Embed Size (px)
Citation preview
NAMAS, a Division of DoctorsManagement, LLC 10401 Kingston Pike ◊ Knoxville, TN 37922 ◊ 877-418-5564 ◊ www.namas.co
‘Hands on Auditing’
Session Encounters
Presented by: Shannon DeConda, CPC, CPC-I, CEMC, CMSCS, CPMA®
President and Founder of NAMAS; Partner with DoctorsManagement, LLC


Patient Name: Tommy Miller Patient DOB: 01/28/2005 Date: 06/06/2014 History of Present Illness: Here with mom for vomiting and diarrhea that started last night around 10:30 p.m. and lasted until 2:00 a.m. He has had severe stomach pain/cramps. Mom said he’s had a fever but she did not take his temperature. Past Medical History: ADHD; Infantile Asthma – No SX since Age 4 (mostly environmental triggers such as mold in the home) Surgical History: Tympanostomy tubes; tonsillectomy; adenoidectomy; colonoscopy Family History: No significant family medical history. Social History: No smoking in home. Current Meds: None Allergies:
1. Zymine 2. Omnicef 3. Dust Mites
Vitals: Temp: 100.1 F; Weight: 60 lb; Height: 49.5 in; BP: 98/56; BMI: 17.21 Physical Exam General appearance: pleasant moddhydrated. Oral Cavity: normal, moist mucosal membranes. Heart: regular, normal S1 S2, no murmurs. Lungs: clear, no crackles or wheezes. Abdomen: Soft, BS present, no guarding or rigidity, no masses felt. Brief Normal Exam: HEENT: TMs pearly bilaterally, pharynx and tonsils normal. Assessment Gastroenteritis – 558.9 (Primary)
The Growing Strong Clinic
of the Greater Metro Area

Viral gastroenteritis is most likely Treatment: Discussed the condition. Informed that this is caused by a viral illness and that there is no treatment as such, that the illness needs to run its course but it is important to try to rehydrate the child at home. Advised to offer Pedialyte or Gatorade as rehydration fluids and to offer these fluids in small amounts frequently. Suggested the volume of fluid that needs to be offered to prevent dehydration. Also advised offering the child starchy foods such as potatoes, rice, etc and not to offer juice, Kool-Aid or sodas since they can make the symptoms worse. Also discussed signs of dehydration to look for such as sunken eyes, the absence of tears in the eyes, dry tongue, excessive sleepiness and decreased urine output and to call me if she noticed any of the symptoms. Mom expressed understanding of this plan. Also advised to use children’s dose of Pepto OTC to help control the symptoms Signatures: Electronically signed by: Karen Moore, MD
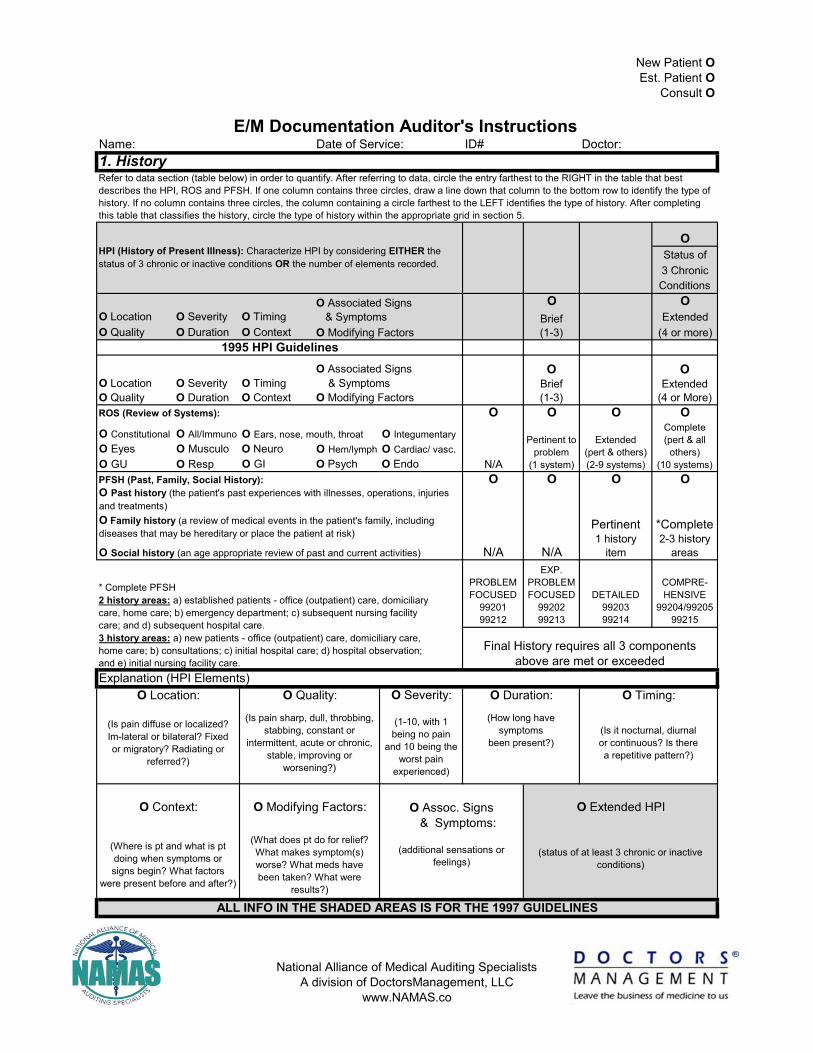
Name: ID# Doctor:1. History
OStatus of3 ChronicConditions
O OO Location O Severity O Timing ExtendedO Quality O Duration O Context (4 or more)
ROS (Review of Systems): O O O OO Constitutional O All/ImmunoO Eyes O Musculo O Neuro O Hem/lymph O Cardiac/ vasc.O GU O Resp O GI O Psych O EndoPFSH (Past, Family, Social History): O O O O
PROBLEMFOCUSED
9920199212
EXP.PROBLEMFOCUSED
9920299213
DETAILED9920399214
COMPRE-HENSIVE
99204/9920599215
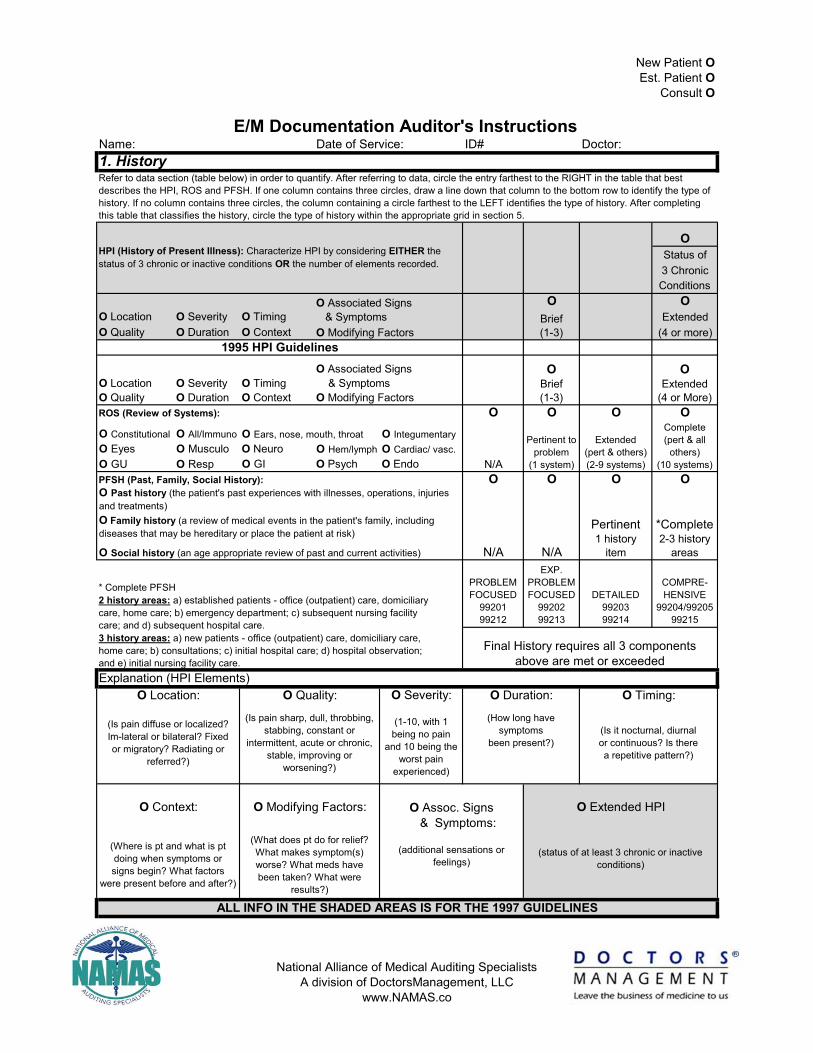
Explanation (HPI Elements)O Severity:
Brief (1-3)O Modifying Factors
ALL INFO IN THE SHADED AREAS IS FOR THE 1997 GUIDELINES
(Is it nocturnal, diurnal or continuous? Is there a repetitive pattern?)
(Where is pt and what is pt doing when symptoms or signs begin? What factors
were present before and after?)
(What does pt do for relief? What makes symptom(s) worse? What meds have been taken? What were
results?)
(status of at least 3 chronic or inactive conditions)
(additional sensations or feelings)
(Is pain diffuse or localized? Im-lateral or bilateral? Fixed or migratory? Radiating or
referred?)
(How long have symptoms
been present?)
Final History requires all 3 componentsabove are met or exceeded
* Complete PFSH 2 history areas: a) established patients - office (outpatient) care, domiciliary care, home care; b) emergency department; c) subsequent nursing facility care; and d) subsequent hospital care. 3 history areas: a) new patients - office (outpatient) care, domiciliary care, home care; b) consultations; c) initial hospital care; d) hospital observation; and e) initial nursing facility care.
Extended(pert & others)(2-9 systems)
Pertinent1 history
item
*Complete2-3 history
areas
O Ears, nose, mouth, throatComplete(pert & all
others)(10 systems)
O Past history (the patient's past experiences with illnesses, operations, injuries and treatments)
1995 HPI Guidelines
O Social history (an age appropriate review of past and current activities) N/A N/A
OBrief (1-3)
OExtended
(4 or More)O LocationO Quality
O SeverityO Duration
O Integumentary
N/A
Pertinent toproblem
(1 system)
O Family history (a review of medical events in the patient's family, including diseases that may be hereditary or place the patient at risk)
HPI (History of Present Illness): Characterize HPI by considering EITHER the status of 3 chronic or inactive conditions OR the number of elements recorded.
O Associated Signs & Symptoms
O TimingO Context
O Associated Signs & Symptoms O Modifying Factors
(1-10, with 1 being no pain
and 10 being the worst pain
experienced)
O Quality:
New Patient OEst. Patient O
Consult O
E/M Documentation Auditor's InstructionsDate of Service:
Refer to data section (table below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table that best describes the HPI, ROS and PFSH. If one column contains three circles, draw a line down that column to the bottom row to identify the type of history. If no column contains three circles, the column containing a circle farthest to the LEFT identifies the type of history. After completing this table that classifies the history, circle the type of history within the appropriate grid in section 5.
O Location: O Duration: O Timing:
O Context: O Modifying Factors: O Assoc. Signs & Symptoms:
O Extended HPI
(Is pain sharp, dull, throbbing, stabbing, constant or
intermittent, acute or chronic, stable, improving or
worsening?)
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co
B x C = D PointsNumber Points Result 1
Max=2 1 1
1 1
2 1
Max=1 3 1
4 2
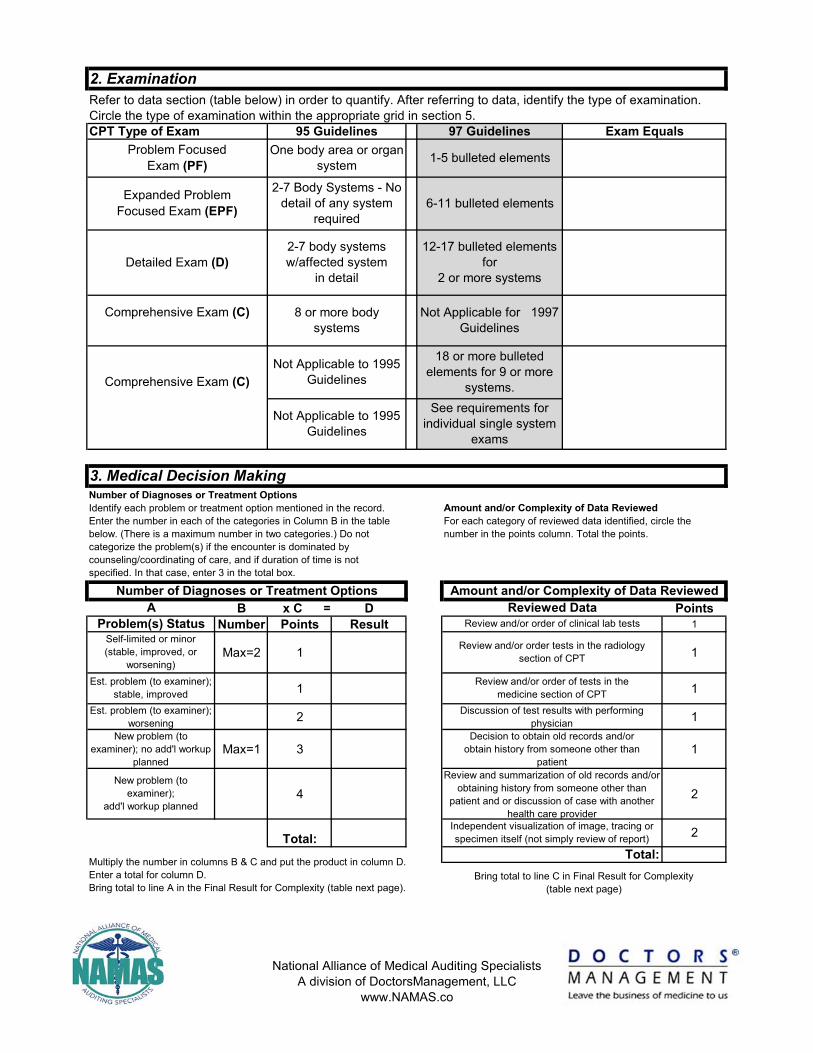
Expanded Problem Focused Exam (EPF)
Comprehensive Exam (C) 8 or more body systems
Not Applicable for 1997 Guidelines
Comprehensive Exam (C)
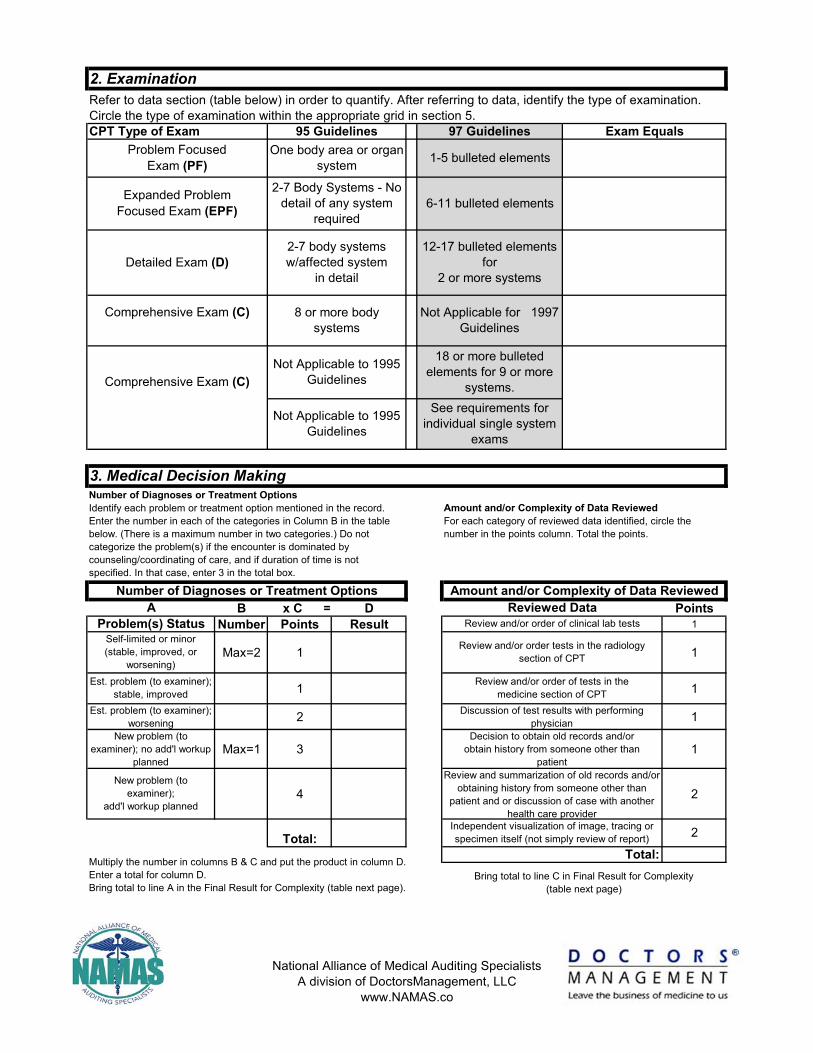
Refer to data section (table below) in order to quantify. After referring to data, identify the type of examination. Circle the type of examination within the appropriate grid in section 5.
Detailed Exam (D)
2-7 Body Systems - No detail of any system
required
2-7 body systemsw/affected system
in detail
Not Applicable to 1995 Guidelines
Exam EqualsOne body area or organ
system 1-5 bulleted elementsProblem Focused Exam (PF)
6-11 bulleted elements
Est. problem (to examiner); stable, improved
2. Examination
12-17 bulleted elements for
2 or more systems
18 or more bulleted elements for 9 or more
systems.See requirements for
individual single system exams
Not Applicable to 1995 Guidelines
CPT Type of Exam 95 Guidelines 97 Guidelines
Multiply the number in columns B & C and put the product in column D. Enter a total for column D. Bring total to line A in the Final Result for Complexity (table next page).
Review and/or order of tests in the medicine section of CPT
A
3. Medical Decision Making
Problem(s) StatusSelf-limited or minor (stable, improved, or
worsening)
Reviewed DataReview and/or order of clinical lab tests
Review and/or order tests in the radiology section of CPT
Number of Diagnoses or Treatment OptionsIdentify each problem or treatment option mentioned in the record. Enter the number in each of the categories in Column B in the table below. (There is a maximum number in two categories.) Do not categorize the problem(s) if the encounter is dominated by counseling/coordinating of care, and if duration of time is not specified. In that case, enter 3 in the total box.
Decision to obtain old records and/or obtain history from someone other than
patientReview and summarization of old records and/or
obtaining history from someone other than patient and or discussion of case with another
health care provider
Est. problem (to examiner); worsening
New problem (to examiner); no add'l workup
planned
New problem (to examiner);
add'l workup planned
Amount and/or Complexity of Data ReviewedFor each category of reviewed data identified, circle the number in the points column. Total the points.
Amount and/or Complexity of Data ReviewedNumber of Diagnoses or Treatment Options
Discussion of test results with performing physician
Total:Bring total to line C in Final Result for Complexity
(table next page)
Total:Independent visualization of image, tracing or specimen itself (not simply review of report) 2
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co
Level of Risk
Minimal
Low
Moderate
High
A 2 Limited
B Low
C 2 Limited
Low Complex
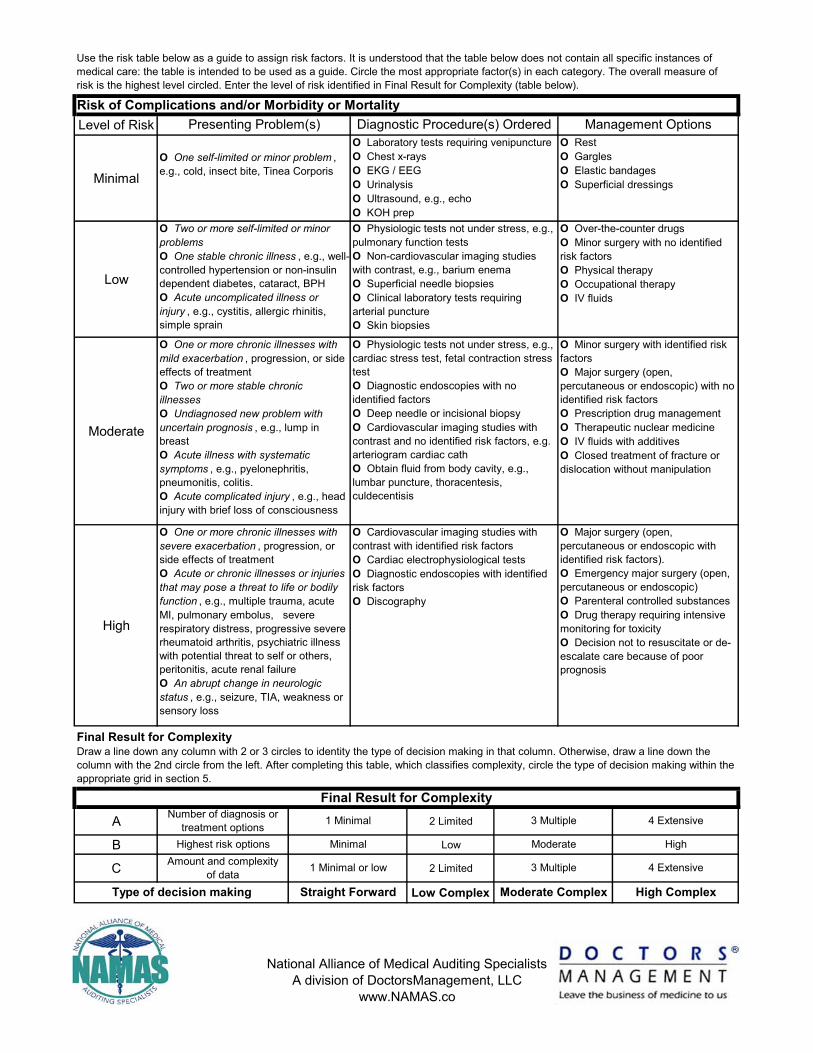
Use the risk table below as a guide to assign risk factors. It is understood that the table below does not contain all specific instances of medical care: the table is intended to be used as a guide. Circle the most appropriate factor(s) in each category. The overall measure of risk is the highest level circled. Enter the level of risk identified in Final Result for Complexity (table below).
Diagnostic Procedure(s) Ordered
O One or more chronic illnesses with severe exacerbation , progression, or side effects of treatmentO Acute or chronic illnesses or injuries that may pose a threat to life or bodily function , e.g., multiple trauma, acute MI, pulmonary embolus, severe respiratory distress, progressive severe rheumatoid arthritis, psychiatric illness with potential threat to self or others, peritonitis, acute renal failureO An abrupt change in neurologic status , e.g., seizure, TIA, weakness or sensory loss
O Cardiovascular imaging studies with contrast with identified risk factorsO Cardiac electrophysiological testsO Diagnostic endoscopies with identified risk factorsO Discography
Presenting Problem(s) Management Options
O Physiologic tests not under stress, e.g., cardiac stress test, fetal contraction stress testO Diagnostic endoscopies with no identified factorsO Deep needle or incisional biopsyO Cardiovascular imaging studies with contrast and no identified risk factors, e.g. arteriogram cardiac cathO Obtain fluid from body cavity, e.g., lumbar puncture, thoracentesis, culdecentisis
O Minor surgery with identified risk factorsO Major surgery (open, percutaneous or endoscopic) with no identified risk factorsO Prescription drug managementO Therapeutic nuclear medicineO IV fluids with additivesO Closed treatment of fracture or dislocation without manipulation
O Two or more self-limited or minor problemsO One stable chronic illness , e.g., well-controlled hypertension or non-insulin dependent diabetes, cataract, BPHO Acute uncomplicated illness or injury , e.g., cystitis, allergic rhinitis, simple sprain
O One self-limited or minor problem , e.g., cold, insect bite, Tinea Corporis
O Laboratory tests requiring venipunctureO Chest x-raysO EKG / EEGO UrinalysisO Ultrasound, e.g., echoO KOH prep
O RestO GarglesO Elastic bandagesO Superficial dressings
O Physiologic tests not under stress, e.g., pulmonary function tests O Non-cardiovascular imaging studies with contrast, e.g., barium enemaO Superficial needle biopsiesO Clinical laboratory tests requiring arterial punctureO Skin biopsies
O Over-the-counter drugsO Minor surgery with no identified risk factorsO Physical therapyO Occupational therapyO IV fluids
Risk of Complications and/or Morbidity or Mortality
O One or more chronic illnesses with mild exacerbation , progression, or side effects of treatmentO Two or more stable chronic illnessesO Undiagnosed new problem with uncertain prognosis , e.g., lump in breastO Acute illness with systematic symptoms , e.g., pyelonephritis, pneumonitis, colitis.O Acute complicated injury , e.g., head injury with brief loss of consciousness
Final Result for ComplexityDraw a line down any column with 2 or 3 circles to identity the type of decision making in that column. Otherwise, draw a line down the column with the 2nd circle from the left. After completing this table, which classifies complexity, circle the type of decision making within the appropriate grid in section 5.
O Major surgery (open, percutaneous or endoscopic with identified risk factors).O Emergency major surgery (open, percutaneous or endoscopic)O Parenteral controlled substancesO Drug therapy requiring intensive monitoring for toxicityO Decision not to resuscitate or de-escalate care because of poor prognosis
Number of diagnosis or treatment options
Highest risk optionsAmount and complexity
of data
4 Extensive3 Multiple
Moderate
3 Multiple
Moderate Complex
Final Result for Complexity
High
4 Extensive
High Complex
1 Minimal
Minimal
1 Minimal or low
Type of decision making Straight Forward
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co

4. Time
Time: __ yes __ no
__ yes __ no
__ yes __ no
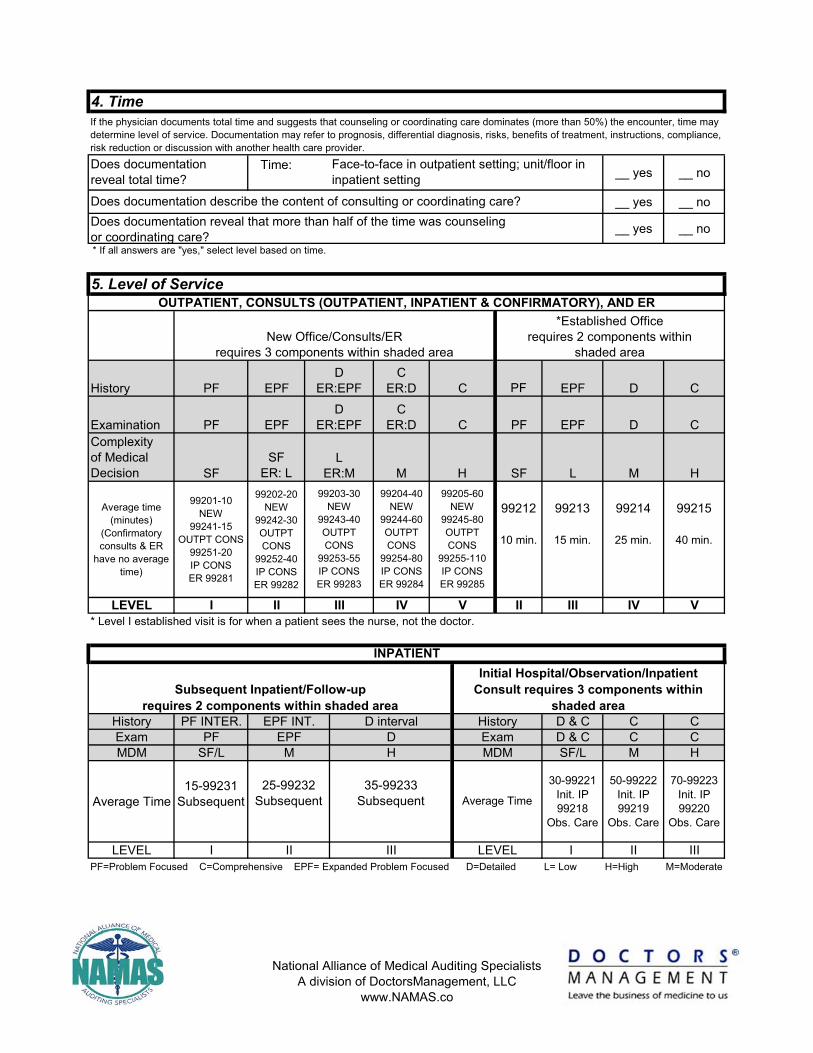
History PF EPF PF EPF D C
Examination PF EPF PF EPF D CComplexity of Medical Decision SF
SFER: L SF L M H
Average time (minutes)
(Confirmatory consults & ER
have no average time)
99201-10NEW
99241-15OUTPT CONS
99251-20IP CONSER 99281
99202-20NEW
99242-30OUTPT CONS
99252-40IP CONSER 99282
99212
10 min.
99213
15 min.
99214
25 min.
99215
40 min.
LEVEL I II II III IV V* Level I established visit is for when a patient sees the nurse, not the doctor.
History PF INTER. D & C C CExam PF D & C C CMDM SF/L SF/L M H
Average Time15-99231
Subsequent
30-99221Init. IP99218
Obs. Care
50-99222Init. IP99219
Obs. Care
70-99223Init. IP99220
Obs. Care
LEVEL I I II IIIPF=Problem Focused C=Comprehensive EPF= Expanded Problem Focused D=Detailed L= Low H=High M=Moderate
rev 111014
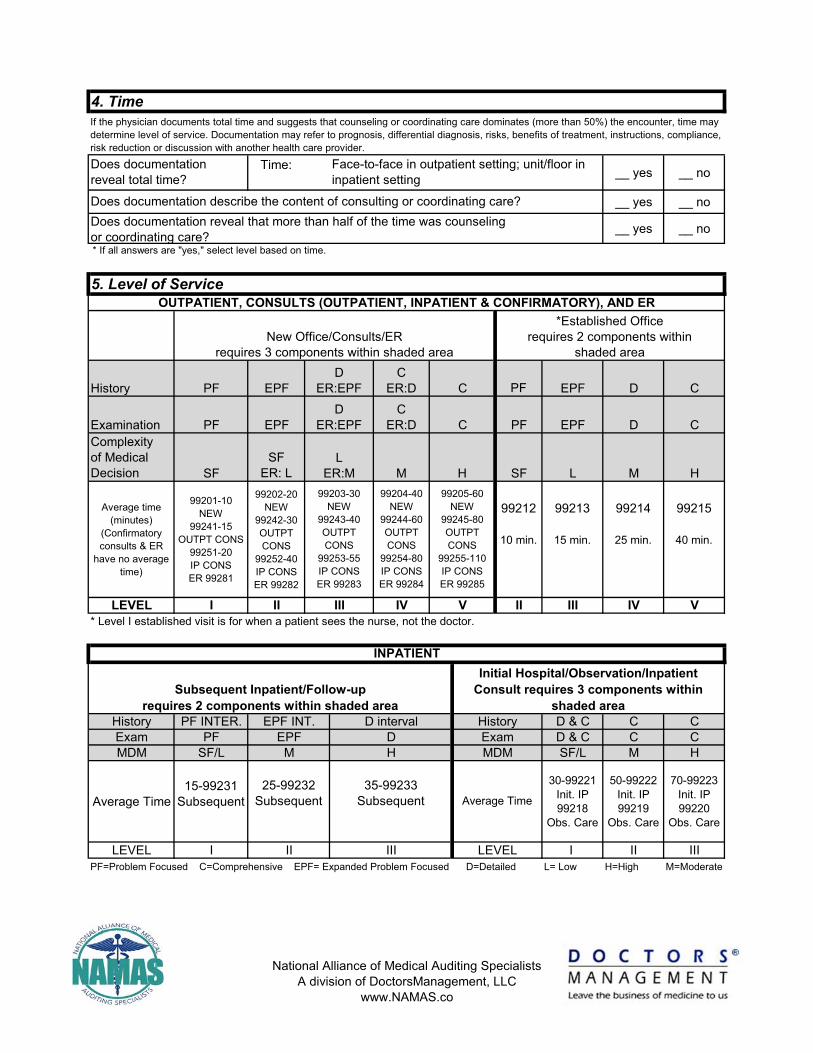
* If all answers are "yes," select level based on time.
If the physician documents total time and suggests that counseling or coordinating care dominates (more than 50%) the encounter, time may determine level of service. Documentation may refer to prognosis, differential diagnosis, risks, benefits of treatment, instructions, compliance, risk reduction or discussion with another health care provider.
Does documentation reveal total time?
Face-to-face in outpatient setting; unit/floor in inpatient setting
Does documentation reveal that more than half of the time was counseling or coordinating care?
Does documentation describe the content of consulting or coordinating care?
5. Level of ServiceOUTPATIENT, CONSULTS (OUTPATIENT, INPATIENT & CONFIRMATORY), AND ER
Average Time
LEVEL
*Established Officerequires 2 components within
shaded area
Subsequent Inpatient/Follow-uprequires 2 components within shaded area
New Office/Consults/ERrequires 3 components within shaded area
99203-30NEW
99243-40OUTPT CONS
99253-55IP CONSER 99283
III
Initial Hospital/Observation/Inpatient Consult requires 3 components within
shaded area
C
C
H99205-60
NEW99245-80OUTPT CONS
99255-110IP CONSER 99285
CER:D
DER:EPF
DER:EPF
LER:M
CER:D
M
HistoryExamMDM
INPATIENT
EPF INT.DH
35-99233Subsequent
III
25-99232Subsequent
99204-40NEW
99244-60OUTPT CONS
99254-80IP CONSER 99284
II
EPF
IV
M
D interval
V
revrevrevrevevrevevrevrevrevrevrevevevevrevrevrevvrevevevvevrevevrevevvvrevrevrevreevvvvrevevevrevrevvevrevvvvvvevevvvvevvvrevevvvvvvvveevvvveeevvvvvrevv 11 11 11111111111111111111111111111111 1111111111111111111 11111111111 1111111 1111111 111111111111111111111111111 11 11 1010101101101101101110111011011011011011010010110110110111011011010110101011011011110010101011010110111 1100011001000110110101011011011011011011011011011010100010110101001010110111101010011 1110001001444444444444444444444444444444444444444444444444444444
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co
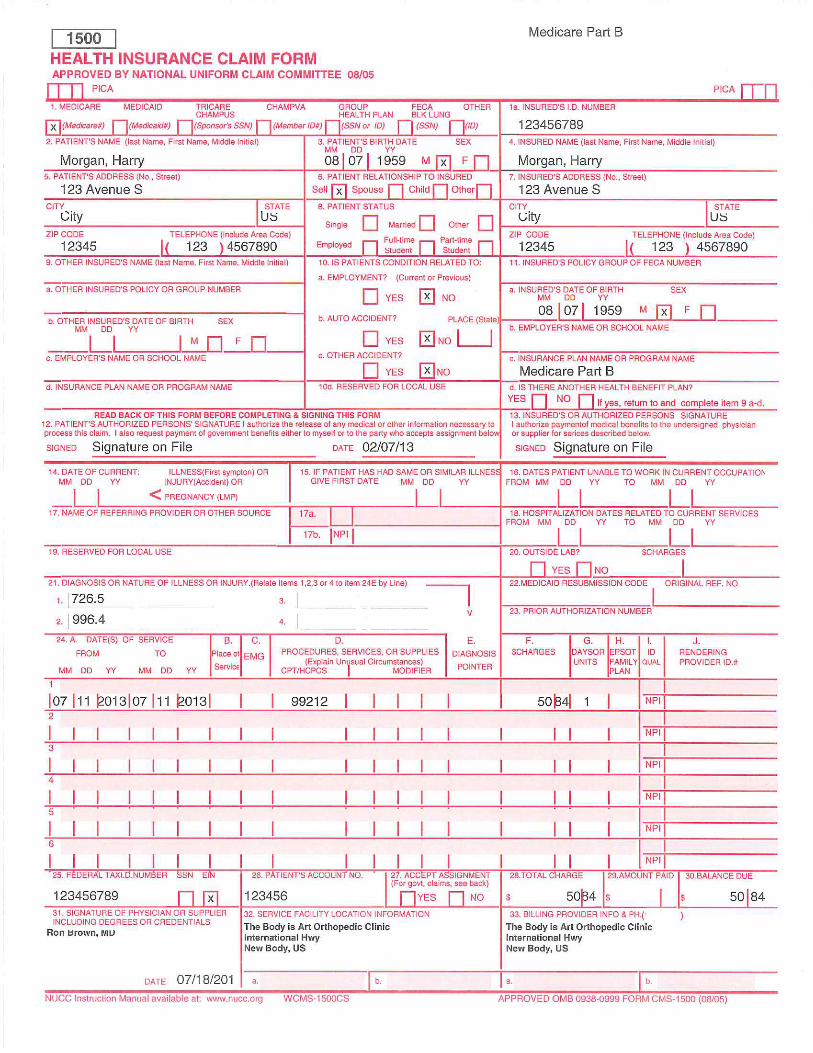
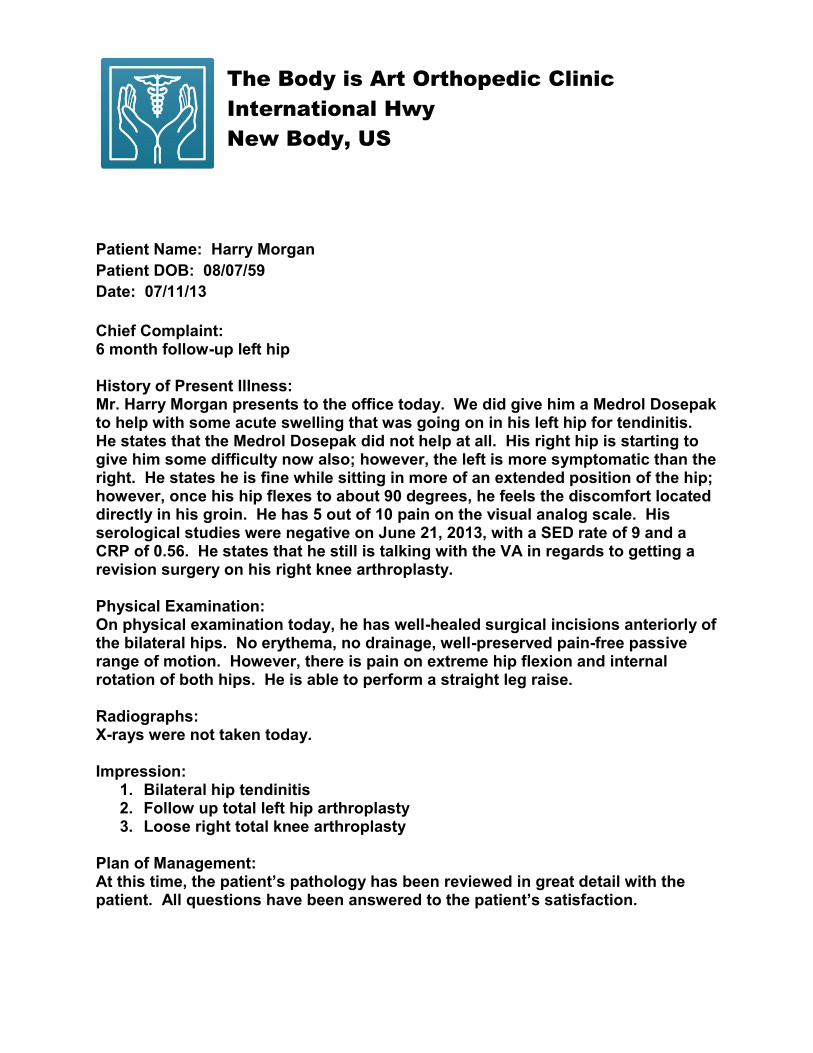
Patient Name: Harry Morgan Patient DOB: 08/07/59 Date: 07/11/13 Chief Complaint: 6 month follow-up left hip History of Present Illness: Mr. Harry Morgan presents to the office today. We did give him a Medrol Dosepak to help with some acute swelling that was going on in his left hip for tendinitis. He states that the Medrol Dosepak did not help at all. His right hip is starting to give him some difficulty now also; however, the left is more symptomatic than the right. He states he is fine while sitting in more of an extended position of the hip; however, once his hip flexes to about 90 degrees, he feels the discomfort located directly in his groin. He has 5 out of 10 pain on the visual analog scale. His serological studies were negative on June 21, 2013, with a SED rate of 9 and a CRP of 0.56. He states that he still is talking with the VA in regards to getting a revision surgery on his right knee arthroplasty. Physical Examination: On physical examination today, he has well-healed surgical incisions anteriorly of the bilateral hips. No erythema, no drainage, well-preserved pain-free passive range of motion. However, there is pain on extreme hip flexion and internal rotation of both hips. He is able to perform a straight leg raise. Radiographs: X-rays were not taken today. Impression:
1. Bilateral hip tendinitis 2. Follow up total left hip arthroplasty 3. Loose right total knee arthroplasty
Plan of Management: At this time, the patient’s pathology has been reviewed in great detail with the patient. All questions have been answered to the patient’s satisfaction.
The Body is Art Orthopedic Clinic International Hwy New Body, US

At this time, Mr. Harris is going to go to formal physical therapy for bilateral hip tendinitis including strengthening, stretching, ultrasound, and ionophoresis. He was also given a prescription for Mobic today. He will follow up in our office in six weeks to assess his progress. If he has any other difficulties, he may contact the office. Electronically signed by Ron Brown, MD

Name: ID# Doctor:1. History
OStatus of3 ChronicConditions
O OO Location O Severity O Timing ExtendedO Quality O Duration O Context (4 or more)
ROS (Review of Systems): O O O OO Constitutional O All/ImmunoO Eyes O Musculo O Neuro O Hem/lymph O Cardiac/ vasc.O GU O Resp O GI O Psych O EndoPFSH (Past, Family, Social History): O O O O
PROBLEMFOCUSED
9920199212
EXP.PROBLEMFOCUSED
9920299213
DETAILED9920399214
COMPRE-HENSIVE
99204/9920599215
Explanation (HPI Elements)O Severity:
Brief (1-3)O Modifying Factors
ALL INFO IN THE SHADED AREAS IS FOR THE 1997 GUIDELINES
(Is it nocturnal, diurnal or continuous? Is there a repetitive pattern?)
(Where is pt and what is pt doing when symptoms or signs begin? What factors
were present before and after?)
(What does pt do for relief? What makes symptom(s) worse? What meds have been taken? What were
results?)
(status of at least 3 chronic or inactive conditions)
(additional sensations or feelings)
(Is pain diffuse or localized? Im-lateral or bilateral? Fixed or migratory? Radiating or
referred?)
(How long have symptoms
been present?)
Final History requires all 3 componentsabove are met or exceeded
* Complete PFSH 2 history areas: a) established patients - office (outpatient) care, domiciliary care, home care; b) emergency department; c) subsequent nursing facility care; and d) subsequent hospital care. 3 history areas: a) new patients - office (outpatient) care, domiciliary care, home care; b) consultations; c) initial hospital care; d) hospital observation; and e) initial nursing facility care.
Extended(pert & others)(2-9 systems)
Pertinent1 history
item
*Complete2-3 history
areas
O Ears, nose, mouth, throatComplete(pert & all
others)(10 systems)
O Past history (the patient's past experiences with illnesses, operations, injuries and treatments)
1995 HPI Guidelines
O Social history (an age appropriate review of past and current activities) N/A N/A
OBrief (1-3)
OExtended
(4 or More)O LocationO Quality
O SeverityO Duration
O Integumentary
N/A
Pertinent toproblem
(1 system)
O Family history (a review of medical events in the patient's family, including diseases that may be hereditary or place the patient at risk)
HPI (History of Present Illness): Characterize HPI by considering EITHER the status of 3 chronic or inactive conditions OR the number of elements recorded.
O Associated Signs & Symptoms
O TimingO Context
O Associated Signs & Symptoms O Modifying Factors
(1-10, with 1 being no pain
and 10 being the worst pain
experienced)
O Quality:
New Patient OEst. Patient O
Consult O
E/M Documentation Auditor's InstructionsDate of Service:
Refer to data section (table below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table that best describes the HPI, ROS and PFSH. If one column contains three circles, draw a line down that column to the bottom row to identify the type of history. If no column contains three circles, the column containing a circle farthest to the LEFT identifies the type of history. After completing this table that classifies the history, circle the type of history within the appropriate grid in section 5.
O Location: O Duration: O Timing:
O Context: O Modifying Factors: O Assoc. Signs & Symptoms:
O Extended HPI
(Is pain sharp, dull, throbbing, stabbing, constant or
intermittent, acute or chronic, stable, improving or
worsening?)
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co

B x C = D PointsNumber Points Result 1
Max=2 1 1
1 1
2 1
Max=1 3 1
4 2
Expanded Problem Focused Exam (EPF)
Comprehensive Exam (C) 8 or more body systems
Not Applicable for 1997 Guidelines
Comprehensive Exam (C)
Refer to data section (table below) in order to quantify. After referring to data, identify the type of examination. Circle the type of examination within the appropriate grid in section 5.
Detailed Exam (D)
2-7 Body Systems - No detail of any system
required
2-7 body systemsw/affected system
in detail
Not Applicable to 1995 Guidelines
Exam EqualsOne body area or organ
system 1-5 bulleted elementsProblem Focused Exam (PF)
6-11 bulleted elements
Est. problem (to examiner); stable, improved
2. Examination
12-17 bulleted elements for
2 or more systems
18 or more bulleted elements for 9 or more
systems.See requirements for
individual single system exams
Not Applicable to 1995 Guidelines
CPT Type of Exam 95 Guidelines 97 Guidelines
Multiply the number in columns B & C and put the product in column D. Enter a total for column D. Bring total to line A in the Final Result for Complexity (table next page).
Review and/or order of tests in the medicine section of CPT
A
3. Medical Decision Making
Problem(s) StatusSelf-limited or minor (stable, improved, or
worsening)
Reviewed DataReview and/or order of clinical lab tests
Review and/or order tests in the radiology section of CPT
Number of Diagnoses or Treatment OptionsIdentify each problem or treatment option mentioned in the record. Enter the number in each of the categories in Column B in the table below. (There is a maximum number in two categories.) Do not categorize the problem(s) if the encounter is dominated by counseling/coordinating of care, and if duration of time is not specified. In that case, enter 3 in the total box.
Decision to obtain old records and/or obtain history from someone other than
patientReview and summarization of old records and/or
obtaining history from someone other than patient and or discussion of case with another
health care provider
Est. problem (to examiner); worsening
New problem (to examiner); no add'l workup
planned
New problem (to examiner);
add'l workup planned
Amount and/or Complexity of Data ReviewedFor each category of reviewed data identified, circle the number in the points column. Total the points.
Amount and/or Complexity of Data ReviewedNumber of Diagnoses or Treatment Options
Discussion of test results with performing physician
Total:Bring total to line C in Final Result for Complexity
(table next page)
Total:Independent visualization of image, tracing or specimen itself (not simply review of report) 2
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co

Level of Risk
Minimal
Low
Moderate
High
A 2 Limited
B Low
C 2 Limited
Low Complex
Use the risk table below as a guide to assign risk factors. It is understood that the table below does not contain all specific instances of medical care: the table is intended to be used as a guide. Circle the most appropriate factor(s) in each category. The overall measure of risk is the highest level circled. Enter the level of risk identified in Final Result for Complexity (table below).
Diagnostic Procedure(s) Ordered
O One or more chronic illnesses with severe exacerbation , progression, or side effects of treatmentO Acute or chronic illnesses or injuries that may pose a threat to life or bodily function , e.g., multiple trauma, acute MI, pulmonary embolus, severe respiratory distress, progressive severe rheumatoid arthritis, psychiatric illness with potential threat to self or others, peritonitis, acute renal failureO An abrupt change in neurologic status , e.g., seizure, TIA, weakness or sensory loss
O Cardiovascular imaging studies with contrast with identified risk factorsO Cardiac electrophysiological testsO Diagnostic endoscopies with identified risk factorsO Discography
Presenting Problem(s) Management Options
O Physiologic tests not under stress, e.g., cardiac stress test, fetal contraction stress testO Diagnostic endoscopies with no identified factorsO Deep needle or incisional biopsyO Cardiovascular imaging studies with contrast and no identified risk factors, e.g. arteriogram cardiac cathO Obtain fluid from body cavity, e.g., lumbar puncture, thoracentesis, culdecentisis
O Minor surgery with identified risk factorsO Major surgery (open, percutaneous or endoscopic) with no identified risk factorsO Prescription drug managementO Therapeutic nuclear medicineO IV fluids with additivesO Closed treatment of fracture or dislocation without manipulation
O Two or more self-limited or minor problemsO One stable chronic illness , e.g., well-controlled hypertension or non-insulin dependent diabetes, cataract, BPHO Acute uncomplicated illness or injury , e.g., cystitis, allergic rhinitis, simple sprain
O One self-limited or minor problem , e.g., cold, insect bite, Tinea Corporis
O Laboratory tests requiring venipunctureO Chest x-raysO EKG / EEGO UrinalysisO Ultrasound, e.g., echoO KOH prep
O RestO GarglesO Elastic bandagesO Superficial dressings
O Physiologic tests not under stress, e.g., pulmonary function tests O Non-cardiovascular imaging studies with contrast, e.g., barium enemaO Superficial needle biopsiesO Clinical laboratory tests requiring arterial punctureO Skin biopsies
O Over-the-counter drugsO Minor surgery with no identified risk factorsO Physical therapyO Occupational therapyO IV fluids
Risk of Complications and/or Morbidity or Mortality
O One or more chronic illnesses with mild exacerbation , progression, or side effects of treatmentO Two or more stable chronic illnessesO Undiagnosed new problem with uncertain prognosis , e.g., lump in breastO Acute illness with systematic symptoms , e.g., pyelonephritis, pneumonitis, colitis.O Acute complicated injury , e.g., head injury with brief loss of consciousness
Final Result for ComplexityDraw a line down any column with 2 or 3 circles to identity the type of decision making in that column. Otherwise, draw a line down the column with the 2nd circle from the left. After completing this table, which classifies complexity, circle the type of decision making within the appropriate grid in section 5.
O Major surgery (open, percutaneous or endoscopic with identified risk factors).O Emergency major surgery (open, percutaneous or endoscopic)O Parenteral controlled substancesO Drug therapy requiring intensive monitoring for toxicityO Decision not to resuscitate or de-escalate care because of poor prognosis
Number of diagnosis or treatment options
Highest risk optionsAmount and complexity
of data
4 Extensive3 Multiple
Moderate
3 Multiple
Moderate Complex
Final Result for Complexity
High
4 Extensive
High Complex
1 Minimal
Minimal
1 Minimal or low
Type of decision making Straight Forward
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co
4. Time
Time: __ yes __ no
__ yes __ no
__ yes __ no
History PF EPF PF EPF D C
Examination PF EPF PF EPF D CComplexity of Medical Decision SF
SFER: L SF L M H
Average time (minutes)
(Confirmatory consults & ER
have no average time)
99201-10NEW
99241-15OUTPT CONS
99251-20IP CONSER 99281
99202-20NEW
99242-30OUTPT CONS
99252-40IP CONSER 99282
99212
10 min.
99213
15 min.
99214
25 min.
99215
40 min.
LEVEL I II II III IV V* Level I established visit is for when a patient sees the nurse, not the doctor.
History PF INTER. D & C C CExam PF D & C C CMDM SF/L SF/L M H
Average Time15-99231
Subsequent
30-99221Init. IP99218
Obs. Care
50-99222Init. IP99219
Obs. Care
70-99223Init. IP99220
Obs. Care
LEVEL I I II IIIPF=Problem Focused C=Comprehensive EPF= Expanded Problem Focused D=Detailed L= Low H=High M=Moderate
rev 111014
* If all answers are "yes," select level based on time.
If the physician documents total time and suggests that counseling or coordinating care dominates (more than 50%) the encounter, time may determine level of service. Documentation may refer to prognosis, differential diagnosis, risks, benefits of treatment, instructions, compliance, risk reduction or discussion with another health care provider.
Does documentation reveal total time?
Face-to-face in outpatient setting; unit/floor in inpatient setting
Does documentation reveal that more than half of the time was counseling or coordinating care?
Does documentation describe the content of consulting or coordinating care?
5. Level of ServiceOUTPATIENT, CONSULTS (OUTPATIENT, INPATIENT & CONFIRMATORY), AND ER
Average Time
LEVEL
*Established Officerequires 2 components within
shaded area
Subsequent Inpatient/Follow-uprequires 2 components within shaded area
New Office/Consults/ERrequires 3 components within shaded area
99203-30NEW
99243-40OUTPT CONS
99253-55IP CONSER 99283
III
Initial Hospital/Observation/Inpatient Consult requires 3 components within
shaded area
C
C
H99205-60
NEW99245-80OUTPT CONS
99255-110IP CONSER 99285
CER:D
DER:EPF
DER:EPF
LER:M
CER:D
M
HistoryExamMDM
INPATIENT
EPF INT.DH
35-99233Subsequent
III
25-99232Subsequent
99204-40NEW
99244-60OUTPT CONS
99254-80IP CONSER 99284
II
EPF
IV
M
D interval
V
revrevrevrevevrevevrevrevrevrevrevevevevrevrevrevvrevevevvevrevevrevevvvrevrevrevreevvvvrevevevrevrevvevrevvvvvvevevvvvevvvrevevvvvvvvveevvvveeevvvvvrevv 11 11 11111111111111111111111111111111 1111111111111111111 11111111111 1111111 1111111 111111111111111111111111111 11 11 1010101101101101101110111011011011011011010010110110110111011011010110101011011011110010101011010110111 1100011001000110110101011011011011011011011011011010100010110101001010110111101010011 1110001001444444444444444444444444444444444444444444444444444444
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co

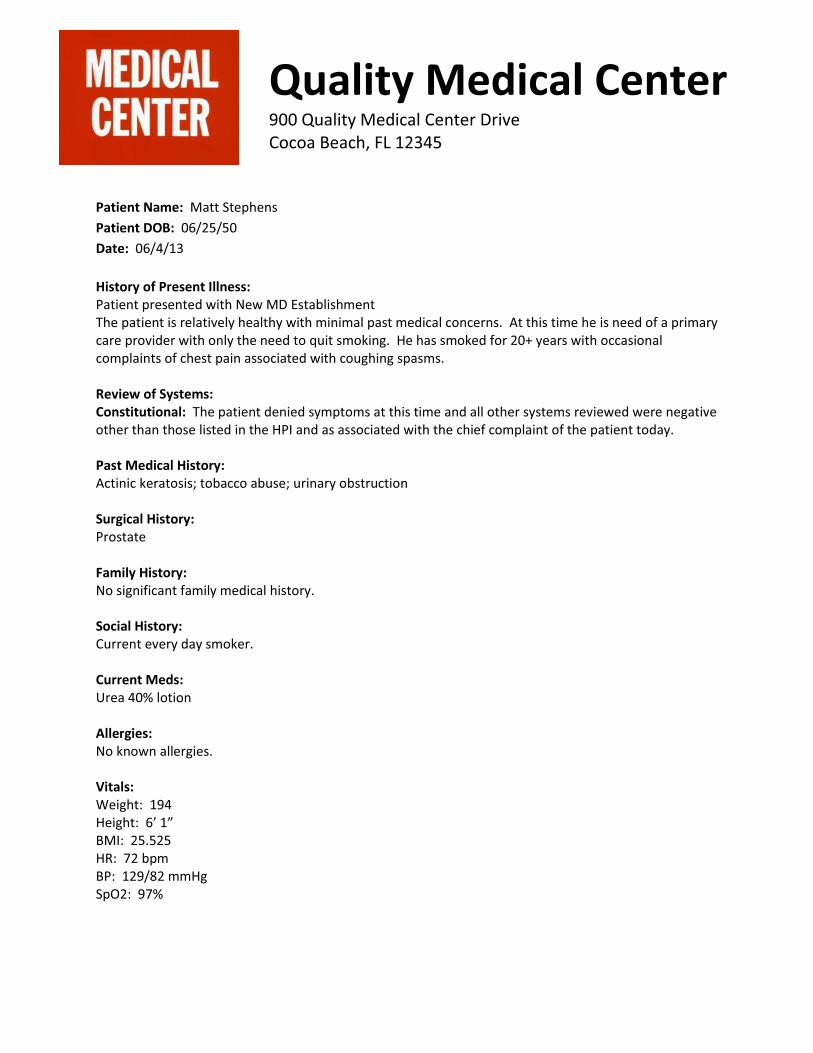
Patient Name: Matt Stephens Patient DOB: 06/25/50 Date: 06/4/13 History of Present Illness: Patient presented with New MD Establishment The patient is relatively healthy with minimal past medical concerns. At this time he is need of a primary care provider with only the need to quit smoking. He has smoked for 20+ years with occasional complaints of chest pain associated with coughing spasms. Review of Systems: Constitutional: The patient denied symptoms at this time and all other systems reviewed were negative other than those listed in the HPI and as associated with the chief complaint of the patient today. Past Medical History: Actinic keratosis; tobacco abuse; urinary obstruction Surgical History: Prostate Family History: No significant family medical history. Social History: Current every day smoker. Current Meds: Urea 40% lotion Allergies: No known allergies. Vitals: Weight: 194 Height: 6’ 1” BMI: 25.525 HR: 72 bpm BP: 129/82 mmHg SpO2: 97%
Quality Medical Center 900 Quality Medical Center Drive Cocoa Beach, FL 12345

Physical Exam Constitutional: General appearance: well nourished and in no acute distress. Eyes: Conjunctiva/eyelids: Conjunctiva clear and eyelids normal. Ears/Nose/Throat: Otoscopic exam: external auditory canals clear and tympanic membranes clear. Oral Cavity/pharynx/larynx: mucus membranes moist. Neck: Thyroid: normal size. Inspection of neck: no masses, no lymphadenopathy. Respiratory: Auscultation: breath sounds clear bilaterally. Respiratory effort/rhythm: normal rate. Cardiovascular: Auscultation of heart: regular rate, normal heart sounds and no murmurs. Abdomen: Abdominal exam: no tenderness and normal bowel sounds. Liver and spleen exam: no hepatosplenomegaly. Lymphatic: Neck nodes: anterior cervical chain benign and posterior cervical chain benign. Integument: Inspection of skin: no rash, lesions, good turgor. Neurologic: Gait: no ataxia, no unsteadiness. Psychiatric: Appearance: grooming; healthy. Diagnosis Tobacco Abuse Actinic keratosis Urinary obstruction Rx Chantix continuing month box 1 mg tablet, tablet(s) orally, daily, 2 refills and for a total of 1. Chantix starting month box 0.5 mg (11)-1 mg (42) tablets in dose pack, tablet(s), orally and for a total of 1. Plan Labs, CBC and Lipids Panel when fasting. Chest x-ray. Chantix start box. Encouraged low saturated fat diet and exercise. Will call with results of labs. Electronically signed by Sarah Taylor, ARNP

Name: ID# Doctor:1. History
OStatus of3 ChronicConditions
O OO Location O Severity O Timing ExtendedO Quality O Duration O Context (4 or more)
ROS (Review of Systems): O O O OO Constitutional O All/ImmunoO Eyes O Musculo O Neuro O Hem/lymph O Cardiac/ vasc.O GU O Resp O GI O Psych O EndoPFSH (Past, Family, Social History): O O O O
PROBLEMFOCUSED
9920199212
EXP.PROBLEMFOCUSED
9920299213
DETAILED9920399214
COMPRE-HENSIVE
99204/9920599215
Explanation (HPI Elements)O Severity:
Brief (1-3)O Modifying Factors
ALL INFO IN THE SHADED AREAS IS FOR THE 1997 GUIDELINES
(Is it nocturnal, diurnal or continuous? Is there a repetitive pattern?)
(Where is pt and what is pt doing when symptoms or signs begin? What factors
were present before and after?)
(What does pt do for relief? What makes symptom(s) worse? What meds have been taken? What were
results?)
(status of at least 3 chronic or inactive conditions)
(additional sensations or feelings)
(Is pain diffuse or localized? Im-lateral or bilateral? Fixed or migratory? Radiating or
referred?)
(How long have symptoms
been present?)
Final History requires all 3 componentsabove are met or exceeded
* Complete PFSH 2 history areas: a) established patients - office (outpatient) care, domiciliary care, home care; b) emergency department; c) subsequent nursing facility care; and d) subsequent hospital care. 3 history areas: a) new patients - office (outpatient) care, domiciliary care, home care; b) consultations; c) initial hospital care; d) hospital observation; and e) initial nursing facility care.
Extended(pert & others)(2-9 systems)
Pertinent1 history
item
*Complete2-3 history
areas
O Ears, nose, mouth, throatComplete(pert & all
others)(10 systems)
O Past history (the patient's past experiences with illnesses, operations, injuries and treatments)
1995 HPI Guidelines
O Social history (an age appropriate review of past and current activities) N/A N/A
OBrief (1-3)
OExtended
(4 or More)O LocationO Quality
O SeverityO Duration
O Integumentary
N/A
Pertinent toproblem
(1 system)
O Family history (a review of medical events in the patient's family, including diseases that may be hereditary or place the patient at risk)
HPI (History of Present Illness): Characterize HPI by considering EITHER the status of 3 chronic or inactive conditions OR the number of elements recorded.
O Associated Signs & Symptoms
O TimingO Context
O Associated Signs & Symptoms O Modifying Factors
(1-10, with 1 being no pain
and 10 being the worst pain
experienced)
O Quality:
New Patient OEst. Patient O
Consult O
E/M Documentation Auditor's InstructionsDate of Service:
Refer to data section (table below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table that best describes the HPI, ROS and PFSH. If one column contains three circles, draw a line down that column to the bottom row to identify the type of history. If no column contains three circles, the column containing a circle farthest to the LEFT identifies the type of history. After completing this table that classifies the history, circle the type of history within the appropriate grid in section 5.
O Location: O Duration: O Timing:
O Context: O Modifying Factors: O Assoc. Signs & Symptoms:
O Extended HPI
(Is pain sharp, dull, throbbing, stabbing, constant or
intermittent, acute or chronic, stable, improving or
worsening?)
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co
B x C = D PointsNumber Points Result 1
Max=2 1 1
1 1
2 1
Max=1 3 1
4 2
Expanded Problem Focused Exam (EPF)
Comprehensive Exam (C) 8 or more body systems
Not Applicable for 1997 Guidelines
Comprehensive Exam (C)
Refer to data section (table below) in order to quantify. After referring to data, identify the type of examination. Circle the type of examination within the appropriate grid in section 5.
Detailed Exam (D)
2-7 Body Systems - No detail of any system
required
2-7 body systemsw/affected system
in detail
Not Applicable to 1995 Guidelines
Exam EqualsOne body area or organ
system 1-5 bulleted elementsProblem Focused Exam (PF)
6-11 bulleted elements
Est. problem (to examiner); stable, improved
2. Examination
12-17 bulleted elements for
2 or more systems
18 or more bulleted elements for 9 or more
systems.See requirements for
individual single system exams
Not Applicable to 1995 Guidelines
CPT Type of Exam 95 Guidelines 97 Guidelines
Multiply the number in columns B & C and put the product in column D. Enter a total for column D. Bring total to line A in the Final Result for Complexity (table next page).
Review and/or order of tests in the medicine section of CPT
A
3. Medical Decision Making
Problem(s) StatusSelf-limited or minor (stable, improved, or
worsening)
Reviewed DataReview and/or order of clinical lab tests
Review and/or order tests in the radiology section of CPT
Number of Diagnoses or Treatment OptionsIdentify each problem or treatment option mentioned in the record. Enter the number in each of the categories in Column B in the table below. (There is a maximum number in two categories.) Do not categorize the problem(s) if the encounter is dominated by counseling/coordinating of care, and if duration of time is not specified. In that case, enter 3 in the total box.
Decision to obtain old records and/or obtain history from someone other than
patientReview and summarization of old records and/or
obtaining history from someone other than patient and or discussion of case with another
health care provider
Est. problem (to examiner); worsening
New problem (to examiner); no add'l workup
planned
New problem (to examiner);
add'l workup planned
Amount and/or Complexity of Data ReviewedFor each category of reviewed data identified, circle the number in the points column. Total the points.
Amount and/or Complexity of Data ReviewedNumber of Diagnoses or Treatment Options
Discussion of test results with performing physician
Total:Bring total to line C in Final Result for Complexity
(table next page)
Total:Independent visualization of image, tracing or specimen itself (not simply review of report) 2
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co

Level of Risk
Minimal
Low
Moderate
High
A 2 Limited
B Low
C 2 Limited
Low Complex
Use the risk table below as a guide to assign risk factors. It is understood that the table below does not contain all specific instances of medical care: the table is intended to be used as a guide. Circle the most appropriate factor(s) in each category. The overall measure of risk is the highest level circled. Enter the level of risk identified in Final Result for Complexity (table below).
Diagnostic Procedure(s) Ordered
O One or more chronic illnesses with severe exacerbation , progression, or side effects of treatmentO Acute or chronic illnesses or injuries that may pose a threat to life or bodily function , e.g., multiple trauma, acute MI, pulmonary embolus, severe respiratory distress, progressive severe rheumatoid arthritis, psychiatric illness with potential threat to self or others, peritonitis, acute renal failureO An abrupt change in neurologic status , e.g., seizure, TIA, weakness or sensory loss
O Cardiovascular imaging studies with contrast with identified risk factorsO Cardiac electrophysiological testsO Diagnostic endoscopies with identified risk factorsO Discography
Presenting Problem(s) Management Options
O Physiologic tests not under stress, e.g., cardiac stress test, fetal contraction stress testO Diagnostic endoscopies with no identified factorsO Deep needle or incisional biopsyO Cardiovascular imaging studies with contrast and no identified risk factors, e.g. arteriogram cardiac cathO Obtain fluid from body cavity, e.g., lumbar puncture, thoracentesis, culdecentisis
O Minor surgery with identified risk factorsO Major surgery (open, percutaneous or endoscopic) with no identified risk factorsO Prescription drug managementO Therapeutic nuclear medicineO IV fluids with additivesO Closed treatment of fracture or dislocation without manipulation
O Two or more self-limited or minor problemsO One stable chronic illness , e.g., well-controlled hypertension or non-insulin dependent diabetes, cataract, BPHO Acute uncomplicated illness or injury , e.g., cystitis, allergic rhinitis, simple sprain
O One self-limited or minor problem , e.g., cold, insect bite, Tinea Corporis
O Laboratory tests requiring venipunctureO Chest x-raysO EKG / EEGO UrinalysisO Ultrasound, e.g., echoO KOH prep
O RestO GarglesO Elastic bandagesO Superficial dressings
O Physiologic tests not under stress, e.g., pulmonary function tests O Non-cardiovascular imaging studies with contrast, e.g., barium enemaO Superficial needle biopsiesO Clinical laboratory tests requiring arterial punctureO Skin biopsies
O Over-the-counter drugsO Minor surgery with no identified risk factorsO Physical therapyO Occupational therapyO IV fluids
Risk of Complications and/or Morbidity or Mortality
O One or more chronic illnesses with mild exacerbation , progression, or side effects of treatmentO Two or more stable chronic illnessesO Undiagnosed new problem with uncertain prognosis , e.g., lump in breastO Acute illness with systematic symptoms , e.g., pyelonephritis, pneumonitis, colitis.O Acute complicated injury , e.g., head injury with brief loss of consciousness
Final Result for ComplexityDraw a line down any column with 2 or 3 circles to identity the type of decision making in that column. Otherwise, draw a line down the column with the 2nd circle from the left. After completing this table, which classifies complexity, circle the type of decision making within the appropriate grid in section 5.
O Major surgery (open, percutaneous or endoscopic with identified risk factors).O Emergency major surgery (open, percutaneous or endoscopic)O Parenteral controlled substancesO Drug therapy requiring intensive monitoring for toxicityO Decision not to resuscitate or de-escalate care because of poor prognosis
Number of diagnosis or treatment options
Highest risk optionsAmount and complexity
of data
4 Extensive3 Multiple
Moderate
3 Multiple
Moderate Complex
Final Result for Complexity
High
4 Extensive
High Complex
1 Minimal
Minimal
1 Minimal or low
Type of decision making Straight Forward
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co
4. Time
Time: __ yes __ no
__ yes __ no
__ yes __ no
History PF EPF PF EPF D C
Examination PF EPF PF EPF D CComplexity of Medical Decision SF
SFER: L SF L M H
Average time (minutes)
(Confirmatory consults & ER
have no average time)
99201-10NEW
99241-15OUTPT CONS
99251-20IP CONSER 99281
99202-20NEW
99242-30OUTPT CONS
99252-40IP CONSER 99282
99212
10 min.
99213
15 min.
99214
25 min.
99215
40 min.
LEVEL I II II III IV V* Level I established visit is for when a patient sees the nurse, not the doctor.
History PF INTER. D & C C CExam PF D & C C CMDM SF/L SF/L M H
Average Time15-99231
Subsequent
30-99221Init. IP99218
Obs. Care
50-99222Init. IP99219
Obs. Care
70-99223Init. IP99220
Obs. Care
LEVEL I I II IIIPF=Problem Focused C=Comprehensive EPF= Expanded Problem Focused D=Detailed L= Low H=High M=Moderate
rev 111014
* If all answers are "yes," select level based on time.
If the physician documents total time and suggests that counseling or coordinating care dominates (more than 50%) the encounter, time may determine level of service. Documentation may refer to prognosis, differential diagnosis, risks, benefits of treatment, instructions, compliance, risk reduction or discussion with another health care provider.
Does documentation reveal total time?
Face-to-face in outpatient setting; unit/floor in inpatient setting
Does documentation reveal that more than half of the time was counseling or coordinating care?
Does documentation describe the content of consulting or coordinating care?
5. Level of ServiceOUTPATIENT, CONSULTS (OUTPATIENT, INPATIENT & CONFIRMATORY), AND ER
Average Time
LEVEL
*Established Officerequires 2 components within
shaded area
Subsequent Inpatient/Follow-uprequires 2 components within shaded area
New Office/Consults/ERrequires 3 components within shaded area
99203-30NEW
99243-40OUTPT CONS
99253-55IP CONSER 99283
III
Initial Hospital/Observation/Inpatient Consult requires 3 components within
shaded area
C
C
H99205-60
NEW99245-80OUTPT CONS
99255-110IP CONSER 99285
CER:D
DER:EPF
DER:EPF
LER:M
CER:D
M
HistoryExamMDM
INPATIENT
EPF INT.DH
35-99233Subsequent
III
25-99232Subsequent
99204-40NEW
99244-60OUTPT CONS
99254-80IP CONSER 99284
II
EPF
IV
M
D interval
V
revrevrevrevevrevevrevrevrevrevrevevevevrevrevrevvrevevevvevrevevrevevvvrevrevrevreevvvvrevevevrevrevvevrevvvvvvevevvvvevvvrevevvvvvvvveevvvveeevvvvvrevv 11 11 11111111111111111111111111111111 1111111111111111111 11111111111 1111111 1111111 111111111111111111111111111 11 11 1010101101101101101110111011011011011011010010110110110111011011010110101011011011110010101011010110111 1100011001000110110101011011011011011011011011011010100010110101001010110111101010011 1110001001444444444444444444444444444444444444444444444444444444
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co
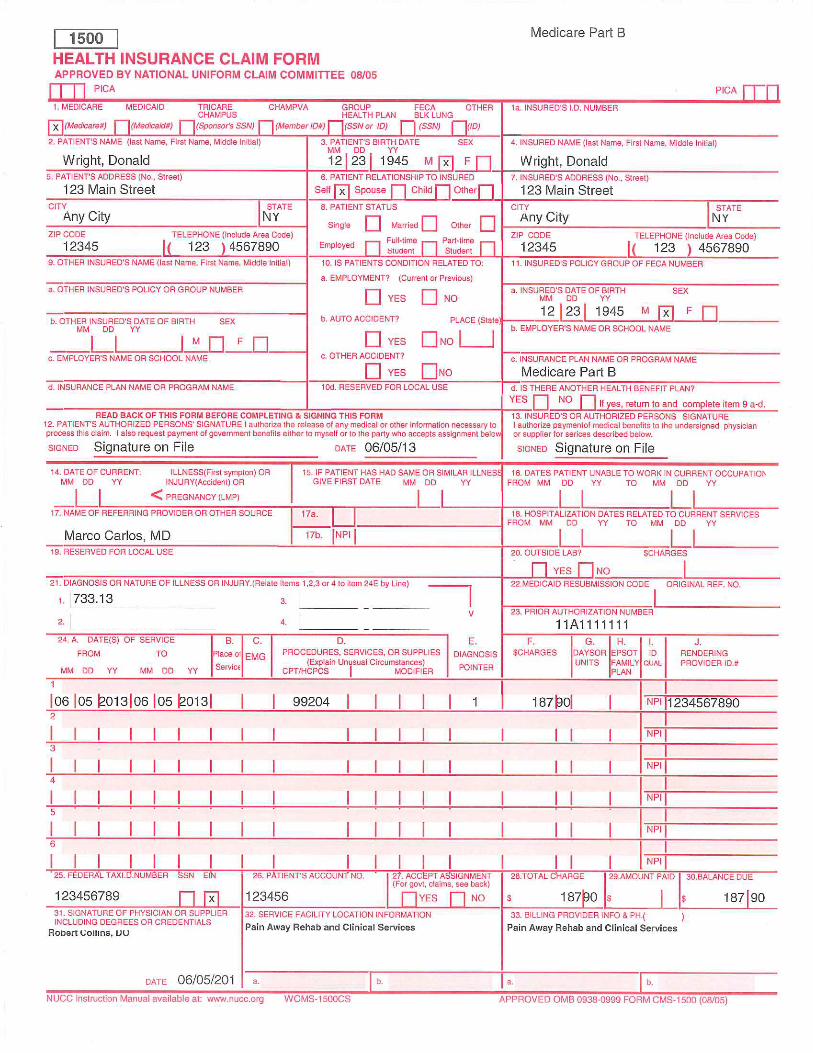

Patient Name: Donald Wright Patient DOB: 12/23/45 Date: 06/05/13 History of Present Illness: Mr. Wright, 67 years old, was seen today regarding his mid back pain. He reports about a year and a half ago, he was picking up something heavy and fell backwards on his left shoulder. At that time, he was told that he had a small fracture. His pain got better until recently where he was having the pain more often. He states that it occurs on and off. It is mostly mid back pain. He denies any radicular component to the pain. Past Medical History: Hypertension, diabetes mellitus, stroke and heart disease. Surgical History: Valve replacement in 1999 and a stent placed in 2011. Family History: Noncontributory. Social History: No smoking. Occasional alcohol use. Current Meds: Metformin 500 mg b.i.d., lisinopril 40 mg daily, Crestor 10 mg daily, warfarin 5 mg daily, metoprolol 50 mg daily and lantus 50 mg daily. Allergies: No known allergies. Review of Systems: He reports having loss of bladder control, frequent urination, numbness, swelling in the joint and swelling in the ankles. No hairloss, no weight loss, and no foot odor reported. Physical Examination: Vital Signs: Weight: 185 pounds, Height: 5 feet 8 inches, Blood Pressure: 114/80. General Appearance: Adult male who is well-nourished, well-developed, alert and oriented in no acute distress. He is cooperative. HEENT: Normocephalic/atraumatic. Pupils are equal and reactive to light. Neck: Supple. No JVD. No lymphadenopathy. Chest: Clear to auscultation bilaterally. Cardiovascular: Regular rate and rhythm. Abdomen: Soft, nondistended and nontender, no HSM. Extremities: No edema. Neurological: Deep tendon reflexes were symmetrical throughout. No spasticity. No Hoffman’s and no clonus. Strength is good in the upper and lower limbs. Good hand grasp.
PPAIN AWAY REHAB AND CLINICAL SSERVICES
Radiological Data: We reviewed the MRI scan of the thoracic spine obtained on 5/15/13, which revealed a chronic compression fracture at T12. There is no canal compromise seen. There is a multilevel mild degenerative disc disease. Impression: Chronic compression fracture at T12. Recommendations: We do not think surgery is indicated. Start physical therapy and a prescription was given to the patient to start this. Follow up here on a p.r.n. basis. Electronically signed by Robert Collins, DO
Name: ID# Doctor:1. History
OStatus of3 ChronicConditions
O OO Location O Severity O Timing ExtendedO Quality O Duration O Context (4 or more)
ROS (Review of Systems): O O O OO Constitutional O All/ImmunoO Eyes O Musculo O Neuro O Hem/lymph O Cardiac/ vasc.O GU O Resp O GI O Psych O EndoPFSH (Past, Family, Social History): O O O O
PROBLEMFOCUSED
9920199212
EXP.PROBLEMFOCUSED
9920299213
DETAILED9920399214
COMPRE-HENSIVE
99204/9920599215
Explanation (HPI Elements)O Severity:
Brief (1-3)O Modifying Factors
ALL INFO IN THE SHADED AREAS IS FOR THE 1997 GUIDELINES
(Is it nocturnal, diurnal or continuous? Is there a repetitive pattern?)
(Where is pt and what is pt doing when symptoms or signs begin? What factors
were present before and after?)
(What does pt do for relief? What makes symptom(s) worse? What meds have been taken? What were
results?)
(status of at least 3 chronic or inactive conditions)
(additional sensations or feelings)
(Is pain diffuse or localized? Im-lateral or bilateral? Fixed or migratory? Radiating or
referred?)
(How long have symptoms
been present?)
Final History requires all 3 componentsabove are met or exceeded
* Complete PFSH 2 history areas: a) established patients - office (outpatient) care, domiciliary care, home care; b) emergency department; c) subsequent nursing facility care; and d) subsequent hospital care. 3 history areas: a) new patients - office (outpatient) care, domiciliary care, home care; b) consultations; c) initial hospital care; d) hospital observation; and e) initial nursing facility care.
Extended(pert & others)(2-9 systems)
Pertinent1 history
item
*Complete2-3 history
areas
O Ears, nose, mouth, throatComplete(pert & all
others)(10 systems)
O Past history (the patient's past experiences with illnesses, operations, injuries and treatments)
1995 HPI Guidelines
O Social history (an age appropriate review of past and current activities) N/A N/A
OBrief (1-3)
OExtended
(4 or More)O LocationO Quality
O SeverityO Duration
O Integumentary
N/A
Pertinent toproblem
(1 system)
O Family history (a review of medical events in the patient's family, including diseases that may be hereditary or place the patient at risk)
HPI (History of Present Illness): Characterize HPI by considering EITHER the status of 3 chronic or inactive conditions OR the number of elements recorded.
O Associated Signs & Symptoms
O TimingO Context
O Associated Signs & Symptoms O Modifying Factors
(1-10, with 1 being no pain
and 10 being the worst pain
experienced)
O Quality:
New Patient OEst. Patient O
Consult O
E/M Documentation Auditor's InstructionsDate of Service:
Refer to data section (table below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table that best describes the HPI, ROS and PFSH. If one column contains three circles, draw a line down that column to the bottom row to identify the type of history. If no column contains three circles, the column containing a circle farthest to the LEFT identifies the type of history. After completing this table that classifies the history, circle the type of history within the appropriate grid in section 5.
O Location: O Duration: O Timing:
O Context: O Modifying Factors: O Assoc. Signs & Symptoms:
O Extended HPI
(Is pain sharp, dull, throbbing, stabbing, constant or
intermittent, acute or chronic, stable, improving or
worsening?)
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co

B x C = D PointsNumber Points Result 1
Max=2 1 1
1 1
2 1
Max=1 3 1
4 2
Expanded Problem Focused Exam (EPF)
Comprehensive Exam (C) 8 or more body systems
Not Applicable for 1997 Guidelines
Comprehensive Exam (C)
Refer to data section (table below) in order to quantify. After referring to data, identify the type of examination. Circle the type of examination within the appropriate grid in section 5.
Detailed Exam (D)
2-7 Body Systems - No detail of any system
required
2-7 body systemsw/affected system
in detail
Not Applicable to 1995 Guidelines
Exam EqualsOne body area or organ
system 1-5 bulleted elementsProblem Focused Exam (PF)
6-11 bulleted elements
Est. problem (to examiner); stable, improved
2. Examination
12-17 bulleted elements for
2 or more systems
18 or more bulleted elements for 9 or more
systems.See requirements for
individual single system exams
Not Applicable to 1995 Guidelines
CPT Type of Exam 95 Guidelines 97 Guidelines
Multiply the number in columns B & C and put the product in column D. Enter a total for column D. Bring total to line A in the Final Result for Complexity (table next page).
Review and/or order of tests in the medicine section of CPT
A
3. Medical Decision Making
Problem(s) StatusSelf-limited or minor (stable, improved, or
worsening)
Reviewed DataReview and/or order of clinical lab tests
Review and/or order tests in the radiology section of CPT
Number of Diagnoses or Treatment OptionsIdentify each problem or treatment option mentioned in the record. Enter the number in each of the categories in Column B in the table below. (There is a maximum number in two categories.) Do not categorize the problem(s) if the encounter is dominated by counseling/coordinating of care, and if duration of time is not specified. In that case, enter 3 in the total box.
Decision to obtain old records and/or obtain history from someone other than
patientReview and summarization of old records and/or
obtaining history from someone other than patient and or discussion of case with another
health care provider
Est. problem (to examiner); worsening
New problem (to examiner); no add'l workup
planned
New problem (to examiner);
add'l workup planned
Amount and/or Complexity of Data ReviewedFor each category of reviewed data identified, circle the number in the points column. Total the points.
Amount and/or Complexity of Data ReviewedNumber of Diagnoses or Treatment Options
Discussion of test results with performing physician
Total:Bring total to line C in Final Result for Complexity
(table next page)
Total:Independent visualization of image, tracing or specimen itself (not simply review of report) 2
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co

Level of Risk
Minimal
Low
Moderate
High
A 2 Limited
B Low
C 2 Limited
Low Complex
Use the risk table below as a guide to assign risk factors. It is understood that the table below does not contain all specific instances of medical care: the table is intended to be used as a guide. Circle the most appropriate factor(s) in each category. The overall measure of risk is the highest level circled. Enter the level of risk identified in Final Result for Complexity (table below).
Diagnostic Procedure(s) Ordered
O One or more chronic illnesses with severe exacerbation , progression, or side effects of treatmentO Acute or chronic illnesses or injuries that may pose a threat to life or bodily function , e.g., multiple trauma, acute MI, pulmonary embolus, severe respiratory distress, progressive severe rheumatoid arthritis, psychiatric illness with potential threat to self or others, peritonitis, acute renal failureO An abrupt change in neurologic status , e.g., seizure, TIA, weakness or sensory loss
O Cardiovascular imaging studies with contrast with identified risk factorsO Cardiac electrophysiological testsO Diagnostic endoscopies with identified risk factorsO Discography
Presenting Problem(s) Management Options
O Physiologic tests not under stress, e.g., cardiac stress test, fetal contraction stress testO Diagnostic endoscopies with no identified factorsO Deep needle or incisional biopsyO Cardiovascular imaging studies with contrast and no identified risk factors, e.g. arteriogram cardiac cathO Obtain fluid from body cavity, e.g., lumbar puncture, thoracentesis, culdecentisis
O Minor surgery with identified risk factorsO Major surgery (open, percutaneous or endoscopic) with no identified risk factorsO Prescription drug managementO Therapeutic nuclear medicineO IV fluids with additivesO Closed treatment of fracture or dislocation without manipulation
O Two or more self-limited or minor problemsO One stable chronic illness , e.g., well-controlled hypertension or non-insulin dependent diabetes, cataract, BPHO Acute uncomplicated illness or injury , e.g., cystitis, allergic rhinitis, simple sprain
O One self-limited or minor problem , e.g., cold, insect bite, Tinea Corporis
O Laboratory tests requiring venipunctureO Chest x-raysO EKG / EEGO UrinalysisO Ultrasound, e.g., echoO KOH prep
O RestO GarglesO Elastic bandagesO Superficial dressings
O Physiologic tests not under stress, e.g., pulmonary function tests O Non-cardiovascular imaging studies with contrast, e.g., barium enemaO Superficial needle biopsiesO Clinical laboratory tests requiring arterial punctureO Skin biopsies
O Over-the-counter drugsO Minor surgery with no identified risk factorsO Physical therapyO Occupational therapyO IV fluids
Risk of Complications and/or Morbidity or Mortality
O One or more chronic illnesses with mild exacerbation , progression, or side effects of treatmentO Two or more stable chronic illnessesO Undiagnosed new problem with uncertain prognosis , e.g., lump in breastO Acute illness with systematic symptoms , e.g., pyelonephritis, pneumonitis, colitis.O Acute complicated injury , e.g., head injury with brief loss of consciousness
Final Result for ComplexityDraw a line down any column with 2 or 3 circles to identity the type of decision making in that column. Otherwise, draw a line down the column with the 2nd circle from the left. After completing this table, which classifies complexity, circle the type of decision making within the appropriate grid in section 5.
O Major surgery (open, percutaneous or endoscopic with identified risk factors).O Emergency major surgery (open, percutaneous or endoscopic)O Parenteral controlled substancesO Drug therapy requiring intensive monitoring for toxicityO Decision not to resuscitate or de-escalate care because of poor prognosis
Number of diagnosis or treatment options
Highest risk optionsAmount and complexity
of data
4 Extensive3 Multiple
Moderate
3 Multiple
Moderate Complex
Final Result for Complexity
High
4 Extensive
High Complex
1 Minimal
Minimal
1 Minimal or low
Type of decision making Straight Forward
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co

4. Time
Time: __ yes __ no
__ yes __ no
__ yes __ no
History PF EPF PF EPF D C
Examination PF EPF PF EPF D CComplexity of Medical Decision SF
SFER: L SF L M H
Average time (minutes)
(Confirmatory consults & ER
have no average time)
99201-10NEW
99241-15OUTPT CONS
99251-20IP CONSER 99281
99202-20NEW
99242-30OUTPT CONS
99252-40IP CONSER 99282
99212
10 min.
99213
15 min.
99214
25 min.
99215
40 min.
LEVEL I II II III IV V* Level I established visit is for when a patient sees the nurse, not the doctor.
History PF INTER. D & C C CExam PF D & C C CMDM SF/L SF/L M H
Average Time15-99231
Subsequent
30-99221Init. IP99218
Obs. Care
50-99222Init. IP99219
Obs. Care
70-99223Init. IP99220
Obs. Care
LEVEL I I II IIIPF=Problem Focused C=Comprehensive EPF= Expanded Problem Focused D=Detailed L= Low H=High M=Moderate
rev 111014
* If all answers are "yes," select level based on time.
If the physician documents total time and suggests that counseling or coordinating care dominates (more than 50%) the encounter, time may determine level of service. Documentation may refer to prognosis, differential diagnosis, risks, benefits of treatment, instructions, compliance, risk reduction or discussion with another health care provider.
Does documentation reveal total time?
Face-to-face in outpatient setting; unit/floor in inpatient setting
Does documentation reveal that more than half of the time was counseling or coordinating care?
Does documentation describe the content of consulting or coordinating care?
5. Level of ServiceOUTPATIENT, CONSULTS (OUTPATIENT, INPATIENT & CONFIRMATORY), AND ER
Average Time
LEVEL
*Established Officerequires 2 components within
shaded area
Subsequent Inpatient/Follow-uprequires 2 components within shaded area
New Office/Consults/ERrequires 3 components within shaded area
99203-30NEW
99243-40OUTPT CONS
99253-55IP CONSER 99283
III
Initial Hospital/Observation/Inpatient Consult requires 3 components within
shaded area
C
C
H99205-60
NEW99245-80OUTPT CONS
99255-110IP CONSER 99285
CER:D
DER:EPF
DER:EPF
LER:M
CER:D
M
HistoryExamMDM
INPATIENT
EPF INT.DH
35-99233Subsequent
III
25-99232Subsequent
99204-40NEW
99244-60OUTPT CONS
99254-80IP CONSER 99284
II
EPF
IV
M
D interval
V
revrevrevrevevrevevrevrevrevrevrevevevevrevrevrevvrevevevvevrevevrevevvvrevrevrevreevvvvrevevevrevrevvevrevvvvvvevevvvvevvvrevevvvvvvvveevvvveeevvvvvrevv 11 11 11111111111111111111111111111111 1111111111111111111 11111111111 1111111 1111111 111111111111111111111111111 11 11 1010101101101101101110111011011011011011010010110110110111011011010110101011011011110010101011010110111 1100011001000110110101011011011011011011011011011010100010110101001010110111101010011 1110001001444444444444444444444444444444444444444444444444444444
National Alliance of Medical Auditing SpecialistsA division of DoctorsManagement, LLC
www.NAMAS.co













![HANDBOOK ON STANDARDS ON AUDITING...[Handbook On Standards On Auditing] CA NITESH KUMAR MORE INDEX OF STANDARDS ON AUDITING (SA) 100 -199 Intro ductory Matters 200 -299 General Principles](https://img.pdfslide.us/doc/110x75/5e7b9d4c5d148b587c2246cb/handbook-on-standards-on-auditing-handbook-on-standards-on-auditing-ca-nitesh.jpg)















