Embed Size (px)
Citation preview

9 780955 399428
ISBN 0-9553994-2-4
Mental Health Commission Coimisiún Meabhair-Shláinte
St. Martin’s House, Waterloo Road, Dublin 4.
t 01 6362400 f 01 636 2440
e [email protected] www.mhcirl.ie
Happy Living Here…A Survey and Evaluation of Community Residential
Mental Health Services in IrelandDr. Donna Tedstone Doherty, Dr. Dermot Walsh, Ms. Rosalyn Moran, Health Research Board
Happy Living Here… A Survey and Evaluation of Com
munity Residential M
ental Health Services in Ireland

A place of SafetyThe artwork on the report cover depicts the reflection of a poem written by Rosaleen Cassidy a
member of the Rehabilitative Arts Programme run by Create-a-Link Arts Centre (HSE)Northwestern Area.
The hostel accommodation represents a place of safety depicted by a bird feathering its nest.The bird, safe and secure in its nest, can fly away at times to explore its environment. It alsoknows that it can come back to its place of safety at any time, and the support mechanisms
depicted by the feathers are aimed at maximising recovery and achieving meaningful interactionand participating in community life.

Glossary 2
Acknowledgments 3
Foreword 4
List of tables and figures 5
Executive summary 7
Chapter 1 The move to community care: policy and practice 11
Chapter 2 Rehabilitation and recovery: an overview 21
Chapter 3 Background to the present study and method 41
Chapter 4 Home sweet home? Description of community residences 55
Chapter 5 Residents: clinical, social and physical functioning 69
Chapter 6 Citizenship: social support, community integration and rights 77
Chapter 7 Getting better: rehabilitation through care and treatment 85
Chapter 8 Our view: satisfaction with care and treatment and other aspects of life 91
Chapter 9 Our roles: staff views of community residences 101
Chapter 10 Life in community residences: conclusion and discussion 109
Chapter 11 The way forward: recommendations 131
References 137
Appendix 1 145
Appendix 2 155
Appendix 3 163
Appendix 4 171
Contents
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 1

ADON Assistant Director of Nursing
Atypical Antipsychotic Drugs Antipsychotic drugs which are newer and more expensive than standard
antipsychotics and produce different side effects. In particular, they givefewer neuromuscular side effects.
Autonomy Freedom to make choices and decisions independently
Care Plan An individualised plan detailing treatment and care needs
Continuity of Care Care offered as a continuous series of contacts over time (longitudinalcontinuity) from a range of service providers (cross-sectional continuity).
Day Centre A day centre provides social care for service users and it may also offertreatment. Rehabilitation and activation services may be provided and mayinclude occupational therapy, social skills training and light industrialtherapy.
Day Hospital A day hospital provides comprehensive treatment equivalent to thatavailable in a hospital inpatient setting for acutely ill service users. A rangeof assessment and investigative procedures and treatments is carried out.The day hospital acts as the focus of psychiatric care in an area and isprimarily for active treatment of patients with psychiatric disorders.
DON Director of Nursing
GAF General Assessment of Functioning
GP General Practitioner
HAIL Housing Association for Integrated Living
HoNOS Health of the Nation Outcome Scale
HRB Health Research Board
HSE Health Service Executive
HSE Administrative Areas In 2005, four new HSE administrative areas replaced the former healthboard areas. Within the four administrative areas there are local healthoffice areas that correspond, in the main, to county catchment areas.
Key Worker A staff member who usually has the most one-to-one contact with themental health service user with complex needs. The key workercommunicates with others involved in the care of the service user.
Long-stay Continuous hospitalisation for over one year.
MHC Mental Health Commission
NPIRS National Psychiatric Inpatient Reporting System
Policy A plan of action that governs mental health service activity and whichemployees are expected to follow.
Protocol A written plan specifying the procedures to be followed in providing carein defined situations (Protocols specify who does what, when and how).
Planning for the Future Title of the report of a study group on the planning of the psychiatricservices. December 1984.
Skill Mix The blend of skills needed amongst a team of staff to ensure effectivehealth care delivery.
STEER A community based user-led mental health organisation. Support –Training – Education – Employment – Research.
A Vision for Change Title of the report of an expert group, which sets out a comprehensivepolicy framework for mental health services (2006)
Glossary
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND2

The authors would like to thank the staff of the HSE local areas who contributed to this study,especially the clinical directors, directors of nursing and assistant directors of nursing andadministrators. But, above all, the authors would like to thank the residents for giving so willingly oftheir time to participate in this project, for welcoming the researcher (DTD) into their homes and fortheir honesty and openness. Without their co-operation this project would not have been possible.
We would also like to thank the advisory committee for their advice and assistance throughout thestudy period. The advisory committee members were:
Bríd Clarke, Mental Health Commission
Fiona Keogh, Mental Health Commission
Derek Griffin, Northern Area
Pat Brosnan, Mid West Area
John Hayes, North West Area
Rhona Jennings, Mental Health Commission
Bernadette McCabe, St Vincent’s Hospital, Fairview
Diarmuid Ring, Mental Health Commission
Mike Watts, Mental Health Commission
Thanks also to colleagues in the Health Research Board for providing assistance during the studyperiod. A special thanks to Yulia Kartalova O’Doherty for her invaluable input throughout the study.
Finally the authors would like to thank the external reviewers, Mr John Saunders and Dr SineadMcGilloway, for their time and invaluable comments.
Funding from the Health Research Board and the Mental Health Commission supported this project.
Acknowledgments
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 3

Significant changes have occurred in the profile of mental health service provision in Ireland during thelast 25 years. The number and composition of community residences have grown considerably. This hashad an immediate effect on reducing the number of long-stay patients in hospital as advocated inPlanning for the Future (1994). In 1984, there were 121 community residences, with nine hundred(900) places. Twenty years later in 2004, the number of people living in community residencesexceeded three thousand (3,065). Community residences are, therefore, now a very important elementof mental health services provision in Ireland, shaping the lives of over three thousand (3,000) peopleand utilising considerable personnel and financial resources.
The Mental Health Commission considered it opportune to review and evaluate the role of communityresidences in Ireland and to report on how the needs of residents were being met and whether thecommunity residences were fulfilling the original mandate of providing a therapeutic and rehabilitationfunction. The study was undertaken by the Health Research Board and jointly funded by the MentalHealth Commission and Health Research Board. The information and knowledge from this study willcompliment the inspections of 24 hour nurse supervised community residences undertaken by theInspectorate of Mental Health Services in 2005 and reported in detail in the Annual Report of theMental Health Commission, including the Report of the Inspector of Mental Health Services 2005.
Research provides new knowledge and understanding and enhances strategic planning and servicedelivery. This study of community residences provides valuable information and evaluation of this keyaspect of mental health services in Ireland. The most important component of this study is the input ofthe residents, who, as the prime reporting agents, expressed their views of their lives and their degreeof satisfaction with current service provision.
We hope this study will inform the current philosophy and operation of community residences andfuture mental health service planning. Issues raised include increasing autonomy and independence ofresidents, promoting growth and choice, creating “a way of living a satisfying, hopeful andcontributing life even with the limitations caused by illness” ( Anthony 1993). Of wider social andeconomic significance the study supports mainstreaming housing provision for people with mentalhealth difficulties and mainstreaming training and employment opportunities.
With the closure of mental hospitals, financial resources will become available for the development ofcommunity-based services. It is imperative that the recommendations of this report are nowincorporated in development plans for mental health services.
I would like, on behalf of the Mental Health Commission, to thank all those involved in this study, theHealth Research Board, the staff from the three Health Service Executive areas and the advisorycommittee. I wish to express my deepest appreciation to the residents who participated in this studyand who shared their experiences and views with us.
Bríd ClarkeChief Executive Officer
Mental Health Commission
January 2007
Foreword
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND4

LIST OF TABLES
Table 3.1 Population figures for study catchment areas and HSE local areas 43
Table 3.2 Factors addressed in each of the four questionnaires 45
Table 4.1 Number (%) of residents in each diagnostic category, by level of support 57
Table 4.2 Total number of residences, number (%) of residents and number (%) of places, by level of support 58
Table 4.3 Mean number of bedrooms in residences and standard deviations by level of support 59
Table 4.4 Mean length of time in minutes (SD) to reach other services and amenities, by level of support 59
Table 4.5 Number (%) of admissions in the last three years (2002-2004), by level of support 60
Table 4.6 Total number of residents discharged and place discharged to, by, level of support 60
Table 4.7 Number (%) of residences employing exclusion criteria and the specific exclusion criteria employed, by level of support 61
Table 4.8 Number (%) of residences that had polices on health and safety and related matters, by level of support 63
Table 4.9 Number (%) of residences that imposed rules and regulationsconcerning freedom within the residences, by level of support 64
Table 4.10 Number (%) of residences that had rules and regulations concerning bedroom use and privacy, by level of support 65
Table 4.11 Number (%) of residences and responsibility for food preparation, by level of support 66
Table 5.1 Percentage of residents in each category of the HoNOS individual items 73
Table 5.2 Percentage of residents experiencing physical health disabilities 73
Table 6.1 Key workers’ reported system of support for residents number (%) in the last year 78
Table 6.2 Number (%) of residents attending activities in the community, by level of support 80
Table 6.3 Information provided to residents on complaints procedures and rights, by level of support 81
Table 6.4 Information provided on the role and functions of the Mental Health Commission, by level of support 82
Table 6.5 Information provided to residents on voting registration and health initiatives, by level of support 82
Table 6.6 Number of residences (n = 102) providing health information and type of information 83
Table 7.1 Number (%) of residents on medication, by category, by level of support 87
List of tables and figures
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 5

Table 7.2 Number (%) of residences showing the proportion of residents attending either day centres or day hospitals, by level of support 88
Table 7.3 Number (%) of residences providing activities and training, by level of support 88
Table 7.4 Number of residences (%) providing activities to aid community integration, by level of support 89
Table 7.5 Number (%) of residences showing the proportion of residents going on independent holidays in the past two years, by level of support 89
Table 7.6 Number (%) of residences showing the proportion of residents going on organised holidays in the past two years, by level of support 90
Table 8.1 Residents’ responses to statements about their care plans (number and percentages) 92
Table 8.2 Residents’ responses to statements about their treatment and care provided by key workers (numbers and percentages) 93
Table 8.3 Total number (%) of residents providing comments under the main themes, by level of support (n = 124) 95
Table 9.1 Number (%) of high support residences within each staffing level, by shift 102
Table 9.2 Frequency (%) of staff, by occupation, by level of support 103
Table 9.3 Number (%) of staff rating the importance of the aims and functions 103
Table 9.4 Number (%) of responses in each category of factors believed to promote independent living 104
Table 9.5 Number (%) of responses in each category of factors believed to impede independent living 106
LIST OF FIGURES
Figure 1.1 Provision of community residential places in Ireland for five-year intervals from 1983 – 2003 17
Figure 4.1 Frequencies of age groups of residents, by level of support 56
Figure 6.1 Resident’s reported social support network in four domains 79
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND6

Substantial change has taken place in the mentalhealth services in Ireland following thepublication of Planning for the Future in 1984.That policy document recommended anaccelerated move towards the provision of carein community settings and the closure of alllarge psychiatric hospitals. Patients withpersistent mental health problems were to berelocated to alternative accommodation incommunity residences. The rationale was thatcommunity residences would fulfil a therapeuticand rehabilitation function such that personswith persistent mental illness would move fromhigher to lower levels of support, and wherepossible, to complete independence. The morerecent mental health policy A Vision for Change(Department of Health and Children, 2006),emphasises the importance of independence andrecovery for those with persistent mental healthproblems. However, there is little information inthe policy about the role of communityresidences, a key component of communitymental health provision – in providing forresidents’ wellbeing and independence. Thepresent study examines the role and functions ofcommunity residences and, in particular, theextent to which they have fulfilled theexpectation of Planning for the Future (1984) infostering rehabilitation and independence. Thestudy details the characteristics of the residentsand the residents’ perceptions of their lives in theresidences. The findings informrecommendations regarding the futuredevelopment and reorientation of this servicecomponent.
The study describes and evaluates the nature andquality of community residential accommodationand the extent to which it met the needs ofresidents. The functioning of communityresidences with reference to the appropriatenessof premises and their operational role inproviding for the residents is discussed. Residentsthemselves were the prime reporting agents asto the view of their lives and their degree ofsatisfaction with current service provision. Theinteraction of the residents with theirneighbourhood and environment was alsoinvestigated. Enquiry was made as to their‘citizenisation’, such as voting registration,participation in social amenities and use ofcommunity services. In addition, staffunderstanding of the aims and functions of theresidences and their perceptions of the factorsthat promoted or impeded independent livingwere investigated.
STUDY FINDINGS
Three HSE local mental health service areas tookpart in the study – North West, Mid West andNorthern Area, comprising eight catchmentareas. One of these catchment areas had nocommunity residences. There was a total of 102residences in these areas, providing 951 places.The majority of these places were high support(584), with 166 medium support places and 201low support places. At the time of the studythere were 871 residents living in the residences,an occupancy rate of 92%. However, 76 placeswere designated for other uses (such as respitecare), resulting in an occupancy rate of 97%.
A total of 138 residents were interviewed for thestudy. Of these, 59% were from high support,18% from medium support and 22% from lowsupport residences. Their average age was 53years (SD 13.4), the majority were single andalmost half had second level education. A largeproportion of the sample were unemployed(40%), while 27% were in sheltered employmentand 7% in either part-time or full-time paidemployment. The residents interviewed had along duration of illness and the majority had adiagnosis of schizophrenia.
The clinical functioning of the residentssuggested that the majority had mild but stablesymptoms. Their general occupational and socialfunctioning was better in medium and lowsupport than in high support; however, all groupratings were above the level that indicates amarked degree of disability. In general, noproblems in social functioning two weeks priorto interview was reported, but mild to moderatedifficulties were reported for activities of dailyliving. The majority of the residents were notexperiencing physical health problems. Thus, theresidents had a low rate of clinical symptoms,generally had good physical health and showedno marked disabilities in occupational and socialfunctioning. The findings suggest that someresidents were over-provided for in terms of thelevel of accommodation in which they wereliving.
The results of the interviews showed that, ingeneral, the residents were satisfied with theirtreatment and care and their currentaccommodation; however a number of residentsindicated that, if given a choice, they wouldprefer more independent living arrangements.The perceptions of the residents regarding life in
Executive Summary
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 7

the residences were mostly positive and residentsreported that they had control over their livesand were happy with their level ofindependence.
While the majority of the residents went out ontheir own and reported that they were happywith their level of participation in thecommunity, few used social amenities in thecommunity. A large proportion of residentsreceived staff help to mange their finances.Almost a quarter were reported to have nosystem of support outside the residences, whileover half had visits from family and friends ormade visits to family and friends. The residentsthemselves reported that they would rely on staffor other residents for support during a crisis, butthat they would use supports from outside theresidences for everyday psychological support, ifavailable.
Among staff, the most commonly perceivedfunctions of the residences were those ofcontinuing care and rehabilitation. In terms ofrehabilitation, the majority of residences werereported as providing a range of therapeuticactivities, mainly social skills training andeveryday living skills training. Fewer residenceswere providing cognitive behavioural therapies oractivities that promoted community integration,mainstream employment or mainstream housing.This is not surprising given the lack of specialisedmulti-disciplinary rehabilitation teams in theservices studied.
The internal environment of the residences wasnot ideal, with a small number of bathroomsand many shared bedrooms. Results indicate thatlack of privacy was an issue for a number ofresidents. In general, there was good access tofacilities such as shops, post offices and GPsurgeries in the external environment. However,few residents had access to their own transport,which was problematic for those in more remotelocations where public transport was oftenunderdeveloped.
The climate and culture of the residencesreflected more those of a ‘mini-institution’ thanof a home-like environment, especially in thehigh support residences. The medium and lowsupport residences were somewhat more relaxed,but a large number employed constricting rulesand regulations, the necessity for which wasquestionable. There appeared to be little in theway of individualised treatment and care
planning in many of the residences, nor wasthere much participation by the residents in theirtreatment and care. The results suggested thatthe philosophy of a ‘recovery’ model was still farfrom realisation in these community residences.There was very close interaction between theresidents and staff, and residents reported in themajority of cases that staff and residents got onvery well together. However, there was evidenceof an excess of care in some cases, for examplethe restrictive nature of residential facilities andthe lack of autonomy of the residents given theircurrent level of functioning. This most likelystemmed from the fact that many staff weretrained in the care philosophy of the oldpsychiatric hospitals.
STUDY IMPLICATIONS
The study has provided a view of the communityresidence service component in the round and,most importantly, through the eyes of those wholive in community residences. The findings showthat there is a high level of satisfaction amongresidents in relation to their treatment and careand the accommodation provided. Manysuggestions for improvement also emerged,which are presented in the recommendationsbelow. But what of the service into the futureand the needs of future residents? The studyrecommendations address the future of thiscommunity residence service component as theprogramme of deinstitutionalisation comes to anend and the services move towards a ‘recovery’approach, whereby individuals are empowered totake more control of their own lives andparticipate more fully in society. Thiscontextualisation calls into question manyaspects of the role and function of communityresidences. These include issues such as theresponsibility for the provision of residences, theinternal and external environment of theresidences, the climate and culture within theresidences, and rehabilitation and recoveryphilosophies of care.
The recommendations below have been made inthe light of the study findings and have takeninto consideration recent policy documents andevidence-based practice. The authors weremindful of the feasibility of implementing therecommendations within the Irish mental healthservices and were of the opinion that therecommendations should be addressed in the
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND8

short to medium term. It is the authors’intention however, that these recommendationswill be evaluated in light of local area needs,requirements and resources and adapted andimplemented accordingly.
STUDY RECOMMENDATIONS
Recommendations are made under four mainheadings – the way forward for rehabilitationand recovery, the way forward for currentcommunity residences, future provision ofhousing and the implementation action plan.
A summary of the recommendations arepresented in the following section under the fourmain headings. Readers are advised to note thefull list of recommendations in Chapter 11.
THE WAY FORWARD FORREHABILITATION AND RECOVERY
Fully staffed specialised rehabilitation andrecovery mental health teams should beestablished in all services as a matter ofurgency.
All members of the specialised rehabilitationteam should be trained in the competenciesand principles of recovery.
All current and potential residents shouldreceive a full multidisciplinary assessment.
Staff should, by attitude and practice, orientresidents towards raising their expectations oftheir capabilities to achieve independence.
Individual care plans should be developedwith residents and should incorporate theirexpectations and be reviewed on a regularbasis.
A key worker system should be in place in allareas.
The pharmacological treatment of residentsshould be reviewed regularly, especially thoseon multiple medications.
Rehabilitative activities should be tailored tomeet the needs of the individual.
The possibility of moving rehabilitativeactivities to the community and availing of
existing community-based activities should beexplored and developed.
Residents should be encouraged and providedwith the necessary skills to look after theirown finances.
Residents should be encouraged to developand extend social support networks.
Mainstream employment using the ‘place andtrain’ model coupled with other employmentand training initiatives should be developedwith the relevant stakeholders and evaluated.
THE WAY FORWARD FOR CURRENTRESIDENCES
Community residences should be used onlyfor support and rehabilitation.
All staff should be trained in thecompetencies necessary to provide a recovery-oriented service.
Residences should provide a ‘home-like’environment for residents.
The number of places in high supportresidences should be reduced to ten.
Nursing resources currently employed incommunity residences should be evaluatedand the proper skill mix of staff ensured.
Evaluation and review plans should beimplemented in the residences to monitorquality, including residents’ satisfaction.
Aims and functions of community residencesshould be reviewed and standardised.
FUTURE PROVISION OF HOUSING
Housing for those with mental healthdifficulties must be provided as part ofmainstream housing and is not theresponsibility of the mental health services.
The provision of low and medium supporthousing should be the responsibility of thelocal housing authorities.
A range of housing alternatives is necessary tomeet the needs and support requirements of
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 9

individuals with different mental healthneeds.
Multi-agency groups involving, among others,local housing authorities and mental healthservice providers, should be set up as a matterof urgency to discuss partnership schemes inthe provision of housing and care.
Pilot schemes for the provision of housingthat have been shown to be effective shouldbe encouraged and should receive financialsupport.
All future housing should be designed withthe principles of recovery in mind.
IMPLEMENTATION ACTION PLAN
The study recommendations must beimplemented without delay.
Intersectoral action plans must be formulatedat central and local level and must representhousing and mental health interests.
The local group will report on progress to thecentral group.
An intersectoral implementation group shouldbe formed at central level. This group shouldlead on intersectoral policy changes required,monitor progress towards implementationand liaise with the implementation andmonitoring bodies of A Vision for Change.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND10

Chapter 1The Move to CommunityCare: Policy and Practice

1.1 INTRODUCTION
It is estimated that 450 million peopleworldwide suffer from mental healthproblems (World Health Organization(WHO), 2003). Furthermore, it is estimatedthat mental health problems will increasefrom 12% of the total burden of diseaseto 15% by 2020. This confirms psychiatricdisorder as one of the leading causes ofdisease and disability. WHO estimates thatone in four people visiting a health servicehas mental health difficulties that are oftenundiagnosed and untreated. WHO reportsthat cost-effective treatments do exist formost mental health problems and, ifappropriately used, could result inenabling most individuals to become fullyfunctioning members of society.
Irish mental health polices, such asPlanning for the Future, have emphasisedthe closing of psychiatric hospitals andsubstituting institutional care with care inthe community (Department of Health andChildren, 1984). In the last twenty years asubstantial change has taken place in theIrish mental health services. Theprogramme of deinstitutionalisation hasaccelerated in most areas and, while this isnot yet complete, many individuals havebeen relocated to community-basedresidences. A recent development has beenthe publication of A Vision for Change(2006), which outlines the continueddevelopments necessary for mental healthservices to meet evidence-based standardsof practice and care and to ensure that thefundamental rights of mental heath serviceusers are met.
Among the recommendations forcommunity care was the provision ofcommunity residential facilities for therelocation of long-stay patients frompsychiatric hospitals. The rationale wasthat these community residences shouldfulfil a therapeutic and rehabilitationfunction such that residents passed fromhigher levels of dependency to lower levelsof support and, where possible, tocomplete independence. No previousresearch in Ireland has investigated thequality of the mental health servicescommunity residences and the extent towhich the services meet the needs of theresidents.
This study aimed to describe and evaluatethe nature and quality of communityresidential accommodation in a sample ofthree HSE local areas in Ireland and theextent to which this provision hasaccomplished the policy objective (moreinformation on the aims and objectives ofthe study are presented in Chapter 2). Thethree participating HSE local areas werethe North West Area, the Mid West Areaand the Northern Area. The North Westincludes the catchment areas of Donegaland Sligo. The Mid West comprises thecatchment areas of Limerick, Clare andNorth Tipperary. The Northern Areaincludes the catchment areas of DublinNorth West (Mental Health Area 6), DublinNorth City (Mental Health Area 7) andDublin North (Mental Health Area 8).These areas are located within two HSEadministrative areas. The North West andthe Mid West are located in HSEadministrative area A, while the HSEadministrative area B includes the NorthernArea. More information on theparticipating areas is presented in Chapter3.
Although there have been some surveys ofthe extent of mental illness in specificpopulation groups, such as the elderly(Shiely & Kelleher, 2004; McGee et al.,2005) no comprehensive community-based data exist on psychiatric morbidityin the general adult population in Ireland.Data from a pilot study suggest that 25%of patients attending general practice inIreland have mental health problems(Copty & Whitford, 2005). The majority ofthese (95%) are dealt with in primary carewith the rest being referred to mentalhealth services. The Mental HealthResearch Division (MHRD) of the HealthResearch Board (HRB) is currently carryingout a survey to assess psychologicaldistress, service use and help-seekingbehaviour in the general population. Thissurvey should help to bridge the currentinformation gap in terms of assessing thelevel of psychological distress in thepopulation and mental health serviceneeds.
There is some indication of the mentalhealth service activity levels at secondary-level care. The Medico-Social ResearchBoard, later to be amalgamated with the
CHAPTER 1
The move to community care: policy and practice
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND12

Medical Research Council (MRC) tobecome the Health Research Board (HRB),has been collecting statistics on activity atinpatient psychiatric hospitals and units foralmost forty years. The latest figures (Dalyet al., 2005) show that there were 22,279admissions to psychiatric hospitals andunits in Ireland during 2004, resulting in arate of 735 admissions for every 100,000persons aged 16 years and over. It isimportant to note that these figuresrepresent all admissions – first admissionsand re-admissions. In the absence of anindividual patient identifier, it is notpossible to determine how many individualpatients are represented in the re-admission figures.1 First admissions, on theother hand, refer to unique individuals andthere were 6,134 first admissions in 2004– a rate of 202 per 100,000 persons aged16 and over. These national inpatient dataare reported on by age, gender and othervariables in annual reports from NationalPsychiatric Inpatient Recording System(NPIRS).
While the inpatient activity of mentalhealth services has been recorded andreported on, there is a lack of informationconcerning activity within othercomponents of the mental health service.This is of particular concern in the currenttime of change and the move towards acommunity based service. The HRB hasdeveloped a database, COMCAR, to recordactivity at community care level. Thisdatabase is currently being piloted innumerous sites around the country, priorto national roll-out. It is important to notethat the absence of mental healthinformation systems has been highlightedin the Report of the Inspector of MentalHealth Services (MHC, 2005a) which statesthat information ‘is fundamental to thedelivery and management of any businessor service’. The HRB and MHC have set upa committee to devise a minimum data setfor mental health services.
Concerning our capacity to respond toproblems of mental illness and the under-funding of the mental health services, theReport of the Inspector of Mental HealthServices (MHC, 2005a) highlighted theunder-funding of the mental healthservices, which in 2004 was 7% of
national health expenditure. The Reportargues that an increase of 5% bringingexpenditure to 12% of the national healthbudget, is required. This is in line with theestimates of mental health problemsaccounting for 12% of the total burden ofdisease and with proportional mentalhealth expenditure in the United Kingdom.
1.2 POLICY FRAMEWORK: THE MOVEFROM INSTITUTIONAL CARE
Prior to the mid-eighteenth century,mental illness was not a major socialconcern and was often viewed as theconsequence of ‘possession’ andwitchcraft. It aroused bewilderment andconfusion and was often dealt withharshly and punitively. A century later, theproblem of mental ill health had increasedto such an extent that a national system oflunatic asylums was established in Ireland.This reflected the national policy ofinstitutionalisation of the mentally ill inIreland as elsewhere which was to persistfor almost a century and a half.
In Ireland, the 1945 Mental Treatment Actallowed for the ‘boarding out’ of detainedpatients and for voluntary admission todistrict psychiatric hospitals. However,admissions to inpatient care continued toincrease and the ‘boarding out’ of patientswas not adopted on a national level.Institutionalisation reached its peak inIreland in 1958 when over 21,000 personswere resident in our psychiatric hospitals,about 3,000 of whom were intellectuallydisabled.
With the growth in provision of alternativeforms of care, such as outpatient clinics,and the introduction of antipsychotic andantidepressant drugs, coupled withconcern about the conditions in psychiatrichospitals and a growing civil rightsmovement, the numbers of those detainedfor long periods in psychiatric hospitalsdeclined. These improvements, which hadbegun in other jurisdictions, spread toIreland, where existing conditions weresharply critised and the need to move tocommunity care for the mentally ill wasemphasised by the Report of the
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 13

Commission of Enquiry on Mental Illness in1966. The recommendations of theCommission were reinforced by anothernational policy document in the field ofmental health, Planning for the Future, in1984.
Policy documents and legalistic provisionsfundamental to the development andchange in mental health services in Irelandhave included Planning for the Future(1984) and the Mental Health Act (2001).More recently a new policy document, AVision for Change (2006), provided apolicy framework for the development ofmental health services for the next sevento ten years.
1.2.1 The community residentialalternative to long-stayhospitalisation
The 1966 Commissionrecommended that the number ofhospitalisations should be reducedby 1981. However, therecommendations relating tocommunity placement of the long-stay inpatient was meagrelyimplemented, so that by 1981 thenumbers hospitalised still stood at15,000 rather than the 8,000 thatthe Commission had visualised.Planning for the Future (1984)specifically addressed this particularproblem.
That report argued for acomprehensive mental health serviceto provide care for the varying needsof people with mental healthproblems. This service was toinclude community-based residencesto which suitable long-stay patientsfrom the psychiatric hospitals couldbe relocated. The report proposedfour categories of persons whowould be more suitably placed inthe community residential services,as follows:
Persons now living in psychiatrichospitals who have no homes oftheir own to return to but who,with adequate preparation andtraining, would be capable ofliving a reasonable life in the
community;
Persons coming forward forpsychiatric care with chronicpsychiatric disability, who haveinadequate or no homes andwho would be capable of livingwith varying degrees ofindependence in accommodationin the community;
Persons with psychiatric problemswhose treatment requires thatthey live apart from their familyor normal associates for a while –such persons include disturbedteenagers who have familydifficulties and patients in needof temporary accommodationdue to any of a variety of socialreasons;
The small group of new long staypatients for whom high supporthostels will provide an alternativeto long-stay hospital care.(Department of Health andChildren, 1984: p.60)
In 1989 the priorities for the futuredevelopment of the mental healthservices were outlined in thedocument Shaping a HealthierFuture (Department of Health andChildren, 1989). These included theestablishment of departments ofpsychiatry in general hospitals andthe introduction of a new MentalHealth Act which would, inter alia,meet the requirements of theEuropean Convention on HumanRights. A White Paper (Departmentof Health and Children, 1995)reaffirmed the need for theprotection of patients admittedinvoluntarily and further highlightedthe need for new legislation.
1.2.2 Mental Health Act 2001
The Mental Health Act of 2001proposes significant changes tocertain aspects of the mental healthservices in Ireland. It is concernedwith the involuntary admission ofpersons in psychiatric hospitals, themonitoring and evaluation of
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND14
1 Local figures from the Mid West suggested that, on average, each person accounted for 2.5 admissions.

approved centres, mental healthservices, and the legal rights ofpsychiatric patients. It also providesthe legislative basis for theestablishment of the Mental HealthCommission (MHC) – anindependent body with responsibilityto promote good practice and highstandards in the delivery of mentalhealth services and to protect theinterest of people admittedinvoluntarily to psychiatric hospitalsand units. The MHC in its StrategicPlan 2004–2005, highlighted andsupported the notion of communitycare in place of inpatient care. TheMHC has also stimulated the debateon mental health service provisionand quality with the publication ofthree discussion papers. These are: AVision for a Recovery Model in IrishMental Health Services (MHC,2005b), Multidisciplinary TeamWorking: From Theory to Practice(MHC, 2006a) and Forensic MentalHealth Services for Adults in Ireland(MHC, 2006b). The MHC alsocommissioned a research studyinvestigating service users’ andstakeholders’ perceptions of qualityin mental health services (MHC,2005c). A recent reportcommissioned by the MHC showedthat the organisation of publicmental health services wasinappropriate and unsuited to theneeds of those who use theseservices (Dunne, 2006). This is animportant step in using research andservice users’ and stakeholder inputto inform practice and policy.
The Mental Health Act 2001provides for the appointment of anInspector of Mental Health Servicesin place of the previous post ofInspector of Mental Hospitals. TheInspector of Mental Health Serviceshas responsibility for the inspectionof all approved inpatient centres andother centres where mental healthservices are provided. In addition,the inspectorate ascertains theservice users’ and carers’ views ontheir local services. This informationfacilitates the Mental Health
Commission’s statutory responsibilityto ‘promote, encourage and fosterthe establishment and maintenanceof high standards and good practicein the delivery of mental healthservices’. The Inspectorate’s first fullreport was published in 2005 (MHC,2005a). This report highlighted that,although the living conditions ofmany people were improved by therelocation from the long stay wardsin hospitals to communityresidences, without specialistrehabilitative input ‘such residencesbecame little better than long-staywards in a community setting’. TheInspector also pointed out that 35rehabilitation teams were requirednationally. The provision of thisspecialised care and support shouldresult in a decrease in the number ofpsychiatric beds as long-staypatients are moved to thecommunity, in addition to areduction in 24-hour staffedcommunity placements as thosenewly presenting with severe mentalillness are provided with care andsupport to live independently in thecommunity (MHC, 2005a).
1.2.3 A Vision for Change
The most recent documentconcerning policy in mental healthservices in Ireland is the report, AVision for Change, by the ExpertGroup on Mental Health Policy(Department of Health and Children,2006). It details recommendationson how the mental health services inIreland should develop over the nextseven to ten years. A phaseddevelopment is recommended whichshould be in line with thereorganisation of the mental healthservices in the new health servicestructures. The document proposesa policy framework that adopts alifespan approach to mental health.It covers all areas of mental healthservice provision from primary careto specialist care. The Reportemphasises a community-basedapproach with inpatient servicesused sparingly. It takes a holistic
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 15

view of mental health that addressesbiological, psychological and socialfactors and consequently advocatesa multidisciplinary approach. TheReport was devised in consultationwith service users, carers, providersand other stakeholders and coveredall aspects of the service fromevidence-based interventions to themanagement and the financing ofthe services. A Vision for Changesees service users’ and carers’ viewsas critical to the development andplanning of services. In addition, theReport recommends the importanceof empowering service users to takeresponsibility for their care inpartnership with providers. Thisdocument clearly sets the scene forthe future development of themental health services which arewithout doubt firmly placed within acommunity-care model.
In relation to the issue of providingfor the recovery and rehabilitation ofpersons with severe and persistentillness, A Vision for Changeenvisioned that the housing forpersons with or recovering frommental illness would be supplied bylocal housing authorities in routine,normal houses which would be inno different from those available toother clients housed by them. TheReport recommended threeresidential units of 10 places eachper 100,000 population for thosewhose enduring problems would beof such intensity that a high level ofsupport by the mental healthservices would be required. It isenvisaged that, once the cohort ofexisting long-stay patients has beenaccommodated, the requirement forhigh support accommodation willdecline. Thus, the main housingrequirement into the future will befor individualised, independentaccommodation with some support,as appropriate, from the mentalhealth services working co-operatively with the housingauthorities. It is pointed outunambiguously that the statutoryresponsibility for housing lies
squarely with the housingauthorities and should not be withinthe remit of the mental healthservices. The Report points out thata considerable deviation of mentalhealth resources has resulted fromthe practice of mental healthservices providing accommodationwhich is statutorily the responsibilityof housing authorities. The Reportfurther alludes to the necessity ofusing housing in a flexibleprogressive fashion to bestaccommodate the changing needsof patients as recovery proceeds. It isfelt that crisis housingaccommodation would best beaccomplished by special crisis unitson the basis of one per region of300,000. It was argued that thecurrent practise of designating anumber of beds in routine mentalhealth housing for this purpose, andthat such mixing of patients, aimsand purposes was not in the bestinterests of either group.
1.2.4 European framework for mentalhealth
The World Health Organization(WHO) European office hasdeveloped a Mental HealthDeclaration for Europe (2005) andan accompanying Mental HealthAction Plan for Europe (2005). Thesehave been endorsed by Ministersfrom the European WHO memberstates (January 2005). Thesedocuments proposed the prioritiesfor mental health over the next 10years and specified actions to meetthese priorities. The following fivepriorities were listed in theDeclaration:
Foster an awareness of mentalhealth.
Tackle stigma, discrimination andinequality and empower thosewith mental health problems andtheir families to engage in thisprocess.
Design and implementcomprehensive mental health
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND16

systems that cover mental healthpromotion, prevention, treatmentand rehabilitation and care andrecovery.
Create a competent workforcewith the necessary skills foreffective treatment and care in allareas.
Recognise the experience of theuser and the families and carersand the importance of thisexperience for service planningand development.
The WHO Action Plan presented anumber of actions under twelveheadings, which ranged frommental health promotion, treatmentand care, evaluation of effectivenessand funding of mental healthservices. Regarding the location ofmental health services, the planadvocated that provision should befirmly placed within the community,with a limited number of hospitalbeds. The document recognised theimportance of a comprehensivemultidisciplinary service thatempowers service users to work inpartnership with service providers.Actions to address stigma and
discrimination were proposed aswere actions to establish partnershipacross sectors. It is envisaged thatthe member states of the WHOEuropean Region will use the actionslaid out in the Action Plan todevelop and implementcomprehensive policies in theircountries. The recently published EUGreen Paper aimed at thedevelopment of an EU strategy onmental health articulates similarthemes (Commission of theEuropean Communities, 2005). Therecommendations of Irish policydocuments, especially thosereported in A Vision for Change arein line with current Europeanthinking in the area.
1.3 FROM POLICY TO PRACTICE:COMMUNITY RESIDENTIAL CAREIN IRELAND
The move in policy and practice tocommunity care in Ireland resulted in adecline in the overall number of inpatientsin psychiatric hospitals and units and anincrease in the number of communityresidential facilities as patients were
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 17
20
40
60
80
100
'03'98'93'88'83
Plac
es p
er 1
00,0
00 p
opul
atio
n
Year
Figure 1.1 Provision of community residential places in Ireland for five-year intervals from 1983to 2003

relocated to the community. As a result ofthe implementation of this policy, thenumber of persons in inpatient care haddeclined to 3,389 persons by the end ofMarch 2006 (Daly & Walsh, 2006). Ofthese, 997 were long-stay in hospital (i.e.in hospital for more than five years) and548 were categorised as ‘new long-stay’(i.e. in hospital for more than one but lessthan five years).
The figures for community residentialfacilities in Ireland were reported in theReport of the Inspectorate of MentalHospitals until 2003 when there was inter-organisational shift in the responsibility forproducing the report of the mental healthservices. Figure 1.1 shows the totalnumber of community residential placesper 100, 000 population for five-yearintervals from 1983 to 2003. Figures forthe number of residents in communityresidential facilities in 2004 were providedby the Mental Health Commission (MHC,personal communication).
There was a total of 111 communityresidential facilities in Ireland in 1983, 233in 1988, 361 in 1993, 386 in 1998 and418 in 2003. Thus, the number ofresidences doubled between 1983 and1988 following the publication of Planningfor the Future (1984). This increasecontinued to 2003, although at a slowerrate. The facilities provided 942 places in1983, which increased to 3,210 in 2003.The corresponding rates were 27 placesper 100, 000 population in 1983 and 82per 100, 000 population in 2003 (Figure1.1). As in the number of facilities, thelargest increase in rate of places per 100,000 occurred following the publication ofPlanning for the Future in 1984 andcontinued during the period 1988 to1993. The most recent figures in 2004reported there were 3,065 residents livingin the community residential facilities, arate of 101.2 residents per 100,000population aged 16 years and over (MHC,personal communication).
These figures suggest that the policy ofdeinstitutionalisation was indeedimplemented in the eighties and earlynineties and that large numbers ofpatients were relocated from inpatient care
to alternative community residences. Thereare now approximately 1,755 patients inpublic psychiatric hospitals – 774 beinglong-stay patients, of whom 408 are agedover 65 years (Daly & Walsh, 2006). Asreviewed above, recent Irish policyadvocated that the remaining psychiatrichospitals be closed and patients moved tocommunity care (MHC 2005a; MHC2006c).
1.4 STRUCTURE OF ADULT MENTALHEALTH SERVICES IN IRELAND
Until 2005 the health services in Irelandwere organised and managed by statutorybodies (health boards) and were based ongeographical regions. These health boardswere responsible for the health and socialservices of the population within thedesignated boundaries. In 2004, thehealth service delivery system wasrestructured by legislation. A new bodywas established, the Health ServiceExecutive (HSE), which resulted in thedissolution of the old health board areas.In addition to taking over the roles andresponsibilities of the previous healthboards, the HSE is tasked with developingservices in line with the most recent healthstrategy, Quality and Fairness: A HealthSystem for You (Department of Health andChildren, 2001), such as the inclusion ofservice users in decision making andservice planning. Changes to theorganisation of the health service cameinto effect in January 2005, with HealthService Executive administrative regionsand local areas replacing health boardareas. Where there were eight healthboard areas, there are now four HSEadministrative areas with populations ofapproximately 1,000,000 each. The localhealth office areas within these areascorrespond, in the main, to the countycatchment areas.
Suggestions as to the best way forward forthe delivery of mental health serviceswithin the new health service structurewas reported in A Vision for Change. Itwas argued that the existing smallcatchment areas of about 100, 000population have hindered the
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND18

development of specialised mental healthservices (Inspector of Mental HealthServices, Mental Health Commission,2005a). A Vision for Change reported thatcatchment areas should be increased insize from approximately 100,000population to between 200,000 and400,000. Catchment area size will dependon the characteristics of the populationand on geographical factors. The largercatchment areas will allow for theinclusion of specialised mental healthservices in areas that are accessible to thepopulation. A Vision for Change proposedthat sectorisation remain and that sectorsize be increased from 25,000 to 50,000.To date, no major changes have occurredin the management or delivery of themental health services since the changes inthe health service structures. Following therecommendations in A Vision for Change,an implementation review committee wasestablished to ensure the implementationand evaluation of the recommendationswithin the seven to ten year time span.
1.5 SUMMARY
The recommendation to move frominstitutional to community care has beenreiterated in many national andinternational policy documents over thepast 40 years. The relocation of patientsfrom large institutions in Ireland has beenslow and variable across the country andthere are now approximately 15 old-stylepsychiatric hospitals still in operation.While inpatient beds have been reduced asthe availability of community residentialplaces increased, no research has beenconducted to evaluate the utility andfunction of these residential facilities on anational level. While there has been localresearch to review communityaccommodation, for example within themental health services in the NorthernArea (Health Service Executive, 2004) andin the North West area (The SainsburyCentre for Mental Health, 2004), there islittle indication of the degree to which theresidents are satisfied with treatment andcare and other aspects of their lives or theextent of their autonomy.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 19

A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND20

CHAPTER 2Rehabilitation and Recovery:An Overview

2.1 INTRODUCTION
The following sections provide a briefoverview of the literature relevant to thestudy. Given the wide breath of the topicscovered and the vast amount of empiricalliterature in the areas, an in-depth reviewof the literature was beyond the scope ofthe study.
Traditionally, mental health services weredelivered mainly within a structuredhospital setting and physical treatmentsand medication were the main treatmentsprovided to patients. Very little attentionwas given to other aspects of the person’swellbeing in the way of addressing socialor occupational disabilities or follow-upand support on hospital discharge. In fact,the culture and the atmosphere ofpsychiatric hospitals were thought toexacerbate and add to the problems oflong-stay patients (British PsychologicalSociety, 2000). With the movementtowards community-based care, otheraspects of the person’s treatment andwellbeing needed consideration and this,in turn, led to the development ofcommunity psychiatry.
2.2 COMMUNITY PSYCHIATRYDEFINED
In the 1980s, following the move tocommunity care, Tansella (1986) definedcommunity psychiatry as
“a system of care devoted to a definedpopulation and based on a comprehensiveand integrated mental health service,which includes outpatient facilities, dayand residential training centres, residentialaccommodation hostels, shelteredworkshops and inpatient units in generalhospitals, and which ensures, withmultidisciplinary team-work, earlydiagnosis, prompt treatment, continuity ofcare, social support and a close liaisonwith other medical and social communityservices and, in particular, with generalpractitioners.”
Tansella’s definition thus included thesocial, physical and mental wellbeing ofthe individual. Szmukler and Thornicroft
(2001) argued that community psychiatryreferred to the work not only of themedical professionals, but of all mentalhealth professionals, including nurses,psychologists, social workers andoccupational therapists. They stressed thatcommunity psychiatry should providewhatever care and treatment is necessaryto meet the needs of a definedpopulation. They argued that the threefundamental principles underlyingcommunity psychiatry were:
Care and treatment should be providedto all in the population in relation toneed.
Evidence-based treatment should bedelivered wherever necessary and suchtreatment should be accessible to andaccepted by the patient.
Care and treatment involve a networkof elements addressing health andsocial care. Services required may beprovided by voluntary, private or publicsectors. The quality of the service willdepend on the interconnectedness ofthese elements.
The principle of a network of elements ofcare is very important, especially for thosewith persistent symptoms, which cancause distress for the individual and theirfamily. However, the reduction ofsymptoms is not necessarily sufficient tobring about an improvement in the qualityof life of the individual (Mikrim &Namerow, 1991). Social, cognitive andoccupational functioning can impactimmensely on the quality of life and thesocial inclusion of the individual. Problemsin functioning can occur as a direct resultof the disorder or indirectly, for example asa result of the side effects of medication,stigma, institutionalisation or socialexclusion. There is a need for a holisticapproach to treatment and care, asopposed to the traditional medicalapproach.
Thornicroft and Tansella (1999) define acommunity mental health service as
one which provides a full range ofeffective mental health care to adefined population, and which is
Chapter 2
Rehabilitation and recovery: an overview
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND22

dedicated to treating and helpingpeople with mental disorders, inproportion to their suffering or distress,in collaboration with other localagencies.
Quality of services must be evaluated onthe principles underlying communitymental health care. These principles, asidentified by Tansella and Thornicroft(2001), include:
Autonomy – the freedom to makeindependent choices despite thepresence of symptoms of disabilities
Continuity – the ability of services toprovide consistent interventions at thepatient level or at the local level
Effectiveness – proven interventionsoffered to patients
Accessibility – the ability of the servicesto provide care when and whererequired
Comprehensiveness – the ability ofservices to provide treatment and careacross a range of severities and patientcharacteristics
Equity – the fair allocation of resourcesfor services, based on needsassessment.
Accountability – the ability of servicesto meet the expectations of the patient,families and the wider public
Co-ordination – the ability of services toprovide a coherent treatment plan forpatients that include clear goals andinterventions that are needed andeffective. Services should be co-ordinated within an episode of careand between agencies
Efficiency – the ability of services toprovide economic efficiency byminimising the costs of inputs toachieve required outcomes or byincreasing the effectiveness or quality ofoutcomes on a fixed budget.
More recently, Thornicroft and Tansella(2004) argued for a balanced approach tomental health service provision that
includes both modern hospital-based careand modern community-based care. Thebalanced-care approach focuses onproviding services in community settingsand prompt admission to hospital-basedcare only when necessary. Care in thecommunity should be provided as close aspossible to the population served.
2.3 PSYCHIATRIC REHABILITATION
Concepts of community psychiatry andcommunity-based care highlighted theneed for services that were traditionallybased within the hospital to move to thecommunity. Rehabilitation services forthose with severe mental illness weretraditionally offered within the hospitalsetting. The rehabilitation and teaching ofskills within the artificial setting of thehospital did not readily transfer to theindividual’s real world on discharge(Anthony et al., 1982). Furthermore, asprogrammes were based in hospitals,patients had little opportunity to integratewith the local community. Theprogrammes were not aimed at theindividual’s needs and requirements, ratherthey tended to be offered on a groupbasis. This resulted in maintenanceprogrammes as opposed to programmesthat empowered the individual to move tothe next stage of independence. Psychiatricrehabilitation attempted to address issue.
Psychiatric rehabilitation is defined as aprocess that enables those who areimpaired, disabled or handicapped by amental disorder to reach their optimal levelof functioning in the community (WHO,1996). The level of functioning includessocial, occupational and economicfunctioning and aims to help the individualachieve as independent a life as possible inthese areas. Psychosocial rehabilitationaims to reduce sympotomatology and thenegative effects of medications, improvesocial competence, reduce stigma anddiscrimination, improve family and socialsupport and increase consumerempowerment (WHO, 2003). Therefore,psychosocial rehabilitation should not onlybe concerned with the rehabilitation of anindividual’s psychosocial functioning, but
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 23

should also address psychosocial factors ata service level such as policy and quality ofcare and at a societal level such as publicattitudes and legislation. Interventionsaimed at improving psychosocialfunctioning operate at the individual level.At the service level, psychosocialrehabilitation is concerned with policy,funding, staff training and quality of care.Legislation, user involvement and publicattitudes and opinions occur at thesocietal level of operation.
A programme of rehabilitation shouldinclude medical treatments and otherinterventions such as vocationalrehabilitation, social skills training, provenpsychosocial interventions and integrationinto the community (SchizophreniaIreland, 2003). The following interventionshave been identified as important in therehabilitation of the individual towards anoptimal level of functioning (WHO, 1996).Individuals should be able to access theseservices when and as they need them.
Pharmacological treatment – it isessential that appropriate medicationbe used for the reduction of symptomsand reducing relapse
Independent living skills and social skillstraining – these are most beneficialwhen offered in a real everyday setting
Psychological support to patients andtheir families – this includespsychological interventions aimed atproviding support and education toservice users and their families. It alsoinvolves the provision of informationregarding rights and the availability ofpsychosocial resources
Vocational rehabilitation andemployment – the importance ofemployment and training isemphasised. Training must be providedin a real-world context. Employmentcan take the form of shelteredemployment or supported employmentin the competitive job market.Supported work projects withorganisations have become thepreferred model of employment withinthe UK (Royal College of Psychiatrists,2003)
Social support networks – socialsupport has a positive role in themental health of an individual instrengthening the ability to cope.Individuals should be supported andencouraged to develop a social supportnetwork
Leisure – all individuals must have theopportunity to participate and enjoyleisure activities of their own choice.Access to activities and freedom ofchoice are essential.
Effective rehabilitation will involve medicaland other professionals. The currentrecommendation for staffing of an adultmental health rehabilitation service teamincludes a psychiatrist, mental healthnurses, mental health support workers,occupational therapists, social workers,clinical psychologists, cognitive behaviourtherapists, addiction counsellors, skilltraining staff, administration and staff forday centres and community residences (AVision for Change). There is a need for therehabilitation and recovery mental healthteam to work closely with other statutoryhealth and social services and voluntarygroups. For example, unmet housing andemployment needs can cause immensedifficulties for those with severe mentalhealth problems. Close liaison of therehabilitation and recovery mental healthteam with services that have a statutoryresponsibility in these areas is of greatimportance to the individual’s recovery.
The Royal College of Psychiatrists (2003)pointed out that rehabilitation servicesmust address issues of access to welfarerights and advocacy. There should be adetailed assessment which includes clinical,physical and social functioning, user andcarer aspirations, psychiatric history, andrisk assessment and management. Fromthis assessment an individual care planshould be drawn up and a key workerassigned to the individual. Assessmentsshould involve the individual and in somecases, with the consent of the individual, arelative or advocate (Schizophrenia Ireland,2003). Components of the rehabilitationprogramme should be accessed when theyare needed and the interventions shouldbe detailed in the care plan. Needs should
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND24

be regularly reviewed and the care planamended as necessary (Department ofHealth, 2000).
To summarise, psychiatric rehabilitationrequires a comprehensive range ofmedical, psychological and social therapiesaimed at the needs of the service user. AVision for Change recommends thatmultidisciplinary community mental healthteams should include the ‘core skills ofpsychiatry, nursing, social work, clinicalpsychology and occupational therapy’. Itfurther argues that the principle ofrecovery should underlie the work ofmultidisciplinary rehabilitation communitymental health teams. The following sectionelaborates on this principle.
2.4 THE SERVICE-USER MOVEMENTAND RECOVERY
There are now growing service-usermovements in the UK, Ireland andelsewhere. Within Ireland the usermovement is evident in SchizophreniaIreland (SI), Support-Training-Education-Employment-Research (STEER), MentalHealth Ireland (MHI) and the IrishAdvocacy Network. The aims of the usermovement include: to encourage self-help,to challenge assumptions about mentalillness, to engage in advocacy and tocampaign for improved services and tocombat stigma. The user movementadvocates that a sense of control overone’s life is important, and holds thatthose who rely on services for support areoften placed in a dependent position. Themovement proposes that those who haveexperienced mental health problems havegained an expertise that can be of greatbenefit to others. People who have hadpsychotic experiences can co-educateothers who have psychotic episodes, aswell as mental health professionals andthe public, so that these experiences canbe viewed in a more positive light.
Recovery has been the topic ofphilosophical debate over the last 20 yearsand is an important concept within theservice-user movement. The most widelyaccepted definition of recovery is that of
Anthony (1993) who said that recovery is‘a deeply personal, unique process ofchanging one’s attitudes, values, feelings,goals skills and roles. It is a way of living asatisfying, hopeful, and contributing lifeeven with limitations caused by illness’.The recovery approach focuses on theindividual’s personal path of recovery(Roberts & Wolfson, 2004) and the processby which the person adapts to living withmental health difficulties. The principle ofrecovery requires mutual respect across allservice levels and the belief that all serviceusers can gain control over their lives andparticipate fully in the community. Theprocess of recovery is most eloquentlydescribed in personal narratives and theviews of ‘experts by experience’ (Ralph etal., 2002).
Efforts to measure recovery are still at anearly stage of development. While scaleshave been developed to measurerehabilitation in terms of sympotomologyand social functioning, no quantitativemeasure exists whereby the concept ofrecovery can be measured. The concept ofrecovery is a complex one and, therefore,to assess it using a single measure isdifficult. The recovery approach does notdismiss the importance of medical ormental health professionals (Roberts andWolfson, 2004; Liberman and Kopelowicz,2005). Rather the approach sees the roleof the professional as providing support bylistening to the individual’s life story andhelping them identify necessary resourcesand skills training. The move to a recovery-oriented service involves a change in therole of the professional from ‘expert andauthority figure’ to ‘coach or personaltrainer’ (Anthony, 1993). The role of theprofessional is not to ‘do things topeople’, as was in the past, but rather tolisten to the individuals who areexperiencing symptoms and advise themon appropriate interventions that bestmeet their needs. Professionals can offerskills and knowledge while at the sametime listening and valuing the service useror ‘expert by experience’. It is no longeracceptable that the people using mentalhealth services remain passive users of theservice (Anthony, 1993). Care providersmust realise that ‘each person must be incharge of and responsible for his or her
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 25

own recovery’ (Copeland, 2006). Copelandargues that there is a need for mentalhealth service users to learn their rights –those that ‘most people take for granted’and to ‘speak out’. These include the rightto choice and the right to determine whatbest meets their needs. It must be noted,however, that many people will have beenin a service that for the most part hasignored their voices, therefore training andeducation in the principles of recovery arenecessary.
The move to a recovery approach inmental health services has been slow, buthas gathered some momentum in recentyears. For example, the Royal College ofPsychiatrists, (2003) in the UK emphasisedthe importance of the principles ofrecovery in redefining rehabilitationservices, as did A Vision for Change inIreland. A Vision for Change states that ‘astrong commitment to the principle of“recovery” should underpin the work ofthe rehabilitation CMHT – the belief that itis possible for all service users to achievecontrol over their lives, to recover theirself-esteem, and move towards building alife where they experience a sense ofbelonging and participation’.
A recent study on service users’ viewshighlighted the lack of a recovery-orientedmental health service in Ireland(Schizophrenia Ireland, 2006), with service-users reporting little choice in their mentalhealth treatment. The MHC (2005b)stimulated debate on the recoveryapproach in Ireland with the discussionpaper A Vision for a Recovery Model inIrish Mental Health Services. It is envisagedthat, following feedback fromstakeholders, service providers and serviceusers, a position paper on the role of therecovery approach in mental healthservices in Ireland will be published. Thisdiscussion paper highlighted importantdevelopments and advances in othercountries for a recovery-oriented service.
In the absence of a comprehensiverehabilitation and recovery-orientedservice, aspects of recovery such asemployment, housing and social isolationwill be neglected. The importance of aservice that actively promotes and
encourages recovery and rehabilitationfrom mental illness cannot be over-stressed. There is a need to move awayfrom the traditional maintenancerehabilitation model to a model thatemphasises recovery, instils hope andempowerment and encourages users togain control over their lives and achievetheir own life goals. Rehabilitation servicesshould have multiple points of access andshould offer choices to service users.Rehabilitation services should emphasise apartnership between service users andservice providers. The MHC in it’sdiscussion paper highlights that the‘recovery model’ in mental health servicesemphasises the expectation of recoveryfrom mental ill health and promotes bothenhanced self-management for serviceusers and the development of serviceswhich facilitate the individual’s personaljourney towards recovery. As discussed byboth the MHC discussion paper (2005b)and A Vision for Change, there is a needfor the mental health services in Ireland toadopt a recovery-oriented approach.
2.5 SOCIAL INCLUSION
The importance of social inclusion forrecovery from mental illness cannot beoverstressed (Warner, 1985). Socialinclusion refers to the right of theindividual to participate in all areas ofsociety and the community that they live inand to access services that are provided inthat community. Unless individuals canavail of these rights, their participation inthe community is limited and therefore,recovery inhibited. Social exclusion isdefined as ‘a series of problems that areinterconnected and include poverty,discrimination, unemployment, low skills,poor housing and poor health’ (Rankin,2005a). The Irish National Action Planagainst Poverty and Social Exclusion2003–2005 is an important document thatidentified specific targets for addressingsocial exclusion in Ireland (Office for SocialInclusion, 2003).
People with mental health problems areone of the most excluded groups insociety, whether they live in the hospital or
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND26

the community (British PsychologicalSociety, 2000). Those experiencing mentalhealth problems should have the samebasic rights of access to education andemployment as others in society, buttypically do not exercise these rights. Thedependence on state benefits can oftenresult in further exclusion from servicesbecause of poverty and other factors. Astudy of people attending long-term daycare found that one-third did not use anyrecreational facilities (e.g. libraries, pubs,public leisure centres, community centres)and a small but significant percentage didnot use public services such as shops, postoffice and public transport (Brugha et al,1988). The evidence suggests that socialexclusion can exacerbate clinical symptomsand social functioning and thatimpairments thought to be a direct resultof the illness can in fact be due to socialfactors (British Psychological Society,2000). Furthermore, those with mentalhealth problems are one of the groupsthat have benefited least from policies thattackle disadvantage in the UK (SocialExclusion Unit, 2004). Within the Irishcontext, the Irish National Action Planagainst Poverty and Social Inclusion 2003– 2005, failed to identify those withmental illnesses as a vulnerable group(Office for Social Inclusion, 2003). Therewere no specific targets set in relation tothose with mental health problems and,thus, the potential of the policy for thispopulation will not be realised. A Visionfor Change highlights the cycle ofexclusion for those with mental healthproblems. This cycle can lead towithdrawal from society, which in turnmay lead to reduced quality of life,worsening mental health, loss of socialnetworks, poverty and unemployment.Mental health problems are often episodicand prone to recur resulting in loss ofincome, loss of employment andconsequently poverty. In addition, thedevelopments of social contacts at workand in the community are oftenhampered.
2.5.1 Stigma and discrimination
Stigma and discriminationassociated with mental ill health ispervasive and more than forty
negative consequences of stigmahave been identified (Byrne, 1997).These include discrimination inhousing, employment andeducation. Furthermore, it can leadto incidences of harassment forthose living in the community. Astudy by MIND found that 50% ofrespondents with mental healthproblems had experiencedharassment in the community andworkplace (Read & Baker, 1996). Amore recent study by Berzins et al(2003) found that people withmental health difficulties were twiceas likely to experience harassment aspeople in the general population.Many of the fears and prejudices ofthe general public are based onmyths about ill health (SocialExclusion Unit, 2004; Commission ofEuropean Communities, 2005).Individuals can experience stigmaand discrimination even aftersymptoms have subsided (SocialExclusion Unit, 2004). In anAustralian study, service users andtheir families identified ‘less stigma’as the most important thing thatwould improve their lives (cited inHocking, 2003), suggesting thatstigma can act as a barrier towardsoptimal recovery. Furthermore, theyreported that it was not just stigmafrom the community that affectedtheir lives, but also stigma fromhealthcare workers. Educationprogrammes aimed at tacklingstigma and discrimination haveshown positive results (Wolff et al.,1996). The National Institute forMental Health in England (NIMHE,2004) published a five-year strategyaimed at tackling stigma anddiscrimination. The strategy is basedon international evidence and istargeted at young people, media,health and social care providers,public and private organisations andthe voluntary sector. Mental HealthIreland has run a debatingcompetition to increase awarenessof mental health problems insecondary schools. In addition,Schizophrenia Ireland (2005)
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 27

launched a media-watch campaignto challenge the way schizophreniais portrayed in the media. NewZealand campaigns aimed attackling stigma have included theLike Minds project. Increasedcontact between the communityand those with mental healthdifficulties has been shown toreduce the prejudice and stigmaassociated with mental illness(Couture & Penn, 2003). A Vision forChange recommended that issues ofstigma and discrimination beaddressed by developing andputting into action evidence-basedprogrammes for the widercommunity.
2.5.2 Social isolation, communityintegration and participation
People with mental health problemsreport high levels of social isolation(MIND, 2004) and this is especiallyso for those with severe andpersistent mental illness. Individualsin community residential facilitiestend to have smaller social networksand these networks tend to bedominated by staff, professionalsand other residents as opposed tofriends from outside the services(Goering et al, 1992). The socialnetworks of those with severemental illness are significantlysmaller than those of age-matchedcommunity controls (Becker et al,1997). In addition, those withmental illnesses who have smallernetworks tend to have morehospitalisations and make less use ofexternal services (Becker et al.,1997). Social networks improve forthose who participate inprogrammes directly aimed attargeting social networks(Thornicroft & Breakey, 1991).
In terms of social integration, thoserelocated to community facilitiestend to show an increase in contactwith non-mental health services andengage in more leisure and socialactivities in the community(Shepherd & Murray, 2001).
However, the advantages of socialintegration may depend on thequality of the interactions asopposed to the quantity. An Italianstudy found that the number ofactivities offered in communityresidential facilities did not correlatewith the residents’ clinical and socialfunctioning (de Girolamo et al.,2002). It has been reported thatcommunity integration can beincreased by moving activities (e.g.leisure, art) normally provided inmental health day facilities into thecommunity and by providingactivities in which the widercommunity can partake (Shepherd &Murray, 2001).
The Values to Action programmehighlighted in A Vision for Changewas specifically designed to addresspoor self-image, one of the factorsthat may prevent people fromintegrating and participating in thecommunity. This programme wasoffered to mental health serviceusers and staff. The staff felt that itenriched their role as mental healthprofessionals and positive effects forthe service users were alsoillustrated.
2.5.3 Employment
Those with mental health problemsoften find it difficult to secure orretain competitive employment.Competitive employment refers to aregular job, supervised by theemployer, for regular wages and inan integrated work setting (Drake etal, 1999). The reported US rates forcompetitive employment of thosewith mental illness are low, and aretypically less than 15% (cited inDrake et al., 1999). In the UK, anemployment rate of 24% for thosewith long term mental healthproblems has been reported (Rankin,2005b). Yet research shows that alarge proportion, between 60% and70% of those with severe mentalillness want to work in mainstreamemployment (Rankin, 2005). Thebarriers to employment include low
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND28

self-esteem, low expectations ofservice users by staff, employerattitudes and difficulties movingfrom benefits to work (SocialExclusion Unit, 2004).
There is now a variety of services tomeet the vocational andoccupational needs of those withmental health problems. Theserange from day centres to supportedemployment programmes.Historically, sheltered workshops andday centres were provided by mentalhealth services as an alternative tocompetitive employment. Shelteredwork programmes include manualnon-skilled work and skilled worksuch as carpentry, while day centrescater for the social care of theindividual and may also providevocational training. These workshopsare based on the premise that thosewith severe mental illness areunsuited to competitive employmentwhere the stress of the workplacewould have detrimental effects ontheir mental health. Most often,individuals tend to become trappedin sheltered work programmes andthe transition to competitiveemployment is never achieved(Drake et al, 1999). The pre-vocational workshops or ‘train andplace’ programmes are provided inthe mental health centre or similarsetting and are aimed at providingthe individual with the necessaryskills for the real workplace. It isassumed that through theseworkshops the individual will gainthe necessary skills for competitiveemployment in the real world. Theseprogrammes train the user on theassumption that the skills aretransferable to the real workplace,with the goal of finding placementin competitive employment.However, the success of the transferof skills from artificial environmentsto real-world settings is still beingdebated. Two types of open workprogrammes that are implementedin real-world settings and comeunder the ‘place and train’ model ofemployment, are the social co-
operatives and transitionalemployment. Social co-operativesare non-profit-making organisationsthat provide a valuable service to thecommunity and employ anintegrated workforce. The workforceis paid by the social co-operativesand the organisations receive asubsidy for each worker. Thetransitional employment modelprovides mental health service userswith part-time and time-limitedplacements in the community. Theservice users are paid the prevailingwage, directly from the employer.The purpose of these programmes isto aid transition to competitiveemployment, develop the curriculumvitae and improve self-esteem. Verylittle scientific evidence for thesuccess of these models exists(Thornicroft & Tansella, 2003).However, a study by Corrigan andMcCracken (2005) showed that aplace and train model increased theability of people to attain theiremployment and housing goalscompared with the traditional modelof train and place.
More recently the supportedemployment model, as opposed tothe traditional shelteredemployment model, has become thepreferred model of employment forthose with severe mental illness.Research findings showed thatsupported employment modelsresulted in higher levels ofcompetitive employment and higherearnings and that these positiveeffects increased over a 24-monthperiod (Cook et al., 2005). Thesupported employment model of‘place and train’ proposes thatindividuals be placed in competitiveemployment and trained in thenecessary skills. It emphasises aclient-centred approach withemployment specialists workingclosely with case managers andclinical teams. The team approachprovides practical assistance infinding and maintainingemployment. A Vision for Changehighlighted the importance of the
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 29

‘place and train’ model. Anotherapproach within the supportedemployment model is the ‘choose,get and keep’ approach (Bond et al.,1997). This approach emphasisescareer planning and choice ofclients. As the name suggests, theapproach helps clients to set goals,job search, choose suitableemployment and secure placements.Ongoing support in terms of skilldevelopment and interventionswhen necessary is provided.Supported employment for peoplewith severe mental illness is anevidence-based practice withresulting benefits for the individual’sclinical and social functioning (Bond,2004). The benefits of supportedemployment include improved self-esteem and better symptom control.It has recently been recommendedthat mental health services shouldinclude a variety of vocationaltraining and employment optionsdepending on user needs andaspirations. These options includeapproaches from both the shelteredemployment model and thesupported employment model(Thornicroft & Tansella, 2003). It isargued that choice and variety areimportant factors and that someform of meaningful activity isbeneficial to the client’s wellbeing,be that paid employment, voluntaryemployment or education and skillsdevelopment (Rankin & Regan,2004).
2.6 HOUSING MODELS OFRESIDENTIAL CARE
Johnson (2005) argued that qualityhousing is of paramount importance incommunity care and that safe and securehousing is one of the key factors for betterquality of life and a ‘place’ within the localcommunity. Shepherd and Murray (2001)argued that an adequate range ofresidential accommodation is at the coreof attempts to develop community-basedsystems of care. The policy of bedreduction in hospitals in Ireland was
accompanied by an increase in theresponsibility of the mental health servicesfor the management and provision ofalternative accommodation for those inneed. Two main models of housing areprovided for those with severe mentalillnesses – the sheltered housing modeland the supported housing model.
2.6.1 Sheltered housing model
During the 1980s the prevailingmodel for community care was thecontinuum model, otherwise knownas the sheltered housing model(Carling, 1993). Adherents of thismodel proposed that a variety ofresidential facilities should becreated to provide a linearcontinuum of care from high to lowlevels of restrictiveness (Drachman,1981; Wing & Furlong, 1986). Thiscontinuum model of care assumedthat residents would move fromhigh support to low support, withthe final outcome beingindependent living in thecommunity. Within this model therange of residential accommodationproved difficult to categorise.However in a UK study, Lelliott et al,(1996) proposed categoriesdepending on level of staff cover,number of beds and staff to residentratio. Four categories of communityresidential facilities, ranging fromhigh support hostels to grouphomes were proposed. The majorityof sheltered residential facilities nowuse these categories, or a version ofthem. The categories include:
High support residences havenursing staff present 24 hours aday, with staff remaining awakeat night-time;
Medium support residences arestaffed 24 hours a day, with staffsleeping at night-time;
Low support residences are notstaffed, but on-call staff areavailable when necessary. Staffvisit on a regular basis during theday;
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND30

Group homes are the leastrestrictive and are not staffed,although staff visit regularly.
The category of medium supportresidences in Ireland differs fromthat described above. Some mediumsupport residences are not staffedthroughout the day or at night, buthave staff visiting daily. Othermedium support residences havesupervision at night by non-nursingstaff. The low support residencesand group homes have staff visitingoccasionally. The lack of astandardised definition of supportlevels in Ireland has been a cause ofconcern. Definitions of levels ofsupport adopted by this study werethose put forward by theconsultants of the specialisedrehabilitation and recovery mentalhealth teams and are detailed inChapter 3.
The sheltered housing model ofresidential care has been stronglycriticised by Carling (1993). Heargued that the model confuseshousing and treatment needs.Furthermore, alternative housing isoften not available at the precisetime that the person’s need changesand frequent relocation can oftenupset or disrupt aftercare and socialnetworks. The findings of studiesinvestigating mobility betweenresidential facilities do not supportthe sheltered housing model. AnItalian study found very littlemobility between residential facilities(de Girolamo et al., 2002) andresults from a UK study indicatedthat residential facilities willprobably be ‘homes for life’ for themajority of residents (Trieman et al.,1998). Likewise, Geller and Fisher(1993) in the US argued that thecontinuum model of residential carewas never actualised and failed tofunction in the way in which it wasintended. They found that only7.9% of people were in residentialplacement that was less restrictivethan their placement four yearspreviously. Of the residents who
were judged as potentially suitablefor independent living, only 16%were living independently at follow-up four years later.
Noteworthy is the comment made inthe Report of the Inspectorate ofMental Hospitals (Department ofHealth and Children, 2004)regarding dependency and lack ofmobility within the communityresidences:
“The Inspectorate had beenstruck by how little rehabilitationtook place in the communityresidences and how theirmanagement was orientedtowards continuing care, ratherthan decreasing dependency. “
The report went on to add that theresidences were over-staffed, did nothave the proper skill mix of staff andthat there was little investment inoccupational rehabilitation ortraining for the residents.
2.6.2 Supported housing model
The supported housing model hasreplaced the notion of transitionalcare inherent in the shelteredhousing model. This modelemphasised permanent andsupervised housing arrangementsand has been widely accepted in theUS and UK (Trieman et al, 1998).Advocates of the supported modelproposed that independent livingfacilities be made available andservices recently termed ‘floatingsupports’ be provided depending onthe individual’s level of need(Johnson, 2005; Rog, 2004). Animportant feature of the supportedhousing model is that return toindependent living is not consideredthe ultimate goal. It isacknowledged that some residentswill not return to independent livingand that the provision of a flexiblesystem of support allows for afluctuating level of need. Thus, theobjective of the intervention differsfrom that of the sheltered housingmodel of return to independent
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 31

living. The Supporting PeopleProgramme in the UK recognises theimportance of the supportedhousing model and of identifyinglocal service need and co-ordinatingfunding for all supported housingservices.
In summary, the sheltered housingmodel requires residents to move toa house to avail of different levels ofsupport according to changingneeds, while the supported housingmodel advocates permanency ofhousing for residents and a flexiblesupport service that can be availedof when necessary to meet changingneeds. In both models, a problemmay arise if support is not matchedto need. If needs are overprovidedfor, this may have negativeconsequences for the individual’sfunctioning. It is suggested that,rather than having one model ofcare, both models could beincorporated in a service to suit theneeds of individuals (Geller & Fisher,1993; Johnson, 2005). For example,transitional housing may bebeneficial to those who have beenin long-term care and who requirevarious levels of rehabilitation beforemoving to independent living.Supported housing may be moresuitable to people who have notbeen hospitalised for long periods oftime, but who may need a flexiblelevel of care. Research investigatingthe effectiveness of supportedhousing versus other housingapproaches has been scarce andequivocal (Shepherd & Murray,2001; Rog, 2004). It would appearthat housing with supports in anyform increases housing stability,decreases homelessness anddecreases hospitalisation (Rog,2004). In addition, health care costsare reduced for those in higher-quality housing and neighbourhoods(Harkness et al., 2004). Furthermore,research suggests that the density ofhouses for socially marginalisedgroups, such as those with mentalhealth problems, can affect re-hospitalisation rates and reduce
demand for mental health serviceinterventions (Johnson, 2005). Toomany houses in the same area maycreate a ghetto, while too few canlead to isolation and socialexclusion.
2.7 PROVISION OF HOUSING ANDCARE
Aside from the housing model adopted,the responsibility for the provision ofhousing within the mental health serviceshas been an issue of debate for a numberof years. The most common practice inIreland has been that mental healthservices provide both housing and care.During the deinstitutionalisationprogramme, the mental health servicesprovided housing for those beingrelocated from psychiatric hospitals. Thishousing was also used and continues tobe used for those who come into contactwith the mental health services and whocannot live without some form of support.A Vision for Change argued that localauthorities should provide housing forservice users in need, which is theirobligation under the Housing Act 2002.However, the provision of housing by themental health services has unfortunatelyresulted in reducing the chances of localauthority housing for these individuals. InSweden (Brunt & Hansson, 2004), housingfor those with mental illnesses is providedby local authorities, while care is providedby health services. However, the UKprovides an alternative model ofindependent sector providers.
2.7.1 Social housing in Ireland
The history of social housing inIreland dates back to the Housing ofthe Working Classes Act of 1890.This legislation put in placemechanisms for allowing, if notobliging, local authorities to providehousing in urban areas. However,little progress was made until theHousing Act of 1919, wasintroduced which obliged localauthorities to provide housing whereit was needed, with the addedincentive that subsidisation became
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND32

available from central sources.
During the 1930s, large scaleprovision of urban housing forworking people saw theestablishment of housing estateswhere occupiers became tenants ofthe local authority on a rental basis.People were placed on a housing listin the growing local authorityprovision. This was the genesis ofthe waiting list phenomenon whichpersists to this day and which reliedheavily on a points system indetermining priority for families onthe list, with points being allocatedon the basis of number of children,health and other considerations.Progress slowed during the war of1939 – 45 but accelerated in the1950s and 1960s, and the legislativeframework within which localauthorities operated was extendedand modernised by the Housing Actof 1966.
Possibly because the existingarrangements were perceived asencouraging dependence andinhibiting self-determination andbecause of financial considerations,two main considerations enteredthinking in relation to local authorityprovision and central funding. Thefirst was the encouragement ofvoluntary involvement, partly on apublic/private basis, and the secondthe encouraging of tenants tobecome purchasers and owners ofrented property. This new thinkingwas ratified in policy documentssuch as A Plan for Social Housing of1991 and Social Housing – the WayAhead of 1995. This latterpublication aspired to an annualsocial housing provision of 7,000new homes. The limiting factor inthis aspiration was the rising price ofland acquisition, the hoarding ofland banks and increasingconstruction costs. In face of theseconsiderations and problems, aseries of further reports issued,collectively called The BaconReports, the last of which, Action onHousing, appeared in 2000. The
National Development Plan 2000 –2006 included housing as animportant element and allocatedfour billion Euro for social andaffordable housing with theambition, inter alia, of commencing23,000 new social housing units inthe local authority, voluntary and co-operative housing sectors over thethree years 2006 to 2008. ThePlanning and Development Act of2000, inter alia, empoweredplanning authorities to set aside20% of housing developments forsocial and affordable housing andobliged local authorities to deviseand implement housing strategies.Finally, the Department of theEnvironment published in 2005 adocument titled Housing PolicyFramework – Building SustainableCommunities in which there was anacknowledgement of the specialhousing needs of several groups,including persons with disabilities,encompassing persons with mentalhealth disabilities, although thisgroup was not specificallymentioned.
The central body charged withresponsibility for housing issues isthe Department of the Environment,Heritage and Local Government. TheDepartment has a number ofsections which impact on groupssuch as the elderly, travellers, etc,including the Housing Policy Sectionand the Social Inclusion Section,both based in headquarters inDublin and the Voluntary HousingSection located in Ballina. TheGovernment’s Homelessness: AnIntegrated Strategy obliges localauthorities to draw up action plansto provide a coherent response tohomelessness. The Departmentassists local authorities to providehousing through its CapitalAssistance Scheme, but themanagement and the maintenanceof local authority housing is theauthorities’ own responsibility. TheCapital Assistance Scheme has beensomething of an ad hocarrangement and needs
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 33

establishment on a continuing basisto remove uncertainty from thefunding it provides.
While officially there are currently45,000 – 50,000 persons awaitinglocal authority housing, there isscepticism in some quarters aboutthe validity of this figure and a beliefthat the real number is substantiallylower. It was reported that thosepersons who constitute familygroupings can, at least in the Dublinarea, be housed almost immediatelyalthough not necessarily in theirlocation of choice. In contrast astudy investigating social housingneeds in a peripheral rural areaargued that local authority housinglists grossly underestimate thehousing need (Heaune, 2006). Theauthor reported that people for avariety of reasons do not apply forlocal authority housing, especiallythose requiring special needs orsheltered social housing. To add tothis, families are given priority in theallocation of local authority housing.Housing single persons who do not,in the ordinary sense, comprise ahousehold, poses more difficulties,although authorities are embarkingon providing apartments rather thanthe conventional three-bed roomedhouse hitherto regarded as thenorm. In addition, some housingauthorities consider persons inmental health community residencesas housed and therefore not in needof housing, despite the fact that asmall, but unknown, proportion ofresidents, particularly in grouphomes, are already on the housingwaiting list. Additionally, localauthorities view persons withpsychiatric histories as potentiallytroublesome and feel that, even ifthey were to provide for them, theywould get inadequate support fromthe mental health services in caringfor their mental health needs. Asrecommended in A Vision forChange there needs to be closeliaison between local housingauthorities and mental healthservices to ensure that those who
need housing are housed and thatsufficient care and support isprovided to ensure wellbeing andsuccessful tenancy.
It has been the rule that grouphomes have housed three to fourpersons and there is no reason whythis grouping should not constitutea household for local authorityhousing purposes to avoid theobvious hazards of placing a personwith mental health problems in theisolation of a single-occupancyapartment. Recently, novel schemesinvolving housing authoritiesentering into arrangements withlandlords to provide tenancysustainment services where theinterest of the tenant are progressedand supported by the localadministration are being developed.
In its preventative strategy targetedat specific groups the HomelessAgency includes ‘people leavingmental health residential facilities’and sets out that all psychiatrichospitals will provide a formal andwritten discharge policy to serviceusers and carers. Psychiatric teamswill have a nominated professionalacting as discharge officer andrecords will be kept of patientsdischarged and the accommodationto which they are being discharged.As distinct from prevention asenvisaged above, there is noreference to the housing authorities’responsibility to provide for thehousing requirements of thosebeing discharged. In effect, it mightbe conceived that the documentbars the discharge of patients whoare homeless and requires thehospital or the mental healthservices to act as housing agents. Inrelation to providing for thementally ill homeless in Dublin anumber of specialist teams havebeen established. A Vision forChange recommended two full-timemultidisciplinary teams for theDublin area.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND34

In no housing policy document isthere a specific provision for thehousing of persons with mentalhealth problems and consequentlythe majority of the housing forthose with mental illness in need ofhousing is provided by the mentalhealth services. The mental healthservices provide most housing eitheron an owned or rented basis.However, a small housing stock,usually of three- to four-bedroomhouses, for group home purposes isprovided by some local housingauthorities. In addition, a number ofprojects have been undertaken andrealised by voluntary housingagencies, with some forming localhousing associations, mostly withsubstantial grant aid from theDepartment of the Environment,Heritage and Local Government.
2.7.2 Housing provision for thementally ill in the UK: analternative model
In the UK, the National HealthService (NHS) and Community CareAct enabled agencies other than theNHS and local authorities to becomeinvolved in operating and managingresidential facilities. This resulted ina greater involvement of non-statutory agencies (Shepherd &Murray, 2001). A large amount ofaffordable housing for those withmental health problems is providedby Registered Social Landlords.These may be industrial andprovident societies, registeredcharities or companies. There are anumber of different managementand care arrangements for this typeof housing. Firstly, the sociallandlords may hand overmanagement responsibilities tovoluntary organisations who takeresponsibility both for the housingmanagement and care services.Secondly, the social landlord maytake control of the housingmanagement while entering into asupport agreement with a careagency to provide care services.Alternatively, what is becoming
more common, the social landlordprovides housing management andcare services without theinvolvement of external agencies.Given the vast range ofmanagement and care providers, theNational Housing Federation and theMental Health Foundation(NHF/MHF) have produced ahousing, care and support code(1996). The code lists 12 standardsthat organisations should commit toin order to achieve reliability andgood quality in the care theyprovide. The Sainsbury Centre forMental Health (Warner et al.,1997)produced a report on good practicein the provision of housing andsupport for people with mentalhealth problems. This report coversall aspects of good practice, fromthe rights of the residents, stafftraining, individual care plans andthe physical environment to theevaluation and monitoring of thesesupported housing arrangements.
In 2005, the Office of the DeputyPrime Minister (ODPM) published aguide to accommodation andsupport options for people withmental health problems. This guidediscussed the support needs ofpeople with mental healthproblems, the services provided bythe Supporting People Programmeand the range of housing andsupport options that are available.The purpose of this guide was toensure that decision makers andhealth service providers were awareof and had access to importantinformation on the range of servicesand options available to meet theneeds of the service user.
Research on the evaluation of thistype of provision (i.e. interagencyworking) has been limited andresults have been equivocal. One ofthe first problems identified wasthat these services tended to takethe ‘easier’ clients, leaving it moredifficult to place those thought tobe more ‘difficult’ (i.e. those withco-morbid problems, those who had
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 35

contacts with police, those who haddifficulties engaging with services)(Shepherd & Murray, 2001).Effective partnerships betweenstatutory and non-statutory agenciesrequired close interagencydevelopment. However as Shepherdand Murray (2001) point out,interventions for achieving effectivepartnerships have received littleattention. The selection, recruitmentand training of staff andmanagement also have receivedlittle attention in terms of evaluativeresearch. Finally, the expectations ofresidents and their preferences interms of care have received littleconsideration. The NHF/MHFhousing care and support codeaddresses all these issues. The code,however, was intended as avoluntary guide for those providinghousing and care and to rewardthose organisations that met thestandards. The Sainsbury report(Warner et al., 1997) provides goodpractice guidelines on how toachieve these standards.
2.8 STAFF TRAINING INRESIDENTIAL CARE
Studies have shown that a largeproportion of the staff in communityresidential facilities have no formal trainingin mental health (de Girolamo & Bassi,2004; Lelliott et al., 1996). One UK surveyreported that over half of the staff had notraining, not even in risk or violencemanagement (Lelliott et al., 1996). Thismay be advantageous in that ‘institutionalattitudes’ are not present. However, if thestaff are not trained to deal with difficultsituations, a residential facility may have toimpose stricter selection criteria, resultingin difficult-to-manage individuals beingrefused admittance. The PRISM PsychosisStudy (Thornicroft et al., 1998) carried outin the UK argued that the quantity of thestaff was not as important as the qualityof the staff. It is more important to havethe proper skill mix of staff, includingpsychiatrists, psychologists, nursing staffand care staff (Department of Health and
Children, 2006). In addition, all staffwithin residential facilities, regardless ofprofession or grade and including qualifiedand non-qualified staff, should be trainedin the competencies and principles ofrecovery (MHC, 2005b). A documentpublished by the New Zealand MentalHealth Commission (2001) outlined thecompetencies necessary for mental healthcare workers and the Mental HealthCommission in Ireland stressed that this isan invaluable document for services thatare moving towards a recovery-basedservice.
As already mentioned, effectiveinteragency co-operation is necessary toprovide a comprehensive and seamlessservice. This should include health andsocial workers, housing agencies,occupational providers, primary care teamsand police and probation officers. Itshould be borne in mind that the greatmajority of staff in Irish communityresidences, whether based therein orcalling in on a daily basis, are trainedpsychiatric nurses who nevertheless requiremore specialised training in rehabilitationskills and in the competencies andprinciples of recovery.
2.9 RESIDENTIAL CARE IN THECOMMUNITY: A RESEARCHOUTLINE
Three main studies of the provision, rangeand adequacy of community mental healthcare facilities have influenced themethodology and procedures of thepresent study. Two of these were carriedout in the UK (Lelliott et al., 1996; O’Driscoll & Leff, 1993; Donnelly et al.,1994) and one in Italy (de Girolamo et al.,2002). Both the UK studies surveyed asample of residential facilities, while theItalian study surveyed communityresidential facilities throughout Italy.
In the UK, the Team for the Assessment ofPsychiatric Services (TAPS) was establishedin 1985 to oversee and evaluate the movefrom hospital care to community care (O’Driscoll and Leff, 1993). This longitudinalstudy investigated the transition from
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND36

hospital to community care over a five-yearperiod. The findings regarding progressionfrom high support hostels to low supportand eventually to independent livingshowed very little mobility betweendiffering levels of care, with 61% of theformer patients remaining in the originalplacements. The authors proposed that, atleast for patients who were resettled fromhospital care, these hostels remained‘homes for life’ for many (Trieman et al,1998). Findings in relation to clinical andsocial outcomes were more positive (Leff &Trieman, 2000). While there was nochange in the patients’ clinical state or inproblems of social behaviour, the residentshad gained domestic and communityliving skills. A high percentage (84%)reported satisfaction with their currentcommunity accommodation and wished toremain there. Increases in social networksand more intimate relationships in thecommunity were evident over the five-yearperiod. Physical health declined for someresidents, which was attributable to theage profile of the study group. This studywas valuable in that it included measuresdirectly aimed at the residents’ views oftheir lives including accommodation andtreatment. Regarding staff, in line with thefindings of Lelliott et al, (1996), this studyrevealed that the majority of care staff hadno formal qualifications. Training needswere not being met and there were fewcareer opportunities (Senn et al., (1997).Staff reported that while formal trainingwas offered, it was often impossible toavail of due to limited budgets andworkloads. This large-scale studyhighlighted the benefits of communitycare for long-stay patients resettled fromlarge psychiatric hospitals.
A similar study was carried out in NorthernIreland – Opening new doors - to evaluatethe move to community care (Donnelly etal., 1994). Interestingly, this study foundthat the majority of the patients went tostaffed accommodation even though theyhad quite high skill levels. The skills level ofthe residents did not change over a two-year period and very few had moderate ormajor difficulties with daily living skillsafter six years (Donnelly at al., 1997). Inaddition residents’ views indicated thatthey preferred the community
accommodation over hospital and weremore satisfied with their lives, felt healthierand felt more independent (Donnelly etal., 1996). Regarding social supportnetworks, a large proportion reported thatthey had no friends outside of theresidence, twelve months followingdischarge, suggesting that residents werenot easily integrating into the localcommunity. The utilization of services 6 –12 months following relocation showedthat general practice, communitypsychiatric nurses and social workers werethe mostly used services. Approximately aquarter were attending day centres andclubs, while only a small minority hadgained open employment or shelteredemployment (Mc Gilloway and Donnelly,1998).
The Mental Health Residential Care Studyby Lelliott et al., (1996) assessed theprovision of residential facilities withincommunity mental health services in theUK. This study employed a facilityquestionnaire and resident questionnaire.The facility questionnaire was gathered byinterviewing service managers, while theresident questionnaire providedinformation for each resident from theindividual’s key worker. In terms ofcommunity residential facilities, the mainfinding was the categorisation of facilitiesinto high, medium and low support, basedprimarily on the staff to resident ratio andthe extent of cover. There was widevariation in the training of staff, with morethan half of the staff having no formalqualifications. There was very little supportfrom external services, such as visits frompsychiatrists, psychologists, social workersor community psychiatric nurses. Themajority of residents had long-term mentalillness, with over 62% having had a firstcontact with mental health services morethan 10 years previously. The majority werediagnosed as having schizophrenia. Alarge number (56%) had a physicaldisability or had had physical healthproblems in the last month. Those in thehigh support hostels were the mostvulnerable and most impaired in activitiesof daily living when compared withresident groups in medium and lowstaffed hostels, acute wards and grouphomes. The study identified those receiving
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 37

residential care in the 1990s and madesome attempt at classifying residencesaccording to extent of care and staff toresident ratio. However, the study did notaddress the physical environment of theresidences, the management polices or therehabilitative efforts of the different levelsof facility to integrate the residents intothe community. While the study didinclude a residents’ profile, this wascompleted by the staff and not by theresidents themselves. This imposes anumber of limitations. Firstly, the majorityof staff were untrained, bringing intoquestion the validity of their subjectivejudgements of the residents’ levels offunctioning and diagnoses. Secondly, noattempt was made to ascertain theresidents’ satisfaction with the facilitiesand services. And finally, no effort wasmade to quantify the subjective quality oflife of the residents.
The Italian study (de Girolamo et al., 2002;de Girolamo & Bassi, 2004) was a nationalsurvey of non-hospital residential facilitiesin Italy. It included measures from bothTAPS (O’ Driscoll & Leff, 1993) and theBritish Residential Care Study (Lelliott et al.,1996). This was a two-phase study withthe first phase surveying all facilities basedin the community with four or moreresidential places. The first phase was acensus of all the aforementioned facilitiesand looked at the provision of services,staffing, and patient demographics.Results were very much in line with thoseof previous work in the UK (Lelliott et al.,1996; Trieman et al., 1998) and the US(Geller & Fisher, 1993) in that there wasvery little mobility between the residences,approximately 40% of staff had no formalqualifications and the majority of theresidents were diagnosed withschizophrenia. The residents differed fromthose in the UK studies in that the majority(48%) had never been admitted toinpatient care, although the median lengthof illness was 22 years. In the UK studies,the residents had all been relocated frompsychiatric hospitals. The second phaseinvolved a random sample of 20% of allresidences. It included two schedules – thestructure schedule and the patientschedule. The structure schedule coveredall aspects of the facilities from
organisation, treatment plans, staffing,external and internal rehabilitative activitiesto linkages to other facilities. The findingssuggest that the physical environment, thesize and the staffing pattern in terms ofquantity and skill mix of staff may haveinfluenced the residents’ quality of life andcreated a more home-like environment(Picardi et al., 2006). The patient scheduleincluded items such as diagnosis, patternof symptoms, appropriateness ofplacement, former place of residence andprediction of place of residence in sixmonths. This schedule also included theHealth of the Nation Outcome Scale(HoNOS), the Global Assessment ofFunctioning (GAF) and the Physical HealthIndex (PHI). Few managers judgedresidents as having short-term prospects ofdischarge and discharge to independentliving was uncommon (Santone et al.,2005). The majority of the residences hadone or more type of rehabilitative activityeither internal or external to the facility,with only 12% providing no rehabilitativeactivity. Interestingly, there was noassociation between the intensity of therehabilitative activities (i.e. the number ofactivities provided) and the staff ratings ofthe residents’ functioning. The authorssuggested that quality may have been amore important factor than quantity. Thislarge-scale study provided importantinformation on the provision and type ofresidential care in Italy. It extended thework previously carried out in the UK byincluding process of care items such as theprovision of internal and externalrehabilitation facilities. However, one ofthe limitations of the study was the failureto obtain the residents’ views.
A review of the literature revealed that themajority of users would preferindependent living arrangements withflexible staff levels (Shepherd, 1998). It isargued that common indicators of qualityof care in residential facilities include thequality of the physical environment,individualisation of care, privacy, autonomyand the attractiveness of theneighbourhood. These quality of carefactors have been shown to be related toquality of life measures (Shepherd &Murray, 2001) such as satisfaction withtreatment and care, food, accommodation
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND38

and relationships with others.Furthermore, the differences in quality oflife ratings between community-basedresidents and hospital-based patientsseemed to be the result of apparentlyminor factors such as access to kitchens,choice at mealtimes, being able to lock thebathroom door and access to one’s owntelevision. The results would suggest thatquality of care items such as these areindeed linked to subjective satisfaction andquality of life.
It must be kept in mind that independentliving is not always feasible for someindividuals often because of treatment-resistant psychotic illness (Macpherson &Jerrom, 1999). An appropriate alternativeis the 24-hour nursing facility; individualsplaced in these services have been shownto have improved social functioning andreport higher satisfaction than those ininstitutions (Shepherd, 1998). The increasein functioning resulted in approximately40% of those referred being able to moveto less supervised settings within two tothree years (Shepherd, 1998). However,this option still remains unattractive tomany service users, specially the youngerpatients who demand a certain level ofautonomy and privacy, but may requirehigh levels of support with managementof money, preparation of food and othersocial amenities. Thus, a 24-hour servicemust ensure that it meets the needs ofthese service users so that it is an acceptedservice that encourages and promotesrecovery. The balance between users’preferences and a cost-effective and safelevel of care will not be achieved withoutthe combination of community-basedhousing with support from highlyspecialised rehabilitation and recoverymental health teams who adhere to arecovery ideology.
2.10 THE PRESENT STUDY
The Mental Health Research Division(MHRD) of the Health Research Board(HRB) has over the years carried out healthservice research in the mental health area.The first study in the series was a review ofthe availability and utilisation of acute
psychiatric beds (Keogh et al., 1999). Thesecond was a review of the purposes andfunctions of day hospitals and day centres(Hickey et al., 2003). The third in the series– the present study – reviews theprovision, functions and purposes ofresidential services. Significant changes tomental health policy, coupled with the lackof previous mental health services researchinto community residential care, led to thefunding of this important study by theMental Health Commission and the HealthResearch Board.
The study aimed to describe andinvestigate the function of communityresidences with reference to theappropriateness of the premises and theextent to which the residence meets theneeds of the residents. Residentsthemselves were the prime reporters as totheir views of their lives and their levels ofsatisfaction with current service provision.The interaction of residents with thecommunity and their satisfaction with theirneighbourhood and environment was alsoinvestigated. Enquiry was made as to their‘citizenisation’, i.e. they were on theRegister of Electors, whether they usedcommunal social amenities, participated inlocal activities and used general healthcare services. In addition, staff perceptionsof the aims and functions of theresidences were investigated, as well astheir perceptions of the factors thatimpeded or promoted independent living.It was envisaged that the study wouldmake recommendations regarding theappropriate structures and functions ofcommunity residences and the necessaryprogrammes, mechanisms and conditionsto promote independent living, self-reliance and community integration. Thespecific aims of the study were to:
Examine the physical environment ofthe residential facilities
Report on the demographic and clinicalprofile of residents
Examine the staffing, management andcare practices in the facilities
Investigate residents’ levels of disabilityand of clinical, physical and socialfunctioning and the extent to which
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 39

impairments and disabilities reducedperformance of everyday living activities
Investigate residents’ satisfaction withcare and treatment, accommodationand other aspects of their lives
Determine the extent to which civilrights were met
Report on the perceived functions ofthe residences and the extent to whichthey met the residents’ needs.
2.11 SUMMARY
This chapter has defined what communitycare means for mental health servicepersonnel and the problems associatedwith the move to community-based care.Models of housing provision for those withsevere and persistent mental illness,together with considerations relevant totheir effective operation, particularly inrelation to rehabilitation, have beenreviewed. There has been a change inrecent years in Ireland, albeit gradual, to arecovery philosophy emphasising theprinciples of individual choice, partnership,empowerment and control. However,recent documents have highlighted theimportance of the recovery-orientedservices (Department of Health andChildren, 2006; Mental HeathCommission, 2005b). The move tocommunity care in Ireland has beenongoing for over 30 years. The move hasbeen unstructured and variable across thecountry. In addition, no evaluations on anational level of the community residentialfacilities or the treatment and care in thesefacilities have taken place. Local mentalhealth service research has taken place; theimportance of this research for localservice planning and development cannotbe over-emphasised. Of particularimportance in terms of the recoveryphilosophy are the residents’ perceptionsof their lives and their satisfaction withservices, and the level of autonomy withintheir lives.
It is important that research informs policyas to the best way forward in serviceplanning and delivery, taking into account
both service providers’ perceptions andservice users’ views. Given the currentclimate of policy development and servicechange in Ireland, research of this kind isparticularly necessary. The present studyattempts to remedy a current deficit in thisarea.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND40

CHAPTER 3Background to the PresentStudy and Methodology

3.1 INTRODUCTION
The current study was conducted duringthe period 01/06/04 to 31/05/06 andemployed both qualitative and quantitativemethods. Questionnaires were designed toevaluate the residential facilities, collectdemographic information, assess theclinical and psychosocial functioning of theresidents and perceptions of the residentsand staff. Quantitative data wereaugmented by qualitative informationgathered from open-ended questions,informal observation and socialinteractions in the course of fieldwork.During data collection, the primaryresearcher spent time in the residencesobserving and talking with the staff andresidents.
A two-phase procedure was adopted inthe study. The first phase of the studyinvolved the completion of questionnairesby directors of nursing for all communityresidential facilities in the three HSE areas.The returned questionnaires were thenused to classify the residences as high,medium or low support using thefollowing definitions:
High support - 24-hour nursing care
Medium support – supervision (non-nursing) at night, with staff membervisiting regularly
Low support – no supervision at night,with staff visiting regularly.
The next phase involved the randomselection of a sample of high, medium andlow support facilities within eachcatchment area in the three participatingHSE areas. From these, a random sampleof residents was selected to beinterviewed.
In addition, staff present in the selectedresidences completed a questionnaireregarding the aim and function ofcommunity residences and the factors thatpromote or impede return to independentliving.
3.2 STUDY AREAS
The study began in June 2004, prior to therestructuring of the health services (seeSection 1.4). At the beginning of thestudy, the health service was structured byhealth board area. Three health boardareas were selected for participation in thestudy, based on their geographical location(rural or urban), their provision of arepresentative range of residentialaccommodation and their willingness toparticipate. Following the restructuring ofthe health service, the three health boardareas became three HSE local areas withintwo HSE administrative regions. However,as already mentioned (Section 1.4), fewchanges had occurred at the time of thestudy in the management and delivery ofthe mental health services despite theimplementation of the new structures in2005.
The three HSE local areas that participatedin the study are outlined in Chapter 1. Forreasons of confidentiality, they will bereferred to as HSE local areas A, B and C.Within these three HSE local areas therewere a total of eight catchment areas eachrepresenting individual services. Table 3.1shows the population figures for theindividual catchment areas and totalpopulation figures for the HSE local areas(MHC, 2005a). HSE area C had the largestpopulation. The total populations for thoseover 16 years of age were 384,236 in areaC, 262,249 in area B and 168,867 in areaA. The adult mental health servicesprovided services for all those over 16years of age in the population. In onecatchment area in Area B – area B3 –community services were provided by thisarea but inpatient services were providedby another local area service, which wasnot participating in the study. However,there were no community residences inthe B3 catchment area. While catchmentarea B3 is included in the populationnumbers for completeness, it is excludedfrom all other analyses.
Chapter 3
Background to the present study and methodology
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND42

Area A has the lowest population, isprimarily rural and spans a widegeographical area. The physical geographyof the area and the lack of publictransport made it difficult to ensure thatservices were accessible to all. One of twocatchment areas with communityresidences in Area B (Catchment B1) isprimarily urban, while the other(Catchment B2) is primarily rural. Area Chas also got one catchment area which islargely urban, while the remaining two aremore rural. Area C includes some of themost deprived inner-city electoral areas.The tendency for a drift of disadvantagedpersons to inner city areas, poor housingand the lack of social or family supportresulted in a greater demand for mentalhealth services in these areas. Moreinformation on the mental health servicesin the three study areas is provided at theend of this chapter in order tocontextualise the study findings.
3.3 STUDY PARTICIPANTS
All community residential facilities (n =102) in the three participating areascompleted a questionnaire for the firstphase of the study. The total number of
returned questionnaires was validated withthe liaison person within the area.Following this the facilities were classifiedinto high, medium and low support. Astratified random sample (based on thelevel of support) of the residences fromeach of the catchment areas (see Section3.2) were selected for participation in thenext phase of the study. Based on thefigures from the Report of the Inspector ofMental Hospitals (2003), it was envisagedthat approximately 40% of the totalresidences would be included in the nextphase of the study. A total of 43residences were selected for participationin the next phase resulting in 42% (43 /102) of the total number of residences.
For individual interview a random sampleof residents was selected from the high,medium and low residences. The sampleof residents from the different levels ofsupport was in proportion to the totalnumber of residents in each supportsetting. The target sample size was 120residents and over-sampling was necessaryto ensure that those who refused toparticipate could be replaced. Of allresidents in the residences at the time ofthe study, approximately 16% (138 / 871)were interviewed. Similar proportions wereinterviewed from each of the three study
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 43
CATCHMENT AREA POPULATION*
Catchment A1 129, 008
Catchment A2 93, 754
Total Area A 222, 762
Catchment B1 175, 304
Catchment B2 103, 277
Catchment B3 61, 010
Total Area B 339, 591
Catchment C1 143, 029
Catchment C2 133, 559
Catchment C3 210, 346
Total Area C 486, 934
Source: Census 2002
Table 3.1 Population figures for study catchment areas and HSE local areas

areas (15% from local area A; 14% fromlocal area B and 19% from local area C).Of those who were asked to participate inthe study, sixteen (10%; 16 / 154) refused.The final sample interviewed resulted in atotal of 15% (82 / 552) of the total high,16% (25 / 153) of the total medium and19% (31 / 164) of the total low supportresidents.
Staff questionnaires were only given tothose residences that were selected for thesecond phase of the study. A total of 52staff returned questionnaires. As actualnumbers of staff were not recorded at thetime of the study, the percentage of staffwho returned the questionnaires iscalculated from the return of staffnumbers on the facility questionnaire. It isestimated that the 52 staff who returnedquestionnaires account for approximately36% of total staff, including nursing staffand care staff. The estimated percentageof nursing staff returning questionnaireswas 37% (39 / 105) and the estimatednumber of care staff returningquestionnaires was 22% (9/40).
3.4 MEASURES
The study incorporated a total of fourquestionnaires – Facility Questionnaire,Residents Questionnaire, Key WorkerQuestionnaire and Staff Questionnaire (seeAppendix 1 - 4). All the aims of thecurrent study could not be met by anyexisting questionnaire, therefore inaddition to standardised questionnaires,measures were developed and customisedto meet the study aims. Internationalresearch guided the questionnaire design.The Facility Questionnaire, ResidentQuestionnaire and Key WorkerQuestionnaire were informed by threeinternational studies (de Girolamo et al.,2002; Lelliott, et al., 1996; Trieman et al.,1998). The Staff Questionnaire wasdesigned primarily to gather informationon the staff’s perceptions of the aims ofthe residential facilities and factors thatpromoted or impeded return toindependent living within the Irish context.The content and context validity of thequestionnaires was ensured through
consultation with key stakeholders andrelevant experts (i.e. Advisory Committeefor the study, MHC, researchers, serviceproviders, mental health managers andservice users). A summary of the sectionswithin each of the questionnaires aredetailed in Table 3.2 and is followed by abrief description of each.
3.4.1 Facility questionnaire
This questionnaire was informedmainly by the study by de Girolamoet al (2002) and amended to suit toIrish context. The questionnaireswere completed by the nursingofficers in charge of the residence(see Section 3.5). There were a totalof 13 sections in the questionnaire(Table 3.2). The following sectionsummaries each section (SeeAppendix 1 for specific questions).For ease of reading, information onthe scoring of the scales are alsogiven in the appropriate place in theresults sections.
Building features - ownership ofbuilding, location, and number,type and use of rooms. Access toservices - time to reach otherfrequently used services such asGP, shopping and post office.
Rules and regulations – rulesgovern the residents dailyactivities, privacy and controlover finances.
Meals – who prepares the meals
Staff – number of staff, shiftsand emergency staff
Admission procedures – formaladmission procedures, exclusioncriteria, bed use, ownership ofbeds and specialisedrehabilitation teams.
Meetings – type and frequency ofmeetings in the residence.
Evaluation process andprocedures – annual planning,evaluation of quality services andcontrol, assessment of residents.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND44

System files and regulation –health and safety, rights ofresidents, complaints and healthinitiatives.
Resident characteristics - number,age, gender, diagnosis andemployment.
Activity – activities offered toresidents e.g. social skills,employment type, physicalactivity, education and supportactivities.
Community integration –activities that promotecommunity integration such asintegrated social activities andactivities to facilitate re-housingand employment.
3.4.2 Resident questionnaire
The resident questionnaires werecompleted at the individualinterviews with the sample ofresidents. See Table 3.2 for sectionswithin the questionnaire andAppendix 2 for specific items withinthe sections. This questionnairegathered information ondemographic information, activitiesof the residents and if they hadexperienced harassment in thecommunity. It also contained fivequestionnaires, detailed below.
Satisfaction with treatment andcare – this questionnaire wasbased on a section of the CoreAssessment and OutcomesPackages for Mental HealthServices (FACE Recording &Management Systems, 2000),which is widely used as an
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 45
Facility questionnaire Resident questionnaire Key worker questionnaire Stafffor resident questionnaire
Building Demographic Psychiatric Aims / functionsfeatures information history of residence
Access to services Activities Global Assessment of Functioning
Rules / Regulations Harassment Factors that impede independent living
Food preparation Satisfaction of Physical Healthtreatment / care Index
Wardrobe Health of the Factors thatNation Outcome Scale promote
independent living
Staff Quality of Life
Admission procedures Disability DisabilityAssessment Scale Assessment Scale
Meetings Social Support
Evaluation processes BPRS
Files/regulations Perception of life in residence
Resident characteristicActivitiesCommunity integration
Table 3.2 Factors addressed in each of the four questionnaires

evaluation tool in the UK and NIand has recently been used bysome services in Ireland (e.g. HSEMid Western Area, HSE NorthernArea). Only Your Treatment andCare questionnaire was used inthe current study to assess theservice users’ experience oftreatment and care. It contains atotal of 22 items assessing theservice users’ knowledge of careplans and relationships with keyworkers and psychiatrists. Serviceusers indicate their response tothe statements by ‘yes’, ‘no’ or‘not sure’. Two general questions,using a four point scale,enquiring about the overallsatisfaction of the residents withtreatment and care and theinformation they received wasassessed at the end of thequestionnaire.
Quality of life - the quality of lifemeasure used was loosely basedon the Satisfaction for LifeDomains Scale (Tempier et al.,1997) measuring satisfactionwith life in general and in 17 lifedomains (see Appendix 2).Residents indicated theirsatisfaction on a three-point scalefrom 0 – 2, with higher scoresindicating greater satisfaction.The scores on the 18 items weresummed to give a total quality oflife score.
Disability Assessment Scale (WHODAS II) – this scale measuredfunctioning and disability in thelast thirty days. It assessedfunctioning and disability in sixdomains including understandingand communication, gettingaround, self-care, getting alongwith others, household and workactivities and participation insociety. Both residents and theresidents’ key worker completeda version of this scale, resultingin two measures for eachresident. The scale contains 12items and is rated on a five-pointscale from 0 – 4.
Social support – the scale used tomeasure social support wassimilar to the MannheimInterview on Social Support(Veiel, 1990) in that it askedabout social support in fourdomains including everydaypsychological support, everydayinstrumental support,instrumental crisis support andpsychological crisis support (seeSection 6.1.1 for more details).Residents were asked to indicatewho they asked for help duringthese times.
Brief Psychiatric Rating Scale(BPRS) – this is a widely usedmeasure within psychiatry andwas employed to measure theresident’s currentpsychopathology. The 24symptoms were rated by theresearcher on a seven-point scale(i.e. 1 = not present to 7 =extremely severe).
Perception of life in the residence– this scale was devised by theauthors to measure the residents’perceptions of live in theresidence. Residents rated theirperceptions on 12 areasincluding living in the house,how well residents got ontogether and with staff, howmuch control they had to leadtheir live as they wanted andhow happy they were with theirlevel of independence. At theend of the residentquestionnaire, residents wereasked an open-ended questionregarding their life in theresidence and what it was like tolive there (see Section 8.5).
3.4.3 Key worker questionnaire forresident
The key worker questionnaire wasemployed to gather furtherinformation about the resident. Itincluded psychiatric history, systemof support, appropriateness ofplacement, general functioning,physical health, psychopathology
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND46

and disabilities. See Appendix 3 forspecific items on the questionnaire.Below is a short description of thestandardised measures used.
Global Assessment of Functioning(GAF American PsychiatricAssociation, 1994) – provides theclinician’s judgement of theindividual’s overall level offunctioning. The GAF scale israted with respect topsychological, social andoccupational functioning onlyand does not include impairmentdue to health or environmentallimitations. The key worker ratedthe resident on a scale from oneto 100.
Physical Health Index– this is asimple measure for assessingphysical health and has beenused by the UK study (O’Driscolland Leff, 1993) and the Italianstudy (di Girolamo et al., 2005).This measured physical healthproblems on a scale of 0 – 3 withhigher scores indicating greaterdisability. It is also used to ratethe level of assistance requiredfor disabilities on a scale of 0 – 7,again with higher scoresindicating greater assistancerequired. Health in eight domainsis assessed.
Health of the Nation OutcomeScale (HoNOS) – this scale wasdesigned to assesspsychopathology and disability inthe previous two-weeks and haspreviously been used in theItalian study (di Girolamo andBassi, 2004). The scale measuredclinical and social functioning in11 domains using a five-pointscale from 0 (no problems) to 4(severe problems).
Disability Assessment Scale (WHODAS II) – key workers rated theresidents on the DAS, asdescribed above.
3.4.4 Staff questionnaire
The staff questionnaire wasdesigned by the authors to assessthe staff perceptions of the aimsand functions of the residences andthe factors that promoted orimpeded return to independentliving for the residents (see Appendix4). Following the demographicinformation section, the staff wereprovided with a list of eight possibleaims and functions of the residenceand were asked to rate theimportance of each on a scale from1 (no importance) to 4 (greatestimportance). They were then askedopen-ended questions regarding thethree main factors that they feltpositively and negatively influencedreturn to independent living.
3.5 PROCEDURE
All research instruments were pilotedbefore fieldwork proper began andadjustments were made to instrumentsand procedures as needed. Followingexperience gained from the pilot study, thefollowing procedure was adopted duringfieldwork. The researcher contacted thedirector of nursing regarding completionof the facility questionnaires. These werecirculated by the director of nursing to thenursing officers in charge of theresidences. The principle researcher’s nameand telephone number were included in allcorrespondence, ensuring that nurses hada contact number for any questions orqueries that might arise. Completedquestionnaires were returned to thedirector of nursing who returned them tothe researcher. Following the return of thequestionnaires the director of nursingidentified a person with whom theresearcher could liaise for the secondphase of the study. The liaison person inthe majority of instances was an assistantdirector of nursing.
A random sample of high, medium andlow support residences was selected forthe second phase of the study. The liaisonperson was informed of the residencesselected, the approximate number of
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 47

interviews required, the requirement of thekey worker or staff nurse to complete aquestionnaire for every residentinterviewed, and suitable dates forinterviewing. The contact person theninformed the clinical nurse manager of theresidences of the visit and the nursesinformed the residents. The clinical nursemanager provided the researcher with alist of residents’ names, excluding all thosewith organic brain injury and those inrespite beds for less than three months.The interviews took place in the residentialfacilities or in some cases at a day carecentre. The researcher arranged eveningmeetings for those residents that were notavailable during the day.
Prior to the interview, the researcher metwith the resident and explained thecontent, context and purpose of the study.Conditions for study participation wereexplained to residents both verbally andsummarised in a written summary ofinformation given to participants beforewritten consent was obtained. Participantswere assured verbally and in writing thatno personal identifying information wouldbe recorded on the research instruments,that the information they disclosed wouldnot be available to staff or other residentsand would be used in the research reportin a manner which would not allow foridentification of the respondents. Theinformation sheet explained that theinformation collected would be availableto the research team only and that thequestionnaires and other researchmaterials would be destroyed inaccordance with the HRB’s recordmanagement policy (i.e one year followingpublication of study). Residents wereinformed that unwillingness to participatewould not affect their treatment and care,and that they were free to take a break inthe middle or withdraw from the interviewat any time. They were also informed thata nurse would complete anotherquestionnaire detailing their psychiatrichistory and clinical, social andoccupational functioning. If the residentagreed to participate, they signed thestudy consent form and the interviewbegan.
On completion of the interview with theresident, the key worker questionnaire wasgiven to the key worker or nursing staffmember. In most instances, there was noassigned key worker and the questionnairewas given to the nursing staff forcompletion. These questionnaires werecompleted on site in the majority ofresidences. However, in some instances,especially in the low and medium supportfacilities, there was no nurse on hand tocomplete the key worker questionnaire. Inthese instances the questionnaires wereleft with the liaison person to distribute tothe appropriate nursing staff. Thesequestionnaires were returned by post tothe researcher when completed.
Nursing or care staff members who wereon duty on the day of the visit completedthe staff questionnaires. In addition,questionnaires were left at the site forcompletion by fellow staff members andwere posted back to the researcher. Allstaff questionnaires were anonymous.
3.6 ETHICAL APPROVAL
International best practice (e.g. WHO,1999) in relation to the conduct of ethicalresearch in the social sciences informedthe selection of methods and proceduresfor the present study. A Research AdvisoryCommittee was established to advise onthe project. The committee includedrepresentatives from the MHC, user groupsand from the participating HSE areas.
The study proposal underwent internal andexternal peer review following theprocedure set down by the HRB. The studyreceived ethical approval from the HRBResearch Ethics Committee (REC) inOctober 2004. Ethical approval for thestudy was also received from the REC ineach of the catchment areas of the HSEareas. For those areas where there was noREC in place, approval was sought fromthe clinical directors. In addition, briefingmeetings were held in each HSE area toinform service managers, staff and usersabout the study and to obtain their views.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND48

3.7 DATA ANALYSIS
Analysis of the data was primarilydescriptive. In most cases, descriptivestatistics are presented , by level ofsupport of the residence (i.e. high support,medium support and low support). Chi-square tests (with Yates’ correction for 2 x2 tables) were used to analyse categoricalvariables. The chi-square results are notreported when more than 20% of cellshad an expected frequency of less thanfive. T-test or one-way analysis of variance(ANOVA) were used as appropriate tostudy differences in the mean ofcontinuous variables between groups.ANOVA was followed by post-hoccomparisons according to the Bonferronimethod. Non-parametric statistics wereused to examine variables not normallydistributed. As not all questions wereanswered on the questionnaires, degreesof freedom may differ throughout thereport. SPSS Text Analysis for Surveys wasused to analyse the qualitative data.
3.8 CONTEXTUALISING THEPARTICIPATING HSE LOCALAREAS
In order to contextualise the results, it wasnecessary to provide some backgroundinformation to the study areas. Theinformation was obtained from clinicaldirectors, directors of nursing and generalmanagers of the services in the areas.Background documentation was gatheredand unstructured interviews were carriedout in the three HSE local areas.Information was gathered on thedevelopment and the characteristics of themental health services and the context inwhich service developments occurred. Dataincluded information on the philosophyand the aims of the residential facilities. Inaddition, the wider societal andenvironmental aspects of the study areaswere investigated and their impact onmental health services and their users wasexplored. The role and function of relatedstatutory and voluntary agencies in theareas were investigated. The followingdescriptions are based on the interviewer’snotes of the meetings with servicemanagers and providers.
3.8.1 Resettlement of patients
In HSE Area A, resettlement ofpatients into community residencesin their local communities began inthe mid-eighties. The philosophyunderlying the communityresidential facilities, at least for thehigh support, supervised residentialunits (SRUs), was that these houseswere ‘homes for life’ wheretreatment and care would beprovided in a homelike environment.Properties were acquired on an adhoc basis, with facilities selected onthe basis of availability, size andaffordability. Rehabilitation toprepare residents for the move wasprovided within the hospital bynursing staff prior to relocation. Thestaff played an important role in thecontinuing care of the residents interms of monitoring medication andproviding education and training insocial skills and daily living skills. InArea A, the move to residential carein the community occurred over arelatively short period of time andwas accompanied by the closure ofone of the two large psychiatrichospitals in the area (in 1991).While the remaining hospital hadbeen retained, it now has only twolong-stay wards remainedaccommodating approximately 20patients. It was reported that thelack of places in supervisedresidential facilities prevented themove of eight patients, while twelvepatients were unsuitable forcommunity care and needed to beaccommodated elsewhere. Aregional special care unit in the areaaccommodated eight patients. Itwas anticipated that the function ofthis unit would be readdressed inthe near future, and attempts wouldbe made to find more suitableaccommodation for its clients.
The resettlement of patients tocommunity residential care in Area Bwas similar to that in Area A andbegan in the mid-eighties followingthe publication of Planning for theFuture in 1984. The underlying
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 49

ethos here again was that thefacilities were ‘homes for life’, withthe staff helping the residents toadjust to life in the community.Basic assessments took place in a‘filter’ ward in the hospital. Thenurses had the responsibility ofselecting those whom they deemedsuitable for relocation to thecommunity. The initial houses weremedium or low support (they didnot have 24-hour nursing care), butsome of these were later redefinedas high support. Attempts weremade to get ordinary, large housesand to link the patients with thecommunity from whence they came.The main criteria for the acquisitionof premises were that they were in‘normal’ type environments –neither deprived nor affluent areas –and were accessible to amenitiessuch as churches, shops and busservices. One of the two largehospitals closed in Area B in 1999.The remaining hospital catered for118 long-stay patients.
The resettlement in Area C beganprior to Planning for the Future(1984). As early as the 1970s therewere patients sleeping in communityresidential facilities in some areas inarea C, but spending their days inthe psychiatric hospital. Thisarrangement had evolved because ofthe large number of houses thatwere once provided for staffworking in the hospital and were nolonger required. For those serviceswhere resettlement had alreadybegun, Planning for the Futurerecommended that emphasis shouldbe placed on independent livingthrough rehabilitation and re-socialisation programmes. For theservices that did not have aresettlement programme already inplace, Planning for the Futurestressed that deinstitutionalisationand the process of rehabilitation andresettlement should begin. Whilethe community residences weredesigned to provide step-downaccommodation for those who ondischarge from hospital could not
live in their own homes, there waslimited success in moving people on.As in the other areas, the process ofdeinstitutionalisation was regardedby many within the service, bothstaff and patients, as the provisionof a ‘home for life’ for thoserelocated from the hospital. A studyin Area C (Health Service Executive,2004) reported that staff andprofessionals described the majorityof residents as needing a ‘home forlife’. There were two largeinstitutions in area C, whichaccommodated approximately 200long-stay patients.
In summary, the resettlement ofpatients from large institutions andthus the development of communityresidences began in some areas inIreland as early as 1960. In theseareas resettlement was slow andonly involved those who were leastimpaired. There were few or norehabilitation or re-socialisationprogrammes in place. Theresettlement of patients from largeinstitutions gathered momentum inthe 1980s with the publication ofPlanning for the Future (1984).
It was reported in all areas that,while government policy was behindthe move, backing in terms ofresources was meagre. Nurses andothers within the hospitalsundertook the rehabilitation and re-socialisation functions. Communityaccommodation was purchasedwhere available and modifiedappropriately. Given the continuedscarcity of resources, thedevelopment of communityresidential services was slow.
While all the three areas studied hadbegun the process ofdeinstitutionalisation, they were atdifferent stages of evolution in thisprocess at the time of the study. Anumber of service managers andproviders pointed out that thephilosophy of the communityresidential facilities at the time wasthat the patients were moving to
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND50

their new homes, which would behomes for life. A large number ofthese residents still remained in thecommunity residences to which theyhad come from inpatient care. Forthese residents, the communityresidential facilities have functionedas continuing care facilities.
3.8.2 Characteristics of the generalmental health services in thethree areas studied
Area A had a large number ofpsychiatric nurses in both catchmentareas, with the majority employed inbed-based facilities. A largeproportion of these nurses wereattached to community residences.This left little resource forcommunity-based care, andcommunity mental health teams hadbeen slow to develop. There was aninsufficient number ofmultidisciplinary community healthteams and a number ofprofessionals worked in isolation,taking referrals from various sources,including direct referrals fromprimary care. There was a lack ofresources for the development ofmultidisciplinary teams and therewas a need for more professionals inclinical psychology, social work andoccupational therapy. There were nospecialist rehabilitation services;however, one catchment area wasexpected to have a specialistrehabilitation psychiatrist in post inthe near future.
Both catchment areas in Area B hadcommunity mental health teams inoperation although there was ashortfall in the number of teams. Inaddition, the teams were notadequately staffed with thenecessary professionals, particularlyin social work and occupationaltherapy. There was only onespecialised rehabilitation team.
Community mental health teamswere in operation in all catchmentareas in Area C although there wasa critical shortage of core staff. Inone catchment there were no
clinical psychologists or socialworkers. Catchment Area C2 hadthree management bodies, whichincluded the HSE and two hospitalboards in the area. There was onlyone specialised multidisciplinaryrehabilitation team, and it wassignificantly understaffed.
3.8.3 Management of the mentalhealth services
It was reported in the backgroundinterviews that the mental healthservices were managed on aregional level and on a catchmentarea level. The role of the regionalmanagement unit included funding,accountability and governance,planning, policy setting, andperformance management. Theregional management team alsooversaw external relations with otherbodies (HSE, MHC) andcollaborations with other services,such as voluntary groups and localauthorities. The catchmentmanagement teams’ roles andresponsibilities focused on thedelivery of services and clinicalleadership. The catchmentmanagement teams wereconsultant-led multidisciplinaryteams. They had responsibility forlocal service provision and clinicalleadership. In addition, there wereconsultant-led sector managementteams that had an operational rolewithin the sector. In some cases,members of the sectormultidisciplinary team were sharedwith other sectors. As noted above,two of the catchment areas in thestudy had dedicated rehabilitationteams, yet neither of these teamshad the full complement ofmultidisciplinary staff.
The referrals for the communityresidential facilities in all areas cameexclusively from the sector teams.The responsibility for placementdiffered across the catchment areas.In four of the seven catchmentareas, decisions about admissionsand discharges to community
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 51

residential care were theresponsibility of the consultant-ledteams. In two of the catchmentareas, referrals were made to thededicated rehabilitation psychiatristand placement decisions were madein conjunction with themultidisciplinary rehabilitation team.In one of the catchment areas,placement was co-ordinated by amultidisciplinary rehabilitationplacement committee. Thiscommittee was led by the assistantdirector of nursing.
3.8.4 Aims and functions of thecommunity residential facilities
It was reported at the interviewswith service managers, clinicaldirectors and directors of nursingthat the community residentialfacilities had become a continuingcare facility for those relocated fromthe psychiatric hospitals. This wasdue mainly to the fact, that in thepast, that both staff and residentsbelieved that this indeed was thefunction of the residences. Therewas very little in the way of formalrehabilitation except for that offeredby nursing staff. Residents helpedabout the house with everydayactivities and it was reported thatthe positive changes in someresidents were remarkable since theyhad arrived in the residence fromthe hospital. However, few of theseresidents had moved on to lowerlevels of support.
It was reported that staffperceptions of the aims andfunctions of community residenceshad changed in that they were nowmore often viewed as part of therehabilitation process as opposed toa ‘home for life’. During theinterviews, management and clinicalstaff confirmed the importance ofrehabilitation. They definedrehabilitation as a process ofenabling the person to function atan optimal level and in as normal asocial context as possible. Twocatchment areas had specialised
rehabilitation teams, albeitincomplete, and could thereforeprovide a proactive rehabilitative roleas part of community care. Withinthe other catchment areas, it wasacknowledged that the concept ofrehabilitation and recovery was veryimportant and needed to bedeveloped within the services. It wasreported that scarcity of resourcesand the inefficient deployment ofnursing staff led to anunderdeveloped rehabilitativeservice. Lack of training wasreported as being an importantfactor that inhibited rehabilitation,as the majority of the staff weretrained in the philosophy ofcustodial care as opposed tocommunity care.
3.8.5 Constraints on the efficientmanagement of communityresidential facilities
There were a number of constraintsthat limited the efficient running ofthe community residential facilitiesand that inhibited the rehabilitationof the residents. These constraintswere not common to all areas,although some issues were relevanton a national basis.
The issue of long-term stay chargeshas been an active topic of debateover the last two years. The HealthAmendment Act 2005 and theHealth (Charges for InpatientServices) Regulations 2005addressed the issue of charges forlong-term institutional care. Prior to2005, residents of communityresidential care were charged aweekly rent by the health services.This amount varied within andbetween catchment areas. However,in 2005 the Supreme Court foundthat there was no legal basis for thecharges and consequently all HSEareas had to abolish the weekly rentcontributions paid by residents.Later in the year, a repaymentscheme for the refund of paymentsmade to the health service wasannounced. Most of the service
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND52

managers and providers reportedthat this caused a certain amount ofupset in the residential facilities.Firstly, residents and their familieswere confused about the legislation.Secondly, service providers arguedthat the process of moving peopleto independent living was furtherimpeded by the suppression of lowcost accommodation previouslyoffered in mental health residences,which limited the ability of staff toteach residents budgeting skills. Inaddition, one area reported thatencouraging the residents to do theshopping was extremely problematicas they now had to have receipts foreverything. It was felt that thisfurther impacted on therehabilitation process. The situationwas further exacerbated when, inJuly 2005, new regulations whichprovided for different chargingarrangements depending on thelevel of nursing care wereintroduced. This caused theresidents and staff more distress asthe maximum charge for 24-hournursing facilities was €120 perweek, or the amount of anindividual’s income that remainedafter €35 had been allowed forpersonal use. This left residents withlittle money to survive on and madeit even more difficult to gatherfinances to secure deposits forindependent accommodation. Atthe time of this study, the newregulations on long-stay chargeshad not been implemented,although residents in one area hadreceived letters regarding chargesand back payments.
Common to all 24-hour nursingfacilities was the Hazard Analysisand Critical Control Points (HACCP)Health and Safety legislation. Thislegislation requires an analysis ofrisks associated with cateringestablishments, includingcommercial services and healthservices, and is carried out byenvironmental health officers. Theanalysis looks at operational hygiene
and the implementation of thesecontrols, identifies hazards andcritical controls necessary. Thesituation in the majority of highsupport residences was thatresidents did not have access to thekitchen because of HACCPlegislation.
Another common problem identifiedwas the advanced age of residentswho now made up a largeproportion of the population inresidential facilities; most of theseresidents had been relocated fromlarge institutions. It was reportedthat the physical problems of thispopulation outweighed the mentalhealth problems and that theseresidents were much more in needof physical care rather thanpsychiatric intervention. A numberof the residential facilities wereunsuitable for those with physicaldisabilities. Community hospitalsand homes for the elderly were notalways willing to accept residentsfrom mental health residentialservices, preferring instead to takethose who were living alone. It wasacknowledged that there was anethical issue in moving residents tonursing homes away from theirfriends. In one catchment area,residential facilities for persons withlearning disabilities were provided bythe mental health services, yet theservice did not have access to aconsultant psychiatrist with a specialinterest in the psychiatry of learningdisabilities. There was no fundingfor this post and services felt thatthis was a neglected area.
In all background interviews carriedout, the issue of housing was raised.It was felt that provision of housingwas not the responsibility of themental health services and thathousing should be provided by thelocal authority. It was highlightedthat there was a possibility that themedium and low support facilitieswere becoming ‘homes for life’ asthere was no alternativeindependent housing available for
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 53

residents. As one service managerreported ‘group homes were homesfor the homeless until they got ahouse of their own’. It was reportedthat few residents were registeredon their local housing list, althoughin one HSE area all residents incommunity accommodation wereregistered on the housing waitinglist. However, the waiting time onthat list stood at seven years and thechance of acquiring local housingwas reported to be slim. All areasreported that links with localhousing authorities needed to bestrengthened. It was felt that, whilethe mental health services shouldnot be responsible for the provisionof housing, they were responsiblefor liaison with local authorities,voluntary groups and privatelandlords to ensure suitableaccommodation was available. Someof the areas had already got linkswith voluntary groups whichprovided housing for those withmental health problems (e.g. MentalHealth Association, HousingAssociation for Integrated Living,STEER), but these could be furtherdeveloped.
Another issue put forward aslimiting the efficient use ofcommunity residential facilities wasthe division of services by sector. Itwas reported that this limited choicefor the service user. Commentsincluded the need for morecollaboration between sectors andcatchment areas. Another concernwas where the location of facilitiesthat provided for an entirecatchment area population. Onearea that serviced a largegeographical area was particularlyconcerned about the appropriatelocation of services that would resultin equity and accessibility for allservice users.
The definition of high, medium andlow support accommodationdiffered between and within areasand the need for a standardiseddefinition of level of support was
noted.
3.8.6 Developments for the future
Services reported that they hopedthat the Mental Health Commissionand the Expert Group on MentalHealth Policy would provideguidelines on best practice for themanagement and provision of themental health services. Issues seenas the most important included:
Retraining and professionaldevelopment of nursing and carestaff
Reorganisation of budgets formental health care and care ofthe elderly
Reorganisation of services toincrease choice for service users
Greater emphasises onrehabilitation and recovery
Sufficient resources to implementand develop specialistrehabilitation and recoverymental health teams
Development of the interfacebetween mental health servicesand other health and social careservices
Best practice in the area ofhousing to meet the needs ofthose with mental healthproblems.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND54

CHAPTER 4Home Sweet Home?Description of CommunityResidences

Chapter 4 presents the data collated from thefacility questionnaires. The questionnaires werecompleted by the nursing officers in charge ofthe community residences. The researcherforwarded questionnaires to the directors ofnursing in the three study areas, who forwardedthem to the relevant nursing officers incommunity residences in the three study areas.All nursing officers in the community residencesin the mental health services in the three areascompleted a questionnaire (n = 102). Thesewere then returned to the directors of nursingwho forwarded them to the researcher.
The questionnaires gathered information on thedemographic and diagnostic profile of residents,the numbers of residences and places in eachresidence, the location, and ownership ofresidences and the access to local services andamenities. Information was also provided onpatient movement (admissions and discharges)within residences, use of respite and crisis beds,relevant exclusion criteria, waiting lists,management and policies, and, finally, foodpreparation.
4.1 DEMOGRAPHIC PROFILE OFRESIDENTS
There were 871 residents in the residencesat the time of the study. A total of 64% (n= 554) were in high support residences,
18% (n = 153) were in medium supportresidences and 19% (n = 164) were in lowsupport residences. Of the total residents61% (n = 532) were male. A slightlyhigher proportion of the high supportresidents (60%; 333 / 554) and mediumsupport residents (56%; 85 / 153) weremale, while the majority of the lowsupport residents (69%; 114 / 164) werefemale.
Almost half (47%; n = 413) of theresidents were aged between 46 and 65years. Only 21% (n = 185) were aged 45years or under; 31% (n = 273) were agedover 65 years. Only 9% (n = 80) ofresidents were under the age of 35 years.Those in the high support residences hadan older age profile than those in mediumand low support (see Figure 4.1). Therewas a higher proportion of residents inhigh support over the age of 65 years(37%; n = 205), than in medium (20%; n= 30) or low support (23%; n = 38) anda higher proportion of those in mediumsupport (27%; n = 42) and low support(23%; n = 38) were in the lower agerange of 26 to 45 years than in highsupport residences (14%; n = 91).
Table 4.1 shows the diagnostic categoriesassigned to residents at the time of thestudy. Of the 871 residents, 542 (62%)had a primary diagnosis of schizophrenia.
Chapter 4
Home sweet home? Description of community residences
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND56
0
5
10
15
20
25
30
35
40
>6556-6546-5536-4526-3518-25
% o
f re
side
nts
Age Group
High Medium Low
Figure 4.1 Frequencies of age groups of residents, by level of support

The second most frequent diagnosis wasdepression (11%; n = 97), followed byintellectual disability (6%; n = 53) andmania (5%; n = 44). These proportionswere similar across the high, medium andlow support residences. As expected, fewresidents had a primary diagnosis oforganic brain injury (2%). A total of 22(2%) had a primary diagnosis of alcoholdisorder or drug dependence. Fewresidents were reported as having a co-morbid alcohol (5%; n = 43) or drug (1%;n = 8) problem. A total of 35 (4%)residents had an unspecified primarydiagnosis.
A small proportion of residents werereported as being in employment (21%;181/871). Of these, 48 (5%) were in paidemployment in the community and 133(15%) were in sheltered employment. Ofthose in paid employment in thecommunity, 46% (22 / 48) were in full -time employment and 54% (26 / 48) werein part-time employment.
4.2 THE PHYSICAL ENVIRONMENTOF THE COMMUNITYRESIDENCES
4.2.1 Number of residences andnumber of places
There was a total of 102 residencesreported by the directors of nursingfor the three HSE local areas, Area A(n = 39), Area B (n = 31) and AreaC (n = 32). Of the total residences,36 (35%) were high support, 25(24%) were medium support and 41(40%) were low support (Table 4.2).Area A provided no medium supportresidences and had a greaternumber of low support residencesthan Area B or Area C.
There was a total of 951 residentialplaces in the three HSE areas. Ofthese, 61% (n = 584) were in highsupport, 18% (n = 166) were inmedium support and 21% (n =201) were in low support residences(Table 4.2).
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 57
High Medium Low Total(n = 554) (n = 153) (n = 164) (n = 871)
Organic 17 (3.1) 0 1 (0.06) 18 (2.1)
Schizophrenia 313 (56.5) 97 (63.3) 132 (80.5) 542 (62.2)
Other psychoses 21 (3.8) 6 (3.9) 4 (2.4) 31 (3.6)
Depression 78 (14.0) 12 (7.8) 7 (4.3) 97 (11.1)
Mania 30 (5.4) 10 (6.5) 4 (2.4) 44 (5.0)
Neurosis 11 (2.0) 2 (1.3) 2 (1.2) 15 (1.7)
Personality disorder 10 (1.8) 2 (1.3) 2 (1.2) 14 (1.6)
Alcohol disorder 15 (2.7) 2 (1.3) 4 (2.4) 21 (2.4)
Drug dependence 1 (0.01) 0 0 1 (0.01)
Intellectual disability 35 (6.3) 11 (7.2) 7 (4.3) 53 (6.1)
Unspecified 23 (4.1) 11 (7.2) 1 (0.06) 35 (4.0)
Total 554 (100.0) 153 (100.0) 164 (100.0) 871 (100.0)
Table 4.1 Number (%) of residents in each diagnostic category, by level of support

4.2.2 Location and ownership of thecommunity residences
Almost two-thirds of the residenceswere situated in urban areas (70%;n = 71) or on their periphery (23%;n = 24). Significantly more of themedium (80%) and low (80%)support residences than of the high(50%) support residences weresituated in urban areas (chi-square,p < 0.001). Few residences weresituated in rural areas (7%; n = 7).
It was reported that the majority ofthe buildings housing the residenceswere owned by the HSE (74%; n =76); only two were reported asleased from the local authority (onehigh and one medium), six werereported as owned by the voluntarysector (one high, two medium andthree low) and 16 of the lowsupport residences were reported asleased from private owners.
4.2.3 Physical environment and accessto local services and amenities
As expected, high supportresidences had a significantly higheraverage number of bedrooms thanmedium and low support residences(Kruskal Wallis, p < 0.001; Table4.3). Within the high supportresidences, there were more doublerooms than single rooms. There wasa similar number of double andsingle bedrooms in medium supportresidences while low supportresidences had more single roomsthan double rooms. Only four of theresidences had bedrooms with three
or more beds.
The average number of bathroomswas greater in the high supportresidences (mean 3.89) than inmedium support (mean 2.12) andlow support (mean 1.44; (F (2, 101)= 13.76, p < 0.001). The ratio ofresidents to bathrooms was 5.96 : 1in high support, 4.50 : 1 in mediumsupport and 3.92 : 1 in low support.This mean ratio was significantlygreater in the high supportresidences than in the low supportresidences (F = (2, 96) = 7.29, p <0.001).
Overall, the majority of residenceswere unsuitable for those withmobility problems (72%). However,significantly more of the highsupport residences (44%) than ofthe medium (20%) or low support(17%) were suitable for those withmobility problems (chi square, p <0.05). The majority providedresidents with access to publicphones on the premises (71%).
4.2.4 Smoking arrangements
The nursing officers reported thatover half of the residences providedresidents with access to a smokingroom (58%). The smoking room waslocated outside in the majority ofcases (56%). In 30% (n = 18) of theresidences an inside smoking areawas provided and it was reportedthat 14% (n = 8) had smokingrooms both inside and outside the
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND58
Level of support Number of Number of Number ofresidences residents places
High 36 (35.3) 554 (63.6) 584 (61.4)
Medium 25 (24.6) 153 (17.6) 166 (17.5)
Low 41 (40.1) 164 (18.8) 201 (21.1)
Total 102 (100.0) 871 (100.0) 951 (100.0)
Table 4.2 Total number (%) of residences, number (%) of residents and number (%) of places,by level of support

residence. Of the high supportresidences, 89% (n = 32) provided asmoking room and 47% of theseprovided an indoor smoking room.A total of 48% (n = 12) of mediumsupport and 37% (n = 15) of lowsupport residences reported theprovision of a smoking room.
4.2.5 Access to local amenities andservices
Table 4.4 shows the mean length oftime taken to reach local servicesand amenities from the residences.Time taken to walk to the shops (F(2,99) = 3.40, p <0.05) and toreach the day centre /day hospital (F(2, 101) = 4.59, p < 0.05) byminibus differed significantlyaccording to the support level of theresidence. In all cases it took
statistically significantly longer toreach these amenities from the highsupport residences than the lowsupport residences. However thesedifferences were small (5 – 7minutes), except in the case of theday centres / hospitals where it tookon average 20 minutes longer toreach from the high support thanfrom the low support residences.
Few residents (4%; n = 32) had access totheir own transport. Of these who had, 10had a car, 21 had a bike and 1 had amotorbike. A total of 3% (17 / 554) ofresidents from high support facilities hadtheir own transport; 5% (7 / 153) ofmedium support residents had their own,as had 5% (8 / 164) of residents from lowsupport residences.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 59
High Medium LowMean SD Mean SD Mean SD
Total bedrooms 9.64 5.71 5.00 1.55 3.73 1.41
Single rooms 3.81 5.44 2.44 1.50 2.59 1.55
Double rooms 4.83 3.25 2.32 1.31 1.07 0.9
Table 4.3 Mean number of bedrooms in residences and standard deviations, by level of support
High Medium Low TotalMean SD Mean SD Mean SD Mean
Time to walk to shops 11.50 11.43 9.36 4.94 6.78 5.13 9.03
Time to get to shops on public transport 9.83 10.07 7.85 4.06 6.22 3.38 7.96
Time to walk to post office 18.24 15.55 16.72 11.92 14.88 9.59 16.48
Time to post office on public transport 8.10 8.09 8.05 4.89 6.59 3.12 7.64
Time to walk to pub 11.67 11.67 9.48 9.48 8.66 8.66 9.92
Time to walk to GP surgery 21.61 21.61 17.00 17.00 14.61 14.61 17.55
Time to reach GP surgery on public transport 8.19 8.19 10.37 10.37 8.31 8.31 8.96
Time to reach day centre/hospital by minibus 36.69 38.82 27.72 34.10 15.07 20.79 25.80
Table 4.4 Mean length of time in minutes (SD) to reach other services and amenities, by levelof support

A total of 28% of the residences hadaccess to a minibus (i.e. 47% of the highsupport residences, 24% of the mediumsupport residences and 15% of the lowsupport residences). All the medium andlow support residences shared the minibuswith other residences, while only 35% ofthe high support residences did so.
4.3 ADMISSIONS AND DISCHARGES
Table 4.5 shows the number andproportion of admissions to the high,medium and low support residences in thethree years prior to data collection (2002 –2004). A total of 137 admissions to theresidences was reported for the last sixmonths, with the majority of these beingto high support residences (65%; n = 89).The highest number of admissions was tothe high support units, with 359 residentsbeing admitted over a period of 36
months. The year prior to the study a totalof 259 admissions were reported.
Regarding discharges in the year prior todata collection for the study (2004), therewas a total of 179 discharges. Thesedischarges were reported for a total of61% of the residences (26% high, 15%medium, 20% low). Table 4.6 shows thenumber of discharges and place ofdischarge of the residents. The majority ofthese were from high support residences(75%; n = 135) with few from medium(12%; n = 21) or low (13%; n = 23)support residences. Of the total, 39% weredischarged home or to family. A total of27% (n = 48) were discharged to a highersupport level, while 7% (n = 12) weredischarged to the same level of supportand 18% (n = 33) to a lower level ofsupport. Only two residents weredischarged to nursing homes and threewere discharged to a hospice. A total of11 residents were discharged to a general
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND60
High Medium Low Total
Less than 6 months prior to the study 89 (24.8) 34 (22.4) 14 (36.8) 137 (24.9)
6 – 12 months prior to the study 79 (22.0) 34 (22.4) 9 (23.7) 122 (22.2)
13 – 36 months prior to the study 191 (53.2) 84 (55.2) 15 (39.5) 290 (52.8)
Total 359 (65.4) 152 (27.7) 38 (6.9) 549 (100.0)
Table 4.5 Number (%) of admissions in the last three years (2002 – 2004), by level of support
High Medium Low Total
Higher support 36 (26.7) 7 (33.3) 5 (21.8) 48 (26.8)
Same level of support 5 (3.7) 2 (9.5) 5 (21.8) 12 (6.7)
Lower support 27 (20.0) 5 (24.0) 1 (4.3) 33 (18.4)
Home / family 56 (41.5) 7 (33.3) 7 (30.4) 70 (39.1)
General hospital 8 (6.0) 0 3 (13.0) 11 (6.1)
Hospice / nursing home 3 (2.2) 0 2 (8.7) 5 (2.8)
Total 135 (100.0) 21 (100.0) 23 (100.0) 179 (100.0)
Table 4.6 Total number of residents discharged and place discharged to, by level of support

hospital. Over a quarter (27%) of thedischarges from high support residenceswere to higher levels of support. Althoughthe questionnaire did not specify to whichunit the discharges went, it may beassumed that a higher level of support forthose in a high support residence wouldbe an inpatient facility. One-third of thosefrom medium support and 22% of thosedischarged from low support went tohigher levels of support. Nearly half of thehigh support discharges went home or tofamily (41%), while 33% of thosedischarged from medium support and30% of those discharged from lowsupport were discharged home or tofamily.
4.4 USE OF PLACES, EXCLUSIONCRITERIA AND WAITING LISTS
4.4.1 Respite and crisis beds
Of the total 951 places (beds) in theresidences, 55 were designated asrespite beds (n = 46) or crisis beds(n = 9). The nursing officersreported that these beds wereprovided in 29% (31 / 102) of theresidences. The majority of therespite beds were in high support(37 / 46) as were the majority of
crisis beds (7 / 9). It was alsoreported that a total of 21% (21 /102) of the residences had beds thathad been used to accommodatetransfers from acute units due tobed shortages. Again the majority ofthese beds were in high supportresidences (16 / 21). Of the totalnumber having designated respitebeds (n = 24), 17 had policiesregarding the use of such beds. Ofthe total number of residenceshaving designated crisis beds (n =seven), four had related policies.Only five of the residences hadpolicies relating to the use of bedsfor transfers from acute units.
4.4.2 Exclusion criteria and waitinglists
The questionnaire provided a list ofpossible exclusion criteria foradmission to the residences andrespondents were asked to indicatewhich ones applied in their case. In64% one or more of the exclusioncriteria for admission to theresidences were employed (Table4.7). The majority of high support(81%) and low support (63%)residences employed exclusioncriteria, as did 40% of the mediumsupport. Severe physical disease
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 61
High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
Applying any exclusion criteria 29 (80.6) 10 (40.0) 26 (63.4) 65 (63.7)
Excluding acute psychotic disorders 19 (52.8) 2 (8.0) 17 (41.5) 38 (37.3)
Excluding substance abuse 9 (25.0) 2 (8.0) 2 (4.9) 13 (12.7)
Excluding alcohol abuse 11 (30.6) 7 (28.0) 8 (19.5) 26 (25.5)
Excluding severe physical disease 22 (61.1) 7 (28.0) 23 (56.1) 52 (51.0)
Excluding organic brain disease 19 (52.8) 6 (64.0) 23 (56.1) 48 (47.1)
Excluding intellectual disability 9 (25.0) 6 (24.0) 11 (26.8) 26 (25.5)
Excluding violent behaviours 14 (38.9) 7 (28.0) 13 (31.7) 34 (33.3)
Excluding former CMH patient 7 (19.4) 2 (8.0) 9 (22.0) 18 (17.6)
Table 4.7 Number (%) of residences employing exclusion criteria and the specific exclusioncriteria employed, by level of support

(51%) and organic brain disease(47%) were the most frequentlyemployed exclusion criteria. Overone-third of the residences reportedthat they employed criteriaexcluding those with substance and/ or alcohol abuse problems (38%)or violent behaviours (33%).
A total of 31% of high, 32% of mediumand 5% of low support residences hadwaiting lists for placements. Only two ofthe residences reported estimated waitingtime for a place in the residence. Thesewaiting times were six weeks and twelveweeks.
4.5 MANAGEMENT AND POLICES
4.5.1 Placement rights
The nursing officers of theresidences were asked who hadownership of beds (placementrights), referring to who hadresponsibility for admissions anddischarges to the residences. Thenursing officers reported that theplacement rights lay with the HSElocal area in 12% of the residences.A total of 34% of the nursingofficers specifically stated that theplacement rights lay with theconsultant psychiatrist. A largeproportion of the placement rightswere regarded as being with therehabilitation team (31%; n = 32)while 13% of the nursing officersreported that the placement rightslay with the sector team. In only oneinstance was it reported thatplacement rights lay with the acutehospital, and 9% reported that theplacement rights lay with the socialsupport team.
4.5.2 Assessment
Just over half of the residences(55%) had carried out a formalassessment of residents prior toadmission, while 27% had aninformal assessment and 14% hadno assessment procedure. Thequestion was not answered in 4% ofthe residences. Over half of the high
(53%) and medium (84%) supportresidences, and 39% of the lowsupport residences had a formalassessment procedure. Of the highsupport residences, 44% performedinformal assessments of theresidents, while 4% of the mediumand 27% of the low supportresidences had such an assessmentprior to admission. One highsupport facility (3%) had noassessment procedure and 13 (32%)of the low support residences hadno assessment procedure. All of themedium support residences thatanswered the question reportedhaving assessments (3 did notanswer).
4.5.3 Staff meetings
In half of the residences, there wereno planned formal staff meetings(51%). A total of 44% of mediumand 71% of low support residenceshad no formal staff meetings.However, the majority of the highsupport residences had plannedformal meetings for staff (72%). Thenursing officers reported that themajority of the residences had staffmeetings to discuss the treatmentprovided to residents and responseto treatment (81%). Over half of theresidences (52%) did not haveplanned meetings open to residentsto discuss the organisation andprocedures of the residence. Fewresidences had planned meetingswith relatives (15%).
4.5.4 Quality monitoring
A total of 27% of the residences hadan evaluation and review plan formonitoring of the services.Regarding evaluation of the qualityservices and management in theresidences, only 22% of theresidences used performanceindicators to evaluate the service,23% logged surveillance ofproblematic situations, 19%monitored residents’ satisfaction and17% monitored family satisfaction.
4.5.5 Health and safety
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND62

The majority of residences hadpolicies in place regarding healthand safety issues (Table 4.8). Fewhad information on treatmentintervention programmes (32.4%) orresident and family feedback (47%).Over half of the high supportresidences had information onintervention programmes (61%) andobtained resident and familyfeedback (56%). Less than half ofthe high (47%) and low (37%)support residences providedinformation packs for residents,while only 52% of medium supportresidences provided such packs.
4.5.6 Rules and regulations
Table 4.9 shows the number ofresidences where rules andregulations were imposed on theresidents. The table shows that therewas little difference between thethree levels of support in thefrequency with which rules andregulations were employed inrelation to unsupervised leave,locking of the bathroom door,unscheduled visiting hours andunscheduled bedtimes.
4.5.6.1 Leaving the residence
In the high supportresidences, staff supervisedthe daytime comings andgoings of the residents andin only 22% were residentsprovided with front doorkeys. Bedtime checks werecarried out in all highsupport residences and86% required residents tonotify staff if they weregoing out, compared with64% of medium and 10%of low support residences.It is interesting to notethat, while low supportresidences were notstaffed, a small proportionappeared to restrictresidents’ activities. Forexample, in 10% of lowsupport residences thecomings and goings ofresidents were supervised,while in 71% residentswere required to be up ata certain time duringweekdays. Furthermore, in10% it was reported thatresidents were required toinform staff where theywere going.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 63
2 One question, relating to problems with living conditions, was omitted as irrelevant to the study.
High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
Dangerous situations 35 (97.2) 22 (88.0) 35 (85.4) 92 (90.2)
Health and safety policy 36 (100) 16 (64.0) 26 (63.4) 78 (76.5)
Electronic fire alarm 36 (100) 23 (92.0) 39 (95.1) 98 (96.1)
Intervention programmes 22 (61.1) 7 (28.0) 4 (9.8) 33 (32.4)
Resident and family feedback 20 (55.6) 6 (24.0) 22 (53.7) 48 (47.1)
FOI / Protection act information 24 (66.7) 16 (64.0) 34 (82.9) 74 (72.5)
Emergency telephone numbers 24 (66.7) 23 (92.0) 37 (90.2) 84 (82.4)
Information pack for residents 17 (47.2) 13 (52.0) 15 (36.6) 45 (44.1)
Table 4.8 Number (%) of residences that had polices on health and safety and related matters,by level of support

4.5.6.2 Bedroom use and privacy
Table 4.10 shows thenumber of residenceswhere rules andregulations concerningbedroom use and privacywere imposed. Regardingprivacy, it was reported inthe majority of communityresidences that residentshad access to their ownspace (86% of high, 100%of medium and 93% oflow support residences).Nursing officers reportedthat only a few of theresidences allowedresidents the choice ofsingle rooms, although68% of low supportresidences were able toprovide residents with thechoice of single rooms. AsTable 4.3 shows, thesharing of rooms was mostlikely due to the lack ofsingle rooms in the
residences. The majority ofresidents had to share aroom, yet in only 58% ofhigh, 12% of medium and49% of low supportresidences were residentsgiven the choice of whomto share the room with.Again, this was most likelya result of the inability ofresidences to provideresidents with a choice oftype of room. Residentswere allowed in bedroomsduring the day in over halfof the residences, but itwas reported that this wasnot encouraged. It wasreported, that in 61% ofthe low supportresidences, residents wereable to lock the bedroomdoors; in only 19% of thehigh and 28% of themedium supportresidences were residentsallowed to do so. Again,
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND64
High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
Supervised daytime comings and going (yes) 36 (100) 5 (20.0) 4 (9.8) 45 (44.1)
Unsupervised leave (yes) 34 (94.4) 23 (92.0) 41 (100) 98 (96.1)
Front door key (yes) 8 (22.2) 22 (88.0) 41 (100) 71 (69.6)
Lock bathroom (yes) 29 (80.6) 22 (88.0) 41 (100) 92 (90.2)
Scheduled visiting hours for visitors (yes) 2 (5.6) 3 (12.0) 1 (2.4) 6 (5.9)
Scheduled bedtime for residents (no) 29 (80.6) 20 (80.0) 41 (100) 90 (88.2)
Bedtime checks by staff (yes) 36 (100) 21 (84.0) 2 (4.9) 59 (57.8)
Residents had to be up at certain time during weekdays (yes) 33 (91.7) 20 (80.0) 29 (70.7) 82 (80.4)
Residents had to be up at certain time during be up weekends/ holidays (yes) 12 (33.3) 2 (8.0) 1 (2.4) 15 (14.7)
Residents informed staff where they are going (yes) 31 (86.1) 16 (64.0) 4 (9.8) 51 (50.0)
Residents check in at certain time (yes) 20 (55.6) 14 (56.0) 4 (9.8) 38 (37.3)
Table 4.9 Number (%) of residences that imposed rules and regulations concerning freedomwithin the residences, by level of support

this could have been afeature of shared rooms asopposed to a restriction onaccess to bedrooms. Asexpected, the nursingofficers reported that lessthan 3% of high ormedium supportresidences allowedresidents to smoke in thebedrooms, as compared to20% of the low supportresidences.
4.5.6.3 Restrictiveness
In order to assess the overallcharacteristics of the socialclimate of the residences arestrictiveness score wascomposed by the researcherusing the 22 items on thequestionnaire dealing with theinternal rules of the residence.The researcher scored eachitem as ‘0’ (absent) or ‘1’(present). Restrictivenessscores could range from 0 -22, with higher scoresindicating a higher degree ofrestrictiveness. The meanrestrictiveness score wassignificantly different in thethree levels of support (F(2,101) = 70.94, p < 0.001),with the high support beingmore restrictive. The meanrestrictiveness score for high
support was 11.0, while formedium it was 8.4 and lowwas 3.8.
4.5.7 Food
Table 4.11 shows who hadresponsibility for the preparation ofthe resident’s food. A quarter ofboth high support (25%) and lowsupport (24%) residences had theirfood prepared by kitchen staff in apsychiatric unit or hospital. Kitchenstaff prepared the food in themajority of high support residences(58%), while the staff and residentsprepared the food in the majority ofthe medium support residences(52%). Care staff and residents(44%) or residents themselves (39%)prepared the food in the lowsupport residences.
4.6 SUMMARY
The majority of the residents were 46 yearsof age or over at the time of the study.One-third were over the age of 65 years.The age profile in the high supportresidences was older than that in themedium and low support, and theyoungest age profile was in the mediumsupport residences. The majority of theresidents had a primary diagnosis ofschizophrenia. A very small proportion ofresidents were employed either in thecommunity or in sheltered employment.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 65
High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
Residents stay in bedrooms during daytime (yes) 22 (61.1) 12 (48.0) 26 (63.4) 60 (58.8)
Can residents lock bedroom? (yes) 7 (19.4) 7 (28.0) 25 (61.0) 39 (38.2)
Can residents smoke in bedrooms? (yes) 1 (2.8) 1 (2.8) 8 (19.5) 10 (9.8)
Do residents have their own space? (yes) 31 (86.1) 25 (100) 38 (92.7) 94 (92.2)
Can residents choose whom to share room with? (yes) 21 (58.3) 3 (12.0) 20 (48.8) 44 (43.1)
Can residents choose single rooms? (yes) 11 (30.6) 5 (20.0) 28 (68.3) 44 (43.1)
Table 4.10 Number (%) of residences that had rules and regulations concerning bedroomuse and privacy, by level of support

The data presented here detail theprovision of all community residences inthe three study areas. On average, highsupport residences provided 16.2 (SD7.76) places per residence, mediumsupport residences provided 6.9 (SD 2.24)places and low support residencesprovided 4.90 (SD 1.94) places. There wasa total of 951 places with over half in highsupport (60%), one-fifth in low support(21%) and only 16% in medium support.Not all the places were occupied at thetime of the study, with only 871 people inthe residences. This resulted in 80 emptyplaces, although there were 55 designatedrespite or crisis places and 21 residencesreported having to use places for transfersfrom acute units, making a total of 76such places. The issue of whether places incommunity residences should be used forthese purposes is discussed in Chapter 10.Very few single rooms were available inhigh support residences, with slightly moreavailable in medium and low supportresidences. There was a higher ratio ofresidents to bathrooms in high supportresidences than in medium or low support.
The majority of the residences weresituated in urban areas and were ownedby the HSE. The length of time taken towalk from the community residences tolocal amenities such as the shops, postoffice or GP was, on average, less than 20minutes. However, the time taken to reachthe day hospital or day centre from thecommunity residences by transport was,on average, over half an hour for those in
high support. Very few of the residentshad their own transport, while just over aquarter of the facilities had access to aminibus. Less than half of the high supportresidences had access to a minibus and, ofthose that had, just over one-third of theresidences shared the minibus with otherresidences.
A total of 259 admissions and 179discharges were reported for the 12months prior to the study. The majority ofthese related to high support residences.
Over half of the community residencesreported that they employed one or morecriteria for excluding potential residents.The exclusion criteria most frequentlyreported were severe physical disease andorganic brain disorder. It was reported thata large proportion of the residencestended to exclude those who might havebeen more difficult to treat (i.e. substanceand alcohol abusers and those with violentbehaviours).
Waiting lists were reported forapproximately one-third of the high andmedium support residences, while a muchlower proportion of the low supportresidences reported waiting lists. Theapproximate time on the waiting list wasnot reported for the majority of residences.
While over half of the residences a formalassessment procedure was reported to bein operation, few had planned meetingsthat involved staff and residents orresidents’ families. The majority had
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND66
High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
Psychiatric hospital kitchen staff 9 (25.0) 1 (4.0) 10 (24.4) 20 (19.6)
Residents 1 (2.8) 5 (20.0) 16 (39.0) 22 (21.6)
Staff 1 (2.8) 5 (20.0) 4 (9.8) 10 (9.8)
Staff and residents 11 (30.6) 13 (52.0) 18 (43.9) 42 (41.2)
Kitchen staff 21 (58.3) 1 (4.0) 3 (7.3) 25 (24.5)
Staff, kitchen staff, residents 2 (5.6) 1 (4.0) 0 3 (2.9)
Table 4.11 Number (%) of residences and the responsibility for food preparation, by level ofsupport

polices regarding health and safety,dangerous situations, freedom ofinformation and emergency telephonenumbers. However, few had polices inplace that concerned interventionprogrammes or feedback from residentsand families.
The results suggested that the highsupport facilities were the most restrictivein terms of the internal rules of theresidence. This was followed by themedium support facilities, with the lowsupport residences the least restrictive.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 67

A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND68

CHAPTER 5Residents: Clinical, Physicaland Social Functioning

We now pass from description of the entirenumber of residents (871) to the sample of 138who were interviewed. We begin with a reviewof the demographic, clinical and functionalcharacteristics of these 138 residents andcontinue with a review of the perceivedappropriateness of their placement. Clinicalstatus and functioning are then presented on thebasis of data obtained by the researcher bymeans of the key-worker questionnaire and theresidents themselves (through self-reportDisability Assessment Scale II (DAS II)).
5.1 DEMOGRAPHIC AND CLINICALCHARACTERISTICS OF THESAMPLE
5.1.1 Demography
A sample of 138 residents wasinterviewed for the study,comprising 16% of the totalresidents in the three participatingareas (138 / 871). Of these, 59% (n= 82) were from high supportresidences, 18% (n = 25) were frommedium support residences and22% (n = 31) were from lowsupport residences. This comparesto 64% of high support residents,18% of medium support residentsand 19% of low support residents inall community residential facilities inthe three study areas.
There was no significant genderdifference in the sample (males49%, females 51%; p > 0.05), norwas there any significant genderdifference, by level of support (p >0.05). There was a slightly lowerproportion of males than females inthe sample interviewed (49%) asopposed to the total residentsreported for all residences (61%) inthe area.
The mean age of the sample was53.7 years (SD 13.4). The age rangewas 22 to 88 years and there wasno significant difference in the meanages between high (mean 53.7years, SD 12.5), medium (mean 58.2years, SD 13.3) and low (mean50.16 years, SD 15.1) support.
The largest proportion of the samplewas aged between 46 and 65 years(57%). Only 24% (n = 33) of theresidents were under the age of 45years. A total of 22% (n = 31) wereover the age of 65 years while 9%(n = 13) were under the age of 35years. Of those in the high supportresidences, 22% were over the ageof 65 years, compared with 28% inmedium support and 19% in lowsupport residences. The age profileof the sample of residentsinterviewed was very similar to thatreported for all 871 residents. Inboth groups a large proportion ofthe residents were between the agesof 46 and 65 years (47% versus57%). Only a small proportion inboth groups were under the age of35 years (both 9%).
A large proportion of the sample weresingle (87%), with 3% married and 10%separated or divorced. Few had post-secondary or third-level education (22%);however, 46% had attended secondaryschool.
Not unexpectedly a total of 40% of thesample were unemployed. Only 2% wereemployed full time and only 5% wereemployed part time. A total of 27% werein sheltered employment. This gives a totalof 34% of the sampled residents insheltered or paid employment. A total of25% of the sample were in training, oncourses or retired. Comparisons withinformation from all residents in residentialfacilities would suggest that a greaterproportion of those sampled wereemployed. For example, 5% of all residentswere reported as being in paidemployment and 15% were reported asbeing in sheltered employment.
5.1.2 Psychiatric history
The duration of illness ranged from3 to 62 years, with a mean durationof 26.6 years. The age of firstcontact with services ranged from15 to 70 years, with a mean age of26.3 years. The length of time thatthe residents had lived in theircurrent accommodation rangedfrom 0.5 to 25 years, with an overall
Chapter 5
Residents: clinical, physical and social functioning
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND70

mean of 6.8 years. One-way ANOVAon the mean length of time theresident had lived in the currentaccommodation showed that thosein medium support residences hadbeen there significantly longer(mean 8.52 years) than those inhigh (mean 5.2 years) or low (mean6.8 years) support residences (F (2,137) = 3.89, p < 0.05). Despitethese relatively lengthy periods ofresidence, there was significantmovement in and out of theresidences, as evidenced by thenumber of admissions in the past 12months as detailed in Section 4.3.
The majority of the residents hadhad periods of inpatienthospitalisations (97%) in psychiatricunits or hospitals. Hospitalisationwhile a resident was greatest forthose in low support (42%), whileonly 27% of high and 20% ofmedium support residents werehospitalised while a resident. A largeproportion of the sample had nohospital admissions in the last fiveyears (64%), with a greaterproportion of the medium support(82%) than the high (61%) or low(59%) support residents having hadno admissions. For those who hadinpatient hospitalisations in the lastfive years, the average number ofadmissions was 2.6. There was nosignificant difference (p > 0.05)between the average number ofhospitalisations for residents in high(mean 3.0), medium (mean 1.7) andlow (mean 1.8) support residences.
Regarding the course of illness inthe last five years, only 9% of theresidents had an absence ofsymptoms. These included 5% ofhigh support, 20% of mediumsupport and 13% of low support.Remission with intermittent episodesover the last five years was evidentin 5% of the residents, while partialremission was evident in 16%. Themost commonly reported course ofillness in the last five years for high(66%), medium (60%) and low(52%) support residents was
symptoms that were persistent, butstable. Only 3% of the residentswere reported as having progressivedeterioration.
5.2 CLINICAL, SOCIAL AND PHYSICALFUNCTIONING AND LEVEL OFDISABILITY IN EVERYDAY LIVINGACTIVITIES
5.2.1 Clinical functioning
5.2.1.1 Level of symptoms
The Brief Psychiatric RatingScale (BPRS) wascompleted by theresearcher at the interviewwith the resident. The scalewas used to measure thepsychopathology of theresidents over the twoweeks prior to interview.The 24 symptomsmeasured are rated on aseven-point scale (i.e. 1 =no symptoms, 7=extremely severesymptoms). The totalscores on the BPRS canrange from 24 (nosymptoms present) to 168(extremely severe in allsymptoms). The averageBPRS score was 35.8(range 24 – 76) for highsupport residents, 30.2(range 24 – 45) formedium support residentsand 30.3 (range 24 – 45)for low support residentsindicating that BPRS meanscores for all groups werein the mild category. Notsurprisingly however therewere significant groupdifferences, with thosefrom low supportresidences having asignificantly lower scorethan those from highsupport residences (F (2,128) = 8.96, p = 0.01).
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 71

5.2.1.2 Global functioning
The Global Assessment ofFunctioning Scale (GAF)provided a measure of theclinician’s judgement ofthe individual’s overallcurrent level offunctioning. It takes intoconsiderationpsychological, social andoccupational functioningon a hypotheticalcontinuum of mentalhealth– illness. Eachindividual was rated on ascale of 0 – 100, withhigher scores indicatingsuperior functioning. Themean score of the highsupport residents (55.37;range 20 – 90) fell withinthe moderate symptomrange (moderate symptomsor moderate difficulty insocial or occupationalfunctioning), while themean scores for theresidents in mediumsupport (66.84; range 35 -95) and in low support(61.94; range 25– 85) fellwithin the mild symptomsrange (some mildsymptoms or somedifficulty in social oroccupational functioning,but generally functioningpretty well and has somemeaningful interpersonalrelationships). There was asignificant difference inmean GAF scores betweenthe levels of support (F (2,137) = 4.92, p < 0.01).The high support groupscored significantly lowerthan the medium and lowsupport groups, with themedium support residentshaving the highest level offunctioning.
5.2.1.3 Psychopathology anddisability
The Health of the Nation
Outcome Scale (HoNOS)was designed to assesspsychopathology anddisability in the two weeksprior to interview. It is a12-item scale measuringclinical and socialfunctioning and is rated ona five-point scale (0 – 4),with 3 – 4 indicatingsignificant or severeproblems.2 Total scores onthe HoNOS used in thisstudy can range from 0 –44. Table 5.1 shows thepercentage of residents ineach of the categories foreach individual item.
Total scores were computed for residentsand subjected to a Kruskal Wallis Test.Analysis on the total HoNOS scores yieldedsignificant group differences (p < 0.001).Those in high support residences hadhigher mean scores (11.9; range 0 - 30)than those in medium (5.6; range 0 - 17)or in low support (6.2; range 0 - 26).
5.2.2 Physical Health Index
The Physical Health Index (PHI) wasused to measure the physical healthof the sample of residents and wascomprised of eight items. This wascompleted by the key workers. Thisquestionnaire asked about physicalhealth disabilities in eight domainsand was rated on a four-point scalefrom 0 – 3. Total scores on the PHIcan range from 0 – 24. Table 5.2summarises the results on each ofthe PHI items. As can be seen, andcontrary to expectations given theage and clinical profile, a fewresidents were experiencingmoderate to severe health problemswith the majority experiencing nodisabilities. The mean scores for thethree groups were 1.79 (range 0 –13) for high support residents, 0.80(range 0 – 5) for medium supportresidents and 1.06 (range 0 – 6) forlow support residents. A one-wayANOVA comparing the mean scoreswas not significant (p > 0.05).
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND72

5.2.3 Functioning in the last thirtydays
The WHO Disability AssessmentScale (DAS II) is a measure offunctioning and disability. The scaleis a 12-item questionnaire and eachitem is rated on a five point scalefrom 0 – 4. Total scores can rangefrom 0 – 48 with a lower scoreindicating less disability. It assessesfunctioning and disabilities in the
last 30 days. The domains offunctioning assessed by the DAS IIinclude understanding andcommunicating, getting around, selfcare, getting along with others,household and work activities andparticipation in society. Two DAS IIquestionnaires were employed in thecurrent study. One was completedby the key worker for the residentand one was based on the self
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 73
Item No problem Minor / mild Moderate/ severe
Overactive, aggressive, disruptive or agitated behaviour 65.9 21.0 11.6
Non-accidental self-injury 95.7 2.2 0.7
Problem drinking or drug taking 84.1 14.5 0.7
Cognitive problems 42.0 38.4 17.4
Physical illness or disability problems 60.9 27.5 10.8
Problems associated with hallucinations and delusions 47.8 34.0 16.6
Problems with depressed mood 47.8 44.2 6.5
Other mental and behavioural problems 47.8 34.0 14.4
Problems with relationships 44.9 39.1 15.2
Problems with activities of daily living 33.3 38.4 26.8
Problems with occupation and activities 37.0 34.0 26.1
Table 5.1 Percentage of residents in each category of the HoNOS individual items
Disability No Mild Moderate Severe disability disability disability disability
Cardiovascular 84.1 10.1 5.8 0
Respiratory 85.5 5.8 8.7 0
Digestive 83.3 11.6 4.3 0.7
Urogential 92.0 2.2 4.3 1.4
Motor 89.1 5.8 4.3 0.7
Central nervous system 87.0 6.5 6.5 0
Metabolic / endocrine system 82.6 9.4 7.2 0.7
Infective system (including HIV) 100 0 0 0
Table 5.2 Percentage of residents experiencing physical health disabilities

report of the residents. Thus twoDAS II questionnaires werecompleted for every resident. Thisallowed comparison between theresident’s perception of their ownfunctioning and the key worker’sperception of the functioning of theresident. There was a significantpositive correlation, albeit weak,between resident’s total DAS IIscores and the key worker’s rating ofthe resident (Pearson’s r = 0.314, p< 0.001). However, it is importantto note that while there was asignificant correlation between thescores, the total mean scoresdiffered between the residents’ andthe key workers’ ratings (t (237.3) =-5.43, p < 0.001). The total meanscore for the residents’ ratings was6.35 (range 0 – 34) and the totalmean score provided by the keyworkers was 12.51 (range 0 – 46).Kruskal Wallis Tests on both scoresyielded significant differencesbetween residents in high, mediumand low support residences (residentratings p < 0.01; key worker ratings(p < 0.001). In both analyses, notunexpectedly, the high supportresidents had greater mean scoressuggesting that they experiencedgreater disability than the mediumand low support residents.
5.3 APPROPRIATENESS OFPLACEMENT
The key workers were asked to indicatewhether they thought the resident wasappropriately placed in the residence atthe time of the study. Of all residents, 85%were reported as being appropriatelyplaced and 2% of the residents’ keyworkers reported that they were unsure ofthe appropriateness of placement. A totalof 17 (13%) residents were reported bykey workers as being inappropriatelyplaced. Of these, ten were in high supportresidences, two were in medium supportresidences and five were in low supportresidences. Only three residents (one eachin high, medium and low residences) werereported as being more appropriately
placed in independent living. It wasreported that four would be better placedin an independent group home (two highand two low support residents) and four(two high and two low support residents)would be better placed in a mediumsupport home. A total of two residentswould be better placed in a higher support(one high and one medium supportresident) and another two would be betterplaced in a nursing home (two highsupport residents). The main barrier toappropriate placement was unavailablefacilities (n = 8), while three reported thata facility was available but had a waitinglist. The mental state of the resident wasreported as the precluding discharge ofthree of the residents inappropriatelyplaced. In two of the inappropriatelyplaced residents, the resident’s relativeshad refused transfers and in one thedoctor’s opinion was considered to havebeen a barrier to appropriate placement.
The key workers were asked where theysaw the resident living in six months time.A total of 88% of the key workers reportedthat the residents would be living in thesame residences. Only six residents werepredicted to be living in lower support andonly two were predicted as living inindependent accommodation.
5.4 SUMMARY
A total of 138 residents participated in theinterview stage of the study. This samplewas 16% of the total number of residentsin the three study areas. The majority ofthe participating sample of residents werefrom high support residences (59%), while18% were from medium support and 22%from low support. The sample of residentsinterviewed was representative of those inall the residences in terms of gender andage. The employment question for thesample of residents interviewed enquiredas to whether the resident was in training,education or retired while the question forthe nursing officers only sought the totalnumber of residents in sheltered or paidemployment. When looking at theproportions in sheltered and paidemployment, the results for all residents in
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND74

the residences and the residents that wereinterviewed were similar for paidemployment. For example, 7% of thesample interviewed was in paidemployment compared to 5% of allresidents in the residences. Of theresidents interviewed, 27% were insheltered employment compared to 15%of the total sample.
The duration of illness among theresidents interviewed ranged from three tosixty-two years. The average duration ofillness was 26 years and the average ageat first contact with services was 26 years.The residents had lived in their currentaccommodation for an average of sevenyears. Residents in the medium supportresidences were significantly longer in theircurrent accommodation than those in highor low support. Notwithstanding thestatistical significance of the result, therewas little difference in the average lengthof time in the current accommodation,with a difference of approximately threeyears from the highest average length oftime to the lowest. The majority of theresidents had had previoushospitalisations, but a smaller percentagehad had inpatient hospitalisations in theprevious five years. Only a few of theresidents were reported as having anabsence of symptoms in the previous fiveyears. Of those who had symptoms, forthe majority the symptoms werepersistent, but stable. This is in line withfindings regarding current symptomswhere the resident’s mean score indicatedthat symptoms were present, but mild.The majority of the residents were judgedby key worker as being appropriatelyplaced at the time of the study. Of thosewho were inappropriately placed, it wasreported that the majority would be betterplaced in independent group homes or inmedium support residences. The mainbarriers perceived by key workers toappropriate placement were unavailabilityof appropriate facilities. Furthermore, keyworkers predicted that the majority ofresidents would be in the sameaccommodation in six months’ time.
There was a significant difference in theoverall current level of functioning of theresidents between high, medium and low
support residences, with residents fromhigh support having poorer functioning tothose in medium or low support. Theresidents in high support were reported ashaving moderate difficulties in social oroccupational functioning, while those inmedium and low support were reported ashaving mild difficulties.
Regarding clinical and social functioning inthe previous two weeks, the majority ofthe residents were reported by key workersas having no problems. An exception tothis was in relation to activities of dailyliving. Over one-third of the residents werereported as having mild problems and overa quarter were reported as havingmoderate to severe difficulties. There wasa significant difference between thegroups on the total score, indicating thatthe high support residents had poorerfunctioning to those in medium and lowsupport.
The majority of residents were reported bythe key workers as having no currentphysical health problems and there was nosignificant difference between the physicalhealth functioning of residents in high,medium and low support residences.
Functioning and disability in relation tocommunication, self-care, social contacts,activities and participation in society overthe last month were rated by key workersand by the residents themselves. Theresults showed that overall, the keyworkers rated the residents’ functioning aslower than that provided by the resident’sthemselves. There was weak significantpositive correlation between the scores,demonstrating that the higher theresident’s rating of functioning, the higherthe key worker’s rating also. The residentsin high support were reported, both bythe key workers and by themselves, asfunctioning at a lower level than those inmedium or low support.
In most areas the high support residentswere functioning at a significantly lowerlevel than the medium and low supportresidents although the extent to which thislower level of functioning would affectindependent living is questionable. Forexample, the findings highlighted that the
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 75

majority of the residents were experiencingfew problems in clinical, physical andsocial functioning and it was only in theactivities of daily living that mild tomoderate problems were evident. Yet thekey workers judged the majority ofresidents to be appropriately placed,whether in high, medium or low supportfacilities. This anomaly causes someconcern and would suggest that the careprovided to residents in communityresidences may over-provide for theirneeds.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND76

CHAPTER 6Citizenship: Social Support,Community Integration andRights

This chapter provides information on the sampleof 138 residents relating to their status ascitizens, as supplied by key workers and residentsand, in the case of rights, by the facilitiesquestionnaire.
6.1 SOCIAL SUPPORT,INDEPENDENCE ANDCOMMUNITY INTEGRATION
6.1.1 Social support
The social support network of theresidents was assessed by the self-reports of the residents and byasking the key worker questionsregarding visits to family and friendsand the system of support providedto the resident in the last year.
Table 6.1 presents the key workers’reported system of support (i.e.family and friends) for the residentsin high, medium and low levels ofsupport over the last year. A total of38% were perceived to have familyand friends who were interested andwilling to provide support. The keyworkers reported that 24% ofresidents had a support systemavailable, but that family and friendshad doubts about their ability toprovide support. The key workersreported that 11% of the residentshad family and friends with thepotential to provide support, butthat they had severe difficulties inputting this into action. It wasreported that a total of 28% of theresidents had no family or friends toprovide support.
Key workers were asked to indicatewhether the residents had visits fromfamily and friends or if the residents wentto visit family and friends. A total of 72%of high, 56% of medium and 55% of lowsupport residents had visits from familyand friends to the residence, while 68% ofhigh, 76% of medium and 84% of lowsupport residents visited family and friendsin their own homes.
The residents’ self-reported social supportnetwork was assessed in four domains –everyday psychological support, everydayinstrumental support, instrumental crisissupport and psychological crisis support.Examples of these social support domainsinclude:
Everyday psychological support – whomdo you like to do everyday things with?
Everyday instrumental support - whomdo you turn to when you need a smallfavour?
Instrumental crisis support – whomwould you discuss an importantdecision with?
Psychological crisis support – whomwould you turn to if you wanted to talkto someone during an upsetting time?
Residents were asked to indicate whetherthey would use social support networks(i.e. nursing or care staff, other residentsor family and friends from outside theresidence) in the above scenarios and, ifso, whom would they ask for help. Figure6.1 shows the percentage of residentswho would seek help from others in each
Chapter 6
Citizenship: social support, community integration and rights
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND78
High Medium Low Total(n = 82) (n = 25) (n = 31) (n = 138)
Family / friends interested and willing to provide support 27 (32.9) 12 (48.0) 13 (41.9) 52 (37.7)
Family / friends have doubts about ability to provide support 18 (22.0) 6 (24.0) 9 (29.0) 33 (23.9)
Potential to provide support but severe difficulties putting into action 13 (15.9) 1 (4.0) 1 (3.2) 15 (10.9)
Absence of family / friends to provide support 24 (29.3) 6 (24.0) 8 (25.8) 38 (27.5)
Total 82 (100.0) 25 (100.0) 31 (100.0) 138 (100.0)
Table 6.1 Key workers’ reported system of support for residents (number (%)) in the last year

of the social support domains. This showsthat support was sought from only nursingand care staff most often for everydayinstrumental support, instrumental crisissupport and psychological crisis support.Only family and friends or only otherresidents were most often reported asproviding everyday psychological support.All three groups of support networkstogether (i.e. staff, family or friends andother residents) were seldom sought forsupport. A total of 25% of residentsreported that they had no one to doeveryday things with (everydaypsychological support). Likewise, 23%reported that there was no one to whomthey would turn to during times ofpsychological need (psychological crisissupport). A total of 20% reported thatthey would not ask anyone to do a favourfor them (everyday instrumental support)and 18% reported that would not askanyone for support if they had to make animportant decision (instrumental crisissupport).
To summarise the social support providedand availed of by residents, it was reportedby the key workers that over a quarter of
the residents had no family or friends toprovide support. For the majority of theresidents (62%) it was reported that familyand friends were present to providesupport, although for 24% doubts as totheir ability to provide support wasreported. It was reported that 73% of theresidents went to visit family and friendsand 65% had visits from family andfriends. A quarter of the residents reportedthat they would ask nobody for everydaypsychological support or psychologicalcrisis support. The residents reported thatthey would most likely ask nurses / staffwhen in need of a small favour, when theywanted to discuss an important decisionor when they wanted to talk aboutsomething that was upsetting them. Incontrast, family and friends were reportedas the support network most likely to turnto for everyday psychological support.
6.1.2 Independence and communityintegration
Residents were asked to indicatewhether they were aware of themoney they received weekly, if theyvoted and if they left the residenceson their own, for example to visit
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 79
0
5
10
15
20
25
30
35
40%
of
resi
dent
s
Support Network
Nursin
g / c
are s
taff
Other
resid
ents
Fam
ily / f
riend
s
Nurse
s and
oth
er re
siden
ts
Other
resid
ents
and
Fam
ily / f
riend
s
All thr
ee g
roup
s
Wou
ld tu
rn to
nob
ody
Everyday psychologicalsupport
Everyday instrumentalsupport
Instrumental crisis support
Psychological crisis support
Figure 6.1 Resident’s reported social support network in four domains

the general practitioner. The majority(71%) of the residents were awareof the amount of money theyreceived each week. Just over half(51%) received help to manage theirfinances. There were no significantdifferences in the awareness andmanagement of finances betweenthose in high, medium and lowsupport residences (Chi-square, p >0.05).
A total of 78% of residents voted.The majority of residents went outon their own (85%). Differences inthe proportion of residents fromhigh, medium and low support thatreported voting and going out ontheir own were not statisticallysignificant (Chi-square, p > 0.05).Only 66% of the high supportresidents visited the GP bythemselves, while 84% of themedium support and 84% of lowsupport residents did so.
Residents were asked if theyattended particular activities in thecommunity such as bingo,community centres and so on (Table6.2). Of all residents, only a smallpercentage reported attendingactivities in the community with thehighest proportion attending pubsetc. (see Table 6.2). There weresignificant differences in theproportions of residents from high,medium and low support residencesattending social clubs (chi-square, p< 0.001), bingo (chi-square, p <
0.01) and community centres (chi-square, p < 0.001). In all cases, asignificantly greater proportion ofmedium support residents attendedthese activities.
The key workers were asked to rate theresidents’ motivation in relation toparticipation in activities taking place inthe residences. They reported that 33% ofthe residents were motivated and activelyengaged in activities, 21% wanted toparticipate but did not have strongmotivation to do so and 33% of residentswere reported as passively engaging inactivities. The key workers reported that8% of the residents had littleunderstanding of activities and 4% refusedto participate.
Only 12% (n = 16) of the residentsreported having experienced harassment inthe community. Of these, eight hadexperienced name calling. Four hadexperienced a random attack in thecommunity (e.g. bag snatched). Oneparticipant had experienced sexualharassment and three reported havingexperienced harassment in psychiatrichospitals they had attended.
6.1.3 Money management
Nursing officers reported that inonly 8% of the high supportresidences were residents unable tolook after their own monies. In 92%of the high support residences itwas reported by nursing officersthat some (81%) or all (11%)
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND80
High Medium Low Total(n = 82) (n = 25) (n = 31) (n = 138)
Social clubs 4 (4.9) 8 (32.0) 5 (16.1) 17 (12.3)
Bingo 9 (11.0) 6 (24.0) 0 15 (10.9)
Community centres 8 (9.8) 11 (44.0) 2 (6.5) 21 (15.2)
Pubs, clubs, restaurants 37 (45.1) 13 (52.0) 17 (54.8) 67 (48.6)
Leisure centre 5 (6.1) 3 (12.0) 2 (6.5) 10 (7.2)
Library 4 (4.9) 4 (16.0) 3 (9.7) 11 (8.0)
Cinema 24 (29.3) 6 (24.0) 5 (16.1) 53 (25.4)
Religious activities 25 (30.5) 11 (44.0) 7 (22.6) 43 (31.2)
Table 6.2 Number (%) of residents attending activities in the community , by level of support

residents were able to look aftertheir own monies, while all themedium and low support residencesreported that some (medium 68%,low 41%) or all (medium 32%, low58%) residents could do so.
6.2 INFORMATION PROVIDED TORESIDENTS
Questions were asked in the facilityquestionnaires about the informationprovided to the residents on rights andcomplaints procedures, the role andfunctions of the Mental HealthCommission, voting registration and healthinitiatives. The questionnaire did notaddress how the information was providedto the residents, however, enquiry wasmade as to whether notices regardinginformation on rights and on thecomplaints procedures were displayed onthe walls of the residences. The dataconcerning the information provided toresidents derived from all communityresidences in the three HSE local areas(n=102) and were provided by the nursingofficer in charge of the residences. Thenursing officers in the communityresidences were asked a series of questionsrelating to the information that was
provided to the residents. The specificquestions that were asked are presented inTable 6.3, Table 6.4 and Table 6.5. Thetables present the number and theproportion of high, medium and lowresidences that were reported as providingresidents with this information. Forcompletness, the proportion of missingresponses (i.e. number of residences that aresponse was not provided for) is alsonoted in the table. The analyses below,however, were performed on thecompleted data and missing categorieswere excluded.
6.2.1 Information on complaintsprocedures and rights
Table 6.3 presents the proportion ofhigh, medium and low supportresidences reporting thatinformation on complaintsprocedures and rights were providedto residents. In 88% of theresidences it was reported thatresidents were provided withinformation on rights. The nursingofficers were asked if the residentswere provided with information onthe complaints procedures (i.e. theprocess of making a complaintwithin the mental health services)
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 81
Information provided High Medium Low(n = 36) (n = 25) (n = 41)
Are residents given information on rights? Yes 35 (97.2) 21 (84.0) 34 (82.9)No 1 (2.8) 3 (12.0) 6 (14.6)
Missing 0 1 (4.0) 1 (2.5)Total 36 (100) 25 (100) 41 (100)
Are residents informed about the complaints procedure? Yes 33 (91.7) 15 (60.0) 29 (70.7)No 3 (8.3) 9 (36.0) 11 (26.8)
Missing 0 1 (4.0) 1 (2.4)Total 36 (100) 25 (100) 41 (100)
Are residents told the name of the local complaints officer? Yes 27 (75.0) 15 (60.0) 15 (36.6)No 8 (22.2) 9 (36.0) 25 (61.0)
Missing 1 (2.8) 1 (4.0) 1 (2.4)Total 36 (100) 25 (100) 41 (100)
Are notices regarding rights and complaints procedures displayed on the walls of the residence? Yes 19 (52.8) 10 (40.0) 14 (34.1)
No 17 (47.2) 12 (48.0) 26 (63.4)Missing 0 3 (12.0) 1 (2.4)
Total 36 (100) 25 (100) 41 (100)
Table 6.3 Information provided to residents on complaints procedures and rights, by level ofsupport

and if they were informed of thename of the local complaints officer.Again, in a large percentage (75%)of the residences it was reportedthat the residents were providedwith information on the complaintsprocedure. It was reported in asignificantly greater proportion ofhigh support residences that theresidents received information oncomplaint procedures (92%) than inthe medium (60%) and low (71%)support residences (chi-square, p <0.05). In contrast, the nursingofficers reported that the residentswere informed of the name of thelocal complaints officer in only 54%of the residences. Again, it wasreported in a significantly greaterproportion of the high supportresidences (75%) that residents wereinformed of the name of thecomplaints officer than in medium(60%) or low (37%) supportresidences (chi-square, p < 0.01).
Nursing officers were asked whethernotices providing residents withinformation on the complaintsprocedures and rights were
displayed on the walls of theresidences. It was reported that thisinformation was displayed on thewalls in only 42% of residences.There was no significant differencebetween the proportions of high,medium or low support facilitiesreported as displaying thisinformation (Chi-square, p > 0.05).In approximately half of thoseresidences where it was reportedthat information on rights wasprovided to the residents, thatinformation was displayed on thewalls of the residences. Of thosewhere it was reported thatinformation on the complaintsprocedures was provided, 54% ofthe nursing officers reported thatthe information was on display inthe residence.
6.2.2 Information on the MentalHealth Commission
It was reported in only half of theresidences in the three study areasthat residents were provided withinformation on the roles andfunctions of the MHC by the staff inthe residences. Table 6.4 shows the
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND82
Information Provided High Medium Low(n = 36) (n = 25) (n = 41)
Are residents informed of the Mental Health Commission (role and functions)? Yes 25 (69.4) 12 (48.0) 14 (34.1)
No 11 (30.6) 12 (48.0) 25 (61.0)Missing 0 1 (4.0) 2 (4.9)
Table 6.4 Information provided on the role and functions of the Mental Health Commission, bylevel of support
Information Provided High Medium Low(n = 36) (n = 25) (n = 41)
Are residents asked if they wish to vote and are they assisted in voter registration? Yes 36 (100) 25 (100) 41 (100)
No 0 0 0Missing 0 0 0
Total 36 (100) 25 (100) 41 (100)
Are residents informed of national health initiatives (e.g., breast screening) or other health information? Yes 33 (91.7) 22 (88.0) 37 (90.2)
No 3 (8.3) 2 (8.0) 4 (9.8)Missing 0 1 (4.0) 0
Total 36 (100) 25 (100) 41 (100)
Table 6.5 Information provided to residents on voting registration and health initiatives, bylevel of support

proportion of high, medium andlow support residences whereresidents were provided with thisinformation. A total of 69% ofnursing officers in the high supportresidences reported that theyinformed the residents about theMHC, a significantly greaterproportion than that in the medium(48%) or low (34%) supportresidences (c2 (4) = 8.64, p < 0.01).
6.2.3 Information on votingregistration and healthinitiatives
Table 6.5 shows the proportion ofthe residences where it was reportedby nursing officers that residentswere provided with information onvoting registration and thatassistance was provided to residentsin exercising their voting rights. Thisis in line with findings in 6.1.2 that78% of residents reported that theyexercised their voting right.
A total of 90% of the residencesreported that residents wereprovided with information onnational health initiatives or otherhealth information. The type ofhealth information given, thenumber of residences providing itand the mode of delivery arepresented in Table 6.6.
In 35% of the residences it wasreported that residents were
provided with talks and literature onphysical and mental health andwellbeing while 13% reported thatthey specifically providedinformation on smoking cessation,diet and cancer awareness. Only twonursing officers reported that theyspecifically provided information onBreast Check. The nursing officers in14% of the residences reported thatthey provided general healthinformation in the form of leafletsand talks that were posted on noticeboards or delivered within theresidences or day centres. In oneHSE area (Area B) the residents weregiven a ‘Solutions to Wellness’programme. This was a structuredprogramme that focused on healthyeating and physical exercise.
6.3 SUMMARY
Key workers reported that a quarter of theresidents had no family / friends to providesupport. The majority of residents’ keyworkers stated that they received visitsfrom relatives and friends and also wentout to visit relatives or friends. Regardingthe residents’ self-reports of social supportnetworks, between 18% and 25%reported that they could not / would notseek support from anyone during times ofneed. This included everyday psychologicalsupport, everyday instrumental support,psychological crisis support or instrumental
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 83
Type of information Number of residences that provided information
Breast check, smoking cessation 2
Information section on notice board and talks in day centre on a number of health initiatives 1
General health information leaflets from health centers and general practice 7
General health information presented notice boards and in group sessions in the residences 6
Smoking cessation, diet, cancer awareness and educational groups 13
Solutions to wellness programme 6
Talks and literature provided on physical health and mental health 36
Table 6.6 Number of residences (n = 102) providing health information and type ofinformation

crisis support. The residents stated thatthey most often did everyday things withother residents or family and friends fromoutside the residence. In comparison,support from nurses and care staff wasmost often sought in times of crisis ordecision-making.
The nursing officers reported that in only8% of the high support residences werenone of the residents able to look aftertheir own money, while it was reportedthat some or all the residents in mediumand low support were able to managetheir own finances. The majority ofresidents interviewed indicated that theywere aware of how much money theyreceived on a weekly basis, but halfreceived support from the staff to managetheir finances.
Most of the residents stated that theywent out on their own, that they visitedthe GP on their own and that they voted.There were no differences in theproportions of high, medium or lowsupport residents that voted, visited the GPby themselves, or went out on their own.Only a small number of residents reportedthat they attended activities in thecommunity and a greater proportion ofthe medium and low support residentsstated that they did so than the highsupport residents. The greatest proportionof residents reported that they went topubs, clubs and restaurants, as opposed toother community activities such as bingo,cinema, social clubs and communitycentres. Over 10% of the residents hadexperienced harassment in the communityand, in the majority of cases, this hadbeen in the form of name calling.
It was reported by the majority of nursingofficers in the residences that residentswere provided with information oncomplaints procedures and rights.However, in just over half of the residenceswas it stated that residents were providedwith the name of the local complaintsofficer and in less than half that theresidence displayed notices about rightsand complaints procedures. It wasreported in a greater proportion of highsupport residences that residents wereprovided with information on rights and
complaints procedures. Almost all nursingofficers in high support residences statedthat they provided such information andthree-quarters reported that residents wereprovided with the name of the localcomplaints officer.
In few of the residences was it reportedthat residents were informed about therole and functions of the MHC, althoughthis was more likely to occur in highsupport residences. This information isespecially important for residents whohave been or may be involuntarilyadmitted to psychiatric units or hospitals.This information may be more relevant forthis population than for those in mediumor low support.
It was indicated in all residences that theresidents were provided with support invoting registration. This is congruent withthe results from the residents themselves –with nearly 80% reporting that theyexercised their voting rights.
Approximately 90% of the nursing officersindicated that information on healthinitiatives was provided to residents.However few nursing officers reportedwhat these specific health initiatives werewhen asked to identify what informationwas provided to residents. The majority ofthe nursing officers who reported the typeof information provided indicated that thisconcerned general physical and mentalhealth. Smoking cessation, diet and cancerawareness was also provided.
In summary while some information wasprovided to residents, information onrights and complaints procedures were notmade available in all residences nor, moregenerally, was information on nationalhealth initiatives such as cancer screeningand prevention and healthy living and dietprovided. As reported in Section 4.4.4.5,few residences provided information packsto residents.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND84

CHAPTER 7Getting Better: Rehabilitationthrough Care and Treatment

This chapter is concerned with the measurestaken to reduce the impairments and disabilitiesof residents by reducing or modifying their levelof symptoms and by improving their socialfunctioning.
7.1 SPECIALISED REHABILITATIONTEAMS
Two of the three HSE local areas surveyedhad specialised rehabilitation teams.Within these two areas there were 29 (9high support, 13 medium support, 7 lowsupport) community residences reportedfor the study. All the specialisedrehabilitation teams had a consultantpsychiatrist, a mental health nurse andsocial worker. More than two-thirds of the29 community residences serviced by thespecialised rehabilitation teams had anoccupational therapist (69%; 20 / 29) andpsychologist (65%; 19 / 29) on themultidisciplinary team.
7.2 CARE PRACTICES
Only a small number of residents inmedium (8%) and low (29%) supportresidences were provided with aprovisional diagnosis on admission,compared with 58% of high supportresidents. This is somewhat surprising,given that the majority of the residentswould have been well known to theservices, but may have resulted from amisunderstanding of the study question(i.e. Is there a provisional admittingdiagnosis drawn up once the patient hasbeen admitted?).
7.2.1 Care plans and key workers
Nearly all nursing officers in highsupport residences reported havingcare plans for residents (97%) as didthe medium support residences(92%). The nursing officers in 68%of the low support residencesreported having resident care plans.Of those reporting the use of careplans, the majority (96%) reportedthat the care plans containedinformation on medical treatment.The nursing officers reported that
only 55% of the residences had careplans that outlined theresponsibilities of the teammembers. They reported that 86%of the residences had care plans thatcontained documentation indicatingdiagnosis and 92% had care plansthat outlined treatment andrehabilitation activities for theresidents.
It was reported that the majority(66%) of the residences had a keyworker system in place. A total of72% of the high support, 84% ofthe medium support and 49% ofthe low support residences had akey worker system in place.
7.2.2 Medication
Not surprisingly, a total of 98% (n =135) of the sample of residents wereon prescribed medication at thetime of the study. Two residentswere on no medication and theinformation was missing for oneresident. Table 7.1 shows thenumber of residents on medicationat the time of the study, by level ofsupport. Totals in the table refer tomultiple responses (i.e. an individualcould be in more than one category)and therefore, totals for high,medium and low support do notmatch sample totals. The totalspresented in the table are the rowpercentages. Of the residents onmedication at the time of the study(n = 135), the majority of residents(85%) were on Clozapine or otheratypical antipsychotic medication. Atotal of 49% of residents were ontypical antipsychotic drugs. Keyworkers reported that 16 residentswere prescribed atypical and typicalantipsychotic drugs simultaneouslyat the time of the study. A total ofeight residents were prescribed bothClozapine and another atypicalantipsychotic drug at the time of thestudy. There was no overlapbetween Clozapine and typicalantipsychotic drugs (i.e. no residentwas prescribed Clozapine and atypical antipsychotic drug).
Chapter 7
Getting better: rehabilitation through care and treatment
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND86

A total of 86% (71 / 82) of high supportresidents were prescribed atypicalantipsychotic drugs, while 60% (49 / 82)were prescribed typical antipsychoticdrugs. Of the medium support residents,64% (16 / 25) were prescribedantipsychotic drugs, with 36% (9 / 25) ontypical antipsychotic drugs. Thecorresponding proportions for low supportresidents were 90% (28 / 31) for atypicalantipsychotic drugs and 26% (8 / 31) fortypical antipsychotic drugs. In addition, atotal of 26% (21 / 82) of high support,36% (9 / 25) of medium support and 19%(6 / 31) of low support residents were onantidepressants at the time of the study.There was a greater proportion of mediumsupport residents (36%; 4 / 25) on bipolardisorder drugs than high (26%; 27 / 82) orlow (19%; 4 / 31) support residents. Thispattern was the same for anti-Parkinsoniandrugs (medium 40%; high 33%; low16%). Finally, the proportion of highsupport residents on hypnotics (26%; 21 /82) was similar to the proportion ofmedium support residents (24%; 6 / 25);while a lower proportion of low supportresidents were on hypnotics (13%; 4 / 31).
7.3 ATTENDANCE AT DAY CENTRES /DAY HOSPITALS
This section refers to the total number ofresidents (n = 871) in the three areas
across all 102 facilities. It was reported bynursing officers that 40% (349 / 871) ofresidents attended a day centre or dayhospital. Of these, 30% (168 / 554) werehigh support residents, 57% (88 / 153)were medium support residents and 57%(93 / 164) were low support residents.Table 7.2 shows the number of residencesreporting the proportion of residents thatwere attending day centres or dayhospitals. Analysis revealed that only 17%of the high support residences had 81% to100% of residents attending dayresidences, compared to 24% of themedium support residences and nearly half(46%) of the low support residences. Aquarter of the high support residences hadno residents attending day centres or dayhospitals, compared to 8% of the mediumand 22% of the low support residences.
7.4 REHABILITATIVE TRAINING ANDACTIVITIES TO PROMOTEWELLBEING
Table 7.3 shows the activities provided forresidents. In nearly all cases, a greaterproportion of the high support residencesthan the lower support residencesprovided activities for the residents.However, less than half of the highsupport residences provided vocationaltraining (44%) compared to 60% of themedium support and 39% of the low
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 87
Medication High Medium Low Total
Clozapine and other atypical antipsychotic drug 71 (61.7) 16 (13.9) 28 (24.3) 115 (100)
Typical antipsychotic drug 49 (74.2) 9 (13.6) 8 (12.1) 66 (100)
Antidepressant 21 (58.3) 9 (25.0) 6 (16.7) 36 (100)
Bipolar disorder drug 27 (77.1) 4 (11.4) 4 (11.4) 35 (100)
Other psychotropic drug 18 (81.8) 0 4 (18.2) 22 (100)
Anti-Parksonian drug 27 (64.3) 10 (23.8) 5 (11.9) 42 (100)
Hypnotic 21 (67.7) 6 (19.4) 4 (12.9) 31 (100)
Total 234 (67.5%) 54 (15.5%) 59 (17.0%) 347 (100%)
Table 7.1 Number (%) of residents on medication, by category, by level of support

support residences. Very few of theresidences provided cognitive behaviouraltherapy (high support 22%, mediumsupport 16% and low support 12%). Themajority of high, medium and low supportprovided practical living skills, social skillstraining and budget training. Nearly all thehigh support (94%) and a smallerproportion of medium (68%) and low(61%) support residences provided leisureactivities. It was reported by the nursingofficers that fewer than one-third of theresidences provided family educationprogrammes (31%). Of the high supportresidences, 44% provided suchprogrammes, while only 28% of themedium and 22% of low supportresidences did so.
7.5 COMMUNITY INTEGRATION
Table 7.4 shows activities that wereprovided to aid community integrationand the proportion of residences providingthese activities. A large proportion of theresidences provided activities to promotecommunity integration (67%). A total of52% of the residences provided activitiesthat involved members of the localcommunity and 63% participated in eventsorganised by community groups with agreater proportion of high supportfacilities providing these activities. It wasreported in less than half of the highsupport residences that activities toencourage work (39%) or collaborationwith others to find employment for
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND88
% of residents attending High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
None 9 (25.0) 2 (8.0) 9 (22.0) 20 (19.6)
1% – 20% 10 (27.8) 1 (4.0) 1 (2.4) 12 (11.8)
21% – 40% 7 (19.4) 6 (24.0) 6 (14.6) 19 (18.6)
41% – 60% 2 (5.6) 6 (24.0) 2 (4.9) 10 (9.8)
61% – 80% 2 (5.6) 4 (16.0) 4 (9.8) 10 (9.8)
81% – 100% 6 (16.7) 6 (24.0) 19 (46.3) 31 (30.4)
Table 7.2 Number (%) of residences showing the proportion of residents attending either daycentres or day hospitals, by level of support
High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
Vocational training 16 (44.4) 15 (60.0) 16 (39.0) 47 (46.1)
Cognitive behavioural therapy 8 (22.2) 4 (16.0) 5 (12.2) 17 (16.7)
Practical living skills 34 (94.4) 19 (76.0) 34 (82.9) 87 (85.3)
Social skills training 32 (88.9) 18 (72.0) 29 (70.7) 79 (77.5)
Budget training 29 (80.6) 16 (64.0) 26 (63.4) 71 (69.6)
Physical activities 31 (86.1) 11 (44.0) 21 (51.2) 63 (61.8)
Addiction counselling 11 (30.6) 5 (20.0) 11 (26.8) 27 (26.5)
Family education 16 (44.4) 7 (28.0) 9 (22.0) 32 (31.4)
Leisure activities 34 (94.4) 17 (68.0) 25 (61.0) 76 (74.5)
Table 7.3 Number (%) of residences providing activities and training, by level of support

residents (43%) was provided. Just overhalf of the high support residencesencouraged rehousing (55%), with 40% ofthe medium support and 67% of the lowsupport residences doing so.
7.6 INDEPENDENT AND ORGANISEDHOLIDAYS
The nursing officers in the residences wereasked to indicate the number of residentsthat had been on independent ororganised holidays in the last two years.Independent holidays referred to holidaysthat were organised by the residentthemselves. Organised holidays referred toholidays organised by the staff of theresidences. Table 7.5 and Table 7.6 showthe proportion of residents who went on
independent or organised holidays in thelast two years.
A total of 19% (n = 168) of residentswere reported to have gone onindependent holidays in the last two years,while just less than half (44%; n = 385)went on organised holidays. A total of13% of high support residents went onindependent holidays, while less than onethird of medium support residents and27% of low support residents went onindependent holidays). Regardingorganised holidays, 41% of the highsupport residents, 46% of mediumsupport residents and 54% of the lowsupport residents opted to go on theseholidays in the last two years. A third ofthe residences (33%) reported that noneof the residents went on independentholidays over the last two years (Table 7.5),
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 89
High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
Activities to involve community members 23 (63.8) 10 (40.0) 20 (48.8) 53 (52.0)
Activities to promote community integration 27 (75.0) 16 (64.0) 25 (61.0) 68 (66.6)
Activities to encourage work 13 (36.1) 7 (29.2) 20 (51.3) 40 (39.2)
Events organised by community groups 25 (69.4) 15 (60.0) 24 (58.5) 64 (62.7)
Collaboration with others to find employment 13 (36.1) 10 (41.7) 21 (53.8) 44 (43.1)
Activities to facilitate rehousing 19 (52.7) 10 (40.0) 27 (67.5) 56 (54.9)
Table 7.4 Number (%) of residences providing activities to aid community integration, by levelof support
% of residents High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
None 10 (27.8) 9 (36.0) 15 (36.6) 34 (33.3)
1% –20% 17 (47.2) 2 (8.0) 4 (9.8) 23 (22.5)
21% – 40% 8 (22.2) 6 (24.0) 12 (29.3) 26 (25.5)
41% – 60% 1 (2.8) 4 (16.0) 5 (12.2) 10 (9.8)
61% – 80% 0 1 (4.0) 4 (9.8) 5 (4.9)
81% – 100% 0 3 (2.9) 1 (2.4) 4 (3.9)
Table 7.5 Number (%) of residences showing the proportion of residents going on independentholidays in the past two years, by level of support

while 21% reported that none of theresidents went on organised holidays(Table 7.6).
7.7 SUMMARY
Two of the HSE local areas had consultant-led specialist rehabilitation teams. Morehigh support (58%) than medium (8%)and low support residences (29%) wereprovided with provisional diagnoses ofresidents on their admission. The greatmajority of high and medium supportresidences reported having care plans forresidents, as compared to 68% of lowsupport residences. Ninety-eight per centof residents were on prescribed medicationat the time of the study. No less than 85%of residents were on Clozapine or otheratypical anti-psychotics and 49% of the135 residents on medication were ontypical anti-psychotics with 16 residentstaking both atypicals and typicalssimultaneously; however, no resident wastaking Clozapine and a typical anti-psychotic at the same time. The highestproportions of residents on anti-psychotics, atypical and typical, were thosein high support. Just over a quarter ofresidents were prescribed anti-depressants.In addition, a sizeable proportion ofresidents were taking medication forbipolar disorder, medication to counterside effects of anti-psychotics, hypnotics orother medications.
A greater proportion of high support thanof lower support residences provided
activities of a rehabilitative or trainingnature. Only 44% of high supportresidences, compared to 60% of mediumsupport residences, made vocationaltraining available and cognitivebehavioural therapy was provided in lessthan one-fifth of residences. However,training in practical living skills and socialtraining and instruction in budgeting wereundertaken in the majority of residences.Physical and leisure-time activities were therule in most residences. A range of otheractivities was undertaken in manyresidences.
Efforts to encourage communityintegration were in progress in over two-thirds of residences – more so in highsupport than in medium and low supportsettings. On the other hand less than halfof residences undertook initiatives to helpresidents find employment, whereasmatters were somewhat better in relationto having residents seek rehousing.
The results showed that a greaterproportion of residents in medium andlow support than in high supportresidences went on holidays, eitherindependently or organised by the services.A very small proportion of residents fromhigh support went on independentholidays while a greater proportion wenton supervised holidays. Overall, only asmall proportion of residents had been onholiday in the last two years, either ontheir own or with the staff from theresidences. .
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND90
% of residents High Medium Low Total(n = 36) (n = 25) (n = 41) (n = 102)
None 9 (25.0) 6 (24.0) 6 (14.6) 21 (20.6)
1% –20% 5 (13.9) 1 (4.0) 2 (4.9) 8 (7.8)
21% – 40% 4 (11.1) 4 (11.1) 8 (19.5) 16 (15.7)
41% – 60% 5 (13.9) 7 (28.0) 5 (12.2) 17 (16.7)
61% – 80% 3 (8.3) 2 (8.0) 9 (22.0) 14 (13.7)
81% – 100% 10 (27.8) 5 (20.0) 11 (26.8) 26 (25.5)
Table 7.6 Number (%) of residences showing the proportion of residents going on organisedholidays in the last two years, by level of support

CHAPTER 8Our View: Residents’Satisfaction with Care andTreatment and Other Aspectsof Life

All the information reported in this chapterconcerns the residents’ views of their lives in thecommunity residential facilities.
8.1 SATISFACTION WITH, ANDPREFERENCE FOR,ACCOMMODATION
The residents were asked if they wished tostay in their current accommodation and ifthey had a choice where they would preferto live. A total of 76% (n = 105) of theresidents were willing to stay in theircurrent accommodation. The residents inmedium support facilities appeared mostcontent with their accommodation, in that96% indicated a willingness to remain intheir community homes compared to only68% of the high support and 81% of thelow support residents. A large proportionof the residents (59%; n = 82) were happywhere they were (high support 52%;medium support 80%; low support 61%).Of those who, if given the choice, wouldlike to move (n = 56), the majority wouldprefer independent living (20%; n = 28) orto live at home (13%; n = 18). A total of40% of the high support residents wouldprefer independent living or would preferto live at home. By comparison, 16% ofthe medium support and 29% of the lowsupport residents would preferindependent living or living at home. Only7.2% residents reported that they wouldprefer to live in a group home or anotherhostel.
8.2 RESIDENTS’ SATISFACTION WITHTREATMENT AND CARE
Table 8.1 presents the questions thatresidents were asked regarding their careplans. Totals refer to the number ofresidents who responded to the questions.
Only 20% of the residents reported thatthey had knowledge of their care plans.For those who reported that they wereunsure or did not know, the researcherexplained the term care plan so that theremaining questions could be asked. Of allresidents, 21% reported that they wereinvolved in drawing up their care plan;24% reported that their care plan hadbeen explained to them prior to theinterview; 27% reported that they knewwhen their care plan would be reviewed.Nearly two-thirds of the residents (64%)reported that they knew what theirmedication was for, and 46% reportedthat they knew about the possible sideeffects of their medication.
Residents were also asked a number ofquestions regarding their satisfaction withtheir key worker (see Table 8.2). Just over aquarter (29%) of the residents reportedthat the term key worker had beenexplained to them. For those who reportedthat they were unsure or did not know,the researcher explained the term keyworker so that the remaining questionscould be asked. It appeared to theresearcher on a number of occasions thatthe residents in high support residenceswere answering the questions in relation
Chapter 8
Our view: residents’ satisfaction with care and treatment andother aspects of life
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND92
Yes Not sure No Total
I know what my care plan is. 27 (20) 17 (12) 92 (68) 136 (100)
I was involved in drawing up my care plan. 29 (21) 21 (15) 86 (63) 136 (100)
My care plan has been explained to me. 33 (24) 20 (15) 83 (61) 136 (100)
I know what my medication is for. 86 (64) 30 (22) 19 (14) 135 (100)
I know the possible side effects of my medication. 62 (46) 24 (17) 49 (36) 135 (100)
I know when my care plan is going to be reviewed. 37 (27) 41 (30) 58 (43) 136 (100)
Table 8.1 Residents’ responses to statements about their care plans (number and percentages)

to the nurse in charge of the residence, asthey appeared not to have a specific keyworker assigned to them. Less than half ofthe high support residents (43%) reportedthat they knew the name of their keyworker. The majority (67%) of the highsupport residents, however, stated that thenurses who worked in the residenceprovided them with practical help. Whileresidents may not have had or wereunaware of the identity of their keyworker, a large percentage reported thatthey were getting support from nurses.
Of the total sample of residents, just overhalf (53%) said they knew the name oftheir key worker and 56% reported thatthe key worker had explained to themtheir view of their problems. Nearly two-thirds (72%) felt that their key worker washelping them to cope and 74% indicatedthat their key worker was easy to contact,when necessary. Regarding help withproblems, again nearly two-thirds (72%)felt that the key worker helped them with
practical problems and 68% felt they couldeasily talk to their key worker aboutpersonal problems. Fifty-nine percent ofthe residents reported that the key workerkept the GP informed of their progress andalso made sure that they kept theirappointments with the psychiatrist. A largeproportion of the residents indicated thatthey could rely on the key worker to turnup at arranged times (65%) and 58%reported that the key worker would checkthat they were all right if they missed anappointment.
Regarding support from the psychiatrist,over half of the residents (63%) felt thatthey could easily talk to their psychiatristabout personal problems and 71% feltthat the psychiatrist was helping themwith their mental health problems. Onlyhalf (51%) of the residents reported thatthe psychiatrist explained their problems tothem. Likewise, just over half (57%) feltthat the psychiatrist kept them informed oftheir progress, with 43% reporting that
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 93
Yes Not sure No Total
The term key worker has been explained to me. 39 (29.3) 12 (9.0) 82 (61.6) 133 (100.0)
I know the name of my key worker. 70 (52.6) 17 (12.8) 46 (34.6) 133 (100.0)
My key worker has explained to me their view of my problems. 75 (56.4) 19 (14.3) 39 (29.3) 133 (100.0)
My key worker is helping me cope with my mental health problems. 96 (72.2) 17 (12.8) 20 (15.0) 133 (100.0)
If I have a problem I can easily contact my key worker. 99 (74.4) 16 (12.0) 18 (13.5) 133 (100.0)
My key worker helps me with practical problems. 96 (72.2) 16 (12.0) 21 (15.8) 133 (100.0)
I can easily talk about my personal problems with my key worker. 90 (67.7) 19 (14.3) 24 (18.0) 133 (100.0)
My key worker lets my GP know how I am getting on. 79 (59.4) 23 (17.3) 31 (23.3) 133 (100.0)
I can always rely on my key worker to show up at arranged times. 87 (65.4) 25 (18.8) 21 (15.8) 133 (100.0)
My key worker helps make sure I keep my appointment with the psychiatrist. 78 (58.6) 27 (20.3) 28 (21.0) 133 (100.0)
My key worker makes sure I am all right if I don’t turn up for an appointment. 77 (57.9) 30 (22.5) 26 (19.6) 133 (100.0)
Table 8.2 Residents’ responses to statements about treatment and care provided by keyworkers (numbers and percentages)

the psychiatrist explained how theirproblems affected their lives.
The majority of residents stated that theywere ‘quite happy’ or ‘very happy’ withthe treatment and care provided (85%).Only 12% reported that they were ‘notvery happy’ or ‘not at all happy’. A total of63% of the sample reported that they had‘enough information’ on their illness. Only10% reported that they had received ‘noinformation’ or ‘little information’ on theirillness. A total of 24% stated that theywould have liked more information ontheir mental health problems.
8.3 RESIDENTS’ SELF-REPORTEDQUALITY OF LIFE ANDPERCEPTIONS OF LIFE IN THERESIDENCE
Residents were asked to rate their qualityof life on 18 items. The items were scoredon a three-point scale from 0 – 2, withhigher scores indicating greatersatisfaction. The scores on the 18 itemswere summed to give a total quality of lifescore. Total scores could range from 0 to36. There was a significant differencebetween the levels of support on theQuality of Life Questionnaire (F (KruskalWallis Test, p < 0.01). Residents from highsupport residences reported significantlylower quality of life (30.0; range 0 – 41)than residents from medium (33.7; range21 – 36) or low (33.1; range 21 – 42)support residences.
Residents were asked to rate theirperceptions of life in the residence on 12items. The items were scored on a four-point scale from 0 – 3, with higher scoresindicating more positive perceptions. Therewere no significant differences betweenlevel of support on the twelve individualitems (p >0.05). The residents’perceptions of life in the residences weremostly positive. A total of 67% of theresidents reported that they thought it was‘good’ or ‘great’ to live in their currentaccommodation and a similar proportion(66%) felt that the atmosphere within theresidence was positive most or all of thetime. The majority of the residents
indicated that residents got on welltogether (75%) and felt that the staff goton well with residents (81%). Regardingactivities during the day, only 6% reportedthat they were bored during the weekdays‘all of the time’ or ‘most of the time’,while 8% felt bored ‘all of the time’ or‘most of the time’ at weekends. Just over athird (39%) of residents felt that they hada ‘moderate’ or ‘a lot’ of say in the day-to-day running of the household; however,almost two-thirds (72%) reported thatthey were ‘happy most of the time’ or‘very happy’ with their involvement in therunning of the residence. Likewise, overhalf the residents reported that they had‘no input’ or ‘little input’ with regard totheir treatment (55%). Only a smallproportion of residents felt that they had‘no control’ or ‘little’ control over howthey lead their lives (7.8%), with over two-thirds reporting ‘moderate’ to ‘a lot’ ofcontrol (76%). In addition, the majority ofresidents were ‘happy most of the time’ or‘very happy’ with their level ofindependence (75%) and were happy withtheir involvement in the community (76%).
8.4 QUALITATIVE ANALYSIS OFRESIDENTS’ COMMENTS
Of the 138 participants in the studysample, 90% (n = 124) providedresponses to open-ended questions. Theresidents were asked to tell the interviewer‘a bit about what it was like to live here intheir current accommodation’. Thefollowing prompts were used to guide theconversation:
What are the best bits about livinghere?
What are the worst bits?
What would you improve?
Where do you see yourself living in thefuture?
What are your hopes for the future?
The information provided by the residentswas analysed using SPSS for Text Analysis.A total of eight main categories were
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND94

extracted during data analysis. Thesecategories included accommodation, otherresidents, nurses and staff, psychiatristsand doctors, medication, finances, hopesfor the future and work. The categoriesincluded both negative and positiveresponses. The frequency of responses andexamples of the residents’ views takenfrom researchers’ notes are presentedbelow. Table 8.3 shows the frequencies ofthe positive and negative responses withinthese categories from high, medium andlow residents.
8.4.1 Accommodation
Responses in this category includedthe residents’ satisfaction withcurrent accommodation, preferencefor accommodation, room sharingand food. A total of 81 (65%) ofrespondents reported that they were
happy in their currentaccommodation, at least for thepresent.
Comfortable and good food.Nurse will go shopping with you
However, nearly a quarter of therespondents indicated that theywould like to move, either now oreventually, to independent living –an apartment of their own (23%)and 19 (15%) reported that theywould like to go back to their ownhome. Some residentsacknowledged the benefit of thecurrent accommodation and thesupports provided, but stated thatthey would like to move in thefuture. Other residents recognisedthe need for support even if theywere living independently. It isinteresting to note that only three
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 95
Level of supportMain themes High Medium Low Total
Accommodation Happy here 44 (54.3) 17 (21.0) 20 (24.7) 81 (100.0)Independent living 17 (58.6) 2 (6.9) 10 (34.5) 29 (100.0)Would like to go home 16 (84.2) 1 (5.3) 2 (10.5) 19 (100.0)Perceive residence as home 1 (33.3) 1 (33.3) 1 (33.3) 3 (100.0)Own room 10 (52.6) 3 (15.8) 6 (31.6) 19 (100.0)Sharing room 3 (75.0) 1 (25.0) 4 (100.0)
Food Food - positive 10 (71.4) 1 (7.1) 3 (21.4) 14 (100.0)Food - negative 6 (66.7) 2 (22.2) 1 (11.1) 9 (100.0)
Residents Residents - positive 7 (58.3) 3 (25.0) 2 (16.7) 12 (100.0)Residents - negative 9 (69.2) 2 (15.4) 2 (15.4) 13 (100.0)
Nursing and staff Nurses and staff - negative 7 (50.0) 1 (7.1) 6 (42.9) 14 (100.0)Nurses and staff - positive 15 (60.0) 4 (16.0) 6 (24.0) 25 (100.0)
Doctor Doctor - positive 1 (50.0) 1 (50.0) 2 (100.0)Doctor - negative 8 (80.0) 1 (10.0) 1 (10.0) 10 (100.0)
Medication Medication - negative 8 (53.3) 1 (6.7) 6 (40.0) 15 (100.0)Medication - positive 3 (75.0) 1 (25.0) 4 (100.0)
Finances Money - negative 10 (90.9) 1 (9.1) 11 (100.0)Money - positive 2 (66.7) 1 (33.3) 3 (100.0)
Employment Would like to work 9 (56.3) 3 (18.8) 4 (25.0) 16 (100.0)
Future Hopes for future – negative 11 (68.8) 2 (12.5) 3 (18.8) 16 (100.0)Hopes for future - positive 17 (58.6) 3 (10.3) 9 (31.0) 29 (100.0)Total 73 (58.9) 22 (17.7) 29 (23.4) 124 (100.0)
Table 8.3 Total number (%) of residents providing comments under the main themes, by levelof support (n = 124)

respondents referred to theresidence as home.
Would like to go home in thefuture with some support.
Group home is grand. Eventuallywould like my own place. Nameon waiting list, but about six yearwait.
So happy here – staff areexcellent. In the future would liketo go home and get part-timejob and eventually a council flat.
Only four (3%) residents reportedthat they liked sharing a room. Thecomments made by these residentssuggested that they liked having thecompany and had shared a room forso long that they would be lonely ifin a room by themselves. On theother hand, more residents raisedthe issue of single rooms (15%, n =15). For those who had their ownrooms, they stated that the privacyof single rooms was a great benefitwhen sharing accommodation.Likewise, residents who weresharing rooms, felt that singlerooms would offer more privacy.
Better than the streets butovercrowded, no privacy.
Good that I can have visitors.Have my own room.
Would like more privacy, but noman is an island, you have todepend on others.
Food in the residence was referredto by 18% of the respondents, with14 (61%) making positive commentsabout the food and 9 (39%) makingnegative comments. Positivecomments mainly referred to goodfood. The negative food commentsin general referred to the fact thatresidents did not have a choice inthe type of food they ate or in fact,when they ate it. In addition, thelack of kitchen facilities to cook yourown food was highlighted.
Food is good. Share a room –don’t mind.
Not good that you can’t makeyour own tea. Can’t choose whatto eat.
Food could be better.
8.4.2 Residents
This category referred to commentsmade regarding the other residentsin the residence. There were 25responses in this category. Of these,48% (12) were positive comments,while 52% (13) were negativecomments. The positive commentsreferred to the fact that residentsgot on well together as did residentsand nursing staff. However, it wasalso pointed out there were toomany people in some residences andthat it was difficult to live withpeople 24 hours per day when youdon’t get along with them.
Difficult to deal with otherpeople.
Happy to stay here, but do notlike one woman. Blames you foreverything.
Great friends with others.
Too many people here.
8.4.3 Nurses and staff
A total of 14 (11%) residents madenegative comments about the staff(nurses, care workers). Theseresidents most often commentedthat the nursing staff did not taketheir views into account regardingmedication, health and well-beingand their willingness to go home.
District nurse wouldn’t let me gohome. Can’t take it anymore –not being able to go home. I’mbetter now – no illness, shouldbe able to go home. Nurseswon’t let me.
Need to build a relationship withnurses. They are a bit bossy.
Notwithstanding this, a greaterproportion (20%, n = 25) of theresidents made positive commentsabout the staff referring to their
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND96

understanding and support theyprovided to the residents.
Staff are nice and look afterpeople well.
Staff are very good, nice andhelpful.
Supervisor is very good, arrangeseverything for you, they do yourchores.
Good supervisors and great tohave support.
8.4.4 Psychiatrists and doctors
Interestingly only two positivecomments were made about thedoctors while ten negativecomments were made. Thesegenerally made reference to the lackof consultations with the doctor andfrequent change in doctors.
“Would like to see the psychiatristmore often.”
“Psychiatrist change very often,cannot easily talk to them.”
“I see a psychiatrist every six weeks,which is not helpful.”
8.4.5 Medication
There were 19 comments regardingmedication. Of these, four positivecomments (21%) were made aboutthe effects of the medication while15 (79%) comments were maderegarding the negative effects ofmedication. These commentshighlighted that residents wanted tohave input into their medication,but were often not listened too.
“I would like more rehabilitation.Feel disoriented after ECT.”
“Asked the doctor to get medicationchanged and they said this wasthe best medication.”
“Get injections once a month and Idon’t need it. Would like to get ittwice a year.”
“Would like to know more aboutmedication and have it reduced.”
“The worst is that you cannot self-medicate.”
8.4.6 Finance
A total of 14 (11%) people raisedthe topic of finance and a largeproportion voiced thier concernsabout money (78%). Residents wereconcerned that they were notmanaging their own money andwere only given a certain amount tolive on each week. They felt that theallocated amount was not enoughand that they should be allowed tospend it as they want.
“Did not have enough money to buycigarettes. Had to quit smoking.”
“Should let me go to the pub. Whathappens to the rest of the moneyafter cigarettes? Why save whenyou are 74, only to leave itbehind. I want the 54 Euro that Ihave left. Don’t want to save it.”
“I am worried that someone willtake my money from the bank if Ihave too much.”
“Don’t know where my money is.”
“Out of 160 Euro I get just 40. I waspaying rent of 70 Euro and now Iam not. I am a bit traumatised bythat.”
8.4.7 Hopes for the future
There was a total of 45 commentsmade regarding hope for the future.Of these, 16 comments (35%)indicated that residents had nohopes for the future or didn’t thinkabout the future. A total of 29comments (64%) were maderegarding positive hopes for thefuture. These hopes generallyreferred to the residents gettingtheir own accommodation andentering the work force.
“In the future I would like a simplejob and more money for ahouse.”
“In the future I would like to go toanother place or flats in anotherplace.”
“I would like to leave here and getbetter. Doctor told me it will be 2
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 97

– 5 years before I get home.”
“My hopes are that I complete mycourse by Christmas and that Imanage my health to a level thatI don’t have to go to hospital.”
“Future – haven’t thought about it.”
“Happy living here. Not thinkingabout the future, take one day ata time.”
8.4.8 Work
A total of 16 comments (13%) weremade regarding work. The majorityof these were made in relation tohopes for getting work in thefuture.
“Future – would like to go to agroup home and after a whileget part-time work / communityscheme.”
“Hope to get another job and placeto live on my own.”
“Waiting on communityemployment scheme. Waiting forsix months.”
“Would like to get back to work.”
8.5 SUMMARY
The majority of the residents reported thatthey wanted to stay in their currentaccommodation. The analysis of responsesto the open ended questions qualifiesthese results to some extent. The residentsfelt that the current accommodation wascomfortable and positive comments weremade regarding the quality of the food. Asubstantial number of the residents,however, reported that, if they had achoice, they would prefer to be at homeor in accommodation of their own.
Generally, the residents reported that theywere satisfied with their treatment andcare. While few residents knew what theircare plan was, when it was explained, theyreported that they had one somewhere.The majority reported that they knew whattheir medication was for. The qualitative
results suggested that the residents had anegative view of the medication, and thiswas in terms of not having control overthe medication that they were taking. Anumber of residents reported that theyhad asked questions regarding changingthe medication with the medical staff, butthey felt that they were not listened to.Just over a quarter of the residentsreported that they had the term keyworker explained to them. When theresearcher explained the term key worker,over half of the residents reported thatthey knew the name of their key worker.Overall, the majority of residents weresatisfied with the treatment and careprovided by the key worker, or where therewas not a key worker, by the nurses orcare staff in the residences. The majority ofthe residents reported that the key workerhelped them with practical problems andthat they could easily talk to their keyworker about personal problems. Thiscorresponds to self-reports of the socialsupport network, where the majority ofresidents reported that they would askstaff for help with small favours and withcrises (Section 6.1.1). The majority ofresidents also reported that they could talkeasily to the psychiatrist and that he / shewas helping them to cope. However,comments from the residents suggestedthat the psychiatrists changed too oftenand that they did not attend thepsychiatrist as often as they would like.Generally the residents reported that theywere happy with the treatment and carethey received. A quarter of the residentsreported that they would like moreinformation on their problems; while themajority reported that they had enoughinformation.
Overall, the residents had high scores onthe quality of life questionnaire suggestingthat they were satisfied with most areas oftheir lives. The residents in the mediumand low support residences weresignificantly more satisfied than those inhigh support. The residents’ commentssuggested that they had hopes for thefuture, and these hopes were: to getbetter, get their own accommodation andimprove their occupational functioning.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND98

The residents’ perceptions of life in theresidences were mostly positive. This wasevident in the comments made by theresidents especially in terms ofrelationships between residents andbetween residents and staff. They alsoreported that the atmosphere in theresidence was generally good. Someresidents, however, made commentsregarding the lack of privacy and nothaving access to single rooms. Fewresidents reported that they were boredduring the weekdays, with slightly morereporting boredom during the weekends.The results showed that residents had littleinput to the running of the residences, butthe majority were happy with thissituation. The majority of the residentsreported that they could lead their life asthey wanted and that they were happywith their current level of independence. Itmust be noted that, while residentsreported being happy with their level ofindependence on the questionnaire, theircomments indicted that they hoped toimprove their current situation and thismost often included gaining greaterindependence from the services. Theresidents’ responses to the questionnaireswere qualified and elaborated on inresponse to the open-ended questions.This issue is further addressed in Chapter10.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 99

A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND100

CHAPTER 9Our Roles: Staff Views ofCommunity Residences

This chapter describes the staffing of communityresidences, staff perceptions of the role andfunction of residences and the factors thatpromoted or constrained independence andprogression to independent community living.
9.1 STAFFING LEVELS WITHIN THECOMMUNITY RESIDENCES
Nursing officers from participating highsupport residences reported the number ofstaff including nursing staff, care staff andhousehold staff working at three time-intervals throughout the day (morningshift 8am to 2pm, afternoon shift 2pm to8pm and night shift 8pm to 8am). Staffinglevels within this shift rota were reportedfor the majority of residences; however,some residences had slightly differentrotas. Some residences had staff employedon a part time basis, thus it was possiblefor residences to have 0.5 staff on a givenshift. As expected, the low supportresidences had no staff present on a full-time basis, but had regular visits fromnursing staff. The medium supportresidences had night-time supervision bynon-nursing staff. These residences had,on average, one care staff on the night
shift and few had staff during the morningor afternoon shift.
There was an average of 2.37 and 2.25nursing staff in the high supportresidences in the morning and afternoonshifts, respectively. There were slightlyfewer nurses on the night shift (mean1.72). The average number of care staffwas 0.25 for the morning and theafternoon shifts and the average numberof household staff for these shifts was1.15 and 1.05. The average number ofstaff in the high support residences wascalculated for a 24-hour period. During a24 hour period there was on average 6.34nurses, 0.50 care staff and 2.15 householdstaff. This resulted in an estimated totalaverage staff number of 8.99 staffworking in the high support residenceswithin a 24-hour period.
Table 9.1 shows the number of highsupport residences within each staffinglevel category at each shift. The majority ofthe high support residences had less thanthree nurses on duty during the morning(83%), afternoon (86%) and night shift(94%). Regarding household staff, thehigh support residences had approximately
Chapter 9
Our roles: staff views of community residences
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND102
Morning Afternoon Night
1 - 2.9 nurses 30 (83.3) 31 (86.1) 34 (94.4)
1 - 2.9 care staff 8 (22.2) 8 (22.2) 13 (36.1)
1 - 2.9 household staff 27 (75.0) 23 (63.8) 0
3 – 4.9 nurses 4 (11.1) 3 (8.3) 2 (5.5)
3 – 4.9 care staff 0 0 0
3 – 4.9 household staff 1 (2.7) 1 (2.7) 0
5 – 6.9 nurses 1 (2.7) 1 (2.7) 0
5 – 6.9 care staff 0 0 0
5 – 6.9 household staff 0 0 0
7 – 8.9 nurses 1 (2.7) 1 (2.7) 0
7 – 8.9 care staff 0 0 0
7 – 8.9 household staff 0 0 0
Table 9.1 Number (%) of high support residences within each staffing level, by shift

one household staff and one care staff forthe morning and afternoon shifts.
The nursing officers reported that a totalof 26% (n = 27) of the residences hadtrainees or volunteers on placement. Ofthe high support residences, 79% hadtrainees or volunteers within theresidences. A total of 7% of the mediumsupport and 15% of the low supportresidences had trainees / volunteers onplacement.
The majority of the medium and lowsupport residences had emergency staff oncall on weekdays (medium 88%; low61%). Few had emergency staff on call onSaturdays (medium 24%; low 36%), onSundays or public holidays (medium 24%;low 36%).
9.2 STAFF PERCEPTIONS OF THEAIMS AND FUNCTIONS OFCOMMUNITY RESIDENCES
Information is now presented on staffperceptions of the aims and functions ofcommunity residences. The staff on duty inthe residences where the sample ofresidents was interviewed were asked toparticipate . No staff member refused toparticipate. The majority of staffcompleted the questionnaire and returnedit to the researchers while they were onsite. The questionnaires provided staff witha list of eight functions of the communityresidences and staff members wererequired to rate these functions on level ofimportance (see Appendix 4 forquestionnaire). The questionnaire also
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 103
Occupation High Medium Low Total
Mental health nurse 29 (85.5) 3 (30.0) 7 (87.5) 39 (75.0)
Care worker 1 (2.9) 6 (60.0) 1 (12.5) 8 (15.4)
Care assistant 0 1 (10.0) 0 1 (1.9)
Domestic staff 2 (5.9) 0 0 2 (3.8)
Other 2 (5.9) 0 0 2 (3.8)
Total 34 (100) 10 (100) 8 (100) 52 (100)
Table 9.2 Number (%) of staff, by occupation, by level of support
Aims and functions No Moderate High Question importance importance importance unanswered
Service to shorten inpatient treatment 11 (21.2) 8 (15.4) 28 (53.8) 5 (9.6)
Alternative to inpatient care 12 (23.1) 9 (17.3) 27 (51.9) 4 (7.7)
Failure of outpatient care/ day care/ home care 13 (25.0) 12 (23.1) 21 (40.4) 6 (11.5)
Crisis intervention 15 (28.9) 10 (19.2) 23 (44.2) 4 (7.7)
Rehabilitation to independent living / lower support 2 (3.8) 1 (2.0) 47 (90.4) 2 (3.8)
Psychosocial rehabilitation and support 0 1 (2.0) 49 (94.2) 2 (3.8)
Home for life 6 (11.5) 6 (11.5) 40 (77.0) 0
Respite care 14 (26.9) 8 (15.4) 26 (50.0) 4 (7.7)
Table 9.3 Number (%) of staff rating the importance of the aims and functions

asked staff for their perception of thefactors that impeded or promoted theresidents’ return to independent living.
9.2.1 Profile of respondents
A total of 52 staff from the sampledresidences completedquestionnaires. Of these, 65%worked in high support residences,19% were in medium supportresidences and 15% were in lowsupport residences. Seventy-one percent of the staff were female. Table9.2 presents the professional statusof the staff, by level of support. Themajority of staff in the high supportresidences were mental healthnurses (85%) as were the majority ofthe low support staff (87%). Themajority of staff allocated to themedium support residences (70%)were care workers or care assistants,while 30% were mental healthnurses. While no mental healthnursing staff worked withinindividual medium or low supportresidences, there were nursingofficers in charge of theseresidences. Their role is to overseethe residences and monitor thehealth and wellbeing of theresidents.
Most of the staff surveyed were onpermanent contracts (88%) and infull-time employment (81%). Only15% of staff were employed on apart-time basis, with two membersof staff job sharing. The majority ofthe staff (58%) were mental healthprofessionals for 16 years or more,with 38% employed as mentalhealth professionals for 26 years ormore. Only 10% were employed forfive years or less, and 21% wereemployed for ten years or less at thetime of the study. The length of timein the current post was five years orless for 48% of the respondents,while 40% were in their current postbetween 6 and 16 years. A total of11% of respondents did not answerthe question. These resultssuggested that the majority of thestaff surveyed were highlyexperienced mental health nurses.
9.2.2 Perceived aims and functions ofcommunity residences
Staff of the residences surveyedwere asked to rate eight variables(scale of 1 - 3) relating to theimportance of the aims andfunctions of the residence. Table 9.3shows the eight possible functionsand the number and percentage of
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND104
Categories N = 126(%)
Support from staff team – well trained, encouraging, trust, respect, good environment/atmosphere 27 (21.4)
Independence/responsibility/making decisions/choice/participation 26 (20.6)
Community support and community involvement 21 (16.7)
Training/education/guidance/rehabilitation 18 (14.3)
Confidence, self-esteem 14 (11.1)
Support from family/friends 10 (7.9)
Compliance with medication/treatment programmes 6 (4.8)
Suitable employment 4 (3.2)
Total responses 126 (100.0)
Table 9.4 Number (%) of responses in each category of factors believed to promoteindependent living

staff reporting their perception ofthe importance of each function.
A large number of staff perceivedthe community residences as havinga function in the rehabilitation ofresidents so that they mightprogress to lower levels of supportor independent living (90%). AsTable 9.3 shows, the majority ofstaff perceived the residences asproviding a psychosocialrehabilitation function and asproviding support to residents. Overthree-quarters (77%) of staff alsoperceived the residences as beinghighly important in terms ofproviding a home for life (Table 9.3).A total of 54% of the staff perceivedthat the community residence wasof high importance in providing aservice to shorten inpatienttreatment, and 52% perceived it ascentral to providing an alternative toinpatient care. Fifty per cent of thestaff reported that communityresidences were important inproviding respite care. Forty per centof staff stressed the complementaryfunction of community residences asan adjunct to other elements ofservices (i.e. outpatient / day care /home care), while 44% of staffperceived the community residencesas important for the provision ofcare during crisis.
9.3 STAFF PERCEPTIONS OFFACTORS THAT PROMOTEDINDEPENDENT LIVING
Staff were asked to identify the three mostimportant factors that they felt promotedindependent behaviour. The researchercategorised responses into eight maincategories. Table 9.4 shows the eightcategories and the number of responses ineach category. The percentage of the totalresponses is provided in brackets. Thenumber of responses does not refer to thenumber of staff, as staff provided morethan one response to the questions. Table9.4 presents the categories in the order ofthe frequency of responses.
Staff frequently reported ‘support from thestaff’ (21%) as an important factor in thepromotion of independent living.Responses that fell into this categoryconcerned well-trained staff who wereencouraging, trustworthy, and respectfuland provided a good atmosphere orenvironment for residents. In addition,staff highlighted the importance of choice,privacy and an independent environmentfor residents:
supportive / dynamic multi-disciplinaryteam
team that allows for and knowsindividual differences
well trained staff who show interest inclient
open-minded staff, consistentapproach, committed and genuinelycare
environment that encourages choice,privacy, independent environment
A total of 21% of the staff responses wascategorised into the independence, choiceand participation category. The staffperceived participation in decision making,acceptance of responsibility for personalcare and having a level of independenceand choice as important factors inpromoting independent living.
give residents responsibility
taking control of personal activities –medication and household chores
taking charge of their own money
active participation in decision makingregarding their care plans
autonomy
making decisions for themselves
A total of 17% of responses from the staffaddressed the importance of communitysupport and involvement in the promotionof independent living. Staff felt thatresidents need more integration into thecommunity in the form of social activitiesand other community schemes such asworklink.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 105

community acceptance andinvolvement
going to pictures, days out and tryingto get back into community as best aspossible
support with other communitydisciplines and systems – worklink etc.
integration and involvement in thecommunity
A total of 14% of the responses of staffrecognised the importance of training,education, guidance and rehabilitation inpromoting independent living. Theseresponses referred mainly to rehabilitationprogrammes and included:
education in daily living skills
guidance
behavioural therapy interventions
occupational work or training
rehabilitation and relearning
individualised training programmes
rehabilitation process
Only 11% (n = 14) of staff responsesreferred to the importance of confidenceand self-esteem in promoting independentliving. For example, responses referred to‘confidence building’, ‘bolster self-esteem’and ‘high self-esteem’ as important factorsin promoting independent living. A totalof 8% of responses reported family andfriends support as the important factors topromote independent living. Compliancewith medication was mentioned in only5% (n = 6) of staff responses, whilesuitable employment was mentioned inonly 3% (n = 4) of responses.
9.4 FACTORS PERCEIVED TO HAVEIMPEDED INDEPENDENT LIVING
Staff responses to the factors thatimpeded independent living best fittedwithin ten categories. Table 9.5 showsthese response categories and the numberof responses in each category. Categoriesare ordered by frequency of responses.There were 103 responses regarding
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND106
Categories
Staff and health care team – lack of training, lack of encouragement, lack of interest, not multi-disciplinary 23 (22.3)
Lack of independence, responsibility, participation, decisions 16 (15.5)
Illness – severe symptoms, relapse, re-admissions, fear of relapse 11 (10.7)
Lack of support from community, family, friends 10 (9.7)
Routine – too much, monotony 6 (5.8)
Apathy, negativity of individual 9 (8.7)
Poor compliance with medication / treatment programmes 8 (7.8)
Institutionalisation 8 (7.8)
Lack of training, education and rehabilitation of patient 6 (5.8)
Inadequate personal finances 6 (5.8)
Total 103 (100.0)
* Note; more than one response was provided by staff to this question
Table 9.5 Number (%) of responses in each category of factors believed to impede independentliving*

factors that impede return to independentliving.
The most frequently reported response hadto do with staff and health care team. Atotal of 22% of responses were relevant tothis category. Responses referred to thelack of staff training, lack ofencouragement, lack of interest and non-multidisciplinary work practices as factorsimpeding independence.
“staff doing too much for clients”
“staff not interested”
“lack of training for staff, specifically forrehab purposes”
“lack of understanding and patience”
“lack of multidisciplinary intervention”
The second most frequent factor perceivedby staff as impeding return to integratedliving in the community was lack ofindependence of the resident. Thisincluded lack of responsibility, lack ofparticipation in treatment and care andnon-involvement in decision making. Someexamples of the responses in this categoryincluded:
“rigid thinking, restrictive, judgementalapproaches from staff”
“too much medication”
“no individual or personal responsibility”
“no participation in decision makingprocess regarding their care plans”
“not letting people do things forthemselves”
A total of 11% of the responses referredto the illness and the severity of the illnessas factors that impeded return toindependent living. These responsesreferred specifically to severe and recurringsymptoms. For example, recurringsymptoms, addiction and drug abuse werespecially mentioned.”
A total of 10% of the responses reportedthat the lack of support from thecommunity, families and friends hinderedthe residents’ return to independent living.
Nine per cent of the responses referred toapathy and lack of motivation of theresident as impeding return toindependent living. Other factors thatwere mentioned less frequently includedinstitutionalisation (8%), and poorcompliance with medication and treatmentprogrammes (8%), routine and monotony(6%), lack of training and rehabilitation(6%) and inadequate personal finances(6%).
9.5 SUMMARY
Of staff who responded to thequestionnaires, the majority were femaleand mental health nurses. They had beenemployed as mental health professionalsfor some time and most had permanentcontracts.
Regarding the aims and functions of theresidences, the staff perceived that theresidences had an important role to play inthe rehabilitation of the residents toindependent living or towards lower levelsof support. However, a large proportion ofthe staff felt that the residences also hadan important role in providing a ‘home forlife’ for the residents. The resultssuggested that staff viewed the residencesas having a dual purpose – rehabilitationand long term care. It was also interestingto note that half of the staff perceived theresidences as having a function in the careand treatment of the patients tocomplement other mental health servicecomponents such as inpatient, respite andcrisis care. It was clear that the staff didnot view the residences as filling just onefunction, but rather as filling a number ofimportant and diverse functions.
Factors most frequently perceived aspromoting independent living weresupport from the staff, independence andautonomy of the residents and communitysupport and involvement. It is clear thatthe staff felt that they had an importantrole in helping and supporting theresidents achieve independent living. Thisthey perceived was helped by giving theresident independence, choice,responsibility and encouragement to
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 107

participate in all areas of their lives.Likewise the most frequently reportedfactor considered by staff as impedingreturn to independent living was lack ofstaff training in rehabilitation, lack ofencouragement, lack of interest and non-multidisciplinary teams. In addition,dependency of the resident, be it eitherthrough their own choice or through theover provision of care and support fromthe staff, was perceived as an impedimentto returning to integrated living in thecommunity. Severity of illness and relapsewere also frequently considered by staff asfactors that impeded return toindependent living while inadequatepersonal finance was perceived only byapproximately 6% of staff as a factor thatprevented the return of the residents tointegrated living.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND108

CHAPTER 10Life in CommunityResidences: Conclusion andDiscussion

The present study was carried out in response tosignificant changes in mental health policy andthe lack of mental health services research incommunity residential care In Ireland. The studyaimed to review the provision, functions andpurposes of community residential services. Ofprimary importance were the residents’ views ofthe treatment and care provided by mentalhealth services and their perceptions of theirlives. The study set out to determine wherecommunity residential care was provided, whatcare was provided, to whom it was provided andsatisfaction levels of residents and the extent towhich the service was meeting residents’ needs.Finally, the study sought to determine whetherthose in community residential care wereappropriately placed and, if not, what alternativecare would best meet their needs.
To provide an overall picture of communityresidential care, Chapter 10 will amalgamate thefindings presented in the previous chapters anddiscuss these results in terms of the nature andquality of community residential accommodationand the extent to which it met the needs of theresidents. Based on the study findings, a series ofrecommendations is made in Chapter 11.
10.1 RESIDENCES AND THERESIDENTS
This study was primarily quantitative in itsemphasises, but included a series of open-ended questions which were analysed inorder to illustrate residents’ and staff viewsabout different aspects of care. Manypositive findings have come out of thequestionnaires as to how the residentsviewed their lives and the perceivedindependence and control they had inleading their lives as they wished. Thefindings have shown that, in general, themajority of the residents were satisfiedwith their current accommodation andtreatment and care. The perception of lifein the residences was positive and self-reports of quality of life rated it as high. Ingeneral, the residents felt that they hadcontrol over their lives and were happywith their level of independence. However,residents were also asked open-endedquestions regarding their lives and theircurrent accommodation. Their responsesqualified and elaborated on their views oftheir lives. For example, although residents
reported that they were happy in theircurrent accommodation, this may havebeen a result of their perceptions that theyhad no where else to go. Given the lack ofthe provision of more independentaccommodation to meet the needs ofthese residents, such perceptions wereaccurate. In addition, residents reportedthat, if things could be changed, theywould like more independence in terms ofbeing able to cook and eat when andwhat they liked and to spend their moneyas they pleased. While many residentsappeared to know what money theyreceived each week, many received help tomanage their finances. The researchernoted during site visits that most residentswere not concerned about handingcontrol of their finances to nursing staffand did not take responsibility for theirown finances, nor, in fact, did they feelthey had the skills to do so. However, anumber of residents did feel that theyshould have control of their own moneyand wanted to spend it as they saw fit.Many of the residents had previousinpatient admissions for long periods oftime and, in fact, many had beenrelocated from the large psychiatrichospitals. Many, therefore, had spent longperiods of time in a culture of dependencyand guardianship, as opposed to one ofindependence and control. It is possiblethat residents failed to see the possibilityfor change in a system that they hadbecome accustomed to for the best part oftheir lives. In addition, as the majority ofstaff had been in the system for longperiods of time, they also may have failedto see the system as one that emphasisedrecovery as opposed to maintenance.These results highlight the need fortraining and education for all incommunity residential facilities in thecompetencies and principles of recovery.These points will be reiterated andqualified throughout the discussion asappropriate.
Before addressing the occupancy of theresidences and the care and treatmentprovided it is necessary to highlight thecharacteristics of the residents in terms oftheir socio-demographic and clinical profileand the level of support that wasprovided.
Chapter 10
Life in community residences: conclusion and discussion
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND110

10.1.1Level of support provided incommunity residences
Residential accommodation forpeople with mental health problemsin Ireland is provided on three levelsof support – high, medium and lowsupport. An important point to noteis that these levels of support werenot uniformly defined throughoutthe study areas, nor are they, in fact,on a national level. High supportresidences throughout the countryare standardised in that all provide24-hour nursing. However,definitions of medium support andlow support vary. Medium supportin some areas included night-timesupervision, while in others nosupervision at night was provided.Low support was generallystandardised, with regular visitsfrom staff. However, in some areasstaff visited on a daily basis while inothers staff visited on a weeklybasis. Concern regarding thevariation in the definition of levels ofsupport in a national context wasexpressed on a number of occasionsby the management and staff of theresidences. For the purposes of thisresearch the following definitionswere used as these are the mostcommon definitions of the threelevels of support:
High support – 24-hour nursedcare
Medium support – night-timesupervision by non-nursing staff
Low support – regular visits bystaff
These definitions equate with thosein the UK (Lelliott et al., 1996;Donnelly et al., 1994) in that highsupport have 24-hour nursed careand low support are not staffed, buthave regular staff visits. However, inthe U.K., medium support facilitiesare staffed 24-hours, with staffsleeping at night-time.
10.1.2A profile of the sample ofresidents
The average age of the residents incommunity residences was 53 years,with the majority between the agesof 46 and 65 years. Few were underthe age of 35 years and almost one-third were over the age of 65 years.A slightly higher proportion of theresidents were male and bothgenders were equally represented inthe interviews. Most of the residentswere single and approximately halfhad attended secondary school,with only a quarter having post-secondary or third-level education.
Similarly to previous research inresidential care (Lelliott et al., 1996;de Girolamo et al., 2002; Donnellyet al., 1996) the majority of theresidents had a diagnosis ofschizophrenia and had a longduration of illness. The majority ofresidents had previous inpatienthospitalisations; however, there werefew admissions reported over theprevious five years. Thiscorresponded to the clinicalsymptoms reported for residentswho were interviewed, with themajority experiencing mildsymptoms. In addition, few residentsshowed moderate or severeimpairments in clinical functioningin the previous two weeks. It wouldappear that symptoms had beenrelatively stable for some time. Thecourse of illness for the majority ofresidents in the previous five yearswas persistent, but stable, and therewere no significant differencesbetween those in high, medium andlow support residences.
In terms of the general level ofoccupational and social functioning(GAF), the high support residentsgenerally had lower levels offunctioning; however, the clinicalsignificance of these differences isquestionable. The mean scores of allgroups were above 40 (scores lessthan 40 indicate a marked degree ofdisability (de Girolamo et al., 2004).
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 111

Difficulties were reported asmoderate for the high supportresidents, while mild difficulties werereported for the medium and lowsupport residents. On average, fewproblems with clinical and socialfunctioning were reported for theresidents in the two weeks prior tointerview, while, slightly more werereported as having experienced mildto moderate problems in activities ofdaily living and occupation (HoNOS).This is in line with previous researchthat indicated that those inresidential accommodation hadrelatively high skills level (Donnelly etal., 1996). Interestingly, Donnelly etal., (1996) found that highly staffedaccommodation could result in adeterioration of skills, specificallyself-care skills. This suggests thatover-providing for the residents mayactually be detrimental to theirmove towards independence. Thisnotion has also being highlighted byresidents themselves in that theyviewed lack of encouragement fromstaff to do things for themselves asan important factor that impededthe return to independence. Aninteresting finding was thatresidents rated themselves asfunctioning at a higher level thanthat rated by key workers, althoughthere was a significant positivecorrelation, albeit weak, betweenthe two ratings. Two possibleexplanations are presented as towhy this would occur. This findingcould be due to the over-estimationby the residents of their ownfunctioning or the under-estimationof the key workers of the residents’functioning. It has been shown thatstigma surrounding mental illnessmay also be present in mentalhealth care professionals (Hocking,2003). The key workers ratings maybe influenced by their lowexpectations of the residents arisingfrom the lack of training in recoveryand rehabilitation and previousexperience of working in a systemthat aspired to maintenance ofcurrent skills and abilities as
opposed to development andrecovery. This issue requires furtherresearch.
In contrast to the study by Lelliott etal., (1996) in the UK, the majority ofresidents in high, medium and lowsupport were not experiencingphysical health problems. In fact,few residents had severe physicalhealth disabilities with only a verysmall proportion having mild tomoderate problems most commonlyin the metabolic / endocrine systemand cardiovascular and digestivedisabilities. This most likely reflectsthe younger age profile of theresidents interviewed in this study,which is more comparable with thatof residents in the Italian study (deGirolamo et al., 2002) than those inthe UK study (Lelliott et al., 1996).
In summary, the residents in thissample showed a low rate of clinicalsymptoms and generally had goodphysical health. In addition, theirgeneral occupational and socialfunctioning was above the level thatindicates marked disability. Thisbrings into question the need forthe levels of care and supportprovided to these residents andwould argue that the needs of theresidents are over-provided for interms of the clinical and physicalneeds. However, as will be discussedfurther on, other needs are clearlynot being met, such as independentliving and rehabilitation, suggestingthat the current levels of serviceprovision are not appropriatelytargeted to meet the specific needsof some residents. This underminesthe principle of recovery wherebyindividuals are empowered to takecontrol of their lives.
10.2 COMMUNITY RESIDENTIALPLACES AND OCCUPANCY RATE
There were 102 residences reported forthe three HSE local areas, providing a totalof 951 residential places. This represented
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND112

a rate of 96 places per 100,000 totalpopulation in the areas studied.
10.2.1Rate of places
The majority of these places were in24-hour-staffed residences (584)with a smaller number in mediumsupport (166) and low support(201) residences. The Report of theInspector of Mental Health Services(MHC, 2005a) pointed out thatvariation existed within Ireland inthe rate of 24-hour-staffedresidential places per 100,000population with the highest atapproximately 190 per 100,000 andthe lowest at 8 places per 100,000.The average rate of places in highsupport residences in the three areasstudied was 76 per 100,000 adultpopulation, ranging from 85 placesper 100,000 in Area B, 77 placesper 100,000 in Area A and 36places per 100,000 in Area C. Thedevelopment of residential facilitieswas based on the existence ofpsychiatric hospitals anddeinstitutionalisation, as opposed toa population needs-based approach.It had been highlighted by theInspector of Mental Hospitals(Department of Health and Children,2004) that areas where largepsychiatric hospitals existed had thehighest number of 24-hour-staffedresidential places. There were largepsychiatric hospitals located in allareas studied, three of which hadbeen closed completely, one had 20patients remaining and threehospitals catered for approximately318 patients in total. The area thathad the lowest rate of residentialplaces was indeed the area wherethe psychiatric hospitals had not yetbeen closed (i.e. Area C) and cateredfor the greatest number of patients.While high rates of places may havebeen necessary during theprogramme of deinstitutionalisation,the continued need for so manyhigh support places is questionable.As the number of individualsrelocated from psychiatric hospitalsdecreased so too should the number
of high support places. There is aconcern that the availability ofplaces may lead to the admission ofthose who could be better providedfor in their own environment. Aneeds-based approach to planning isnecessary. This will ensure that thebest care is provided to service usersin their own environment and that asufficient number of high supportplaces is available for those in needof high levels of care.
The planning norm recommendedfor 24-hour-staffed residences in AVision for Change was 30 places per100,000 in large urban areas andfewer places in areas with lowdeprivation levels. It must be notedthat this figure was an estimate forthe number of high supportresidential places required for thefuture. In two of the participatingareas, the number of high supportresidences far exceeded this estimate(77 places per 100,000 and 85places per 100,000), while the areathat had not completely closed thelarge psychiatric hospitals had a rateof places similar to thatrecommended in A Vision forChange (36 places per 100,000). Inaddition, A Vision for Changerecommends that 120 intensive-carerehabilitation places should beprovided nationally and 80 places inhigh support intensive-careresidences. In addition, A Vision forChange recommended that 130places nationally should be providedas crisis places. Thus, with theinclusion of these residential places,two of the areas in the current studyhave close to the recommendedprovision of places necessary forvarious forms of high support, whileone area requires the provision ofmore high support places. It isnecessary to note that, while thenumber of places in high support isclose to the recommended number,the aims and functions of theseresidences may change.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 113

10.2.1.1 High support
On a national level a census in 2006indicated that there were 1,412persons resident in high supportresidences (Tedstone Doherty et al.,in press). The number of places inhigh support residences was 1,383in 2003 (Department of Health andChildren, 2004). If we take, asrecommended in A Vision forChange, 30 high support places per100,000 population with 10 placesin each unit, this results in a total of1170 places nationally. When afurther 120 intensive-carerehabilitation places, the 80 placesin high support intensive-careresidences and the 130 places incrisis residences are added thiscomes to 1500 community-basedhigh support places, which is similarto that now provided, even if thelatter three categories are not strictlycomparable in purpose with thebulk of non-specialised high supportcommunity-based accommodation.The inevitable conclusion is that, ifdemand quantitatively remains as itis, there will be little change in highsupport accommodation either inphysical provision or in staffinglevels, and, therefore, little savingfor the mental health servicesthrough reduced high supportprovision. Indeed, the reduction insize of the high support residencesto ten places, as advocated in AVision for Change, may require anincrease in staffing numerically.Whereas the clientele of the presenthigh support residences was largelydrawn from the psychiatric hospitalold long-stay population, whosecharacteristics are well known, thisaccommodation in the future will berequired for younger, new long-staypeople. These people will not belong-stay in the hospital sense, butlong-stay in the sense of havingnewly derived persistent illness,mainly psychotic, with housingneeds. There is an uncertainty aboutthe characteristics and needs of thisnewly accruing population, many ofwhom are likely to have co-morbid
substance abuse and may be lesslikely to settle easily into highsupport accommodation than theirelder peers who wereinstitutionalised for many yearsbefore being moved to communitysettings. This newer group is alreadybeginning to increase in numbersand information on their needs hasto be retrospectively andprospectively accumulated to guidefurther high support planning. So,while there may be enoughresidences in terms of quantity, theaims and functions and the qualityof these residences need to beaddressed.
It must also be borne in mind that ithas been recommended that thepublic psychiatric hospitals close assoon as possible (A Vision forChange; MHC 2006c). Thesehospitals cater for approximately774 long-stay patients, of whomover half are 65 years or over. Withthe closure of these hospitals,alternative community-basedresidential accommodation ofvarying levels of support for themore active and mobile of thesepatients, who constitute themajority, will be required. For thosewhose physical health iscompromised or who have severemobility or cognitive problems,nursing home placement will benecessary. A similar considerationalso applies to current residents incommunity residences with similardisabilities.
10.2.1.2 Medium and low support
It is the medium and, particularly,the low support places, of whichthere were approximately 1,827 in2003 (Department of Health andChildren, 2003) that pose particularconcern. It would seem from therecommendations of A Vision forChange that local authorities shouldprovide housing for this group, butthe practicalities and the reality ofimplementing this recommendationneeds to be addressed. For example,
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND114

and not especially encouragingindications of why this may fail tobe realised, are the facts already setout in Chapter 2 – the extent of thewaiting lists, the fact that theresidents are considered by housingauthorities to be housed, that theydo not in general constitute familyunits, that some are quite elderlyand that, even if the authorities didprovide housing, are suspect thatthe mental health services wouldnot provide the necessary care.Furthermore it is the low andmedium support residents whoshow the greatest potential forindependent living.
One possible solution is to inducelocal housing authorities to takepossession of low support residencesin so far as their administration andmaintenance requirements areconcerned. This would fulfil theircommitment as set out in the 2005Housing Policy Framework – BuildingSustainable Communities – to theextent that special needs would bemet for those with disabilitiesincluding psychiatric disabilities.There should be a commitment thatthis housing stock remainsexclusively for the use of personswith mental health problems. Thisentails a partnership approach withthe mental health services providingthe necessary level of care. As far asensuring that residents becometenants of the local authority in thetrue sense of that word, theprovisions of the 2004 ResidentialTenancy Act need to be fulfilled (i.e.security of tenure, periods of notice,registration). Side by side with thisare the innovative tenancy trainingschemes and the newly derivedinitiative by local authorities insetting up new tenancyarrangements with landlords in amutually sustainable partnershipsuch as is being promoted by theTenancy Sustainable Group.
As far as medium supportaccommodation is concerned,greater involvement of voluntary
agencies, such as has already beenachieved by Respond, HAIL, STEERand local mental health associations,should be encouraged, with greaterinvolvement in the procurement ofproperties and in the organisation,management and maintenance ofsuch settings jointly with residentsthemselves, and a retraction of thepsychiatric professional presenceother than in a care and clinicalsupport and rehabilitative capacity. Itshould be borne in mind that manylocal mental health associations areheavily representative of mentalhealth professionals.
The provision of housing and care isfurther addressed in Section 10.3,giving examples of alternativemodels of provision in the UK and inIreland.
10.2.2Occupancy rate
At the time of the study there were871 residents in the residences.Based on the number of residents inplaces, the occupancy rate was92%. However, this did not reflectthe 76 places designated for otheruses (i.e. respite and crisis care).Thus, inclusion of these placesresulted in an occupancy rate ofalmost full capacity (i.e. 99.6%).While only 8% of the places werereported by nursing officers asdesignated respite or crisis places,interviews with staff confirmed thata significant number perceived thatthe provision of respite care was animportant function of thecommunity residential facilities. Ashighlighted in A Vision for Change,the use of community residentialplaces for other purposes such asrespite or crisis care must bequestioned especially in terms of thesensitivities of the core residents ofthe facility. The use of places forthese purposes may impactnegatively on the care andtreatment of the residents bydisturbing their social environmentor by distracting staff from theirprimary function of providing
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 115

therapeutic activities for the coreresidents. A Vision for Changerecommended that additional placesbe provided for crisis care,recommending 130 placesnationally.
10.3 PROVISION OF RESIDENTIALACCOMMODATION AND CARE
The majority of the high supportresidences were large renovated houses inprivate grounds and were owned by theHSE. The majority of the medium and lowsupport residences were also owned bythe HSE and were semi-detached housessituated in housing estates. Sixteen of thelow support residences were leased fromprivate owners. These findings confirmedthat mental health services are the primaryproviders of accommodation for thosewith persistent mental health problemsand housing needs.
10.3.1Lack of alternativeaccommodation
As highlighted in Section 2.6.5.1,there was no policy in place thatspecifically addressed housing needsfor those with mental healthproblems. Residents were entitled togo on the local authority waitinglists and it was reported by nursingofficers that many were on theselists and had been for some time. Asmentioned above, social housingcontinues to be based on a pointssystem, resulting in those withchildren being giving priority forhousing. The high number of singlepersons in community residences,coupled with the under-provision ofsocial housing at a national level,has in the past resulted in fewhousing alternatives for people incommunity residences in mentalhealth services.
In line with previous findings, thedesire for alternative independentliving was reflected in the commentsmade by the residents (Shepherd,1998). While the majority ofresidents were happy in their current
accommodation, some commentedthat if given the choice they wouldlike to have their own home. Anumber said that they would liketheir own accommodation, but hadnowhere else to go. Residentsreported that they had been on thelocal authority housing waiting listfor some years (one residentreported a seven year waitingperiod) and felt that they had nohope of getting local authorityaccommodation in the near future.In addition, while residents reportedthat they would like their ownhome, many also expressed a needfor support. In a review of theliterature, Shepherd (1998) foundthat the majority of people wouldprefer their own homes, eventhough they acknowledged the needfor flexible support. The residents inthis study felt that independentaccommodation would result in theloss of needed support and,consequently, they were best placedin their current accommodation. Asignificant number of residents hadno alternative option that met theircurrent housing need and alsoprovided the necessary supports,both medical and psycho-social.Management in communityresidences reported that they felt theresponsibility for housing should bethe sole responsibility of the localhousing authorities and not mentalhealth services.
10.3.2Non-statutory agencies and theprovision of housing
Given the current shortage of socialhousing in Ireland, what alternativemodels of provision are available?Alternative models for housingprovision for those with mentalhealth difficulties have been outlinedin Section 2.6.5.2. One such modelimplemented in the UK, termedRegistered Social Landlords, providesresidential facilities. Previously, thesesocial landlords provided housingwith external agencies such asvoluntary agencies providingmanagement and care practices.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND116

More recently, there has been amove towards social landlordsproviding both management andcare services. However, a number ofproblems with this model have beenidentified. Firstly, training of staffresponsible for management andcare has been criticised, with themajority of staff poorly trained andthe self-reporting of unmet trainingneeds (Senn et al, 1997). Secondly,there has been a bias towards theselection of clients thought to bemore ‘easily’ treated (Shepherd &Murray, 2001). And thirdly, themonitoring of these facilities interms of quality of care and bestpractice has been criticised(Shepherd & Murray, 2001). A codeof standards in the provision ofhousing and support for peoplewith mental health problems, and aguide on how to achieve thesestandards, have been produced inthe UK (NHF/MHF, 1996; Warner etal., 1997). The first step towardsrealising this model of provision inIreland would be the establishmentof effective partnerships and closeinteragency co-operation, so that aplanned and informed approachcould be developed from the outset,ensuring quality and good practice.
10.3.3Local housing associations andvoluntary groups
Within Ireland, a small number oflocal housing associations have beenformed by voluntary agencies suchas STEER and HAIL with grant aidfrom the Department of theEnvironment, Heritage and LocalGovernment. An example of arecent project which aims to addressthe provision of affordable socialhousing for people with mentalhealth problems is the STEERHousing Association. This iscurrently being developed in one ofthe study areas and aims to providesecured tenancies with appropriatelevels of support for client groups.The project will provide one, twoand three bedroom dwellings tomeet the housing needs of a diverse
range of potential clients in bothurban and rural settings. ‘Recoveryguides’ will be available to providetenants with non-medicalinterventions to maintain andpromote positive mental health andfor the maintenance of the tenancy.The trained ‘recovery guides’ will bepast or present service users and willprovide low to medium levels ofsupport. Each housing scheme willhave a communal centre that will bestaffed both morning and night toprovide the required level of supportto tenants as and when it is needed.The centre will be used for socialevents and for the provision ofcourses and training on social andlife skills. This model of housing andcare provision is based on therecovery model of care (Anthony,1993) emphasising independence,dignity and support, followingconsultation with service users. Themodel values the concept of theindividual having their own homeand at the same time the necessarysupports to ensure self-confidenceand self-efficacy. This model ofprovision will be piloted in one ofthe HSE areas of the study. It isenvisaged that this housing will notentirely replace the current model ofhousing and care provision (i.e. HSEprovision of high, medium and lowsupport), but rather will be a part ofa range of options that clients canavail of to suit their needs. It isimperative that this model ofhousing and care provision isevaluated from the outset takinginto consideration the health servicemanagement, service users and careproviders perspectives. This willensure that quality and best practiceprevail and also the identification ofthose best suited to this type ofcare. This model should be assessedas a possible model of housing andcare provision to be provided on anational basis. Other models ofhousing provision by local housingassociations and voluntary groupsaround the country should also beevaluated as above.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 117

10.3.4The way forward
It is clear from the findings of thecurrent study that the provision ofhousing for those with persistentmental health problems has longbeen the responsibility of the mentalhealth services. This has been theresult of the lack of social housingprovision by local authorities,especially duringdeinstitutionalisation programmes.Many of the residents interviewedhad no alternative but to avail ofcommunity residential care. Yetmany voiced their desire and hopeto live in a less clinical communitysetting, based in ordinary housing.There is a need within Ireland toprovide a more comprehensiverange of residential facilities forthose with severe and persistentmental illness than that currentlyprovided. Such facilities are neededto provide for different levels offunctioning. It is envisaged that theywill include housing with high levelsof clinical support (e.g. 24-hournursed care) and more independentsettings with supports availablewhen needed and preferablyprovided by non-clinically trained‘recovery guides’. As suggested in AVision for Change, only a smallnumber of high support places willbe necessary in each local area. Themajority of people should besupported in ordinary housing. Theprovision of housing should not bethe responsibility of the mentalhealth services and, thus, there is anurgent need for mental healthservices to collaborate with localhousing authorities and voluntarybodies to identify needs andrequirements in local areas. Forthese partnerships to workeffectively, there needs to be mutualunderstanding and respect betweenthe agencies in relation to theirrespective roles and responsibilities.
10.4 THE ENVIRONMENTAL FEATURESAND CLIMATE AND CULTURE OFTHE RESIDENCES
The internal environment, managementstyle and climate and culture of thecommunity residential facilities can impacton the residents’ satisfaction (Rog, 2004).Of particular importance is respect for theindividual and the principle of informedchoice (Schizophrenia Ireland, 2006). A‘client orientated’ management style,involving high levels of positive staff-clientinteractions, is likely to contribute to theresidents’ wellbeing. An authoritarianregime which denies basic rights andprivacy is not conducive to the residents’wellbeing particularly when they aresubjected to unnecessary rules andregulations (Shephard & Murray, 2001).Quality of care indices in residentialfacilities have included quality of thephysical environment, individualisation ofcare, privacy, autonomy and theattractiveness of the neighbourhood(Shepherd, 2000; Schizophrenia Ireland,2006). Few residences in the current studyhad evaluation and review plans formonitoring the quality of servicesprovided.
10.4.1The aims and functions of theresidences
It was reported by management andclinical staff that, initially, thecommunity residences were viewedas ‘homes for life’ by both staff andresidents. However they felt that asthe deinstitutionalisationprogramme advanced and withinthe current climate of change in themental health services, the aims andfunctions of the residences werechanging to one of rehabilitationand recovery. There was concernvoiced as to the situation of thosewho have lived in communityresidences for long periods of time.It was felt that moving them,possibly away from familiar friendsand neighbourhoods, would causeunnecessary distress to this ageingpopulation. The concept of a ‘homefor life’ was also seen as animportant aim of the residences by
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND118

the staff working in them. Thesefindings reflected the dual role ofthe residences as one of long termcare for some and as a rehabilitationand as a stepping stone to moreindependent living for others. Thiswas evident also in the commentsby residents, with some hoping tocomplete the remainder of their livesin the residences while others hadhopes of moving to moreindependent living and getting aplace of their own. This begs thequestion – can these facilitiesperform this dual role effectively tomeet the needs of those concerned?Does the prolonged care of someresidents hinder the intensiverehabilitation required by others tomove to lower levels of support? Itis possible that having such a diversegroup of people with differentneeds in the same residence doesnot help to tailor the treatment andcare provided to individuals. Inaddition, the role of the nursing andcare staff is divided betweenproviding continuing care to someand intensive rehabilitation toothers. The lack of a co-ordinatingrehabilitation team further increasesthe difficulty, a point made in therecent report of the Inspector ofMental Health Services (MHC,2006c). There is a need to redefinethe aims and functions ofcommunity residential facilities.While there is a need for a nationaldefinition of the type of careprovided, within this definition, localneed should determine the use ofthe current residential facilities.
10.4.2Internal environment
The current study assessed theinternal environment of theresidences in terms of the staffinglevels, sleeping arrangements andnumber of bathrooms. On average,there were 15 residents in highsupport residences, six in mediumsupport residences and four in lowsupport residences. Within the highsupport residences there was onaverage a ratio of staff to residents
of one to seven for daytime and oneto nine at nighttime. In line withprevious research, this nursing levelwould seem particularly high,especially as residents psycho-socialfunctioning and psychopathologywas not problematic (Donnelly et al.,1997). The employment of highlyskilled nursing staff foradministrative or basic tasks may notbe the best way in which to deployvaluable resources. While it may benecessary to have two staff presentin the residences at any time in caseof emergency, one nursing staffmember and one care staff membermay be sufficient. In addition, withan average of 15 residents in highsupport residences, it is more likelyto resemble a large institution asopposed to a small residence thatcreates a more home-likeenvironment (MHC, 2006c). A Visionfor Change recommended thatresidences should cater for amaximum of 10 residents. Picardi etal., (2005) argued that the size andstaffing pattern and skill mix caninfluence the residents’ quality oflife. For example, similar to thisPicardi et al., (2005) found thatmany of the residential facilities inItaly did not have access to thoseprofessionals that would beexpected to have more skill inproviding psychosocialrehabilitation. Many of the nursingstaff in the residences in this studywere providing these rehabilitativeinterventions without the propertraining. This can cause stress bothfor the nursing staff and residents,which can impact negatively onmental health.
The size of the residence appearedto be related to the possibility ofhaving a single room. The smaller,medium and low support residenceshad a greater number of singlerooms than the high supportresidences. In most cases, residentsshared twin rooms. Wheneverpossible, residents were able tochoose who they shared with, butthis was often not possible. This
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 119

inability to provide residents with asingle room impacted on theirprivacy and was reflected incomments by the residents. Oneresident made reference to the fact,that while the community residencewas better than the streets, therewas no privacy. However someresidents also commented that theyliked having a room-mate. Thishighlighted the different needs ofresidents and the importance ofchoice. The importance of choice inmental health services was alsomade in a recent report of service–users’ views (Schizophrenia Ireland,2006). The lack of bathrooms andshowers was also highlighted in thecurrent study. The high ratio ofresidents to bathrooms isunacceptable and en-suitebathrooms should be available, as isnow the norm in many homes. Theprivacy of en-suite bathrooms iseven more imperative for peoplewho are unrelated and who shareaccommodation. The planning ofsmaller residences with single roomsand en-suites will improve theprivacy and comfort of the residents.
In this study 29% of the residencesdid not provide residents with accessto public phones makingcommunication with family andfriends difficult. It was reported thatresidents could use the office phone;however, this again was detrimentalto the privacy of the resident andincreased their dependency on staff.The ownership of mobile phoneswas not addressed in the study anda number of residents may haveowned a mobile phone.
Service managers, clinical directorsand directors of nursing pointed outthat residential accommodation wasmainly purchased on an ad-hocbasis during thedeinstitutionalisation programmeand renovated as necessary. Duringsite visits the researcher came acrossonly one specially designed highsupport residence. This explainedthe less than ideal situation of many
of the residences. Many of theresidences were not suitable forthose with mobility problems. Thiswas especially problematic for theageing population, with nearly athird of all residents being over theage of 65 years. This washighlighted on many of the sitevisits. Many of the bedrooms in theresidences were upstairs and manyof the residences, especially theolder ones, could not be fitted withlifts. During site visits, the researcherwas informed in one instance thatthe visiting room in one of theresidences was currently being usedas a bedroom for a resident whowas quite ill.
Very few of the residences hadevaluation and review plans thatmonitored the quality of services orthe satisfaction of the service usersor their families. A Vision forChange highlights the importance ofservice evaluation, especially in termsof quality of life measures and theimpact of services on service usersand their families. One method forevaluating quality has been the FACE(Functional Assessment of CareEnvironments) tool which has beenused in Northern Ireland as a formalquality evaluation procedure inmental health services (Mc Gillowayet al., 1999).
10.4.3External environment –accessibility
On average, the residences werelocated within walking distance ofshops, post office and GP surgery,with the distance to the day centreor day hospital somewhat greater.Enquiries about the possession ofprivate transport showed that veryfew residents owned a car, bike ormotorbike. This finding was similarto that found in the Italian study(Santone at al., 2005). Thepossession of some form oftransport is the norm for themajority of people and for theresidents it would greatly increasetheir autonomy and their ability to
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND120

meet some of their daily needsindependently. This may not beespecially problematic for thoseliving in urban areas, but for thosein rural areas with underdevelopedpublic transport services, access totransport is a necessity forautonomy and independence. Themajority of the high supportresidences had access to a minibusfor transportation, which was mainlyused for transporting residents today centres. Given that the majorityof residents did not have access totheir own transport,accommodation should be providedin urban areas, close to allamenities.
10.4.4Climate and culture of theresidences: a home-likeenvironment
The philosophy behind the policywas that residential facilities wouldprovide a more home-likeenvironment for residents than thatprovided in large institutions. Thisstudy found that the residences,even the medium and low supportresidences, were quite restrictive inwhat the residents were allowedand did not differ significantly in thisregard to the large institutions. Theinstitutional design and practice ofthe 24-hour nursed facilities wasalso raised in the Report of theInspector of Mental Health Services(MHC, 2006c). For example, thecomings and goings of the residentswere often monitored; residents didnot have their own door key andcould not lock their bedroom doors.In addition, residents did not haveaccess to the kitchen in high supportfacilities. Even residents in mediumand low support facilities often hadtheir food cooked elsewhere (e.g.day centre). While some residentssaid that they were happy with thissituation and made positivecomments about the food, othersfelt that they should have been ableto make their own food and have achoice in what they ate. This wasexemplified in a comment by one of
the residents that it was not goodthat you couldn’t make your owntea and choose what to eat. Healthand safety legislation, such asHACCP (see Section 3.3.6), preventsresidents from having access tokitchens and it is important that thisis revisited in relation to communityresidences, whereby independence isencouraged and supported. Asexpected the high supportresidences were most restrictive interms of rules and regulations andsome of these are in the bestinterest of the residents for safetyreasons. Nevertheless overprotectionof residents with unnecessary rulesand regulations is not in their bestinterest and encourages dependencyrather than decreasing it, a pointpreviously made by the Departmentof Health and Children (2003). Intimes of illness the need to restrictresidents’ activities for short periodsof time may be warranted andshould be discussed with theresident. However, the imposition ofrules and regulations on all residentsregardless of functioning or needs isnot beneficial. Donnelly et al.,(1996) pointed out that, even if adegree of risk is involved, staffshould find ways to encourageresidents to partake in activitiesoutside the residences that lead topersonal development. The provisionof smaller residences would allowfor more individualised plans so thatthe resident and key worker couldwork together to determine what isin the resident’s best interest.
There was close interaction betweenresidents and staff in the residences.Most of the residents were long-term users of mental health servicesand consequently were well knownto staff, with close personalrelationships developing over theyears. The residents made manypositive comments about thenursing staff, with very few makingnegative comments. The negativecomments referred mainly to the‘protective’ nature of the nurses’attitudes (i.e. not letting residents
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 121

do what they want). This lack ofchoice and the ability to determineone’s own treatment washighlighted in a report of the serviceusers’ views of mental healthservices (Schizophrenia Ireland,2006). The majority of the nursesworking in the residences wereexperienced mental health nurseswho had previously been employedin the large psychiatric institutionsand their psychiatric training wouldhave been mainly in custodial care.The comments from staff themselveshighlighted the importance of stafftraining and the impact it can haveon the return of the resident toindependent living. These findingssuggest that there is a need toprovide staff, both nursing and non-nursing staff, with the necessarytraining in recovery andrehabilitation. This should includenot only the necessary competenciesin recovery, but also the underlyingprinciples of recovery that impartsresidents the right to control theirlives. A Vision for Changerecommends that all staff workingin rehabilitation should be trained inthe competencies and principles ofrecovery.
10.4.5The main issues
A number of important pointsarising from the environment andthe climate and culture of theresidences need reiteration and willneed to be addressed in the future.Firstly, the residences wereperforming a dual function ofcontinuing care on one hand andrehabilitation on the other. Secondly,residences that are not situatedclose to an efficient public transportservice need to be located close tolocal amenities and services. Andfinally, the unnecessary rules andregulations of the residencesencouraged dependency, asopposed to independence, andthese need to be revised.
10.5 REHABILITATION AND RECOVERY
Those with severe and persistent mentalillness require a range of rehabilitativemeasures to address problems that arise asa direct and indirect result of their illness.These have been outlined in Section 2.3.As stated in previous reports (A Vision forChange, 2006; Mental Health Commission,2005b), the principle of recovery shouldunderpin rehabilitation.
10.5.1Participation in care andtreatment
The extent to which the care of anindividual is tailored to his or herneeds is usually achieved throughthe use of care plans. These careplans should be constructed, not onbehalf of the individual, but ratherby the individual and their keyworker and, if appropriate, a relative(Schizophrenia Ireland, 2003). Thecare plan should containinformation from a detailedassessment that includes clinical,physical and social functioning, userand carer aspirations, psychiatric riskassessment and management (RoyalCollege of Psychiatrists, 2003).Individual care plans should beregularly reviewed and amended toaddress the changing needs of theservice user. The present study foundthat the majority of nursing officersreported that care plans were usedby the residences and that a keyworker system was in place. It wasreported by the majority that thesecare plans contained information onmedical treatment and rehabilitationactivities of the residents. This wasin contrast to the findings fromthose residents who wereinterviewed, with the majorityreporting that they did not knowwhat a care plan was, were notinvolved in drawing up the care planand did not know or were not surewhen the care plan would bereviewed. This is an especiallyworrying finding that needs furtherinvestigation as to whether careplans are in fact in place and whythe residents cannot identify what
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND122

the care plan is and when it will bereviewed. This finding suggests thatcare plans, when in place, involvedvery little participation by theindividuals themselves andsuggested that individuals did nothave responsibility for their owntreatment and recovery. Staffidentified the lack of responsibilityand participation by the resident indecision-making as an impedimentto independent living. Previousresearch has highlighted the lack ofchoice in mental health treatment inIreland and furthermore, the lack ofsupport from mental healthprofessionals when service users’made decisions about theirtreatment (Schizophrenia Ireland,2006). This highlighted the lack of arecovery-oriented service. Given therecent policy document thatemphasises a move to a recovery-oriented service (A Vision forChange) it is critical that all residentshave a formal multidisciplinaryassessment, are involved in devisingtheir care plan and have access to adesignated key worker. It isimportant that residents are giventhe responsibility and ownership oftheir care plan and moreover,provided with the appropriatesupport to participate in decision-making regarding their treatment.
In the present study, over half of theresidents reported that they knewwhat their medication was for, andjust under half reported that theywere aware of the possible sideeffects. Likewise, just over half ofthe residents felt that thepsychiatrist explained their problemsto them and kept them informed oftheir progress. The comments madeby the residents suggested thatmany felt that the psychiatrist didnot listen to their concerns orproblems, and that the psychiatristwas always right. A number ofresidents reported that they did notsee the psychiatrist often enoughand that there was a frequentchange of psychiatrist, which theydid not feel gave them continuity of
care. Over a quarter of the residentsreported that they would have likedmore information on their problems.In order for residents to makeinformed choices and participatefully in their care and treatment,they need to have information on alltreatment and care options availableto them. This information should beprovided in an easily understoodformat explaining pros and cons.Given that the majority of residentshad been in mental health servicesfor an extended period of time, onewould have expected that theyshould already have had thisinformation.
10.5.2Giving residents back control oftheir lives
The principle of recovery has beenproposed for some time but it isonly in recent years that it hasgathered momentum in Ireland. Thisprinciple has moved away from theprevious thinking of ‘custodial’ careand ‘doing things to people’ to amore person-centred approachwhich gives people control over theirlives and the basic human rightsthat many people take for granted(A Vision for Change, Roberts &Wolfson, 2004). It is clear from thefindings of this study, for examplethe restrictive nature of theresidences and the lack ofparticipation by residents in theircare and treatment, that theprinciple of recovery has been poorlyembraced or realised in thecommunity residential facilities. Forthe principle of recovery to underpinmental health services, the re-training and education of manypeople will be required. Of particularimportance to this report are theresidents, staff and managementresponsible for communityresidences, staff from other agenciessuch as housing, social benefits andemployment, and last but not least,the general public. The need forstaff training and re-education incommunity residences has beenpreviously addressed. Concerning
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 123

the change of attitude of the serviceusers the Values for ActionProgramme outlined in A Vision forChange showed that attitudes ofstaff and service users changedfollowing completion of theprogramme. This programme lookedat the extent to which a number ofvalued life experiences (e.g. choice,relationships, independence) wereavailable in the service users’experience of mental health services.Following completion of theprogramme, comments from staffshowed that they felt that their rolewas enriched and comments fromservice users indicated that they feltthey had regained their self respect.There is a necessity to educate thosewho are or will work closely withthose with severe and persistentproblems on the principles ofrecovery, for example, those inhousing authorities and potentialemployers.
10.5.3Are residents moving on?
First and foremost, the results fromthe present study showed that therewas little movement of residents tolower levels of support. Only 179discharges were reported for theprevious year and, of these, 43 wereto higher levels of support. Thisresulted in 136 discharges in thepast year to lower levels ofaccommodation – 14% of the totalnumber of places. In addition, thekey workers reported that 85% ofresidents were currentlyappropriately placed and predictedthat in the following six monthsmost would remain in their currentresidence. This is somewhat incontrast to the key worker reports offew disabilities in the resident’sclinical, social, occupational andphysical health functioning. Theseanomalies may be due to the staffperceptions of the residences as‘homes for life’, the institutionalisednature of the residences and lack oftraining in rehabilitation andrecovery. As in previous studies inthe UK (Trieman et al., 1998) and
Italy (de Girolamo et al., 2005) theturnover of residents was low andthe findings would suggest that amodel of continuing carepredominated, as opposed to amodel emphasising rehabilitation,recovery and progression to lowerlevels of independence.
10.5.4Lack of rehabilitation andrecovery mental health teams
The majority of the residences werereported as providing rehabilitativeinterventions that have been shownas important in aiding theindividual’s optimal level offunctioning (WHO, 1996). Beforediscussing the extent to which theseinterventions were provided it isnecessary to highlight that theseinterventions were provided in mostareas without the assistance of arehabilitation and recovery mentalhealth team. In only three areaswere rehabilitation and recoverymental health teams available toservices and these were poorlystaffed. A Vision for Changeoutlined the necessary staff and skillmix required for an effectiverehabilitation and recovery mentalhealth team. It is of utmostimportance that these teams are inpost as soon as possible, asrecommended by A Vision forChange. .
10.5.5Pharmacological treatment
The majority of residents were onprescribed medication. There isconcern that some residents wereon both atypical and typical anti-psychotic medication. Themedication prescribed to residentsshould be monitored and evaluatedto ensure that the appropriatemedication and dosage areprescribed at all times and are in linewith best practice guidelines. Someresidents made comments regardingthe lack of information about theirmedication and their willingness tochange or reduce their medication.However, they felt that theiropinions were not valued by the
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND124

doctors. These negative attitudestowards psychiatrists and the lack ofinformation on medication may leadto less co-operation and compliancewith medication. Of utmostimportance is that it infringes on theindividual’s basic right to decide ontheir own treatment.
10.5.6Access to rehabilitative activities
The study results found that themajority of residences wereproviding activities and training forthe residents. These included livingskills and social skills training andleisure and physical activity. Thesewere provided either in theresidences or in the day centres on agroup basis. It is important to notethat these programmes should beaimed at the individual’s needs andrequirements (Anthony et al., 1982,Royal College of Psychiatrists, 2003)as opposed to being offered on agroup basis. It has been argued thatthe provision of group programmesresults in maintenance programmes,as opposed to programmes thatempower the individual to move tothe next level of independence(Anthony et al., 1982). It has beensuggested that the quality of theactivities to aid return toindependent living may impact onthe quality of life of the resident (deGirolamo et al., 2005). The currentstudy did not address the quality ofthe activities in communityresidence. There is a need for furtherresearch to address the issue ofrehabilitative activities and theimpact on the service user’s qualityof life.
10.5.7Attendance at day centres / dayhospitals
In line with previous research, lessthan half of the residents werereported as attending a day centre /day hospital (Donnelly et al., 1996).While attendance at a day centremay not be ideal, the lowattendance rate brings into questionhow residents spend their day.
The vast majority of the residents,however, reported that they werenot bored during the day. A Visionfor Change recommends that daycentres be available for those whoare not in community-basedemployment or engaged inrecreational activities; however, themajority of the interviewed residentswere not availing of these options.These findings suggest that manyresidents were not getting access torehabilitative activities. The issue ofchoice must again be reiterated.Many residents may prefer not toattend day centres, and servicesmust provide a range of options,such as the provision of activities incommunity facilities that includenon-users of mental health services.In fact, residents must be activelyencouraged to engage in activitiesthat are already provided bycommunity local services andcommunity groups. Furthermore,the quality of the activities in daycentres must be evaluated alongwith the extent to which they meetthe needs of the attendees.
10.5.8Employment options forresidents
Only a small number of residences inthis study provided vocationaltraining. This is important, asrelatively few of the residentsinterviewed were in paidemployment in the community,while a slightly larger number werein sheltered employment. Thisreplicates findings from previousstudies in Northern Ireland (McGilloway and Donnelly, 2000).Research has shown that a largeproportion of those with severemental illness want to work inmainstream employment (Bond etal., 2001), a finding that has beenreplicated in the comments from theresidents participating in this study.It was of concern, that only a few ofthe residences provided activities toencourage work or collaboratedwith other agencies to findemployment. WHO (1996) has
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 125

argued that training must beprovided in a real-world context. The‘place and train’ model ofemployment has been shown toincrease the rate of mainstreamemployment, as opposed tosheltered employment (A Vision forChange; Corrigan and McCracken,2005), and has become thepreferred model in the UK and theUS (Royal College of Psychiatrists,2003; Corrigan and McCracken,2005). These programmes place theindividual in mainstreamemployment and gives them thenecessary training and supportsrelevant to their employment. Itmust be noted also that meaningfulactivity is the important factor, be itpaid employment, voluntary work oreducation and skills development(Rankin and Regan, 2004). Mentalhealth services should provide theresident with a range of options sothat they can choose those whichbest suit their needs. A Europeanpsychosocial intervention –Assessment Counselling andCoaching in Employment Placementand Training (ACCEPT) aimed attargeting employment wasevaluated in Northern Ireland(McGilloway and Donnelly, 2000).This multi-agency programme aimedto provide information, support,training and placement inemployment for those whoseemployability was likely to beaffected by mental health problems.The clients of the programmeviewed it in a positive light andapproximately half were in paidemployment or part-time or full-time voluntary work or workexperience at the end of the study.Further research is needed toinvestigate the appropriateness ofdifferent models of employment,such as the ‘place and train model’,within the Irish context.
10.5.9Psychological support for theresidents and their families
WHO (1996) proposes thatpsychological supports in the formof support and educational servicesshould be provided to service usersand their families. This informationshould include information on rightsand the availability of psychosocialresources. In terms of the provisionof information to families, less thanhalf of the residences routinelyprovided family educationprogrammes or had meetings opento relatives. However, it is possiblethat information was provided torelatives on an informal basis, as anumber of staff reported thatrelatives were welcome to come atany time to discuss issues thatconcerned them. Staff alsosuggested that research into thesupports needs of the familiesshould be undertaken. While it wasnot possible address these issues inthe current study, the MHRD of theHRB undertook a study toinvestigate the needs and supportrequirements of families of relativeswith severe and persistent mentalillness (Kartalova O’Doherty et al.,2006). In terms of the psychologicalsupports provided to residents, fewresidences reported that cognitivebehavioural therapy was offered.The majority of the residentsreported, however, that the keyworker was helping them cope withtheir mental health difficulties andpersonal problems. In addition, themajority of residents reported thatthey would seek psychologicalsupport from staff during crisis.Regarding the rights of theresidents, the majority of thenursing officers reported thatresidents were given information ontheir rights, informed aboutcomplaints procedures in place andtold the name of the localcomplaints officer. The findingssuggest that staff did providepsychological support to residentsand that information was providedon rights and complaints
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND126

procedures, but findings regardingthe provision of information torelatives were somewhat less clear.
In terms of support from familiesand friends, nursing officersreported that a quarter of theresidents had no system of supportoutside of the residences. However,the remainder of the residents hadsome system of support. Well overhalf of the residents were reportedto have visits from family and friendsor went out to visit family andfriends. The use of these supportsfor emotional and practical purposesshould be encouraged by staff in theresidences. In fact, the residentsinterviewed reported that theywould turn to family and friends asopposed to other residents or staffwhen needing everydaypsychological support.
10.6 ARE RESIDENTS INTEGRATEDINTO THE COMMUNITIES INWHICH THEY LIVE?
Social inclusion refers to the extent towhich individuals are part of thecommunity in which they live (Rankin,2005a). The findings from the currentstudy demonstrated that less than half ofthe residents attended activities in thecommunity, such as social clubs, bingo,pubs, restaurants and cinemas. Therestrictive nature of the residences or thelack of social contacts from outside mayhave prevented residents from engaging inthese activities. Activities to promotecommunity integration, such as activitiesthat involved members of the community,were reported to be provided in themajority of residences; however, this wasnot reflected in the activities in whichresidents attended. Previous research hasshown that limited social networks canimpact negatively on the individual’smental health and use of external services(Becker et al., 1997). It has beensuggested that moving activities such asthose mentioned earlier (i.e. physical andleisure, training and education) to facilitiesin communities rather than locating themin day centres, and providing activities that
the wider community can partake canimprove community integration for thosein residential facilities (Shephard & Murray,2001). It is important that programmesare individualised and that residents aregiven choices as opposed to group outingsthat currently prevail. These large groupoutings can be stigmatising and are notconducive to integration into the widercommunity.
10.7 TO WHAT EXTENT DO THERESIDENTS SHOWINDEPENDENCE?
The residents who participated in thestudy reported that they were aware of themoney they received each week and halfsaid they received help to manage theirmonies. Yet the nursing officers reportedthat all residents in medium and lowsupport facilities were capable ofmanaging their own money and only 8%of the high support residents werereported as being unable to manage theirown money. This is in sharp contrast tothe proportion of those interviewed whowere taking control of their finances withno significant differences between those inhigh, medium or low support residences.The nurses were asked a general questionregarding the proportion of residents whocould manage their own finances andwere not asked about individual residents.A few possible explanations could accountfor the apparent anomaly in theproportion of residents who were thoughtable to manage their finances and theactual proportion of residents in thesample who do manage their own money.Firstly, nursing officers may have over-estimated the proportion of the residentsthat were managing their own finances.Secondly, residents may have beenreceiving help from others (of which thenurses were unaware), such as family andfriends, although this would seem unlikely.And thirdly, while residents may have beenable to manage their finances, theinstitutional culture of the residences maynot have encouraged them to do so. Themajority of residents went out on theirown, yet only two-thirds of high supportresidents visited the GP by themselves. The
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 127

majority of residents also reported thatthey had moderate control over their livesand how they led them and that they werehappy with their level of independence.On average, the residents rated theirquality of life highly, although those fromhigh support reported a significantly lowerquality of life than those from medium orlow support residences. The possibilityexists that residents do not expect thebasic rights that many people take forgranted and, given that they have been inthe mental health services for a long time,have come to believe that they areincapable of independence. This highlightsthe importance of expectation andproviding residents with competencies andeducation in the principles of recovery.
10.8 LIMITATIONS OF THE STUDYAND FUTURE RESEARCH
This has been the first comprehensivestudy in Ireland to evaluate the communityresidential accommodation for those withsevere mental illness. One of the strengthsis that it examined life in the residencesfrom the viewpoint of the residents. This isan important aspect of the study and onethat provides invaluable information thatcan be used to design and develop theseservices in the future.
Given the resources required for such alarge scale study on a national level,available resources allowed only three localHSE areas to participate in the currentstudy. The areas were selected based onthe number of residences and theirwillingness to participate. However theauthors and advisory group felt that thethree areas were generally representativeof the community residential mental healthservices in Ireland in relation to level ofdevelopment, number of facilities and theirlocation.
While a sufficient number of residentswere interviewed for the total sample, thesmall numbers when stratified by level ofsupport precluded any in-depth sub-groupanalysis. Furthermore, the sample excludedto a large extent those who moved rapidlythrough the system, either to independent
living or re-hospitalisation.
Sampling of staff was less than ideal.Given the high turn-over of staff it isdifficult to know how representative thesample was. The results suggest that thestaff sampled had worked in residentialfacilities, either inpatient or community, fora long time. Newer staff or those who hadworked primarily in community care mayhave had different perceptions of thecommunity residential facilities. Anestimated response rate to the staffquestionnaires is provided, however giventhe fluctuation in staff hours the exactnumber of staff working in the residencewas difficult to estimate.
This study described and evaluated theresidential facilities in Ireland. Due to thelack of fully developed rehabilitation teamsand services, alternative models ofrehabilitation could not be assessed. Inaddition, the majority of the residentialfacilities at all levels of support wereprovided by the mental health services,thus the evaluation of alternative modelswas not possible. It is important thatresearch and evaluation be carried out onthese models as they develop. There is aneed to identify which settings are bestsuited to particular groups of residentsand how this improves the quality andappropriateness of care delivered andresidents’ quality of life.
This study has highlighted a number ofareas for further research. Given the lowlevels of employment of residents, it is notpossible to investigate the benefits ofvarious employment models that cater forthose in community mental healthresidential settings within the Irish context.The area of rehabilitation and recovery hasreceived little attention in mental healthresearch. Further research in this area isneeded to investigate the process ofrecovery from the service users’ viewpoint.In addition, further research into thepsycho-social, cognitive and clinical factorsthat influence rehabilitation and recovery isrequired.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND128

10.9 SUMMARY
The aim of this study was to describe thecommunity residential facilities for thosewith severe mental illness in three HSElocal areas in Ireland. While the studyinvestigated only three areas, there is noreason to assume that the range andprovision of residential facilities in theseareas are not broadly representative of theresidential facilities in Ireland. As pointedout previously (Section 4.2), practically allthe residential accommodation in Irelandhas been provided by the mental healthservices and thus, while there may beslight differences between local areas, themethod of care and treatment is similarthroughout the country. Thus, therecommendations made in Chapter 11apply to all residential accommodation inIreland which must take into account theneeds of the local area and service users.
One of the prime aims of this study was toinvestigate the residents’ views of theirlives and self-reports of quality of life andsatisfaction with treatment and care.Practically all residents were happy in theircurrent accommodation. However, if givena choice, a number of residents wouldrather be at home or in independentaccommodation. The vast majority ofresidents perceived their lives in theresidences positively. They perceived thatthey had control over their lives and couldlead their lives as they wanted. Perceptionsof their life in the community were alsopositive. The residents were mostlysatisfied with the treatment and careprovided in the residences. They also ratedtheir quality of life positively, with themajority of residents ‘mostly satisfied’ withthe way things were. However, aspreviously mentioned, this must becompared with the findings from theopen-ended questions, whereby theperceptions of the residents somewhatdiffered from the responses to thequestionnaire measures. Responses to theopen-ended questions showed thatresidents had hopes and expectations forthe future that involved taking morecontrol of their lives and gainingindependence from services. It is possiblethat these anomalies occurred because ofa failure on the part of the residents to see
a change in a system that they havebecome accustomed to, theirunwillingness to be ‘negative’ towardsthose who have provided them with careand treatment over long periods of timeand with whom they had established aclose relationship and the lack ofalternative options available to them. It isimportant that service users’ hopes andaspirations for the future should be part ofthe individualised care planning process. Inaddition, many of the staff had worked inthe system for long periods of time andthey also may have failed to see the systemas one that emphasised recovery asopposed to maintenance. This highlightsthe need for the training and educationfor all in community residential facilities inthe competences and principles ofrecovery.
There were significant differences in theclinical and psychosocial functioning of theresidents in high, medium and lowsupport residences, with high supportresidents having lower functioning thanthose in medium or low. However theclinical significance of these differences isquestionable. The mean scores of allgroups fell within the mild to moderaterange of clinical symptoms and disabilitiesin psychosocial functioning scores werealso in the mild to moderate range. Thisbrings into question the basis upon whichresidents were assigned to these levels ofsupport. The low level of movement fromoriginal placements also suggests thatthere was a tendency for residents toremain in original placements.
Just over half of the residences had formalassessments of residents, but did not havea full multidisciplinary team to do thisassessment, which may have resulted inthe inappropriate placement of someresidents. While the majority of residenceswere reported to have a care plans systemin use, the residents did not seem to beaware of this. The purposes of care plansare to detail the residents’ aims and goalsof treatment and rehabilitation. Inaddition, rehabilitation programmesseemed to be offered on a group basisand not tailored to meet the needs of theindividual residents. Nevertheless, thenursing staff within the residences must be
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 129

commended for their provision ofinterventions aimed at rehabilitation. Thismust have been especially difficulty giventhe lack of training aimed specifically atrehabilitation and the lack of arehabilitation and recovery mental healthteam. The two rehabilitation and recoverymental health teams that were in placewere under-staffed and did not have theproper skill mix for the team to runefficiently and effectively. The finding thatfew residents were in employment, eithersheltered or mainstream, and the apparentlack of the residents’ integration into thecommunity in which they lived suggestedthat the interventions aimed atrehabilitation to lower levels of support orindependent living were not meeting theneeds of the residents.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND130

CHAPTER 11The Way Forward:Recommendations

This chapter will make specific recommendationsregarding the future development of thecommunity residences based on the findings ofthe study and the information and experiencegathered during the fieldwork. The studyrecommendations take into account the twomost relevant recent Irish documents, A Visionfor Change and The Report of the Inspector ofMental Health Services 2005 (MHC, 2006c) andevidence-based practice. The authors weremindful of the feasibility of implementing therecommendations within the Irish mental healthservices and were of the opinion that therecommendations should be addressed in theshort to medium term, without delay. It is theauthors’ intention however, that theserecommendations will be evaluated in light oflocal area needs, requirements and resources andadapted and implemented accordingly.
The recommendations are organised under threemain headings: the way forward forrehabilitation and recovery, the way forward forcommunity residences, and future provision ofhousing for those with mental health problems.In addition, recommendations are maderegarding the best way forward for theimplementation of these recommendations.Many of the recommendations from the presentstudy are dependent on the implementation ofthe multidisciplinary rehabilitation and recoverymental health teams advocated in A Vision forChange, and these must be implemented assoon as possible.
11.1 THE WAY FORWARD FORREHABILITATION AND RECOVERY
As highlighted above, the first step indeveloping rehabilitation and recoveryservices is the provision of properlystaffed multidisciplinary rehabilitationand recovery mental health teams,which should be put in place as soonas possible.
All members of the rehabilitation andrecovery mental health team should betrained in the competencies andprinciples of recovery.
Residents currently in the residencesshould receive a full multidisciplinaryassessment, as should potentialresidents.
Staff should, by attitude and practice,orient residents towards raising theirexpectations of their capabilities toachieve independence.
Care plans should be developed inconsultation with residents, and theseshould be reviewed on a regular basis.It is imperative that residents areactively encouraged to partake in thecare planning process. If necessary, anadvocate should be present.
A key worker system should be in placein all residences and the resident shouldbe made aware of this system.
The pharmacological treatment ofresidents should be monitored regularlyand residents should be able to makeinformed choices about theirmedication.
Rehabilitative activities should betailored to meet the needs of theindividual, and linked to care plans andshould be offered in communityfacilities whenever possible. Thedevelopment of these activities shouldbe informed by, and evaluated withreference to, best practice the extent towhich they are meeting the needs ofthe residents.
Residents who are able should beencouraged to look after their ownfinances. This means collecting moneyat the post office, saving money, andhaving the independence to spend theirmoney as they wish.
Residents should be encouraged toattend social amenities and events inthe community. Those who havedifficulty integrating into thecommunity should be provided withspecific programmes that address theseneeds. It is imperative that residents areencouraged to participate in socialactivities provided by local services andcommunity groups.
Residents should be encouraged to useand develop support networks fromoutside the residences. The inclusionand participation of relatives andfriends in the day-to -day activities ofthe residences and in the treatment
Chapter 11
The way forward: recommendations
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND132

and care of the resident, may helpdevelop these support systems.
Participation in mainstreamemployment should be encouraged andthe ‘place and train’ model should beevaluated in the Irish context. For thisto be realised, interagency co-operationbetween mental health services,training agencies and employers needsto be developed.
For those who cannot or do not wantto enter mainstream employment,other options for meaningful activitiesshould be provided. These could takethe form of voluntary work, pursuit ofhobbies, further training or furthereducation.
11.2 THE WAY FORWARD FORCURRENT RESIDENCES
Community residences should not beused for purposes other than supportand rehabilitation. The use of beds fortemporary respite, crisis care oremergency transfers in place of acutecare is not in the best interests of thosewho live in the residences. Otherprovisions should be made for thesegroups.
All staff working in communityresidences and those working with thispopulation should be trained in thecompetencies and principles ofrecovery.
The rules and regulations of theresidences should be re-visited. Whilesome general rules and regulations arerequired, those regarding the freedomof the residents should be amended tomeet individual needs. The residencesshould provide as homelike anenvironment as possible.
The aims and functions of thecommunity residences should bestandardised so that both staff andresidents are aware of theirresponsibilities to meet these aims andfunctions. Furthermore the aims andfunctions of the different levels of
support should be specified andstandardised throughout the countryand residents informed of these.Currently the residences are providingtwo main functions – continuing care,and rehabilitation to more independentsettings. It is debatable as to whetherthe alliance of two apparentlyconflicting functions is the best way tomeet the needs of the differentresidents. The findings of the currentstudy would suggest that the needs ofthose who wish to move to lower levelsof support but need intensiverehabilitation are not being met.
The rate of provision of places,particularly of high support residentialplaces (76 per 100,000), is higher thanthe recommended 30 places per100,000 by A Vision for Change. Theauthors acknowledge that a smallminority of individuals will continue toneed high support care and that someof the current high support residencesshould be maintained for thesepurposes. It is also acknowledged that,in some areas, patients still remain inpsychiatric hospitals and will needrelocation to alternative residences.Residents who have been relocated tocommunity settings from psychiatrichospitals or those who have spent longperiods of time in their currentaccommodation should have the rightto remain in these facilities, if they sowish. Newer residents or potentialresidents should be informed of thetemporary nature of their placementand should be encouraged andsupported to prepare for moreindependent living.
As outlined in Chapter 10, thefunctions of some of the high supportresidences may change in line withrecommendations from A Vision forChange (i.e. intensive rehabilitationplaces, crisis care places). Communityresidences that will be no longerneeded for current purposes can be re-designed to provide for other functionssuch as intensive rehabilitation, crisiscare and high support care. Mentalhealth services should keep this housingstock in mind when addressing the
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 133

needs of future communityrequirements, such as mental healthcentres as recommended in A Vision forChange.
The number of places in manyindividual high support residences is atpresent above the recommended tenadvocated in A Vision for Change. Thenumber of places per residence hasimplications for the privacy of theoccupants. All high support residencesshould reduce the number of places tothe recommended level. No residentsshould have to share a room with morethan one person and, if at all possible,single rooms should be provided. If theenvironment allows, bedrooms shouldbe renovated to include en-suitebathrooms or shower rooms.
The nursing staff resources currentlyemployed in the residences should beevaluated in terms of the need fornursing and non-nursing staff and thecurrent blend of skill mix. Excessnursing staff currently employed in theresidences should be re-allocated tocommunity mental health teams.
The health and safety regulations and,in particular, Hazard Analysis andCritical Control Points (HACCP) shouldbe revisited. These currently preventresidents from using kitchen facilities inhigh support residences, an importantaspect of independence.
Evaluation and review procedures tomonitor quality should be implementedin all residences. These should takeaccount of the residents’ satisfactionand, wherever possible, the relatives’views.
Any outstanding issues in relation topayment of rent should be finalised toavoid any distress to residents, staff andmanagement.
Local authorities have a responsibility toprovide nearly 2,000 housing places inmedium and low support residences.Intersectoral and interagencycollaboration is needed to stimulatelocal authorities to start providing the2,000 places identified as needed. The
Departments of Health andEnvironment, local housing authorities,the HSE and voluntary agencies need towork together to set up innovative,imaginative and pilot partnershipsschemes to provide accommodation forthose with medium and low supportneeds.
The possibility of the local housingauthorities taking over responsibility forthe provision and management of lowsupport residences should be discussedwith representatives from relevantstakeholder groups and service users ata national level.
The possibility of voluntary agenciestaking a greater role in the provision ofmedium support residences should beencouraged, with the setting up ofpilot partnership projects involving allstakeholders.
Mental health services should contactlocal housing authorities to determinethe possibility of setting up pilothousing projects for groups of three tofour individuals. At least two pilot areasin Ireland should be selected andevaluated. The Dublin City Council hasalready expressed interest in such aninitiative.
11.3 FUTURE PROVISION OF HOUSING
Housing for those with mental healthdifficulties must be provided inmainstream housing in the community.The provision of housing is not theresponsibility of the mental healthservices. As reported in A Vision forChange the ‘statutory responsibility toprovide this housing is not within theremit of the mental health services orthe HSE’.
The future provision of housing, inparticular medium and low supporthousing, for those with mental healthproblems should not be theresponsibility of the mental healthservices. There is a need for statutoryand non-statutory bodies to work incollaboration with mental healthservices to define their roles in relation
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND134

to the needs and support requirementsof this population. Some examples havebeen provided in the report and theseshould be evaluated within the Irishcontext. The authors acknowledge thatbuilding effective interagencypartnerships will take time. Yet thisshould begin as soon as possible withthose at the highest level of the HSEand governmental bodies providingleadership and direction to those atlocal level.
Interagency working will be mosteffective when the roles andresponsibilities of each agency areclearly defined. In addition, agenciesmust have mutual trust, respect andunderstanding of their respective rolesand responsibilities.
Voluntary agencies, working closelywith mental health services and serviceusers, have begun to provide housingand care for vulnerable groups andthese existing models should beevaluated and if effective, publiclyencouraged and promoted bygovernment.
A range of housing alternatives isnecessary for those with differing levelsof need and support requirements. Incontrast to what is currently provided,the level of support should be flexible.Provision of support by ‘recoveryguides’ (as in the STEER project) shouldbe evaluated as a possible model forthe provision of low to medium levelsof support.
All future housing for those withmental health problems should bedesigned with the principles of recoveryin mind. All residents sharingaccommodation should have their ownen-suite bedroom. All new housingshould be life-time adaptable.
11.4 IMPLEMENTATION ACTION PLAN
To enable implementation to proceedrapidly, intersectoral action plans areneeded at central and local levels.
Local groups, one for each catchmentarea of approximately 300,000population as recommended in AVision for Change, should have theappropriate representation of housingand mental health interests that willdraw up action plans at local level andreport to the central group.
At central level an intersectoralimplementation group should beformed. This group might comprise thefollowing stakeholders - theDepartment of the Environment,Heritage and Local Government, theDepartment of Health and Children, theHSE, Mental Health Commission, localhousing authorities, local mental healthservices, local housing associations, andrepresentatives of service-user groups.
The group would:
• Lead on the intersectoral policychanges required to implement therecommendations and develop acentral intersectoral action planaccordingly.
• Work through local groups tomonitor progress towardsimplementation.
• Liaise in this endeavour with theimplementation and monitoringbodies of A Vision for Change.
• These recommendations should beimplemented without delay. Manyof the recommendations areresource neutral but whereresources are required they shouldbe made available.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 135

A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND136

References

Anthony WA, Cohen, M & Farkas M (1982) A psychiatric rehabilitation programme, can I recognise oneif I see one? Community Mental Health Journal, 18: 83–95.
Anthony WA (1993) Recovery from mental illness: the guiding vision of the mental health servicesystem in the 1990’s. Psychosocial Rehabilitation Journal, 16: 11–23.
Becker T, Thornifcroft G, Leese M, McCrone P, Johnson S, Albert M & Turner D (1997) Social networkand service among representative cases of psychosis in South London. British Journal of Psychiatry, 171:15–19
Berzins K M, Petch A & Atkinson JM (2003) Prevalence and experience of harassment of people withmental health problems living in the community. British Journal of Psychiatry, 183: 526–533.
Bond GR, Drake RE, Mueser KT & Becker, DR (1997) An update on supported employment for peoplewith severe mental illness. Psychiatric Services, 48: 335–346.
Bond GR, Becker DR, Drake RE, Rapp CA, Meisler N, Lehman AF, Bell MD & Blyer CR (2001)Implementing supported employment as an evidence-based practice. Psychiatric Services, 52: 313–322.
Bond GR (2004) Supported employment: evidence for an evidence-based practice. PsychiatricRehabilitation Journal, 27(4): 345–359.
British Psychological Society (2000) Recent advances in understanding mental illness and psychoticexperiences. London: The British Psychological Society.
Brugha TS, Win, JK, Brewin CR, MacCarthy B, Mangan S, Lesage A & Mumford J (1988) The problemsof people in long-term psychiatric day care. An introduction to the Camberwell High Contact Survey.Psychological Medicine, 18: 443–456.
Brunt D & Hansson L (2004) The quality of life of persons with severe mental illness across housingsettings. Nord J Psychiatry, 58(4): 293–298.
Byrne P (1997) Psychiatric stigma. Journal of Research and Social Medicine, 90: 618 – 621.
Carling PJ (1993) Housing and supports for persons with mental illness: Emerging approaches toresearch and practice. Hospital and Community Psychiatry, 44(5): 439–449.
Commission of the European Communities (2005) Green Paper: Improving the mental health of thepopulation: Towards a strategy on mental health for the European Union. Brussels: EuropeanCommission and Health & Consumer Protection Directorate General.
Cook JA, Leff SH, Blyler CR, Gold PB, Goldberg RW, Mueser KT, Toprac MG, McFarlane WR, Shafer MS,Blankertz LE, Dedek K, Razzano LA, Grey DD & Burke-Miller J (2005) Results of a multisite randomizedtrial of supported employment interventions for individuals with severe mental illness. Archives ofGeneral Psychiatry, 62: 505–512.
Copeland ME (2006) Finding our voice! Ending the silence. Retrieved 26 April 2006 fromwww.akmhcweb.org/recovery/MaryEllenCopeland/finding_our_voice.htm
Copty M & Whitford D (2005) Mental health in general practice: Assessment of current state and futureneeds. Irish Journal of Psychological Medicine, 22 (3) 83–86.
Corrigan PW & McCracken SG (2005). Place first, then train: an alternative to the medical model ofpsychiatric rehabilitation. Social Work, 50, (1): 31 – 39.
Couture S & Penn D (2003) Interpersonal contact and the stigma of mental illness: a review of theliterature. Journal of Mental Health, 12 (3) 291–305.
Daly A & Walsh D (2002a) Irish Psychiatric Hospitals and Units Census 2001. Dublin: Health ResearchBoard.
References
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND138

Daly A & Walsh D (2002b) Activities of Irish Psychiatric Services 2001. Dublin: Health Research Board.
Daly A, Walsh D, Comish J, Kartalova O’Doherty Y, Moran R & O’Reilly A (2005) Activities of IrishPsychiatric Hospitals and Units 2004. Dublin: Health Research Board.
Daly A & Walsh D (2006) Irish psychiatric unit and hospital census. Dublin: Health Research Board.
de Girolamo G, Picardi A, Micciolo R, Fallon I, Fioritti A (2002) Residential care in Italy. National surveyof non-hospital facilities. British Journal of Psychiatry, 181: 220–225.
de Girolamo G & Bassi M (2004) Residential facilities as the new scenario of long-term psychiatric care,Current Opinion in Psychiatry, 17: 275–281.
de Girolama G, Picardi A, Santone G, Falloon I, Morosini P, Fioritti A & Micciolo R (2005) The severelymentally ill in residential facilities: A national survey in Italy. Psychological Medicine, 35: 421– 431.
Department of Health (1966) Commission on Inquiry on Mental Illness 1966 Report. Dublin: StationeryOffice.
Department of Health and Children (1984) The Psychiatric Services – Planning for the future. Report ofa study group on the development of the psychiatric services. Dublin: Stationery Office.
Department of Health and Children (1989) Shaping a Healthier Future – Health Strategy. Dublin:Stationery Office.
Department of Health (1995) White Paper: A New Mental Health Act. Dublin: Stationery Office.
Department of Health and Children (2001) Report of the Inspectorate of Mental Hospitals, 2000.Dublin: Stationery Office.
Department of Health and Children (2001) Quality and Fairness, A health system for you, HealthStrategy, Dublin: Stationery Office.
Department of Health and Children (2003) Report of the Inspectorate of Mental Hospitals, 2002.Dublin: Stationery Office.
Department of Health and Children (2004) Report of the Inspectorate of Mental Hospitals, 2003.Dublin: Stationery Office.
Department of Health and Children (2006) A Vision for Change: Report of the expert group on mentalhealth policy. Dublin: Stationery Office.
Department of Health (2000) The journey to recovery – The Government’s vision for mental health care.London: HMSO.
Department of the Environment, Heritage and Local Government (2005) Housing Policy Framework:Building Sustainable Communities. Dublin: DEHLG.
Donnelly M, McGilloway S, Mays N, Perry S, Knapp M, Kavanagh S, Beecham J, Fenyo A & Astin J(1994)
Opening New Doors: An Evaluation of Community Care for People Discharged from Psychiatric andMental Handicap Hospitals. London: HMSO.
Donnelly M, McGilloway S, Mays N, Perry S & Lavery C (1997) A three to six year follow-up of formerlong stay psychiatric patients. Social Psychiatry and Psychiatric Epidemiology, 32: 451-458.
Drachman D (1981) A residential continuum for the chronically mentally ill: a Markov probability model.Eval Health Prof, 4: 93–104.
Drake RE, Becker DR, Clark RE & Mueser KT (1999) Research on the individual placement and support
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 139

model of supported employment. Psychiatry Q. 70(4): 289 – 301.
Dunne E (2006) The views of adult users of the public sector mental health services. Dublin: MentalHealth Commission.
Geller JL & Fisher WH (1993) The linear continuum of transitional residences: debunking the myth.American Journal of Psychiatry, 150(7): 1070–1076.
Goering P, Durbin J, Foster R, Boyles S, Babiak T & Lancee B (1992) Social networks of residents insupportive housing. Community Mental Health Journal, 28: 199–214.
Government of Ireland (1945) Mental Treatment Act, 1945. Dublin: Stationery Office.
Government of Ireland (1995) White paper on Mental Health. Dublin: Stationery Office.
Government of Ireland (2001) Mental Health Act, 2001. Dublin: Stationery Office.
Government of Ireland (2002) Housing (Miscellaneous Provisions) Act, 2002. Dublin: Stationery Office.
Harkness J, Newman SJ & Salkever D (2004) The cost-effectiveness of independent housing for thechronically mentally ill: do housing and neighbourhood features matter? Health Services Research,39(5): 1341–1360.
Health Service Executive (2004) Review of community accommodation within the mental health servicein the Northern Area. Dublin: Health Service Executive.
Heanue K (2006) The need for social housing in peripheral rural areas. Administration, 52 (3): 3 – 21.
Hickey T, Moran R & Walsh D (2003) Psychiatric Day Care – An unused option? Dublin: Health ResearchBoard.
Hocking B (2003) Reducing mental health stigma and discrimination – everybody’s business. TheMedical Journal of Australia, 178 (9): 47 – 48.
Johnson R (2005) Mental health, housing and community: making the links in policy, research andpractice. Journal of Public Mental Health, 4(4): 21 – 29.
Jones L (1996) George III and changing views of madness. In Heller T, Reynolds J, Gomm R, Mustan R,Pattison S (eds) Mental health matters: A reader. London: MacMillian: Open University.
Jorm AF, Korten AE and Jacomb PA (1997) “Mental health literacy”. A survey of the public’s ability torecognise mental health disorders and their beliefs about the effectiveness of treatment. The MedicalJournal of Australia, 166: 182 – 186.
Keogh F, Roche A & Walsh D (1999) We have no beds…: An enquiry into the availability and use ofacute psychiatric beds in the Eastern Health Board Region. Dublin: Health Research Board.
Liberman RP & Kopelowicz A (2005) Recovery from schizophrenia: a concept in search of research.Psychiatric Services, 56 (6): 735 – 742.
Leff J (1997) Care in the community. Illusion or reality? Chichester: Wiley.
Leff J & Trieman N (2000) Long-stay patients discharged from psychiatric hospitals – Social and clinicaloutcomes after five years in the community. The TAPS Project 46. British Journal of Psychiatry, 176:217–223.
Lelliott P, Audini B, Knapp & Chisholm D (1996) The Mental Health Residential Care Study: classificationof facilities and description of residents. Hospital and Community Psychiatry, 37: 901–907.
Macpherson R & Jerrom B (1999) Review of twenty-four hour nursed care. Advances in PsychiatricTreatment, 5: 146–153.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND140

McGee H, O’Hanlon A, Barker M, Hickey A, Garavan R, Conroy R, Layte R, Shelly E, Horgan F, CrawfordV, Stout R & O’Neill D (2005) One island – two systems. A comparison of health status and health andsocial service use by community-dwelling older people in the Republic of Ireland and Northern Ireland.Dublin: Institute of Public Health in Ireland, Report No. 5.
McGilloway S, Donnelly M & Mays N (1997) The experience of caring for former long-stay psychiatricpatients. British Journal of Clinical Psychology, 36: 149-151.
McGilloway S & Donnelly M (1998) Service utilisation by former long-stay psychiatric patients inNorthern Ireland. International Journal of Social Psychiatry, 44: 12-21.
McGilloway S & Donnelly M (1998) On the Way to Work: An Evaluation of ACCEPT. Belfast: N. IrelandEuropean Horizon Project.
McGilloway S & Donnelly M (2000) Work, rehabilitation and mental health. Journal of Mental Health,9: (2), 199-210.
Mental Health Commission (2001) Recovery competencies for New Zealand mental health workers.Wellington: Mental Health Commission.
Mental Health Commission (2005a) Annual Report 2004. Including the Report of the Inspector ofMental Health Services. Dublin: Mental Health Commission
Mental Health Commission (2005b) A vision for a recovery model in Irish mental health services. Dublin:Mental Health Commission.
Mental Health Commission (2005c) Quality in mental health – your views. Dublin: Mental HealthCommission.
Mental Health Commission (2006a) Multidisciplinary team working: from theory to practice. Dublin:Mental Health Commission.
Mental Health Commission (2006b) Forensic mental health services for adults in Ireland. Dublin: MentalHealth Commission.
Mental Health Commission (2006c) Annual Report 2005. Including the Report of the Inspector ofMental Health Services. Dublin: Mental Health Commission.
Mirkin SM & Namerow MJ (1991) Why study treatment outcome. Hospital and Community Psychiatry,42(10): 1007–1013.
Mind (2004) Not alone? Isolation and mental illness. [Electronic version]. Retrieved 24 March 2005from www.mind.org.uk
National Housing Federation and The Mental Health Foundation (1996) Code of conduct for housingcare and support. London: National Housing Federation and the Mental Health Foundation.
National Institute for Mental Health in England (2004) From here to equality. [Electronic version.]Retreived 30 January 2005 from nimhe.csip.org.uk.
O’Driscoll C & Leff J (1993) The TAPS Project .8. Design of the research study on the long stay patients.British Journal of Psychiatry, 162: 18–24.
Office for Social Inclusion (2003) National Action Plan against Poverty and Social Exclusion 2003 –2005, Dublin: Office for Social Inclusion.
Office of Deputy Prime Minister (2005) Supporting people guide to accommodation and supportoptions for people with mental health problems. London: Office of Deputy Prime Minister.
Picardi A, de Girolamo G, Santone G, Falloon I, Fioritti A, Micciolo R, Morosini P, Zanalda E (2006) The
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 141

environment and the staff of residential facilities: Data from the Italian ‘progress’ National Survey.Community Mental Health Journal, 42 (3): 263 – 279.
Ralph RO, Lambert D & Kidder KA (2002) The recovery perspective and evidence based practice forpeople with serious mental illness: A guideline developed for the Behavioural Health Recovery
Management Project, University of Chicago, Centre for Psychiatric Rehabilitation [Electronic Version].http://bhrmorg/guidelines/mhguidelines.htm
Rankin J (2005a) Mental health and social inclusion. London: Institute for Public Policy Research.
Rankin J (2005b) Mental health in the mainstream. London: Institute for Public Policy Research.
Rankin J & Regan S (2004) Meeting complex needs. London: Institute for Public Policy Research.
Roberts G & Wolfson P (2004) The rediscovery of recovery: open to all. Advances in PsychiatricTreatment, 10: 37–49.
Rog DJ (2004) The evidence on supported housing. Psychiatric Rehabilitation Journal, 27(4): 334–344.
Royal College of Psychiatrists (2003) Rehabilitation and recovery now. London: Royal College ofPsychiatrists.
Santone G, de Girolamo G, Falloon I, Fioritti A, Micciolo R, Picardi A & Zanalda E (2005) The process ofcare in residential facilities. A national survey in Italy. Social Psychiatry and Psychiatric Epidemiology, 40(7): 540 – 550.
Schizophrenia Ireland (2003) Towards recovery: principles of good practice in the treatment, care,rehabilitation and recovery of people with a diagnosis of schizophrenia and related mental disorders.Ireland: Schizophrenia Ireland/Lucia Foundation and Irish Psychiatric Association.
Schizophrenia Ireland (2005) Media watch report 2004: tackling stigma. Ireland: SchizophreniaIreland/Lucia Foundation and Irish Psychiatric Association.
Schizophrenia Ireland (2006) Talking about choice: developing the dialogue for individual’s recoveryand partnership.. Ireland: Schizophrenia Ireland/Lucia Foundation and Irish Psychiatric Association.
Senn V, Kendal R & Trieman N (1997) The TAPS project 38: level of training and its availability to carerswithin group homes in a London district. Social Psychiatry and Psychiatric Edidemiology, 32: 317–322.
Shepherd G, Muijen M, Dean R & Cooney M (1996) Residential care in hospital and in the community.Quality of care and quality of life. British Journal of Psychiarty, 168: 448–456.
Shepherd G, Beadsmoore A, Moore C, Hardy P & Muijen M (1997) Relation between bed use, socialdeprivation, and overall bed availability in acute adult psychiatric units, and alternative residentialoptions: a cross sectional survey, one-day census data and staff interviews. British Medical Journal,262–266.
Shepherd G (1998) System failure? The problems of reductions in long-stay beds in the UK.Epidemiologia e Psichiatria Sociale, 7(2): 127–134.
Shepherd G & Murray A (2001) Residential care. In Thornicroft, G & Szmukler, G (eds) Textbook ofCommunity Psychiatry. pp. 309–320 Oxford: Oxford University Press.
Shiely F & Kelleher C (2004) Older people in Ireland: A profile of health status, lifestyle and economicfactors from SLAN. Report No. 82. Dublin: Department of Health and Children.
Social Exclusion Unit (2004a) Mental health and social exclusion. London: Office of the Deputy PrimeMinister.
Social Exclusion Unit (2004b) Action on mental health. A guide to promoting social inclusion. London:Office of the Deputy Prime Minister.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND142

Szmuckler G & Thornicroft G (eds) (2001) Textbook of Community Psychiatry. Oxford: Oxford UniversityPress.
Tansella, M (1986) Community psychiatry without psychiatric hospitals – the Italian experience – areview. Journal of the Royal Society of Medicine, 79(11): 664–669.
Tansella M & Thornicroft G (2001). The principles underlying community care. In Thornicroft, G &Szmukler, G (eds) Textbook of Community Psychiatry. pp. 155 – 165. Oxford: Oxford University Press.
Tempier R, Mercier C, Leouffre P & Caron J (1997) Quality of life and social integration of severelymentally ill patients: a longitudinal study. Journal of Psychiatry & Neuroscience, 22 (4), 249 – 255.
Tomasi R, de Girolamo G, Santone G, Picardi A, Micciolo R, Semisa D & Fava S (2005) The prescriptionof psychotropic drugs in residential facilities: A national survey in Italy. Acta Psychiatrica Scandinavica,113 (3): 212 – 223.
The Sainsbury Centre for Mental Health (2004) A new model for mental health services in the NorthWest of Ireland. Ireland: North Western Health Board.
Thornicroft G (2004) Components of a modern mental health service: a pragmatic balance ofcommunity and hospital care. Overview of systematic evidence. British Journal of psychiatry, 185,283–290.
Thornicroft G (2005) Components of a modern mental health service: a pragmatic balance ofcommunity and hospital care. Paper presented at WHO European Ministerial Conference on MentalHealth: Facing the Challenges, Building Solutions, Helsinki, 12–15 January 2005.
Thornicroft G & Breakey W (1991) The COSTAR programme: improving social networks of the mentallyill. British Journal of Psychiatry, 159: 245–249.
Thornicroft G & Tansella M (1999). The Mental Health Matrix: A Manual to Improve Services.Cambridge: Cambridge University Press
Thornicroft G & Tansella M (1999) The mental health matrix. A manual to improve services. Cambridge:Cambridge University Press.
Thornicroft G & Tansella M (2003) What are the arguments for community based health care?Denmark: WHO Regional Office for Europe’s Health Evidence Network (HEN).
Thornicroft G & Tansella M (2004) Components of a modern mental health service: a pragmatic balanceof community and hospital care. The British Journal of Psychiatry, 185: 283–290.
Thornicroft G, Wykes T, Holloway F et al., (1998) From efficacy to effectiveness in community mentalhealth services. PRISM Psychosis Study 10. British Journal of Psychiatry, 173: 423–427.
Trieman N, Smith HE, Kendal R et al . (1998) The TAPS project 41: homes for life? Residential stabilityfive years after hospital discharge. Community Mental Health Journal, 34: 407–417.
Warner, R (1985) Recovery from schizophrenia. Psychiatry and political economy. New York: Routledgeand Kegan Paul.
Warner S, Bennett S, Ford R, Thompson K (1997) Home from home: A guide to good practice in theprovision of housing and support for people with mental health problems. London: The SainsburyCentre for Mental Health.
Wing JK & Furlong R (1986) A haven for the severely disabled within the context of a comprehensivepsychiatric community service. British Journal of Psychiatry, 149: 499–457.
Wolff G, Pathare S, Craig T & Leff J (1996) Public education for community care: a new approach.British Journal of Psychiatry, 168: 441–447.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 143

World Health Organization (1996) Psychosocial Rehabilitation: A consensus statement. Geneva: WHO,Division of Mental Health and Prevention of Substance Abuse.
World Health Organization (2003) Mental Health in the WHO European Region. Fact SheetEURO/03/03. Geneva: World Health Organisation.
World Health Organization (2003) The mental health context [Electronic version]. Mental health policyand service guidance package. Retrieved 06 September 2004 from:http://www.who.int/mental_health/resources/en/context.PDF.
World Health Organization (2005) European Ministerial Conference on Mental Health: Facing theChallenges, Building Solutions. Helsinki, 12–15 January 2005.
Veiel HOF (1990) The Mannheim Interview on Social Support. Social Psychiatry and Social Epidemiology,25 (5): 250 – 259.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND144

APPENDIX 1Facility Questionnaire

Name of residence ___________________________ Health Board ______________________
Date schedule completed ____/_____/_____ Year residence opened_______________
Level of supportHigh ( )Medium ( )Low ( )Other ____________________
Completed by: _____________________Job title __________________ Contact No. _____________
Where is the building located Located in same building along with other residential units ( )Situated in a housing estate ( )Situated within the grounds of the psychiatric hospital ( )Private building on own ( )Other (please specify) ___________________________________
Description of the location of the buildingUrban ( ) Periphery ( ) Rural ( )
Is the building owned by: Health Board ( ) Voluntary ( ) Private ( )
Building Features
Interior total (sqm) _______________Exterior total (sqm i.e. balcony, garden, etc) _________________Number of Bedrooms single ______ double ______ triple _______ others ______Number of Bathrooms _________________Number Bathroom for residents use only ________________Number Living Rooms _________________Are there any rooms for staff use only (e.g. dressing room, bedroom, office, conference room, etc.) Yes ( ) No ( )Is there a kitchen? Yes ( ) No ( )Is there a designated visiting room (i.e. not TV room)? Yes ( ) No ( )Is the building suitable for those with mobility problems? Yes ( ) No ( )
Appendix 1
Facility questionnaire
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND146

If no, what are the barriers?_________________________________________________________________________________Number of public phones _____________Is there a smoking room? Yes ( ) No ( )If yes, is it Inside residence ( ) Outside residence ( )
ACCESS TO SERVICES
Time in minutes to reach shopping centre or general shop on foot ________Time in minutes to reach shopping centre or general shop by public transport ________Time in minutes to reach post office on foot ________Time in minutes to reach post office by public transport ________Time in minutes to reach pub on foot ________Time in minutes to reach primary care centre (GP) on foot ________Time in minutes to reach primary care centre (GP) by public transport ________Number of residents that have access to own transportation (e.g. car, bike) ________
Please enter number of individuals with particular form of transport in bracketsPersonal car ( ) Bike ( ) Motorcycle ( )Does the residence have minibus to transport residents? Yes ( ) No ( )Is the transport shared with other residence facility? Yes ( ) No ( )How long does it take to get to day hospital / centre by minibus / public transport? _______________
RULES & REGULATIONSDo residential staff supervise daytime comings and goings of residents? Yes ( ) No ( )Are residents allowed to leave the unit unsupervised? Yes ( ) No ( )Do residents have a front door key? Yes ( ) No ( )Can residents lock bathroom facilities? Yes ( ) No ( )Are visiting hours scheduled? Yes ( ) No ( )Are residents required to go to bed at a given time? Yes ( ) No ( )Do staff run a check to make sure that residents are in their bed? Yes ( ) No ( )Are residents required to be up at a given time?a) Weekdays Yes ( ) No ( )b) Weekend, holiday and bank holiday Yes ( ) No ( )When checking out - are residents required to notify staff where they go? Yes ( ) No ( )Are residents required to check in at a given time? Yes ( ) No ( )Can residents stay in their bedrooms during the day? Yes ( ) No ( )Can residents lock their bedrooms? Yes ( ) No ( )Are residents allowed to smoke in their bedrooms? Yes ( ) No ( )Are there any areas where residents can be left on their own? Yes ( ) No ( )Can residents choose whom they share their bedrooms with? Yes ( ) No ( )Can residents choose to stay in single rooms? Yes ( ) No ( )The following items are allowed:Razor, knife, scissor Yes ( ) No ( )Matches, lighters Yes ( ) No ( )Medication Yes ( ) No ( )Money Yes ( ) No ( )Do staff run a check on residents’ belongings? Yes ( ) No ( )Are residents’ belongings listed? Yes ( ) No ( )Can residents administer their own finances?Yes( ) Some ( ) No ( )
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 147

MEALS
Is the food prepared by the psychiatric hospital? Yes ( ) No ( )Who prepares the meals?
Weekdays WeekendsResidents ( ) ( )Staff ( ) ( )Residents and Staff ( ) ( )Kitchen Staff ( ) ( )
Number of residents having their main meals outside residence( )Do staff have their main meals in residence? Yes ( ) No ( )Can residents choose the menu? Yes ( ) No ( )Can residents follow a diet? Yes ( ) No ( )Do residents purchase/ shop for the food? Yes ( ) No ( )Do residents have unrestricted access to the kitchen? Yes ( ) No ( )
STAFF
Number of daily working hours in residence ( )Number of staff for each scheduled shiftHours Nurses Care staff Household Others8am-14pm14pm-20pm20pm-8amVisit dailyVisit weekly
Do named core staff, staff this residence? Yes ( ) No ( )
Do staff rotate at set intervals? Yes ( ) No ( )If so, is it 6 Months ( ) Yearly ( ) 2 years ( )
Is there an emergency call service in place during night shifts for the residence or group of residences?Yes (doctor-on- call) ( ) Yes (staff-on-call) ( ) No ( )
Does emergency call run for 24 hours including Saturdays? Yes ( ) No ( )Does emergency call run for 24 hours on Sundays and public holidays? Yes ( ) No ( )Are there volunteers and/or trainees on placement? Yes ( ) No ( )
ADMISSION PROCEDURES
Is there a formal assessment prior to admission?Yes formally structured ( ) Yes but not formally structured ( ) No ( )
How many places are there in the residence? ( )Are there any designated
Respite beds ( )Crisis beds ( )Beds for other uses (please specify) ______________________________________
Is the residence ever used to accommodate transfers fromthe acute unit due to bed shortages? Yes ( ) No ( )If applicable, is there a policy regarding the following admissions?
Respite beds Yes ( ) No ( )Crisis beds Yes ( ) No ( )Transfers from acute units due to bed shortages Yes ( ) No ( )
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND148

Which, if any, criteria are used as exclusion criteria?Acute psychotic disorders Yes ( ) No ( )Substance abuse (history) Yes ( ) No ( )Alcohol abuse Yes ( ) No ( )Severe physical disease Yes ( ) No ( )Organic brain disorder Yes ( ) No ( )Intellectual disability Yes ( ) No ( )History of violent behaviours Yes ( ) No ( )Former residents of psychiatric hospitals Yes ( ) No ( )Former residents of criminal psychiatric hospital Yes ( ) No ( )
Is there a waiting list? Yes ( ) No ( )If yes,
Number of week ( )Number of applications ( )
Is there a specialised rehabilitation team for the service? Yes ( ) No ( )If so, does it have ownership of beds? Yes ( ) No ( )If not, who has ownership of beds (please specify)? ________________________________________Who decides on the placement, discharge or transfer of patients?Specialised rehabilitation team Yes ( ) No ( )Individual’s care team Yes ( ) No ( )Specialised rehabilitation team and patients own care team Yes ( ) No ( )Other, please specify ______________________________________________________________If there is a specialised rehabilitation team is it multidisciplinary? Yes ( ) No ( )If so, what professionals are included:Psychiatrist Yes ( ) No ( )Mental health nurse Yes ( ) No ( )Clinical psychologist Yes ( ) No ( )Social worker Yes ( ) No ( )Occupational therapist Yes ( ) No ( )Other _______________________________________________________________Is there a provisional admitting diagnosis drawn up once a patient has been admitted?Yes one week to one month ( ) Yes one to three months ( ) Yes less than three months ( ) No ( )
Does each resident have an individual treatment plan with a clear aim? Yes ( ) No ( )
Does the treatment plan include the following (please tick all appropriate boxes)The specific medical treatment Yes ( ) No ( )The responsibilities of each member of the treatment team Yes ( ) No ( )Adequate documentation to justify the diagnosis Yes ( ) No ( )The treatment and rehabilitation activities carried out Yes ( ) No ( )
Are treatment plans reviewed by those responsible for the care of the resident? Yes ( ) No ( )
Is there an admission form to be singed by the resident or/and family members containing details ontreatment goals and residential unit process and procedures? Yes ( ) No ( )
Is there a qualified professional assigned to each resident thatone can refer to throughout treatment? Yes ( ) No ( )
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 149

MEETINGS
Are there planned and regular meetings held by staff within the residence? Yes ( ) No ( )If yes how often are they held?Daily ( ) Weekly ( ) Every quarter ( ) Every month ( ) Very seldom ( ) None planned ( )
Are there meetings between the specialised rehabilitation team andresidential staff? Yes ( ) No ( )If so, how often are they held?Daily ( ) Weekly ( ) Every quarter ( ) Every month ( ) Very seldom ( ) None planned ( )
Are there meetings to discuss treatment and the resident’s response to treatment? Yes ( ) No ( )
Are there meetings open to residents to discuss the hostel’s organisation andprocedures? Yes ( ) No ( )If yes, how often are they held?Daily ( ) Weekly ( ) Every quarter ( ) Every month ( ) Very seldom ( ) None planned ( )
Are there meetings for relatives and families of each resident? Yes ( ) No ( )If yes how often are they held?Daily ( ) Weekly ( ) Every quarter ( ) Every month ( ) Very seldom ( ) None planned ( )
Are there meetings where families of residents can attend together? Yes ( ) No ( )If yes how often are they held?Daily ( ) Weekly ( ) Every quarter ( ) Every month ( ) Very seldom ( ) None planned ( )
EVALUATION PROCESS and PROCEDURES
Is an annual planning report compiled by the residential unit? Yes ( ) No ( )
Is there an evaluation plan underlining the hostel’s quality services and control? Yes ( ) No ( )
If yes please specify?Performance indicators monitoring system Yes ( ) No ( )Clinical Evaluation of medical conditions examined by using designated evaluation tools Yes ( ) No ( )Surveillance of certain situations or problematic situations Yes ( ) No ( )Evaluating residents satisfaction Yes ( ) No ( )Evaluating residents’ family satisfaction Yes ( ) No ( )Integrated Evaluation within programmes jointly coordinated with other services Yes ( ) No ( )
Is there a standard clinical and psychosocial evaluation procedure to assess residents? Yes ( ) No ( )
If yes, please give details _______________________________________________________
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND150

SYSTEM FILES and REGULATION
Are there guidelines or/and regulation in respect of dangerous situation staff maybe dealing with, i.e. aggressive behavior; harassment; etc.? Yes ( ) No ( )Is there Health and Safety Policy in the workplace? Yes ( ) No ( )Is there an electronic fire alarm system in place? Yes ( ) No ( )Is there documentation on intervention programmes offered by the hostel available for residents to consult? Yes ( ) No ( )Is there a procedure to take into account residents and families feedback? Yes ( ) No ( )Is there an information protection act to safeguard confidentiality or/and afreedom of information act for admistration staff when they may have todisclose information to a relative or a representative without prior patient consent? Yes ( ) No ( )Is an information pack given to residents on admission(residence rules and regulations of residence, policies and procedures booklet)? Yes ( ) No ( )Are residents given information on emergency telephone numbers? Yes ( ) No ( )Are the emergency telephone numbers posted? Yes ( ) No ( )Are residents given information on rights? Yes ( ) No ( )Are residents provided with information on the complaints procedure? Yes ( ) No ( )Are residents told the name of the local complaints officer? Yes ( ) No ( )Are residents informed of the Mental Health Commission (including role and function in mental health services)? Yes ( ) No ( )Are notices concerning rights and complaints displayed on the walls Yes ( ) No ( )Are residents asked if they wish to vote, and assisted in voter registration and voting, as necessary Yes ( ) No ( )Are residents informed of national health initiatives (e.g. breast screening, smoking cessation) Yes ( ) No ( )If so, what information is provided (please specify) _____________________________________________
Residents Characteristics
Number of residents ( )Total men
18 – 25 years ( )26 - 35 years ( )36 - 45 years ( )46 - 55 years ( )56 - 65 years ( )>65 years ( )
Total women 18 – 25 years ( )26 - 35 years ( )36 - 45 years ( )46 - 55 years ( )56 - 65 years ( )>65 years ( )
Number of residents that have been admitted since…< 6 months ( )6-12 months ( )13-36 months ( )≥ 36 months ( )
Have any residents been discharged in the last 12 months? Yes ( ) No ( )
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 151

Please specify where residents (number) went after discharge: Other health unit with higher support ( ) Other health unit with same level support ( )Other health unit with lower support ( )Hospice ( )Family ( )Home ( )Other, please specify...........................................
Have any residents been re-admitted after being discharged during last year? Yes ( ) No ( )If yes, how many ( )How many residents attend a day centre / hospital? ( )How many residents are in full-time sheltered employment? ( )How many residents are in full-time supported paid employment? ( )How many residents are in part-time supported paid employment in the community? ( )
Please complete the number of residents with a primary diagnosis of:
Primary Diagnosis Number of residentsOrganic categorySchizophreniaOther psychosisDepressive disordersManiaNuerosisPersonality disorderAlchol disordersDrug dependanceMental handicap
How many residents have a comorbid alcohol disorder _______________How many residents have a comorbid drug dependence _______________
Does your service provide the following activities for residents? If so, please indicate the providers ofthe activity and where the activity occurs (*Inside residence refers to activities held in theresidence. Outside residence refers to those held outside the residence). You can tick more thanone box if necessary.
Activity Provider of activity Location *(Please tick) (please tick)
Vocational training |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) ______________
Sheltered work |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) ______________
Supported work in community |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) ______________
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND152

Cognitive behavior therapies |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) _____________
Practical living skills |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) ____________
Social skills |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) _______
Budgeting skills |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) _______________
Physical activities |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) _______________
Alcohol / addiction counseling |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) _______
Family education, support, |__| Nurse Inside residence ( )counselling |__| Occupational therapist Outside residence ( )
|__| Social groups, volunteers, Other (specify) _____________
Leisure activities |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) _____________
Other (please specify, if applicable) |__| Nurse Inside residence ( )|__| Occupational therapist Outside residence ( )|__| Social groups, volunteers, Other (specify) _____________
Physiotherapy |__| Physiotherapist Inside residence ( )Outside residence ( )
Activities Activity Provision Organiser:
Please tickTo initiate activities that would yes |__| |__| Nurseinvolve members of the community no |__| |__| Occupational therapist
|__| Social groups, volunteers, familyOther (please specify) ____________________________
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 153

Promote participation in integratedsocial activities with the community no |__| |__| Occupational therapist
|__| Social groups, volunteers, familyOther (please specify)
____________________________
Promote participation in events yes |__| |__| Nurseorganized by community groups no |__| |__| Occupational therapist
|__| Social groups, volunteers, familyOther (please specify)
__________________________________
Facilitate residents going back to yes |__| |__| Nursework informally to help improve no |__| |__| Occupational therapistsocial integration |__| Social groups, volunteers, family
Other (please specify) ________________________________
Facilitate residents finding work yes |__| |__| Nursethrough employment agency, regional no |__| |__| Occupational therapistand local enterprise agencies |__| Social groups, volunteers, family
Other (please specify) ________________________________
Facilitate re-housing yes |__| |__| Nurseno |__| |__| Occupational therapist
|__| Social groups, volunteers, familyOther (please specify)
________________________________Please indicate if the following activities occur
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND154

APPENDIX 2Residents Questionnaire

Site _______________ Resident ID no._____________ Gender:male ( ) Female ( )
What is your present address? _________________________________________________
How long have you lived here? _____________________________ What age are you?______________Martial status: Single ( ) Married / cohabiting ( )
Separated / Divorced ( ) Widowed ( )
Education: Some primary ( ) Completed primary ( )Some secondary ( ) Completed secondary ( )Some post secondary ( ) Certificate / Diploma ( )One or more university degrees ( ) Other ______________________________________
Current employment status:
Employed full-time ( ) Employed part-time ( )Unemployed ( ) Homemaker ( )Study / ( ) Retired ( )Sheltered employment ( ) Training ( )Other ___________________
Occupation (if unemployed or retired, what was previous occupation); _________________
Do you wish to stay in your current accommodation? Yes ___ No ___
If you had a choice, where would you like to live? _____________________________
Do you attend any of the following activities in the community?Social clubs Yes ___ No ___Bingo Yes ___ No ___Community centres Yes ___ No ___Pubs / clubs / restaurantsYes ___ No ___Leisure centres Yes ___ No ___Library Yes ___ No ___Cinema Yes ___ No ___Religious worship Yes ___ No ___
Other, please specify
Do you know how much money you receive per week? Yes ___ No ___Do you receive help with your finances? Yes ___ No ___Do you vote? Yes ___ No ___Do you visit the GP by yourself? Yes ___ No ___Do you go out on your own? Yes ___ No ___
Have you ever experienced harassment in the community (verbal abuse, physical abuse) Yes ___ No ___
If so, could you describe (type of harassment, who committed it, why it occurred, to whom was itreported, how did it make you feel, did it stop you from using community facilities)
Appendix 2
Residents questionnaire
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND156

If yes, is the harassment continuing?Yes ____No ____Occasionally ____
Did you experience any of the following feelings?Adverse effect on mental health Yes ____ No ___Anger and annoyance Yes ____ No ___Fear Yes ___ No ___
YOUR TREATMENT AND CARE
Below are some statements about how you are getting on with psychiatrist and key worker and if youhave all the information you need about your treatment and care. From these questions we will be ableto gain an idea of how satisfied residents are with the care they receive. Your comments on thisquestionnaire and all others will be treated in the utmost confidence and will not be shown to any ofthe doctors or nurses. I will be the only one to see your responses. I will read out the statements to youand please respond to the questions by answering yes, not sure or no. (tick appropriate box and repeatanswer options to participant when necessary)
Yes Not Notsure
Your care planI know what my care plan isI was involved in drawing up my care planMy care plan has been explained to meI know what my medication is forI know about the possible side effects of my medicationI know when my care plan is going to be reviewed
The help you receive from your key workerThe term ‘key worker’ has been explained to meI know the name of my key workerMy key worker has explained to me their view of my problemsMy key worker is helping me to cope with my mental health problemsIf I have a problem I can easily contact my key workerMy key worker helps me with practical problemsI can easily talk about my personal problems with my key workerMy key worker lets my GP know how I am getting onI can always rely on my key worker to show up at arranged timesMy key worker helps make sure I keep my appointments with the psychiatristMy key worker makes sure I am alright if I don’t turn up for an appointment
The help you receive from your psychiatristMy psychiatrist has explained my problems to meI can easily talk about my personal problems with my psychiatristMy psychiatrist is helping me with my mental health problemsMy psychiatrist keeps me informed about my progressMy psychiatrist has explained how my problems affect my life
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 157

These are more general questions (read out responses and tick appropriate one)
How happy are you with the treatment and care you have received?
Very happy Quite happy Not very happy Not at all happy
How much information have you received on your problems?
None A little Would like more Enough
PERCEPTIONS OF LIFE IN THE RESIDENCE The following are a list of questions regarding various aspects of life in this house. When answering thequestion please think of how you feel generally. I will read you a number of options and you tell mehow you usually feel (show flashcard 3).
How good do you think it is to live here in this house?1 - Not good at all 2 - good sometimes 3 – good most of the time 4 - Great
How good is the atmosphere around the house?1 - Not good at all 2 - good sometimes 3 – good most of the time 4 - Great
How well do the people who live here get on with each other?1 - Not at all well 2 - well sometimes 3 - well most of the time 4 -Extremely well
How well do the people who live here get on with the staff?1 - Not at all well 2 - well sometimes 3 - well most of the time 4 -Extremely well
Do you ever feel bored during the weekdays or evenings?1 - All of the time 2 - sometimes 3 - most of the time 4 - Never
Do you ever feel bored at weekends?1 - All of the time 2 - sometimes 3 - most of the time 4 - Never
How much say do you have in the day-to-day running of the house?1 - None 2 - little 3 - moderate 4 - A lot
How happy are you with your involvement in the running of the residence? 1 - Not at all happy 2 - slightly happy 3 – happy most of the time 4 -Very happy
How much input do you have with regard to your treatment?1 - None at all 2 - little input 3 - moderate amount 4 - A lot of input
How much control do you feel you have to lead your own life as you want?1 - None at all 2 - little control 3 - moderate control 4 - A lot
How happy are you with your level of independence?1 - Not at all happy 2 - slightly happy 3 – happy most of the time 4 -Very happy
How happy are you with your involvement in the community?1 - Not at all happy 2 - slightly happy 3 – happy most of the time 4 -Very happy
Satisfaction for Life Domains Scale - Quality of LifeThe following questionnaire is designed to gather information on how satisfied you are with
specific aspects of your life. You are to answer these questions using one of these answers(show flashcard 4) – mostly not satisfied, mixed feelings – about equally satisfied andnot satisfied, mostly satisfied. Are you ready?
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND158

How do you feel about:
DISABILITY ASSESSMENT SCHEDULE (WHO DAS II)
This interview is about difficulties people have because of health conditions. (show flashcard1). By health conditions I mean diseases or illnesses, other health problems that may be short orlong lasting injuries, mental or emotional problems and problems with alcohol or drugs. Keep allyour health problems in mind as you answer the questions. When I ask you about difficulties indoing an activity think about Increased effort, discomfort or pain, slowness or changes in theway you do the activity (point to flashcard 1). Think over the past 30 days when answering thequestions and respond using the following scale (show flashcard 2).
The place you live?The area you live in?Your food?Your clothes?Your health?People you live with?Your friends?Your love life?Relationship with your family?The way you get along with others?The way people in your neighbourhoodtreat you?Your activities?The way you use your leisure time?What you do outside for your leisure?Services and facilities in your area?Your finances?Your drug treatment?Your life in general?
Mostly dissatisfied Mixed – about Mostly satisfiedequally satisfiedand dissatisfied
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 159

Standing for long periods such None Mild Moderate Severe Extreme / cannot doas 30 minutes?
Taking care of your household None Mild Moderate Severe Extreme / cannot doresponsibilities?
Learning a new task, None Mild Moderate Severe Extreme / cannot dofor example, learning how toget to a new place?
How much of a problem did you None Mild Moderate Severe Extreme / cannot dohave in joining in communityactivities (for example, festivities,religious or other activities) in thesame way as anyone else can?
How much have you been None Mild Moderate Severe Extreme / cannot doemotionally affected by yourhealth problems?
Concentrating on doing None Mild Moderate Severe Extreme / cannot dosomething for ten minutes?
Walking a long distance such None Mild Moderate Severe Extreme / cannot doas a mile?
Washing your whole body? None Mild Moderate Severe Extreme / cannot do
Getting dressed? None Mild Moderate Severe Extreme / cannot do
Dealing with people you do None Mild Moderate Severe Extreme / cannot donot know?
Maintaining a friendship? None Mild Moderate Severe Extreme / cannot do
Your day to day work / training? None Mild Moderate Severe Extreme / cannot do
In the last 30 days, how much difficulty did you have in:
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND160

MANNHEIM INTERVIEW ON SOCIAL SUPPORT
I am going to ask you some questions about family and friends that you have incertain situations.
SECTION A. Everyday Psychological Support:
Whom do you like to do things with?For example, go for a walk, go for a drink, play sportWith whom do you like to talk about things that interests you, such as everyday events, TV,family and son on?
Nursing/care staff Other residents
Family/ friends outside hostel
SECTION B. Everyday Instrumental Support:
If you had to asked someone a small favour, for example to lend you something, to helpout with small household repairs or do some shopping for you, whom could you turn to?
Nursing/care staff Other residents
Family/ friends outside hostel
SECTION C. Instrumental Crisis Support:
If you had to make a very important personal decision, for example about moving toanother house. With whom could you discuss your decision with?
Nursing/care staff Other residents
Family/ friends outside hostel
SECTION D. Psychological Crisis Support:
Imagine a very close friend or relative is about to die or has died and you just need to talkabout it to someone. Whom could you turn to?
Nursing/care staff Other residents
Family/ friends outside hostel
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 161

Brief Psychiatric Rating Scale
Instructions: This form consists of 24 symptom constructs, each to be rated on a 7-pointscale of severity ranging from not present to extremely severe. If a specific symptom is notrated, mark NA (not assessed). Circle the number headed by the term that best describesthe patient’s present condition. The time frame for the interview questions is 2weeks. The time frame for the observational questions is the interview periodonly. Say to participant; I am going to ask you some questions to do with symptoms, thatwe ask everyone. When answering the questions, please think of your experiences over theover the last 2 weeks.
NA 1 2 3 4 5 6 7Not Not Very Mild Moderate Moderately Severe Extremelyassessed present mild Severe
Somatic concer NA 1 2 3 4 5 6 7Anxiety NA 1 2 3 4 5 6 7Depression NA 1 2 3 4 5 6 7Guilt NA 1 2 3 4 5 6 7Hostility NA 1 2 3 4 5 6 7Suspiciousness NA 1 2 3 4 5 6 7Unusual thought content NA 1 2 3 4 5 6 7Grandiosity NA 1 2 3 4 5 6 7Hallucinations NA 1 2 3 4 5 6 7Disorientation NA 1 2 3 4 5 6 7Conceptual disorganization NA 1 2 3 4 5 6 7Excitement NA 1 2 3 4 5 6 7Motor Retardation NA 1 2 3 4 5 6 7Blunted Effect NA 1 2 3 4 5 6 7Tension NA 1 2 3 4 5 6 7Mannerisms & posturing NA 1 2 3 4 5 6 7Uncooperativeness NA 1 2 3 4 5 6 7Emotionally withdrawn NA 1 2 3 4 5 6 7Suicidality NA 1 2 3 4 5 6 7Self-neglect NA 1 2 3 4 5 6 7Bizarre NA 1 2 3 4 5 6 7Elated mood NA 1 2 3 4 5 6 7Motor hyperactivity NA 1 2 3 4 5 6 7Distractibility NA 1 2 3 4 5 6 7
Can you tell me a bit about what it is like to live here?
Prompts – What are the best bits about living here? What are the worst bits about living here?What would improve living here?Focus other prompts on issues raised.Where do you see yourself living in the future?What are your hopes for the future?
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND162

Appendix 3Keyworker Questionnaire

Site ID ________ Resident ID no. ________ Gender: Male Female
Former place of residence immediately prior to admission to current residence:
Home High support facilityMedium support facility Low support facilityPsychiatric hospital Central Psychiatric hospitalAcute psychiatric unit PrisonNo fixed dwelling
If answer ‘Home’ who was the person living with?
Alone Spouse / partnerPartner and children ChildrenParents Other relativesFriends
Income:Disability pension SalaryOther Specify __________________
Psychiatric History:
Date accepted / transferred to residence ____/_____/_____/
Approximate duration of illness in years ________________
Age of first contact with psychiatric services __________
Previous inpatient hospitalisation yes noInpatient hospitalisation while a resident yes no
Duration of last inpatient hospitalisation ____________________
Reason for last inpatient admission:
Recurrence of symptoms Depression / suicidal ideasUnable to cope Behavioural problemsOther If other, please specify _______________________
Number of inpatient admissions in the past five years __________
Degree of symptoms in the last five years:Absence of symptoms Single episode / complete remission Numerous episodes /
Appendix 3
Keyworker questionnaire
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND164

complete remission Numerous episodes/ partial remissionSymptoms persistent /stable Symptoms persistent /
progressive deteriorationType of symptoms in the last five years:
Psychotic (positive / negative) Affective (depressive /manic)
Obsessive / compulsive Other _____________________________________
Currently receiving pharmacological treatment yes no
If currently receiving medication please enter drug trade name, route dosage:
Drug Route of administration Dosage (mg)
Please indicate the substances used in the past year using the following key:
0 = no use1 = infrequent (1 – 10 times)2 = occasionally (11 = 20 times)3 = frequent (21 – 100 times in the year, but not every day)4 = every day or nearly every day5 = dependent on substance
Substance Frequency Alcohol intakeCannabis / marijuana/ hashishStimulants (amphetamines, ecstasy, etc.) Opiates (heroin, morphine, etc.)Tobacco (number of cigarettes, cigars per day)
Does this person have an alcohol abuse / misuse problem Yes ( ) No ( )Does this person have a drug abuse / dependence problem Yes ( ) No ( )
System of support in the last year:
Family, friends or other interested in resident and willing to provide supportFamily, friends or other interested in resident, but have doubts about ability to provide support
Potential for providing support, but severe difficulties in putting it into actionAbsence of family, friends or other to provide support
Do family / friends visit the resident? Yes ( ) No ( )Does the resident go out to visit family / friends? Yes ( ) No ( )
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 165

Participation of the resident in activities in the residence in the last year:
Actively engages, strong motivationWants to engage, but motivation is not strongPassively engages in activitiesShows very little interest or understanding of activitiesActively refuses to participate in activities
Appropriate placement
In your opinion, is the resident appropriately placed in this residential facility Yes ( ) No ( )
If no, where do you think the resident would be more appropriately placed:Independent living:Independent group home:Rehabilitation unit: Low support home:Medium support home:High support home:Nursing home:
If the resident is inappropriately placed, what do you see are the barriers towards appropriateplacement?
Mental state or behaviour precludes discharge / transferResident refuses transferRelatives refuse transferFacility unavailableFacility available, but will not acceptFacility available, but has waiting listOther reason, please specify ______________________________________________________
Where do you see the resident living in six months time?In the same residential facility?In a higher support facility?In a lower support facility?In an independent setting?With the family?Nursing home?Other?
Global Assessment of Functioning is for reporting the clinician’s judgment of the individual’soverall level of functioning and carrying out activities of daily living. One score is given in the boxto indicate the individual’s current level of functioning. Consider psychological, social, andoccupational functioning on a hypothetical continuum of mental health-illness. Do not includeimpairment in functioning due to physical (or environmental) limitations.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND166

Code Note: One score is given to indicate current functioning. Feel free to use intermediatecodes (95, 46), e.g., if resident has superior functioning then a score somewhere between91 and 100 is given.
100 Superior functioning in a wide range of activities, life’s problems never seem to get out ofhand, is sought out by others because of his or her many positive qualities. No symptoms.
9190 Absent or minimal symptoms, good functioning in all areas, interested and involved in a
wide range of activities, socially effective, generally satisfied with life, no more thaneveryday
81 problems or concerns (e.g., an occasional argument with family members.)80 If symptoms are present, they are transient and expectable reactions to psychosocial
stressors (e.g., difficulty concentrating after family argument); no more than slightimpairment in social,
71 occupational, or school functioning.70 Some mild symptoms (e.g., depressed mood and mild insomnia) OR some difficulty in
social, occupational, or school functioning, BUT generally functioning pretty well and hassome
61 meaningful interpersonal relationships.60 Moderate symptoms (e.g. flat affect and circumstantial speech, occasional panic attacks)
OR moderate difficulty in social, occupational, or school functioning5150 Serious symptoms (e.g., suicidal ideation, severe obsessional rituals, frequent shoplifting)
OR any serious impairment in social, occupational, or school functioning (e.g., few friends,unable to keep a job)
4140 Some impairment in reality testing or communication (e.g., speech is at times illogical,
obscure, or irrelevant) OR major impairment in several areas, such as work or school,family relations, judgment, thinking, or mood (e.g., depressed man avoids friends, neglectsfamily, and is unable to
31 work).
30 Behaviour is considerably influenced by delusions or hallucinations OR serious impairmentin ı communication or judgement (e.g., sometimes incoherent, acts grossly inappropriately,suicidal preoccupation) OR inability to function in almost all areas (e.g., stays in bed allday; no job, home or
21 friends).
20 Some danger of hurting self or others (e.g., suicide attempts without clear expectation ofdeath;frequently violent manic excitement) OR occasionally falls to maintain minimal personalhygiene
11 OR gross impairment in communication (e.g., largely incoherent or mute)
10 Persistent danger of severely hurting self or others (e.g., recurrent violence) OR persistentinability to maintain minimal personal hygiene OR serious suicidal act with clearexpectation
1 of death0 Inadequate information
Insert score here
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 167

Physical Health Index
Please rate the disabilities in the following areas and the amount of assistance required, ifapplicable
Disabilities Key0 = no disability, 1 = mild disability, 2 = moderate disability, 3 = severe disability
Assistance Key0 = absence of meaningful pathology / does not need medical attention for this problem, 1 =assume daily therapy without surveillance, 2 = has regular appointments with the GP, 3 = hasregular appointments with the hospital specialist, 4 = assumes daily therapy under surveillance, 5= followed regularly but not daily by nursing staff, 6 = followed daily by nursing staff, 7 =followed daily to medical level.
Cardiovascular = to include congenital, ischemic and cardiac valve pathologies, peripheralhypertension and vascular pathologies.
Respiratory = to include conditions like asthma and chronic obstructive pathology.
Digestive = to include gastrointestinal problems including faecal incontinence of any aetiology.
Urogential = to include the urinary incontinence of any aetiology.
Motor = to include motor deficits of any aetiology except that of neurological causes.
Central nervous system = to include particular feelings, epilepsy, the presence of inducedtremors or less from substances, and or motor deficits of neurological causes.
Metabolic endocrine system = to include blood diseases, allergic disturbances (reactions),abnormal height / weight relationships, and dermatological problems.
Cardiovascular 0 1 2 3 0 1 2 3 4 5 6 7Respiratory 0 1 2 3 0 1 2 3 4 5 6 7Digestive 0 1 2 3 0 1 2 3 4 5 6 7Urogential 0 1 2 3 0 1 2 3 4 5 6 7Motor 0 1 2 3 0 1 2 3 4 5 6 7Central nervous system 0 1 2 3 0 1 2 3 4 5 6 7Metabolic endocrine system 0 1 2 3 0 1 2 3 4 5 6 7Infective (including HIV) 0 1 2 3 0 1 2 3 4 5 6 7
Disability Assistance required
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND168

Health of the Nation Outcome Scales (HoNOS)
Please circle ONE number for each symptom as appropriate. Rate 9 if not known. Please base theratings on the previous two weeks.
1. Overactive, aggressive, disruptive or agitated behaviour 0 1 2 3 4Include such behaviour to any cause (drugs, alcohol, dementiapsychosis, depression ect.)Do not include bizarre behaviour rated in scale 6.
2. Non-accidental self injury 0 1 2 3 4Do not include accidental self-injury due to dementia orsevere learning disability.
3. Problem drinking or drug taking 0 1 2 3 44. Cognitive problems 0 1 2 3 4
Include problems of memory, orientation, and understandingassociated with any disorder: learning disability, dementia, schizophrenia etc.
5. Physical illness or disability problems 0 1 2 3 4Include illness or disability from any cause. Include side-effectfrom medication.
6. Problems associated with hallucinations and delusions 0 1 2 3 4Include hallucinations, delusions and odd or bizarre behaviourassociated with hallucinations or delusions.
7. Problems with depressed mood 0 1 2 3 48. Other mental or behavioural problems 0 1 2 3 49. Problems with relationships 0 1 2 3 410. Problems with activities of daily living include problems
with basic activities or self-care. Also include complex skills such as budgeting, organisation, shopping, occupation etc. 0 1 2 3 4
11. Problems with occupation and activities 0 1 2 3 4Rate the overall level of problems with quality of day-timeenvironment. Is there help to cope, opportunities for maintaininand improving occupational and recreational skills and activities?
Consider factors such as stigma, lack of qualified staff, staffing andequipment of day centres, workshops and social clubs.
Disability Assessment Schedule (WHO DAS II)
This questionnaire asks about difficulties due to health conditions. Health conditions includedisease or illness, other health problems that may be short or long lasting, injuries, mentalor emotional problems, and problems with alcohol or drugs.
Think back over the last 30 days and answer these questions thinking about how much difficultythe individual had doing the following activities. Difficulties refer to increased effort,discomfort or pain, slowness or changes in the way they do something. For each question,please circle only one response.
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND 169

Is there anything else that you would like to elaborate on in relation to this person? For example,their placement, the treatment and care or clinical or social functioning. Or on factors thatpromote or impede the individual from achieving their optimal level of functioning? Is thereanything else you would like to elaborate on in relation to the roles or functions of theresidence?
Standing for long periods such as 30 None Mild Moderate Severe Extreme / cannot dominutes?
Taking care of his / her household None Mild Moderate Severe Extreme / cannot doresponsibilities?
Learning a new task, for example, None Mild Moderate Severe Extreme / cannot dolearning how to get to a new place?
How much of a problem did he / she None Mild Moderate Severe Extreme / cannot dohave in joining in community activities(for example, festivities, religious orother activities) in the same way as anyone else can?
How much has he /she been emotionally None Mild Moderate Severe Extreme / cannot doaffected by his / her health problems?
Concentrating on doing something None Mild Moderate Severe Extreme / cannot dofor ten minutes?
Walking a long distance such as a mile? None Mild Moderate Severe Extreme / cannot do
Washing his / her whole body? None Mild Moderate Severe Extreme / cannot do
Getting dressed? None Mild Moderate Severe Extreme / cannot do
Dealing with people he / she does None Mild Moderate Severe Extreme / cannot donot know?
Maintaining a friendship? None Mild Moderate Severe Extreme / cannot do
His / her day to day work / training? None Mild Moderate Severe Extreme / cannot do
In the last 30 days, how much difficulty did this individual have in:
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND170

Appendix 4Staff Questionnaire

The following staff schedule is designed to gather information on a sample of staff within theresidence. One schedule is to be completed for each member of staff selected. The first part ofthe schedule is designed to gather demographic data. Following this information will be collectedon beliefs about aims and functions of the residences and factors that impede or promoteindependent living for the residents.
STAFF SCHEDULE
Site ID _________ Gender: Male Female
For how long have you been employed as a mental health professional (in years)?_____________________
How long have you been in your current post in this residence?___________________________________________
Which of the following best describes your occupation? (please tick)
Mental Health NurseCare workerNursing assistantCare assistantDomestic staff
Other, please describe _______________________________________________
Which of the following best describes your post in the team?Permanent contractBank staffAgency employedStudent placement
Other, please describe _________________________________________________
Are you employed Full-time Part-time Other
AIMS AND FUNCTIONS OF THE HOSTEL
Please rate the aims and functions of your hostel according to the following key:1 = no importance; 2 = moderate importance; 3 = great importance; 4 = greatest importance
Service to shorten inpatient treatment 1 2 3 4Alternative to inpatient care 1 2 3 4Failure of outpatient care/ day care/ home care 1 2 3 4Crisis intervention 1 2 3 4Rehabilitation to independent living / lower level of support 1 2 3 4Psychosocial rehabilitation and support 1 2 3 4Home for life 1 2 3 4Respite care 1 2 3 4
Other (please elaborate) ___________________________________________________________________________________What are the three main factors that you perceive promote independent behaviour in individuals
with mental illness?
___________________________________________________________________________________What are the three main factors that you perceive impede independent behaviour in individuals
with mental illness?
Appendix 4
Staff questionnaire
A SURVEY AND EVALUATION OF COMMUNITY RESIDENTIAL MENTAL HEALTH SERVICES IN IRELAND172




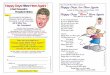












![Living Happy Without Religion [TEDxEdges 2011]](https://img.pdfslide.us/doc/110x75/54c917d14a79591a728b45fb/living-happy-without-religion-tedxedges-2011.jpg)