Embed Size (px)
Citation preview

1
Impression Management in a Health Center: The Case of Frontline Employees Millie Harrison, M.A., Doctoral Student, Moody College of Communication, [email protected] | 256.762.3143 W. Roth Smith, M.A., Doctoral Student, Moody College of Communication Mackenzie R. Greenwell, M.A., Doctoral Student, Moody College of Communication Keri K. Stephens, Ph.D., Associate Professor & Associate Director, UT Center for Health Communication, Moody College of Communication Terri Sabella, RN BSN, JD, Doctoral Student, University of Texas Health Science Center Houston, School of Public Health - Management, Policy, and Community Health, and Chief Operating Officer & Chief Nursing Officer CommUnityCare Brief Abstract: Using Goffman’s (1959) dramaturgical perspective, the present study focuses on the impression management of frontline employees (FLEs) at a Federally Qualified Health Center (FQHC). Qualitative analysis reveals how FLEs in medical clinics engage in frontstage and backstage communication to perform their jobs and facilitate patient care. Data highlight three broad themes in which FLEs’ communication compounds frontstage and backstage practices: performing on multidimensional stages, enacting complementary and competing roles, and incorporating regulatory strategies to accomplish their work. A model of FLE performance is advanced, and implications for clinical FLEs, patient care, and patient privacy are discussed. Keywords: frontline employees (FLEs); impression management; frontstage and backstage communication; Goffman; grounded theory *The work will be presented at the International Communication Association in San Diego, CA, in May 2017.
Background and Rationale Frontline service is an integral part of the customer experience (Brown & Lam, 2008;
Hartline, Maxham, & McKee, 2000). This is particularly striking in healthcare environments where frontline administration—such as office clerks, account specialists, and clinic directors—are often the first and last points of patient contact. As Payne and Webber (2006) and Dagger and colleagues (2013) argue, the interaction between FLEs and patients form a critical foundation for the kind of service expected for the rest of a patient’s visit. In addition to helping and satisfying patients, FLEs must also coordinate relationships inside the organization, such as managing the needs of physicians and nurses (Plouffe, Bolander, Cote, & Hochstein, 2016). FLEs play an important “boundary-spanning role” (Bitner et al., 1994) and can be categorized as caught between patients who need their attention and healthcare management and providers who demand productivity and efficiency (Bateson, 1985).
To better understand how healthcare professionals meet service demands and enact their roles in organizations like medical clinics, several communication scholars have turned to Goffman’s (1959) theory of impression management and dramaturgical perspective to explain

FRONTLINE EMPLOYEES AND FRONT AND BACKSTAGE
2
how professionals “present” themselves and “perform” their roles (see Ellingson, 2003, 2005; Lewin & Reeves, 2011). Specifically, Goffman’s concepts of frontstage (formal, more public communication space) and backstage (informal, more private communication space) allow scholars to explore the formal and informal routes through which employees engage in patient care. However, extant literature primarily has investigated the performativity of physicians and nurses, without considering the performative influence of healthcare administration in the patient experience. Thus, our study focuses on the staged performance of FLEs to grasp a more complete understanding of their “boundary-spanning” roles in a healthcare context. Employing qualitative methods, the purpose of this paper is to elucidate how FLEs in medical clinics engage in frontstage and backstage communication to perform their jobs and facilitate patient care. Our research question is as follows:
RQ: How do FLEs create and communicate within frontstage and backstage spaces?
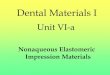
Method The organization selected for this study was CommUnityCare, a Federally Qualified Health Center (FQHC) that provides approximately 90% of care for the uninsured and underinsured in a major metropolitan area in the southern U.S. This particular study focused on FLEs called medical admitting clerks (MACs), who are responsible for checking patients in and out, verifying identification and insurance, collecting fees, scheduling appointments, and communicating information to providers. Their workspaces are located between the patient waiting areas and the treatment rooms (see Figure 1 for clinic layout) and are highly visible to patients at all times.
The data used for this study were gathered during new employee training and in the clinical setting. Data included observations, formal and informal interviews, and document analysis. Four researchers attended new employee training and generated 45 pages of field notes from their observations over two 8-hour periods. The organization also provided our team with complete copies of 497 pages of training materials, including information on patient satisfaction, values and mission of the organization, safety training, and computer-based software training. Our team also conducted participant observations in three health center sites (Site A, Site B, and Site C), spending more than 50 hours in the field. To obtain the most accurate portrayal of MAC workflow, researchers varied observation times, days, and shifts. These observations generated 81 pages of single-spaced field notes and 94 photos. Interview Recruitment and Participants
Researchers also conducted structured, semi-structured, and informal interviews, stemming from questions asked during observations. Interview participants were MACs and MAC supervisors who agreed to participate voluntarily while we conducted observations. When they agreed to be interviewed, we provided participants with an informed consent document. Follow-up questions were asked during observations to clarify participant behaviors and gain further insight into MAC roles, duties, and interactions. In total, we conducted 16 formal interviews with MACS, one with a MAC supervisor, and two with practice leaders. The formal interviews ranged from 10 to 50 minutes and were transcribed verbatim resulting in 159 pages of single-spaced text. Informal interviews generated an additional 24 pages of single-spaced text. Data Analysis
We used a constructivist approach to grounded theory (Charmaz, 2006; Glaser & Strauss, 1967), where data collection and analysis occurred iteratively and codes were constantly compared. The researchers met weekly during data collection to discuss emerging themes. After

FRONTLINE EMPLOYEES AND FRONT AND BACKSTAGE
3
immersing ourselves into the data, we began to “separate, sort, and synthesize…data through qualitative coding” (Charmaz, 2006, p. 3). In this open coding stage, codes were largely descriptive of what was happening in the scene. Next, we used focused codes to hone in on particular areas. In each stage, categories were organized based on theoretical and practical similarity to the other categories. This iterative process resulted in a total of three major themes and seven subthemes reflected in the data.
Findings Data analysis revealed the health center frontstage and backstage is more complex
communicatively than previous literature has described. Our data highlight three broad themes in which MACs working at an FQHC communicate compounding frontstage and backstage practices. Specifically, FLEs perform on multidimensional stages, enact complementary and competing roles, and incorporate regulatory strategies to accomplish their work. Multidimensional Stages
Although research often focuses on the duality of frontstage and backstage, our analysis reveals that the FLE environment is much more complex. Our research supports Ellingson’s (2003, 2005) findings highlighting the fluidity of front and back regions; however, our analysis shows not only do FLEs move in between front and backstages, but they transition between and manage impressions on multiple stages, often simultaneously. Our data show MACs juggle performances on the physical stage (material features and architectural layout), relational stage (managing relationships among patients, medical staff, and administrative superiors), and technologically-mediated stage (performances through information communication technologies, like the telephone, text, or email). Complementary and Competing Roles
In addition to performing on multiple stages, FLEs also enact different roles in these multifaceted performance spaces. Specifically, our data reveal MACs perform for and with others. Depending on the context, MACs can engage in a frontstage presentation by performing for a certain audience, or MACs can work collaboratively with others by performing with them to ensure the patient-care production runs smoothly. We describe the “performing for” role as the actor, which is supported by previous literature (Goffman, 1959; Brissett & Edgley, 2009). We introduce a nuanced role of stage manager to demonstrate how MACs perform with their peers, other professional groups, and patients to mediate the fluidity of frontstage and backstage. Regulatory Strategies
Just as actors might swallow a spoonful of honey before going on stage to enhance their lines, MACs use different communication strategies to help them play their different parts on various clinic stages. We define regulatory strategies as the tactics MACs use to maintain their façade and enhance their performativity. Two primary strategies emerged from our data: involvement shields and performance aids. Involvement shields are barriers that helped the MACs exclude certain audiences in an exceedingly public area. In other words, they help MACs create a backstage within a frontstage space (e.g., covering their mouths or turning their backs when speaking on the phone to protect patient privacy). While involvement shields block particular audiences from the action, performance aids are items that help enhance stage acting. These performance aids include both personal and organizational tools, such as MACs placing motivational quotes by the desk to remember to be positive or making memos in the “Patient Notes” section of the organization’s database to help recall patient preferences (e.g., language). FLE Performance Model

FRONTLINE EMPLOYEES AND FRONT AND BACKSTAGE
4
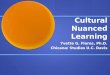
In all, our data capture the complexity of FLEs’ frontstage and backstage processes. As our results highlight, MACs working at this FQHC communicatively construct and enact intricate and compounding frontstage/backstage practices. Specifically, FLEs perform on multidimensional stages, enact complementary and competing roles, and incorporate regulatory strategies to accomplish their work. Although we presented stages, roles, and strategies in a linear order, they should not be considered as separate and mutually exclusive phenomena. Instead, we argue these concepts are best understood as overlapping, at times competing, and always constitutive of the FLE experience. Figure 2 presents the interplay of these various components.
Discussion Our findings extend previous research on Goffman’s (1959) dramaturgical approach to
show frontstage and backstage performances are more complex communicatively than previous studies have described. Perhaps the most salient conclusion from this research is that, contrary to extant literature, there are multiple stages of performance requiring many role switches and strategies for managing these roles. A significant consequence of this multifaceted performativity is that the MACs may be left without a backstage to disengage from work. Three primary implications of this finding are: The absence of a backstage presents significant concerns regarding (1) FLEs’ inability to “turn off,” (2) the quality of patient care provided, and (3) patient privacy violations. Concerns for Inability to “Turn Off”
Our findings show MACs are situated among the watchful eyes of patients, managers, and the health center staff with no backstage space to metaphorically “remove their masks” and recharge emotionally or physically. Utilizing backstage spaces aids in maintaining frontstage performances not only by providing a designated area in which to “perfect” performances, but also by allowing an appropriate space to relax (Joseph, 1990; Lewin & Reeves, 2011). Therefore, with the lack of a physical backstage, it is reasonable to believe that this multi-stage, multi-role environment could accelerate FLE burnout—a concern identified by FQHC management. Concerns for Quality of Patient Care
Another critical function of the backstage identified by the literature is to enhance frontstage performance (Ellingson, 2003, 2007; Wittenberg-Lyles et al., 2009) or to collaborate with others (Lewin & Reeves, 2011). Thus, a lack of backstage could also have detrimental effects on MACs’ ability to provide quality customer service for patients. Ellingson (2003) claims seven communication techniques that occur in backstage areas can help improve overall patient care, such as formal reporting and addressing patient progress. Without a backstage, it may be difficult for MACs to engage in these communication techniques, thus reducing their ability to provide high quality care. Concerns for Patient Privacy
A deficiency in backstage space can also impede MACs from maintaining patient privacy. Research has found that backstage spaces allow individuals to collaborate with one another and work around the limitations of the frontstage (Lewin & Reeves, 2011). For MACs, these collaborations often involve confidential or sensitive patient information, which could be overheard by uninvolved parties if addressed in the minimally private MAC workspace. Although not explicitly supported by our data, the absence of a backstage may have the potential to violate the privacy and security standards set by The Health Insurance Portability and Accountability Act (HIPAA) for health information.
Conclusion

FRONTLINE EMPLOYEES AND FRONT AND BACKSTAGE
5
This study offers an empirical example of how FLE performativity is carried out in an FQHC. Three broad themes related to FLE performativity emerged from our data: FLEs perform on multidimensional stages, enact complementary and competing roles, and incorporate regulatory strategies to accomplish their work. It is our goal that the summative model of the FLE performance experience presented in this study can propel future scholarship at the intersection of frontline service work and healthcare. Additional directions for future research and limitations of the study are also addressed.
References
Bateson, J. E. (1985). Perceived control and the service encounter. In J. Czepiel, M. Solomon, &
C. Suprenant (Eds.) The service encounter: Managing employee/customer interaction in service businesses (pp.67-82) Lexington, MA: Lexington Books.
Bitner, M. J., Booms, B. H., & Mohr, L. H. (1994). Critical service encounters: The employees viewpoint. Journal of Marketing, 58, 95-106. Retrieved from http://www.jstor.org/stable/1251919
Brissett, D., & Edgley, C. (2009). Life as theater: A dramaturgical sourcebook. New Brunswick, NJ: Transaction Publishers.
Brown, S. P., & Lam, S. K. (2008). A meta-analysis of relationships linking employee satisfaction to customer service responses. Journal of Retailing, 84(3), 243-255. doi:10.1016/j.jretai.2008.06.001
Charmaz, K. (2006). Constructing grounded theory: A practical guide through qualitative research. London, UK: Sage.
Dagger, T. S., Danaher, P. J., Sweeney, J. C., & McColl-Kennedy, J. R. (2013). Selective halo effects arising from improving the interpersonal skills of frontline employees. Journal of Service Research, 16(4), 488-502. doi:10.1177/1094670513481406
Ellingson, L. L. (2003). Interdisciplinary health care teamwork in the clinical backstage. Journal of Applied Communication Research, 31(2), 93-117. doi:10.1080/0090988032000064579
Ellingson, L. L. (2005). Communicating in the clinic: Negotiating frontstage and backstage teamwork. Cresskill, NJ: Hampton Press, Inc.
Ellingson, L. L. (2007). The performance of dialysis care: Routinization and adaptation on the floor. Health Communication, 22(2), 103-114. doi:10.1080/10410230701453926
Glaser, B. S., & Strauss, A. (1967). The discovery of grounded theory: Strategies for qualitative research. London, UK: Weidenfeld and Nicolson.
Goffman, E. (1959). The presentation of self in everyday life. Garden City, NY: Doubleday Anchor Books.
Hartline, M. D., Maxham, J. G., & McKee, D. O. (2000). Corridors of influence in the dissemination of customer-oriented strategy to customer contact service employees. Journal of Marketing, 64(2), 35-50. doi:10.1509/jmkg.64.2.35.18001
Joseph, M. (1990). Sociology for everyone (2nd ed.). Cambridge, UK: Polity Press. Lewin, S., & Reeves, S. (2011). Enacting ‘team’ and ‘teamwork’: Using Goffman’s theory of
impression management to illuminate interprofessional practice on hospital wards. Social Science & Medicine, 72(10), 1595-1602. doi:10.1016/j.socscimed.2011.03.037
Payne, S. C., & Webber, S. S. (2006). Effects of service provider attitudes and employment status on citizenship behaviors and customers' attitudes and loyalty behavior. Journal of Applied Psychology, 91(2), 365. doi:10.1037/0021-9010.91.2.365

FRONTLINE EMPLOYEES AND FRONT AND BACKSTAGE
6
Plouffe, C. R., Bolander, W., Cote, J. A., & Hochstein, B. (2016). Does the customer matter most? Exploring strategic frontline employees’ influence of customers, the internal business team, and external business partners. Journal of Marketing, 80(1), 106-123. doi:10.1509jm.14.0192
Wittenberg-Lyles, E. M., Gee, G. C., Oliver, D. P., Demiris, G. (2009). What patients and families don’t hear: Backstage communication in hospice interdisciplinary teams. Journal of Housing for the Elderly, 23(1-2), 92-105. doi:10.1080/027638908026650
Figure 1 Clinic A Layout

FRONTLINE EMPLOYEES AND FRONT AND BACKSTAGE
7
This figure displays the layout for Clinic A. The = symbol represents doorways, and the boxes between the MAC workspace and patient waiting rooms represent windows.
Adult Waiting Room
MAC Workspace
Pediatric Waiting Room 1
Pediatric Waiting Room 2
Patient Rooms and Medical Staff Space
=
=
=
=
=
=
Figure 2 FLE Performance Model

FRONTLINE EMPLOYEES AND FRONT AND BACKSTAGE
8
This figure illustrates the FLE performance model. Specifically, FLEs perform on multidimensional stages, enact complementary and competing roles, and incorporate regulatory strategies to accomplish their work. These concepts are best understood as overlapping, at times competing, and always constitutive of the FLE experience. This figure presents the interplay of these various components.
Multidimensional Stages
Complementary and Competing
Roles
Regulatory Strategies
Multidimensional Stages
Complementary and Competing Roles
Regulatory Strategies
• Physical• Relational• Technologically-Mediated
• Actor• Stage Manager
• Involvement Shields• Performance Aids