Embed Size (px)
Citation preview

826
RESTORING PHYSICAL MOBILITYC h a p t e r
32
Media Resources • Nursing Skills Online
• Evolve Website http://evolve.elsevier.com/Harkreader/
• Companion CD
• Skills Video Clips
Learning ObjectivesAfter studying this chapter, you should be able to do the following:• Describe the concepts of the structure and function
of the musculoskeletal system pertaining to mobility• Discuss factors affecting mobility• Describe the assessment of a client with impaired
mobility• Identify appropriate nursing diagnoses for clients
with mobility problems
• Identify expected outcomes for permanent and temporary mobility problems
• Intervene to assist a client with restoring or improving mobility
• Evaluate nursing care for the nursing diagnoses Impaired physical mobility and Activity intolerance
Key Terms fl accidhemiparesishemiplegiaisometric exerciseisotonic exercise
kyphosisparaparesisparaplegiaPQRST modelproprioception
quadriparesisquadriplegiarange-of-motion exercisesspasticsynovium

C h a p t e r 32 Restoring Physical Mobility 827
K ristina Lasauskas has been in an assisted living facil-ity since her husband died 5 years ago. Last year she
had a stroke, which left her weak on the right side. She ambulates independently with a cane. This morning her neighbor found her on the fl oor, and she was subsequently diagnosed with a fractured hip. She was admitted to the hospital for emergency surgery to repair the hip.
After the surgery, the nurse assesses her to identify nursing diagnoses and subsequent interventions. Because the client has previous right-sided weakness and has had surgery on her left hip, the nurse considers Impaired physical mobility and Activity intolerance as potential nurs-ing diagnoses (see key nursing diagnoses box). The nurse also expects the client to have pain.
before puberty. In adults, the parathyroid hormone, es-trogens, and glucocorticoids work together to ensure a balance in calcium, phosphorus, and vi tamin D. Over 99% of the body’s calcium and 90% of the body’s phos-phorus are stored in a total of 206 bones.
From puberty through young adulthood, the amount of bone formation (osteoblastic activity) is greater than the amount of bone resorption, or destruction (osteo-clastic activity). Beginning at about 35 years, osteoclastic activity becomes greater than osteoblastic activity. The resulting decreased bone mass predisposes middle-age and older adults to bone injury.
Besides forming the skeletal framework and storing vital minerals, bone assists in movement of joints, and it produces red blood cells (RBCs) in its red marrow. Long bones that bear weight, such as the femur, manufacture more RBCs than short bones, such as the phalanges (fin-gers and toes). Some of the flat bones, especially the ster-num and part of the pelvis, also contain blood-forming cells. These sites are commonly used for bone marrow aspiration and analysis to determine the body’s ability to produce RBCs.
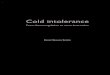
Joints. A joint is the point of articulation between two or more bones, and it usually allows voluntary move-ment. The most common type of joint is the freely mov-able synovial, or diarthrodial, joint (Figure 32-1). The surface of each bone end of a synovial joint is covered with articular cartilage and attached by ligaments. The synovium (synovial membrane) is the inner layer of the articular capsule surrounding a freely movable joint. It is loosely attached to the external fibrous capsule and secretes a thick fluid to lubricate the joint and absorb shock.
As adults age, deterioration of cartilage causes pain and possible inflammation. Arthritis, or joint inflamma-tion and degeneration, results from “wear and tear” and can limit mobility.
Some joints are not movable, such as those in the adult skull. They are called synarthrodial joints. In the normal newborn infant, however, the cranial bones are separated by fibrous tissue (sutures) in which growth occurs.
CONCEPTS OF PHYSICAL MOBILITYNo matter which health care setting you practice in, you will care for clients with varying limitations in physical mobility. These limitations commonly result from mus-culoskeletal or neurological injury, disease, or surgery. However, any severe illness or injury may affect a client’s physical mobility. For example, congestive heart failure can cause severe fatigue. Complications of long-term impaired mobility, regardless of cause, can lead to seri-ous or life-threatening conditions, such as pneumonia. You will need to understand the structure and function of the musculoskeletal system to assist clients with prob-lems related to mobility.
STRUCTURE OF THE MUSCULOSKELETAL SYSTEMAs a body system, the musculoskeletal system is second in size only to the integumentary system. It includes bones, joints, skeletal muscles, and other soft tissues.
Bones. Bone is a highly vascular and dynamic body tissue. Throughout childhood until puberty, many hor-mones and other substances influence bone tissue growth. Growth hormone, secreted by the anterior lobe of the pituitary gland, determines bone structure formed
KEY NURSING DIAGNOSES FOR MOBILITY
Impaired physical mobility: A limitation in independent, purposeful physical movement of the body or of one of the extremitiesActivity intolerance: Insuffi cient physiological or psycho-logical energy to endure or complete required or desired daily activities
© 2007, JupiterImages Corporation.

UNIT VII I • Act iv i ty–Exercise Pattern828
Other joints, called amphiarthrodial joints, are slightly movable. Joints within the pelvis must be slightly mov-able to allow for childbirth. Joints between the ribs and sternum are slightly movable to allow the chest to ex-pand with respiration.
Skeletal Muscles. Unlike the smooth, or nonstriated, muscles in organs and the muscle in the heart, skeletal muscles are under voluntary control by the central and peripheral nervous systems. Skeletal muscles are sur-rounded by dense, fibrous tissue called fascia. Small bundles of muscle tissue, blood vessels, and peripheral nerves make up compartments in the extremities, espe-cially the distal part of each extremity.
As part of aging, muscle fibers decrease in size and number. Exercise helps keep intact fibers from atrophy, a decrease in the size of a normally developed tissue or organ caused by inactivity or diminished function. Muscle atrophy causes weakness that can limit physical mobility.
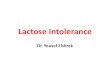
Soft Tissues. Adjacent fibrous tissues, such as tendons and ligaments, support skeletal muscles and bones. Tendons attach muscles to bone (Figure 32-2); ligaments attach bones to bones at joints. Both of these soft tissue types are prone to injury, especially during contact sports, such as football, or physically demanding activi-ties, such as tennis and skiing.
Cartilage is found on bone ends of synovial joints, the rib-sternum junctions (costal cartilage), nasal septum and trachea (hyaline cartilage), and external ear (yellow cartilage). Cartilage is flexible tissue, but it can withstand enormous tension.
FUNCTION OF THE MUSCULOSKELETAL SYSTEMTogether with the nervous system, the musculoskeletal system enables us to move in a coordinated manner. Muscles are grouped according to the type of movement they allow. For example, flexors allow a joint or an ex-tremity to flex or bend; extensors allow the joint or extremity to extend or straighten out. The elbow is an example of a synovial joint that can flex and extend. These movements are discussed later under range-of-motion (ROM) exercises.
Regulation of Movement. Movement is regulated by the central and peripheral nervous systems. The primary mo-tor area (the motor “strip”), located in the frontal lobe of the cerebrum, is responsible for voluntary muscle con-traction of muscle groups. Adjacent to the motor area is the premotor area, which directs new movements or movements that have been changed. Motor neurons and premotor neurons, also referred to as upper motor neu-rons, synapse with the corticospinal tract nerve fibers and descend into the spinal cord. At the level of the me-dulla, these fibers cross to the opposite side of the body. Thus, the left motor area in the brain controls the right side of the body, and vice versa.
As the nerve fibers descend into the spinal cord, some synapse with peripheral nerves that supply the head, trunk, and limbs (lower motor neurons). Others synapse with interneurons in the cord. The peripheral nerves contain motor, sensory, and sometimes auto-nomic fibers. The motor fibers stimulate muscles to
Bone
Jointcapsule
Synovium
Subchondralbone plate
Joint cavity
Articularcartilage
Tendon
Muscle
FIGURE 32-1 Structure of a synovial joint. (From Ignatavicius, D. D., Workman, M. L., & Mishler, M. A. [1999]. Medical-surgical nursing across the health care continuum [3rd ed.]. Philadelphia: Saunders.)
Gastrocnemius muscle
Soleus muscle
Achilles tendon
FIGURE 32-2 Tendons attach to muscles and bone.

C h a p t e r 32 Restoring Physical Mobility 829
contract. Special chemicals called neurotransmitters, such as acetylcholine, facilitate muscle contraction. After muscle contraction, the muscle then relaxes be-cause certain enzymes destroy the neurotransmitters after muscle contraction.
Proprioception. Proprioception is sensation pertain-ing to stimuli originating from within the body regard-ing spatial position and muscular activity, or to the sen-sory receptors that they activate. It is our awareness of body position, posture, and movement. Small receptor cells in skeletal muscle, subcutaneous tissue, and the in-ner ear respond to stimuli within the body, such as pres-sure or muscle stretch, promoting this awareness. For example, we know if we are standing or sitting, even if our eyes are closed. In a sense, proprioception is a pro-tective function, enabling us to be aware of our bodies without actually seeing them.
Body Mechanics. Body mechanics describes the use of the body in movement and at rest. Improper use can cause fatigue and injury, such as back strain. Back injury among health care workers and others who perform physical activities is a common and costly health prob-lem that commonly results from poor body mechanics. Health care workers must use proper body mechanics as a baseline effort to prevent injury, maintain balance, and conserve energy.
Components. The center of gravity, located within the pelvis, is the point where the body’s mass is cen-tered. The body maintains optimal balance and align-ment when the line of gravity (an imaginary line) passes through the center of gravity. The base of support for the body includes the feet and the distance between the feet.
Principles. While sitting, standing, or lying, the body can easily maintain alignment. However, when lifting,
pushing, or pulling an object, the center and line of grav-ity shift, possibly causing poor body alignment and in-jury from loss of balance or stress on soft tissues.
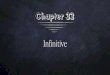
Large muscle groups in the legs and arms should per-form the work required to lift an object. As seen in Figure 32-3, the proper use of these muscles helps prevent back stress and strain. The back must remain straight during lifting, pulling, or pushing. Moving the feet farther apart broadens the base of support and keeps the body bal-anced during physical activity. Twisting the body should also be avoided. Pivoting on the ball of one foot keeps the back straight. Table 32-1 summarizes key principles of proper body mechanics.
Body Alignment. When the body is not moving, align-ment is also important. When in a standing, sitting, or lying position, the body should be aligned so that the line of gravity passes through the center of gravity and the longer and stronger muscles do the work. Poor posi-tioning changes the center and line of gravity, causing muscle fatigue and stress. When sitting, standing, or walking, good posture allows the least amount of stress on muscles, joints, and soft tissues because the line of gravity passes perfectly through the center of gravity.
Children. When an infant sits, the thoracic spine appears curved or convex because of weak chest and truncal muscles. As the muscles strengthen and the child begins to walk, the back straightens. Normal tod-dlers and preschool children may actually appear to have an increased lumbar concavity because they have protuberant abdomens. Adolescents who grow quickly may slouch forward, producing a round-shouldered appearance.
Adults. Good posture for adults means that the head is held erect, shoulders are back, and vertebral column is held straight. Poor posture can result in back discomfort
Straight back
Rounded back
FIGURE 32-3 Lifting an object using proper (left) and improper (right) body mechanics.

UNIT VII I • Act iv i ty–Exercise Pattern830
Principles and Benefits of Proper Body Mechanics
PRINCIPLE BENEFIT
• Pull, push, or roll objects rather than lifting them. Reduces the workload• Pulling is usually easier than pushing, so pull clients toward you rather than pushing them.• Lower the head of the bed to move a client up in bed. Decreases opposition from gravity and
decreases friction and shear• Size up your load to determine whether you need help. Prevents muscle strain• Keep your back straight when moving an object.• Use the longest and strongest muscles of your legs and arms rather than the weaker muscles
of your back.• Rock your body to use the weight of your body to enhance the force of your arm muscles.• Move your body as a unit when twisting, stretching, or reaching.• Lower your center of gravity by bending your knees. Maintains stability• Widen your base of support by moving your feet apart.• Maintain your center of gravity (your pelvis) over your base of support. To support a client,
stand close; carry an object close to your body.
from excessive strain. As adults age, especially post-menopausal women, vertebral bone mass decreases and the thoracic spine becomes more convex, or curved.
Gait. The manner in which we walk is referred to as gait. As a person ages, the long, smooth steps often shorten and become less steady. This change is particu-larly obvious for older women who have decreased ver-tebral bone mass. The normal, automatic gait has two phases—the stance phase and the swing phase (Figure 32-4). The stance phase includes the heel strike through the push-off action of the first foot. An abnormality in
the stance phase is called an antalgic gait. The swing phase includes the action of the second foot from accel-eration through deceleration. An abnormality in this phase is called a lurch. Pain, muscle weakness, and limb shortening are common causes of abnormal gait.
FACTORS AFFECTING MOBILITYMany factors can affect a person’s mobility, including lifestyle, environment, physical development, and patho-physiological conditions.
Table 32-1
Heel strike
STANCE PHASE
SWING PHASE
Acceleration Mid-swing Deceleration
Foot flat Mid-stance Push offFIGURE 32-4 Normal phases of gait. (From Ignatavicius, D. D., Workman, M. L., & Mishler, M. A. [1999]. Medical-surgical nursing across the health care continuum [3rd ed.]. Philadelphia: Saunders.)

C h a p t e r 32 Restoring Physical Mobility 831
LIFESTYLE FACTORSSome recreational activities place people at a high risk for musculoskeletal injury. For example, physically de-manding sports such as skiing, football, and tennis can result in fractures or soft tissue damage. Failure to ade-quately train or physically prepare for these activities contributes to injuries. Carelessness and unnecessary risk taking also cause accidents, which may be fatal.
Diet and exercise affect mobility. A diet low in cal-cium, protein, and other vital nutrients prevents bone growth and development in children and contributes to bone loss in older adults. The resulting “brittle” bones are prone to deformity and fracture. Regular exercise helps build strong bones and muscle tissue. Assess your client’s cultural beliefs about diet and other lifestyle con-siderations to determine factors that might affect mobil-ity. Box 32-1 offers one example.
ENVIRONMENTAL FACTORSEnvironmental factors can lead to accidents or injury either in the workplace or at home. You can be instru-mental in teaching clients about ways to prevent muscu-loskeletal injury.
Workplace. In the United States, the Occupational Safety and Health Administration (OSHA) establishes standards for workplace safety. The purpose of OSHA is to protect workers from injuries and accidents. The three major causes of worker injury are repetitive motion, poor body mechanics, and accidents.
Lifting and moving clients while using poor body mechanics can cause musculoskeletal injury. Back sup-ports are commonly required for workers who lift ob-jects as part of their jobs. Nurses have an alarming rate of back injury, with 52% of registered nurses (clustered with licensed practical nurses, nurse’s aides, and atten-dants) reporting chronic back pain (Nelson, 2003). The problem is so significant that the American Nurses
Association has launched the Handle With Care cam-paign to promote safe client handling and to prevent musculoskeletal disorders among nurses in the United States (www.NursingWorld.org/handlewithcare/). In 2003, OSHA put forth voluntary ergonomics guidelines to help prevent musculoskeletal disorders in workers in nursing homes.
Effective January 1, 2006, Texas was the first state to legislate that hospitals and nursing homes must imple-ment safe client handling and movement programs. The intent is to reduce the risk of injury to clients and health care workers associated with lifting, transferring, reposi-tioning, and moving clients. The intent is to eliminate manual lifting and mandate the use of assistive devices in routine care. This landmark legislation has spurred similar types of legislation in other states and may be the precursor to a federal initiative for no-lift health care environments (Hudson, 2005).
Home. Accidents from environmental hazards also occur in the home. Because OSHA has no jurisdiction in private residences, the homeowner must ensure that the home structure and equipment are safe. For older adults, reducing environmental hazards is especially important for preventing falls (see Chapter 23).
DEVELOPMENTAL FACTORSMost age-groups are at risk for decreased mobility, espe-cially children, young adults, and older adults.
Children. Infants may be born with congenital muscu-loskeletal deformities that decrease their ability to crawl or walk. Abnormal fixed positions of the feet, such as metatarsus varus (pigeon toe, toes pointing in), metatar-sus valgus (duck walk, toes pointing out), and talipes equinovarus (clubfoot or twisted foot) can worsen and delay physical development if not corrected.
Congenital dysplasia of the hip is one of the most common musculoskeletal malformations. The femoral
Caring for a Lithuanian American Woman
Mrs. Lasauskas is a Lithuanian American who came to the United States when she was 30 years old with her husband and two small children. The family lived with relatives in Boston, where her husband worked as a janitor while he perfected his English. He then received a position as a col-lege professor. Kristina is a devout Catholic and has enjoyed being visited by the young priest from her parish. Her daugh-ter lives nearby and visits her mother daily and sometimes brings the great-grandchildren to play games with “Nana.” Although each person is an individual and customs vary, some Lithuanian Americans may share the following values (Leininger, 1991):• Closeness among extended family members• Religious beliefs and prayers (Roman Catholic)• The importance of education
• Hard work and industriousness• Thriftiness and good use of material resources• Endurance, persistence, and suffering with economic
hardships• Charity to others• Helping in times of need• Hospitality to others• Sharing with others• Flexibility• Cooperation with others• Praying with others• Using subtle humor
Cross-Cultural CareBOX 32-1

UNIT VII I • Act iv i ty–Exercise Pattern832
head is partially displaced from the pelvic acetabulum. If this condition is not diagnosed until after the child walks, the child will have a limp. If both hips are af-fected, the child will have a waddling gait.
A small number of infants are born without complete extremities, causing marked problems with learning to sit, crawl, and walk. In other infants, toes or fingers may be webbed, ultimately resulting in decreased function.
Congenital spinal deformities may also occur (Figure 32-5). The most common is scoliosis, a lateral deviation of the spine typically diagnosed in preadolescent and adolescent children. If not corrected, this deformity can also affect the cardiopulmonary system.
Young Adults. The highest incidence of musculoskel-etal injuries is among young men between ages 18 and 25. Young men often take risks, such as driving at ex-cessive speeds or without a seat belt or operating a motorcycle without a helmet. Alcohol or drug con-sumption increases the risk associated with these activities.
Older Adults. Aging typically results in muscle weak-ness and atrophy, decreased coordination and balance, and loss of bone tissue. These physiological changes de-crease mobility but should not prevent independent function. Staying active and exercising help keep intact muscle fibers strong and promote coordination and bal-ance. In hospitalized older adults, however, decondition-ing can occur in a matter of days (Graf, 2006). This makes it imperative to be concerned with maintaining mobility throughout hospitalization (Fletcher, 2005; Gillis & MacDonald, 2005).
As discussed earlier, after the age of 35, bone break-down exceeds bone formation. After menopause in women, bone mass decreases (osteoporosis), possibly causing painful fractures of the wrist, vertebral column, and hip. Men have large amounts of tes tos ter one, which
results in continued formation of bone until about age 80. After age 80, men also have a high risk of hip frac-tures. Measures to prevent or slow bone loss include calcium supplements, exercise, and precautions to pre-vent falls.
PHYSIOLOGICAL FACTORSMany acute and chronic health problems can decrease mobility; this discussion is limited to common prob-lems affecting the musculoskeletal and nervous systems.
Musculoskeletal Problems. Musculoskeletal problems can be divided into inflammatory, degenerative, trau-matic, and congenital problems. Rheumatoid arthritis is one of the most common inflammatory problems occur-ring at any age and potentially causing joint deformity and chronic pain. This systemic disease also affects ma-jor body organs and must be treated aggressively to slow its progress. Degenerative joint disease, or osteoarthritis, is an example of a degenerative process that is seen most often in older adults, but also commonly affects athletes and obese individuals.
Trauma often results in bone fractures or dislocations and soft tissue damage. Fractures occur in any age-group, but they heal most readily in infants and young children. A young, healthy adult heals in 4 to 6 weeks; young chil-dren heal in 1 to 2 weeks, and older adults may take up to 3 months for bone healing.
Neurological Problems. Brain or spinal cord damage is a leading cause of immobility. Depending on the level of injury, the person will be weak (paresis) or paralyzed (ple-gia). When injured at the cerebral or cervical spine level, the client may experience quadriplegia—an abnormal condition characterized by paralysis of the arms, legs, and trunk below the level of the injury. Quadriplegia may also be called tetraplegia. Alternatively, the client might experi-ence quadriparesis, a numbness or other abnormal or impaired sensation in all four limbs and the trunk. Lower-level spinal injuries result in paraplegia—paralysis char-acterized by motor or sensory loss in the legs and trunk. Or the client might experience paraparesis, a numbness or other abnormal or impaired sensation in the legs and trunk.
Middle-age and older adults are at risk for degenera-tive or thrombotic neurological health problems. Parkinson’s disease is a common degenerative, pro-gressive process in which the client eventually becomes completely immobile. Cerebrovascular accidents (strokes) are the most costly disability. Part of the brain becomes damaged (infarcted) from hyp oxia caused by a thrombus (stationary blood clot), embolus (dislodged blood clot), or hem or rhage. The typical cli-ent with a stroke has hemiplegia (paralysis of one side of the body) or hemiparesis (numbness or other ab-normal or impaired sensation on one side of the body), which may limit mobility and activities of daily living (ADLs).
Lordosis Scoliosis Kyphosis
FIGURE 32-5 Common congenital spinal deformities. (From Ignatavicius, D. D., Workman, M. L., & Mishler, M. A. [1999]. Medical-surgical nursing across the health care continuum [3rd ed.]. Philadelphia: Saunders.)

C h a p t e r 32 Restoring Physical Mobility 833
Recall the case study: Kristina Lasauskas’s previous stroke had left her with hemiparesis. What concerns should you have about her postoperative rehabilitation program? Might she be at risk for another stroke?
ASSESSMENT
GENERAL ASSESSMENT OF PHYSICAL MOBILITYHealth problems that impair mobility may affect any body system. To assess physical mobility, collect data related to the musculoskeletal system.
Health History. The health history elicits information about the client’s chief complaint, risk for musculoskel-etal health problems, previous or current treatment plan, and current condition.
Chief Complaint. The most common complaints as-sociated with musculoskeletal health problems are pain, muscle weakness, and inflammation. Pain may be acute or chronic; it may be assessed using the following PQRST model of symptom analysis:P—What was the provoking incident that caused the pain,
if any?Q—What is the quality of the pain? Is it burning, throb-
bing, stabbing?R—Where is the region of pain? Does it radiate? Does
anything relieve the pain?S—How severe is the pain?T—What is the timing of the pain? When does it occur
and how long does it last?Also assess any history of muscle weakness or
inflammation:• Have you experienced muscle weakness or fatigue? If
so, when does it occur?• Do you find that you drop items or stumble at times
when walking?• Have you noticed any redness or excessive warmth
around your joints or over muscles?• Have you been unable to carry out any usual daily
activity? Have you had to restrict some of your usual activities?Risk for Musculoskeletal Health Problems. Determine
which factors place the client at risk for a musculoskeletal health problem, such as age, work and home environ-ments, lifestyle, and personal and family history of muscu-loskeletal problems. Some health problems tend to recur. A complete history of previous problems and how they were managed could provide important data that aids in diagnosis and management of the current condition.
Ask the client about treatments that have been or are being received that could contribute to the current health problem. You might use the following questions:• Have you had any surgery? If so, what and when?
(Previous surgery could cause nerve or muscle weakness.)
• What medications are you taking, including both prescription and over-the-counter? (Some medica-tions have side effects that cause weakness, lowered blood pressure, or muscle atrophy. Other medica-tions may be given to prevent musculoskeletal prob-lems, such as calcium and alendronate [Fosamax], to prevent or treat osteoporosis.)
• Are you currently under a physician’s care? If so, what for and how is it being treated?Physical Examination. The musculoskeletal physical
examination includes assessing body alignment, gait, joints, and skeletal muscles. For clients who experience musculoskeletal trauma or surgery, you frequently mon-itor neurovascular function as well.
Body Alignment. If possible, observe the client’s posture and positioning while sitting, lying, and stand-ing. Assess for scoliosis and kyphosis. In scoliosis, the vertebral column deviates laterally. In children or ado-lescents, it may result from habit (functional), muscle weakness, contractures, or a tilted pelvis. Have the cli-ent bend forward at the waist. If the deviation disap-pears when the client bends forward, the problem is functional. If it does not disappear, the problem may require treatment.
Kyphosis is an abnormal condition of the vertebral column characterized by increased convexity in the tho-racic spine when viewed from the side. It is common in middle-age and older adults. The client’s shoulders are slouched, and the vertebral bones are very prominent. Check to ensure that this problem is not interfering with breathing.
Gait. Observe while the client ambulates if the client can walk. Note the stance and swing phases, looking for limps or other abnormalities in gait. If the lower extremi-ties are not the same length, the client will walk with a limp. Ask the client if there is a congenital abnormality or if surgery was performed on one or both extremities.
Joints. The best method for assessing joints is to use a head-to-toe approach, beginning with joints of the head and neck and progressing to the lower extremities. Inspect the joints for proper alignment, symmetry, red-ness, and swelling. Then, palpate each joint for tender-ness and masses. Finally, put each joint through its ROM to determine function and listen for crepitus, a continu-ous grating sound caused by joint deterioration.
Assessing the extremities is particularly important because the client needs full use of these joints for per-forming ADLs. For example, clients with shoulder limita-tions and pain may not be able to perform hair groom-ing. Clients with hand deformities due to arthritis may have trouble cutting food or opening food containers.
Ask the client to move each joint through its ROM. The normal ROM for each joint is illustrated in Table 32-2. As long as the client can perform ADLs, a slight limitation of ROM is acceptable, especially for older adults.
Text continued on p. 836

UNIT VII I • Act iv i ty–Exercise Pattern834
AREA OF BODY/MOTION AREA OF BODY/MOTION
NECKFlexion (45 degrees),
extension (45 degrees), hyperextension (50 degrees)
Lateral flexion (40 degrees)
Rotation (70 degrees)
SHOULDERFlexion (180 degrees),
extension (180 degrees), hyperextension (50 degrees)
Abduction, adduction
SHOULDER—CONT’DCircumduction (360 degrees)
External rotation (90 degrees), internal rotation (90 degrees)
ELBOWFlexion (160 degrees),
extension (160 degrees)
Rotation for supination, rotation for pronation (180 degrees)
WRISTFlexion (90 degrees),
extension (90 degrees), hyperextension (70 degrees)
Table 32-2 Reviewing Range of Motion
Abduction
Adduction
External
Internal
Flexion
Extension
Supination Pronation
Hyperextension
Extension
Flexion

C h a p t e r 32 Restoring Physical Mobility 835
HIP—CONT’DAbduction (30-50 degrees),
adduction (30-50 degrees)
Circumduction (foot makes small circle)
External rotation, internal rotation (90 degrees)
KNEEFlexion, extension
(120-130 degrees)
WRIST—CONT’DUlnar flexion
(adduction) (30-50 degrees), radial flexion (abduction) (30 degrees)
HAND AND FINGERSFlexion (90 degrees),
extension (90 degrees), hyperextension (150 degrees)
Abduction, adduction (spreads to 90 degrees)
Opposition of thumb (thumb touches each finger)
HIPFlexion (90-120 degrees),
extension (90-120 degrees), hyperextension (30-50 degrees)
AREA OF BODY/MOTION AREA OF BODY/MOTION
Table 32-2 Reviewing Range of Motion
Ulnar flexion
(adduction)
Radial flexion
(abduction)
Hyper-extension Extension
Flexion
Flexion
ExtensionHyper-extension
AdductionAbduction
Flexion: Bending at a joint in the natural direction of movement.Extension: Moving from the flexed position to a neutral or straight position.Hyperextension: Moving beyond a straight or neutral position.Rotation: Pivoting a body part on its axis.Abduction: Movement of a limb in a direction away from the midline of the body.Adduction: Movement of a limb in a direction toward the midline of the body.Circumduction: A combination of movements that causes a body part to move in a circle.External rotation: Rotation from a joint in the direction away from the midline of the body.Internal rotation: Rotation from a joint in the direction toward the midline of the body.Supination: Rotation of the palm of the hand upward or in the anterior direction.Pronation: Rotation of the palm of the hand downward or in the posterior direction.Opposition: The relationship of the thumb and fingers for the purpose of grasping objects.Eversion: Movement of the ankle to turn the sole of the foot laterally (away from the midline).Inversion: Movement of the ankle to turn the sole of the foot medially (toward the midline).Dorsal flexion: Flexion of the ankle in the direction of the dorsal surface.Plantar flexion: Flexion of the ankle in the direction of the plantar surface.
Flexion
Extension
Continued

UNIT VII I • Act iv i ty–Exercise Pattern836
RATING DESCRIPTION5 Normal: ROM unimpaired against gravity with full resis-
tance4 Good: Can complete ROM against gravity with some
resistance3 Fair: Can complete ROM against gravity2 Poor: Can complete ROM with gravity eliminated1 Trace: No joint motion and slight evidence of muscle
contractility0 Zero: No evidence of muscle contractility
Skeletal Muscles. Skeletal muscles can be examined at the same time as joints. Observe each major muscle group for symmetry in size, shape, tone, and strength. Palpate the muscle, and ask the client to demonstrate its strength—for example, by squeezing your hand or a sphygmomanome-ter. The latter method provides a numerical score that can be used later for comparison. To check for movement against resistance, ask the client to move an extremity while you are trying to prevent that movement.
Physical and occupational therapists perform more detailed assessments of muscle strength using various scales. Table 32-3 describes Lovett’s scale for determining muscle strength. Using this scale, the therapist assesses each muscle and scores it as a rating out of a possible 5.
FOOT AND TOESFlexion (30-60 degrees),
extension (30-60 degrees)
Abduction (15 degrees or less), adduction (15 degrees or less)
ANKLEExtension (20-30 degrees),
flexion (45-50 degrees)
Eversion (10-20 degrees), inversion (10-20 degrees)
AREA OF BODY/MOTION AREA OF BODY/MOTION
Table 32-2 Reviewing Range of Motion—cont’d
Eversion Inversion
Dorsiflexion (flexion)
Plantarflexion (extension)
Adduction
Abduction
Flexion
Extension
Table 32-3 Lovett’s Scale of Muscle Strength
From Ignatavicius, D. D., & Workman, M. L. (Eds.). (2002) Medical-surgical nursing: Critical thinking for collaborative care (4th ed.). Philadelphia: Saunders.ROM, Range of motion.
For example, if a muscle is rated as a 3/5, the client has fair strength, can complete ROM, but cannot move against resistance. If it is available, review the client’s muscle strength evaluation to help determine how much assistance you might need when getting the client out of bed or ambulating.
Neurovascular Status. Your major responsibility is frequent monitoring of neurovascular status, or CMS (circulation, movement, sensation) assessment (Alitzer, 2004). Check for skin color, temperature, movement, sensation, pulses, capillary refill, and pain; document and report adverse changes. Always compare the affected limb with the unaffected one. Table 32-4 describes neu-rovascular assessment and gives the normally expected findings.
This assessment is especially important when external devices, such as casts and bulky dressings, can compress the compartments created by sheaths of inelastic fascia, causing extensive tissue damage. Excessive tissue fluid from severe burns, insect bites, or infiltration of intrave-nous fluids can increase compartmental pressure. If this pressure is not relieved, isch emic tissue necrosis can result in 4 to 8 hours. Known as compartment syndrome, this phe-nomenon occurs in the extremities, especially the legs, where a sheath of inelastic fascia partitions blood vessel, nerve, and muscle tissue, and the pressure in this compart-ment is normally less than capillary pressure.
Action Aler t! Notify the physician immediately of signs of compartment syndrome.

C h a p t e r 32 Restoring Physical Mobility 837
Increased pain on passive motion when compared with active motion, or loss of sensation in the web space between the great and second toes (or between the thumb and second finger on the hand), indicates early compartment syndrome. When the client is in late-stage compartment syndrome and damage is not reversible, the six “Ps” may be pres ent, including the following:• Pain not relieved• Paresthesias• Pallor• Pulse absent (pulselessness)• Paralysis• Palpated tense tissue
Do not wait until these signs and symptoms are pres-ent. The earlier compartment syndrome is treated, the better the prognosis is. Compartment syndrome may require amputation of the limb if the neurovascular compromise is not promptly assessed and managed.
Postoperatively, Mrs. Lasauskas has a physician’s order to perform “CMS checks” every 4 hours. Why is this client at risk for neurovascular compromise?
Diagnostic Tests. Diagnostic tests are commonly per-formed to determine the nature and extent of musculosk-eletal health problems that may interfere with mobility.
Radiographs (or x-ray films) detect bone density, swell-ing, alignment, and continuity. Joint structure can be visu-alized, but soft tissues are not always clearly differentiated. Remind the client to remain still during the procedure even though the table may feel cold and hard.
The computed tomography (CT) scan provides a better picture of soft tissues and less-dense bone than standard x-rays, especially in the vertebral column. It can also identify problems of the central nervous sys-tem, such as strokes and tumors. A CT scan may be done with or without use of a contrast medium to en-hance the views. If contrast will be used, check that the client has had nothing by mouth (NPO status) for at least 4 hours, that there is no allergy to iodine or sea-food, and that the client has signed an informed con-sent form.
Magnetic resonance imaging (MRI) is often more ac-curate than either standard x-rays films or a CT scan for detecting soft tissue damage. The image is produced by the interaction of radio waves and magnetic fields. As with the CT scan, a contrast medium may be used to enhance the view. Ask the client to remove any metal objects, such as clothing with metal fasteners. Metal joint implants are safe, but pacemakers are not.
An arthrogram is an enhanced radiograph of a joint obtained after contrast is injected; it is performed most commonly for knees and shoulders. Inquire about aller-gies to iodine and seafood. Explain that joint swelling caused by the injection fluid will diminish within a day or two. If the joint injury is not severe, usual activities can typically be resumed within 12 to 24 hours.
A myelogram is a radiograph of the vertebral spine obtained after injecting a contrast medium into the lum-bar subarachnoid space. The spinal cord, vertebral bones, intervertebral disks, and surrounding soft tissues can be visualized. The client assumes a fetal position or
CHARACTERISTIC ASSESSMENT TECHNIQUE NORMAL FINDINGS
Skin color Inspect the area distal to the injury. No change in pigmentation compared with other parts of the body.
Skin temperature Palpate the area distal to the injury (the dorsum of the hands is most sensitive to temperature).
The skin is warm.
Movement Ask the client to move the affected area or the area distal to the injury (active motion).
The client can move without discomfort.
Move the area distal to the injury (passive motion). No difference in comfort compared with active movement.Sensation Ask the client if numbness or tingling is pres ent
(paresthesia).No numbness or tingling. No difference in sensation in the
affected and unaffected extremities.Palpate with a safety pin or paper clip, especially
the web space between the first and second toes or the web space between the thumb and forefinger.
Loss of sensation in these areas indicates peroneal nerve or median nerve damage.
Pulses Palpate the pulses distal to the injury. Pulses are strong and easily palpated; no difference in the affected and unaffected extremities.
Capillary refill Press the nail beds distal to the injury until blanch-ing occurs (or the skin near the nail blanches if nails are thick and brittle).
Blood returns (return to usual color) within 3 seconds (5 seconds for older adult clients).
Pain Ask the client about the location, nature, and fre-quency of pain.
Pain is usually localized and is often described as stabbing or throbbing.
Table 32-4 Assessing Neurovascular Status
From Ignatavicius, D. D., & Workman, M. L. (Eds.) (2002). Medical-surgical nursing: Critical thinking for collaborative care (4th ed.). Philadelphia: Saunders.

UNIT VII I • Act iv i ty–Exercise Pattern838
sits and bends at the waist to open the lumbar interver-tebral space before injection.
If a cervical myelogram is done, the client bends the neck forward. The injection site is locally anesthetized. After the contrast medium is injected, the client is moved into various positions while radiographs are taken. After the test, the client must be properly positioned to pre-vent cerebrospinal fluid (CSF) leakage and subsequent headaches.
Action Aler t! To prevent spinal headache or meningeal ir-ritation, the client must remain flat after use of an oil-based contrast or in a semi-Fowler’s position after use of a water-based contrast for at least 4 to 8 hours. Check the injection site for CSF leak. Also, frequently monitor the level of consciousness, and the ability to move and feel the limbs, and void spontaneously.
An arthrocentesis may be performed for diagnostic or treatment purposes. A sample of synovial fluid is with-drawn and sent to the laboratory for analysis. Clients with rheumatoid arthritis usually have copious synovial fluid that contains antibodies and white blood cells that are characteristic of inflammatory disease. If the joint swells excessively, some fluid can be removed to alleviate discomfort. Instruct the client that this test is usually done in the physician’s office, in a clinic, or at the bed-side. The injection site is locally anesthetized before the larger aspirating needle is inserted. After the aspiration, apply pressure until fluid leakage subsides.
In a healthy person, calcium and phosphorus have an inverse relationship, meaning that when the serum cal-cium level decreases, phosphorus increases, and vice versa. Bone disease and parathyroid dysfunction can cause alterations in this relationship.
Alkaline phosphatase is an enzyme that tends to in-crease when bone or the liver is damaged. Increases in serum levels reflect an increase in osteoblastic (bone-building) activity.
When skeletal muscles are damaged or diseased, se-rum muscle enzymes typically increase, including skele-tal muscle creatine kinase, lactate dehydrogenase, aspar-tate aminotransferase, and aldolase. Muscle trauma, polymyositis, and muscular dystrophy commonly cause increased serum muscle enzymes.
FOCUSED ASSESSMENT FOR IMPAIRED PHYSICAL MOBILITYNursing assessment includes interpreting data to select ap-propriate nursing diagnoses. A client has Impaired physical mobility when there is a limited ability to physically move. If the client has a prolonged impairment, complications of immobility may occur (see Chapter 33).
Defining Characteristics. Defining characteristics for the nursing diagnosis Impaired physical mobility include the following:• Postural instability while performing ADLs• Limited ability to perform gross or fine motor skills,
uncoordinated or jerky movements, limited range of motion, or difficulty turning
• Decreased reaction time• Slowed movement or movement-induced shortness
of breath or tremor• Gait changes (such as decreased walk speed, diffi-
culty initiating gait, small steps, shuffling of feet, exaggerated lateral postural sway)
• Substitutions for movement (such as increased at-tention to other’s activity, controlling behavior, fo-cus on activities that occurred before the illness or disability)A client’s inability to move includes bed mobility,
transfers from bed to chair, and ambulation. Assessing a client’s ability to move and perform ADLs is referred to as a functional assessment. Several functional assess-ment tools can be used to determine a client’s func-tional level. A very simple classification system is often used to designate the functional status. This system rates the client’s functional ability from a 0 (com-pletely independent) to a 4 (dependent and does not participate in activity). Box 32-2 illustrates the effects of impaired mobility on the life of one person.
Some clients may be able to move but are reluctant to do so because of pain or discomfort, fear of falling, or fear that they will dislodge or disrupt equipment be-ing used in their care, such as intravenous therapy. Reassure the client that the pain can be controlled and should not be tolerated. If equipment and lines are the concern, secure them so they will not kink, become dislodged, or disconnect.
Diseases such as arthritis and trauma such as fractures limit ROM in synovial joints, which reduces the client’s ability to move and perform ADLs. ROM is also limited in clients with contractures.
Prolonged immobility can cause muscle atrophy that then worsens the immobility. Neuromuscular diseases, such as Parkinson’s disease, muscular dystrophy, and amyotrophic lateral sclerosis, are characterized by mus-cle atrophy and subsequent decreased muscle strength. Clients with these disorders often experience respiratory failure because of muscle fatigue.
Spinal cord injuries disrupt nervous system commu-nication between the brain and peripheral muscles. A cervical or high thoracic injury (quadriplegia) spares the lower motor neurons, so reflex activity remains intact. The skeletal muscles below the injury are spastic, that is, they contract by reflex activity rather than by central ner-vous system control.
Injuries occurring in the lower thoracic or lumbosa-cral spine may result in paraplegia. The lower motor neurons, or reflex arcs, are damaged and the client’s muscles are flaccid—the state of being weak, soft, and flabby, lacking normal muscle tone, or having no ability to contract. Flaccid muscles tend to atrophy and decrease in mass more quickly than spastic muscles.
Related Factors. Factors related to the diagnosis Impaired physical mobility include the following:• Medications

C h a p t e r 32 Restoring Physical Mobility 839
• Prescribed movement restrictions or lack of knowl-edge about the value of physical activity
• Discomfort, intolerance to activity, reluctance to initi-ate movement, limited cardiovascular endurance, or decreased strength and endurance
• Body mass index above the age-appropriate 75th percentile
• Sensoriperceptual, neuromuscular, or musculoskele-tal impairments; cognitive impairment; pain
• Depression, anxiety, lack of physical or social envi-ronmental supports
• Decreased muscle strength, control, or mass; joint stiffness or contractures
• Sedentary lifestyle, disuse, or deconditioning• Selective or generalized malnutrition, altered cellular
metabolism• Loss of integrity of bone structures• Developmental delay• Cultural beliefs regarding age-appropriate activity
Many chronic diseases, such as coronary artery dis-ease, chronic respiratory disorders, terminal cancer, and neuromuscular diseases, can cause decreased muscle strength and endurance. Assess muscle strength using the Lovett scale, or suggest a physical therapy evaluation to assess individual muscle groups.
Older adults may have decreased muscle strength and impaired mobility because of the combined effects of the aging process, reduced overall activity level, and co-existing health problems that limit mobility. See
Box 32-3 for evidence-based guidelines for assessing physical mobility of older adults.
Acute or chronic pain may prevent a person from mov-ing a part or all of the body. Assess the type, nature, dura-tion, and location of pain as discussed in Chapter 37. Repositioning the client, providing massage, or enhanc-ing imagery may help relieve pain and promote mobil-ity. For more severe pain, administer a prescribed analge-sic and evaluate its effectiveness.
Action Aler t! For clients who cannot verbalize complaints of pain, especially older adults who have dementia or delirium, use nonverbal cues, such as moaning, crying, or restlessness, to assess their pain level. Anticipate the need for pain relief inter-ventions, including medication.
Neuromuscular or musculoskeletal impairments may be acute and reversible or chronic and disabling. In ad-dition to the chronic spinal cord injuries, stroke, and neuromuscular diseases described earlier, clients may experience acute problems that temporarily decrease mobility. Fractures or other soft tissue injuries are com-mon examples of acute musculoskeletal impairments. When these injuries heal, the client usually returns to baseline activity level.
Clients with dementia, as in late-stage Alzheimer’s disease, experience Impaired physical mobility and usually die as a result of complications of immobility. The client forgets how to perform ADLs and ambulate.
“Fortunately, I Had Nurses and Therapists Who Took Time to Get to Know Me”
A Patient’s PerspectiveBOX 32-2
As a medic tending the wounded, I saw the ravages of World War II up close. One day I was treating three or four wound-ed men in a trench when an enemy mortar shell scored a direct hit. My right leg was gone; my left leg and arm were shredded by shrapnel, which also tore through my spine. If the shrapnel hadn’t seared the arteries in my legs, I would have bled to death then and there. My first thought was, “There go my dreams: college, a career in professional bas-ketball, marriage, everything I’d hoped for. I was right about basketball but wrong about everything else.”
The first year at home was the hardest, like a dark tun-nel, wondering what the future had in store, wanting to be as independent as possible—so much to learn. Fortunately, I had nurses and therapists who took time to get to know me before prescribing just how I should achieve maximum independence. They listened. They understood my disabil-ity and the limits it imposed. They tried to get me to do as much as possible for myself but didn’t push me too hard or too fast. You need to go at your own speed in learning about assisted living. Each person is different. I’m living proof that with the right care and therapy, the body can rebuild itself marvelously.
The beautiful black-haired girl I was engaged to still wanted to marry me, disabilities and all. We’ve been together 53 years now. She’s the greatest thing that ever happened
to me. With her love and support, I completed a 2-year busi-ness college course in accounting and worked as an accoun-tant for a trucking company until 1948, when the poor circu-lation in my legs and my spinal problems made it impossible to work at a desk job.
From day one, the VA (Veterans Administration) system has done wonders for me, both in the hospital and out. Whatever I needed for assisted living—wheelchairs, pros-thetic legs—they’ve provided. With the support of the VA, I designed my own house with everything on one level and totally accessible. The sidewalks are 48 inches wide so I can go outside, work in the garden, or do projects in my wood-working shop. I’ve made furniture, cabinets—you name it, I’ve made it.
Fifty years with a disability have taught me a lot. Probably the most important lesson is that attitude is everything. How you perceive and respond to your situation has a tremen-dous influence on your life—your physical, emotional, and spiritual well-being.
I’ve had a wonderful life: marriage to the woman I love, two sons, eight grandchildren, and, just last week, our first great-grandson. Because I’ve been so blessed, I enjoy giving to others, especially people who are just learning to live with disabilities. Until 2 years ago, I did chaplaincy work in nursing homes and hospitals.

UNIT VII I • Act iv i ty–Exercise Pattern840
In the case study, Mrs. Lasauskas had been living independently in an assisted living residence. Why might you expect her to be confused immediately after surgery? Did surgery cause her confusion?
FOCUSED ASSESSMENT FOR ACTIVITY INTOLERANCEActivity intolerance results when a client has insufficient physiological or psychological energy to endure or com-plete a desired activity. It is evidenced when the client reports fatigue, weakness, or dizziness, experiences ab-normal vital signs or electrocardiographic (ECG) changes, or has exertional discomfort or dys pnea during or after the activity. If a client has Activity intolerance, health care professionals tend to document that the client did not “tolerate” the activity. If the client was able to tolerate the activity without the fatigue or abnormal vital signs or ECG changes, the documentation may be summarized as “tolerated well.”
Action Aler t! The term tolerated well is a vague judgment. Use a more specific description, such as “walked 50 feet without changes in vital signs, shortness of breath, fatigue, or weakness.” This provides a clear benchmark against which to compare future activity.
Defining Characteristics. Before asking clients to per-form any activity, question whether they are tired or weak. Fatigue or weakness can have a number of causes, including pain, hyp oxia, fluid and electrolyte imbal-ances, and decreased muscle tone and strength. During
the activity, major defining characteristics are dizziness or increased fatigue or weakness; discontinue the activity if necessary. At 3 minutes after an activity, defining char-acteristics are dizziness, dys pnea, exertional fatigue, res-pirations greater than 24 per minute, and pulse greater than 95 beats per minute (Carpenito-Moyet, 2006).
Some clients with coronary artery disease or respira-tory disease are particularly likely to experience changes in heart rate or electrocardiogram recording during ADLs or after a physical therapy plan of care. Other signs of concern would be confusion and pallor or cyanosis.
Clients experiencing pain may have increased discom-fort during activity. Evaluate the change in the client’s pain level, and discontinue the activity if indicated. Clients with respiratory or coronary artery disease may experience exertional dys pnea during activity. Assess the client before, during, and after the activity for changes in breathing pattern or rate.
Related Factors. Prolonged immobility due to chronic disease or severe injury leads to generalized weakness and subsequent Activity intolerance. These clients need to be out of bed and moved as much as possible. Assess changes in muscle tone and joint ROM.
All body tissues require oxygen. When an oxygen defi-cit occurs or the demand for oxygen exceeds available oxygen, fatigue develops and vital signs change. If the oxygen deficit is severe, ECG changes can occur. For clients with cardiovascular or respiratory problems, use a pulse oximeter to check for oxygen saturation before, during, and after activity. Arterial blood gases provide additional information about oxygenation (see Chapter 34).
Assessing Physical Mobility of Older Adults
Problem: Physical mobility is primarily dependent upon physi-cal strength and endurance, cognitive abilities and motiva-tion, illness, and environment. Sometimes older adults may not have the ability to be physically independent because of alterations in any of these factors. The nurse needs to know how to provide safe, effective, comprehensive care to older clients with deficits affecting alterations in mobility.
EvidenceThe guideline Assessment of function: Of critical importance to acute care of older adults was developed for nurses by a group of nursing experts from across the country as part of the Nurses Improving Care for Health System Elders (NICHE) project, under sponsorship of The John A. Hartford Foundation Institute for Geriatric Nursing. The method used to collect or select evidence was by searches of Medline, an electronic database. Thirty-seven source documents were used. The method used to assess the quality and strength of the evidence was by expert consensus.
Application to PracticeThe objectives of the guideline were the following:• To identify physical functioning as an important clinical
indicator of health/illness, response to treatment, and need for services
• To describe common components of standardized func-tional assessment instruments
• To identify unique challenges to gathering information from older adults regarding functional assessments
• To assist bedside nurses in monitoring function in elders, preventing decline, and maintaining the function of elders during acute hospitalizationThe guideline can be found at http://www.guideline.gov/
summary/summary.aspx?ss�15&doc_id�3504&nbr�2730.
ReferenceKresevic, D. M., & Mezey, M. (2003). Assessment of func-
tion. In M. Mezey, T. Fulmer, I. Abraham, & D. A. Zwicker (Eds.). Geriatric nursing protocols for best practice (2nd ed., pp. 31-46). New York: Springer Publishing [18 references].
Evidence-Based PracticeBOX 32-3

C h a p t e r 32 Restoring Physical Mobility 841
DIAGNOSIS
IMPAIRED PHYSICAL MOBILITYAND ACTIVITY INTOLERANCEWhen caring for a client with musculoskeletal, neuro-muscular, or neurological problems, analyze the assess-ment data to identify which nursing diagnoses will guide your care. If clients are at risk for any of the diagnoses, add Risk for at the beginning of the diagnosis—for ex-ample, Risk for activity intolerance.
Also identify the related factors for actual nursing diagnoses and the risk factors for potential diagnoses. For example, clients with back injury have Pain related to muscle spasms. But they may also be at Risk for im-paired physical mobility related to pain, depending on how severe the back injury is. The related factors or risk factors also aid in goal development and help guide nursing interventions.
RELATED DIAGNOSESClients with either Impaired physical mobility or Activity intolerance often have additional nursing diagnoses. Assess the client comprehensively.
Clients who cannot bathe, dress, groom, toilet, or feed themselves will have Self-care deficit in one or more functional areas. Clients experiencing neurological, neu-romuscular, or musculoskeletal health problems are of-ten unable to move and therefore cannot perform ADLs independently. Perform functional assessments periodi-cally to determine clients’ progress in achieving indepen-dence, if possible. Do your best to consider each client’s situation with an open mind, no matter how difficult the circumstances.
Immobile clients are at a high risk for pressure ul-cers, especially over bony prominences, and the nurs-ing diagnosis Risk for impaired skin integrity may apply. Thin, emaciated, and poorly nourished clients are at the highest risk of any group. Assess the skin for red-dened areas. Assess nutritional status, especially labo-ratory indicators such as serum albumin, prealbumin, and transferrin. When these indicators are decreased, the client has inadequate protein stores to prevent or heal tissue breakdown.
Mrs. Lasauskas is a petite woman, weighing 102 pounds. What preventive measures should you use to help prevent skin breakdown after her surgery?
Exercise, hydration, and fiber are necessary to prevent Constipation. Clients who are immobile cannot exercise and often have an inadequate intake of food and water. Assess intake, especially intake of dietary fiber and flu-ids. Older adult clients are particularly prone to de-creased peristalsis and constipation. Monitor bowel habits and the consistency of stools.
The inactive client is at risk for deterioration of all body systems, sometimes referred to as disuse syn-drome or complications of immobility. For these cli-ents, the diagnosis Risk for disuse syndrome may apply. Assess every body system for possible complications or risk of complications. Chapter 33 discusses disuse syn-drome in detail.
The client with osteoporosis may have Risk for injuryfrom falls and fractures. Anemia often contributes to the risk. In addition, the client is at risk for thromboembolic complications.
As described earlier, clients with musculoskeletal trauma or conditions that increase peripheral compart-ment pressure are at high risk for neurovascular compro-mise, and the nursing diagnosis Risk for peripheral neuro-vascular dysfunction may apply. Monitor clients frequently for this potentially serious complication.
Musculoskeletal injury, surgery, or disease can be very painful, so you will need to assess for acute pain in a cli-ent with an injury, such as a fracture, or surgical repair of an injury. For these clients, the nursing diagnosis Acute pain may apply. Clients with chronic joint diseases such as degenerative or rheumatoid arthritis experience chronic pain, which is often difficult to control. For these clients, the diagnosis Chronic pain may apply.
Clients who have chronic musculoskeletal, neuro-muscular, or neurological health problems may feel hopeless when they are unable to move or care for themselves. They depend on others for care and often feel that they are a burden to their families and sig-nificant others. This sense of hopelessness can result in clinical depression or suicide. Assess the client’s response to illness, and identify clients at risk for Hopelessness.
Table 32-5 shows examples of clustering data to arrive at appropriate nursing diagnoses.
PLANNINGOnce the nursing diagnoses have been determined, think about what client outcomes can be expected. To the extent possible, outcomes should be individual-ized, measurable, and realistic. For the client with Impaired physical mobility, the overall goal is to improve mobility and prevent complications of immobility. For the client who has Activity intolerance, the goal is to improve endurance and tolerance to activities.
EXPECTED OUTCOMES FOR THE CLIENT WITH IMPAIRED PHYSICAL MOBILITYImprovement in mobility depends on several factors. First, try to determine whether the mobility deficit is permanent or temporary. A severed spinal cord results in permanent paralysis below the level of injury. Therefore expecting the client to walk is not likely. However, ex-pecting the client to be able to move about in a wheel-

UNIT VII I • Act iv i ty–Exercise Pattern842
Mobility Problems
DATA CLUSTER DIAGNOSIS
An older adult woman who fell, resulting in a fractured hip; history of previous stroke with hemiparesis; cries out when moved; degenerative arthritis in both knees
Impaired physical mobility related to muscle weak-ness, severe pain, and joint degeneration
A 12-year-old girl with rheumatoid arthritis; uses a walker to ambulate short distances but relies on wheelchair most of the time; becomes very fatigued when walking; takes two to three naps each day
Activity intolerance related to generalized weakness and fatigue
An older adult woman with acute vertebral compression fractures; complains of severe pain when moved; heart rate 120 beats per minute and weak; blood pressure 180/90 mm Hg
Acute pain related to muscle spasm and nerve impairment
A 53-year-old woman, first day after total abdominal hysterectomy; requires morphine for pain control; blood pressure low for her
Activity intolerance related to pain after surgery and cardiovascular instability
chair may be very realistic. The client with a total knee replacement is expected to walk with a walker or cane within a few days after surgery. This client’s physical mo-bility impairment is temporary.
Second, look at the causes or related factors that could be managed or resolved. For example, if the client can-not move because of pain and discomfort, then interven-tions directed at pain relief should improve physical mobility.
Third, assess the client’s willingness to participate in the treatment plan. If exercises are expected to increase muscle strength and endurance, the client must be will-ing and able to exercise as prescribed.
The outcomes that might be expected for the client with a permanent impairment in mobility may include the following:• Moves independently in a wheelchair• Transfers independently from the bed to chair and
vice versa using a sliding board• Performs ADLs independently using assistive or
adaptive devices• Maintains intact skin, especially over bony
prominences• Drinks at least 2000 mL of fluid daily to prevent
constipation and renal or urinary calculi• Demonstrates passive and active ROM exercise
techniquesPossible expected outcomes for a client with a tempo-
rary or less severe impairment in mobility may include the following:• Ambulates independently in home using a walker,
crutches, or cane• Maintains optimal joint function• Performs ADLs independently• States that pain is reduced or relieved
Each long-term outcome can be broken into progres-sive stages. For example, for the postoperative client with a total knee replacement, a realistic intermediate out-come is to walk in the hospital room using a walker. By
discharge from the rehabilitation program several weeks later, the client is expected to walk up and down stairs using the walker or cane.
EXPECTED OUTCOMES FOR THE CLIENT WITH ACTIVITY INTOLERANCEThe major expected outcome for Activity intolerance is that the client tolerates activity without evidence of diz-ziness, fatigue or weakness, abnormal vital signs, ECG changes, or exertional discomfort or dys pnea.
INTERVENTIONInterventions to promote mobility and improve activity intolerance are interrelated. Mobility skills cannot im-prove unless the client can tolerate the interventions that are directed toward building tolerance. Therefore inter-ventions for Activity intolerance are discussed first.
You will collaborate with members of the interdisci-plinary team, including rehabilitation nurses, physical therapists (PTs), occupational therapists (OTs), and physicians, when planning and implementing these interventions. The rehabilitation team is discussed in Chapter 44. Regardless of whether your client is being treated by rehabilitation services, you must still carry out interventions that help the client achieve the ex-pected outcomes.
INTERVENTIONS TO IMPROVE ACTIVITY TOLERANCEInterventions for improving activity tolerance center around building muscle mass and strength while man-aging other causes of activity intolerance, such as pain and discomfort.
Building Muscle Mass and Strength. A structured, consis-tent exercise program is started as soon as the client is medically stable. Several types of exercise may be used to build muscle mass and strength, including isometric, isotonic, and isokinetic exercises.
Table 32-5 Clustering Data to Make a Nursing Diagnosis

C h a p t e r 32 Restoring Physical Mobility 843
Isometric exercise (Figure 32-6, A) is a form of active exercise that increases muscle tension by applying pres-sure against stable resistance. Isometric contractions can be accomplished by opposing different muscles in the same person. There is no joint movement and the length of the muscle remains unchanged, but the tone and strength are maintained or increased. They are also called static or setting exercises. Ask the client to tighten certain muscle groups without moving the adjacent joints. These exercises are particularly helpful for strength-ening leg, hip, and abdominal muscles. Clients who have lower extremity musculoskeletal surgery, such as hip and knee replacements, are taught how to do “quad setting” exercises. Ask the client to tighten the quadri-ceps muscles and hold for a few seconds. Then repeat this exercise about 10 times in a set at least twice a day.
Isometric exercises also may increase heart rate and cardiac workload, especially if clients tense the entire body and close the glottis (increasing intrathoracic pres-sure) during muscle-setting exercises. Supervise clients with cardiac or vascular disease to ensure that they breathe during these exercises; also be aware that blood flow to other parts of the body is not increased with these exer-cises. In addition, these exercises are not helpful in pre-venting contractures because joints do not move.
Isotonic exercise (Figure 32-6, B) is a form of active exercise in which the muscle contracts and moves. There is no significant change in the resistance, so the force of the contraction remains constant. Isotonic exercise has the advantage of increasing cardiopulmonary function and blood flow, preventing contractures, and building muscle mass and strength. These dynamic exercises in-volve muscle contraction and muscle shortening. Examples of isotonic exercises performed in a hospital are straight leg raises after hip or knee surgery. Swimming, walking, and cycling are examples of isotonic exercises that the cli-ent can do independently to continue the physical condi-tioning of muscles. These exercises are sometimes referred to as isokinetic (Figure 32-6, C) because they are dynamic exercises performed at a constant velocity.
Mobilizing the Client Progressively. When a client expe-riences an acute musculoskeletal or neurological health problem, recovery may be gradual. Being confined to bed for more than a day can cause generalized weakness. Anesthesia during surgery also causes weakness and fa-tigue, sometimes for several weeks after surgery. Infections and other illnesses also deplete the client’s energy.
Therefore you will want to slowly build the client’s activity tolerance level. For instance, before a client gets out of bed for the first time, raise the head of bed slowly and have him or her sit on the side of the bed with legs dangling. The client may be able to tolerate only this simple activity the first time. Once the client tolerates dangling, help the client transfer from bed to chair. Each time the client gets out of bed, increase the activity, so that eventually the client can walk a few steps.
Action Aler t! Monitor the client for vital sign changes, fa-tigue, and exertional discomfort or dys pnea before, during, and after each activity. If the client’s heart is monitored, look for ECG changes. Discontinue the activity immediately if any of these changes occur, and notify the physician.
Controlling Pain and Discomfort. If pain occurs before, during, or after an activity, the client may be reluctant to increase the activity level or even perform the same activity again. Before the client gets out of bed or goes for therapy, administer pain medication or provide other appropriate pain-relief measures. Check with your physical therapy department, however, because heavy sedation could pre-vent client participation in the treatment plan. In some instances, physical therapists do not want clients to have medication because pain is used as an indicator that the client needs to discontinue treatment for that session.
Isometric
Isotonic
Isokinetic
FIGURE 32-6 Three types of exercise: A, Isometric. B, Isotonic. C, Isokinetic.
A
B
C

UNIT VII I • Act iv i ty–Exercise Pattern844
INTERVENTIONS TO PROMOTE MOBILITYYou and the therapist are responsible for promoting mo-bility, including ADLs. The goal is that the client will be as independent as possible by hospital discharge. Maintaining or improving joint mobility helps with transfer and ambulation skills. Alternative methods for promoting mobility are available to those who can make use of them, as outlined in Box 32-4.
Maintaining Joint Mobility. Range-of-motion exercisesinclude any body action (active or passive) involving the muscles, joints, and natural directional movements, such as abduction, extension, flexion, pronation, and rotation. They are the most important interventions to promote and maintain joint mobility. ROM exercises are isotonic exer-cises in which the client or health care provider moves each synovial joint through its complete range of motion (see Table 32-2). When the client can perform the exer-cises, they are termed active. When you or the physical therapist performs the exercises on the client’s joints, they are termed passive. These exercises also prevent contrac-tures and help build activity tolerance.
If the clients can move, teach them how to perform active ROM exercises. They can move each joint through its range of motion several times a day independently. If they cannot move or exercise their own joints, perform passive ROM exercises for each joint as described in
Procedure 32-1. If the clients can assist you, the ROM exercises are called active-assistive.
Action Aler t! Follow these safety guidelines when putting a joint through its range of motion:• Position the bed at an appropriate height to maintain good
body mechanics.• Support the limb being moved, above and below the joint.• Do not force the joint into any position.• Move the body part smoothly and slowly, observing the client
for discomfort and listening for crepitus.
Assisting With Movement. If clients are strong enough, teach them how to get out of bed independently, as de-scribed in Box 32-5. Otherwise you will need to provide assistance. When assisting clients, be sure to use appro-priate assistive devices to prevent musculoskeletal injury to yourself, those assisting you, or the client.
Transferring the Client. If clients cannot transfer inde-pendently, you will need to assist them. Always remem-ber to use good body mechanics and use a lateral trans-fer or lift device. At least two people are needed to move a client who cannot help with the transfer. Also, if the client is obese or has multiple pieces of equipment, seek extra help.
Transferring From Bed to Chair. A client may need assistance transferring from the bed to a regular chair, wheelchair, or bedside commode. Transfer belts pro-
Alternatives for Restoring Physical Mobility
Considering the AlternativesBOX 32-4
Duval, C., Lafontaine, D., Hebert, J., Leroux, A., Panisset, M., & Boucher, J. P. (2002). The effect of Trager therapy on the level of evoked stretch responses in patients with Parkinson’s disease and rigidity. Journal of Manipulative and Physiological Therapeutics, 25(7), 455-464.Friedrich, M., Gittler, G., Arendasy, M., & Friedrich, K. M. (2005). Long-term effect of a combined exercise and motivational program on the level of disability of patients with chronic low back pain. Spine, 30(9), 995-1000.Yeh, S. H., Chuang, H., Lin, W. L., Hsiao, C. Y., & Eng, H. L. (2006). Regular tai chi chuan exercise enhances functional mobility and CD4CD25 regulatory T cells. British Journal of Sports Medicine, 40(3), 239-243.
DisadvantagesDoes not include strengthening of muscles because it is not
an exerciseMay delay traditional therapySome people may not want to be touched
Exercise Plus MotivationAdvantagesTwice the improvement in disability scores as exercise alone
(Friedrich, Gitler, Arendasy, & Friedrich, 2005)Fewer side effects than medicationsInvolves clients directly in their recoveryDisadvantagesRequires additional effort by practitionersMay postpone traditional therapiesRequires active participation by clients
Tai ChiTai chi is a system of postures linked by elegant and graceful movements, whose purpose is to balance energies within the body.AdvantagesEnhances functional mobility and regulatory T-cell function
(Yeh, Chuang, Lin, Hsiao, & Eng, 2006)As an exercise, has side benefit of improving depressionPotential cardiovascular benefit because it is a form of
exerciseDisadvantagesMay require weeks to see benefitsRequires instruction to beginMay delay traditional therapy
Trager TherapyTrager is a type of massage that uses gentle rocking motions.AdvantagesMay be perceived as less stressful by client than exerciseInhibits the evoked stretch responses, allowing increased
mobility (Duval et al., 2002)Can be performed on clients who cannot move themselves

Range-of-motion (ROM) exercises maintain joint flexi-bility and movement when the client is unable to move or is confined to bed. They also stimulate circulation and relax the body. ROM exercises may be full, which includes all the joints, or for selected joints. ROM will
PERFORMING RANGE-OF-MOTION EXERCISES
PROC E DU RE 32-1
TIME TO ALLOW: NOVICE: 15-30 min. EXPERT: 15-30 min.
not maintain or improve strength. You need to be famil-iar with the normal range of motion for each joint. Complications could include pain or joint injury if done too vigorously.
1 Perform preliminary actions (see inside front cover).2 Explain the procedure to the client, and assess the client’s ability to assist with the exercises. If the client can assist or can perform the exercises independently, active-assistive or active ROM can be performed rather than passive ROM.3 If moving the joints of the entire body through their ROM, use a head-to-toe approach (see Table 32-2). Thisapproach helps to organize the intervention so that all joints are moved through their range of motion.4 Support the client’s body part by cradling or cupping above and below the joint being moved (see illustra-tion). Supporting the joint prevents injury and stress on the joint and also promotes client comfort.
5 Put the joint through its complete ROM, but do not force it beyond where it will move comfortably. CompleteROM of each joint is beneficial in preventing contractures, maintaining joint flexibility, and building muscle tone.6 Throughout the exercises, observe the client for toler-ance, including pulse rate and discomfort, if any. Do not exercise to the point of producing pain. If the client can-not tolerate the exercises, discontinue them immediately.
HINTS
Use slow, smooth movements. Move joint only to the point where you feel resistance. Stop if you reach the point of pain. Assess for fatigue. Finish with the joint in good alignment. Check physician’s instructions about the number of sets and repetitions. A typical protocol is four sets daily, with five repetitions for each joint.
PEDIATRIC CONSIDERATIONS
Explain the procedure to the child using age-appropri-ate language. Teach ROM exercises to caregivers as part of the routine care for a client who has mobility limitations.
GERIATRIC CONSIDERATIONS
Use caution when performing ROM exercises in older adults to avoid injury. Do not exercise past the point of resistance.
HOME HEALTH CARE CONSIDERATIONS
ROM exercises should be taught to family caregivers as part of the routine care for a client who has mobility limitations. The family may need help to make ROM part of all activities rather than trying to make room in a crowded schedule for several ROM sessions.
DELEGATION GUIDELINES
Following assessment of your client’s functional status and joint mobility, you may delegate the performance of ROM exercises to a nursing assistant who has received special training in the performance of this skill. Provide special instructions outlining those observations and findings that should be reported to you immediately.
EQUIPMENT NEEDED
◗ Bath blanket to cover the body other than the part being exercised
◗ Pillows for positioning
Step 4. Supporting the body part above and below the joint being moved.
C h a p t e r 32 Restoring Physical Mobility 845

UNIT VII I • Act iv i ty–Exercise Pattern846
The physician wants Mrs. Lasauskas out of bed in a chair on the first full postoperative day. Given her weakness, hemiparesis, and pain, what transfer tech-nique would you use? How many people should be
used to transfer her?
Newer types of lift devices include ceiling-mounted lifts and floor-based air lifts (Nelson et al., 2004). Ceiling mounted lifts increase available floor space during the transfer and allow nurses easier access to the client. Air lifts use separately inflated air chambers to lift a client from the floor to bed or stretcher, such as after a fall.
vide extra security during a transfer. Procedure 32-2 describes how to help a client from a bed to a chair with or without a transfer belt. This procedure assumes that the client is strong enough to help you with the transfer.
For clients who are totally immobile and unable to assist with the transfer, use a mechanical lift device, as seen in Procedure 32-3. The sling used in the lift remains under the client at all times. Position the client in the chair in proper alignment using pillows and bath blan-kets for support. Be sure that the client’s feet are sup-ported by the footrest and that all necessary items are within reach, including the call light.
You can help a client get out of bed with or without a transfer belt. A transfer belt is a woven canvas belt about 21⁄2 to 3 inches wide and 6 feet long. It is fastened around the client’s waist and secured with a locking
HELPING A CLIENT GET OUT OF BEDNursing Skills Online: Safety, Lesson 3
PROC E DU RE 32-2
TIME TO ALLOW: NOVICE: 15 min. EXPERT: 10 min.
device. The belt is used to maintain control of clients when you help them stand, transfer to a chair, or walk. Transferring with a belt is safer and avoids pulling on the arm and shoulder joints.
DELEGATION GUIDELINES
Once you have assessed that the client can stand safely, you may delegate assistance with bed-to-chair transfer to the nursing assistant. The nursing assistant should receive specific instruction in body mechanics and safety concerns related to client mobility. Instruct the nursing assistant to report to you any client complaints
of dizziness and any observation of unsteady gait or imbalance.
EQUIPMENT NEEDED
◗ Transfer belt◗ Supportive shoes with rubber soles◗ A bathrobe
Getting Out of Bed Independently
Purpose: To promote client independence in transfer skills, which has the added benefits of increasing mobility, main-taining muscle tone and endurance, and increasing self-esteem.Expected Outcome: The client will transfer from bed to chair independently.
Client Instructions• If you have an electric bed, put the bed in its lowest position.• Raise the head of the bed if needed to decrease the dis-
tance to a sitting position.• Turn onto your side. (If you are stronger on one side than
the other, turn toward the stronger side.)
Teaching for Self-CareBOX 32-5
• Push against the mattress with either your elbows or hands to raise your upper body off the bed.
• Once you are in a sitting position, let your legs dangle for a moment over the side of the bed. This will help you get your balance and make sure you are not dizzy.
• If you are not dizzy, go ahead and stand up.Hint: If the client is too weak to push up from the bed,
set up an overhead frame and trapeze for the client to pull on. Clients with lower-extremity trauma or surgery, including amputations, especially benefit from this device.

C h a p t e r 32 Restoring Physical Mobility 847
WITHOUT A TRANSFER BELT
1 Perform preliminary actions (see inside front cover).2 Place the bed in its lowest position, and raise the head of the bed. Having the bed in the lowest position is safest in case the client falls. The client can sit up more easily if the head of the bed is up.3 Place a chair or wheelchair at a 45-degree angle to the bed. Plan for the client to get out of bed on the stronger side. Having the client get out of bed on the strong side helps prevent loss of balance and possible falls.4 Using good body mechanics, help the client to a full sitting position while swinging the client’s legs over the edge of the bed in a single, smooth motion (see illustra-tion). Support the upper body as the client comes to the sitting position. Moving the client’s legs reduces friction or shearing from the sheets while increasing the force of the movement. Supporting the upper body keeps the client from falling backward.
6 If the client is able, have the client place his or her hands on your shoulders or on the mattress on either side of the body. When you help the client stand, the client can assist you by balancing against your shoulders while using the leg muscles to stand or by pushing off the mattress with the hands.7 Place your hands under the client’s arms. Place your knees in front of the client’s knees, and help the client rise to a standing position (see illustration). Keeping your knees against the client’s knees prevents them from buckling, thus reducing the risk of a fall. Avoid axillary pressure.
Step 4. Assisting the client to a full sitting position.
5 Support the client in a sitting position on the side of the bed with the feet dangling (see illustration). Movingfrom a lying to sitting position can cause postural hypotension, which can lead to dizziness and a subsequent fall unless the client has time to gather equilibrium.
Step 5. Supporting the client in a sitting position.
Step 7. Helping the client to a standing position.
8 Pivot with the client toward the chair or wheelchair, being careful not to dislodge equipment or lines (see il-lustration). Pivoting prevents twisting your spine and caus-ing injury.
Continued

9 Using good body mechanics, lower the client into the chair or wheelchair slowly and reposition the client in proper body alignment. Make the client as comfortable as possible. Moving slowly helps prevent dizziness or other discomfort.
WITH A TRANSFER BELT
1 Place a transfer/gait belt around the client’s waist (after completing steps 1 to 5 in the previous section). The transfer belt allows you to guide the client, and it offers support during the transfer.2 Standing in front of the client, grasp the transfer belt on both sides toward the client’s back (see illustration). Assess whether the client has the strength to stand. When the client is ready, help him or her to a standing position by rolling your body and arms upward, pulling the client with the transfer belt. Favoring the client’s weaker side helps prevent falls because most clients drift to-ward, or lose balance on, their weaker side.
3 Pivot the client toward the chair, and lower the client slowly into it. Ideally, the client will take two or three small steps to get into position to sit. Pivoting prevents twisting of your spine.4 Have the client reach for the armrests, if available, while lowering into the chair. Holding on to the armrests provides additional support for the client.
PEDIATRIC CONSIDERATIONS
Use age-appropriate explanations about the procedure. Include family in teaching whenever possible.
GERIATRIC CONSIDERATIONS
Proceed slowly to alleviate any fears related to the proce-dure. Explain the steps to the client as the procedure progresses.
HOME HEALTH CARE CONSIDERATIONS
Teach family caregivers how to use good body mechan-ics to prevent back injuries when transferring the cli-ent. Most caregivers can be easily taught how to use a transfer belt. If the family cannot transfer the client to a chair, they can rent a mechanical lift or a geriatric chair. The chair reclines, and the feet can be elevated. It also has a tray that fastens on the front for meals and other activities.
Step 8. Pivoting and turning the client toward the wheel-chair.
Step 2. Grasping the transfer belt to assist the client to a standing position.
UNIT VII I • Act iv i ty–Exercise Pattern848

A mechanical lift uses a hydraulic pump or electric motor to hoist a sling. With the sling around the client, the lift can raise the client off the bed, swing the client into position above a chair, and lower the client while he
USING A MECHANICAL LIFTPROC E DU RE
32-3TIME TO ALLOW: NOVICE: 20 min. EXPERT: 15 min.
or she is slowly rolled into the chair. Possible disadvan-tages are the insecurity clients may feel while suspended in air and the training required to properly use the lift.
1 Perform preliminary actions (see inside front cover).2 Obtain a functioning lift, and move it into the cli-ent’s room (see illustration). Lock both the bed and chair before beginning. Make sure that the lift works cor-rectly and safely to prevent accidents. Practice before you take it into the client’s room. Locking the bed and chair helps prevents accidents.
4 Place the bed in a low position. Securely attach the sling to the lift. Have the client cross the arms across the chest. Crossing the arms will help prevent injury caused by the client trying to help, thus causing instability of the lift.5 Raise the lift to elevate the client enough to clear the bed. If the client is not completely off the bed, shearing or friction of the skin can result. Promote the client’s security by moving slowly and avoiding erratic movements; protect the head if necessary.6 Move the lift until the client is aligned with the chair, lock the wheels, release the pressure valve, and lower the client slowly into the chair. Correct alignment with the chair prevents the client from falling or other injury.7 Keep the sling under the client, but position the cli-ent into comfortable and functional body alignment. The sling remains under the client until it is used again to return the client to bed. Disconnect the sling from the lift, and store the lift in a corner out of the way of traffic.
PEDIATRIC CONSIDERATIONS
This procedure may be unnecessary in very young and lightweight clients. Use age-appropriate explanations about the procedure. Include family in teaching when-ever possible.
GERIATRIC CONSIDERATIONS
Proceed slowly to alleviate any fears related to the lift procedure. Explain the steps to the client as the proce-dure progresses.
HOME HEALTH CARE CONSIDERATIONS
Teach family caregivers how to use the mechanical lift, and help them practice until they are proficient and feel secure before trying to move the client.
DELEGATION GUIDELINES
The use of a mechanical lift for client transfer may be delegated to a nursing assistant who has received train-ing in body mechanics, safety, and the use of this equip-ment. When reviewing the key aspects of this skill with your assistant, place special emphasis on the client’s per-ception of the experience of being suspended in the air and on protecting the skin from injury.
EQUIPMENT NEEDED
◗ Mechanical lift◗ Bedside chair or wheelchair◗ Bath blanket
Step 2. Mechanical lift. (Courtesy Vancare, Inc., Aurora, NE.)
3 Place the one- or two-piece sling under the client by turning the client onto the side, placing the sling along the back, and having the client roll onto the sling. Make sure the sling supports the shoulders and buttocks. Take care not to injure the client’s skin with the metal attachments. If the sling is not positioned correctly, the client will not feel secure and may slide out of the sling.
C h a p t e r 32 Restoring Physical Mobility 849

UNIT VII I • Act iv i ty–Exercise Pattern850
Transferring From Bed to Stretcher. Transferring a client from the bed to a stretcher requires at least two people and the use of a lateral transfer device to reduce the risk of harm to both client and health care person-nel (Baptiste, Boda, Nelson, Lloyd, & Lee, 2006; Pellino, Owen, Knapp, & Noack, 2006). Lateral trans-fer devices may be made of a rigid plastic, and the new-est ones can be filled with air. Both reduce friction and shear, increasing the safety of the procedure to client and health care personnel. If a lateral transfer device is not available, then you will need to use a turning sheet or drawsheet placed under the client. First, adjust the height of the client’s bed to be even with the height of the stretcher. Ensure that the wheels on both the bed and the stretcher are locked. Turn the client, and posi-tion the transfer device under the client’s sheet or turn-ing sheet. Pull the sheet to slide the client over the transfer device and onto the stretcher in unison. For air transfer devices, follow product literature. Place a pil-low under the client’s head, pull up the stretcher side rails, fasten the strap around the client, and push the stretcher from the head.
Supporting the Ambulating Client. Some clients cannot ambulate independently and require human or mechani-cal assistance. The transfer belt serves as the gait or walking belt that you can hold during ambulation. If the client is weaker on one side than the other, stand on the weaker side. The client can also push a portable intravenous pole and use it as an extra support if needed (Procedure 32-4).
If the client starts to fall or faint, support the client and ease him or her to the floor. Make the client as comfortable as possible, and stay with the client until help arrives.
Compensating for Physical Impairments. When human assistance is not available or the client is ready to learn to ambulate independently, assistive devices may be used. If available, a physical therapist will do the initial teaching, but you will need to reinforce the techniques
that were taught. Walkers, canes, crutches, and wheel-chairs allow independence in ambulation.
Using a Walker. Walkers provide better support than either a cane or crutches (Figure 32-7). They are used most often for older adults who have decreased muscle strength. The standard walker can be adjusted for the client’s height so that the hand bar is just below the client’s waist and the client’s elbows are slightly flexed. The standard walker is used for clients who can bear partial weight, and it must be picked up to be used correctly. Exercises to strengthen the arms are important. For clients who have insufficient arm strength, roller walkers with two or four wheels can be substituted. Some roller walkers have a seat where the cli-ent can sit when fatigued.
FIGURE 32-7 Client using a walker.
The first time a client gets out of bed after anesthesia, prolonged illness, or bed rest, assist with ambulation to ensure the client’s safety. It is better to be overly cautious by providing assistance than to risk a fall.
SUPPORTING THE AMBULATING CLIENTPROC E DU RE
32-4TIME TO ALLOW: NOVICE: 20 min. EXPERT: 10 min.
DELEGATION GUIDELINES
You may delegate assisting the client with ambulation after your initial assessment of the client’s functional status and the client’s risk factors for falling. The nursing assistant should receive training in body mechanics, safety, and assisting with mobility.
EQUIPMENT NEEDED
◗ Comfortable, supportive shoes with rubber soles◗ Bathrobe◗ Transfer/gait belt

Step 3. Standing at the client’s side while holding on to the back of the transfer belt.
Step 9. Supporting the client and easing her to the floor.
Continued
1 Perform preliminary actions (see inside front cover).2 Apply a gait belt (also called a transfer or walking belt) around the client’s waist, and help the client to a standing position as outlined in Procedure 32-2.3 Stand at the client’s side and slightly behind, and walk with the client while holding on to the back of the belt (see illustration). By holding on to the gait belt while the client is walking, you provide support for the client and you gain some control over ambulation. Grasp the belt from beneath the belt in a manner that will allow you to lift up if the client starts to fall. Your second hand may be used to guide the client’s posture to an upright position.
7 If the client starts to fall, do not try to prevent the fall by supporting the weight with your own body. Rather, help the client fall safely, without injury to either of you.8 As the client starts to fall, move your feet so your stronger leg is somewhat behind you. This action forms a solid base of support for you and allows you to bear most of the weight on your stronger leg.9 At the same time, use the transfer belt to pull the cli-ent toward you, allowing the client to slide against you, supported, as you ease him or her to the floor (see illus-tration).
4 The client with an intravenous pole can push the pole while walking. The client with an intravenous line will need a portable rolling pole. However, these poles roll freely and should be used to guide, not to support the client’s weight.5 If the client is weaker on one side than the other, walk on the weak side while grasping the belt and guid-ing the client’s posture. The client will tend to lean and could fall toward the weaker side. Remind the client to lean toward the strong side.6 If the client is especially weak or this is the first time ambulating, ask another person to walk with you to sup-port the client. If necessary, have another assistant follow with a wheelchair in case the client becomes too weak to stand. An additional person helps by supporting the client from the opposite side or by moving portable equipment that must go with the client.
10 Stay with the client until help arrives. Assess the cli-ent for injury before trying to move him or her (see il-lustration). Even a minor fall can result in a fractured hip for an older adult, especially one who has osteoporosis. Use an air or mechanical lift rather than having the client try to stand. Have the client evaluated by a physician.
Step 10. Staying with the client until help arrives.
11 Document the events leading up to the fall, your cli-ent assessment, notification of the physician, and any action taken.
C h a p t e r 32 Restoring Physical Mobility 851

UNIT VII I • Act iv i ty–Exercise Pattern852
When teaching a client how to use a walker, place a gait belt around the client and help him or her to a standing position. Tell the client to place both hands on the walker. If a client has severe arthritis in the hands, platforms for resting the arms can be used instead of handgrips. Teach the client to lift the walker and move it about 1 to 2 feet forward, depending on the client’s com-fort level and strength. While resting on the walker, ask the client to take one or two small steps and check bal-ance. Repeat this procedure while ambulating. You should grasp the gait belt until the client is strong enough to ambulate independently with the walker.
Using a Cane. A variety of canes are available for ambulation, depending on the amount of support the client needs. The quadripod (“quad”) and hemicane provide the most support (Figure 32-8). They are used most often for clients who have had strokes. The straight cane provides the least support. All canes should have rubber tips on the end to prevent slipping.
When teaching the client how to use a cane, again use a gait belt and help the client to a standing position. Have the client place the cane in the hand of the stronger side of the body. The length of the cane should permit the el-bow to be slightly flexed. Have the client move the cane forward about a foot and about 6 inches to the side, then move the weaker leg one step forward. Then have the cli-ent move the stronger leg forward and check the balance.
Like walkers, canes may be used on a temporary or a permanent basis. Some clients learn to ambulate using a walker and then progress to a series of canes as needed.
Using Crutches. For most clients, crutches are used as a temporary measure until they regain full mobility. However, for clients with permanent disability, they may be needed on a permanent basis. Axillary crutches are used most often when temporary support is needed. Lofstrand crutches are used most often for permanent needs (Figure 32-9). Before use, the client
PEDIATRIC CONSIDERATIONS
The client’s size determines the amount of assistance needed. Encourage family to participate as they are able and interested, but do not relinquish your responsibility for the client’s safety.
GERIATRIC CONSIDERATIONS
Recall that reaction times are slower in older adults, so proceed slowly and provide explanations about the procedure.
HOME HEALTH CARE CONSIDERATIONS
Help the family caregivers assess their home environ-ment for hazards, such as throw rugs, slick floors, or obstructed pathways, before getting the client out of bed to walk. A chair should be available that is sturdy, com-fortable, and easily accessible. A high-backed chair is preferable to support the client’s neck in anatomical alignment.
FIGURE 32-8 Client using a “quad” cane. FIGURE 32-9 Client using Lofstrand crutches.

C h a p t e r 32 Restoring Physical Mobility 853
should be measured carefully for adjustments to pre-vent axillary nerve damage or muscle strain. Each crutch end should have a rubber tip to prevent slipping.
Arm strength needs to be assessed. If needed, the cli-ent performs exercises to prepare for the demands of crutch walking. The basic crutch stance is called the tri-pod, or triangle, position. It provides a broad base of support. Several gaits can be used for ambulating, de-pending on the injury and the client’s weight-bearing status. The four-point gait provides the most support,
Crutches are usually used for clients with orthopedic injuries who are unable to bear weight on one or both legs. Using crutches properly requires good upper body
WALKING WITH CRUTCHESPROC E DU RE
32-5
TIME TO ALLOW: NOVICE: 20-30 min. EXPERT: 20-30 min.
strength and balance. Complications of improper use could include falls and reinjury.
1 Perform preliminary actions (see inside front cover).2 Inspect the prescribed crutch or crutches to make sure that the rubber tips are in place. Rubber tips prevent slipping and therefore promote safety.3 Reinforce the importance of arm exercises, such as flexing and extending the arms, body lifts, and squeezing a rubber ball. Arm muscles need to be toned to use crutches. Upper body strength is required.4 Check that crutches are the correct length (see illustration).a. First, have the client stand.b. Next, with the crutch tips and the client in the basic
crutch stance (tripod position), check the distance between the axilla and the top of the crutch. It should be at least three finger widths, or 1 to 2 inches (2.5 to 5 cm). If the crutches are not the correct length, the client could sustain axillary nerve damage.
DELEGATION GUIDELINES
The evaluation of the need for crutches and instruction in the use of crutches may not be delegated to a nursing assistant. Assessment and instruction for crutch walking are the domain of a licensed professional, such as you or a physical therapist. Once a client has been instructed and successfully demonstrates crutch walking, you may
assign or delegate a nursing assistant to accompany the client, much as you would do with ambulation.
EQUIPMENT NEEDED
◗ Crutches with rubber tips◗ Supportive shoes with rubber soles
6 in.
6 in.
3 finger widths(1-2 in., 2.5-5 cm)
30 degreesflexion
but it requires coordination to maneuver. The three-point gait requires that the client be able to bear full weight on the unaffected leg. The two-point gait is the quickest and requires at least partial weight-bearing abil-ity for both legs. Procedure 32-5 describes these gaits and how to manage stairs and sitting.
Swing-to or swing-through gaits are used for clients who are paralyzed in both legs. Teach the client to move both crutches ahead together by about 2 feet, then lift the body and swing to or past the crutches, whichever is most comfortable and balanced.
Step 4. Measuring crutch length.
Continued

5 Teach the client how to balance using the tripod (tri-angle) position by placing the crutches 6 inches (15 cm) in front of the feet and out laterally about the same dis-tance (see illustration). The tripod position provides a wide base of support and balance to prevent falls.
6 in. (15 cm)
6 in. (15 cm)
6 in. (15 cm)
Step 5. Basic crutch stance, tripod position.
6 Check with the physician or physical therapist to determine which gait the client needs: a four-point, three-point, or two-point gait. The type of injury and the client’s balance determine which gait will be recommended.a. For a four-point gait, have the client follow this series
of steps (see illustration): (1) Move the right crutch forward about 6 inches
(15 cm). (2) Move the left foot forward. (3) Move the left crutch forward. (4) Move the right foot forward.
Tripod position
1. Right crutch advances.
2. Left foot advances.
4. Right foot advances.
3. Left crutch advances.
Step 6a. Four-point gait.
UNIT VII I • Act iv i ty–Exercise Pattern854

b. For a three-point gait, have the client follow this se-ries of steps (see illustration):
(1) Move both crutches and the weaker leg for-ward.
(2) Move the stronger leg forward.
Tripod position
1. Both crutches and weaker leg advance.
2. Stronger leg advances.
Step 6b. Three-point gait.
c. For a two-point gait, have the client follow this series of steps (see illustration):
(1) Move the left crutch and the right foot forward at the same time.
(2) Move the right crutch and the left foot forward at the same time.
Tripod position
1. Left crutch and right foot advance
2. Right crutch and left foot advance
Step 6c. Two-point gait.
Continued
C h a p t e r 32 Restoring Physical Mobility 855

7 Teach the client how to ascend stairs:a. Step up first with your stronger leg (see illustration).
b. Shift your weight to the crutches, and move the strong leg onto that step.
c. Repeat these steps until the stairs are negotiated. The crutches always support the weaker or affected leg.
9 Teach the client how to get in and out of a chair. Thefollowing technique supports the weaker leg and provides the best balance for the client:a. Stand with the chair behind you, making sure that
the back of your stronger leg is against the chair.b. Transfer your crutches to your weaker side, and hold
them by the hand bar.c. Grasp the arm of the chair with the hand on your
strong side, then lean forward and flex your hips and knees while lowering yourself into the chair.
d. To get out of the chair, move to the edge of the chair and position the stronger foot to support your weight when arising.
e. Hold both crutches by the hand bar, using the hand on your weaker side. Hold the arm of the chair with the hand on your stronger side.
f. Push down on the crutches and the armrest to push yourself out of the chair.
PEDIATRIC CONSIDERATIONS
Use age-appropriate explanations when teaching this skill to children. Ensure that crutches are fitted properly to prevent nerve plexus injury. Teach client and family safety measures, such as not using crutches on wet or slippery floors.
GERIATRIC CONSIDERATIONS
Assess the older adult for musculoskeletal ability to use crutches. Ensure that crutches are fitted properly. Provide teaching about maintaining safety. Older adults may need additional teaching time to master new tech-niques.
HOME HEALTH CARE CONSIDERATIONS
Help the client do a safety check of the home environ-ment for slippery floors, loose throw rugs, or obstruc-tions in walkways. If the client will need to use stairs, it is preferable to have a handrail.
Step 7a. Stepping up first with the stronger leg.
b. Shift your weight to the strong leg, and move the crutches and weaker leg onto the same step.
c. Repeat these steps until the stairs are negotiated. The crutches always support the weaker or affected leg.
8 Teach the client how to descend stairs:a. Shift your weight to the stronger leg, and move the
crutches and the weaker leg onto the lower step (see illustration).
Step 8a. Stepping down first with the weaker leg.
UNIT VII I • Act iv i ty–Exercise Pattern856

C h a p t e r 32 Restoring Physical Mobility 857
In our case study, Mrs. Lasauskas required rehabilita-tion for her fractured hip repair. By the fifth postop-erative day, she was discharged to the hospital’s tran-sitional care unit (TCU). She was able to transfer from
her bed to a chair and walk about 15 feet using a walker. Beyond that distance, she became dyspneic and tired. The plan for her continued rehabilitation in the TCU is to increase her ambulation distance and continue to build her tolerance for activity so that she can return to her assisted living apartment.
In this example, the client has progressed slowly but can ambulate with a walker independently for a short distance. The intermediate expected outcomes were met, but the long-term outcomes still need to be achieved before she can be discharged back into the community. Box 32-6 illustrates Mrs. Lasauskas’s care after surgery, when she is ready to get out of bed for the first time. When she is discharged to the rehabilitation setting, the nurse writes the following note:
SAMPLE DOCUMENTATION FOR MRS. LASAUSKAS
Discharged to Meridian Rehabilitation per stretcher. Trans-portation provided by a van from Elderly Assistance, Inc. Vital signs stable. Pain controlled with Vicodin given 30 minutes be-fore getting out of bed. Can feed self and dress with assistance. Physical therapy reports she is ready to begin walking a few steps with a walker. Report called to Meridian.
Using a Wheelchair. For some clients, walking is no longer possible. Clients with complete spinal cord inju-ries, advanced multiple sclerosis, cerebral palsy, or mus-cular dystrophy are often confined to a wheelchair. These clients ambulate in their wheelchairs using their arms or other part of the body to propel the chair. Some use electric wheelchairs that can be advanced by a hand control or with a slight head movement.
Clients who are confined to wheelchairs are at risk for skin breakdown and other complications of immobility previously described. Teach the client and family or sig-nificant others to inspect skin every day, and have the client perform wheelchair pushups if possible to de-crease pressure on the ischial tuberosities. Pushups also build arm strength, which is essential for propelling a manual wheelchair.
As a result of the federal Americans With Disabilities Act, all public places are wheelchair accessible. Ramps, handicapped toilets, and designated parking spaces have allowed wheelchair-bound people access to places they were previously not able to visit.
EVALUATIONEvaluation involves determining whether expected out-comes have been met. If they have not been met, the plan may need modification.
Continued
BOX 31-12 A Client With a Fractured Hip
Admission DataMrs. Kristina Lasauskas is an 80-year-old woman admitted for a fractured left hip. She was taken from the emergency department to the operating room, where she had an open reduction and internal fixation. She was in the recovery room 3 hours and has been admitted to an orthopedic nursing unit.
Physician’s OrdersD5
1⁄2NS @ 75 mL/hrUp in a chair tid as tolerated starting in AMROM four times dailyLaxative of choiceLovenox 30 mg subcutaneous q12hRegular diet, encourage fluidsPlan for discharge to a rehabilitation unit
Nursing AssessmentIt is now the morning after her surgery. You receive the fol-lowing report: Mrs. Lasauskas is 1 day post an open reduc-tion and internal fixation of a fractured left hip. Her vital signs are stable. She is awake, alert, and oriented � 3. Lungs clear. Bowel sounds hypoactive. IV site patent and free of inflammation. She has right-sided weakness from a previous cerebrovascular accident but was able to walk with a cane. She is to be up in a chair today, and physical therapy will start ROM. She is depressed because she believes she will never walk again.
Nursing Care PlanBOX 32-6
NANDA-I Nursing Diagnosis
NOC Expected Outcomes With Indicators
NIC Interventions With Selected Activities Evaluation Data
Impaired Physical Mobility Joint Movement Exercise PromotionData Gathered at Dischargeto Rehabilitation Setting
Related Factor:• Right-sided weakness
and healing fracture of left hip
• Active• Transfer performance
• Strength training• Joint mobility.

UNIT VII I • Act iv i ty–Exercise Pattern858
BOX 31-12 A Client With a Fractured Hip
Nursing Care Plan—cont’dBOX 32 -6
NANDA-I Nursing Diagnosis
NOC Expected Outcomes With Indicators
NIC Interventions With Selected Activities Evaluation Data
Impaired Physical Mobility Joint Movement Exercise PromotionData Gathered at Discharge to Rehabilitation Setting
The Client Will• Maintain full ROM• Increase upper body
strength• Transfer from bed to chair
with assistance• Sit in a chair without
fatigue or change in vital signs
• Perform resistance exer-cises to right leg and ROM to left leg
• Stand at bedside with par-tial weight bearing to left hip
• Full active/passive ROM by physical therapy 0800, 1300 and by nursing 1700, 2100.
• Use client’s history of self-determination to motivate.
• Use 3-pound weights to exercise arms during ROM.
• Have great-grandchildren bring colored weights and make a game of exercising.
• Pivot to chair 1000, 1500, 1900.
• Sit in chair as tolerated, increasing to 30 min.
• Use light resistance for ROM to right leg.
• Has full ROM in upper extremities.
• Can perform active ROM.• Performs active ROM on right
leg.• Straight leg raising to a
30-degree angle.• Can raise left leg by bending
knee to 30-degree hip flexion.• Exercises arms with 3-pound
weights.• Tolerates flexion at elbow.
Raising weight over her head tires right arm.
• Can stand and pivot to chair with assistance.
• Can raise right leg against light resistance of nurse’s hand on knee.
• Puts left leg on floor for balance when standing.
• Minimal if any weight bearing.
Critical Thinking Questions1. Estimate Mrs. Lasauskas’s potential for rehabilitation on a
scale of 1 to 10, with 10 meaning she will be able to walk as well as she did before she fell.
2. List the criteria you used to make the decision in question 1.3. Mrs. Lasauskas refuses to do active ROM exercises with
her arms. How would you motivate her?
Nursing outcome and intervention labels from Johnson, M., Bulechek, G., Butcher, H., Dochterman, J. M., Maas, M., Moorhead, S., et al. (Eds.). (2006). NANDA, NOC, and NIC linkages: Nursing diagnoses, outcomes, & interventions. St. Louis, MO: Mosby.
▼ KEY PRINCIPLES
• Physical mobility requires functional joints, muscles, and bones.
• Factors affecting mobility include lifestyle, environment, growth and development, and pathophysiological factors, especially musculoskeletal and neurological health problems.
• Impaired physical mobility occurs when the client experi-ences limited ability to move within the physical environ-ment.
• Activity intolerance results when a client has insufficient physiological or psychological energy to endure or com-plete a desired activity.
• Physical examination of a client with Impaired physical mobility includes assessment of body alignment, gait, joints, skeletal muscles, and neurovascular function.
• Diagnostic tests help you select appropriate nursing diag-noses for clients with musculoskeletal health problems.
• Functional assessment includes determining a client’s abil-ity to move and perform activities of daily living.
• Assessment of the client with Impaired physical mobilityshould be holistic and include assessment of all functional health patterns for emotional as well as physiological responses, including hopelessness and pain or chronic pain.
• Expected outcomes for clients with musculoskeletal prob-lems are that the client will experience improved mobility and tolerance to activities.
• Interventions for improving activity tolerance focus on building muscle mass and strength, progressive mobiliza-tion, and controlling pain and discomfort.
• Interventions for improving mobility include maintaining joint mobility, assisting with movement, and compensating for physical impairments.
• Evaluation of outcomes for clients with musculoskeletal problems involves promoting ambulation (including wheel-chair ambulation), preventing complications of immobility, and building activity tolerance.

C h a p t e r 32 Restoring Physical Mobility 859
■ REVIEW QUESTIONS
1. The ambulatory care nurse anticipates that which of the following clients should be screened for scoliosis during the routine clinic visit?1. 4-year-old 3. 27-year-old2. 13-year-old 4. 45-year-old2. Which of the following clients assigned to the nurse would be a good candidate for using a walker as a mobility aid?1. A client who is fully weight bearing and has poor upper
body strength2. A client who is fully weight bearing and has adequate
upper body strength3. A client who is partial weight bearing and has poor upper
body strength4. A client who is partial weight bearing and has adequate
upper body strength3. The nurse is teaching the client to walk using crutches and a four-point gait. The nurse would instruct the client to do which of the following steps first?1. Move the right crutch forward about 6 inches (15 cm).2. Move the left foot forward.3. Move the left crutch forward.4. Move the right foot forward.4. You are preparing to use a gait belt when assisting a cli-ent, who can stand safely, to get out of bed into a chair. The client asks why you are using the device. What would be the best explanation?1. “The belt can be used to help pull you up from the bed
before sitting in the chair.”2. “The belt can help reassure you that you are not going to
fall during the transfer.”3. “The belt can be used to lower you to the floor if you
fall.”4. “The belt will allow me to guide you and offer support as
you complete the transfer.”5. A client who badly sprained an ankle has been measured for crutches and will begin to ambulate. To ensure proper fit before teaching the client the proper gait, the emergency department nurse checks to see that there is how much room between the axilla and the pad at the top of each crutch?1. 1⁄2 to 1 inch 3. 2 to 3 inches2. 1 to 2 inches 4. 3 to 4 inches
B i b l i o g r a p h yAlitzer, L. (2004). Compartment syndrome. Orthopedic
Nursing, 23(6), 391-396.American Nurses Association. Position statement on elimina-
tion of manual patient handling to prevent work-related musculoskeletal disorders. Retrieved July 16, 2006, from http://www.nursingworld.org/readroom/position/workplac/pathand.pdf.
Baptiste, A., Boda, S., Nelson, A., Lloyd, J., & Lee, W. (2006). Friction reducing devices for lateral patient transfers: A clinical evaluation. American Association of Occupational Health Nurses Journal, 54(4), 173-180.
Barry, J. (2006). The HoverMatt system for patient transfer: Enhancing productivity, efficiency, and safety. Journal of Nursing Administration, 36(3), 114-117.
Carpenito-Moyet, L. (2006). Handbook of nursing diagnosis(11th ed.). Philadelphia: Lippincott Williams & Wilkins.
Dabke, H., Gupta, S., Holt, C., O’Callaghan, P., & Dent, C. (2004). How accurate is partial weight-bearing? ClinicalOrthopedic Related Research, (421), 282-286.
Daniels, C., Huang, G., Feuerstein, M., & Lopez, M. (2005). Self-report measure of low back-related biomechani-cal exposures: Clinical validation. Journal of Occupational Rehabilitation, 15(2), 113-128.
de Castro, A. B. (2004). Handle with care: The American Nurses Association’s campaign to address work-related musculoskeletal disorders. Online Journal of Issues in Nursing, 9(3), 3.
Fletcher, K. (2005). Immobility: Geriatric self-learning mod-ule. Medsurg Nursing, 14(1), 35-37.
Gillis, A., & MacDonald, B. (2005). Deconditioning in the hospitalized elderly. Canadian Nurse, 101(6), 16-20.
Graf, C. (2006). Functional decline in hospitalized older adults. American Journal of Nursing, 105(1), 58-68.
Hudson, M. (2005). Texas passes first law for safe patient handling in America: Landmark legislation protects health-care workers and patients from injury related to manual patient lifting. Journal of Long Term Effective Medical Implants, 15(5), 559-566.
*Ignatavicius, D. D., Workman, M. L., & Mishler, M. A. (1999). Medical-surgical nursing across the health care con-tinuum (3rd ed.). Philadelphia: Saunders.
Ignatavicius, D. D., & Workman, M. L. (eds.). (2002). Medical-surgical nursing: Critical thinking for collaborative care(4th ed.). Philadelphia: Saunders.
*Johnson, M., Bulechek, G., Butcher, H., Dochterman, J. M., Maas, M., Moorhead, S., et al. (Eds.). (2006). NANDA, NOC, and NIC linkages: Nursing diagnoses, outcomes, & interventions. St. Louis, MO: Mosby.
NANDA International. (2007). Nursing diagnoses: Definitions and classification, 2006-2007 (6th ed.). Philadelphia: Author.
Nelson, A. (2003, March). State of the science in patient care ergonomics: Lessons learned and gaps in knowledge. Presented at the Third Annual Safe Patient Handling and Movement Conference, Clearwater Beach, FL.
Nelson, A., Powell-Cope, G., Gavin-Dreschnack, D, Quigley, P., Bulat, T., Baptiste, A., et al. (2004). Technology to pro-mote safe mobility in the elderly. Nursing Clinics of North America, 39(3), 649-671.
Pellino, T., Owen, B., Knapp, L., & Noack, J. (2006). The evaluation of mechanical devices for lateral transfers on perceived exertion and patient comfort. Orthopedic Nursing, 25(1), 4-12.
*Asterisk indicates a classic or definitive work on this subject.