Embed Size (px)
Citation preview

Harnessing Louisiana Electronic Medical Records for Pediatric Obesity Research
Amanda E. Staiano, Ph.D., M.P.P.
Pennington Biomedical Research CenterOctober 28, 2015
Childhood Obesity and Public Health Conference 2015

Presentation Outline
• The Era of Digital Data
• What can we do with these data?
Improve screening and treatment
Identify high risk patients/groups
Engage patients in healthcare
• What are the strengths and limitations?

What is an EMR?

HOW CAN WE USE THESE DATA?
1. Improve screening and treatment
2. Identify high risk patients/groups
3. Engage patients in healthcare

1. IMPROVE SCREENING AND
TREATMENT OPTIONS
Obesity Toolkit
Access Health
Louisiana

Louisiana Pediatric ObesityP
edia
tric
Obesity P
revale
nce
Year
0
5
10
15
20
25
30
35
2005 2006 2007 2008 2009 2010 2011 2012 2013
U.S.
LA Health
SBHCs
HPFA
Bogalusa
RWJF “F as in Fat” 2012

http://www.pbrc.edu/obesitytoolkit/

Barlow et al. Pediatrics 2007;120:s164-92

Use of EMR Improves Clinical Care
• 19% of physicians aware of recommendations, only 3% adhere to all of them (Kologatla & Adams, 2004)
• Barriers include (Rattay et al., 2009):– low self-efficacy,
– inadequate tools/resources,
– lack knowledge/skills,
– lack of time,
– competing priorities,
– insufficient reimbursement, and
– lack of awareness of community resources.
Kolagotla & Adams, Obes Res 2004;12(2):275-83
Rattay et al., Pediatrics 2009;123:S100-7

• In 740k pediatric visits, EMR decision tools (Coleman et al., 2012):
– BMI measurement: 66% to 94%
– Obesity diagnosis: 12% to 61%
– Counseling rates: 1% to 50%
• RCT: Decision alerts, counseling
template, and diagnosis order set:
– Obesity diagnosis: 7% to 22%
– Weight-specific counseling: 15% to 27% (Tang et al., 2012)
• Physician & staff training needed (Coleman et al., 2012)
Keehbauch et al., Clin Pediatr 2012;51(1):31-8
Tang et al., JGIM 2012;27(8):933-9
Coleman et al., J of Peds 2012;160(6):918-22
Use of EMR Improves Clinical Care

Prevent, Identify, Treat Childhood Obesity
• Require BMI assessment; prompt if elevated
• Link to screenings; follow-up visits
• Online database of community resources
• Online counseling
• Monitor patients more frequently

Washington FQHC , Bogalusa
Albert Cammon Middle School/St. Rose Elementary SBHC, St. Rose
St. Charles FQHCs, Luling (2), Norco, Kenner
Bonnabel High School SBHC, KennerJohn Ehret High School SBHC, MarreroJoshua Butler Elementary School SBHC, WestwegoRiverdale High School SBHC, JeffersonWest Jefferson High School SBHC, Harvey
Belle Chasse FQHC, Belle Chasse
Ruth Fertel/Tulane FQHC, New Orleans
St. Bernard FQHC, Chalmette
St. Tammany FQHCs, Slidell, Covington
Warren Easton SBHC, New Orleans
Partnership with Access Health Louisiana

2. IDENTIFY HIGH RISK
PATIENTS/GROUPS
LSU Hospitals and Clinics

0
5
10
15
20
25
0
1
2
3
4
5
6
7
8
1958 61 64 67 70 73 76 79 82 85 88 91 94 97 00 03 06 09
Nu
mb
er
wit
h D
iab
ete
s (
Millio
ns)
Perc
en
tag
e w
ith
Dia
bete
s
Year
Percentage with Diabetes
Number with Diabetes
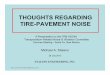
Number and Percentage of U.S. Population with Diagnosed Diabetes,
1958–2010
CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at
http://www.cdc.gov/diabetes/statistics
Slides from Dr. Jackie Stephens



% of adults
with diabetes

*Am. Diabetes Assn 2014, National Center for Chronic Disease Prevention 2010, Caregiving 2013.
Louisiana’s Chronic Disease Burden
These 3 diseases alone cost
the state $10.6 billion/year.

Adult-Onset Diabetes?
0.24 per 1000
or 1 child in every 4000
African Americans have 6x
higher prevalence than Whites

LSU Hospitals & Clinics
• LSU Data Management Evaluation Database (DMED)
• Since 1990, 1.6 million unique patients
– (35% of Louisiana population)
• Under- and uninsured population
– 46% free care,
– 10% self-pay,
– 20% Medicaid,
– 14% Medicare,
– 10% commercial insurance

LSU DMED
Encounter Data
Demographics
Blood Pressure and
Anthropometry
Labs and Pathology
Diagnoses Procedures
Medications, Allergies,
Immunizations
Tobacco Use and Smoking
Cessation
n =
1.6 mil

Characteristics of pediatric sample
Average Diagnosis Age
15.2 y for type 1 diabetes
16.3 y for type 2 diabetes
Unpublished data; In preparation

3. ENGAGE PATIENTS
IN THEIR OWN HEALTHCARE
PROPEL
&
REACHNet

Identify patients that qualify
Reports of patient health data during study enrollment
PI: Peter Katzmarzyk, Ph.D.
Test a 2-y obesity treatment program delivered
in primary care setting to an underserved population

Research Action for Health Network
REACHnet:Research Action for Health Network
(Formerly known as the Louisiana Clinical Data Research Network)
PI: Thomas Carton, Ph.D.
Slides provided by
Beth Nauman, MPH, PhD – Research Director
Louisiana Public Health Institute

Research Action for Health Network
PCORnet

Research Action for Health Network
An informatics and stakeholder engagement infrastructure for multi-site research in Louisiana and Texas
Goal: To facilitate the efficient conduct of patient-centered comparative effectiveness research by establishing a data network containing clinical records for more than 1 million patients
PARTNERS
REACHnet

Research Action for Health Network
Common Data Model

WHAT ARE THE STRENGTHS AND
LIMITATIONS OF DIGITAL DATA?

Strengths
• Large cohorts of chronic diseases and risk factors
• Cost effective
• Focus on ethnic minority groups and those at/near the poverty line
• Assessments actually conducted in clinical settings
• Can improve clinical diagnosis & treatment

Limitations
• Self-selected appointments
• Physician-selected assessments
• Retrospective data
• Limited validity and reliability

Concluding Thoughts
"Evidence is the cornerstone of
a high-performing healthcare
system." - Institute of Medicine

Concluding Thoughts
Glaeser et al., NBER 2014; Working Paper No. 20291
"Evidence is the cornerstone of
a high-performing healthcare
system." - Institute of Medicine

Acknowledgements
Our Lady of the Lake
Children’s Hospital