Embed Size (px)
Citation preview
HANNAH TOWERCONCORDIA COLLEGE
MOORHEAD, MN
Nutrition Implications of Starvation and Refeeding
Syndrome
Objectives
Describe the pathophysiology of starvation and refeeding syndrome (RFS)
Explain and identify signs and symptoms along with risk factors of starvation and RFS
Be able to recognize a patient at risk of starvation and RFS
Describe the medical nutrition therapy (MNT) for starvation and RFS
Describe ways to prevent starvation and RFS
What is RFS?
Term used to describe several metabolic alterations that occur during nutritional repletion of starved patients Electrolyte depletion Fluid shifts Glucose derangements
Can occur when reinstating nutrition orally, enterally, or parenterally
It was first reported among those released from concentration camps after WWII
- Long, S., Nelms, M., & Suchner, K. (2007). - Marinella, M. A. (2003).
Pathophysiology: Early Fasting State
Tissues cannot get their energy from ingested glucose and other macromolecules Glycogenolysis
Gluconeogenesis assists in maintaining blood glucose levels
Glucose from the liver to the muscles comes from the recycling of lactate and glycogenolysis
Rate of glucose use is greater than production by gluconeogenesis and the stores diminish rapidly
- Gropper, S. S., Smith, J. L., & Groff, J. L. (2009).
Pathophysiology: Fasting State
- Gropper, S. S., Smith, J. L., & Groff, J. L. (2009).- Tresley, J., Sheean, P. M. (2008).
18-48 hours of no food intakeAmino acids from muscle protein breakdown
provide the main substrate for gluconeogenesis
The shift to gluconeogenesis is signaled by the secretion of glucagon
Ketogenic amino acids released by muscle protein hydrolysis are converted into ketones
Large daily loses of nitrogen in the urine
Gropper, S. S., Smith, J. L., & Groff, J. L. (2009).
Pathophysiology: Starvation State
Goal: spare body proteinFat stores main energy source The shift to fat breakdown releases large amounts of
glycerol Assure a continued supply of glucose as fuel for the brain
Eventually ketosis occurs Ketone bodies are delivered to skeletal muscle, heart, and brain
Survival time 3 months
When the fat reserves are depleted the body uses essential protein Loss of liver and muscle function and eventually death
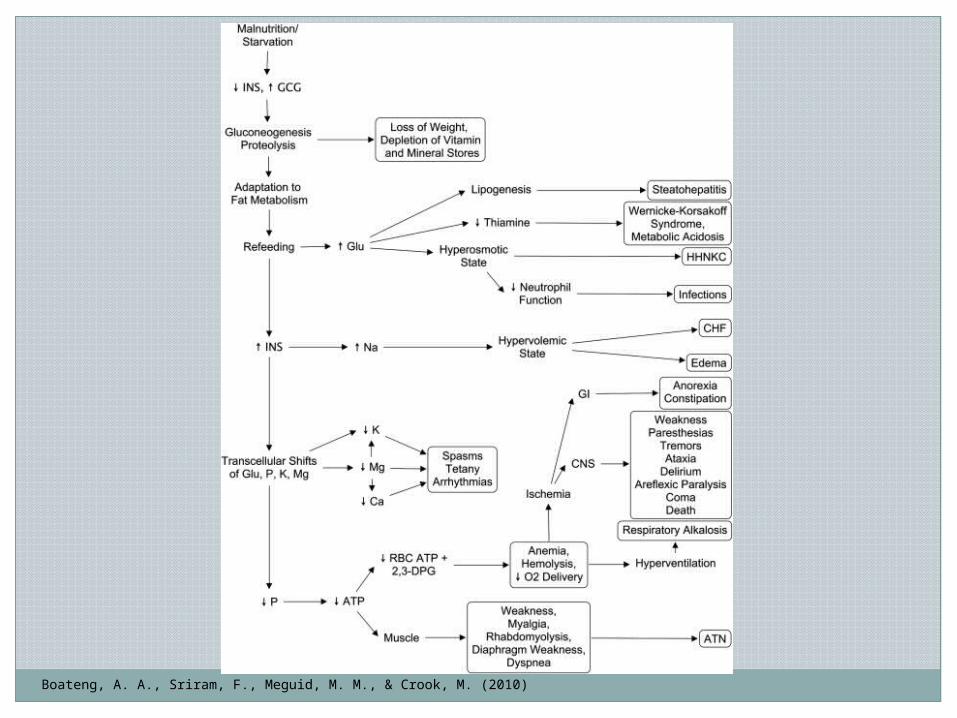
Pathophysiology of RFS
Boateng, A. A., Sriram, F., Meguid, M. M., & Crook, M. (2010)
Reintroduction of carbohydrates (CHO) causes increase in insulin production
Body fluid disturbances Fluid overload pulmonary edema
HyperglycemiaThiamin deficiencyElectrolyte depletion
Phosphate Potassium Magnesium
Boateng, A. A., Sriram, F., Meguid, M. M., & Crook, M. (2010)
Hyperglycemia
Boateng, A. A., Sriram, F., Meguid, M. M., & Crook, M. (2010).
Blood glucose level above normalResults from glucose introduction into a
starved system adopted for fat metabolismInfections are more commonThiamin deficiency
Wernicke’s encephalopathy
Thiamin Deficiency
Tresley, J., Sheean, P. M. (2008).
Thiamin is required as a cofactor in the oxidation of CHO
Wernicke’s encephalopathy Symptoms generally do not appear until refeeding of
CHO Confusion Ocular disturbances Ataxia Coma
Common in alcoholics
Hypophosphatemia
- Marinella, M. A. (2003). - Tresley, J., Sheean, P. M. (2008).
Low serum phosphate Moderate: <2.5 mg/dL Severe: <1.0 mg/dL
Caused by starvation-induced loss of lean tissue mass, minerals, and water
Transcellular shift of phosphorus and a decline in the serum phosphorus
Can lead to: Irregular heartbeat Respiratory failure Confusion
Hypokalemia
- Boateng, A. A., Sriram, F., Meguid, M. M., & Crook, M. (2010)- Tresley, J., Sheean, P. M. (2008)
Low serum potassium <2.5 mEq/L
Results from the cellular uptake of potassiumCan result in:
Paralysis Compromised respiratory system Muscle necrosis Irregular heartbeat
Hypomagnesemia
- Boateng, A. A., Sriram, F., Meguid, M. M., & Crook, M. (2010). - Tresley, J., Sheean, P. M. (2008).
Low serum magnesium <1.0 mg/dL
Results from cellular uptake of magnesium after feeding
Can result in: Convulsions Seizures
Risk Factors
- Marinella, M. A. (2003). - Tresley, J., Sheean, P. M. (2008).
Anorexia nervosa
http://www.doctortipster.com/tag/anorexia-fear
Prolonged starvation
http://poorfund.blogspot.com/2010/06/third-worldstarvation.html
Risk Factors cont.
- Marinella, M. A. (2003).
Alcoholism
http://www.drug-rehabilitation.com/alcoholism.htm
Homelessness
http://homelesschicago.wordpress.com/
Risk Factors cont.
- Marinella, M. A. (2003). The refeeding syndrome and hypophosphatemia. Nutrition Reviews, 61 (9), 320-323.
Obesity with significant weight loss
http://www.fitnessthroughfasting.com/water-fasting-for-weight loss.html
History of cancer
http://www.topnews.in/health/diseases/cancer
Risk Factors cont.
- Boateng, A. A., Sriram, F., Meguid, M. M., & Crook, M. (2010)- http://directory.ac/dr-carson-liu.html
Prolonged vomiting and diarrheaRecent major surgeryDepression in the elderlyPoorly controlled diabetesProlonged NPO statusBariatric surgery
Signs and Symptoms
- Boateng, A. A., Sriram, F., Meguid, M. M., & Crook, M. (2010)- Stanga, Z., Brunner, A., Leuenberger, M., Grimble, R.F., Shenkin, A., Allison, S.P., & Lobo, D.N. (2008).
CVS Sudden death Heart failure
GI Anorexia Abdominal pain Constipation or diarrhea Vomiting
Neurologic Tremors Coma Ataxia
Metabolic Metabolic alkalosis Metabolic acidosis Respiratory alkalosis
Respiratory Respiratory failure Ventilator dependency
Musculoskeletal Weakness Osteomalacia
Identifying Patients at a High Risk of RFS
- National Institute for Health and Clinical Excellence (NICE) (2006).
National Institute for Health and Clinical Excellence (NICE) Guidelines
Patient has one or more of the following BMI < 16 kg/m2
Unintentional weight loss > than 15% (3-6 months) Little or no nutritional intake >10 days Low levels of potassium, phosphate or magnesium
prior to feedingOR …
Identifying Patients at a High Risk of RFS cont.
- National Institute for Health and Clinical Excellence (NICE) (2006).
Patient has two or more of the following BMI < 18.5 mg/m2
Unintentional weight loss > than 10% (3-6 months) Little or no nutritional intake > 5 days History of:
Alcohol abuse Insulin Chemotherapy Antacids Diuretics
Clinical Indicators
Escott-Stump, S. (2012).
Clinical/ History Height Weight Blood pressure BMI Desirable BMI % UBW History of weight changes Tricep skin fold Diet history I & O Temperature Edema Bone pain Dizziness Diarrhea/vomiting
Lab values Serum phosphate Magnesium Potassium Glucose Sodium Cholesterol/TG Serum iron BUN
MNT for RFS
Stanga, Z., Brunner, A., Leuenberger, M., Grimble, R.F., Shenkin, A., Allison, S.P., & Lobo, D.N. (2008)
Energy intake should be instituted carefully, and gradually increased over 4-10 days
Supplementation of electrolytes and vitamins can be started before feeding
Monitor fluid administration carefully
MNT for RFS
Stanga, Z., Brunner, A., Leuenberger, M., Grimble, R.F., Shenkin, A., Allison, S.P., & Lobo, D.N. (2008).
Days 1-3 Energy: 10 kcal/kg/day (5 kcal/kg/day if BMI <14)
CHO: 50-60% Protein: 15-20% Fat: 30-40%
Electrolytes: measure daily during feeding and increase if necessary Phosphate: .5-.8 mmol/kg/day Potassium: 1-3 mmol/kg/day Magnesium: .3-.4 mmol/kg/day
Fluid: restrict to maintain renal function About 20-30 mL/kg/day
Sodium Minerals: 100% DRI Vitamins: 200% DRI
Thiamine: 200-300 mg i.v. 30 minutes prior to feeding
MNT for RFS
Stanga, Z., Brunner, A., Leuenberger, M., Grimble, R.F., Shenkin, A., Allison, S.P., & Lobo, D.N. (2008).
Days 4-6 Energy: 15-20 kcal/kg/ day
Days 7-10 Energy: 20-30 kcal/kg/day Iron: supplement after day 7
Medications
Escott-Stump, S. (2012).
Replacement of phosphorus, potassium, and magnesium if depleted
Insulin to correct hyperglycemia100 mg thiamin bolus daily for three days
Other B-complex and vitamins if needed
Current Research
- Wagstaff, G. (2011).- American Dietetic Association (2009).
No recent randomized, controlled trials exist
Ethical issuesEAL: Does serum prealbumin correlate with
weight loss in starvation? One non-randomized trial found that serum
prealbumin does not correlate with weight loss in starvation
Evidence comes from case studies, case series, and cohort studies
Current Research cont.
Wagstaff, G. (2011).
Electronic, anonymous, internet survey sent out covering current practice, perceived prevalence of refeeding risk, and opinions on the NICE guidelines. Target population: RD’s in London working with
adults Response rate: 168 RD’s, 30.8%
Current Research cont.
Wagstaff, G. (2011).
Results 89.8% have read the NICE guidelines History of nutritional intake and biochemistry are the
most important factors when treating RFS 89.5% do not wait for biochemistry to normalize before
commencing feeding 31.2% classified and fed pt. 1 according to NICE
recommendations 22.7% for pt. 2 19.5% for pt. 3
Conclusions Limited by small sample size Inconsistent dietary practices regarding refeeding
syndrome
Keys’ Study
- Franklin, J. C., Schiele, B. C. Brozek, J., Keys, A. (1945).
36 young men between the ages of 20-33 served as volunteer subjects
Study began in 1944 and lasted a yearControl data was obtained for three months
3,492 calories/daySemistarvation period for six months
Stimulate the quantity and quality of the food available in western and central Europe
1,570 calories/dayControlled rehabilitation for three months
Keys’ Study: Physical Changes
- Franklin, J. C., Schiele, B. C. Brozek, J., Keys, A. (1945).
24% body weight lossFace and body showed
great emaciationClothes and shoes too
largeMuscle wastingEdema in knees, ankles,
and facesNails grew slowerHair lossSlower wound healingMuscle cramps and
soreness
Tolerance to heat was increased
Cold body temperatureBlackouts and faintingInability to focusNauseaDecrease in pulse rateFatigue and weaknessLoss of ambitionDepressionPolyuria and nocturia
Keys’ Study: Physical Changes cont.
- http://leanmeanvirilemachine.com/2010/10/25/why-eat-less-exercise-more-doesnt-work/
Keys’ Study: Hunger and Appetite
- Franklin, J. C., Schiele, B. C. Brozek, J., Keys, A. (1945).
In total starvation the sensation of hunger rapidly disappears, not true in semistarvation
Subjects referred to sensations located in the abdomen Mild to intense pain Varied for each subject
http://www.sophisticateddorkiness.com/2010/02/review-the-great-starvation-experiment/
Keys’ Study: Eating Habits
Franklin, J. C., Schiele, B. C. Brozek, J., Keys, A. (1945).
Anticipation of eating heightened the craving for food
Each subject defensively guarded his plate
Food had to be very hot in order to be satisfying
During meals they were silent, deliberate, and gave total attention to their food
Played with their foodSpend hours eating their
meal
Saved parts of their meal for later
Taste appeal of the meals increased
Food substitution Gum chewing
Limited to two packs a day
Large amounts of water Smoking Coffee and tea
Limited to nine cups per day
Keys’ Study: Rehabilitation Phase
Franklin, J. C., Schiele, B. C. Brozek, J., Keys, A. (1945).
Purpose: measure the relative efficiency of several levels of refeeding in order to secure the most efficient, practical, and economic regimen for dietary rehabilitation
First six weeks: 2,448 caloriesSeventh to tenth weeks: 3,257 caloriesEleventh and twelfth weeks: 3,518 calories
Keys’ Study: Rehabilitation Stage cont.
- Franklin, J. C., Schiele, B. C. Brozek, J., Keys, A. (1945). -http://www.psychologytoday.com/blog/hunger-artist/201011/starvation-study-shows-recovery-anorexia-is-possible-only-regaining-weight
At the end of the 12 weeks the subjects in the highest caloric group regained <60% of the weight lost
120 calories moreLowest group
Gained no weight during the first six weeks Regained 20% of weight lost after the 12 weeks
Recovery from dizziness, apathy, and lethargy was the most rapidLittle change and some increase in edemaAppetites were insatiableFrustration with lack of strength and endurance
Prevention
- Hearing, S. D. (2004). - Marinella, M. A. (2003). - Boateng, A. A., Sriram, F., Meguid, M. M., & Crook, M. (2010).
Improve awareness General physicians, surgeons, RD’s, nurses
Recognition of patients at risk Knowing the warning signs and risk factors
Prevent the development of severe symptomsLessen the symptoms is RFS has already
developed
Role of the RD
Make recommendations for providing, withholding, or withdrawing nutrition in individual cases
Promote the right of the individual patientAssist the healthcare team in recognizing
RFS Signs and symptoms Risk factors
Case Study: Hunger Striker
- http://www.huffingtonpost.com/greg-boose/the-sign-guy-goes-on-hung_b_187190.html- Stanga, Z., Brunner, A., Leuenberger, M., Grimble, R.F., Shenkin, A., Allison, S.P., & Lobo, D.N. (2008).
27 y.o. male went on hunger strike for 4 months Refused any nourishment
Except tea and coffee with sugar Lost further 2 kg in hospital and became weaker, more inactive,
and apathetic Treated with enteral and parenteral nutrition
1600 kcal/day Gained 5 kg due to salt and water retention Hypokalemia, hypomagnesaemia, and hypophosphatemia
200 mg thiamine was administered as well as potassium phosphate for three days (40 mmol) and magnesium sulphate (20mmol)
After three days electrolyte/ mineral concentrations were in the normal range, and three days later oral nutrition was started
Discharged after 57 days
Case Study: Anorexia Nervosa
- http://www.101healthsolution.com/anorexia-nervosa/- Stanga, Z., Brunner, A., Leuenberger, M., Grimble, R.F., Shenkin, A., Allison, S.P., & Lobo, D.N. (2008).
40 y.o. woman with long standing anorexiaUpon admission
Ankle edema Hypotension Phosphate, magnesium, and potassium were low
Oral supplementation of vitamins and electrolytes Regardless she developed muscle weakness, drowsiness,
and rapid heartbeatI.V. supplements of electrolytes and minerals
Within 2 days muscle weakness and heart rate were resolved and serum electrolyte concentrations were normal
Ethical Issues
- American Dietetic Association (2008).
ADA position: individuals have the right to accept or refuse nutrition and hydration as MNT
Experiments Can’t ethically subject
people to starvation like in Key’s Study
http://www.massbar.org/for-attorneys/ethical-inquiries
Summary
Starvation is severe reduction in energy, vitamin, and mineral intake
RFS is a term used to describe several metabolic alterations that occur during nutritional repletion of starved patients
RFS is caused by rapid refeeding after a period of undernutrition
Characterized by hypophosphatemiaGradually introduce feeding





























