Embed Size (px)
Citation preview

Hashimoto’s thyroiditis associated with idiopathic retroperitonealfibrosis: case report and review of the literature
Summary
Idiopathic retroperitoneal fibrosis (IRF) is arare disease of unknown origin, characterisedby an inflammatory proliferative fibrosingprocess occurring in the retroperitoneum.Hashimoto’s thyroiditis (HT) is a form ofchronic thyroiditis that in some cases showsan extensive replacement of thyroid paren-chyma by fibrous tissue. We report the rareassociation of IRF with HT in a 68-year-oldwoman presenting with pulmonary oedema,acute renal failure due to bilateral hydroneph-rosis and a firm diffuse goitre with hypothy-roidism. The so far reported cases of IRFassociated with chronic thyroiditis arereviewed, and the possible aetiopathogeneticlink between these two entities is discussed.
Introduction
Retroperitoneal fibrosis is a rare disease firstlyreported in the English literature by Ormondin 1948 (1). It is characterised by an inflam-matory proliferative fibrosing process occur-ring in the retroperitoneum (2). Clinically,the retroperitoneal fibrosis usually results inprogressive renal failure due to constrictionand final obliteration of the ureters (1,2).Nonetheless, a wide array of clinical manifes-tations has been observed (3,4). Moreover, itsfrequent association with either fibrosinglesions in other body sites (thyroid, mediasti-num, eyes, gallbladder and parotid) (5–8) ordifferent disorders of autoimmune origin (9–11) has been described. From an aetiologicpoint of view, the retroperitoneal fibrosis isclassified as primary or secondary. Secondaryretroperitoneal fibrosis may be caused bymalignancies (12), infections (13), medica-tions (namely, methysergide and methyldopa)(14,15) or previous surgery; the primary ret-roperitoneal fibrosis, named idiopathic retro-peritoneal fibrosis (IRF), is a diagnosis ofexclusion. Although the aetiology of IRF stillremains unclear, both the evidence of itscombination with multifocal fibrosis andautoimmune disorders and its partial or com-plete response to immunosuppressive therapy(16,17) support the current opinion that itrepresents one manifestation of a systemicimmunologic hypersensitivity disorder.
To our knowledge, only four cases of chro-nic thyroiditis associated with IRF have beenso far reported (9,10,18). Here, we report afurther case of association between IRF andHashimoto’s thyroiditis (HT) in a womanpresenting with pulmonary oedema, acute
renal failure due to hydronephrosis and afirm goitre with hypothyroidism.
Case report
A 68-year-old woman was admitted to thehospital complaining of dyspnoea, palpita-tions and pain in the lumbar region andlower abdomen. She was taking b-blockersand nifedipine because of a long-lasting his-tory of hypertension. She smoked about 20cigarettes ⁄ day and did not drink any alcohol.There was no history of chest pain, fever, cor-onary heart disease, diabetes mellitus, urinaryfrequency or previous surgery. On admission,the temperature was 36 �C, the pulse was92 bpm and the respirations were 28 ⁄ min.The blood pressure was 190 ⁄ 110 mmHg. Theurine was scarce and trace-positive for pro-tein; the sediment contained two red cells perhigh-power field (HPF), four white cells perHPF and a few bacteria per HPF. On chestexamination, diffuse crackles were heard, con-sistent with pulmonary oedema. A holosystolicmurmur of mild intensity (2 ⁄ 6) was presentalong the left sternal border. The abdomenwas painful on palpation, but it was neitherdistended nor tender; no abdominal masseswere found; bowel sounds were regular; theliver and the spleen were not felt. The resultsof neurologic examination were normal. Asmall firm goitre with irregular margins waspalpated, but neither thyroid nodules norneck lymph node enlargement were detected.
The measurement of arterial blood gasesindicated only mild hypoxaemia (PaO2 = 63mmHg). One hundred per cent oxygen wasdelivered by a venti-mask, and furosemidewas given intravenously, thus obtaining aslight improvement of both dyspnoea andurine flow. Laboratory analysis showed a cre-atinine 4.3 mg ⁄ dl and a haemoglobin 10 g ⁄ dlassociated with elevated values of erythrocytesedimentation rate, ferritin and C-reactiveprotein, a picture consistent with chronic dis-order anaemia. Cardiac enzymes were in thenormal range. Thyroid function tests showeda thyrotropin (TSH) 6 lUI ⁄ ml (normal val-ues: 0.3–4.5), free thyroxine (FT4) 10.5 pg ⁄ ml(normal values: 9–19) and free triiodotironine(FT3) 2.3 pg ⁄ ml (normal values: 2.1–4.1).Antithyroglobulin (TG-Ab) and antithyro-peroxidase (TPO-Ab) antibodies were bothelevated at 79 UI ⁄ ml (normal values:<40 UI ⁄ ml) and 215 UI ⁄ ml (normal values:<35 UI ⁄ ml), respectively. An electrocardio-gram showed atrial fibrillation. Radiographsof the chest detected hyperinflated lungs with
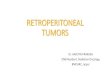
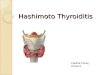
hilar congestion and a mild left pleural effu-sion. A cardiac ultrasonographic examinationdemonstrated Doppler evidence of mild tri-cuspid and mild-to-moderate mitralic regur-gitation; ejection fraction rate was 66%.Ultrasound examination of both the abdomenand the thyroid gland, respectively, disclosedbilateral hydronephrosis and a diffuselyhypoechoic thyroid containing pseudonodularareas and a 17-mm hypoechoic nodule withundefined margins in the right lobe. Com-puted tomography (CT) scan of the abdomenshowed an isodense mass surrounding theaorta just under the kidneys as far as the ori-gin of iliac vessels, and causing bilateral dila-tation and dislocation of both ureters.Administration of iodinated contrast mediumwas avoided because of renal failure. Magneticresonance imaging (MRI) of the abdomen(Figure 1) confirmed the presence of a massextending along the common iliac vessels,encasing the left renal vein, imprinting theaorta just above its bifurcation and ureters,and causing bilateral hydronephrosis. On T2-weighted images, the signal intensity of themass was reduced and homogeneouslyenhanced after gadolinium administration.Due to these features, MRI diagnosis wasconsistent with retroperitoneal fibrosis. Anexploration laparoscopy of the abdomen wasperformed to obtain a biopsy specimen; his-tological examination showed a dense fibrosiscontaining a heavy inflammatory infiltrationcomposed of lymphocytes, eosinophils andpolymorphonucleates (Figure 2). A histologi-cal diagnosis of IRF was finally made.
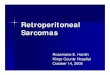
Figure 1 Magnetic resonance imaging (MRI) of theabdomen. Bilateral hydronephrosis, particularlypronounced on the left
doi: 10.1111/j.1742-1241.2006.00842.x
CASE REPORT
ª 2006 The Authors162 Journal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, January 2006, 61, 1, 162–167

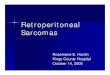
A stent was positioned in both ureters,with subsequent improvement of serum creat-inine concentration (1.6 mg ⁄ dl). A fine nee-dle aspiration biopsy of the 17-mm nodule inthe right thyroid lobe was performed; cytolo-gical examination revealed abundant lympho-cytes of different maturation with normalthyrocytes, Hurthle cells without atypias andfibrosis, a finding consistent with HT. MRI ofthe thyroid (Figure 3) demonstrated a diffuseheterogeneous hyperintensity throughout thegland, particularly on T2-weighted images.
The patient was given prednisone20 mg ⁄ day, tamoxifen 20 mg ⁄ day and l-thy-roxine 50 mcg ⁄ day. At 9-month follow-up,the patient is eupnoic and asymptomatic.Nonetheless, a slight reduction of the abdom-inal mass size was demonstrated by MRIscan.
Discussion
The association of IRF with HT is here repor-ted. In this patient, the suspicion of IRF was
raised by the clinical, laboratory and imagingfindings and was finally confirmed by histol-ogy. Due to exuberant fibrosis invading theretroperitoneum and obliterating the ureters,IRF usually results in progressive renal failure(1–4). Ultrasound is a sensitive tool in thedetection of hydronephrosis, and it success-fully revealed ureteral dilatation in ourpatient. However, it is not as accurate as CTand MRI in the study of retroperitoneum(19). On CT scan, IRF appears as a peritonealsoft tissue that in most patients encases thesurrounding vessels and the ureters (11,19). Astrong limitation of CT is the concomitantpresence of renal insufficiency that contrain-dicates the administration of iodinated con-trast medium. This was the case of ourpatient too. MRI is the gold standard in thediagnosis of IRF (20), owing to both betteranatomical definition of soft tissues anddetection of fibrosis than CT, and useof non-iodinated contrast medium. In ourpatient, the retroperitoneal mass showedhypointensity on T2-weighted images and ahomogeneous enhancement after gadoliniumadministration. Hypointensity in fibrosingdiseases is caused by fibrous tissue extendingthrough the retroperitoneum, and reducingMRI signal intensity in all pulse sequences,because of an extremely short T2 value andlong T1 values (21). In the present case, theretroperitoneal fibrosis was definitively con-firmed by histological examination that dis-played the picture of an active disease withabundant inflammatory infiltration.
With regard to the thyroid disease of ourpatient, the diagnosis of chronic thyroiditiswas made by the following findings: firm goi-tre on palpation; laboratory evidence of bothelevated thyroid antibody titres and hypothy-roidism; diffusely hypoechoic gland on ultra-sound; cytological examination displayingHurthle cells and inflammatory cells (22). Inthis case, the differential diagnosis includedRiedel’s thyroiditis (RT) and the fibrous vari-ant of HT. The simultaneous occurrence ofRT and IRF has been reported (5,23,24) and
is part of the spectrum of ‘multifocal idio-pathic fibrosis’. However, in our patient, RTwas ruled out, and the diagnosis of HT couldbe made, by the following features. Firstly, inRT, the thyroid antibody (i.e. TG-Ab andTPO-Ab) levels may be normal or slightlyelevated, whereas in HT they are usuallystrongly elevated (25), as in our patient. Sec-ondly, in most RT cases, attempts at fine nee-dle aspiration biopsy do not yield adequatematerial for a cytological diagnosis, and whenthey do, the smears contain few thyrocytes,fibrous tissue fragments and scatteredlymphocytes with no evidence of Hurthle cells(22,25–27). Conversely, HT smears are usuallycellular and include Hurthle cells, abundantinflammatory cells and sometimes a ariableamount of fibrosis, as was seen in our patient(25). Finally, MRI picture is pathognomonicof RT if it reveals hypointense signal onT2-weighted images, whereas in all other thy-roid diseases (HT included) a hyperintensityis invariably demonstrated (27), as was thecase of this woman.
Whether HT and IRF are aetiologicallylinked may not be answered. Including thepresent patient, five cases of association ofchronic thyroiditis (four HT and one Graves’disease) with IRF have been so far reported(9,10,18) (Table 1). Two of these patients(9,10) also had an RT, and such evidence ledsome authors to propose that RT may repre-sent a late stage (i.e. the progression to afibrotic stage) of chronic thyroiditis. Thefundamental concept of this theory – alsocalled ‘the intrathyroidal hypothesis’ (27) – isthat the fibrosing process of RT is specificallyrelated to the thyroid and does not take intoaccount the extracervical manifestations ofthe disease. A further theory that is actuallyaccepted by most authors is the so-called‘autoimmune systemic hypothesis’ (27): it ispostulated that RT is a primary disease offibroblasts triggered by autoimmune stimuli;as such, it represents just one manifestationof a systemic fibrosclerotic process that mayalso include IRF.
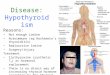
Figure 2 Biopsy specimen of the retroperitoneum.Retroperitoneal fibrosis (haematoxylin–eosin: 20·)
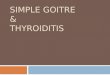
Figure 3 Magnetic resonance imaging (MRI) of thethyroid gland. The thyroid appears ashomogeneously hyperintense on T2-weightedimages
Table 1 So far reported cases of association between idiopathic retroperitoneal fibrosis and chronicthyroiditis
Author
(Reference) Form of thyroiditis Sex
Age
(years) Thyroid function
Thyroid
autoimmunity
Best et al. 1991 (9) Hashimoto’s thyroiditis and F 57 Overt hypothyroidism TG-Ab+Riedel’s thyroiditis TPO-Ab+
Julie et al. 1997 (10) Hashimoto’s thyroiditis and F 38 Overt hypothyroidism TG-Ab+Riedel’s thyroiditis TPO-Ab+
Armigliato et al. 2002 (18) Hashimoto’s thyroiditis F 67 Subclinical hypothyroidism TPO-Ab+Armigliato et al. 2002 (18) Graves’ disease F 61 Overt thyrotoxicosis TG-Ab+
TPO-Ab–Pizzini et al.
(present case), 2005Hashimoto’s thyroiditis F 68 Subclinical hypothyroidism TG-Ab+
TPO-Ab+
F, female; TG-Ab, antibodies against thyroglobulin; TPO-Ab, antibodies against thyroperoxidase.
Hashimoto’s thyroiditis and idiopathic retroperitoneal fibrosis 163
ª 2006 The AuthorsJournal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, January 2006, 61, 1, 162–167

The present case supports the theory of theautoimmune aetiology of IRF, and the needof monitoring IRF patients for the develop-ment of further autoimmune disorders.
A. M. Pizzini,1 S. Corrado,2 E. Radighieri,1
G. Ferretti,1 C. Carani,1 G. Papi11Department of Internal Medicine,
Endocrinology Unit, 2Department ofMorphological and Forensic Sciences, Section
of Pathology, University of Modena andReggio Emilia, Italy
Correspondence to:Dr Papi Giampaolo
Departimento di Medicina Interna,Reparto di Medicina 1, Ospedale ‘Ramazzini’,
Via S. Giacomo 2, 41012 Carpi (MO), ItalyTel.: + 39 059 659 309Fax: + 39 059 659 273
Email: [email protected]
References
1 Ormond JK. Bilateral ureteral obstruction due to
envelopment and compression by an inflammatory
retroperitoneal process. J Urol 1948; 59: 1072–9.
2 Mitchinson MJ. The pathology of retroperitoneal
fibrosis. J Clin Pathol 1970; 23: 681–9.
3 Baker LRI, Mallinson WJM, Gregory MC et al. Idio-
pathic retroperitoneal fibrosis: a retrospective analy-
sis of 60 cases. Br J Urol 1987; 60: 497–503.
4 Vivas I, Nicolas AI, Velazquez P et al. Retroperito-
neal fibrosis: typical and atypical manifestation. Br J
Radiol 2000; 73: 214–22.
5 Natt N, Heufelder AE, Hay ID et al. Extracervical
fibrosclerosis causing obstruction of a ventriculo-
peritoneal shunt in a patient with hydrocephalus
and invasive fibrous thyroiditis (Riedel’s struma)
Clin Endocrinol (Oxf) 1997; 47: 107–11.
6 Bartholomew LG, Cain JC, Woolner LB et al. Scle-
rosing cholangitis. Its possible association with
Riedel’s struma and fibrous retroperitonitis. N Engl
J Med 1963; 269: 8–12.
7 Comings DE, Skubi KB, Eyes JV, Motulsky AG.
Familial multifocal fibrosclerosis: findings suggesting
that retroperitoneal fibrosis, mediastinal fibrosis, scle-
rosing cholangitis, Riedel’s thyroiditis, and pseudotu-
mor of the orbit may be different manifestation of a
single disease. Ann Intern Med 1967; 66: 884–92.
8 Hamano H, Kawa S, Hochi Y et al. Hydronephrosis
associated with retroperitoneal fibrosis and sclero-
sing pancreatitis. Lancet 2002; 359: 1403–4.
9 Best TB, Munro RE, Burwell S et al. Riedel’s thy-
roiditis associated with Hashimoto’s thyroiditis,
hypoparathyroidism, and retroperitoneal fibrosis.
J Endocrinol Invest 1991; 14: 767–72.
10 Julie C, Vieillefond A, Desligneres S et al. Hashimo-
to’s thyroiditis associated with Riedel’s thyroiditis
and retroperitoneal fibrosis. Pathol Res Pract 1997;
193: 573–7.
11 Kamisawa T, Matsukawa M, Ohkawa M. Autoim-
mune pancreatitis associated with retroperitoneal
fibrosis. JOP 2005; 6: 260–3.
12 Thomas MH, Chisholm GD. Retroperitoneal fibrosis
associated with malignant disease. Br J Cancer 1973;
28: 453–8.
13 Mathisen W, Holta AL. Idiopathic retroperitoneal
fibrosis. Surg Gynecol Oncol 1966; 122: 1278–82.
14 Graham JR, Suby HI, LeCompte RR, Sadowsky
NL. Fibrotic disorders associated with methyserg-
ide therapy for headache. N Engl J Med 1966;
274: 359–68.
15 Iversen BM, Nordahl E, Johannesen JW et al. Retro-
peritoneal fibrosis during treatment with methyld-
opa. Lancet 1975; 2: 302–4.
16 Moulik PK, Al-Jafari MS, Khaleeli AA. Steroid
responsiveness in a case of Riedel’s thyroiditis and
retroperitoneal fibrosis. Int J Clin Pract 2004; 58:
312–5.
17 Loffeld RJLF, van Weel TF. Tamoxifen for retroperi-
toneal fibrosis. Lancet 1993; 341: 382.
18 Armigliato M, Paolini R, Bianchini E et al. Hashimo-
to’s thyroiditis and Graves’ disease associated with
retroperitoneal fibrosis. Thyroid 2002; 12: 829–31.
19 Kottra JJ, Dunnick NR. Retroperitoneal fibrosis.
Radiol Clin North Am 1996; 43: 1259–75.
20 Burn PR, Singh S, Barbar S et al. Role of gadolin-
ium-enhanced magnetic resonance imaging in retro-
peritoneal fibrosis. Can Assoc Radiol J 2002; 53:
168–70.
21 Takashima S, Fukuda H, Tomiyama N et al. Hashi-
moto thyroiditis: correlation of MR imaging signal
intensity with histopathologic findings and thyroid
function test results. Radiology 1995; 197: 213–9.
22 De May RM. Riedel’s thyroiditis. In: The Art and
Science of Cytopathology. Aspiration Cytology. Chig-
ago: ASCP Press, 1996: 721–2.
23 Turner-Warwick R, Nabarro JD, Doniach D.
Riedel’s thyroiditis and retroperitoneal fibrosis. Proc
R Soc Med 1966; 59: 596–8.
24 Rao CR, Ferguson GC, Kyle VN. Retroperitoneal
fibrosis associated with Riedel’s struma. Can Med
Assoc J 1973; 108: 1019–21.
25 Papi G, Corrado S, Carapezzi C et al. Riedel’s thy-
roiditis and fibrous variant of Hashimoto’s thyroidi-
tis: a clinicopathological and immunohistochemical
study. J Endocrinol Invest 2003; 26: 444–9.
26 Papi G, Corrado S, Cesinaro AM et al. Riedel thy-
roiditis: clinical, pathological and imaging features.
Int J Clin Pract 2002; 56: 65–7.
27 Papi G, LiVolsi VA. Current concepts on Riedel thy-
roiditis. Am J Clin Pathol 2004; 121: S50–S63.
Paper received September 2005, accepted November 2005
doi: 10.1111/j.1742-1241.2005.00638.x
CASE REPORT
Severe pulmonary haemorrhage accompanying hepatorenal failurein fulminant leptospirosis
Summary
Leptospirosis is a re-emerging spirochetalzoonosis with a worldwide distribution affect-ing both animals and humans. The clinicalsyndromes may vary from a subclinical infec-tion to a severe illness. Although it maypotentially have a fulminant and fatal course,leptospirosis usually remains as an underdiag-nosed cause of multiorgan failure. In thisstudy, we report a patient with leptospirosiswho presented with a fulminant course of dif-fuse alveolar haemorrhage and hepatorenalfailure. His clinical condition deteriorated,despite appropriate antibiotic therapy and
haemodialysis. However, he showed promptclinical improvement when corticosteroidsand plasma exchange were instituted in addi-tion to the original therapy. We conclude thatleptospirosis should be considered in any casepresenting with pulmonary haemorrhage andhepatorenal failure. Plasma exchange and cor-ticosteroids may be a choice of treatment inselected patients unresponsive to conventionaltherapy. Potential benefits of plasma exchangeand corticosteroids may be based on a toxin-and ⁄ or cytokine-mediated pathogenesis of thedisease.
Leptospirosis is a spirochetal zoonosis witha worldwide distribution. The main animal
reservoirs for this disease are both wild anddomestic animals, especially rats. Humans,particularly in regions with humid climates,become infected usually after direct contactwith urine, blood or tissue from an infectedanimal or exposure to a contaminated envi-ronment. Portals of entry include skin abra-sions or cuts, mucous membranes orconjunctiva (1,2). Apart from professionalrisks (veterinarians, rice-field labourers, sewerworkers, farmers, military personnel), recre-ational activities such as canoeing, freshwaterswimming, hunting and gardening may alsobe risky for exposing the organism (2–4).After penetration into the body, the organ-
164 Pulmonary haemorrhage and hepatorenal failure
ª 2006 The AuthorsJournal compilation ª 2006 Blackwell Publishing Ltd Int J Clin Pract, January 2006, 61, 1, 162–167