Embed Size (px)
Citation preview

GEN01-1077-2 BleedGuide_DR3.indd5-15-2018 4:24 PM
1
JobClientMedia TypeLiveTrimBleedPubs
NoneNoneNoneNone21.75” x 17”NoneNone
Job info
None
Notes
Art DirectorCopywriterAccount MgrStudio ArtistProofreader
NoneNoneNoneNoneNone
Approvals
FontsAvenir (Heavy, Black, Book, Roman , Medium, Light, Book Oblique, Oblique, Black Oblique, Heavy Oblique), TradeGothic LT (CondEighteen), TradeGothic LT BdCondTwenty (Regular), Arial (Bold), Minion Pro (Regular)
ImagesGENE1077_2_Dieline.ai (100%), 101317_Hemlibra_US_External_Logo_150_CMYK_TM.eps (16.49%, 16.5%, 7.95%, 8.04%, 13.1%, 13.11%), Genentech_logo.ai (26.5%), Screen Shot 2018-03-20 at 11.42.01.png (RGB; 533 ppi, 518 ppi; 13.5%, 13.87%), Screen Shot 2018-03-20 at 12.19.03.png (RGB; 527 ppi; 13.66%)
Inks Cyan, Magenta, Yellow, Black, Dieline, FPO
Fonts & Images
Saved at Nonefrom Melissa Love’s Macbook Pro Printed At
IndicationHEMLIBRA is indicated for routine prophylaxis to prevent or reduce the frequency of bleeding episodes in adult and pediatric patients with hemophilia A with factor VIII inhibitors.
Important Safety InformationBoxed WARNING: THROMBOTIC MICROANGIOPATHY and THROMBOEMBOLISM Cases of thrombotic microangiopathy and thrombotic events were reported when on average a cumulative amount of >100 U/kg/24 hours of activated prothrombin complex concentrate (aPCC) was administered for 24 hours or more to patients receiving HEMLIBRA prophylaxis. Monitor for the development of thrombotic microangiopathy and thrombotic events if aPCC is administered. Discontinue aPCC and suspend dosing of HEMLIBRA if symptoms occur.
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Treatingbreakthrough bleeds:A new approach Using Bypassing Agents With HEMLIBRA Prophylaxis
For HCP audiences
HEMLIBRA® is a registered trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The HEMLIBRA logo is a trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The Genentech logo is a registered trademark of Genentech, Inc. ©2018 Genentech USA, Inc. All rights reserved. EMI/080317/0065(3) 05/18
A new approach to treating breakthrough bleeds when using concomitant BPAs
• Patients with TMA presented with thrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury, without severe defi ciencies in ADAMTS13 activity
1 additional TMA case occurred after the data cutoff for the primary analysis1
• The patient passed away and the investigator determined the cause of deathwas unrelated to HEMLIBRA
4 events fully resolved following aPCC discontinuation and suspension of HEMLIBRA1,2
• In the limited experience with these events, treatment included supportive care with or without hemodialysis/plasmapheresis
• Evidence of improvementwas seen within 1 week
• Both patients recovered within 3 weeks, with 1 patient electing to resume HEMLIBRA—without recurrence
• No thrombotic event required anticoagulation therapy
• Evidence of improvement wasseen within 1 month
• Both patients fully recovered,with 1 patient electing to resume HEMLIBRA — without recurrence
TMA and thrombotic events reported in HAVEN 1
Thrombotic microangiopathy (TMA) and thrombotic events werereported when on average a cumulative amount of >100 U/kg/24 hours of aPCC was administered for ≥24 hours to patients receivingHEMLIBRA prophylaxis
aPCC=activated prothrombin complex concentrate.† Based on data from HAVEN 1: a randomized, multicenter, open-label clinical trial of patients with hemophilia A with FVIII inhibitors aged 12 years and older (N=109, all males). The primary endpoint was reduction in treated bleeds over 24 weeks with prophylactic HEMLIBRA vs no prophylaxis.
‡ Based on data from HAVEN 2 (interim analysis): a single-arm, multicenter, open-label clinical study of patients with hemophilia A with FVIII inhibitors aged <12 years and 12-17 years weighing <40 kg. HAVEN 2 outcomes are from aninterim analysis. The interim effi cacy analysis examined reduction in bleeds at 30 weeks. The interim intra-patient analysis evaluated ABR in patients switching to HEMLIBRA following previous prophylactic BPAs (n=15) or previous on-demand BPAs (n=3) at a median study duration of 59 weeks. Statistical signifi cance will be conducted at fi nal analysis.1
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=35)
No prophylaxis(n=18)
Median ABR in HAVEN 1 was 0 (IQR: 0; 3.7) with HEMLIBRA prophylaxis vs 18.8 (IQR: 13.0; 35.1) with no prophylaxis
Median ABR in HAVEN 2 was 0 (IQR: 0; 0) with HEMLIBRA prophylaxis 1
Signifi cantly more patients with FVIII inhibitors had 0 bleeds*
with HEMLIBRA vs no prophylaxis
VS
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=59)
Sustained protection meant 0 treated bleeds for most patients1
87% FEWER BLEEDS (95% CI: 72.3; 94.3), P<0.0001ABR 2.9 (95% CI: 1.7; 5.0) vs
23.3 (95% CI: 12.3; 43.9)
98% FEWER BLEEDSin the intra-patient analysis
ABR 0.4 (95% CI: 0.2; 0.9) vs19.8 (95% CI: 15.3; 25.7)with previous BPAs (n=18)
ABR 0.3 (95% CI: 0.1; 0.5)
86%
HAVEN 1: Adults and adolescents†
HAVEN 2 interim analysis: Children1‡
2 TMA cases1 2 thrombotic events1,2
Recovery from these events occurred in the continued presence of HEMLIBRA in plasma2,3
HEMLIBRA prophylaxis calls for a new way of using BPAs for treating breakthrough bleeds
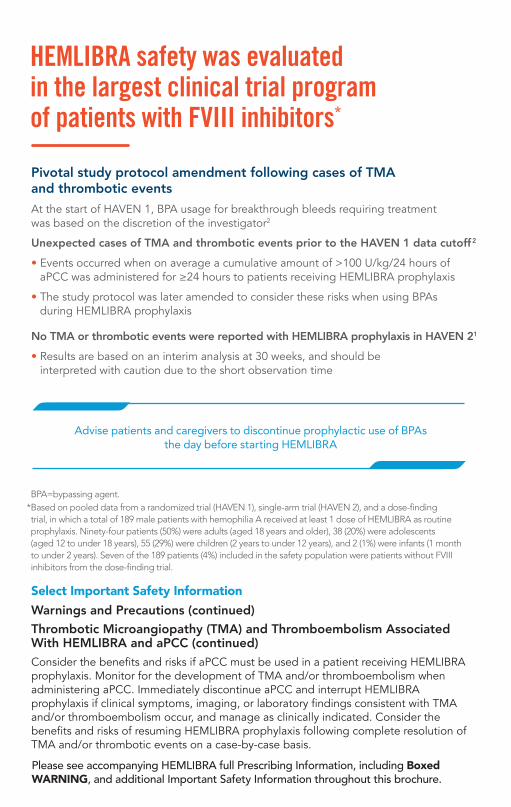
In HAVEN 1 and HAVEN 2, no TMA or thrombotic events wereobserved with use of rFVIIa alone in patients taking HEMLIBRA1, 2
• Clinical experience was limited and of relatively short duration (median treatment exposure was 42 weeks for HAVEN 1 and 29 weeks for HAVEN 2), and cannot exclude the possibility of occurrence of events with rFVIIa when taking HEMLIBRA1
140 treatment instances in patients treated with rFVIIa in HAVEN 11
Treatment average<90 µg/kg/24 h90–180 µg/kg/24 h181–270 µg/kg/24 h>270 µg/kg/24 h
% of treatmentinstances
17343119
There is a possibility for hypercoagulability with rFVIIa with HEMLIBRA based on preclinical experiments
Select Important Safety InformationWarnings and PrecautionsThrombotic Microangiopathy (TMA) and Thromboembolism Associated With HEMLIBRA and aPCCIn clinical trials, TMA was reported in 1.6% of patients (3/189) and thrombotic events were reported in 1.1% of patients (2/189). In patients who received at least one dose of aPCC, TMA was reported in 8.3% of patients (3/36) and thrombotic events were reported in 5.6% of patients (2/36). Patients with TMA presented with thrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury, without severe deficiencies in ADAMTS13.
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Talk to patients and caregivers about how HEMLIBRA increases coagulation potential
Select Important Safety InformationPregnancy, Lactation, Females and Males of Reproductive PotentialWomen of childbearing potential should use contraception while receiving HEMLIBRA. HEMLIBRA should be used during pregnancy only if the potential benefit for the mother outweighs the risk to the fetus. Consider developmental/health benefits, clinical need and potential adverse effects on the breastfed child and mother.
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch. You may also report side effects to Genentech at (888) 835-2555.
Monitor for TMA and thromboembolism if using aPCC*
Ensure patients and caregivers know to seek medical treatment if they suspect these eventsImmediately discontinue aPCC and suspend HEMLIBRA if theseevents occur, and manage as clinically indicatedConsider the benefi ts and risks of resuming HEMLIBRA prophylaxis following complete resolution of TMA or thrombotic events on a case-by-case basis
Educate patients and caregivers to think differentlyDiscuss which types of bleeds require BPAs while taking HEMLIBRA and the importance of seeking medical advice before treating these bleeds Describe the potential risks of TMA and thromboembolism if aPCC is taken during HEMLIBRA prophylaxisEncourage patients to update emergency medical informationand to inform all healthcare providers
* Monitoring includes D-dimer, prothrombin fragment F1+2 (if available), platelet count, serum creatinine, LDH, and peripheral blood smear analysis for schistocytes. For patients who require multiple BPA doses, laboratorymonitoring should be performed every 24 – 48 hours thereafter until 24 – 48 hours following the last BPA doseadministered to treat a given bleed.1
1 PREPAREBEFORE
ANY BLEEDS
3 MONITORBEYOND
THE BLEED
Assess the bleed and proceed with a plan Follow a protocol for when and how patients and caregivers
should use BPAs during HEMLIBRA prophylaxisEnsure patients consult with you fi rst when aPCC doses>100 U/kg are required
Discuss how to approach repeated dosing of any BPA2 IN THE EVENT OF A BLEED
TREAT
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
ABR=annualized bleed rate; FVIII=factor VIII; IQR=interquartile range.* Defi ned as bleeds treated with BPAs (standardized bleed defi nition adapted from the International Society on Thrombosis and Haemostasis [ISTH]).2
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Select Important Safety InformationMost Common Adverse ReactionsThe most common adverse reactions (incidence ≥ 10%) are injection site reactions, headache, and arthralgia.
rFVIIa=recombinant factor VIIa.
References: 1.Data on fi le. Genentech, Inc. 2.Oldenburg J, Mahlangu JN, Kim B, et al. Emicizumab prophylaxis in hemophilia A with inhibitors.N Engl J Med.2017;377(9):809-818, Supplement, and Protocol.3. Uchida N, Sambe T, Yoneyama K, et al. A first-in-human phase 1 study of ACE910, a novel factor VIII–mimetic bispecifi c antibody, in healthy subjects.Blood. 2016;127(13):1633-1641.4.National Hemophilia Foundation. MASAC update on the approval and availability of the new treatment: emicizumab (Hemlibra), for persons with hemophilia A with inhibitors to factor VIII: interim guidance on acute bleed management and use of laboratory assays. 2017;1-4. 5. Kruse-Jarres R, Callaghan MU, Croteau SE, et al. Surgical experience in two multicenter, open-label phase 3 studies of emicizumab in persons with hemophilia A with inhibitors (HAVEN 1 and HAVEN 2) [abstract]. Presented at: ASH 59th Annual Meeting of the American Society of Hematology; December 9-12, 2017; Atlanta, GA.
As observed over 24 weeks (HAVEN 1) and 30 weeks (HAVEN 2)
%63 6%
FPO
T:21.75”
T:17”
B:21.75”
B:17”
F:5.375”
FS:5.125”
F:5.5”
FS:5”
F:5.5”
FS:5”
F:5.375”

GEN01-1077-2 BleedGuide_DR3.indd5-15-2018 4:24 PM
1
JobClientMedia TypeLiveTrimBleedPubs
NoneNoneNoneNone21.75” x 17”NoneNone
Job info
None
Notes
Art DirectorCopywriterAccount MgrStudio ArtistProofreader
NoneNoneNoneNoneNone
Approvals
FontsAvenir (Heavy, Black, Book, Roman , Medium, Light, Book Oblique, Oblique, Black Oblique, Heavy Oblique), TradeGothic LT (CondEighteen), TradeGothic LT BdCondTwenty (Regular), Arial (Bold), Minion Pro (Regular)
ImagesGENE1077_2_Dieline.ai (100%), 101317_Hemlibra_US_External_Logo_150_CMYK_TM.eps (16.49%, 16.5%, 7.95%, 8.04%, 13.1%, 13.11%), Genentech_logo.ai (26.5%), Screen Shot 2018-03-20 at 11.42.01.png (RGB; 533 ppi, 518 ppi; 13.5%, 13.87%), Screen Shot 2018-03-20 at 12.19.03.png (RGB; 527 ppi; 13.66%)
Inks Cyan, Magenta, Yellow, Black, Dieline, FPO
Fonts & Images
Saved at Nonefrom Melissa Love’s Macbook Pro Printed At
IndicationHEMLIBRA is indicated for routine prophylaxis to prevent or reduce the frequencyof bleeding episodes in adult and pediatric patients with hemophilia A with factor VIII inhibitors.
Important Safety InformationBoxed WARNING: THROMBOTIC MICROANGIOPATHY and THROMBOEMBOLISMCases of thrombotic microangiopathy and thrombotic events were reported when on average a cumulative amount of >100 U/kg/24 hours of activated prothrombincomplex concentrate (aPCC) was administered for 24 hours or more to patients receiving HEMLIBRA prophylaxis. Monitor for the development of thrombotic microangiopathy and thrombotic events if aPCC is administered. Discontinue aPCC and suspend dosing of HEMLIBRA if symptoms occur.
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Treatingbreakthrough bleeds:A new approach Using Bypassing Agents With HEMLIBRA Prophylaxis
For HCP audiences
HEMLIBRA® is a registered trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The HEMLIBRA logo is a trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The Genentech logo is a registered trademark of Genentech, Inc. ©2018 Genentech USA, Inc. All rights reserved. EMI/080317/0065(3) 05/18
A new approach to treating breakthrough bleeds when using concomitant BPAs
• Patients with TMA presented with thrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury, without severe defi ciencies in ADAMTS13 activity
1 additional TMA case occurred after the data cutoff for the primary analysis1
• The patient passed away and the investigator determined the cause of deathwas unrelated to HEMLIBRA
4 events fully resolved following aPCC discontinuation and suspension of HEMLIBRA1,2
• In the limited experience with these events, treatment included supportive care with or without hemodialysis/plasmapheresis
• Evidence of improvementwas seen within 1 week
• Both patients recovered within 3 weeks, with 1 patient electing to resume HEMLIBRA—without recurrence
• No thrombotic event required anticoagulation therapy
• Evidence of improvement wasseen within 1 month
• Both patients fully recovered,with 1 patient electing to resume HEMLIBRA — without recurrence
TMA and thrombotic events reported in HAVEN 1
Thrombotic microangiopathy (TMA) and thrombotic events werereported when on average a cumulative amount of >100 U/kg/24 hours of aPCC was administered for ≥24 hours to patients receivingHEMLIBRA prophylaxis
aPCC=activated prothrombin complex concentrate.† Based on data from HAVEN 1: a randomized, multicenter, open-label clinical trial of patients with hemophilia A with FVIII inhibitors aged 12 years and older (N=109, all males). The primary endpoint was reduction in treated bleeds over 24 weeks with prophylactic HEMLIBRA vs no prophylaxis.
‡ Based on data from HAVEN 2 (interim analysis): a single-arm, multicenter, open-label clinical study of patients with hemophilia A with FVIII inhibitors aged <12 years and 12-17 years weighing <40 kg. HAVEN 2 outcomes are from aninterim analysis. The interim effi cacy analysis examined reduction in bleeds at 30 weeks. The interim intra-patient analysis evaluated ABR in patients switching to HEMLIBRA following previous prophylactic BPAs (n=15) or previous on-demand BPAs (n=3) at a median study duration of 59 weeks. Statistical signifi cance will be conducted at fi nal analysis.1
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=35)
No prophylaxis (n=18)
Median ABR in HAVEN 1 was 0 (IQR: 0; 3.7) with HEMLIBRA prophylaxis vs 18.8 (IQR: 13.0; 35.1) with no prophylaxis
Median ABR in HAVEN 2 was 0 (IQR: 0; 0) with HEMLIBRA prophylaxis 1
Signifi cantly more patients with FVIII inhibitors had 0 bleeds* with HEMLIBRA vs no prophylaxis
VS
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=59)
Sustained protection meant 0 treated bleeds for most patients1
87% FEWER BLEEDS (95% CI: 72.3; 94.3), P<0.0001ABR 2.9 (95% CI: 1.7; 5.0) vs
23.3 (95% CI: 12.3; 43.9)
98% FEWER BLEEDSin the intra-patient analysis
ABR 0.4 (95% CI: 0.2; 0.9) vs 19.8 (95% CI: 15.3; 25.7) with previous BPAs (n=18)
ABR 0.3 (95% CI: 0.1; 0.5)
86%
HAVEN 1: Adults and adolescents†
HAVEN 2 interim analysis: Children1‡
2 TMA cases1 2 thrombotic events1,2
Recovery from these events occurred in the continued presence of HEMLIBRA in plasma2,3
HEMLIBRA prophylaxis calls for a new way of using BPAs for treating breakthrough bleeds
In HAVEN 1 and HAVEN 2, no TMA or thrombotic events wereobserved with use of rFVIIa alone in patients taking HEMLIBRA1, 2
• Clinical experience was limited and of relatively short duration (median treatment exposure was 42 weeks for HAVEN 1 and 29 weeks for HAVEN 2), and cannot exclude the possibility of occurrence of events with rFVIIa when taking HEMLIBRA1
140 treatment instances in patients treated with rFVIIa in HAVEN 11
Treatment average<90 µg/kg/24 h90–180 µg/kg/24 h181–270 µg/kg/24 h>270 µg/kg/24 h
% of treatmentinstances
17343119
There is a possibility for hypercoagulability with rFVIIa with HEMLIBRA based on preclinical experiments
Select Important Safety InformationWarnings and PrecautionsThrombotic Microangiopathy (TMA) and Thromboembolism AssociatedWith HEMLIBRA and aPCCIn clinical trials, TMA was reported in 1.6% of patients (3/189) and thromboticevents were reported in 1.1% of patients (2/189). In patients who received at leastone dose of aPCC, TMA was reported in 8.3% of patients (3/36) and thromboticevents were reported in 5.6% of patients (2/36). Patients with TMA presented withthrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury,without severe defi ciencies in ADAMTS13.
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Talk to patients and caregivers about how HEMLIBRA increases coagulation potential
Select Important Safety InformationPregnancy, Lactation, Females and Males of Reproductive PotentialWomen of childbearing potential should use contraception while receiving HEMLIBRA. HEMLIBRA should be used during pregnancy only if the potential benefit for the mother outweighs the risk to the fetus. Consider developmental/health benefits, clinical need and potential adverse effects on the breastfed child and mother.
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch. You may also report side effects to Genentech at (888) 835-2555.
Monitor for TMA and thromboembolism if using aPCC*
Ensure patients and caregivers know to seek medical treatment if they suspect these eventsImmediately discontinue aPCC and suspend HEMLIBRA if theseevents occur, and manage as clinically indicatedConsider the benefi ts and risks of resuming HEMLIBRA prophylaxis following complete resolution of TMA or thrombotic events on a case-by-case basis
Educate patients and caregivers to think differentlyDiscuss which types of bleeds require BPAs while taking HEMLIBRA and the importance of seeking medical advice before treating these bleeds Describe the potential risks of TMA and thromboembolism if aPCC is taken during HEMLIBRA prophylaxisEncourage patients to update emergency medical informationand to inform all healthcare providers
* Monitoring includes D-dimer, prothrombin fragment F1+2 (if available), platelet count, serum creatinine, LDH, and peripheral blood smear analysis for schistocytes. For patients who require multiple BPA doses, laboratorymonitoring should be performed every 24 – 48 hours thereafter until 24 – 48 hours following the last BPA doseadministered to treat a given bleed.1
1 PREPAREBEFORE
ANY BLEEDS
3 MONITORBEYOND
THE BLEED
Assess the bleed and proceed with a plan Follow a protocol for when and how patients and caregivers
should use BPAs during HEMLIBRA prophylaxisEnsure patients consult with you fi rst when aPCC doses>100 U/kg are required
Discuss how to approach repeated dosing of any BPA2 IN THE EVENT OF A BLEED
TREAT
Please see accompanying HEMLIBRA full Prescribing Information, including BoxedWARNING, and additional Important Safety Information throughout this brochure.
ABR=annualized bleed rate; FVIII=factor VIII; IQR=interquartile range. * Defi ned as bleeds treated with BPAs (standardized bleed defi nition adapted from the International Society on Thrombosis and Haemostasis [ISTH]).2
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Select Important Safety InformationMost Common Adverse ReactionsThe most common adverse reactions (incidence ≥ 10%) are injection site reactions, headache, and arthralgia.
rFVIIa=recombinant factor VIIa.
References: 1.Data on fi le. Genentech, Inc. 2.Oldenburg J, Mahlangu JN, Kim B, et al. Emicizumab prophylaxis in hemophilia A with inhibitors.N Engl J Med.2017;377(9):809-818, Supplement, and Protocol.3. Uchida N, Sambe T, Yoneyama K, et al. A first-in-human phase 1 study of ACE910, a novel factor VIII–mimetic bispecifi c antibody, in healthy subjects.Blood. 2016;127(13):1633-1641.4.National Hemophilia Foundation. MASAC update on the approval and availability of the new treatment: emicizumab (Hemlibra), for persons with hemophilia A with inhibitors to factor VIII: interim guidance on acute bleed management and use of laboratory assays. 2017;1-4. 5. Kruse-Jarres R, Callaghan MU, Croteau SE, et al. Surgical experience in two multicenter, open-label phase 3 studies of emicizumab in persons with hemophilia A with inhibitors (HAVEN 1 and HAVEN 2) [abstract]. Presented at: ASH 59th Annual Meeting of the American Society of Hematology; December 9-12, 2017; Atlanta, GA.
As observed over 24 weeks (HAVEN 1) and 30 weeks (HAVEN 2)
%63 6%
FPO
T:21.75”T:17”
B:21.75”B:17”
F:5.375”
FS:5.125”
F:5.5”
FS:5”
F:5.5”
FS:5”
F:5.375”
GEN01-1077-2 BleedGuide_DR3.indd5-15-2018 4:24 PM
1
JobClientMedia TypeLiveTrimBleedPubs
NoneNoneNoneNone21.75” x 17”NoneNone
Job info
None
Notes
Art DirectorCopywriterAccount MgrStudio ArtistProofreader
NoneNoneNoneNoneNone
Approvals
FontsAvenir (Light, Black, Heavy, Book, Roman , Medium, Book Oblique, Heavy Oblique), TradeGothic LT BdCondTwenty (Regular)
ImagesGENE1077_2_Dieline.ai (100%, -100%), 101317_Hemlibra_US_External_Logo_150_CMYK_TM.eps (13.1%, 13.11%)
Inks Cyan, Magenta, Yellow, Black, Dieline
Fonts & Images
Saved at Nonefrom Melissa Love’s Macbook Pro Printed At
In a pooled safety analysis of 189 HEMLIBRA patients
36 patients used aPCC
Reported incidence: TMA 8.3% (3/36); thrombotic events 5.6% (2/36)*
125 instances of aPCC treatment with HEMLIBRA
Average cumulative amount of aPCC over 24 hours (U/kg/24 hours)
aPCC duration(hours)
<50 50–100 >100
<24 7 76 18
24–48 0 6
3 treatment instances
1 thrombotic event
>48 1 4
10 treatment instances
3 TMA cases1 thrombotic
event
No events occurred when aPCC was used for <24 hours
5 of the 13 treatmentinstances reportedTMA and thromboticevents when using cumulative amounts of aPCC averaging >100 U/kg/24 hours for ≥24 hours
HEMLIBRA safety was evaluated in the largest clinical trial program of patients with FVIII inhibitors*
• Analysis of the use of additional BPAs for minor surgeries or procedures was not an objective of the 2 pivotal studies, and there is limited experience from the clinical trials
Management of perioperative BPA treatment was determined based on the investigator’s discretion5
• 29 surgeries were conducted in 22 patients; 69% (20/29) were managed without prophylactic BPAs
Select Important Safety InformationDrug InteractionsClinical experience suggests that a drug interaction exists with HEMLIBRA and aPCC. There is a possibility for hypercoagulability with activated recombinant factor VII (rFVIIa)or FVIII with HEMLIBRA based on preclinical experiments.
* Surgeries included 1 right knee arthroscopy, synovectomy, debridement of arthrofibrosis, and chondroplasty;1 laparoscopic appendectomy; 9 central venous access device-related procedures; 6 tooth extractions; and 12 other minor surgical procedures.
† 3 surgeries resulting in post-operative bleeding were treated with rFVIIa.‡ 8 surgeries were treated with rFVIIa and 1 surgery used a single dose of prophylactic aPCC.
Advise patients and caregivers to discontinue prophylactic use of BPAs the day before starting HEMLIBRA
Pivotal study protocol amendment following cases of TMA and thrombotic eventsAt the start of HAVEN 1, BPA usage for breakthrough bleeds requiring treatment was based on the discretion of the investigator2
Unexpected cases of TMA and thrombotic events prior to the HAVEN 1 data cutoff 2
• Events occurred when on average a cumulative amount of >100 U/kg/24 hours ofaPCC was administered for ≥24 hours to patients receiving HEMLIBRA prophylaxis
• The study protocol was later amended to consider these risks when using BPAsduring HEMLIBRA prophylaxis
No TMA or thrombotic events were reported with HEMLIBRA prophylaxis in HAVEN 21
• Results are based on an interim analysis at 30 weeks, and should beinterpreted with caution due to the short observation time
Clinical experience suggests that a drug interaction exists with HEMLIBRA and aPCC
Retrospective review of BPA use during minor surgeries and procedures in HEMLIBRA clinical studies5*
2 of the 6 post-operative bleeds were treated with on-demand BPAs†
6 (30%) resulted in apost-operative bleed†
(11%) resulted in apost-operative bleed†
1 tooth extraction resulted in asingle treated post-operative bleed†
114 (70%) did not result in
a post-operative bleed(89%) did not result in a post-operative bleed
Of the 20 surgeries managedwithout prophylactic BPAs5†
Of the 9 surgeries managedwith prophylactic BPAs5‡
8
Please see accompanying HEMLIBRA full Prescribing Information, including BoxedWARNING, and additional Important Safety Information throughout this brochure.
Select Important Safety InformationWarnings and Precautions (continued)Thrombotic Microangiopathy (TMA) and Thromboembolism AssociatedWith HEMLIBRA and aPCC (continued)Consider the benefits and risks if aPCC must be used in a patient receiving HEMLIBRAprophylaxis. Monitor for the development of TMA and/or thromboembolism whenadministering aPCC. Immediately discontinue aPCC and interrupt HEMLIBRAprophylaxis if clinical symptoms, imaging, or laboratory findings consistent with TMAand/or thromboembolism occur, and manage as clinically indicated. Consider thebenefits and risks of resuming HEMLIBRA prophylaxis following complete resolution ofTMA and/or thrombotic events on a case-by-case basis.
BPA=bypassing agent.* Based on pooled data from a randomized trial (HAVEN 1), single-arm trial (HAVEN 2), and a dose-finding trial, in which a total of 189 male patients with hemophilia A received at least 1 dose of HEMLIBRA as routine prophylaxis. Ninety-four patients (50%) were adults (aged 18 years and older), 38 (20%) were adolescents (aged 12 to under 18 years), 55 (29%) were children (2 years to under 12 years), and 2 (1%) were infants (1 month to under 2 years). Seven of the 189 patients (4%) included in the safety population were patients without FVIII inhibitors from the dose-finding trial.
* Overall, TMA and thrombotic events were reported in 1.6% (3/189) and 1.1% (2/189) of patients, respectively.
An instance of aPCC treatment is defined as all doses of aPCC received by a patient, for any reason, until there was a 36-hour treatment-free break.
Synergistic thrombin generation has been shown with aPCC in combination with HEMLIBRA in vitro and in vivo2
• aPCC contains coagulation factors that can accumulate with multiple doses, and supplies substrates for HEMLIBRA that result in overcorrection of clotting4
Select Important Safety InformationWarnings and Precautions (continued) Laboratory Coagulation Test InterferenceHEMLIBRA affects intrinsic pathway clotting-based laboratory tests, including activated clotting time (ACT), activated partial thromboplastin time (aPTT), and all assays based on aPTT, such as one-stage factor VIII (FVIII) activity. Intrinsic pathway clotting-based laboratory tests should not be used.
Results affected by HEMLIBRA: aPTT; Bethesda assays (clotting-based) for FVIII inhibitor titers; one-stage, aPTT-based, single-factor assays; aPTT-based Activated Protein C resistance (APC-R); ACT.
T:21.75”
T:17”
B:21.75”
B:17”
F:5.375”
FS:5.125”
F:5.5”
FS:5”
F:5.5”
FS:5”
F:5.375”

GEN01-1077-2 BleedGuide_DR3.indd5-15-2018 4:24 PM
1
JobClientMedia TypeLiveTrimBleedPubs
NoneNoneNoneNone21.75” x 17”NoneNone
Job info
None
Notes
Art DirectorCopywriterAccount MgrStudio ArtistProofreader
NoneNoneNoneNoneNone
Approvals
FontsAvenir (Light, Black, Heavy, Book, Roman , Medium, Book Oblique, Heavy Oblique), TradeGothic LT BdCondTwenty (Regular)
ImagesGENE1077_2_Dieline.ai (100%, -100%), 101317_Hemlibra_US_External_Logo_150_CMYK_TM.eps (13.1%, 13.11%)
Inks Cyan, Magenta, Yellow, Black, Dieline
Fonts & Images
Saved at Nonefrom Melissa Love’s Macbook Pro Printed At
In a pooled safety analysis of 189 HEMLIBRA patients
36 patients used aPCCReported incidence: TMA 8.3% (3/36); thrombotic events 5.6% (2/36)*
125 instances of aPCC treatment with HEMLIBRA
Average cumulative amount of aPCC over 24 hours (U/kg/24 hours)
aPCC duration(hours)
<50 50–100 >100
<24 7 76 18
24–48 0 6
3 treatment instances
1 thrombotic event
>48 1 4
10 treatment instances
3 TMA cases1 thrombotic
event
No events occurred when aPCC was used for <24 hours
5 of the 13 treatment instances reported TMA and thrombotic events when using cumulative amounts of aPCC averaging >100 U/kg/24 hours for ≥24 hours
HEMLIBRA safety was evaluated in the largest clinical trial program of patients with FVIII inhibitors*
• Analysis of the use of additional BPAs for minor surgeries or procedures was not an objective of the 2 pivotal studies, and there is limited experience from the clinical trials
Management of perioperative BPA treatment was determined based on the investigator’s discretion5
• 29 surgeries were conducted in 22 patients; 69% (20/29) were managed without prophylactic BPAs
Select Important Safety InformationDrug InteractionsClinical experience suggests that a drug interaction exists with HEMLIBRA and aPCC. There is a possibility for hypercoagulability with activated recombinant factor VII (rFVIIa)or FVIII with HEMLIBRA based on preclinical experiments.
* Surgeries included 1 right knee arthroscopy, synovectomy, debridement of arthrofibrosis, and chondroplasty;1 laparoscopic appendectomy; 9 central venous access device-related procedures; 6 tooth extractions; and 12 other minor surgical procedures.
† 3 surgeries resulting in post-operative bleeding were treated with rFVIIa.‡ 8 surgeries were treated with rFVIIa and 1 surgery used a single dose of prophylactic aPCC.
Advise patients and caregivers to discontinue prophylactic use of BPAs the day before starting HEMLIBRA
Pivotal study protocol amendment following cases of TMA and thrombotic eventsAt the start of HAVEN 1, BPA usage for breakthrough bleeds requiring treatment was based on the discretion of the investigator2
Unexpected cases of TMA and thrombotic events prior to the HAVEN 1 data cutoff 2
• Events occurred when on average a cumulative amount of >100 U/kg/24 hours ofaPCC was administered for ≥24 hours to patients receiving HEMLIBRA prophylaxis
• The study protocol was later amended to consider these risks when using BPAs during HEMLIBRA prophylaxis
No TMA or thrombotic events were reported with HEMLIBRA prophylaxis in HAVEN 21
• Results are based on an interim analysis at 30 weeks, and should be interpreted with caution due to the short observation time
Clinical experience suggests that a drug interaction exists with HEMLIBRA and aPCC
Retrospective review of BPA use during minor surgeries and procedures in HEMLIBRA clinical studies5*
2 of the 6 post-operative bleeds were treated with on-demand BPAs†
6 (30%) resulted in apost-operative bleed†
(11%) resulted in apost-operative bleed†
1 tooth extraction resulted in asingle treated post-operative bleed†
114 (70%) did not result in
a post-operative bleed(89%) did not result in a post-operative bleed
Of the 20 surgeries managedwithout prophylactic BPAs5†
Of the 9 surgeries managedwith prophylactic BPAs5‡
8
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Select Important Safety InformationWarnings and Precautions (continued)Thrombotic Microangiopathy (TMA) and Thromboembolism Associated With HEMLIBRA and aPCC (continued)Consider the benefits and risks if aPCC must be used in a patient receiving HEMLIBRA prophylaxis. Monitor for the development of TMA and/or thromboembolism when administering aPCC. Immediately discontinue aPCC and interrupt HEMLIBRA prophylaxis if clinical symptoms, imaging, or laboratory findings consistent with TMA and/or thromboembolism occur, and manage as clinically indicated. Consider the benefits and risks of resuming HEMLIBRA prophylaxis following complete resolution of TMA and/or thrombotic events on a case-by-case basis.
BPA=bypassing agent.* Based on pooled data from a randomized trial (HAVEN 1), single-arm trial (HAVEN 2), and a dose-finding trial, in which a total of 189 male patients with hemophilia A received at least 1 dose of HEMLIBRA as routine prophylaxis. Ninety-four patients (50%) were adults (aged 18 years and older), 38 (20%) were adolescents(aged 12 to under 18 years), 55 (29%) were children (2 years to under 12 years), and 2 (1%) were infants (1 month to under 2 years). Seven of the 189 patients (4%) included in the safety population were patients without FVIII inhibitors from the dose-finding trial.
* Overall, TMA and thrombotic events were reported in 1.6% (3/189) and 1.1% (2/189) of patients, respectively.
An instance of aPCC treatment is defined as all doses of aPCC received by a patient, for any reason, until there was a 36-hour treatment-free break.
Synergistic thrombin generation has been shown with aPCC in combination with HEMLIBRA in vitro and in vivo2
• aPCC contains coagulation factors that can accumulate with multiple doses,and supplies substrates for HEMLIBRA that result in overcorrection of clotting4
Select Important Safety InformationWarnings and Precautions (continued)Laboratory Coagulation Test InterferenceHEMLIBRA affects intrinsic pathway clotting-based laboratory tests, including activatedclotting time (ACT), activated partial thromboplastin time (aPTT), and all assays basedon aPTT, such as one-stage factor VIII (FVIII) activity. Intrinsic pathway clotting-basedlaboratory tests should not be used.
Results affected by HEMLIBRA: aPTT; Bethesda assays (clotting-based) for FVIII inhibitortiters; one-stage, aPTT-based, single-factor assays; aPTT-based Activated Protein Cresistance (APC-R); ACT.
T:21.75”
T:17”
B:21.75”
B:17”
F:5.375”
FS:5.125”
F:5.5”
FS:5”
F:5.5”
FS:5”
F:5.375”
GEN01-1077-2 BleedGuide_DR3.indd5-15-2018 4:24 PM
1
JobClientMedia TypeLiveTrimBleedPubs
NoneNoneNoneNone21.75” x 17”NoneNone
Job info
None
Notes
Art DirectorCopywriterAccount MgrStudio ArtistProofreader
NoneNoneNoneNoneNone
Approvals
FontsAvenir (Heavy, Black, Book, Roman , Medium, Light, Book Oblique, Oblique, Black Oblique, Heavy Oblique), TradeGothic LT (CondEighteen), TradeGothic LT BdCondTwenty (Regular), Arial (Bold), Minion Pro (Regular)
ImagesGENE1077_2_Dieline.ai (100%), 101317_Hemlibra_US_External_Logo_150_CMYK_TM.eps (16.49%, 16.5%, 7.95%, 8.04%, 13.1%, 13.11%), Genentech_logo.ai (26.5%), Screen Shot 2018-03-20 at 11.42.01.png (RGB; 533 ppi, 518 ppi; 13.5%, 13.87%), Screen Shot 2018-03-20 at 12.19.03.png (RGB; 527 ppi; 13.66%)
Inks Cyan, Magenta, Yellow, Black, Dieline, FPO
Fonts & Images
Saved atNone fromMelissa Love’s Macbook ProPrinted At
IndicationHEMLIBRA is indicated for routine prophylaxis to prevent or reduce the frequencyof bleeding episodes in adult and pediatric patients with hemophilia A with factor VIII inhibitors.
Important Safety InformationBoxed WARNING: THROMBOTIC MICROANGIOPATHY and THROMBOEMBOLISMCases of thrombotic microangiopathy and thrombotic events were reported when on average a cumulative amount of >100 U/kg/24 hours of activated prothrombincomplex concentrate (aPCC) was administered for 24 hours or more to patients receiving HEMLIBRA prophylaxis. Monitor for the development of thrombotic microangiopathy and thrombotic events if aPCC is administered. Discontinue aPCC and suspend dosing of HEMLIBRA if symptoms occur.
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Treatingbreakthrough bleeds:A new approach Using Bypassing Agents With HEMLIBRA Prophylaxis
For HCP audiences
HEMLIBRA® is a registered trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The HEMLIBRA logo is a trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The Genentech logo is a registered trademark of Genentech, Inc. ©2018 Genentech USA, Inc. All rights reserved. EMI/080317/0065(3) 05/18
A new approach to treating breakthrough bleeds when using concomitant BPAs
• Patients with TMA presented with thrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury, without severe defi ciencies in ADAMTS13 activity
1 additional TMA case occurred after the data cutoff for the primary analysis1
• The patient passed away and the investigator determined the cause of deathwas unrelated to HEMLIBRA
4 events fully resolved following aPCC discontinuation and suspension of HEMLIBRA1,2
• In the limited experience with these events, treatment included supportive care with or without hemodialysis/plasmapheresis
• Evidence of improvementwas seen within 1 week
• Both patients recovered within 3 weeks, with 1 patient electing to resume HEMLIBRA—without recurrence
• No thrombotic event required anticoagulation therapy
• Evidence of improvement wasseen within 1 month
• Both patients fully recovered,with 1 patient electing to resume HEMLIBRA — without recurrence
TMA and thrombotic events reported in HAVEN 1
Thrombotic microangiopathy (TMA) and thrombotic events werereported when on average a cumulative amount of >100 U/kg/24 hours of aPCC was administered for ≥24 hours to patients receivingHEMLIBRA prophylaxis
aPCC=activated prothrombin complex concentrate.†Based on data from HAVEN 1: a randomized, multicenter, open-label clinical trial of patients with hemophiliaA with FVIII inhibitors aged 12 years and older (N=109, all males). The primary endpoint was reduction in treated bleeds over 24 weeks with prophylactic HEMLIBRA vs no prophylaxis.
‡ Based on data from HAVEN 2 (interim analysis): a single-arm, multicenter, open-label clinical study of patients with hemophilia A with FVIII inhibitors aged <12 years and 12-17 years weighing <40 kg. HAVEN 2 outcomes are from aninterim analysis. The interim effi cacy analysis examined reduction in bleeds at 30 weeks. The interim intra-patient analysis evaluated ABR in patients switching to HEMLIBRA following previous prophylactic BPAs (n=15) or previous on-demand BPAs (n=3) at a median study duration of 59 weeks. Statistical signifi cance will be conducted at fi nal analysis.1
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=35)
No prophylaxis(n=18)
Median ABR in HAVEN 1 was 0 (IQR: 0; 3.7) with HEMLIBRA prophylaxis vs 18.8 (IQR: 13.0; 35.1) with no prophylaxis
Median ABR in HAVEN 2 was 0 (IQR: 0; 0) with HEMLIBRA prophylaxis 1
Signifi cantly more patients with FVIII inhibitors had 0 bleeds*
with HEMLIBRA vs no prophylaxis
VS
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=59)
Sustained protection meant 0 treated bleeds for most patients1
87% FEWER BLEEDS (95% CI: 72.3; 94.3), P<0.0001ABR 2.9 (95% CI: 1.7; 5.0) vs
23.3 (95% CI: 12.3; 43.9)
98% FEWER BLEEDSin the intra-patient analysis
ABR 0.4 (95% CI: 0.2; 0.9) vs19.8 (95% CI: 15.3; 25.7)with previous BPAs (n=18)
ABR 0.3 (95% CI: 0.1; 0.5)
86%
HAVEN 1: Adults and adolescents†
HAVEN 2 interim analysis: Children1‡
2 TMA cases1 2 thrombotic events1,2
Recovery from these events occurred in the continued presence of HEMLIBRA in plasma2,3
HEMLIBRA prophylaxis calls for a new way of using BPAs for treating breakthrough bleeds
In HAVEN 1 and HAVEN 2, no TMA or thrombotic events were observed with use of rFVIIa alone in patients taking HEMLIBRA1, 2
• Clinical experience was limited and of relatively short duration (median treatmentexposure was 42 weeks for HAVEN 1 and 29 weeks for HAVEN 2), and cannot excludethe possibility of occurrence of events with rFVIIa when taking HEMLIBRA1
140 treatment instances in patients treated with rFVIIa in HAVEN 11
Treatment average <90 µg/kg/24 h 90–180 µg/kg/24 h 181–270 µg/kg/24 h >270 µg/kg/24 h
% of treatment instances
17 34 31 19
There is a possibility for hypercoagulability with rFVIIa with HEMLIBRA based on preclinical experiments
Select Important Safety InformationWarnings and PrecautionsThrombotic Microangiopathy (TMA) and Thromboembolism Associated With HEMLIBRA and aPCCIn clinical trials, TMA was reported in 1.6% of patients (3/189) and thrombotic events were reported in 1.1% of patients (2/189). In patients who received at least one dose of aPCC, TMA was reported in 8.3% of patients (3/36) and thrombotic events were reported in 5.6% of patients (2/36). Patients with TMA presented with thrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury, without severe deficiencies in ADAMTS13.
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Talk to patients and caregivers about how HEMLIBRA increases coagulation potential
Select Important Safety InformationPregnancy, Lactation, Females and Males of Reproductive PotentialWomen of childbearing potential should use contraception while receiving HEMLIBRA. HEMLIBRA should be used during pregnancy only if the potential benefit for the mother outweighs the risk to the fetus. Consider developmental/health benefits, clinical need and potential adverse effects on the breastfed child and mother.
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch. You may also report side effects to Genentech at (888) 835-2555.
Monitor for TMA and thromboembolism if using aPCC*
Ensure patients and caregivers know to seek medical treatment if they suspect these eventsImmediately discontinue aPCC and suspend HEMLIBRA if theseevents occur, and manage as clinically indicatedConsider the benefi ts and risks of resuming HEMLIBRA prophylaxis following complete resolution of TMA or thrombotic events on a case-by-case basis
Educate patients and caregivers to think differentlyDiscuss which types of bleeds require BPAs while taking HEMLIBRA and the importance of seeking medical advice before treating these bleeds Describe the potential risks of TMA and thromboembolism if aPCCis taken during HEMLIBRA prophylaxisEncourage patients to update emergency medical informationand to inform all healthcare providers
* Monitoring includes D-dimer, prothrombin fragment F1+2 (if available), platelet count, serum creatinine, LDH, and peripheral blood smear analysis for schistocytes. For patients who require multiple BPA doses, laboratorymonitoring should be performed every 24 – 48 hours thereafter until 24 – 48 hours following the last BPA doseadministered to treat a given bleed.1
1 PREPARE
BEFORE ANY BLEEDS
3 MONITOR
BEYOND THE BLEED
Assess the bleed and proceed with a plan Follow a protocol for when and how patients and caregivers
should use BPAs during HEMLIBRA prophylaxisEnsure patients consult with you fi rst when aPCC doses>100 U/kg are required
Discuss how to approach repeated dosing of any BPA 2 IN THE EVENT OF A BLEED
TREAT
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
ABR=annualized bleed rate; FVIII=factor VIII; IQR=interquartile range.* Defi ned as bleeds treated with BPAs (standardized bleed defi nition adapted from the International Society on Thrombosis and Haemostasis [ISTH]).2
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Select Important Safety InformationMost Common Adverse ReactionsThe most common adverse reactions (incidence ≥ 10%) are injection site reactions, headache, and arthralgia.
rFVIIa=recombinant factor VIIa.
References: 1. Data on fi le. Genentech, Inc. 2. Oldenburg J, Mahlangu JN, Kim B, et al. Emicizumab prophylaxis in hemophilia A with inhibitors. N Engl J Med. 2017;377(9):809-818, Supplement, and Protocol. 3. Uchida N, Sambe T, Yoneyama K, et al. A fi rst-in-human phase 1 study of ACE910, a novel factor VIII–mimetic bispecifi c antibody, in healthy subjects. Blood. 2016;127(13):1633-1641. 4. National Hemophilia Foundation. MASAC update on the approval and availability of the new treatment: emicizumab (Hemlibra), for persons with hemophilia A with inhibitors to factor VIII: interim guidance on acute bleed management and use of laboratory assays. 2017;1-4. 5. Kruse-Jarres R, Callaghan MU, Croteau SE, et al. Surgical experience in two multicenter, open-label phase 3 studies of emicizumab in persons with hemophilia A with inhibitors (HAVEN 1 and HAVEN 2) [abstract]. Presented at: ASH 59th Annual Meeting of the American Society of Hematology; December 9-12, 2017; Atlanta, GA.
As observed over 24 weeks(HAVEN 1) and 30 weeks (HAVEN 2)
%63 6
%
FPO
T:21.75”
T:17
”
B:21.75”
B:17
”
F:5.375”
FS:5.125”
F:5.5”
FS:5”
F:5.5”
FS:5”
F:5.375”

GEN01-1077-2 BleedGuide_DR3.indd5-15-2018 4:24 PM
1
JobClientMedia TypeLiveTrimBleedPubs
NoneNoneNoneNone21.75” x 17”NoneNone
Job info
None
Notes
Art DirectorCopywriterAccount MgrStudio ArtistProofreader
NoneNoneNoneNoneNone
Approvals
FontsAvenir (Light, Black, Heavy, Book, Roman , Medium, Book Oblique, Heavy Oblique), TradeGothic LT BdCondTwenty (Regular)
ImagesGENE1077_2_Dieline.ai (100%, -100%), 101317_Hemlibra_US_External_Logo_150_CMYK_TM.eps (13.1%, 13.11%)
Inks Cyan, Magenta, Yellow, Black, Dieline
Fonts & Images
Saved at Nonefrom Melissa Love’s Macbook Pro Printed At
In a pooled safety analysis of 189 HEMLIBRA patients
36 patients used aPCC
Reported incidence: TMA 8.3% (3/36); thrombotic events 5.6% (2/36)*
125 instances of aPCC treatment with HEMLIBRA
Average cumulative amount of aPCC over 24 hours (U/kg/24 hours)
aPCC duration(hours)
<50 50–100 >100
<24 7 76 18
24–48 0 6
3 treatment instances
1 thrombotic event
>48 1 4
10 treatment instances
3 TMA cases1 thrombotic
event
No events occurred when aPCC was used for <24 hours
5 of the 13 treatmentinstances reportedTMA and thromboticevents when using cumulative amounts of aPCC averaging >100 U/kg/24 hours for ≥24 hours
HEMLIBRA safety was evaluated in the largest clinical trial program of patients with FVIII inhibitors*
• Analysis of the use of additional BPAs for minor surgeries or procedureswas not an objective of the 2 pivotal studies, and there is limited experiencefrom the clinical trials
Management of perioperative BPA treatment was determined based on the investigator’s discretion5
• 29 surgeries were conducted in 22 patients; 69% (20/29) were managedwithout prophylactic BPAs
Select Important Safety InformationDrug InteractionsClinical experience suggests that a drug interaction exists with HEMLIBRA and aPCC.There is a possibility for hypercoagulability with activated recombinant factor VII (rFVIIa)or FVIII with HEMLIBRA based on preclinical experiments.
* Surgeries included 1 right knee arthroscopy, synovectomy, debridement of arthrofibrosis, and chondroplasty; 1 laparoscopic appendectomy; 9 central venous access device-related procedures; 6 tooth extractions; and 12 other minor surgical procedures.
† 3 surgeries resulting in post-operative bleeding were treated with rFVIIa.‡ 8 surgeries were treated with rFVIIa and 1 surgery used a single dose of prophylactic aPCC.
Advise patients and caregivers to discontinue prophylactic use of BPAs the day before starting HEMLIBRA
Pivotal study protocol amendment following cases of TMA and thrombotic eventsAt the start of HAVEN 1, BPA usage for breakthrough bleeds requiring treatment was based on the discretion of the investigator2
Unexpected cases of TMA and thrombotic events prior to the HAVEN 1 data cutoff 2
• Events occurred when on average a cumulative amount of >100 U/kg/24 hours ofaPCC was administered for ≥24 hours to patients receiving HEMLIBRA prophylaxis
• The study protocol was later amended to consider these risks when using BPAs during HEMLIBRA prophylaxis
No TMA or thrombotic events were reported with HEMLIBRA prophylaxis in HAVEN 21
• Results are based on an interim analysis at 30 weeks, and should be interpreted with caution due to the short observation time
Clinical experience suggests that a drug interaction exists with HEMLIBRA and aPCC
Retrospective review of BPA use during minor surgeries and procedures in HEMLIBRA clinical studies5*
2 of the 6 post-operative bleeds were treated with on-demand BPAs†
6 (30%) resulted in a post-operative bleed†
(11%) resulted in a post-operative bleed†
1 tooth extraction resulted in a single treated post-operative bleed†
114 (70%) did not result in
a post-operative bleed(89%) did not result in a post-operative bleed
Of the 20 surgeries managed without prophylactic BPAs5†
Of the 9 surgeries managed with prophylactic BPAs5‡
8
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Select Important Safety InformationWarnings and Precautions (continued)Thrombotic Microangiopathy (TMA) and Thromboembolism Associated With HEMLIBRA and aPCC (continued)Consider the benefits and risks if aPCC must be used in a patient receiving HEMLIBRA prophylaxis. Monitor for the development of TMA and/or thromboembolism when administering aPCC. Immediately discontinue aPCC and interrupt HEMLIBRA prophylaxis if clinical symptoms, imaging, or laboratory findings consistent with TMA and/or thromboembolism occur, and manage as clinically indicated. Consider the benefits and risks of resuming HEMLIBRA prophylaxis following complete resolution of TMA and/or thrombotic events on a case-by-case basis.
BPA=bypassing agent.* Based on pooled data from a randomized trial (HAVEN 1), single-arm trial (HAVEN 2), and a dose-finding trial, in which a total of 189 male patients with hemophilia A received at least 1 dose of HEMLIBRA as routine prophylaxis. Ninety-four patients (50%) were adults (aged 18 years and older), 38 (20%) were adolescents(aged 12 to under 18 years), 55 (29%) were children (2 years to under 12 years), and 2 (1%) were infants (1 month to under 2 years). Seven of the 189 patients (4%) included in the safety population were patients without FVIII inhibitors from the dose-finding trial.
* Overall, TMA and thrombotic events were reported in 1.6% (3/189) and 1.1% (2/189) of patients, respectively.
An instance of aPCC treatment is defined as all doses of aPCC received by a patient, for any reason, until there was a 36-hour treatment-free break.
Synergistic thrombin generation has been shown with aPCC in combination with HEMLIBRA in vitro and in vivo2
• aPCC contains coagulation factors that can accumulate with multiple doses, and supplies substrates for HEMLIBRA that result in overcorrection of clotting4
Select Important Safety InformationWarnings and Precautions (continued) Laboratory Coagulation Test InterferenceHEMLIBRA affects intrinsic pathway clotting-based laboratory tests, including activated clotting time (ACT), activated partial thromboplastin time (aPTT), and all assays based on aPTT, such as one-stage factor VIII (FVIII) activity. Intrinsic pathway clotting-based laboratory tests should not be used.
Results affected by HEMLIBRA: aPTT; Bethesda assays (clotting-based) for FVIII inhibitor titers; one-stage, aPTT-based, single-factor assays; aPTT-based Activated Protein C resistance (APC-R); ACT.
T:21.75”T:17”
B:21.75”B:17”
F:5.375”
FS:5.125”
F:5.5”
FS:5”
F:5.5”
FS:5”
F:5.375”

GEN01-1077-2 BleedGuide_DR3.indd5-15-2018 4:24 PM
1
JobClientMedia TypeLiveTrimBleedPubs
NoneNoneNoneNone21.75” x 17”NoneNone
Job info
None
Notes
Art DirectorCopywriterAccount MgrStudio ArtistProofreader
NoneNoneNoneNoneNone
Approvals
FontsAvenir (Heavy, Black, Book, Roman , Medium, Light, Book Oblique, Oblique, Black Oblique, Heavy Oblique), TradeGothic LT (CondEighteen), TradeGothic LT BdCondTwenty (Regular), Arial (Bold), Minion Pro (Regular)
ImagesGENE1077_2_Dieline.ai (100%), 101317_Hemlibra_US_External_Logo_150_CMYK_TM.eps (16.49%, 16.5%, 7.95%, 8.04%, 13.1%, 13.11%), Genentech_logo.ai (26.5%), Screen Shot 2018-03-20 at 11.42.01.png (RGB; 533 ppi, 518 ppi; 13.5%, 13.87%), Screen Shot 2018-03-20 at 12.19.03.png (RGB; 527 ppi; 13.66%)
Inks Cyan, Magenta, Yellow, Black, Dieline, FPO
Fonts & Images
Saved at Nonefrom Melissa Love’s Macbook Pro Printed At
IndicationHEMLIBRA is indicated for routine prophylaxis to prevent or reduce the frequencyof bleeding episodes in adult and pediatric patients with hemophilia A with factor VIII inhibitors.
Important Safety InformationBoxed WARNING: THROMBOTIC MICROANGIOPATHY and THROMBOEMBOLISMCases of thrombotic microangiopathy and thrombotic events were reported when on average a cumulative amount of >100 U/kg/24 hours of activated prothrombincomplex concentrate (aPCC) was administered for 24 hours or more to patients receiving HEMLIBRA prophylaxis. Monitor for the development of thrombotic microangiopathy and thrombotic events if aPCC is administered. Discontinue aPCC and suspend dosing of HEMLIBRA if symptoms occur.
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Treatingbreakthrough bleeds:A new approach Using Bypassing Agents With HEMLIBRA Prophylaxis
For HCP audiences
HEMLIBRA® is a registered trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The HEMLIBRA logo is a trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The Genentech logo is a registered trademark of Genentech, Inc. ©2018 Genentech USA, Inc. All rights reserved. EMI/080317/0065(3) 05/18
A new approach to treating breakthrough bleeds when using concomitant BPAs
• Patients with TMA presented with thrombocytopenia, microangiopathic hemolyticanemia, and acute kidney injury, without severe defi ciencies in ADAMTS13 activity
1 additional TMA case occurred after the data cutoff for the primary analysis1
• The patient passed away and the investigator determined the cause of deathwas unrelated to HEMLIBRA
4 events fully resolved following aPCC discontinuation and suspension of HEMLIBRA1,2
• In the limited experience withthese events, treatment includedsupportive care with or withouthemodialysis/plasmapheresis
• Evidence of improvementwas seen within 1 week
• Both patients recoveredwithin 3 weeks, with 1 patientelecting to resume HEMLIBRA—without recurrence
• No thrombotic event requiredanticoagulation therapy
• Evidence of improvement wasseen within 1 month
• Both patients fully recovered,with 1 patient electing to resumeHEMLIBRA — without recurrence
TMA and thrombotic events reported in HAVEN 1
Thrombotic microangiopathy (TMA) and thrombotic events were reported when on average a cumulative amount of >100 U/kg/24 hours of aPCC was administered for ≥24 hours to patients receiving HEMLIBRA prophylaxis
aPCC=activated prothrombin complex concentrate.† Based on data from HAVEN 1: a randomized, multicenter, open-label clinical trial of patients with hemophilia A with FVIII inhibitors aged 12 years and older (N=109, all males). The primary endpoint was reduction in treated bleeds over 24 weeks with prophylactic HEMLIBRA vs no prophylaxis.
‡ Based on data from HAVEN 2 (interim analysis): a single-arm, multicenter, open-label clinical study of patients with hemophilia A with FVIII inhibitors aged <12 years and 12-17 years weighing <40 kg. HAVEN 2 outcomes are from an interim analysis. The interim effi cacy analysis examined reduction in bleeds at 30 weeks. The interim intra-patient analysis evaluated ABR in patients switching to HEMLIBRA following previous prophylactic BPAs (n=15) or previous on-demand BPAs (n=3) at a median study duration of 59 weeks. Statistical signifi cance will be conducted at fi nal analysis.1
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=35)
No prophylaxis(n=18)
Median ABR in HAVEN 1 was 0 (IQR: 0; 3.7) with HEMLIBRA prophylaxis vs 18.8 (IQR: 13.0; 35.1) with no prophylaxis
Median ABR in HAVEN 2 was 0 (IQR: 0; 0) with HEMLIBRA prophylaxis 1
Signifi cantly more patients with FVIII inhibitors had 0 bleeds*
with HEMLIBRA vs no prophylaxis
VS
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=59)
Sustained protection meant 0 treated bleeds for most patients1
87% FEWER BLEEDS (95% CI: 72.3; 94.3), P<0.0001ABR 2.9 (95% CI: 1.7; 5.0) vs
23.3 (95% CI: 12.3; 43.9)
98% FEWER BLEEDSin the intra-patient analysis
ABR 0.4 (95% CI: 0.2; 0.9) vs19.8 (95% CI: 15.3; 25.7)with previous BPAs (n=18)
ABR 0.3 (95% CI: 0.1; 0.5)
86%
HAVEN 1: Adults and adolescents†
HAVEN 2 interim analysis: Children1‡
2 TMA cases1 2 thrombotic events1,2
Recovery from these events occurred in the continued presence of HEMLIBRA in plasma2,3
HEMLIBRA prophylaxis calls for a new way of using BPAs for treating breakthrough bleeds
In HAVEN 1 and HAVEN 2, no TMA or thrombotic events wereobserved with use of rFVIIa alone in patients taking HEMLIBRA1, 2
• Clinical experience was limited and of relatively short duration (median treatment exposure was 42 weeks for HAVEN 1 and 29 weeks for HAVEN 2), and cannot exclude the possibility of occurrence of events with rFVIIa when taking HEMLIBRA1
140 treatment instances in patients treated with rFVIIa in HAVEN 11
Treatment average<90 µg/kg/24 h90–180 µg/kg/24 h181–270 µg/kg/24 h>270 µg/kg/24 h
% of treatmentinstances
17343119
There is a possibility for hypercoagulability with rFVIIa with HEMLIBRA based on preclinical experiments
Select Important Safety InformationWarnings and PrecautionsThrombotic Microangiopathy (TMA) and Thromboembolism Associated With HEMLIBRA and aPCCIn clinical trials, TMA was reported in 1.6% of patients (3/189) and thrombotic events were reported in 1.1% of patients (2/189). In patients who received at least one dose of aPCC, TMA was reported in 8.3% of patients (3/36) and thrombotic events were reported in 5.6% of patients (2/36). Patients with TMA presented with thrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury, without severe deficiencies in ADAMTS13.
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Talk to patients and caregivers about how HEMLIBRA increases coagulation potential
Select Important Safety InformationPregnancy, Lactation, Females and Males of Reproductive PotentialWomen of childbearing potential should use contraception while receiving HEMLIBRA. HEMLIBRA should be used during pregnancy only if the potential benefit for the mother outweighs the risk to the fetus. Consider developmental/health benefits, clinical need and potential adverse effects on the breastfed child and mother.
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch. You may also report side effects to Genentech at (888) 835-2555.
Monitor for TMA and thromboembolism if using aPCC*
Ensure patients and caregivers know to seek medical treatment if they suspect these eventsImmediately discontinue aPCC and suspend HEMLIBRA if theseevents occur, and manage as clinically indicatedConsider the benefi ts and risks of resuming HEMLIBRA prophylaxis following complete resolution of TMA or thrombotic events on a case-by-case basis
Educate patients and caregivers to think differentlyDiscuss which types of bleeds require BPAs while taking HEMLIBRA and the importance of seeking medical advice before treating these bleeds Describe the potential risks of TMA and thromboembolism if aPCC is taken during HEMLIBRA prophylaxisEncourage patients to update emergency medical informationand to inform all healthcare providers
* Monitoring includes D-dimer, prothrombin fragment F1+2 (if available), platelet count, serum creatinine, LDH, and peripheral blood smear analysis for schistocytes. For patients who require multiple BPA doses, laboratorymonitoring should be performed every 24 – 48 hours thereafter until 24 – 48 hours following the last BPA doseadministered to treat a given bleed.1
1 PREPAREBEFORE
ANY BLEEDS
3 MONITORBEYOND
THE BLEED
Assess the bleed and proceed with a plan Follow a protocol for when and how patients and caregivers
should use BPAs during HEMLIBRA prophylaxisEnsure patients consult with you fi rst when aPCC doses>100 U/kg are required
Discuss how to approach repeated dosing of any BPA2 IN THE EVENT OF A BLEED
TREAT
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
ABR=annualized bleed rate; FVIII=factor VIII; IQR=interquartile range.* Defi ned as bleeds treated with BPAs (standardized bleed defi nition adapted from the International Society on Thrombosis and Haemostasis [ISTH]).2
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Select Important Safety InformationMost Common Adverse ReactionsThe most common adverse reactions (incidence ≥ 10%) are injection site reactions, headache, and arthralgia.
rFVIIa=recombinant factor VIIa.
References: 1.Data on fi le. Genentech, Inc. 2.Oldenburg J, Mahlangu JN, Kim B, et al. Emicizumab prophylaxis in hemophilia A with inhibitors.N Engl J Med.2017;377(9):809-818, Supplement, and Protocol.3. Uchida N, Sambe T, Yoneyama K, et al. A first-in-human phase 1 study of ACE910, a novel factor VIII–mimetic bispecifi c antibody, in healthy subjects.Blood. 2016;127(13):1633-1641.4.National Hemophilia Foundation. MASAC update on the approval and availability of the new treatment: emicizumab (Hemlibra), for persons with hemophilia A with inhibitors to factor VIII: interim guidance on acute bleed management and use of laboratory assays. 2017;1-4. 5. Kruse-Jarres R, Callaghan MU, Croteau SE, et al. Surgical experience in two multicenter, open-label phase 3 studies of emicizumab in persons with hemophilia A with inhibitors (HAVEN 1 and HAVEN 2) [abstract]. Presented at: ASH 59th Annual Meeting of the American Society of Hematology; December 9-12, 2017; Atlanta, GA.
As observed over 24 weeks (HAVEN 1) and 30 weeks (HAVEN 2)
%63 6%
FPO
T:21.75”
T:17”
B:21.75”
B:17”
F:5.375”
FS:5.125”
F:5.5”
FS:5”
F:5.5”
FS:5”
F:5.375”

GEN01-1077-2 BleedGuide_DR3.indd5-15-2018 4:24 PM
1
JobClientMedia TypeLiveTrimBleedPubs
NoneNoneNoneNone21.75” x 17”NoneNone
Job info
None
Notes
Art DirectorCopywriterAccount MgrStudio ArtistProofreader
NoneNoneNoneNoneNone
Approvals
FontsAvenir (Heavy, Black, Book, Roman , Medium, Light, Book Oblique, Oblique, Black Oblique, Heavy Oblique), TradeGothic LT (CondEighteen), TradeGothic LT BdCondTwenty (Regular), Arial (Bold), Minion Pro (Regular)
ImagesGENE1077_2_Dieline.ai (100%), 101317_Hemlibra_US_External_Logo_150_CMYK_TM.eps (16.49%, 16.5%, 7.95%, 8.04%, 13.1%, 13.11%), Genentech_logo.ai (26.5%), Screen Shot 2018-03-20 at 11.42.01.png (RGB; 533 ppi, 518 ppi; 13.5%, 13.87%), Screen Shot 2018-03-20 at 12.19.03.png (RGB; 527 ppi; 13.66%)
Inks Cyan, Magenta, Yellow, Black, Dieline, FPO
Fonts & Images
Saved at Nonefrom Melissa Love’s Macbook Pro Printed At
IndicationHEMLIBRA is indicated for routine prophylaxis to prevent or reduce the frequencyof bleeding episodes in adult and pediatric patients with hemophilia A with factor VIII inhibitors.
Important Safety InformationBoxed WARNING: THROMBOTIC MICROANGIOPATHY and THROMBOEMBOLISMCases of thrombotic microangiopathy and thrombotic events were reported when on average a cumulative amount of >100 U/kg/24 hours of activated prothrombincomplex concentrate (aPCC) was administered for 24 hours or more to patients receiving HEMLIBRA prophylaxis. Monitor for the development of thrombotic microangiopathy and thrombotic events if aPCC is administered. Discontinue aPCC and suspend dosing of HEMLIBRA if symptoms occur.
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Treatingbreakthrough bleeds:A new approach Using Bypassing Agents With HEMLIBRA Prophylaxis
For HCP audiences
HEMLIBRA® is a registered trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The HEMLIBRA logo is a trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan. The Genentech logo is a registered trademark of Genentech, Inc. ©2018 Genentech USA, Inc. All rights reserved. EMI/080317/0065(3) 05/18
A new approach to treating breakthrough bleeds when using concomitant BPAs
• Patients with TMA presented with thrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury, without severe defi ciencies in ADAMTS13 activity
1 additional TMA case occurred after the data cutoff for the primary analysis1
• The patient passed away and the investigator determined the cause of deathwas unrelated to HEMLIBRA
4 events fully resolved following aPCC discontinuation and suspension of HEMLIBRA1,2
• In the limited experience with these events, treatment included supportive care with or without hemodialysis/plasmapheresis
• Evidence of improvementwas seen within 1 week
• Both patients recovered within 3 weeks, with 1 patient electing to resume HEMLIBRA—without recurrence
• No thrombotic event required anticoagulation therapy
• Evidence of improvement wasseen within 1 month
• Both patients fully recovered,with 1 patient electing to resume HEMLIBRA — without recurrence
TMA and thrombotic events reported in HAVEN 1
Thrombotic microangiopathy (TMA) and thrombotic events werereported when on average a cumulative amount of >100 U/kg/24 hours of aPCC was administered for ≥24 hours to patients receivingHEMLIBRA prophylaxis
aPCC=activated prothrombin complex concentrate.† Based on data from HAVEN 1: a randomized, multicenter, open-label clinical trial of patients with hemophilia A with FVIII inhibitors aged 12 years and older (N=109, all males). The primary endpoint was reduction in treated bleeds over 24 weeks with prophylactic HEMLIBRA vs no prophylaxis.
‡ Based on data from HAVEN 2 (interim analysis): a single-arm, multicenter, open-label clinical study of patients with hemophilia A with FVIII inhibitors aged <12 years and 12-17 years weighing <40 kg. HAVEN 2 outcomes are from aninterim analysis. The interim effi cacy analysis examined reduction in bleeds at 30 weeks. The interim intra-patient analysis evaluated ABR in patients switching to HEMLIBRA following previous prophylactic BPAs (n=15) or previous on-demand BPAs (n=3) at a median study duration of 59 weeks. Statistical signifi cance will be conducted at fi nal analysis.1
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=35)
No prophylaxis(n=18)
Median ABR in HAVEN 1 was 0 (IQR: 0; 3.7) with HEMLIBRA prophylaxis vs 18.8 (IQR: 13.0; 35.1) with no prophylaxis
Median ABR in HAVEN 2 was 0 (IQR: 0; 0) with HEMLIBRA prophylaxis 1
Signifi cantly more patients with FVIII inhibitors had 0 bleeds*
with HEMLIBRA vs no prophylaxis
VS
PATIENTS WHO HAD ZERO BLEEDS
HEMLIBRA prophylaxis(n=59)
Sustained protection meant 0 treated bleeds for most patients1
87% FEWER BLEEDS (95% CI: 72.3; 94.3), P<0.0001ABR 2.9 (95% CI: 1.7; 5.0) vs
23.3 (95% CI: 12.3; 43.9)
98% FEWER BLEEDSin the intra-patient analysis
ABR 0.4 (95% CI: 0.2; 0.9) vs19.8 (95% CI: 15.3; 25.7)with previous BPAs (n=18)
ABR 0.3 (95% CI: 0.1; 0.5)
86%
HAVEN 1: Adults and adolescents†
HAVEN 2 interim analysis: Children1‡
2 TMA cases1 2 thrombotic events1,2
Recovery from these events occurred in the continued presence of HEMLIBRA in plasma2,3
HEMLIBRA prophylaxis calls for a new way of using BPAs for treating breakthrough bleeds
In HAVEN 1 and HAVEN 2, no TMA or thrombotic events wereobserved with use of rFVIIa alone in patients taking HEMLIBRA1, 2
• Clinical experience was limited and of relatively short duration (median treatment exposure was 42 weeks for HAVEN 1 and 29 weeks for HAVEN 2), and cannot exclude the possibility of occurrence of events with rFVIIa when taking HEMLIBRA1
140 treatment instances in patients treated with rFVIIa in HAVEN 11
Treatment average<90 µg/kg/24 h90–180 µg/kg/24 h181–270 µg/kg/24 h>270 µg/kg/24 h
% of treatmentinstances
17343119
There is a possibility for hypercoagulability with rFVIIa with HEMLIBRA based on preclinical experiments
Select Important Safety InformationWarnings and PrecautionsThrombotic Microangiopathy (TMA) and Thromboembolism Associated With HEMLIBRA and aPCCIn clinical trials, TMA was reported in 1.6% of patients (3/189) and thrombotic events were reported in 1.1% of patients (2/189). In patients who received at least one dose of aPCC, TMA was reported in 8.3% of patients (3/36) and thrombotic events were reported in 5.6% of patients (2/36). Patients with TMA presented with thrombocytopenia, microangiopathic hemolytic anemia, and acute kidney injury, without severe deficiencies in ADAMTS13.
Please see accompanying HEMLIBRA full Prescribing Information, including BoxedWARNING, and additional Important Safety Information throughout this brochure.
Talk to patients and caregivers about how HEMLIBRA increases coagulation potential
Select Important Safety InformationPregnancy, Lactation, Females and Males of Reproductive PotentialWomen of childbearing potential should use contraception while receiving HEMLIBRA.HEMLIBRA should be used during pregnancy only if the potential benefi t for themother outweighs the risk to the fetus. Consider developmental/health benefi ts, clinicalneed and potential adverse effects on the breastfed child and mother.
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch.You may also report side effects to Genentech at (888) 835-2555.
Monitor for TMA and thromboembolism if using aPCC*
Ensure patients and caregivers know to seek medical treatment if they suspect these events
Immediately discontinue aPCC and suspend HEMLIBRA if theseevents occur, and manage as clinically indicated
Consider the benefi ts and risks of resuming HEMLIBRA prophylaxis following complete resolution of TMA or thrombotic events on a case-by-case basis
Educate patients and caregivers to think differentlyDiscuss which types of bleeds require BPAs while taking HEMLIBRA and the importance of seeking medical advice before treating these bleeds Describe the potential risks of TMA and thromboembolism if aPCC is taken during HEMLIBRA prophylaxis Encourage patients to update emergency medical informationand to inform all healthcare providers
* Monitoring includes D-dimer, prothrombin fragment F1+2 (if available), platelet count, serum creatinine, LDH, and peripheral blood smear analysis for schistocytes. For patients who require multiple BPA doses, laboratory monitoring should be performed every 24 – 48 hours thereafter until 24 – 48 hours following the last BPA dose administered to treat a given bleed.1
1 PREPAREBEFORE
ANY BLEEDS
3MONITORBEYOND
THE BLEED
Assess the bleed and proceed with a plan Follow a protocol for when and how patients and caregiversshould use BPAs during HEMLIBRA prophylaxis Ensure patients consult with you fi rst when aPCC doses>100 U/kg are requiredDiscuss how to approach repeated dosing of any BPA2IN THE EVENT
OF A BLEED
TREAT
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
ABR=annualized bleed rate; FVIII=factor VIII; IQR=interquartile range.* Defi ned as bleeds treated with BPAs (standardized bleed defi nition adapted from the International Society on Thrombosis and Haemostasis [ISTH]).2
Please see accompanying HEMLIBRA full Prescribing Information, including Boxed WARNING, and additional Important Safety Information throughout this brochure.
Select Important Safety InformationMost Common Adverse ReactionsThe most common adverse reactions (incidence ≥ 10%) are injection site reactions, headache, and arthralgia.
rFVIIa=recombinant factor VIIa.
References: 1.Data on fi le. Genentech, Inc. 2.Oldenburg J, Mahlangu JN, Kim B, et al. Emicizumab prophylaxis in hemophilia A with inhibitors.N Engl J Med.2017;377(9):809-818, Supplement, and Protocol.3. Uchida N, Sambe T, Yoneyama K, et al. A first-in-human phase 1 study of ACE910, a novel factor VIII–mimetic bispecifi c antibody, in healthy subjects.Blood. 2016;127(13):1633-1641.4.National Hemophilia Foundation. MASAC update on the approval and availability of the new treatment: emicizumab (Hemlibra), for persons with hemophilia A with inhibitors to factor VIII: interim guidance on acute bleed management and use of laboratory assays. 2017;1-4. 5. Kruse-Jarres R, Callaghan MU, Croteau SE, et al. Surgical experience in two multicenter, open-label phase 3 studies of emicizumab in persons with hemophilia A with inhibitors (HAVEN 1 and HAVEN 2) [abstract]. Presented at: ASH 59th Annual Meeting of the American Society of Hematology; December 9-12, 2017; Atlanta, GA.
As observed over 24 weeks (HAVEN 1) and 30 weeks (HAVEN 2)
%63 6%
FPO
T:21.75”
T:17”
B:21.75”
B:17”
F:5.375”
FS:5.125”
F:5.5”
FS:5”
F:5.5”
FS:5”
F:5.375”