Embed Size (px)
Citation preview

HANGMAN’S FRACTURE
T. G. WILLIAMS, SOUTHAMPTON, ENGLAND
From the Royal South Hants Hospital, Southampton
of four hangman’s fractures of the axis, three occurred in road accidents and were stable, undisplaced
and free of neurological signs, with full recovery after six to twelve weeks in a cervical collar. The fourth
fracture occurred in a fall with profound tefraparesis from haemorrhage into the spinal cord, and the patient
died a week later. There are two types of hangman’s fracture : that of the axis pedicle, which results frommore common than usually supposed because of the
82 THE JOURNAL OF BONE AND JOINT SURGERY
extension and compression of the cervical column, is
slight symptoms it causes.
Originally described in the victims ofjudicial hanging
(Wood Jones 19 13), hangman’s fracture is sometimes seen
in orthopaedic practice after road accidents or simple
falls. A review of the literature, with four case reports,
suggests that this injury may be more common than
hitherto supposed.
Grogono (1954) noted the similarity between the
“ideal” lesion produced by hanging and the radiological
appearance of a bilateral axis pedicle fracture in a woman
with transient tetraplegia after a car accident ; he thought
cord injury a likely sequel of such fractures, but subse-
quent reports have proved otherwise. Garber (1964) pre-
sented eight cases with traumatic spondylolisthesis of the
axis and very slight neurological signs after road accidents,
and considered the lesion a distinct clinical entity which
Schneider, Livingstone, Cave and Hamilton (1965) termed
hangman’s fracture when they reported eight cases after
road accidents and gave a detailed review of the possible
judicial lesions. DeLorme (1967) analysed forty cases of
axis pedicle fracture and suggested that some were flexion
injuries. In a review of fourteen cases, ten of which were
treated operatively by dowel fusion, Cornish (1968) sug-
gested that the axis pedicle fracture in the civilian may
follow extension and compression of the upper cervical
spine. In a larger series of cervical injuries, Norrell and
Wilson (1970) treated five cases of unstable hangman’s
fracture by dowel fusion, a further seven cases being
managed conservatively. Saldeen (1967) presented a case
of hangman’s fracture with decapitation by a loose
diagonal safety belt, and Edgar, Fisher, McSweeney and
Park (1972) described a motor-cyclist who recovered from
profound tetraparesis caused by a distracted hangman’s
fracture sustained when he was caught under the jaw by
a rope across the road. Apart from these specific reports,
isolated cases have been included in larger series of
cervical injuries, such as those of Rogers (1957) and
Norton (1962).
The term hangman’s fracture has thus been used in
the literature to describe both the judicial lesion and its
exact civilian counterpart on the one hand, and the axis
pedicle fracture following road accidents or falls on the
other (Table I). The two types differ markedly in mechan-
ism, clinical features and prognosis, and the aim of this
paper is to examine these differences in the published
literature and in four new cases.
MECHANISM
Hangman’s fracture results from hyperextension of the
upper cervical spine. The axis breaks symmetrically
across its pedicles or lateral masses, and the fracture may
extend across the posterior part of the body. Contrary
to popular belief, the dens always remains intact and
never contributes to cord injury or death in this condition.
The pedicles are the thinnest part of the bony ring of the
axis, weakened by the foramen transversarium on each
side (Figs. 1 to 4). The lateral masses, bearing the
superior articular facets, each straddle the vertebral body
and the inferior facet in the lateral view (Fig. 2), and
therefore they too take the brunt of forces transmitted
through the modified upper two cervical vertebrae to the
cervical spine below (Schneider et a!. 1965). The pedicles
and lateral masses are thus at the point of greatest
leverage between the extending “cervico-cranium” (the
skull, atlas, dens and body of the axis) and the relatively
fixed lower cervical spine, to which the neural arch of
the axis is anchored by its inferior facets, stout bifid
spinous process and strong nuchal muscles (Fig. 5).
Although the true hangman’s fracture and the axis
pedicle fracture sustained in road accidents share the
same radiological appearance, the clinical features re-
viewed in Table I and summarised in Table II differ so
markedly that there must be some fundamental difference
in mechanism. Cornish (1968) suggested that the axis
pedicle fracture from road accidents, which permits
spondylolisthesis of the axis if the anterior ligament is
disrupted, is the result of extension and compression of
the upper cervical spine in contrast to the extension and
distraction which follows hanging (Figs. 6 and 7).
Fracture caused by extension and compression-Extension
of the upper cervical spine with compression may be
produced by a simple forward fall with the chin, forehead
T. G. Williams, B.A., F.R.C.S., Surgical Registrar, Ipswich Hospital, Anglesea Road, Ipswich, Suffolk, England.

Schneider et a!. (1965):“Hangman’s fracture” ; 8 cases
Outcome
Edgar et a!. (1972):1 hangman’s fracture
Cornish (1968): traumaticspondylolisthesis of the axis;14 cases
Local injury toneck and face
Motor-cyclistcaught under jawby rope
Profoundtetraparesis
Skull tractionfor 7 weeks
Slight left-sidedweakness
Vehicle passenger Sound fusion
VOL. 57-B, No. I, FEBRUARY 1975
HANGMAN’S FRACTURE 83
TABLE IREPORTED CASES OF HANGMAN’S FRACTURE
Author and his description Additional injury Cause Neurological signs Treatment
Wood Jones (191 3): The ideallesion in judicial hanging
Grogono (1954): Axis fractureresembles judicial lesion
Garber (1964): traumaticspondylolisthesis ; 8 cases
- Judicial hanging - - Death
- Head jolted in car Transient Skull traction Residual weaknessaccident tetraplegia for 6 weeks of right arm
- Road accidents None or slight Rest and traction Successful
Retropharyngeal Driver, thrown Areflexic Skull traction; Left hemiparesis
swelling marked out of car Minerva jacket
- Thrown from car Minimal Minerva jacket Symptom-free
Laryngeal injury Struck chin on - Skull traction; Symptom-freesteering wheel ; cervical brace other thanwore seat belt laryngeal problems
Fractured pelvis Driver, head-on - Delayed anterior Fusion stable
and ribs accident fusion
Multiple injuries Car accident - Halter traction Solid healing
- Driver, car - Cervical traction Symptom-free
overturned then collar
- Back-seat car - Skeletal traction; Early bony union
passenger Minerva jacketNeck and tongue Front-seat car - Skeletal traction; Not stated.
lacerated passenger cervical brace Good reduction
Saldeen (1967) - Loose seat belt (Decapitation) Death
Norrell and Wilson (1970):12 hangman’s fractures
7 cases; nil.5 cases; nil
Not stated.Not stated
Notstated(?absent)Notstated(?present)
Skull traction;dowel fusion
Successful.Sound fusion
Unstable C.5 on Domestic fall - Dowel fusion Not statedC.6 subluxation
- Bicyclist struck by Incomplete Dowel fusion Considerablecar quadriplegia recovery
Fractured spinous Fall on rocks - Dowel fusion Symptom-freeprocess of C.3
- Thrown from car - Dowel fusion Not stated
- Car passenger - Bed rest Symptom-free
- Thrown out of - Dowel fusion Osteoarthritis of
vehicle C.l on C.2
- Fall from cart - Dowel fusion Neck stiffness
Severe head injury Car driver Flaccid paresis Died from head injury 4 days later
- Car passenger - Dowel fusion Symptom-free
Fractures C.3 and Driver of - Dowel fusion Sound fusionC.6 spinous overturned carprocesses
Locked facet C.7 Road traffic Right-sided Splintage Sound fusionon T.1 accident weakness and
paraesthesiaefrom C.7 only
- Passenger, car - Dowel fusion Not statedoverturned
Fracture posterior Driver of - Dowel fusion Some stiffness (hasarch of atlas overturned car rheumatoid arthritis)
- Splint

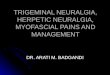
FIG. 1 FIG. 2
Cervico-cranium
Skull
Atlas
Odontoid pegBody of axis
Neural archof axis
Remainingcervical spine
FIG. 5 FIG. 6 FIG. 7
84 T. G. WILLIAM5
THE JOURNAL OF BONE AND JOINT SURGERY
FIG. 3 1I�
Three drawings (Figs. 1 to 3) and one oblique radiograph (Fig. 4) of the isolated axis, showingthe narrow pedicles, the stout spinous process, the wide circular spinal canal, and the way inwhich the superior articular facet straddles the vertebral body and inferior facet on each side.
Diagram showing the axis pedicles as the point of leverage of the extending “cervico-craniuni” (hatched) against the relatively fixed lowercervical spine (Fig. 5). Hangman’s fracture resulting from extension and compression (Fig. 6) and extension and distraction of the upper
cervical spine (Fig. 7).

TABLE IITHE Two TYPES OF HANGMAN’S FRACTURE
True hangman’s fracture Axis pedicle fracture
Mechanism
Typical cause
Radiological
appearance
Cord injury
Neurologicalsigns
Symptoms
Presentation
Prognosis
Treatment Gentle supervised skulltraction (less than 2 kg)with frequent checkradiographs.Proceed to fusion ifdistraction or neuro-logical signs increase
Supportive collar if thereare no cord signs and thefracture isstable.Skull traction for 6weeks, or operative dowelfusion, if symptomssevere or neurologicalsigns develop
(I,’
HANGMAN’S FRACTURE 85
VOL. 57-B, No. 1, FEBRUARY 1975
Extension and distrac-tion of the uppercervical spine
Extension and compres-sion of the upper cervicalspine
Judicial hanging. Blow on the forehead orLoose safety belt vertex with the upper
neck extended
Severe distraction of the Fracture of both pediclestwo fragments of theaxis, broken throughthe pedicles or lateral
of the axis, occasionallyinvolving the body of theaxis. Dens intact.
masses. There may be:-No other cervical bony -spondylolisthesis of theinjury. axisDens intact -one or more fractures
of the upper cervicalspinous processes
-bony injury of themiddle or lowercervical spine
Severe; due to traction Rare; from bleeding inthe cord
Flaccid tetraparesis Rare
Local and neurological Occipital neuralgia ; localcervical discomfort andstiffness
Immediate May be delayed severaldays
Poor; death usually �instant from cord injury
Good; symptoms usuallyslight and resolvecompletely
or vertex striking an obstacle while the body continues
to topple; a similar situation occurs when the unrestrained
car occupant is either projected forward in a head-on
accident and strikes his head on the inside of the vehicle,
or is ejected out and hits his head on the road. Afterwards
the patient usually holds his head slightly flexed, in which
position the fracture is stable although the anterior liga-
ment and the disc below the axis may be disrupted.
Neurological injury is rare, presumably because the spinal
canal is sufficiently wide at this level (Figs. 1 to 4) to
accommodate some movement of the fragments, which
in any case tend to separate and widen the canal; the
rarity of direct cord injury confirms that distraction does
not occur in this type of hangman’s fracture. Cornish
(1968) considered the occasional avulsion fracture of the
tip of the body of the axis inferiorly to be evidence of
extension. Associated mid-cervical injuries and fractures
of the spinous processes are also sometimes seen and
suggest that compression has occurred. Forsyth (1964)
proposed an almost identical mechanism of extension
with compression to explain fracture-dislocations of the
middle of the cervical spine, which were previously con-
sidered flexion injuries; it is therefore interesting that
there were other cervical injuries in some of Cornish’s
patients (Table I). Perhaps the axis snaps if the blow to
the head is received with the upper cervical spine already
extended; Cornish (1968) suggested that the vulnerable
position is with the head “ducked” (Fig. 8). By contrast,
if the neck is in the neutral position when the head is
struck, the soft tissues can take up some of the slack and
the whole cervical spine then extends evenly under tension
until either the anterior ligament gives way at the summit
of the arc or the facets collapse posteriorly (Fig. 9).
Fracture caused by extension and distraction-Distraction
ofthe upper cervical spine follows violent extension when
the rapidly moving body is suddenly restrained under the
chin or across the front of the neck. This is the aim of
judicial hanging by a submental knot and “long drop”
(which varies inversely with the victim’s weight and is
usually about six feet). The subaural knot, recommended
by Lord Aberdare’s Committee in 1886 and still appar-
ently in use in 1947 (British Medicalfournal), is unreliable
and may fracture the base ofthe skull (Wood Jones 1913).
Too short a drop may not break the neck, presumably
leaving the victim to die ofvascular occlusion and cerebral
ischaemia, as often happens in suicidal hanging (Good-
body 1973). If the drop is too long the victim’s head
FIG. 8 FIG. 9
Extension and compression of the upper cervical spine following a blow to the head, producing (Fig. 8) a hangman’s fracture, as suggestedby Cornish (1968); and (Fig. 9) middle cervical injury, as depicted by Forsyth (1964), with anterior ligament disruption anteriorly or
facet disintegration posteriorly.

FIG. I 1�” . 11 II .. 12Case 2-Cervical radiographs showing in Figure 10 a fracture of the hyoid; the axis pedicle fracture was just visible in this view. InFigure 1 1 the axis pedicle fracture is seen in a 20-degree oblique view, and in Figure 12 the mild separation of the fragments on forward
flexion.
86 T. G. WILLIAMS
THE JOURNAL OF BONE AND JOINT SURGERY
may be avulsed completely (Haughton 1866). Similarly,
a loose diagonal seat belt may permit a car occupant to
slide under the belt in a head-on accident, catching his
neck and distracting the axis from the third cervical
vertebra sometimes to the point of decapitation (Saldeen
1967). Distraction is thus a more violent injury than
compression and is usually accompanied by severe ex-
ternal evidence of injury to the neck with pronounced
local symptoms and a greater likelihood of neurological
sequelae from direct injury to the spinal cord.
CLINICAL FEATURES
The diagnosis of the compression type of hangman’s
fracture may not be made for several days after injury.
Presentation may be late, especially if the fracture fol-
lowed a simple fall with no other injury. Three patients
reported by Cornish (1968) presented to his orthopaedic
unit three or more days after injury, although he did not
account for the delay. Initial symptoms are often slight
and the patient usually experiences occipital neuralgia
with some local discomfort and stiffness of the upper
cervical spine. Indeed, the symptoms and signs may
resemble meningism.
CASE REPORT
Case 1-A thirty-four-year-old man attended hospital com-plaining of increasing stiffness and discomfort in his neck fortwenty-four hours, following a car accident he could notclearly recall. Radiographs showed an undisplaced, stablefracture through the body and neural arch of the axis. Therewere no neurological signs and he was discharged fromhospital a week later wearing a soft supportive collar. Localdiscomfort resolved within three months, and neck movementswere full and pain-free two months later.
Two years after the accident the patient was referred backto the orthopaedic department with occipital neuralgia andneck stiffness resembling his original symptoms. He was found
to have viral meningitis.
The doctor may not suspect bony injury in the
absence of local symptoms, or his attention may be
directed towards more obvious injuries sustained by the
patient. Even when bony injury is suspected, lateral and
antero-posterior radiographs may not reveal the fracture
because it is sometimes best seen in oblique views.
Furthermore, the clinician may think that the radiological
appearance suggests an old fracture or even a congenital
anomaly if the symptoms are slight, especially if there is
little prevertebral swelling.
CASE REPORTS
Case 2-A twenty-three-year-old car driver was admitted to
hospital immediately after a violent accident he could notremember. There were abrasions on the right side of hisforehead and left side of his neck, no neurological signs, andapparently pain-free cervical movements. Six hours later the
right side of his neck began to swell, embarrassing swallowingand speech. Cervical radiographs (Fig. 10) showed a hyoidfracture. Oblique views (Fig. 1 1) revealed a fracture acrosseach axis pedicle with mild but stable separation of thefragments on forward flexion (Fig. 12).
Thirty-six hours after admission the patient took his own
discharge against medical advice. He wore a soft supportivecollar for twelve weeks. Six months after injury his onlysymptoms were discomfort and stiffness on extending his neckor turning his head to the right.
Case 3-A seventy-eight-year-old woman sustained a trochan-teric fracture of her right femur in a car accident in which shelost consciousness briefly. On admission she was found tohave some mid-cervical tenderness, and the radiographs (Figs.13 and 14) were thought to show a congenital anomaly orunusual degenerative lesion of the axis. The femoral fracturewas fixed internally and she was discharged to a hospital in herdistant home town wearing a soft supportive collar.
Review of the radiographs confirmed that she had brokenboth pedicles of the axis.
Lateral radiographs in flexion and extension should
be taken, with oblique views if necessary, to confirm the
presence and stability ofcompression hangman’s fracture.
The difficulties already discussed often obscure the correct
diagnosis and it is possible that cases are being overlooked
because of a failure to appreciate that upper cervical bony
injury may be accompanied by slight or delayed symptoms

axis pec..Je fractures thought initially to be a congenital anomaly.
Fio. 16
. . .
‘ 4� �,4.
- #{163}3. 17Case 4. Figure 15-Lateral cervical radiograph showing an oblique fracture through theposterior half of the body and lateral masses of the axis and through the neural arch of theatlas. Figure 16 is a necropsy photograph of the fracture through the right lateral mass of theaxis. It has been superimposed on a diagrammatic sketch of the rest of the vertebra. Thefracture line runs through the base of the odontoid peg. Figure 17 shows the necropsyphotograph of the upper cervical spine bisected slightly to the right of the midline. Theintervertebral discs and the anterior and posterior ligaments are intact ; the spinal cord has not
been injured from without although there has been bleeding into its substance.
HANGMAN’S FRACTURE 87
VOL. 57-B, No. I, FEBRUARY 1975
and no neurological deficit, with equivocal radiological such patients are recorded as surviving tetraparesis
signs. (Cornish 1968 ; Edgar et a!. 1972). The further case
Patients with more severe cord injuries after a hang- presented below is unusual in that the neurological find-
man’s fracture with distraction of the axis fragments ings followed a cervical injury apparently caused by
presumably die without reaching a clinician, and only two extension and compression.

88 T. G. WILLIAMS
THE JOURNAL OF BONE AND JOINT SURGERY
CASE REPORT
Case 4-A forty-year-old mental defective fell forwards duringa grand ma! seizure and banged his head on a doorway. Onrecovering consciousness fifteen minutes later he was unable
to move his limbs. On admission to hospital he was found tohave a flaccid tetraparesis. He had a small laceration abovehis left eye and another on top of his head. Cervical radio-
graphs (Fig. 15) showed a fracture through the neural arch ofthe atlas extending through both lateral masses of the axis,which was subluxated forward on the third cervical vertebra.There was no radiological evidence of prevertebral swelling.
Skulltraction was applied with 6 pounds (2722 kilograms)weight, and ventilation was assisted through an endotrachealtube. Five days later he was breathing on his own and couldmake slight leg movements. He died two days later from theaspiration of vomit.
At necropsy the axis fracture was seen to run obliquelythrough the body and across the lateral masses (Figs. 16 and17). The anterior and posterior ligaments and intervertebraldiscs were intact, though blood had tracked beside them.There was no evidence of compression of the intact spinalcord, but some bleeding had occurred into its substance atthe level of the axis. The vertebral vessels were uninjured.
Perhaps this patient went into opisthotonos during hisepileptic seizure, forcibly extending his neck, which was then
subjected to compression when the top of his head struck the
doorway.
It is interesting that when Grogono (1954) presented
his original case, he suggested that cord injury was a
likely sequel of any axis pedicle fracture, although, as in
the report above, the lesion he discussed had probably
followed extension and compression of the upper cervical
spine.
TREATMENT
Treatment of the undisplaced stable hangman’s fracture
is symptomatic and a supportive collar usually suffices
until symptoms subside over six to twelve weeks. Al-
though some earlier cases were subjected to fusion, this
is now reserved for patients with severe local symptoms
or obvious neurological involvement. Schneider et a!.
(1965) felt that skull traction permitted early bony union
of the fracture-dislocation, though there is a danger of
over-distraction of the obviously unstable injury if trac-
tion exceeds two kilograms or check radiographs are not
sufficiently frequent (Edgar et a!. 1972). Cornish (1968)
condemned traction outright, preferring fusion between
the axis and third cervical vertebra. He approached this
site through a left submental skin crease incision, passing
anterior to the sternomastoid and posterior to the great
vessels, and checked the level radiologically before cutting
a circular bed coronally across the disc space with a tube
saw three-eighths of an inch in diameter. The anaesthetist
stretches the neck whilst the surgeon inserts a bone dowel
seven-sixteenths of an inch in diameter, taken from the
iliac crest. The patient is mobilised with a cervical splint
seven days after operation ; the splint is discarded after
six to ten weeks when radiological union has occurred.
Norrell and Wilson (1970) successfully treated five cases
of unstable hangman’s fracture by bone dowel fusion,
discharging their patients home on average only ten days
after operation.
I thank Professor J. S. Ellis, Mr M. S. Brett and Mr A. C. Warr for permission to report their cases, and Dr R. A. Goodbody for hisdissection and photographs of the post-mortem specimen of the upper cervical spine. I am grateful to Mr T. Earl and the Departmentof Medical Illustration at Southampton University, and to the Department of Medical Photography at Ipswich Hospital, for the diagrams.I thank Dr P. B. Guyer and Dr S. W. Heap for the use of radiographs taken by their Department.
REFERENCES
British Medical Journal (1947) Any Questions : Judicial hanging. British Medical Journal, 2, 160.Cornish, B. L. (1968) Traumatic spondylolisthesis of the axis. Journal ofBone and Joint Surgery, 50-B, 31-43.
DeLorme, T. L. (1967) Axis-pedicle fractures. Journal ofBone andJoint Surgery, 49-A, 1472.
Edgar, M. A., Fisher, T. R., McSweeney, T., and Park, W. M. (1972) Tetraplegia from hangman’s fracture: report of a case with recovery.Injury, 3, 199-202.
Forsyth, H. F. (1964) Extension injuries of the cervical spine. Journal ofBone andJoint Surgery, 46-A, 1792-1796.
Garber, J. N. (1964) Abnormalities of the atlas and axis vertebrae-congenital and traumatic. Journal of Bone and Joint Surgery, 46-A,1782-1791.
Goodbody, R. A. (1973) Personal communication.
Grogono, B. J. S. (1954) Injuries of the atlas and axis. Journal of Bone and Joint Surgery, 36-B, 397-410.
Haughton, S. (1866) On hanging, considered from a mechanical and physiological point of view. London, Edinburgh and Dublin:Philosophical Magazine and Journal of Science, 4th series, 32, 23-34.
Norrell, H., and Wilson, C. B. (1970) Early anterior fusion for injuries ofthe cervical portion of the spine. Journal ofthe American MedicalAssociation, 214, 525-530.
Norton, W. L. (1962) Fractures and dislocations of the cervical spine. Journal ofBone and Joint Surgery, 44-A, 115-139.
Rogers, W. A. (1957) Fractures and dislocations of the cervical spine. Journal ofBone andJoint Surgery, 39-A, 341-376.Saldeen, T. (1967) Fatal neck injuries caused by use of diagonal safety belts. Journal of Trauma, 7, 856-862.
Schneider, R. C., Livingston, K. E., Cave, A. J. E., and Hamilton, G. (1965) “Hangman’s fracture” of the cervical spine. Journal ofNeurosurgery, 22, 141-154.
Wood Jones, F. (1913) The ideal lesion produced by judicial hanging. Lancet, I, 53.








![Scravani - Facial Pain [Read-Only] · 13.4 – Superior laryngeal neuralgia 13.5 – Nasociliary neuralgia 13.6 – Supraorbital neuralgia 13.7 – Other terminal branch neuralgias](https://img.pdfslide.us/doc/110x75/5e9b9e94e532ce0d9f31854b/scravani-facial-pain-read-only-134-a-superior-laryngeal-neuralgia-135-a.jpg)