Embed Size (px)
Citation preview

THE -DUODENO - JEJUNAL FLEXURE: ITS VARIA-TIONS AND THEIR SIGNIFICANCE; By N. BIsHOPHARMAN, B.A., M.:B., M.R.C.S., St John's College, Cann-britlye; Demnonstrator of Anatomy, Camnbridge University.
I IhAVE been led to make some investigations into the anatomyof this region, owing to the finding of the unusual form of the-fexure described below and delineated in figure 1.
(1) Present Descriptions.
The descriptions of the flexure and the commencement of thejejunumn vary considerably in the special monographs on theintestinal canal, and in articles on the part in the text-books.All give fairly full descriptions of the suspensory ligament, ormuscle of Treitz, to which the flexure is due.
Treves (1), in his Hunterian lecture of 1885, gives severalfigures of the flexure, but does not refer to any usual course takenby the commencing jejunum; the figures mostly show a leftwardtendency; whilst one, that of a spider-monkey (fig. 1, B), seems,to indicate a rightward position of the part.
Jonnesco (2) makes no special reference to the direction of the-part, but figures it in that position which appears to be the mostcommon, viz., curving to the left of the median line. In hissection of Poirier's Anatomy, he states that " the jejunum-commences at the level of the duodeno-jejunal tlexure, passing for-wards and downwards to the left; thence it makes a curve fromleft to right."
In other text-books I find the following variations in descrip-tion. Macalister (3) states that " at the flexure the gut makesa sharp bend forwards and leftwards."
Sappey (4): that " the gut passes forwards and to the left, mak-ing, with its continuation downwards and to the right, a semi-,circular curve." This agrees substantially with Jonnesco, and,.also with Gegenbatir (5).

666 N. BISHOPIIARIMAN.
Cunningham (6): that " the jejunum bends suddenly forwards.;aInd downwards upon the duodenum, forming the flexure."
Holden (7): that " the jejunum begins by an abrupt dowin-itir(l bend."Qutain, Mlorris, Gray, Clelandall(l RauIber make no special
mention of the part.These extracts show that the usual description minay 1e ranged
under three forms:1. That which bends forwards and to the left in a fairly-
wide curve, thence passing downwards and to theright.
2. That which bends forwards, downwards, and to the left in,a sharp curve.
3. rllhat which bends directly forwards and downwards alongthe line of the fourth part of the duodenum.
In the series of subjects which I have examined, I have foundall these forms represented, and in addition two other formsin which a slight and a well-inarked bend to the right side ofthe body was exhibited. The position found was in each caseat fixed one, and not subject to the imorements of the intestines..
(2) Desciiptionh (f A$2Iccial Cases.
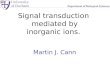
Figure 1 represents the condition of the flexure found iii a-dissecting-room subject (mnale, aged 72 years).
It shows a rightward bend of the commencing jejunuum ofl pronounced character. The exainiiiation was made immedi--attely at the time of the opening of the great sac, before anydissection had been attempted. The abdominal viscera had an.especially healthy appearance, and there was a complete absenceof inflammatory adhesions, so that this common source, of dis--placed( relations could not apply here.From the pylorus to the free part of the jejunum, the gut
flulowe(l a very tortuous course, altering its direction no lessthlan eleven times.
I1'rom the pylorus to the usual site of the flexure there'werelour prominent knuckles formed by these bends. The rut passedfirst laterally beneath the edge of the liver, thence dorsally andinesiallv to become retro-peritoneal; the lesser curvature of the
666i

THE DUODENO-JEJUNAI FLEXURE.
FIG. 1.-Subject, male, aged 72 years. A, retro-peritoneal com-mencement of jejunum, passing column transversely from left toright, at level of 2nd lumbar vertebra. Dd., duodenum. Jj.,jejunum, with free mesentery. S.M.irs., superior mesenteric vessels.Pp., parietal peritoneum. Tr.Mc., site of transverse meso-colon.H.F., site of hepatic flexure. D.C., site of ascending colon. Lv.,liver. x, site of orfice of bile papilla. St., stomach. Cit., annularconstriction of stomach. Py., pylorus. C. A., costal margin. R.X.,site of i0thi costal cartilage. a, fossa duodeno-jejunalis. /3, fossapara-duodenalis. y, dotted line indicates site of freedom of gut fromdorsal parietal peritoneum. 8, site of the colic loop.
6367

6MR N. BISHOP HARMAN.
stomach could be found to be contilnious with the inesial edgeof the gut, as found 'for other cases by Mr Youllg of Liverpool(8). Further, the gut passed obliquely and downwards acrossthe ventral surface of the kidney, reaching to within half aninch of its lateral border; it was here dorsal to a short length ofascending meso-colon, which held a considerable loop of theascending colon lying in the belly cavity, with its convexitydirected towards the middle line. Thence the gut retraced itscourse, making a sharp upward turn to reach the level of thepylorus, as high as the first lumbar vertebra. From this pointit followed the usual course of the duodenum, presentingdescending, transverse, and 'fourth' divisions, and reachingupwards on the left side of the column to the second lumbarvertebra; at this point it was inferior to the line of attachmentof the meso-colon. Instead of becoming free jejunum at thisplace the gut passed across the column transversely, lying onthe second lumbar vertebra, reaching the left side of thatvertebra, and was for this distance (about 2 inches) beneaththe dorsal parietal peritoneum, and immediately ventral to andin contact with the pancreas and superior mesenteric vessels.
The jejunuim then became gradually movable as its meselnteryformed and lengthened, the direction of the first part of theparietal inesenteric attachment being obliquely from right to left..The whole length of the retro-peritoneal gut, from pylorus on-wards, measured about 13 inches.On the upper and left side of the flexure was a well-marked
peritoneal pouch, having a mouth I inch in breadth, and adepth of i inch; its month was directed toward the right side; itdid not penetrate beneath the retro-peritoneal part of the-jejunum. It doubtless represented a ' fossa duodeno-jejunalis';it was noticeable that the direction of its mouth was alteredin a manner consistent with the displacement of the jejunal gut.A shallow ' para-duodenal pouch' existed alongside the arteria
colica sinistra. The subject also presented a well-marked hour-glass constriction of the stomach, which was formed by a completeannular thickening of muscle of considerable substance, dividingthe stomach at the junction of the middle and right thirds of itsaxis into a left chamber of about four-fifths and a right of aboutone-fifth of its total capacity.
668S

THE DUODENO-JEJUNAL FLEXURE.
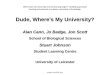
The case delineated in figure 2 was also from a dissectingr-room,subject (male, aged 46 years), and was found at an interval of-three months after the former case. The gut in this casediffered only from the preceding in the absence of complicationin the duodenal part. It passed through its usual bends, andthe shortness of its third part caused it to assume rather a 'Vshape. It agreed with the foregoing case in-
(A) The continuance of the gut beneath th6 dorsal parietal.peritoneum, across the column at the second lumbar vertebra,
d./
FIG. 2.-Subject, male, aged 46 years A, retro-peritoneal jejuniumDd., duodenum. Jj., jejunum with mesentery. Ms., mesentery.S.M.os., superior mesenteric vessels. Ao., aorta. Pp., parietal peri-toneum. Tr.Mc., transverse meso-colon. Pa., pancreas. a, fossaduodenalis superioris. A, a twig from art. colica sinistra which is-within the edge of the above fold. Below the superior fossa is asmall inferior fossa. y, dotted line indicating the extent of thesuperior fossa. 8, dotted line indicating site of freedom of gut fromdorsal parietal peritoneum.
for about 1 1 inches, becoming then free of the wall, save for itscontrolling mesentery, which in its attachment followed a likeoblique leftward and downward direction in its early part.
(B) The complication of the ascending colon by a considerableloop of gut, which was in this case situated at its highest part,close to the hepatic flexure, making the latter to appear as if

7NTR N. BISHOP HARMAN.
double. The convexity of the loop was directed downwards, for-wards, and mesially.
(C) The complete absence of any pathological peritonealadhesions.Two fosse were present in the neighbourhood of the flexure,
which are indicated in the figure. The upper fossa, 'superiorduodenal,' was remarkably large.
Since the finding of the first described case, I have examinednineteen others, noting the condition of the flexure and thecondition of the ascending colon, whether straight or compli-cated by loops. In each case the examination has been madeimmediately on opening the belly.
I found variations which account for the differences in thedescriptions of the several writers quoted above, besides a furthercase in which a rightward tendency was shown, though not tosuch a degree as in the two detailed cases.
(3) lTable of Varieties.
Condition of Ascd.Form. No. of *ass. Direction of Bend. Colon.
1. Four. Directly to left flank in a bold Straight.curve, then downwards. Bendto left = 1 to 2 inches in a descentof 1 inch.
Eight. Forwards, downwards, and to Straight.the left, then downwards. Bendto left - to i inch in descent of1 inch.
3. Six. Forwards, then straight down Straight.on duodenum.
4. One. Forwards. then downwards on Straight.anterior surface of column, tend-ing to right side i inch in descentof 2 inches.
5. Two. Cases detailed: - Forwards, Complicated by loops.transversely to right side, andretro-peritoneal.
From the foregoing table, it will be seen that the leftwardposition (Nos. 1 and 2) occurred in twelve cases, and that it isconsiderably more common than any other form; the directionforward and straight down (No. 3) following with six cases.The rightward position was found in three; though in these, the
670

THE DUODENO-JEJUNAL FLEXURE.
two described at length must be separated from the one in thefourth class, where the tendency rightward was but slight, and thejejunum possessed a mesentery from the flexure; it was, however,fixed in its rightward position by the meso-colon, which crossedi;t.
(4) [le Significance of the Variations.
The two detailed cases are, I think, of interest beyond theirimportance as variations; for the production of the conditionshere found, viz., loss of a normally present mesentery and the-deflected position, may be found to bear on the question as tothe means whereby the duodenum normally loses its originalmesentery, and becomes retro-peritoneal in man.The processes of peritoneal distribution have been accounted
for by the enunciation of two theories:-(1) 0. Hertwig's theory of adhesion of continuously approxi-
mated peritoneal surfaces (9).(2) Treves' theory of peritoneal traction (10).The former theory postulates a deflection of the duodenum by
the over-passing cmecum; the deflected duodenum being appliedto the body wall loses its mesentery first by the adhesion, and:.secondly by the absorption of the contiguous peritoneal surfaces.Such a theory would account for the loss of the jejunal mesentery
-in the above cases, if we can first explain the rightward displace-ment of the gut. There is, however, no over-passing colon, suchas diverts the duodenum; there is no pressure from the left, but-apparently rather the reverse, as the great gut was more ex-tensive on the right side than is normal, so that it actuallypressed upon the small gut from that side by the extra colic loopsdescribed above.On the other hand, Treves, whilst recognizing the possibility
-of the adhesion, and subsequent absorption of approximated--surfaces of peritoneum in some parts, believes that this is notthe process whereby the duodenum loses its mesentery, but ratherthat it is due to an insufficient supply of peritoneal covering_afforded to the rapidly growing ceecum and great gut; so that the-e-ecum in its descent from the region of the pylorus tends to-draw away any redundant peritoneum such as will exist on the-deflection of the duodenum.
671

A62R N. BISHOP HARMAN.
In these two cases there was an excessively long ascendingcolon, which seems to indicate that the growth rightward anddownward of the great gut was greater than usual. This would,in the terms of Treves' theory, cause the requisition of furtherperitoneum from the dorsal parietes. Now, the extremity of theduodenum is fixed by its suspensory band, so that it cannot be-further displaced, but ample supplies could be afforded to thegreat gut if its lateral and downward traction force were-sufficient to retract the redundant peritoneum of the jejunalmesentery immediately succeeding the duodenum. That the-colon could effect such a further traction seems a reasonableconclusion, more especially as this traction would at the sametime produce the rightward deflection of the 'bared' jejunum,which would otherwise remain unexplained.
In the absence of any- evidence as to the existence of some-directing influence, such as Hertwig's theory would require, to'cause the rightward displacement of the jejunum, and on theexistence, on the contrary, of the general tendency which thepresence of the large liver must have in keeping the upper part.of the gut to the left side, these two cases, with their rightwarddirection, retro-peritoneal position, and coincident elongated andlooped ascending colon, must, I think, be allowed to lend con-siderable support to the theory of peritoneal traction, as pro-pounded by Treves.
The supposition that the colic loops indicate an excessive-growth is, I think, warranted by the coincident excess in sizeof the duodenum in the first case, also by reason of the chamberedstomach,1-if we may accept Wiedersheim's suggestion (13) thata bilocular stomach is a progressive feature,-but chiefly by reasonof the uncomplicated condition of the colon in all the other-cases.
(5) Atteqpt at NEdperimental Production.
I have attempted experimentally to determine whether manualtraction on the upper part of the hepatic flexure would producea displacement of the commencement of the jejunum and unfoldits mesentery.
l On bilocular stomach, see Keith, Jour. Anat., April 1898, p. 456.
672)

TIlE PIU( )I)ENN(-JElJU-NAL FLEX IE. 73
The subject used was a female, agred 18 years, deceased onlyone (lay. The commencement of the jejimunu occupied the' third' position, i.e., forwards and downwards. No peritonealfosse were present. The ascending colon was straight.A wooden clanil), 3 inches in lenigthl, was fixed to the colon
immnediatel 1 elow the hepatict flexure: steady traction wasex-erted thereon in a rightward and downward dlirection by meansof a spring balance. The colon rapidly qtc( uired a mesentery,,,and the jejimuiiial iinesentery shifted its position onl the parietesso that the small gut lay transversely to the column. At thispoint the balance registered a tension of 10 11)s. Thlhe peritoneuniDoW unfortuinately tore, leaving, the colonl free. rTle jejunalinesentery was not unfolded by the pulling, 1lit sul)sequent gentletraction with the finger-tips easily displaced it, so that the gutb came retro-peritoneal,-thus, at any rate, showingcr how easilyperitoneal displacement may 1 e effected.
(6) Evlnryological LE idev oe.
I have examined the literature of the (levelopmnent of thepart, hoping that it might throw some light onl the subject, butthere (loes not appear to be any very definite information.
His's figures (11) seem to indicate that as soon as the variousparts of the alimentary canal are differentiated, that which willbe the first part of the jejuniuni occupies .a position to the leftof the median line, from which it pa-sses ilnt( the loose coils ofgut by a gentle curve downwards from left to right.
Dexter (12), in a recent comminnicatiol on1 the subject, saysthat after the recession of the gut from the v-entral hernia, " thejejununm usually forms a simple loop towards the right side ofthe embryo." Apparently this description refers to the jejunumas a whole, so that one cannot make use of the observation here.
[1- EFERENC ES.
6 ?7 3

THE DUODENO-JEJUNAL FLEXURE.
REFERENCES.
Anatomical D)escriptions.
(1) TREVES, "The Anatomy of the Intestinal Canal and Peritoneumin Man," Hunterian Lectures, 1885.
(2) JONNESCO,-(a), Hernies Internes Retro-peritone'ales, 1890.(b), Poirier, Traite d'anatomie hurmaine, vol. iv.
p. 267.+3) MACALISTER, Text-bool of Hunzan Anatowuy, p. 40].(4) SAPPEY, Traite' d'anatomnie descriptive, tome iv. p. 189.(5) GEGENBAUR, Anatomie des llenschen, 1892, band ii. p. 57.(6) CUNNINGHAM, Manual of Practical Anatowy, vol. i. p. 57.(7) HOLDEN, Manual of Anatomy, 1882, p. 475.(8) W. J. YOUNG, " Note on the Curvature of Stomach and Duo-
denum," Proc. Anat. Soc. of Great Britain and Ireland, Feb. 1898,p. 41.
Peritoneal Distribution.
(9) OSCAi HERTWIG, Text-book of Embryology (MNark's translation,1892), p. 301.
(10) TREVES, ride supra, p. 20.
Emtbryology, etc.
(11) His, \V., Anatomie AMenwscllicher Embryonen, sec. iii. p. 24,fig. 14.
(12) DEXTER, F., "On the )evelopment of the Intestine of theCat," Journal of Boston Soc. Med. Sciences, vol. ii. No. 8, p. 127.
(13) WIEDERSHIEIM, Structure of Man (Bernard's translation), p.165.
'674