathy D et al.Multi-national study of the efficacy and safety of human-izedanti-HER2monoclonal antibody inwomenwhohave HER2-overexpressing metastatic breast can-cer that has progressed after chemotherapy formetastatic disease. J Clin Oncol 1999;17:2639–2648.
94. Vogel CL, Cobleigh MA, Tripathy D et al. Effi-cacy and safety of trastuzumab as a single agent infirst-line treatment of HER2-overexpressing meta-static breast cancer. J Clin Oncol 2002;20:719–726.
95. Smith KL, Dang C, Seidman AD. Cardiac dys-function associated with trastuzumab. Expert OpinDrug Saf 2006;5:619–629.
96.Baselga J,Carbonell X,Castaneda-SotoNJetal.Phase II study of efficacy, safety, and pharmacoki-netics of trastuzumab monotherapy administeredon a3-weekly schedule. J ClinOncol 2005;23:2162–2171.
97. Perez EA, Koehler M, Byrne J et al. Cardiacsafety of lapatinib: Pooled analysis of 3689 patientsenrolled in clinical trials. Mayo Clin Proc 2008;83:679–686.
98. Ross HJ, Blumenschein GR, Jr. Aisner J et al.Randomizedphase IImulticenter trial of two sched-ules of lapatinib as first- or second-line mono-therapy in patients with advanced or metastaticnon-small cell lung cancer. Clin CancerRes2010;16:1938–1949.
99. SlamonD,GomezHL, Kabbinavar FF et al. Ran-domized study of pazopanib � lapatinib vs. lapa-tinib alone in patientswithHER2-positive advancedor metastatic breast cancer. J Clin Oncol 2008;26(15 suppl):1016.
100. Portera CC, Walshe JM, Rosing DR et al. Car-diac toxicity and efficacy of trastuzumab combinedwithpertuzumab inpatientswithhumanepidermalgrowth factor receptor2-positivemetastatic breastcancer. Clin Cancer Res 2008;14:2710–2716.
101. Baselga J, Gelmon KA, Verma S et al. Phase IItrial of pertuzumab and trastuzumab in patientswith human epidermal growth factor receptor2-positivemetastaticbreast cancer thatprogressedduring prior trastuzumab therapy. J Clin Oncol2010;28:1138–1144.
102. Lenihan D, Suter T, Brammer M et al. Pooledanalysisofcardiacsafety inpatientswithcancer treatedwithpertuzumab.AnnOncol 2012;23:791–800.
103.MillerK,WangM,GralowJet al. Paclitaxel plus
bevacizumab versus paclitaxel alone for metastaticbreast cancer.NEngl JMed2007;357:2666–2676.
104.Miller KD, Chap LI, Holmes FA et al. Random-ized phase III trial of capecitabine compared withbevacizumabpluscapecitabine inpatientswithpre-viously treated metastatic breast cancer. J Clin On-col 2005;23:792–799.
105.Miller K, O’Neill A, Perez E et al. Phase II feasi-bilitytrial incorporatingbevacizumabintodose-densedoxorubicinandcyclophosphamidefollowedbypacli-taxel inpatientswith lymphnode-positivebreast can-cer:a trialof theEasternCooperativeOncologyGroup(E2104).AnnOncol 2012;23:331–337.
106.BearHD, TangG,Rastogi P et al. Theeffect onpCR of bevacizumab and/or antimetabolites addedto standard neoadjuvant chemotherapy: NSABPprotocol B-40. J Clin Oncol 2011;29(15 suppl):1005.
107.YardleyDA,Hart L,WaterhouseDMetal.Pre-liminary safety results: Addition of bevacizumab to3 docetaxel regimens as adjuvant therapy for earlystage breast cancer. Cancer Res 2009;69(suppl 2):Abstract 4107.
108. Robert NJ, Dieras V, Glaspy J et al. RIBBON-1:randomized, double-blind, placebo-controlled,phase III trial of chemotherapywith orwithout bev-acizumab for first-line treatment of human epider-mal growth factor receptor 2-negative, locallyrecurrent or metastatic breast cancer. J Clin Oncol2011;29:1252–1260.
109. Allegra CJ, Yothers G, O’ConnellMJ et al. Initialsafety report of NSABP C-08: A randomized phase IIIstudy of modified FOLFOX6 with or without bevaci-zumab for the adjuvant treatment of patients withstage II or III colon cancer. J ClinOncol 2009;27:3385–3390.
110.PandeA, LombardoJ, SpangenthalE, JavleM.Hypertension secondary to anti-angiogenic thera-py: Experience with bevacizumab. Anticancer Res2007;27:3465–3470.
111. Spratlin JL, Cohen RB, EadensMet al. Phase Ipharmacologic and biologic study of ramucirumab(IMC-1121B), a fully human immunoglobulin G1monoclonal antibody targeting the vascular endo-thelial growth factor receptor-2. J Clin Oncol 2010;28:780–787.
112.KhakooAY,KassiotisCM,TannirNetal.Heartfailure associatedwith sunitinibmalate: Amultitar-geted receptor tyrosine kinase inhibitor. Cancer2008;112:2500–2508.
113. Barrios CH, LiuMC, Lee SC et al. Phase III ran-domized trial of sunitinib versus capecitabine in pa-tients with previously treated HER2-negativeadvanced breast cancer. Breast Cancer Res Treat2010;121:121–131.
114. Bergh J, Greil R, VoytkoN et al. Sunitinib (SU)in combination with docetaxel (D) versus D alonefor the first-line treatment of advanced breast can-cer (ABC). J Clin Oncol 2010;28(18 suppl):1010.
115. Schmidinger M, Zielinski CC, Vogl UM et al.Cardiac toxicity of sunitinib and sorafenib in pa-tients with metastatic renal cell carcinoma. J ClinOncol 2008;26:5204–5212.
116. Vaklavas C, Lenihan D, Kurzrock R, Tsimberi-dou AM. Anti-vascular endothelial growth factortherapies and cardiovascular toxicity:What are theimportant clinical markers to target? The Oncolo-gist 2010;15:130–141.
117. Escudier B, Eisen T, Stadler WM et al.Sorafenib in advanced clear-cell renal-cell carci-noma. N Engl JMed 2007;356:125–134.
118. RatainMJ, Eisen T, StadlerWMet al. Phase II
230 Targeted Therapy, Cardiotoxicity, and Exercise
©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

placebo-controlled randomized discontinuationtrial of sorafenib in patients with metastatic renalcell carcinoma. J Clin Oncol 2006;24:2505–2512.
119.Wu S, Chen JJ, Kudelka A et al. Incidence andrisk of hypertension with sorafenib in patients withcancer:Asystematic reviewandmeta-analysis. Lan-cet Oncol 2008;9:117–123.
120. Taylor SK, Chia S, Dent S et al. A phase II studyof pazopanib in patients with recurrent or meta-static invasive breast carcinoma: A trial of the Prin-cess Margaret Hospital phase II consortium. TheOncologist2010;15: 810–818.
121. Sternberg CN, Davis ID,Mardiak J et al. Pazo-panib in locally advanced or metastatic renal cellcarcinoma: Results of a randomized phase III trial.J Clin Oncol 2010;28:1061–1068.
122. Alberts SR, Fitch TR, Kim GP et al. Cediranib(AZD2171) in patients with advanced hepatocellu-lar carcinoma: A phase II North Central CancerTreatment Group Clinical Trial. Am J Clin Oncol2012;35:329–333.
123. Batchelor TT, Duda DG, di Tomaso E et al.Phase II study of cediranib, an oral pan-vascular en-dothelial growth factor receptor tyrosine kinase in-hibitor, in patients with recurrent glioblastoma.J Clin Oncol 2010;28:2817–2823.
124.HyamsDM,deOliveiraC, SnyderRetal. Cedi-ranib in combination with fulvestrant in hormone-sensitive metastatic breast cancer: A phase IIrandomized study. Cancer Res 2009;69(suppl 24):Abstract 204.
125. Natale RB, Thongprasert S, Greco FA et al.PhaseIII trialofvandetanibcomparedwitherlotinib inpatientswithpreviously treatedadvancednon-small-cell lung cancer. J ClinOncol 2011;29:1059–1066.
126.Horti J, Widmark A, Stenzl A et al. A random-ized, double-blind, placebo-controlled phase IIstudyof vandetanibplusdocetaxel/prednisolone inpatients with hormone-refractory prostate cancer.Cancer Biother Radiopharm 2009;24:175–180.
127. de Boer RH, Arrieta O, Yang CH et al. Vandet-anib plus pemetrexed for the second-line treat-ment of advanced non-small-cell lung cancer: Arandomized,double-blindphase III trial. J ClinOncol2011;29:1067–1074.
128.MartinM, RocheH, Pinter T et al.Motesanib,or open-label bevacizumab, in combination withpaclitaxel, as first-line treatment forHER2-negativelocally recurrent or metastatic breast cancer: Aphase 2, randomised, double-blind, placebo-con-trolled study. Lancet Oncol 2011;12:369–376.
129. Rugo HS, Stopeck AT, Joy AA et al. Random-ized, placebo-controlled, double-blind, phase IIstudy of axitinib plus docetaxel versus docetaxelplus placebo in patientswithmetastatic breast can-cer. J Clin Oncol 2011;29:2459–2465.
130.KindlerHL, IokaT, RichelDJ et al. Axitinibplusgemcitabine versusplaceboplus gemcitabine inpa-tients with advanced pancreatic adenocarcinoma:A double-blind randomised phase 3 study. LancetOncol 2011;12:256–262.
131. Koch LG, Britton SL, Barbato JC et al. Pheno-typic differences in cardiovascular regulation in in-bred rat models of aerobic capacity. PhysiolGenomics 1999;1:63–69.
132. Barbato JC, Koch LG, Darvish A et al. Spectrumof aerobic endurance running performance in eleveninbredstrainsofrats. JApplPhysiol1998;85:530–536.
133. Konhilas JP, Maass AH, Luckey SW et al. Sex
modifiesexerciseandcardiacadaptationinmice.AmJPhysiolHeartCircPhysiol 2004;287:H2768–2776.
134. Kemi OJ, Loennechen JP,Wisloff U, EllingsenO. Intensity-controlled treadmill running in mice:Cardiac and skeletal muscle hypertrophy. J ApplPhysiol 2002;93:1301–1309.
135.WisloffU,HelgerudJ,KemiOJ,EllingsenO. In-tensity-controlled treadmill running in rats: VO(2max) and cardiac hypertrophy. Am J Physiol HeartCirc Physiol 2001;280:H1301–1310.
136. HooningMJ, Botma A, Aleman BMet al. Long-termriskofcardiovasculardiseasein10-yearsurvivorsofbreast cancer. JNatl Cancer Inst 2007;99:365–375.
137.WangY,WisloffU, KemiOJ.Animalmodels inthe study of exercise-induced cardiac hypertrophy.Physiol Res 2010;59:633–644.
138. Scott JM, KhakooA,Mackey JR et al.Modula-tion of anthracycline-induced cardiotoxicity by aer-obicexercise inbreastcancer:Currentevidenceandunderlying mechanisms. Circulation 2011;124:642–650.
139. Brunello A, RomaA, Falci C, Basso U. Chemo-therapy and targeted agents for elderly womenwith advanced breast cancer. Recent Pat Antican-cer Drug Discov 2008;3:187–201.
140. Jones LW, Liang Y, Pituskin EN et al. Effect ofexercise training on peak oxygen consumption inpatients with cancer: A meta-analysis. The Oncolo-gist 2011;16:112–120.
141. Betof AS, Dewhirst MW, Jones LW. Effectsand potential mechanisms of exercise training oncancer progression: A translational perspective.Brain Behav Immun 2012 [Epub ahead of print].
231Scott, Lakoski,Mackey et al.
www.TheOncologist.com ©AlphaMed Press 2013
by guest on June 13, 2013http://theoncologist.alpham
edpress.org/D
ownloaded from

References http://theoncologist.alphamedpress.org/content/18/2/221#BIBL
This article cites 135 articles, 67 of which you can access for free at: by guest on June 13, 2013
http://theoncologist.alphamedpress.org/
Dow
nloaded from