Embed Size (px)
DESCRIPTION
This curriculum is geared toward Deaf and Hard of Hearing students and focuses on key topics such as peer pressure, self-esteem/worth, and how to say no to tocacco use.
Citation preview
HandsOffTobacco!AnAnti-TobaccoProgramfor Deaf Youth
Cynthia B. Sternfeld, ED.S., LPCSusan M. Barnabei, B.S.Karan Kriger, B.S.Marie H. Katzenbach School for the Deaf
Debra S. Guthmann, ED.D.Frank Lester, M.S.W.California School for the Deaf, Fremont
Barbara A. Berman, PH.D.Division of Cancer Prevention and Control ResearchUCLA School of Public Health andJonsson Comprehensive Cancer Center
Annette E. Maxwell, DR.P.H.Glenn C. Wong, M.P.H.Recruitment, Retention and Communications CoreUCLA Jonsson Comprehensive Cancer Center
PDF processed with CutePDF evaluation edition www.CutePDF.com

HandsOffTobacco!AnAnti-TobaccoProgramfor Deaf Youth
This curriculum was developed through funding from TRDRP, the Tobacco Related Diseases Research Program, University of California (Grants # 10GT-3101, 12HT-3201, Barbara A. Berman, Ph.D., Principal Investigator, UCLA; Debra S. Guthmann, Ed.D., Principal Investigator, California School for the Deaf, Fremont).
We wish to express our deep appreciation to the faculty, staff, students and their parents at the California School for the Deaf, Fremont (Fremont, California), the Marie H. Katzenbach School for the Deaf (Trenton, New Jersey), the California School for the Deaf, Riverside (Riverside, California), and the Minnesota State Academy for the Deaf (Faribault, Minnesota) for their participation in this study.
We also thank Linda Oberg, M.S., M.A.; members of our Expert Curriculum Review Panel (Sook Hee Choi, M.A., Chriz Dally-Johnson, M.A., Janet Dickinson, Ph.D., Thomas Holcomb, Ph.D., Nancy Moser, LCSW, Katherine A. Sandberg, B.S., CCDCR, and Mary Skyer) for their help in the formative stages of curriculum development; Mr. Jon Levy and the faculty, staff and students of the Orange County Department of Education Regional Deaf and Hard-of-Hearing Program, University High School, Irvine, California; and Heidi B. Kleiger, B.S., Lauren Maucere, B.S., and our colleagues at the Greater Los Angeles Agency on Deafness (GLAD), Los Angeles, California, for their help and support in this program of research.
Images used for analysis, critique and description throughout this curriculum were obtained primarily from the website www.trinketsandtrash.org. Additional sources of materials include the American Lung Association and the website www.WhyQuit.com.
©2004, 2007 University of California, Los Angeles

Introduction 1
Introduction for Teachers
C IGARETTE SMOKING is the single most preventable cause of death and disease in
our society. It is responsible for approximately onein five deaths—over 440,000 deaths each year—in the United States. This is more than the numberof people killed by AIDS, alcohol, motor vehicleaccidents, homicide, illegal drugs and suicide,combined. Nearly half of all Americans who continue to smoke will die from a smoking-relateddisease. Across the globe, smoking accounts forapproximately 4.2 million deaths annually, andthis number is growing. By 2025 it is estimatedthat seven million people throughout the worldwill die from tobacco use each year.*
Is tobacco use a problem for young people?
Yes, absolutely. More than 90% of all adult smokers begin to smoke while they are childrenor teenagers. In the United States alone, morethan 4,000 young people under the age of 18smoke their first cigarette each day, and 2,000others go on to become regular, daily, smokers.That's more than 730,000 new underage dailysmokers each year. More than a third of allyoungsters who ever try smoking a cigarettebecome regular, daily smokers by the time theyleave high school. About 4.5 million youth underthe age of 18 are current smokers.
Monitoring the Future, an annual series of nationwide surveys conducted by the Universityof Michigan Institute for Social Research among8th, 10th and 12th grade students, reports thatcigarette use has been falling among Americanadolescents since the mid-1990s. But the rate ofdecline is slowing, and there is growing concernthat these gains may be near an end. And evenwith these gains, which simply offset the dramatic
increases in teen smoking in the first half of the1990s, it is important to note that a quarter ofyoung people —nearly one out of every four—are actively smoking by the time they leave highschool. Furthermore, some young people whoare not smoking in high school will begin afterthey graduate, and others who are not dailysmokers in high school will become daily smokersafter they leave school.
Initiation and development of tobacco useamong children and teenagers involves a processthat starts with attitude formation about smoking,proceeds through trial and experimentation, andall too often ends in regular use. We also knowthat several factors place children and adoles-cents at risk for starting tobacco use and becom-ing an addicted smoker. These include:
W Behavioral risk factors for tobacco use:Poor school performance, low aspirations forfuture success, school absences, and schooldropout. Other behavioral factors includerisk-taking and rebelliousness, coupled with alack of skills to resist influences to use tobac-co, alcohol or drugs.
W Environmental factors:If family members or close friends smoke;and if tobacco products are readily accessi-ble. Advertising and promotion are an impor-tant aspect of the environment, shapingyoung people's views of the utility of smokingand other tobacco use. So too are communi-ty-level factors such as the extent to whichsales to minors are restricted, the cost oftobacco products, and restrictions on smok-ing in public places. These factors influencenot only access to tobacco products, but alsothe perceived acceptability of tobacco use.
W Personal risk factors:These include aspects of a young person'sinteraction with the social environment.Smoking is most likely among youngsters withlow self esteem; who believe that tobaccouse has a valuable social function; who
* Trends and patterns change very quickly. We thereforechoose to provide only limited data in presenting this cur-riculum. The Campaign for Tobacco-Free Kids Web site(www.tobaccofreekids.org), the annual Monitoring theFuture report (www.monitoringthefuture.org or http://dru-gabuse.gov), and the Youth Tobacco Survey are only a fewof the many places on-line where there is easy access tocurrent information regarding changing patterns of tobaccouse among children and teenagers.
Hands Off Tobacco!An Anti-Tobacco Program for Deaf Youth

Introduction 2
Introduction for Teachers
believe that "everyone else smokes;" and who are susceptible to peer pressure tosmoke. Personality factors such as depression,helplessness, aggression, pessimism, and limit-ed ability to conceptualize the future havealso been found to predict smoking amongyoung people. Children from lower incomefamilies are also at greater risk for smokingthan other young people.
Although these characters increase the risk oftobacco use, the fact is that smoking initiationoccurs among young people across all behavioral,environmental and personality characteristics. Tounderstand why young people continue to smokeonce they have started, we need to take intoaccount the very real danger of addiction.
Is tobacco use addicting for children andteenagers?
Certainly. In fact, not only do most adult smokersreport that they started smoking as children orteens-most also report that they were addicted bythe time they left high school. This is why reach-ing out to young people now about avoidingtobacco use is so critical. Tobacco use and addic-tion happen very quickly.
What do we mean by “addiction?” Addiction ischaracterized by compulsive drug-seeking anduse, even when the user knows the dangersinvolved. Tobacco certainly fits this description.Most smokers identify tobacco as harmful andindicate that they would like to quit. Nearly 35million smokers make a serious attempt to stopsmoking every year. But less than 7% of thosewho try to quit on their own stay off cigarettes formore than a year. Most relapse-that is, they goback to smoking in a few days after trying to quit.
The desire to quit is not just expressed by adults.Once children and teenagers begin to smoke,they commonly believe that they can quit when-ever they choose. The truth is that quitting, evenfor a young person, is difficult to do. While someyoung smokers are able to quit before leavinghigh school, nearly three out of every four regularsmokers in high school have already tried to quitbut failed. The most important reason for this isthat tobacco products contain nicotine, a chemi-cal as highly addictive as cocaine and heroin. Andaddiction to tobacco products can occur veryquickly. Children and teenagers who try to quitfind that they experience the withdrawal symp-toms that adults experience, and this frequently
results in relapse when a quit attempt is made.Once they begin, many smokers—young andold—find themselves caught up in a cycle ofaddiction that makes quitting very difficult.
How does the Addiction Cycle work?
While much has still to be learned about theprocess of nicotine addiction, including the roleof genetics in this process, much has already beenlearned (See Figure 1).
W Nicotine is one of more than 4,000 chemicalsfound in the smoke from tobacco productssuch as cigarettes, cigars and pipes, and insmokeless tobacco products such as snuff andchewing tobacco. Nicotine is absorbed throughthe skin and mucosal lining of the mouth andnose or by inhalation in the lungs. It enters theblood stream and travels throughout the body.
W Immediately after exposure to nicotine, thereis a “kick” caused in part by the drug's stimu-lation of the adrenal gland which dischargesepinephrine—adrenaline. The rush of adrena-line stimulates the body and causes a suddenrelease of glucose, an increasing blood pres-sure, respiration, and heart rate.
W Depending on how it is taken, nicotine canreach peak levels in the bloodstream andbrain very quickly. A cigarette, for example, isa highly engineered, efficient drug-deliverysystem. The inhaled smoke from a cigarettecarries nicotine deep into the lungs where it isquickly absorbed into the blood and carriedto the heart and the brain. It reaches thebrain within about ten seconds of inhaling.
W Once in the brain, nicotine stimulates therelease of the neurotransmitter dopamine.Dopamine is involved in regulating feelings ofpleasure, and creates a “reward pathway”that encourages continued nicotine intake bythe tobacco user. Nicotine also has animpact on other brain chemicals that affectmood and performance, including acetyl-choline (arousal, cognitive enhancement),norepinephrine (arousal, appetite suppres-sion), vasopressin (memory improvement),serotonin (mood modulation, appetite sup-pression) and beta-endorphins (reduction ofanxiety and tension).
W Research indicates that other chemicals intobacco may also play a role in the addiction

Introduction 3
Introduction for Teachers
process by decreasing levels of an enzymethat break down dopamine, thereby inhibit-ing the body's ability to block the increase ofdopamine.
W After the initial “hit” of nicotine in the brain,its concentration in the blood begins to fallrapidly. Nicotine is eliminated from the bodyprimarily by the liver. In about 30 minutes thebody has cleaned out much of the nicotine.Without nicotine to provide the pleasurestimulus in the brain, a smoker then begins tofeel tired, jittery and depressed. These feelingsare symptoms of withdrawal, and trigger acraving for another dose of nicotine by smokinganother cigarette, or chewing on another plugof smokeless tobacco. Tobacco users continueto smoke or chew throughout the day tomaintain the drug's pleasurable effects andprevent unpleasant withdrawal symptoms.
W With repeated smoking during the day, nicotine levels accumulate, plateau throughthe day, and then gradually fall overnight.Many smokers describe the first cigarette ofthe day as the most pleasurable because ofthe relief it gives to withdrawal symptomsthey experience upon waking in the morning.
A typical smoker takes about 10 puffs on acigarette during the five minutes that a ciga-rette is lit. A smoker that smokes a pack ofcigarettes a day—20 cigarettes—gets 200“hits” of nicotine to the brain each day.
W As the nervous system adapts to nicotine,smokers tend to develop a tolerance to thechemical. This causes tobacco users to smokeor chew more over time to achieve the samenicotine “hit.”
W When people try to quit they frequentlyexperience withdrawal: irritability, difficultyin concentrating, sleep disturbance, increasedappetite, depression, and fatigue. These feel-ings usually last for a few days or weeks. Butthey can last longer. They can be mild orsevere. They frequently result in relapse totobacco use.
W Behavioral and psychological aspects ofaddiction are also very important and cancontribute to the craving for a cigarette. For some smokers, the feel, smell and sight of a cigarette, and the behaviors associatedwith obtaining, handling, lighting and smoking cigarettes are associated with the
1Within seconds of inhaling,nicotine speeds its way to
the smoker’s brain.
2In the brain, nicotine causes
the release of a chemicalcalled dopamine which stim-
ulates feelings of pleasureand relaxes you.
3But as soon as the person
stops smoking, this stimulationwears off as the nicotine level
in the body falls.
4The smoker’s brain starts to craveanother “hit” of nicotine—which
prompts the person to smokeanother cigarette.
5Over time, the brain
becomes accustomed tonicotine stimulation. Oncethis happens, the smokerexperiences unpleasant withdrawal symptoms if
the nicotine craving is notsatisfied.
6So the person smokes
another cigarette. And thecycle starts over again.
Figure 1: The Addiction Cycle

Introduction 4
pleasurable effects of smoking. Smokers come to associate these behaviors with a reduction in stress.
Given the difficulties in stopping smoking oncesomeone is addicted, it becomes clear why prevention—finding ways to encourage people to never start smoking in the first place—is soimportant. And because most smoking begins inchildhood and adolescence, the importance ofprevention among young people is clear. But prevention is difficult to achieve.
What makes tobacco use prevention such adifficult task?
Prevention is difficult because the act of tobaccouse—smoking cigarettes, cigars, and other tobaccoproducts, or chewing smokeless tobacco—has beenlinked to social meanings and utilities, apart fromits physiological effects, that make tobacco useattractive. The act of smoking or chewing tobaccois associated with independence, toughness,rebellion, camaraderie, sophistication, relaxationand fun. Tobacco use is perceived as being “cool.”
How did tobacco use come to have these socialmeanings? Most of this is the result of the tremen-dous marketing effort put forth by the sellers oftobacco products. First, they developed innova-tive strategies for marketing tobacco, pioneeringthe use of brand names and packaging to segmentmarkets (cigarettes for men versus those forwomen; for tough men versus the sophisticatedindividual; and those for the young). Perhapsmore important, they promoted tobacco use asnot only normal and acceptable, but as a desirable practice as well.
In the early decades of the 20th century, tobaccouse was linked to manliness, success, athleticismand more through carefully crafted marketingstrategies. As a result, before World War I, tobaccouse was primarily a male behavior. Recognizingthat few women smoked, tobacco companies in the1920s and 1930s began to market tobacco productsto women by linking smoking to thinness, emanci-pation, independence, youth, fun and beauty.
The aggressive promotion of tobacco use—espe-cially cigarette smoking—as a socially acceptableand desirable behavior resulted in a dramaticincrease in tobacco use in the 20th century, towhere more than half of all adult men and a thirdof adult women in the U.S. were smokers by the1960s. By this time, however, scientific research
had already linked the rise in tobacco use with anequally dramatic increase in lung cancer andother diseases. Spurred on by these research findings, the government, voluntary agencies andothers began to disseminate information aboutthe health effects of tobacco use. The governmentalso began to make efforts to control the marketingand sale of tobacco products. These efforts led toa greater awareness of the health risks of smokingand to declines in smoking rates since the peakyears in the 1960s. This took place first for men,and then later—and more gradually—for women.Still, the significant fact is that nearly a quarter ofthe adult American population, or about one infour adults in the United States, smokes cigarettes.
And despite what is known and continues to be discovered about the health consequences oftobacco use, the tobacco industry remains a powerful economic and political force, both inthe United States and around the world. Overone billion men and 250 million women in theworld are daily smokers-consuming 15 billion cigarettes every day-and the ranks are growingevery day. Today the tobacco industry spendsupward of $11.5 billion dollars annually on marketing in the U.S.-about $31 million dollarseach day. Some of the most familiar images inmarketing—the Marlboro Man, Joe Camel, andbeautiful Virginia Slims models to name a few—are linked to tobacco products. And marketing is only one of the many ways in which the tobacco industry has sought to gain and retainacceptance for its products and for this industry in the United States and elsewhere.
When it comes to young people, the tobaccoindustry has always denied that it markets itsproduct to children and teenagers. But the indus-try's own internal documents reveal that youngpeople have long been viewed as an importantsegment of the tobacco market. Children andteenagers are susceptible to tobacco messagesand images, teenagers are more likely than adultsto recall tobacco advertising, and a far greaterproportion of young smokers buy the top threebrands of cigarettes—those most heavily adver-tised—than do adults.
While Camel cigarettes no longer uses Joe Camelin its advertising, we can learn a great deal fromthis highly successful campaign. While this cam-paign was taking place, a study of product logorecognition of three-to-six-year-olds revealed thatover 90% of the six-year-olds correctly matchedthe cartoon Camel with cigarettes. Between 1989
Introduction for Teachers

Introduction 5
and 1993 the amount spent on Joe Camel wentfrom $27 million to $43 million. This led to a50% increase in Camel's share of the youth market.It had no impact at all on the company's adultmarket share.
We often think of peer influences and adult rolemodels as key to understanding tobacco use. And without doubt, these are critical factors weneed to take into account. But the social and cultural environment also has a direct impact onthe behavior of young people, and plays animportant role in shaping the behavior of peersand adults. Cigarettes and other tobacco productshave come to have an important place not only in adult culture, but in youth culture, as well.
What are the health and other consequences of smoking?
Condemnation of tobacco dates back for centuries. Prior to the 20th century opposition to tobacco use was often on moral and religiousgrounds. Health concerns were voiced. But theydid not emerge as the most significant argumentuntil the 20th century, when physicians andresearchers began to report the health conse-quences of this behavior. In 1964, in response togrowing calls for action, a landmark report waspublished, Smoking and Health: Report of theAdvisory Committee of the Surgeon General ofthe Public Health Service. This, the first Report ofthe Surgeon General regarding tobacco, docu-mented what was then medically known: smokingwas a cause of cancers of the lung and larynx(voice box) in men and chronic bronchitis in both men and women.
Extensive research into the health effects of smoking continued, from that time until the present, and the understanding of tobacco's rolein disease and death has grown. The SurgeonGeneral’s Report and others have carefully docu-mented many of these issues—the addictivenature of nicotine, the health consequences ofsecondhand smoke exposure, the implications ofsmokeless tobacco use—and more. In 2004, onthe 40th anniversary of the first Surgeon General'sReport, a new report, The Health Consequencesof Smoking: A Report of the Surgeon General,was published. In that report the conclusion isdrawn that smoking harms nearly every organ ofthe body, and that “smoking remains the leadingcause of preventable death and has negativehealth impacts on people at all stages of life. Itharms unborn babies, infants, children, adoles-cents, adults and seniors.”
W Smoking causes cancer and accounts for atleast 30% of all cancer deaths. Tobaccosmoke contains at least 60 cancer causingsubstances. Lung cancer is the leading causeof cancer death in men and women, andsmoking causes about 90% of lung cancerdeaths in men and almost 80% in women.Smoking is also a known cause of cancer ofthe oral cavity, larynx (voice box), pharynx,esophagus, bladder, pancreas, kidney, blood(leukemia) stomach, pancreas and cervix.
W Smoking is a cause of coronary heart disease,the leading cause of death in the UnitedStates. A smoker is four times more likely todie from coronary heart disease than a non-smoker; 21% of all coronary heart diseasedeaths in the U.S. each year are attributed tosmoking.
W Smoking causes respiratory diseases. It is aknown to cause more than 90% of deathsfrom chronic obstructive pulmonary disease(COPD), which includes emphysema andchronic bronchitis; male and female smokersincrease their risk of death from these dis-eases by nearly 10 times. Smoking causeschronic coughing and is linked to pneumonia.Smokers are more susceptible to influenza(the flu) and are more likely to experiencesevere symptoms when they get the flu.
W Smoking causes strokes, the third leadingcause of death in the United States, and circulatory deficiencies which can contributeto infection and tissue death, particularly forparts of the body like hands and feet that aredistant from the heart. It is also known tocontribute to aortic aneurysm, a dangerousweakening and ballooning of the major arterynear the stomach.
W Research has linked smoking to rheumatoidarthritis, hearing loss, vision problems (such ascataracts), facial wrinkling, gum disease (peri-odontitis), reduced bone density among post-menopausal women, hip fractures and osteo-porosis, diabetes, and to making diabetesworse for those who have this disease. It canreduce the effectiveness of medicines used totreat, for example, diabetes, ulcers, sleepless-ness and pain. Smokers who get immuniza-tions such as flu vaccine and hepatitis B vac-cine are not as well protected against the dis-ease as are nonsmokers. Smokers have alower survival rate after surgery compared tothat for nonsmokers because of damage to
Introduction for Teachers
Introduction 6
the body's host defenses, delayed woundhealing, and reduced immune response.Smokers tend to have more ulcers than non-smokers, and smoking keeps ulcers fromhealing. Smoking affects the sense of smelland smokers are more likely than non-smok-ers to snore.
W Women who smoke and take birth controlpills run an increased risk of stroke. Womenwho smoke are at increased risk for infertility.Smoking during pregnancy can cause healthproblems for both mothers and babies, suchas pregnancy complications, premature birth,low birth weight infants, stillbirths, andSudden Infant Death Syndrome (SIDS).Smoking by fathers prior to conception mayhave health consequences for their offspringsas well, even when the mother does notsmoke. Children exposed to secondhandsmoke after birth are at a greater risk of child-hood wheezing, respiratory tract infections, ofgetting or worsening asthma, of chronic respi-ratory symptoms such as colds, coughs, sorethroats, stuffy noses, and middle ear infec-tions, of poorer lung function, increased heartrate, complications after surgery and higherblood levels of lead, a toxic metal.
W Smoking has been linked to erectile dysfunction in men.
W Adults exposed to secondhand smokeincrease their risk of heart disease morbidityand mortality, lung cancer, eye and nasal irritation, pneumonia and other respiratoryinfections.
W Socioeconomically, the costs of smoking arehigh. The financial costs of smoking-relateddiseases are borne by society in the form ofhigher health insurance costs and greaterhealth care expenditures, especially in thepublic, taxpayer-financed health care system.The economic costs include lost productivityin the workplace due to smoking-related illness and premature death. These costs arestaggering. It is estimated in the United Statesthat smoking costs $75 billion in direct medicalexpenses and $82 billion in lost productivityevery year. And there are the additional costsof dealing with the more than 140,000 smoking-related fires in the U.S. each year.
But what do these health impacts mean to youngpeople?
Research has clearly shown that the earlier youngpeople begin to smoke, the greater their risk ofdeveloping smoking-related diseases in adulthood.However, the primary difficulty in communicatingthese health effects to young people is that manyof the most graphic consequences of tobaccouse—lung cancer, heart disease, oral cancer, strokesand so forth—are far off in the future and beyondthe horizon as far as an adolescent is concerned.In a youth-oriented anti-tobacco curriculum, it isimportant to emphasize both the immediatehealth and social consequences of tobacco use.
What are the immediate health consequences oftobacco use for young people?
W First, a young person's lung function is imme-diately impaired, and the effects are consistentwith early signs of obstructive airway disease.What does this mean? Some lung tissue damage occurs, diminishing the ability of thelungs to take in oxygen. This damage getsprogressively worse the more one smokes.Not surprisingly, young people who smokeare less physically active, perform more poorlyat all levels of physical exertion, improvemore slowly with training, and have poorerendurance overall than non-smokers.
W Smoking slows the normal development andgrowth of a young person's lungs. This meansthat young people who take up smokingwhile their bodies are still growing may bepermanently stunting their lung capacity. Thishas been shown to be especially the case forgirls who take up smoking.
W Smoking contributes to the onset of asthma,and can greatly aggravate an existing asthmacondition.
W High school seniors who smoke rate their over-all health more poorly than do nonsmokers.They are more likely than non-smokers to reportexperiencing cough with blood or phlegm,shortness of breath when not exercising, andwheezing and gasping. Young smokers are morelikely to suffer exercise-related injuries thantheir non-smoking peers, and heal more slowlyfrom injuries. Over time, smoking causes pre-mature wrinkling of skin.
Introduction for Teachers

Introduction 7
W There is evidence that smoking is sometimesa first step towards other substance use.Young people age 12-17 who smoke aremore than 11 times as likely to use illicitdrugs and 16 times as likely to drink heavilyas young people who do not smoke.
W But the damage is not confined to tobaccothat is smoked. Smokeless (chewing) tobaccocauses mouth sores and gum disease, even ata young age. Oral and nasopharyngeal cancersare less commonly seen, but can also occur atyoung ages. Both smoking and smokelesstobacco lead to bad breath, yellowed teeth,stained fingers, dulled taste buds, and adulled sense of smell.
W Of course, the most insidious impact of youthsmoking is that those who start smoking at ayounger age are more likely than later startersto develop a long-term addiction to tobacco.The younger a person starts, the greater thedifficulty in quitting tobacco at a later age.
Smoking also has social and economic consequences for young people.
W Some of the effects on personal grooming—bad breath, yellowed teeth, and discoloredfingers—have already been mentioned. Addto this list the smoky odor in hair and clothing,and burn holes in clothing. Smoking maychange social relationships with others,including family, girlfriends or boyfriends,non-smoking friends, teachers, employers,athletic teams and other social groups. Thereare a host of social consequences related tothe act of smoking itself, such as getting punished for breaking school rules, beingasked to step outside of restaurants, or gettingcited for smoking in a public place. Many ofthese social consequences may be moreimmediate, and therefore more important toyoung people, than the long-term health consequences of tobacco use.
W Economically, smoking is an expensive activity.As a daily habit, smoking or chewing tobaccorepresents a high opportunity cost for youngpeople. At anywhere between $3 and $5 perpack of cigarettes, smoking represents a greatdeal of foregone savings or purchases of othergoods, entertainment or services.
What efforts have been made to change theacceptance of tobacco in our culture? Whatcan we do in the future?
The rising prominence of tobacco use in this andother countries has been accompanied by move-ments that seek to control or restrict this behavior.Some of these earliest movements were based on“moral” or “hygienic” concerns. By the mid 20thcentury, the anti-tobacco effort began to crystallizearound the increasing scientific awareness of thehealth consequences of smoking. This growingawareness provided the impetus for new anti-tobacco efforts by government, as well as volun-tary agencies such as the American LungAssociation, the American Cancer Society and theAmerican Heart Association. Today, these groups,together with a host of academic, educational,professional, legal, private and grassroots organi-zations play a significant role in the struggles toprevent tobacco use; educate the public; regulatetobacco distribution, sales and marketing;demand moral and financial accountability fromtobacco companies for the costs of smoking; fightfor non-smokers rights to smoke-free air; craftordinances to limit smoking in public places;examine the marketing practices of tobacco com-panies worldwide; shed light on the politicalstrategies of this industry; and conduct all of theother activities that have become hallmarks of theinternational anti-tobacco movement.
The anti-tobacco movement has become a signifi-cant force for change. Its efforts have contributedto a reduction in tobacco use in our country andother industrialized nations, and steps are beingtaken to ensure international cooperation intobacco control efforts. The World HealthOrganization's (WHO) Framework Convention forTobacco Control, is a pioneering example of suchcooperation. It provides a framework for nationsto work, and work together, to contain the rapidlyspreading tobacco epidemic.
What has been learned to date suggests that nosingle approach can, alone, solve the tobaccocontrol problem. Diverse approaches are needed,and comprehensive programs that include multiplestrategies seem to have the greatest impact.
Economic approaches, such as increasing the costof cigarettes, are seen as key to tobacco control.Research indicates that for every increase of 10%
Introduction for Teachers

Introduction 8
in the cost of cigarettes there is a decline of about4% in tobacco use, and that this impact is greatestamong young people. Increasing the tax on tobaccoproducts is one way to increase their cost.However, the average price of cigarettes and theaverage cigarette excise tax in this country arewell below those in most other industrializedcountries. The taxes on smokeless tobacco prod-ucts are well below those on cigarettes. Othereconomic approaches relate to efforts to reducethe supply of cigarettes, such as by removingprice supports, ensuring that our trade policiesdiscourage—not encourage—the exporting oftobacco products to other countries, and byestablishing and enforcing laws that prevent thesmuggling of cigarettes.
Efforts to limit tobacco industry advertising andpromotion have been attempted since the 1960s.In 1965, general health warnings were placed oncigarette packages. While seen at the time as animportant step forward, placement of these weakmessages in fact prevented any further federal,state or local requirements for health messages.The enactment of the Comprehensive SmokingEducation Act of 1984 (Public Law 98-474)required four rotating warnings on cigarette pack-ages, but failed to adopt other Federal TradeCommunication (FTC) recommendations forstronger messages on packages. Far stronger mes-sages, including visual images, have been enactedin other nations, such as Canada and Brazil.
In another attempt to control advertising, success-ful court action in 1969 invoked the FairnessDoctrine to require broadcast media to air anti-tobacco advertising (at no charge) to counter thepaid tobacco advertising on television and radio.Evidence suggests that the anti-tobacco advertise-ments had considerable impact on the public'sview of cigarettes that alarmed the industry. In1971, the tobacco industry agreed to a ban onthe advertising of tobacco products on broadcastmedia, in part because the legislation also elimi-nated the Fairness Doctrine requirement that ledto the airing of anti-tobacco messages.
Although this agreement was hailed as an importantstep forward for tobacco control, evidence suggeststhat it did little to reduce the advertising and mar-keting efforts of tobacco companies. Tobaccocompanies dramatically increased their print and“point of purchase” advertising; placement oftobacco products in movies; the use of promotion-al logo and brand name items; sponsorship of cul-tural, sports, and other events; as well as politicalcontributions to seek less restrictive legislation ontobacco production, sales and marketing activities.
The growing body of evidence about the healtheffects of environmental tobacco smoke exposurefor children and adults has led to widespreadclean indoor air regulation since the 1970s. Grass-roots action by non-smokers has played a vitalrole in the passage of laws, policies and rules that,
Introduction for Teachers
U.S. entryinto WWI
Great Depression
U.S. entryinto WWII
First modernreports link
smoking andcancer
1964 SurgeonGeneral’s Report
Broadcast advertising ban
Fairness Doctrinerequires free time for anti-tobacco ads
Non-Smokers’Rights Movement
begins
Federal cigarette tax
doubles
Number ofcigarettes
Year
Figure 2. Adult per capita cigarette consumption and majorsmoking and health events, United States, 1900-1999
1998 MasterSettlementAgreement

Introduction 9
today, limit—and in many instances entirely elimi-nate—smoking and exposure to ambient smokein many settings. These include governmentoffices, public places, eating (and drinking) estab-lishments, work sites, military establishments, anddomestic and many international airline flights.Anti-tobacco activists continue work towardsincreasing this regulation in indoor and outdoorsettings, and in encouraging smokers to maketheir homes and cars “smoke free.”
Restricting the access of minors to tobacco prod-ucts has widespread approval. All states prohibitsales or distribution of tobacco to minors, andrecent advances have limited where vendingmachines selling cigarettes can be placed, toreduce the likelihood that they will be used bychildren or teenagers. However, it is not clear thatyoung people have difficulty in obtaining tobaccoproducts, and efforts continue to be made toensure that local ordinances are in place and vigorously enforced.
Significant steps have been taken to help peoplemanage their nicotine addiction. These haveincluded developing and disseminating self-helpmaterials, and strategies that can be used byphysicians, nurses, dentists, and other health careproviders to assist their patients in quitting. Strideshave been made in developing effective pharma-cologic interventions, such as, for example, nicotinereplacement products. Past and current efforts havealso focused on developing products that result in“harm reduction” for tobacco users who do notquit. Encouraging cessation is an important elementof prevention. As smokers and other tobaccousers quit, the health and other consequences oftobacco use decline. As more and more peopleenter the ranks of those who don't smoke or usesmokeless tobacco, acceptance of tobacco use inthe community begins to decline, as well. Normsbegin to change.
Since the 1950s, people have been suing thetobacco companies, using several different privatelitigation strategies. In 1998 a Master SettlementAgreement was negotiated by the tobacco indus-try with 46 states and the District of Columbia,five commonwealths and territories. (The fourremaining states had already successfully sued theindustry.) In exchange for relief from some typesof litigation, the tobacco companies paid a largesum of money, and agreed to change aspects ofits past practices, such as placement of tobaccoproducts in movies and advertising targetingyoung people. The tobacco companies were also
required to fund the American Legacy Foundationwhich has pursued tobacco prevention via itsTruth campaign, support of research, and otheractivities. The hope that states would use fundsthey received in the Settlement to further supportanti-tobacco programming has not, for the mostpart, been realized. It is not clear how dramaticallytobacco industry activities have changed.Litigation continues to the present.
Finally, the anti-tobacco movement has sought to“get the word out”—to educate the public notonly about the health and other consequences oftobacco use, but also about the activities of thetobacco industry. Learning about the industryfrom its own internal documents, made availablefrom industry “insiders” and through litigation, hasbeen an important part of this process. Mass mediacampaigns have played an important role, as well.
The goal of changing adult culture, norms andbehavior has been central to these and othertobacco control efforts. So too has working withchildren to prevent the uptake of tobacco use inthe first place. And, as is so often the case when itcomes to children, this has brought anti-tobaccoactivists and researchers to the school-house door.
What efforts have been made to bring tobaccoprevention to schools?
School-based efforts to encourage young peoplenot to smoke began in the 1960s. The earliestprograms were based on an Information-DeficitModel. These programs assumed that young peo-ple did not know or fully understand the dangersof smoking, and if they did, they would choosenot to smoke. Unfortunately, these programs,which were geared to providing informationabout the health consequences of tobacco use,did not work. They failed to consider the complexlink between knowledge and behavior, that youngpeople would not consider health consequencesthat might occur sometime in the future as rele-vant to their lives, the role of environmental andindividual forces and factors in tobacco use, andthe role of addiction.
To address the limitations of this approach, duringthe 1970s researchers shifted their focus to devel-oping and testing programs based on an AffectiveEducation Model. These programs reflected theobservation that the use of cigarettes was associat-ed with negative or antisocial patterns of adoles-cent behavior. Educators concluded that thesepatterns—and in turn behaviors such as smoking—
Introduction for Teachers

Introduction 10
Introduction for Teachers
refl ected reduced levels of perceived self-worthand poor attitudes toward family, school andcommunity. Affective Education Model preventionprograms focused on clarifying values, buildingself-esteem and a sense of self-worth, and teach-ing general skills such as assertiveness, communi-cation, and problem solving. While these programsdid not work either—indeed, in some instancesthe concern was that they even generated interestin the behaviors they were attempting to discour-age—one positive outcome was that researchersbegan to pay more attention to exploring whyyoung people smoke. They also recognized thatno program would work without addressing theunderlying reasons for this behavior.
A third approach to prevention, known as theSocial infl uences Resistance Model, evolved in the1980s. These programs drew on previous effortsand on the unfolding understanding of the com-plex issues involved in tobacco use by young peo-ple, while focus on recognizing, managing, andresisting the social infl uences that encouragetobacco use. These programs emphasize not onlythe impact of factors in the immediate environ-ment—the role of peers and friends, siblings andparents—but also the infl uence of the wider com-munity and culture, including the mass media andtobacco industry marketing. It is also consideredimportant that students develop an understandingof the norms regarding tobacco use—that mostpeople, including most young people, don’tsmoke regularly and that smoking is increasinglylooked upon negatively by many people of allages. Insight into the addiction process, the shortand long-term consequences of tobacco use, andthe process of cessation are often included.
Anti-tobacco education continues to be a “workin progress.” While we continue to do researchand to learn, we know that:
✷ The peak years for fi rst trying to smoke are the sixth and seventh grades, between the ages of 11 and 12, with a considerable number of young people starting earlier. Therefore, prevention programs in school need to be initiated in middle school or even earlier) and should be continued throughout the high school years. Beginning in high school is too late.
✷ The effectiveness of programs is dose related. A greater number of educational contacts over a longer period of time yield larger and more enduring smoking prevention effects.
✷ School programs are more effective when they are part of a broader, community strategy, when mass media elements are included, and when family members are involved.
✷ While some kinds of information may not be useful in tobacco prevention—such as a focus on long term health consequences using scare tactics—information about the tobacco industry’s infl uence and about secondhand smoke exposure seems to be important to young people.
✷ The impact of social infl uence programs does not seem to be reduced when these programs include more than tobacco—for example, when these programs seek to address other substance use behaviors often linked in the behavioral development of young people.
✷ Various personnel—staff, students—have successfully delivered these programs. These programs have been successful in urban, suburban and rural schools serving diverse populations.
✷ For school programming to be effective it needs to include tobacco-free policies involving faculty, staff, and students and relating to all school facilities, property, ve-hicles and events.
✷ Special programs—guest speakers, special events—cannot be substituted for repeated, intensive, focused classroom programming.
Can self-esteem, the ability to make healthfuldecisions, the skills needed to resist peer andother pressures be taught? Can they be taught in afew sessions in a tobacco-related curriculum? Isthe school the best place to convey these impor-tant lessons? These are not easy questions and wedo not minimize the challenges. But evidencesuggests that intensive, sustained school-basedprogramming can make a difference.
Why tailor a program toDeaf/Hard-of-Hearing youth?
We have sought to develop a tobacco prevention curriculum for Deaf children and adolescents that can help to ensure that these youngsters grow up to be “smoke free.” Our program incorporates what is today known regarding effective anti-tobacco

Introduction 11
education. It is the first-ever effort of its kind toprovide Deaf youth with a comprehensive tobac-co-prevention program that is tailored to their cultural and linguistic needs. We developed thisprogram because we are committed to the beliefthat the ongoing effort to reduce and eliminatetobacco use among young people needs to reachall youngsters.
We also believe that Deaf youngsters are at riskfor tobacco use. We know that children and ado-lescents that struggle with issues of social accept-ance and self-esteem, who experience communi-cation barriers, and who face difficulties when itcomes to school performance, are at great risk fortobacco use and other risk taking behavior. Werecognize that Deaf youth often face these andother challenges. Data regarding tobacco useamong Deaf youngsters is sparse. But in a surveywe conducted among over 400 Deaf/Hard-of-Hearing high school and college students inCalifornia, we found that there is considerableexperimentation with cigarette smoking in thispopulation. Among the 226 high school partici-pants in our study, 45% reported ever havingsmoked cigarettes. The rate was 65% among the241 college students we interviewed. Anecdotalreports from educators, community agencies, andhealth care providers confirm that tobacco use is aproblem among Deaf/Hard-of-Hearing youngsters.
In seeking to craft our program we have called onthe expertise of educators with long experience inDeaf education and in curriculum building for thispopulation, as well as on researchers in the fieldof tobacco prevention and control.
We have adopted a Social Influences ResistanceModel approach to the particular needs of thisstudent population, ensuring that all aspects ofthe program are appropriate and meaningful forDeaf youth, with varying needs, at each gradelevel. We have sought to utilize many visual aidsand illustrations. We have emphasized hands-onactivities. In some instances we have included agreater focus on “information”—for example thehealth consequences of tobacco use—than wouldlikely be provided to hearing youth. We do thisbecause experts in education for this populationhave emphasized to us that Deaf/Hard-of-Hearingyouth may lack access to this information throughthe incidental health communication that reacheshearing young people via mass media and in thedoctors office. This focus on the health implica-tions of tobacco use is certainly not a substitutefor other key elements of the program. We utilizethe D.A.R.E. resistance framework because of its
place in some Deaf/Hard-of-Hearing educationalsettings. We recognize that tobacco use is only oneof many extremely important health issues thatneed to be included, where possible, in what is analready full academic curriculum. To address thisissue we have sought to take steps to organize ourcurriculum in ways that can facilitate its usefulnessand place a minimal burden on the school staff.
How is our curriculum organized?
We have established basic themes which weaddress at every grade level. These include:
Self-esteem and self-conceptThe influence of friends and peersDecision-makingThe influence of tobacco industry marketingThe health effects of tobacco useThe addiction cycleAnti-tobacco efforts and social action
We take the approach of returning to these themesat each grade level. We do so because we believethat these are basic issues that deserve to be revis-ited throughout the middle and senior high schoolyears. We also recognize that students may not beexposed to six years of programming and thus“depending” on prior introduction of material inprevious years would not be appropriate.
However, we also recognize that these are overar-ching themes and the way they are approachedshould vary for students of different ages. In rec-ognizing that material should not simply berepeated from year to year we therefore proposea variety of examples and different projects andactivities. We also make recommendations ineach module that can assist faculty in choosingthemes and topics for classroom discussions andactivities that make best sense in diverse settings,and, in particular, where student requirementsvary, even at a single grade level.
We have had as a guiding principal the view thatthis curriculum can be utilized—in whole orpart—in a range of educational environments. Itcan be implemented in residential programming,in a classroom in a Deaf school, or in a main-stream setting. There are modules that can beused in teaching math, science, social studies andother subjects. They can be utilized in a self-con-tained classroom or as part of a school-wideeffort. Elements of the program—or the programas a whole—can be introduced on a “standalone” basis. Or tobacco prevention can be incor-porated into educational programming that targets
Introduction for Teachers

Introduction 12
Introduction for Teachers
How the Lessons are Organized
Self-Esteem and Self-Concept
Friends and Peers
Decision Making
Media and Other Infl uences to Use Tobacco
Resisting Infl uences to Use Tobacco
Health Effects of Tobacco Use
Addiction
Anti-Tobacco Efforts and Social Action
TopicGrade Level
5th 6th 7th 8th 9th 10th 11th 12th
diverse risk taking behaviors that are of critical importance to young people today and that are certainly of concern among educators of Deaf youth—other substance use, AIDS education, safe sex and more.
We have sought to create a “user friendly” tobacco prevention curriculum that teachers can integrate into their work without having to do additional research or to search for other materials. The cur-riculum for each grade level has a cover sheet that lists needed materials and preparations for each lesson. Using the curriculum will require some advance planning. For example, you may need to contact a speaker or arrange for equipment. Most
materials and all the worksheets for the students are provided on the accompanying CD, but you may have to make copies or transparencies, or adapt materials for use with technologies such as the SmartBoard. All of the images used through-out are also included on the CD as digital fi les, and can be inserted into documents or PowerPoint slides as needed. Homework assignments may also be completed as classroom activities. To minimize the burden on faculty we have not included detailed references to the extensive body of tobacco-related research that serves as the framework for this pro-gram. However, we realize that teachers may seek more information, or may want to direct students to the resources available in this fi eld. With this in
5-1
5-2
5-35-4
5-35-4
5-5
6-16-2
6-36-4
7-1
7-2
7-37-4
7-67-7
7-5
8-1
8-2
8-3
8-5
8-4
8-6
8-7
9-1
9-2
9-3
9-7
9-4
9-5
9-6
10-1
10-3
10-2
10-4
10-5
10-610-7
11-1
11-2
11-7
11-3
11-4
11-511-6
12-1
12-2
12-5
12-6
12-3
12-4
12-7

Introduction 13
Introduction for Teachers
mind we have provided a brief list of references as a starting point. We would be pleased to pro-vide additional references, citations, and materials. Please contact us at:
Debra S. Guthmann, Ed.D.California School for the Deaf, [email protected](510) 794-3684
Barbara Berman, Ph.D.Division of Cancer Prevention and Control ResearchUCLA School of Public Health andJonsson Comprehensive Cancer [email protected](310) 794-9283
A Word about Smoking Cessation
It used to be thought that smoking cessation was only an adult issue. We now know better. Many young people who start to smoke want to quit, but fi nd that they have become addicted tobacco users and that it is hard to stop.
Important strides have been made in identifying cessation strategies that are effective among young people. Dissemination—getting these programs to the teenagers that need them—is a challenge that needs to be faced. Providing school-based cessation programming for these children and teenagers is one of the critically important ways in which this can be done.
While we introduce cessation in Lesson 12-6, provision of a cessation program is beyond the scope of this prevention curriculum. We encourage educators and health care providers serving Deaf and Hard-of-Hearing youth to recognize the impor-tance of such programming, and to seek ways to provide this vital service for their students. Contacting local and State Health Departments and
the Centers for Disease Control and Prevention (CDC) is one way to begin. So too is contacting local chapters of voluntary agencies such as the American Cancer Society, the American Heart Association, and the American Lung Association. For example, the ALA currently has two evaluated cessation programs for young people—NOT-ON-TOBACCO® and Tobacco-Free-Teens® that can be adapted for use among Deaf/Hard-of-Hearing students.
Evaluation of the Curriculum
We developed and evaluated our curriculum through a research project funded by the State of California Tobacco-Related Diseases Research Program. As part of this research effort we asked a group of skilled teachers of Deaf/Hard-of-Hearing young people to help us draft the curriculum. We then asked educators at two Schools for the Deaf to adopt our curriculum, put it to use, adapt the content as necessary, and to share with us their experiences. We asked these teachers to help us understand if the program was useful, what parts of the curriculum “made sense” in the setting in which they teach, and what advice they would give to other educators seeking to use this as a learning tool.
What did we learn?
Our curriculum received praise.
Over 75% of the faculty evaluating specifi c elements of the program rated both the content of the curriculum and suggested classroom activities as “excellent.” Over 80% described the ease of use, appropriateness for grade level, and appropri-ateness for deaf youth as “excellent.”
Other comments regarding specifi c aspects of the curriculum are on the pages that follow.

Introduction 14
Introduction for Teachers
The curriculum provided useful tools, and was well-organized and well laid-out for demonstrat-ing the concepts of tobacco use and prevention.
“There is plenty in the curriculum. Nothing needs to be added. The content is good…”
“Curriculum was WOW, very benefi cial!”
“I was dazzled by the curriculum, the color, [and] the pictures. It is very user friendly.”
“It’s easy to follow and easy to use.”
“The [curriculum] allowed for great fl exibility for me to go to different grade levels to get information and activities that I needed.”
The emphasis on graphic and visual elements was seen as very valuable.
“The graphics provided for this lesson are great! I’ve used them all.” (10-2)
“This lesson is one of my favorites. It is very visually ‘impactive’ with a lot of good graphics.” (10-4)
“Pictures are worth a thousand words…this generated discussion.” (11-3)
“The picture and articles with information were powerful and students were responsive to them.” (12-3)
“Students loved the pictures.” (12-5)
“Visual activities worked for both high and low functioning students.”
Specifi c lessons and content elements were described as particularly valuable and appropriate for the students.
“Advertisements were good visuals for both higher level class as well as lower level classes.” (9-3)
“(I) used the journal idea to create class discussion.” (7-7)
“The stat(istics) help to make points.” (7-7)
“Students really liked the interview process.” (12-4)
“Kids with good language skills really enjoyed the “Lights, Camera, Action” activity.” (8-3)
“Students liked the role play.” (8-3)
“The students really enjoyed refusal skills roulette.” (8-4)
“Tobacco ads on CD were very helpful. They loved interviewing the staff.” (8-5)
“The class can benefi t from this content.” (9-1)
“They liked the inventory list and ‘What’s My Line.’”(9-1)
“Vocabulary words were helpful. (The) DARE worksheet was good. Not everyone remembers DARE. (I) had to review (it).” (11-2)

Introduction 15
Introduction for Teachers
The teachers who used the curriculum felt that it did a good job of conveying the risks of tobacco use, the activities of the tobacco industry, and other important tobacco-related issues – of teach-ing the subject matter.
“Students talked about family member smoking in home or car, and asked what to do about the situation. Good lesson to introduce myths of smoking, and how smoking is often viewed by young people.” (7-4)
“The notion of (the) ‘smoking is cool’ activity is great. It made students think what the advertisement is trying to portray.” (7-7)
“Students were surprised at the variety of tobacco products. They would not have recognized them.” (8-5)
“Students enjoyed making anti-smoking advertisements.” (They) made anti-smoking advertisements that we thought Deaf might like.” (9-7)
“The graphic of (the) addiction cycle in this lesson was a great asset to have. I liked the list of withdrawal symptoms. It was good to repeat the point of why young people start smoking.” (10-5)
“Excellent coverage on how tobacco can affect many parts of the body.” (12-3)
“It was helpful to break down the topic on addiction such as cycle, withdrawal, etc.” (12-4)
“Students related to quitting smoking and the activity trying to quit. They were also interested in fi nding info from school and surveying our own students.” (12-6)
“Students don’t often get to see anti-tobacco messages, so this is a good time and place to show them the messages.” (12-7)
The curriculum was praised for the ways in which it generated good discussions and created learning opportunities in areas well beyond tobacco education.
“This is an excellent starter topic, and helps students see their own strengths.” (7-1)
“(The lesson) helped students consider ‘sensitive issues’, e.g., family smoking and what students can do (about it)” (7-4) (7-6)
“The information on the addiction cycle was used in another situation, especially about drugs. The lessons are worthwhile to repeat for each grade level.”
“Teachers used the curriculum as a jumping off point for the more meaty discussions.”
“Students liked to share their life-experience stories.”
“Also useful were problem-solving discussions to talk about how to deal with diffi cult issues faced by students. i.e., what to do when you are ‘stuck’ with parents who smoke in the house.”
“Lots of sharing and refl ecting…Refl ection is a big part of retention and education. Refl ection is the top of the educational pyramid. If they can refl ect and share opinions that is the top.”
“(This lesson) elicits good discussion among those with good communication skills.”
“Discussing different consequences… helped students to get the big picture and see the future.” (8-6)
“We had a good discussion on friendship.” (7-2)
“My lower level class discussions were less productive but still got the point.” (10-1)

Introduction 16
Introduction for Teachers
We also received some constructive criticism and were informed of way that educators enhanced or could enhance the curriculum.
Changes were made or suggested to maximize the value of the planned activities:
“I used other sources and added what I needed.”
“Emphasis could be made on refusal skills because tobacco could be a gateway to other risky behavior.”
In a number of instances homework and individual assignments were done together as a classroom activity.
“Instead of doing the warning label worksheet (designed as an individual activity), we did the activity as a whole class. Students would come up with ideas of how warning labels should be.” (7-5)
“Students designed their own warning label to place on cigarette boxes.”
To ensure non-threatening content and student safety…
“Rather than ask students about their own characteristics, “I think I’d like to hand out inventories/”What’s My Line” that are fi lled in (for) a fi ctional person and (which can then) generate a discussion on how this person can improve self-esteem.” (9-1)
To enhance communication…
“(It is) diffi cult to express in written form. (I) did it through the air.” (8-2) “I made a Power Point (presentation for the lesson).” (8-2).
“used the journal idea to create class discussion.” (8-3).
“needed to explain the sarcasm behind the pictures.” (9-7)
“A Power Point presentation was developed for each lesson making the class more visually impacting. That helped [keep] the students’ attention. Some students like to see the information in English, which was presented on the screen.”
(Praised the lesson but added) “I used Microsoft Galley Clib of fi sh and hook to illustrate my point of getting hooked and addiction…” (10-5).
“(I) want to try digital camera to generate images of emotion and have students generate (through pictures) things that make them feel this way.“ (9-1)
One teacher put together pictures of different physical systems (respiratory, nervous, skeleton, muscular, etc.) and showed how smoking may have affected each system.
The values of cigarettes in the 1980’s were not used because students could not relate to that period of time. So, the teacher obtained a catalog from Toys R Us and had the students compare the current value
of cigarettes to different products from that store.It was suggested that experiential speakers be invited to take part and to discuss ways to stop smoking. Teachers sharing their own experiences would also be helpful.
Teachers need to capitalize on other technologies such as the board maker and V-Com’s CD’s with signs in .gif and .mov formats.

Introduction 17
Introduction for Teachers
Refl ecting on the 8th grade curriculum she taught, one teacher indicated that “it may be better to do the self-esteem [and other early lessons] after the content lessons. The content lessons were more of a “hook” for the students.” Also, the suggestion was
made that the self-esteem and decision making lessons be embedded into the other content lessons, that counselors be invited to co-teach and help out with the self esteem lessons, and that self-esteem be included as an important theme in all levels.
We will further evaluate the impact of our program through survey data collected among students and faculty, including faculty plans for providing tobacco education programming in the future. This informa-tion will be published in the research literature and communicated to educators serving Deaf/Hard-of-Hearing youth.
We welcome comments from educators who adopt this curriculum. Please contact Dr. Debra S. Guthmann at:
for more information about where to obtain a copy of this curriculum at no cost.
We thank you for your help and support in this effort!
To maximize the value of lessons for students at varying skill levels…
“Levels of function were sometimes low so I used various grade levels in the curriculum and made modifi cations.”
“For 9th grade, many of the kids can’t read so I used various grade levels in the curriculum and signed information in ASL.”
“Facts are easier to teach to children with learning diffi culties than abstract concepts such as feelings and self-esteem.”
“Students could not initiate/identify each tool. I role played each with the word as a demonstration…(and) only show two tools at a time. (I) let them pick one.” (9-1)
“Homework…(was) appropriate for advanced students.” (11-1)
“Matching, scrabble words, word search, and spelling worksheets are best for special needs.” (11-3)
“Replace some defi nitions with …pictures.” (11-4)
“I had to bring everything down a few levels to help them understand.”
Educators expressed that effectiveness relies on preparing in advance and sharing successful adapta-tions with colleagues …
“The curriculum should allow for and communicate that teacher discretion is the key in terms of content and order of presentation.”
“The goal for next year is to break the lessons down more, and do different lessons in different classrooms. Some of the lessons may be appropriate in reading class, i.e. media. Some of the lessons on different body systems may be well taken in biology/science class.”

Resources 18
Additional Resources for Teachers
Additional Resources:
You can use the following resources to obtain additional information about the issues of tobacco use prevention and youth. They can also be ideal sources for students who are interested in conducting additional research, or who may want to become involved in the anti-tobacco movement in their school or community.
The Centers for Disease Control and Prevention
The Centers for Disease Control and Prevention is the lead federal agency for developing and applying disease prevention and control, environmental health, and health promotion and education activities designed to improve the health of the people of the United States. The CDC maintains the following resources for educators and students:
Tobacco Information and Prevention Source (TIPS)www.cdc.gov/tobacco/index.htm
An excellent resource for tobacco-related information that is ideal for educators and students.
Healthy Schools Healthy Youth!http://www.cdc.gov/HealthyYouth/index.htm
A resource for schools and educators that presents the latest information on school-based health education for youth.
Local Voluntary Organizations
The following are all nationwide, community-based voluntary organizations that, as one part of their overall mission, engage in tobacco-related research, education, patient service and advocacy. All maintain local community offi ces that can be valuable resources in providing printed materials, or access to networks of volunteers who can present educational programs for schools and community groups. They can also make referrals to community-based programs addressing such issues as smoking cessation. Access the organizations, and fi nd your local community offi ce, at the following online addresses:
The American Cancer Society at www.cancer.org
The American Heart Association at www.americanheart.org
The American Lung Association at www.lungusa.org
Local and State Departments of Health
Contact your local and State Health Department to identify who is responsible for tobacco-related education. Most departments of health maintain websites that can be accessed through on-line search engines such as Google at www.google.com.

Resources 19
Additional Resources for Teachers
Reports of the Surgeon General www.cdc.gov/tobacco/sgr/index.htm
These are excellent, detailed reports on a number of issues relating to tobacco use. In the curriculum we have referred to the following specifi c reports, but all of these reports are of great value as well. They are all available at the web address above.
✷ U.S. Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Offi ce on Smoking and Health, 2004.
✷ U.S. Department of Health and Human Services. Reducing Tobacco Use: A Report of the Surgeon General. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Offi ce on Smoking and Health, 2000.
✷ U.S. Department of Health and Human Services. Preventing Tobacco Use Among Young People: A Report of the Surgeon General. Atlanta, Georgia: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Offi ce on Smoking and Health, 1994.
Non-Profi t Advocacy Organizations
Many of the following organizations were established to achieve specifi c anti-tobacco-related goals, including:
✷ Providing public education about the dangers and societal costs of tobacco use
✷ Advocating for changes in government policies to reduce tobacco use
✷ Exposing activities of the tobacco industry in marketing and extending the sale of tobacco products
✷ Encouraging social action to control and reduce tobacco use
✷ Providing resources for smoking cessation
Campaign for Tobacco-Free Kids®
www.tobaccofreekids.org
The Campaign for Tobacco-Free Kids is a private, non-profi t organization committed to protecting children from tobacco addiction and secondhand smoke.
www.WhyQuit.com WhyQuit is an online forum devoted to providing support for nicotine dependency cessation, and youth dependency prevention.

Resources 20
Additional Resources for Teachers
Non-Profi t Advocacy Organizations (continued)
The American Legacy Foundationwww.americanlegacy.org
The American Legacy Foundation a national, independent public health foundation that develops national programs to address the health effects of tobacco use through grants, technical training and assistance, youth activism, strategic partnerships, counter-marketing and grass roots marketing campaigns, public relations, and community outreach to populations disproportionately affected by the toll of tobacco.
The foundation sponsors the following major activities:
✷ The Truth® Campaign www.thetruth.com
The Truth Campaign is a major national tobacco youth prevention and educa-tion effort that uses advertising, grassroots and promotional events, and the interactive Web site (www.thetruth.com) to give teens the facts about tobacco use and tobacco marketing and encourage them to get involved in the effort to inform their peers.
✷ Streetheory® www.streetheory.com
Streettheory is a national effort to assist and facilitate the work of the state-based youth activism programs. The web site (www.streetheory.org) provides a central reference tool and repository for youth activists and their ideas for prevention and education.
✷ Circle of Friends: Uniting to be Smoke-Free ww.join-the-circle.org
This program is a national grassroots social movement to support for women struggling to quit smoking, and to highlight the toll of tobacco-related disease on American women, their families and communities.
Americans for Nonsmokers’ Rightswww.no-smoke.org
Americans for Nonsmokers’ Rights is the leading national lobbying organization dedicated to nonsmokers’ rights, taking on the tobacco industry at all levels of government to protect nonsmokers from secondhand smoke and youth from tobacco addiction. Their web site (www.no-smoke.org) provides a wealth of information about the dangers of secondhand smoke, and serves as a resource for advocacy efforts to reduce tobacco use and secondhand smoke exposure. The organization also includes the American Nonsmokers’ Rights Foundation, an educational nonprofi t organization that creates comprehensive programs for school-age youth on issues of smoking prevention and their right to breathe smoke-free air.

Resources 21
Additional Resources for Teachers
Facts and Figures
A number of organizations regularly compile statistics on youth tobacco use and make these available to the public on a recurring basis. Other resources include one-time publications whose presentation of information and data are unique and valuablecontributions to the discussion on tobacco use and youth.
Monitoring the Futurewww.monitoringthefuture.org
Monitoring the Future is an ongoing study of the behaviors, attitudes, and values of American secondary school students, college students, and young adults. Each year, a total of some 50,000 8th, 10th and 12th grade students are surveyed (12th graders since 1975, and 8th and 10th graders since 1991.) In addition, annual follow-up questionnaires are mailed to a sample of each graduating class for a number of years after their initial participation. The study is housed in the University of Michigan’s Institute for Social Research, and the research data are made available on their web site (www.monitoringthefuture.org).
The Youth Behavioral Risk Factor Surveillance Systemwww.cdc.gov/HealthyYouth/yrbs/index.htm
The YRBSS was developed in 1990 to monitor priority health risk behaviors that contribute markedly to the leading causes of death, disability, and social problems among youth and adults in the United States. These behaviors, often established during childhood and early adolescence, include tobacco use, unhealthy dietary behaviors, inadequate physical activity, alcohol and other drug use, sexual behaviors that contribute to unintended pregnancy and sexually transmitted diseases, and unin-tentional injuries and violence. The youth survey data are available online at www.cdc.gov/healthyyouth/yrbs/index.htm.
✷ Berman BA, Eckhardt EA, Kleiger HB et al. Developing a tobacco survey for Deaf youth. American Annals of the Deaf, 2000; 145(3):245-55)
✷ Campaign for Tobacco-Free Kids. Trust Us, We’re the Tobacco Industry. 2001. Available online at:
www.tobaccofreekids.org/campaign/global/framework/docs/TrustUs.pdf
✷ Glantz SA. Tobacco: Biology and Politics. Health EDCO. 1992.
✷ Kluger R. Ashes to Ashes: America’s Hundred-Year Cigarette War, the Public Health, and the Unabashed Triumph of Philip Morris. New York: Random House, 1996.
✷ Lynch BS, Bonnie RJ., Editors. Growing Up Tobacco Free. Institute of Medicine. National Academy Press, Washington, D.C. 1994.
✷ McKay J, Eriksen M. The Tobacco Atlas. Geneva: World Health Organization. 2002.
✷ Meister K, Bowman KC, Ross GL, et al. (Ed.) Cigarettes: What the Warning Label Doesn’t Tell You. Information Tobacco Companies Don’t Want Teens to Know About the Dangers of Smoking. New York: American Council on Science and Health. 2003. The title can be read or downloaded from the following site:
www.acsh.org/publications/pubID.188/pub_detail.asp
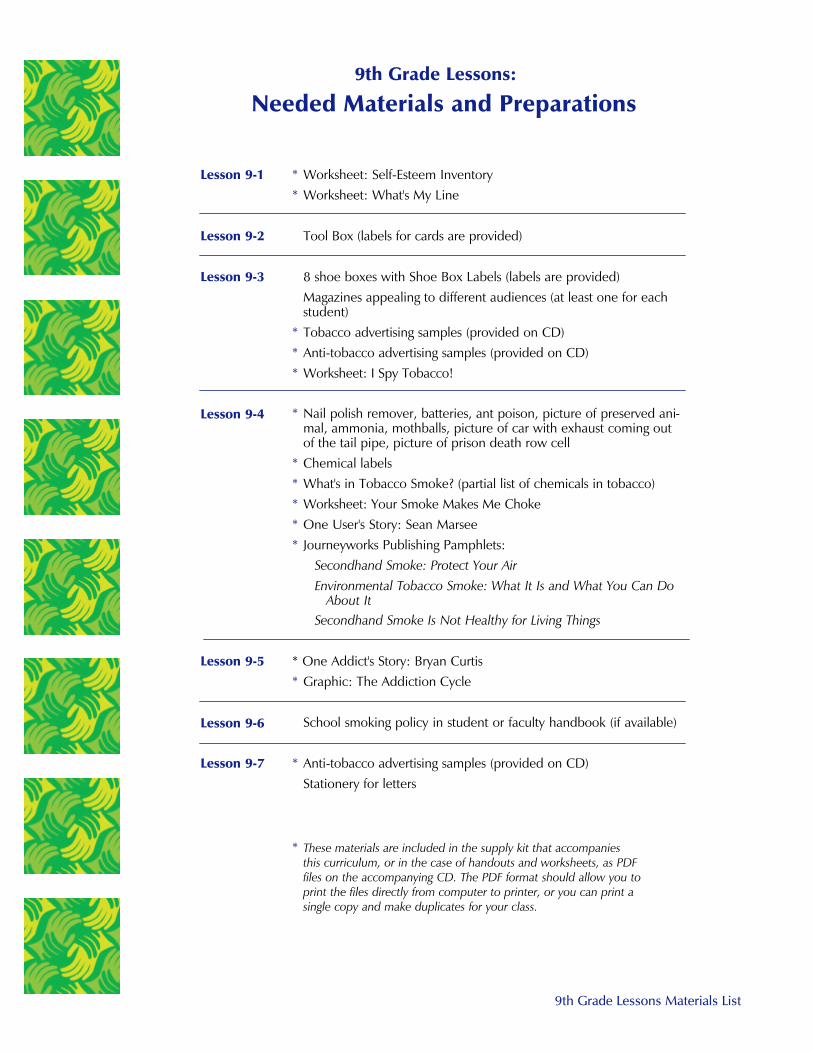
9th Grade Lessons Materials List
Needed Materials and Preparations9th Grade Lessons:
* Worksheet: Self-Esteem Inventory* Worksheet: What's My Line
Tool Box (labels for cards are provided)
8 shoe boxes with Shoe Box Labels (labels are provided)Magazines appealing to different audiences (at least one for eachstudent)
* Tobacco advertising samples (provided on CD)* Anti-tobacco advertising samples (provided on CD)* Worksheet: I Spy Tobacco!
* Nail polish remover, batteries, ant poison, picture of preserved ani-mal, ammonia, mothballs, picture of car with exhaust coming outof the tail pipe, picture of prison death row cell
* Chemical labels* What's in Tobacco Smoke? (partial list of chemicals in tobacco)* Worksheet: Your Smoke Makes Me Choke* One User's Story: Sean Marsee* Journeyworks Publishing Pamphlets:
Secondhand Smoke: Protect Your Air Environmental Tobacco Smoke: What It Is and What You Can Do
About It Secondhand Smoke Is Not Healthy for Living Things
* One Addict's Story: Bryan Curtis* Graphic: The Addiction Cycle
School smoking policy in student or faculty handbook (if available)
* Anti-tobacco advertising samples (provided on CD)Stationery for letters
Lesson 9-1
Lesson 9-2
Lesson 9-3
Lesson 9-4
Lesson 9-5
Lesson 9-6
Lesson 9-7
* These materials are included in the supply kit that accompaniesthis curriculum, or in the case of handouts and worksheets, as PDFfiles on the accompanying CD. The PDF format should allow you toprint the files directly from computer to printer, or you can print asingle copy and make duplicates for your class.

Page 9.1.1
Self-Esteem: How Do You See Yourself?
Lesson 9-1
Lesson Objectives:
By the end of Lesson 9-1, students will:
W Gain awareness of how self-esteem can work for or against them
W Identify areas of self esteem that are high or low
W Develop strategies to increase their self-esteem
Materials: W Self-Esteem Inventory Worksheet
W What's My Line Worksheet
Key Terms:
competence: having the necessary abilitiesor qualities to do things, perform tasks,or get along with others.
self-esteem: belief in one’s worth; selfrespect; the value you place on yourself.
self-image: the inner picture that one has of him- or herself; the concept one has of one’s competence, worth,attractiveness, intelligence and othercharacteristics and traits. Self-image isalso often referred to as self-concept.
worth: the value one places on one’saccomplishments, abilities, and relationships with others.
Introduction:
This lesson introduces students to the concept of self-esteem and how it relates to relationships and behavior. The point is to make students aware of how their ownperceptions of who they are as individuals can affect the ways they behave botharound and towards others. This theme is expanded upon in Lesson 9-2, which looksat how students respond to friend and peer influences.
L91_SelfEsteem

Page 9.1.2
Lesson 9-1: Self-Esteem: How Do You See Yourself?
Procedures:
1. Write the following definitions on the board and facilitate a discussion to ensurethat students understand the terms:
Self-Image: The whole inner picture that you have
of yourself; what you think of your abilities, worth,attractiveness, intelligence, and other aspects of yourself. This is also sometimes described as
self-concept.
Self-Esteem: belief in one's worth; self respect; thevalue you place on yourself.
2. Initiate a discussion of self-image and self-esteem byasking the following:
What is self-esteem? What do we mean when we saysomeone has high self-esteem? Low self-esteem? Does
your self-esteem change according to your surroundings,for example, when you are with your Deaf friends, orwhen you are with hearing friends? When you are here on campus,
or when you are at the local mall? Does your self-esteem affect the way you behave?
3. Ask students to brainstorm ways that low/high self-esteem can affect:
Relationships: If you feel bad about your abilities, intelligence,
or appearance, how do you think that might affect your relationshipswith your family? Deaf friends? Hearing friends? Other peers? Boyfriendor girlfriend? How would things be different if you thought highly
of your abilities, intelligence, or appearance?
Choices: How might the way you feel about yourself affect your decisions in trying new activities? Making friends? Working? Joining a sports team or schoolclub? Using drugs, tobacco or alcohol? What differences do you think high
self-esteem and low self-esteem make in these choices?
4. Pass out the Self-Esteem Inventory and ask students to complete the form. Tell students that there are no right
or wrong answers.
Teacher’s Note:You will be asking students to referto these worksheets in Lesson 9-2.
L91_SelfEsteem2
L91_SelfEsteem1
L91_FeelGood
L91_FeelBad

Page 9.1.3
Lesson 9-1: Self-Esteem: How Do You See Yourself?
5. Ask students to look over their inventories. Discuss how greater counts of “false”
answers may indicate low self-esteem. Lead a discussion about factors that helpto boost or lower self-esteem. Ask the class to brainstorm ways that teenagerscan increase their self esteem.
6. Ask your students to complete the What’s My Line? worksheet in class or forhomework. Explain that most people mark themselves somewhere between thetwo extremes listed for each line. However, they may “lean” more toward one
side or the other (e.g., “I tend to be more sloppy than neat, although I’m not atotal slob.”). Facilitate a discussion about the students’ ratings.
Looking over your worksheets, where do you usually place yourselves? Are thereany areas in which you've placed yourselves at the extreme ends? Are there any
of these areas that you would like to change?
Journal:
If you could change one thing about yourself, what would it be and why?
Procedures: (continued)

What’s My Line?
Lesson 9-1 Worksheet: What’s My Line?
Name __________________________________
Each line below is about you! Put an "X" where you fit on each line.
Total Slob!
Hot Temper!
Jock
Optimist
Leader
Gossip
Grudge Holder
Neat Freak!
Cool Head
Non-Athletic
Pessimist
Follower
Secret Keeper
Forgiving
My room is amess!
I get angry easily
I am really goodat sports!
I always feel positive
I like to makedecisions and
have others follow
I love to spread storiesabout others!
I can stay angry at others for a long time
My room isalways neat!
I rarely get angry
I’m not very good at sports
I always feel likethings are bad
I prefer to let others make
decisions
I never talk aboutother
people’s business
I am able to forgive people
Total Slob! Neat Freak!My room is a
mess!My room isalways neat!
Example
x

Page 9.2.1
Assessing Peer Pressure Strategies
Lesson 9-2
Lesson Objectives:
By the end of Lesson 9-2, students will be able to:
W Identify the Tools of Fools (direct orders, insults, harassment, exclusion), strategies used by people to pressure others into certain actions or behaviors.
Materials: W Tool Box (box with cards, each card imprinted
with one of the Tools for Fools Strategies)
Key Terms:
harassment: Constant badgering or annoyance aimed at persuading someone to do something they otherwise might not want to do.
refusal skills: tools which one can use against friend or peer pressure to dosomething that one finds undesirable,unsafe, or wrong.
refusal strategies: ways of expressingrefusal, divided here into three majortypes: passive, aggressive and assertive.
Passive: refusal in a non-confrontationalmanner without actually saying “No.”Tends to be non-committal(“Um...maybe”), and often involves leav-ing an issue unresolved.
Aggressive: refusal expressed by usingconfrontational strategies.
Assertive: Refusal in a firm, clear, butnon-threatening manner.
For Review:
peer influence: the indirect force thatpeers exert in shaping one's opinions,perceptions, desires and behavior. (See Lesson 8-2)
peer pressure: the more direct force thatfriends and peers often use to shapeone's opinions, perceptions, desires andactions. (See Lesson 8-2)
Introduction: This lesson explores how peer pressure occurs and ways in whichsuch pressure can be resisted. Students are taken through exercises in trying to pressure others into engaging in behaviors such as smoking; and in considering thevarious types of resistance strategies that might be employed to counter this pressure.The link between self-esteem and the ability to resist peer pressure is also reviewed.
L92_PartyPeerPress

Page 9.2.2
Lesson 9-2: Assessing Peer Pressure Strategies
Procedures:
1. Use the following questions to start a discussion aboutpeer pressure:
W What is peer pressure?
W When can peer pressure be a negative force?(Use examples to prompt: when you feel pressured to do something you don't want
to do; smoking, drugs and alcohol use; dangerous driving; etc.)
W Is peer pressure always something negative? When do you think peer pres-
sure can be something positive? (Use examples to prompt: doing well inschool; not acting out in class; working as a member of a team).
W Who exerts peer pressure? Is it different when it comes from your friends
than when it comes from other kids your age that you may not know? In what ways? Do you think you feel more peer pressure from other Deaf kids, or more from hearing kids?
W How can you tell the difference between positive peer pressure and negative peer pressure?
W Think about the times you have felt pressured to do something you
didn't want to do. How did others make you feel that pressure?
W Think about the times you've pressured others to do something. How didyou do it? What techniques did you use?
2. Introduce Tools of Fools. Write on the board the strategies that people use to tryto pressure someone. For each tool, talk about the words or signs that peopleuse, including more subtle non-verbal body language:
W Direct Order (“Do It!”)
W Insults, including name calling and mean gestures (“What are you, a baby?)
W Harassment, including threats (Bothering someone repeatedly to try toconvince them.)
W Exclusion, including making a person feel left out. (“Everyone's doing itexcept you!”)
W Non-verbal or other physical cues, such as: rolling eyes or not giving eyecontact; ignoring you; turning their backs to you; talking about a personbehind their back; etc.
L92_Decisions02
L92_Decisions03
L92_Decisions01

Page 9.2.3
Lesson 9-2: Assessing Peer Pressure Strategies
W Guilt, such as making people feel bad if they don't go along, as a way ofgetting them to do something they otherwise might not do. (“Oh forget it,if you don't want to go, I'll just go by myself!”)
Ask students, “Which of these Tools for Fools have you experienced? From
whom? Do you think that your being Deaf makes you more vulnerable to suchTools? Less vulnerable? Why?”
3. Ask students to think about the Tools for Fools that are being used in each of
the following situations:
W Why don't you smoke cigarettes with us, are you scared?
W Want some pot? C'mon, it won't hurt you. No one will find out. You'll justfeel a little relaxed, that's all.
W Come on, no one will know if we have sex, don't you love me?
W I have some beer in my backpack, meet me after school to drink it.
Everyone else will be there.
W I found some ecstasy in my sister's room, let's try it. Oh, but I forgot—your mommy would get mad at you. Never mind.
W Hey, be a pal and keep these cigarettes in your locker for me until after
school, OK?
4. Explain that sometimes we feel pressure from friendsor peers to do something we don’t want to do, or
think that we shouldn’t do. Tell your students thatrefusing to go along with others—including peoplewhose ideas and opinions are important to us—can
be difficult to do, but that it helps if they know specific ways to say “No!”—resistance strategies.
Remind your students that ultimately they are respon-sible for the decisions they make, no matter how they
are pressured by others. In making these decisions, itcan be helpful to go through the steps of the D.A.R.E.Decision-Making Process.
5. Discuss the different types of resistance that peopleuse. Sometimes these are referred to as passive, aggressive and assertiveresistance strategies. What do these terms mean?
Procedures: (continued)
Teacher’s Note:This discussion on resistance strategies is presented in Lesson 8-4 of the 8th grade curriculum. If your students have already covered this material, review briefly the differenttypes of resistance strategies students can usewhen confronted with pressure to do some-thing they don’t want to do. Otherwise, thatmaterial is covered here as well.
If your class has never covered the D.A.R.E.decision-making process before, you may needto take some time to review the steps with yourstudents. The model can be found in Lesson 7-3,which uses the decision-making process of theDrug Abuse Resistance Education (D.A.R.E.)program, the pioneer prevention effort established in 1983.

Page 9.2.4
Example #1: Passive Resistance
W Your friends ask you to join them behind the gym to smoke cigarettes.
What are the common ways you might resist this request? (e.g., I ignoremy friends’ invitation; I shrug my shoulders; I say, ‘Maybe next time.”;
I giggle and then look away.)
Explain that when we use these methods, we are using passive resistance. We avoid confrontation by being neither agreeing or disagreeing, walking away, or ignoring the issue.
Ask your students:What other types of situations can you think of where you'veused passive resistance? What are some of the advantages ofpassive resistance? What are some of the disadvantages?
Example #2: Aggressive Resistance
Some strategies can be termed aggressive resistance. These usually involve amore confrontational tone, such as taking a cigarette that someone has offered
you and crushing it in your hands, saying, “Get that stuff out of my face!”
Ask your students:What other situations can you thinkof where someone might use aggres-
sive resistance? What are some ofthe advantages and disadvantages ofaggressive resistance?
Example #3: Assertive Resistance
A third resistance strategy is sometimes called assertive resistance. Assertiveresistance usually involves making your resistance known in a direct but non-confrontational manner. For example, “No thanks, I don’t smoke,” or “Let’s NOT
get into your parents’ liquor cabinet—why don’t we find something else to doinstead?”
Ask your students:What other situations can you think of where someone might
use assertive resistance? What are the advantages and disadvantages of assertive resistance?
Lesson 9-2: Assessing Peer Pressure Strategies
Teacher’s Note:Advantages might include avoidingconflict; disadvantages might include
not resolving the problem, or notmaking your decision clear to others.
Teacher’s Note:Advantages might include beingclear and forcefully direct; disad-vantages might include sparking afight or argument, or causing bad
feelings.
Teacher’s Note:Advantages might include being
direct; disadvantages might includecausing bad feelings.
Procedures: (continued)
L92_Passive
L92_Aggressive
L92_Assertive

Page 9.2.5
6. Ask your students:
What can you do if a friend or group of friends wants you to do something—such
as smoke a cigarette, try marijuana, have sex, get drunk—that we are afraid to do,or don't think we should do? It can be hard to stand up to them and say “No,”even when you want to. Different situations may require different strategies. Here
are some techniques you can use to say “No.”
Have your students examine the following techniques. How well do they thinkthey would work in different situations?
Lesson 9-2: Assessing Peer Pressure Strategies
Procedures: (continued)
L92_Refusal01
L92_Refusal02
L92_Refusal03L92_Refusal04
L92_Refusal05
L92_Refusal06
1. Be Direct2. Change the Subject
3. Think of a Clever Response
4. Make a Joke
5. Blame an Adult6. Avoid the Situation
or Walk Away

Page 9.2.6
Lesson 9-2: Assessing Peer Pressure Strategies
Procedures: (continued)
7. Divide the class into two teams. Team A will select a Tools for Fools Card fromthe Tool Box and will show that strategy. For example, the team picks the Insultcard and says, “You are such a wimp if you don’t try smoking!”
Team B must decide which Tool is being used and then decide which of the
refusal strategies will work best for that situation and role play it back.
8. Discuss the following points with the class:
W Which of the Tools was the hardest for you to respond to? Which onecaused you to feel the most pressure?
W Which refusal strategy worked the best for you?
W Practicing refusal skills and knowing what type peer pressure affects you themost will be helpful.
9. Ask students to practice these refusal skills through out their day whenever possi-ble to become more skilled.
10. Have students review their homework from Lesson 9-1 (What's My Line?). Ask
your students how the ways they see themselves might make them more suscep-tible, or less susceptible, to pressure from others.
Journal:
What type of peer pressure makes you feel the worst? Why?
What type of peer pressure is the hardest for you to respond to? Why?

Tools for Fools Labels
Lesson 9-2 Tools for Fools
Name __________________________________
Direct Order“Do It!”
InsultsName-calling, teasing, making
fun of someone
Harassmentbothering someone repeatedly
to try to convince them, includes threats
Making Someone Feel Left Out
Non-VerbalEye-rolling, mean gestures,
dirty looks, etc.
GuiltMaking someone feel guilty
if they don’t go along

Page 9.3.1
Evaluating Media MessagesLesson 9-3
Lesson Objectives:
By the end of Lesson 9-3, students will be able to:
W Identify how marketing strategies target teens.
W Identify ways in which marketing influences young people's decision-making.
W Identify ways in which marketing strategies might be successful (or unsuccessful)in reaching Deaf teens.
W Identify more effective ways to reach Deaf teens with anti-tobacco programming.
Materials:
W 8 shoe-boxes - with Shoe Box Labels
W Magazines appealing to different audiences (at least one for each student)
W Tobacco advertising samples (provided on CD)
W Anti-tobacco advertising samples (provided on CD)
W I Spy Tobacco! Worksheet
Prepare:
W Collect various magazines that appeal to different audiences (for example, busi-ness, women, teens, news, sports, health and fitness, beauty, hobbies, music,skateboarding, etc.). This lesson's exercises will work best if students can view avariety of magazines for diverse audiences. It is best if you start assembling thiscollection as early as possible, or ask your students to bring in different types ofmagazines over the preceding month or so.
W Ask students to look through magazines and newspapers for advertisements,including tobacco ads, and to bring those they find to class.
Key Terms:
advertising: one of the major tools ofmarketing, usually through media suchas magazines, television, billboards, etc.
manipulation: Conscious strategies toshape others’ perceptions of a productor idea through marketing efforts.
marketing: persuasion to buy a product or accept an idea by presenting it in afavorable light that shows its advantagesor attractions; advertising.
Introduction: The lesson asks students to examine the impact of advertising andmarketing on their decision-making, particularly when it comes to evaluating behavioralchoices regarding the use of tobacco. Students review the various types of messagesand appeals that are made and the various strategies used to deliver these messages.Students are then asked to consider the effectiveness and appeal of these messages forDeaf youth, and how these messages can be effectively countered with the marketingof anti-tobacco messages.

Page 9.3.2
Lesson 9-3: Evaluating Media Messages
Procedures:
1. Review some of the factors that encourage smoking that were covered in Lesson9-2, including peer pressure. Ask your students to review some of the ways they
can resist the pressure to smoke or use tobacco.
2. Explain to your students that when people are asked why they started smoking,they often give the following answers:
W curiosity or boredom
W to relieve stress or depression
W to look older, more mature, or cooler; to fit in
W to be rebellious; to have fun
And yet, when scientists talk to young people, they actually find that mostteenagers don’t think smoking is cool. In fact,
W 67% of teenagers say that seeing someone smoke turns them off.
W 65% say that they strongly dislike being around smokers.
W 86% would rather date people who don’t smoke.
Even teenagers who smoke don’t think that smoking is so cool. More than half
want to quit, and 70% wish they had never started smoking in the first place.
3. Ask your students:W Where does the idea that smoking is cool, fun, exciting and rebellious
come from? Maybe because that is how smoking is portrayed in cigaretteadvertising. Can advertising really be that powerful?
4. Begin a discussion of products students like to buy—shoes, soda, clothing,
electronic goods and the like. Ask students to identify the “best” or “coolest”shoes, bags, skateboards, gadgets, clothing and so forth.
Ask your students:
W Why do you choose a particular brand of shoe, or type of soda? What do you think about products such as Nike shoes, or Red Bull,
especially compared to similar products?
Ask students how they know about these products, and why theythink they are the best.
L93_ConsumerGoods

Page 9.3.3
Lesson 9-3: Evaluating Media Messages
Explain that most of the items we think are“best” or “coolest” are often items that areadvertised by celebrities or people we admire,
or that appeal to our desires. Advertisementsand “marketers” try to convince us that if webuy a particular product, we will look better, feel
better, have more fun, be more relaxed, or anynumber of other positive results. This is some-times referred to as manipulation.
W Do you think this manipulation is conscious on the part of advertisers?Why or why not?
5. Using magazines
geared to several different audiences (teens, women's
magazines, popularmusic, cars, skating, homedesign, personal finance), ask students to tear out at least ten advertisements.
Ask them to write on the back of each one the name of the magazine in whichthe advertisement was found. Distribute the advertisements around the classand ask students to
analyze them.
Ask your students:W What is the product being advertised? What is the advertisement telling us
about the product? What is the advertisement trying to tell us if we use
the product?
Explain to students that companies want us to buy their product so that theycan make money. If a company can successfully get people to buy their prod-
uct, the company will make money.
6. Ask students to identify aspects of commercials from TV that appeal to teens.For example:
W Nike—Just Do It! Shows strength and power
W Gatorade—Shows strength, power, speed, slick like water, cool
W Acne medicine—Beauty, building one’s confidence
Ask students for other examples.
Procedures: (continued)
L93_BeautyAd
L93_Magazines

Page 9.3.4
7. Ask your students:
W How do commercials influence how you think about the products?
Explain that companies try to tell us that if we use their product, it will bring usthe things we want. They try to convince us that their product will give us:
W Fun and Pleasure
W Good HealthW Adventure and ExcitementW Money, Fame or Power
W Beauty and PopularityW RomanceW Brains, Intelligence and Wisdom
W Free Stuff!!
8. Cut out the Shoe Box Labels, and glue each one to a shoe box. Ask students tosort the ads into the appropriate shoe boxes.
Discuss how the ads differ by magazine type, and why.
Talk about the importance of the audience:
W What type of advertisements would you
expect to find in a teen magazine? Howabout a gaming magazine? A personalfinance magazine?
Ask students to identify the things that theywould like most from the above list. Which dothey think is most important? How would these
appeals play to people with different levels ofself-esteem?
9. Distribute to the class copies of tobacco adver-
tisements and ask the students to classify theminto the categories above. What are the messagesin these advertisements? What audiences are
targeted in these tobacco advertisements? Askthem if it is clear (visually) what product theadvertisements are selling, and how. Refer to
some of the older advertisements, particularlythose featuring tobacco recommendations bydoctors, and those featuring parents and children.
Lesson 9-3: Evaluating Media Messages
Procedures: (continued)
Teacher’s Note:As part of the 1998 Tobacco Master SettlementAgreement that was reached between major tobaccocompanies and 46 states, the tobacco industryagreed to a number of new restrictions on tobaccoadvertising (joining the ban on television advertise-ments for tobacco products). Included in theserestrictions are bans on the use of cartoons in advertising or packaging for tobacco products; elimination of most outdoor advertising, includingbillboards, and signs and placards in arenas, stadiums,shopping malls, and on transit (e.g., buses andtrains); and bans on the sale or distribution ofapparel and merchandise with brand name logos(although tobacco companies continue to give awayfree merchandise in exchange for “points” or“coupons” earned with each purchase of cigarettes.)
The Master Settlement Agreement also bans paymentsto promote tobacco products in movies, on televisionshows, in videos and videogames, and other enter-tainment. Tobacco companies are also prohibitedfrom brand name sponsorship of events with a significant youth audience (football, basketball,baseball, hockey and soccer).
Students should be encouraged to think about howmarketing to young people might still be occurring,even in the face of these prohibitions.
You can read more about this at:
http://caag.state.ca.us/tobacco/resources/msasumm.htm

Page 9.3.5
Lesson 9-3: Evaluating Media Messages
Procedures: (continued)
L93_CamelPool
L93_Fun
L93_Ad04
L93_Romance
L93_MarlboroCowboy
L93_VSlimsAppeal
L93_VSlims01
L93_Celebrity
What desires do these advertisements for cigarettesappeal to? What experiencesand self-images do theseadvertisements want us toassociate with tobacco use?
What do these advertisements want to say
to us about smoking andour sense of femininity and
masculinity?
Or our sense of the exotic, romanticand fun?

Page 9.3.6
Lesson 9-3: Evaluating Media Messages
Procedures: (continued)
L93_AlecBaldwin
L93_DemiMoore
L93_LindaEvangelista
L93_PenelopeCruz
L93_Navratilova
L93_koolradio
L93_MarlboroPackage
L93_Giveaway
Why do you think tobaccocompanies want to showcelebrities smoking? Why arethese images important totobacco marketers? What doyou think of these ads?
Celebrities are useful even ifthey are not directly promot-ing the use of tobacco. Byusing stars such as MartinaNavratilova in their sponsor-ship of sporting events (sincerestricted under the terms ofthe Master SettlementAgreement), or by usingcelebrities such as PenelopeCruz in producing “lifestyle”magazines (along with manytobacco ads inside) for homedelivery, tobacco companiescan reach out to audiencesthey might not reach other-wise. Who would be excitedabout the Virginia SlimsTennis Championships? Whomight read “Flair” magazine?
Free gifts with the purchaseof cigarettes were an important marketing tool for tobacco companies. This practice has since beenvoluntarily restricted by thetobacco companies under theterms of the Master SettlementAgreement, although they stilloffer sales-linked couponsthat are redeemable for arange of clothing, gadgetsand other goods.

Page 9.3.7
Lesson 9-3: Evaluating Media Messages
Procedures: (continued)
These advertisements are alsofrom the 1940s and 1950s.To whom do you think theseads appeal? Do you thinkyou would see ads like thesetoday? Why or why not?
L93_CamelNoRegret
L93_Doctor1946
L93_Doctor1940
L93_MotherChild
L93_FatherSon1945
Before the harmful healtheffects of tobacco were widelypublicized, tobacco companiessought to allay smokers’health concerns with adver-tisements featuring medicalpersonnel, and others toutingcigarettes that were “mild”and free of “irritation.”
Many of these ads were produced in the 1940s and1950s. Do you think tobaccocompanies could produceadvertisements like thesetoday? Why or why not?What do you think of theseads?

Page 9.3.8
10. Ask your class if anyone has ever seen anti-tobacco advertising. Explain that government agencies and other groups are countering tobacco companies’
advertisements with their own anti-tobacco advertisements.
W What messages are these advertisements trying to convey? Are they effective or convincing? Do you think these advertisements are convincingfor Deaf youth? What kind of advertisement do you think YOU could
design to reach other Deaf kids?
Lesson 9-3: Evaluating Media Messages
Procedures: (continued)
“Many bug sprays contain nicotine.All cigarettes do.”
“The same formaldehyde that preserves dead frogs is found
in cigarettes.”
“Cyanide is the deadly ingredient inrat poison. And just one of the
many in cigarettes.”
Look how these billboards are using the “glamour ofsmoking” as portrayed in tobacco advertisements, andturning the message around to point out why smoking is a bad idea...
s
...while carrying the “masculinity” of the Marlboro Man to itsnatural conclusion if one takes up smoking.
L93_BugSpray L93_Frog L93_RatPoison
L93_MindIfISmoke
L93_Scent
L93_Emphysema L93_IMissMyLung

Page 9.3.9
Lesson 9-3: Evaluating Media Messages
Procedures: (continued)
Some anti-tobacco advertising portrays directly the fearsome consequences of tobacco use.
Others borrow the technique of celebrityappeal to promote bothtobacco use prevention andcessation.
s
L93_TableforOne
L93_ToldYou
L93_BlewAway
L93_FirstWarningSign
L93_BoyzIIMen
L93_Smoking Is Ugly
L93_tonyhawks

Page 9.3.10
Lesson 9-3: Evaluating Media Messages
Procedures: (continued)
Homework:
Distribute the I Spy Tobacco! Worksheet.
W Have students record, while they watch television over
the next week, every situation in which they see smokingor tobacco use of any kind. Ask them to write down thename of the show, and briefly describe the circum-
stances on the worksheet. Remind your students toinclude comedies, movies, newscasts, or even anti-smoking messages.Also, ask them to notice if they see tobacco advertisements when watching
sporting events on television, such as tennis matches, automobile racing,baseball games, and other tobacco-sponsored sports.
W Have students, over the course of the next week, note every instance of
tobacco advertising that they can find or see. Record the location of theseadvertisements on the worksheet. Instruct students to look for such advertising, not just in the usual places (e.g., in magazines), but also on
clothing, hats, at the beach, at sporting events, and so forth.
W If students see a movie, have them record any instances of smoking theysee. Have the students record who is smoking, and a brief description of
the circumstances.
Journal:Companies give away hats and shirts that bear the picture or name of the
product they sell. They do this as a form of advertising, because they know thatwhen people wear these items, they are helping to promote awareness of thecompanies’ products. What are your thoughts on tobacco companies engaging in
this type of marketing?
Teacher’s Note:Use the examples of tobacco
advertising above to review theobjectives of the homework
assignment with your students.

I Spy Tobacco!
Lesson 9-3 Worksheet: I Spy Tobacco!
Name __________________________________
Instructions:1. As you watch television this week, or if you see a movie, record every instance in which
you see smoking or tobacco use of any kind. Write down the name of the show or movieand briefly describe the situation (Who was smoking? Why?).
2. As you walk about over the next week, note every instance of tobacco advertising you cansee, including signs in stores, ads in magazines, on clothing, at the beach—keep a sharpeye out! Record the details below.
TV Show, Movie, or Place You SawSmoking or Tobacco Advertisement
Describe the Situation

Page 9.4.1
So What’s So Bad About Tobacco?
Lesson 9-4
Lesson Objectives:
By the end of Lesson 9-4, students will be able to:
W Identify the types of tobacco use
W List some chemicals in tobacco
W Identify damaging effects of tobacco use
W Identify the dangers of secondhand smoke
Materials:
W Nail polish remover W Batteries
W Ant poison W Picture of a preserved animal
W Ammonia W Mothballs
W Picture of car with exhaust coming out of the tail pipe
W Picture of prison death row cell
W Chemical Labels
W What’s in Tobacco Smoke? Partial list of chemicals in tobacco
W Your Smoke Makes Me Choke Worksheet
W One User’s Story: Sean Marsee Handout (also on CD in the “WebPages” folder)
W Journeyworks Publishing pamphlets:
Secondhand Smoke: Protect Your Air
Environmental Tobacco Smoke: What It Is and What You Can Do About It
Secondhand Smoke Is Not Healthy for Living Things
Key Terms:
inhale: to draw air into the lungs, alongwith any chemicals, dirt, germs, andother particles that may be floating inthe air
passive smoking: Inhaling secondhandsmoke from someone else's smoking,or from their lit cigarette, cigar or pipe.
secondhand smoke: Secondhand smokeis the exhaled smoke from the lungs ofa smoker, as well as the smoke that disperses from a lit cigarette, cigar orpipe. It is also commonly referred to as environmental tobacco smoke, or ETS.
Introduction: Students are presented with a graphic presentation of the differenttypes of chemicals found in tobacco and cigarette smoke. These chemicals are thenlinked to the various health effects of tobacco use (both smoked and smokeless) onthe respiratory and cardiovascular systems of the body, as well as on other tissues andorgan systems. Students are also introduced to the hazards of secondhand smoke.

Page 9.4.2
Lesson 9-4: So What’s So Bad About Tobacco?
Procedures:
1. Have the above-listed items on a table in the front of the room. Ask students toname the items and if they know, what they are used for. Ask students what
would happen if they ingested the items they see on the table.
2. Place the appropriate label (See Chemical Labels) on each of the items. Explainthat the word on the label is one of the poisonous chemicals found in the item.
Explain that each of these chemicals is also contained in cigarette smoke.Tobacco contains more than 4,000 chemicals that enter the body either throughsmoking or chewing tobacco products.
3. Explain that these are just some of the poisons that enter the body throughtobacco use. When tobacco is burned (as in a cigarette), these chemicals enterthe body through the smoke. Similarly, if tobacco is chewed (as in smokeless
tobacco), many of these chemicals are absorbed into the body through the tis-sues of the mouth and throat. Distribute the comprehensive list of chemicals intobacco.
4. Write the words Health Consequences on the board. Explainthat over the past 50 years, scientists have shown that the components of tobacco—the chemicals found in tobacco and
in the smoke when tobacco is burned—can harm the body invery serious ways. Ask your class if they can list some of themost important health consequences of tobacco use.
Classify the responses into the following categories:
5. Effects on the respiratory system: The most common waypeople use tobacco is to burn it and inhale the resultingsmoke, either from a cigarette, cigar, pipe, bidi, kretek, or
waterpipe (hookah). This smoke causes a great deal of damageto the tissues of the respiratory system: that is, the lungs andairways leading to them.
When a person inhales, their lungs fill with air containing oxy-gen. The lungs have tiny air sacs, called alveoli, where the oxy-gen is absorbed into the blood and exchanged with carbon
dioxide, a waste product of the body that is exhaled as the per-son breathes out. This process is called gas exchange, and is
Teacher’s Note:If your students have previouslycompleted the 8th grade unit ofthis curriculum, they may havealready studied the health andsocial consequences of tobaccouse. If so, you may choose to
present an abbreviated version ofthe material presented here.
Valuable Resource:Other facts and figures regarding
smoking and young people can befound at:
http://tobaccofreekids.org/research/factsheets/index.php
Check This Out!:A wonderful interactive animated
presentation of the effects oftobacco on different organ systems
in the body can be found at:
http://www.cdc.gov/tobacco/sgr/sgr_2004/sgranimation/flash/
index.html

Page 9.4.3
Lesson 9-4: So What’s So Bad About Tobacco?
the primary function of the lungs. The oxygen absorbed by theblood in the lungs is then carried to the heart, and all other tis-sues and organs of the body.
When you inhale, the inside of your lungs and airways are
exposed to air, including any germs, dust, dirt particles and otherobjects floating in the air. To clean away these foreign particles,your lungs and airways secrete mucus, which traps the particles.
Little hair-like structures called cilia that line the airways move in a sweeping motion to push this mucus out of the lungs. Thismucus, with its trapped particles, can then be coughed, spit,
or otherwise passed out of the body.
So what does smoking do?
Tobacco smoke slows the motion of the cilia, making it more difficult to movemucus out of the lungs and airways. This makes it more likely likely that germs,
dirt and other contaminants (together with the mucus) will get trapped in thelungs. The more and the longer you smoke, the greater the damage done to thecilia, until they lose almost all of their ability to clean the lungs. The result is
often “smoker’s cough,” the hacking, mucus-laden cough that long-time smok-ers often experience, especially on awakening in the morning. If the lungs andairways become inflamed and clogged with mucus, this can lead to chronic
bronchitis, making it difficult to breathe.
When a person smokes, the tobacco smoke is inhaled into the lungs, where thesmoke leaves behind a sticky residue called tar. Contact with this residue candamage the lungs, and over time may result in diseases such as lung cancer.
Procedures: (continued)
A healthy lung normallyhas a smooth surface.
Compare the healthylung with this diseasedlung of a smoker. This
lung shows lung cancer,the grayish-white bumps
on the lung.
L94_HealthyLung L94_LungCancerSource: The ABC’s of Smoking Source: The ABC’s of Smoking
L94_Alveoli

Page 9.4.4
The smoke also damages also damages the alveoli, the little air sacs
where gas exchange in the lungs takes place. This damage means that your lungs become much less able to perform the gas exchangethat brings oxygen into your body. In some people, this damage
progresses to become a disease called emphysema, where the alveoli (air sacs) have been damaged to the point where oxygen can no longer be absorbed into the bloodstream. Smoking also
causes the airways (the lungs and the tubes leading to them) to overreact to harmful substances, causing them to tighten up (“constrict”), and leading to wheezing and shortness of breath.
This can be especially serious for those people who already suffer from asthma.
Lesson 9-4: So What’s So Bad About Tobacco?
Procedures: (continued)
What does emphysemalook like? Compare thehealthy lung on the pre-vious page with the lungfrom a person withemphysema above.
L94_emphysema
s
6. Effects on the circulatory system: The chemicals found in tobacco havemany effects on the body's circulatory system. Smoking encourages a
process call atherosclerosis, or narrowing of the arteries and blood vessels.This reduces the flow of blood and oxygen to important organs, including the brain and heart. Over time, this narrowing can lead to a heart attack
(if the heart tissue is deprived of the oxygen it needs to keep beating), or a stroke (caused by a blockage of a blood vessel in the brain or neck, leading to tissue damage or death in the brain.)
L94_HeartDetail
Smoking can lead to highblood pressure, which inturn can cause a stroke,or bleeding in the brain.The damage that strokescan do is clear in thespecimen above.
L94_Stroke
s

Page 9.4.5
7. Mouth and throat tissues: The chemicals that cause damage to lung tissues can
also damage tissue in the mouth, leading to gum disease, mouth sores and toothloss. These chemicals can also lead to cancer of the mouth and throat.
Lesson 9-4: So What’s So Bad About Tobacco?
Procedures: (continued)
8. Other organ systems: Over the long term, smoking has also been linked to can-cer of the bladder, kidney, pancreas and other important organs in the body.
9. What about smokeless (chewing) tobacco products?Since these aren’t burned and smoked, doesn’t thatmake them safe? Explain to your students that these
products also contain harmful chemicals that cancause diseases such as oral cancer. Many young peoplebelieve that these types of tobacco are safe because
they are not smoked, but this is an incorrect belief.
10. Social consequences of smoking: Ask your studentsif anyone can think of any reasons—other than harm-
ful health impacts—that would discourage people fromsmoking. Possible prompts include:
Personal appearance/grooming: e.g., bad breath, yellow teeth, discolored
fingers, holes in clothing.
Relationships with others: e.g., upsetting parents, disappointing teachers, putting off friends.
Tobacco use can lead to gum ulcers as inthis picture here. Eventually, this tissuedamage can lead to oral cancer, such asthat featured in the anti-tobacco advertisement at right:
sL94_GumDisease
L94_OralCancer
One User’s Story:If your students are not already familiar withthe story of Sean Marsee, his experience withthe use of smokeless tobacco can be found at:
http://whyquit.com/whyquit/SeanMarsee.html
The story can also be found on the accompanying CD (in the “WebPages” folder,titled “Sean Marsee’s Message”). You mightwant to consider reviewing this story as a classexercise, or having students read it as part ofa homework or journal exercise.

Page 9.4.6
Lesson 9-4: So What’s So Bad About Tobacco?
Rules and regulations: e.g., getting punished for breaking school rules, beingasked to step outside restaurants, getting cited or ticketed in public places for
violating no-smoking regulations.
As the health consequences of tobacco use have become better known, moreand more people in our society and elsewhere have come to recognize thesedangers and have decided to actively fight against smoking. There are increasing
numbers of rules about where one can and cannot use tobacco products.Smoking is now prohibited in many workplaces—including schools, hospitals, airplanes, and public buildings.
Financial considerations: How much does smoking cost?
11. Explain that one of the difficult things about educating young people abouttobacco is that many of the health impacts seem to be so far off into the future
that they don't seem to matter. However, there are some immediate healthimpacts, even for youths. What are these?
W Cigarette smoking during adolescence appears to reduce the rate of lunggrowth, and hence the maximum level of lung function that can be
achieved.
W Young smokers are much more likely to experience shortness of breath,coughing spells, phlegm production, wheezing, and overall diminished
physical health. Often young smokers have more difficulty exercisingbecause they have a hard time getting enough oxygen when they breathehard.
W Young smokers are less physically fit than their non-smoking peers.
W Smoking can contribute to the onset of asthma, or can severely aggravatean existing asthma condition.
W Chewing tobacco can lead to mouth sores and gum disease, even at ayoung age.
W Both smoking and chewing tobacco can lead to bad breath, yellowed
teeth, stained fingers, dulled taste buds, and a dulled sense of smell.
W One unseen impact is that young people who start smoking at a youngerage are more likely than later starters to develop a long-term addiction to
tobacco. If you start smoking at a younger age, chances are you will have amuch more difficult time quitting tobacco use later on, than someone whobegins smoking at a later age.
Procedures: (continued)

Page 9.4.7
Lesson 9-4: So What’s So Bad About Tobacco?
Procedures: (continued)
12. Ask the class if anyone can define the term secondhand smoke. Write otherterms for secondhand smoke on the board: passive smoking, environmental
tobacco smoke (ETS). Explain that secondhand smoke is the smoke that a person breathes in from someone else's cigarette or other tobacco product thatproduces smoke, such as cigars, pipes, bidis, clove cigarettes, or kretek. Explain
that not only does a smoker inhale the chemicals on the table, but so does anyone who inhales the secondhand smoke. Secondhand smoke contains atleast 60 carcinogens (chemicals that are known to cause cancer). A person
exposed to this smoke absorbs these carcinogens just as a smoker does.
13. Ask students if they have ever been exposed to secondhandsmoke. Explain that secondhand smoke can harm non-
smokers. Distribute the Secondhand Smoke pamphlet byJourneyworks Publishing and identify the health risks.Exposure to secondhand smoke:
W increases your risk of lung and nasal sinus cancer,
even if you yourself do not smoke
W causes burning eyes, nasal congestion and wheezing
W increases the prevalence of ear infections,
especially in young children
W increases the risk of bronchitis, pneumonia and other respiratory tract infections, especially in chil-
dren
W is associated with reduced lung function
W increases the risk of heart disease in people who are not smokers
W is linked to SIDS, or Sudden Infant Death Syndrome, that affects newborn babies
W leads to smaller birthweight babies for women exposed to secondhand
smoke during their pregnancies
14. Have the wrappers from four packs of cigarettes on a table.
W Ask students to look carefully at the packs to find something exactly thesame on each pack—the Surgeon General’s Warning.
W Ask students: Who is the Surgeon General?
Answer: The Surgeon General is a doctor who is appointed every fouryears by the President, and serves as the top symbol of the nation’s com-
mitment to protecting and improving the people’s health.
L94_PassiveSmoking

Page 9.4.8
Lesson 9-4: So What’s So Bad About Tobacco?
Procedures: (continued)
W In 1964, the Surgeon General released a landmark report that focusedattention on the dangers to health posed by tobacco and smoking. Thisreport was one of the main forces behind the government’s efforts to begin
labeling tobacco packaging with Surgeon General’s warnings:
W Explain that the government requires a warning on all packs of cigarettesbecause of the danger involved with smoking. Ask students if they think
these warnings are useful? Do they think people read them? Do they thinkthese warnings are effective for young people their age? Why or why not?What messages do they think would work better? Are there any messages
they can think of that could be aimed specifically at Deaf people? Shouldthey warn about other diseases or consequences of smoking?
L94_SGLabels
W Examine the warning labels that are produced by Canada and Brazil. Askyour students: Do you think these are more powerful labels? Why or whynot? Do you think they would be more effective at persuading people not
to smoke? Which country’s labels would be best for the Deaf in your opinion?
L94_Brazil01 L94_Brazil02 L94_Brazil03
Cigarette warning labels required ontobacco products sold in Brazil

Page 9.4.9
Lesson 9-4: So What’s So Bad About Tobacco?
Procedures: (continued)
Homework
Ask students to use the Your Smoke Makes Me Choke worksheet to create a
cartoon related to the issue of secondhand smoke.
L94_Canada01 L94_Canada02
L94_Canada08 L94_Canada13
Cigarette warning labels required ontobacco products sold in Canada

What’s in Tobacco Smoke?
Lesson 9-4 What’s in Tobacco Smoke?
Cancer Causing AgentsNitrosaminesCrysenesCadmiumBenzi (a)pyrenePoloniumNickelP.A.H.sDibenz AcidineB-NaphthylamineUrethaneN. NitrosonomicotineToluidine
MetalsAluminumZincMagnesiumMercuryGoldSiliconSilverTitaniumLeadCopper
AcetoneNail polish remover
Acetic AcidVinegar
AmmoniaFloor and toilet cleaner
ArsenicInsecticides and poisons
ButaneCigarette lighter fluid
CadmiumRechargeable batteries
Carbon MonoxideCar exhause fumes
DDT/DieldrinInsecticides
EthanolAlcohol
FormaldehydeBody tissue preservative
HexamineLighter fluid
Hydrogen CyanideGas chamber poison
MethaneSwamp gas
MethanolRocket fuel
NaphthaleneMoth balls
NicotineInsecticides
Nitrous Oxide PhenolsDisinfectantsCandle waxSolvents
Source of information: American Lung Association

Chemical Labels
Lesson 9-4 Chemical Labels
CadmiumCadmium is a toxic metal. It is used in many manufacturingprocesses, and is used to make products such as household
batteries. It is known to cause cancer in the lung andprostate; and can cause kidney damage and bone disease.
It is found in cigarette smoke.
AcetoneAcetone is a chemical used to make plastics, fibers, drugsand other chemicals. One common use is as a solvent todissolve other substances, as in nail polish. Exposure cancause eye and lung irritation, and dizziness. Exposure to
large amounts can cause unconsciousness or coma.
It is found in cigarette smoke.
AmmoniaAmmonia is a common chemical that is used to make fertil-
izer, textiles, plastics, explosives, and liquid householdcleaning products. Ammonia irritates the skin, eyes, nose,
throat and lungs, and in large doses can cause severe burns.
It is found in cigarette smoke.
ArsenicArsenic is a naturally-occurring chemical that is used to
make ant poison. Arsenic can irritate your throat and lungs,cause nausea and vomiting, damage blood vessels, lead to
abnormal heart rhythm and lower your red and whiteblood cell count. It can increase the risk of cancer of the
lungs, skin, bladder, liver, kidney and prostate.
It is found in cigarette smoke.
FormaldehydeFormaldehyde is a chemical that is used as a preservative,
and is used as an embalming fluid (to preserve dead tissue).Low levels can irritate the eyes, nose, throat and skin.
Formaldehyde has been shown to cause nose cancer in animals, and scientists believe it will also be shown to be a
human carcinogen.
It is found in cigarette smoke.
NaphthaleneNaphthalene is commonly found in the home in moth ballsand other insect repellents. It is also used to make plasticsand toilet deodorant blocks. Exposure to naphthalene candamage or destroy red blood cells. In animal studies, long-
term exposure to this chemical caused nasal and lunginflammation, and lung and nasal tumors.
It is found in cigarette smoke.
Carbon Monoxide (CO)CO is a colorless gas, and is the major component of car
exhaust. At low doses, CO can cause fatigue, and chest painsin people with heart disease. At higher doses, it causes
impaired vision and coordination, headaches, confusion andnausea. In high concentrations it is fatal, causing death by
interfering with oxygen intake.
It is found in cigarette smoke.
CyanideCyanide is an extremely poisonous chemical that in low
levels can cause breathing difficulty, heart pains, vomiting,blood changes, and headaches. High levels harm the brain
and heart, and cause coma and death. Smoking cigarettes isa major source of exposure to cyanide.
It is found in cigarette smoke.
Source of information: Agency for Toxic Substances and Disease Registry, U.S. Centers for Disease Control

Your Smoke Makes Me Choke!
Lesson 9-4 Worksheet: Your Smoke Makes Me Choke!
Name __________________________________
Instructions:
Use the space below to draw a cartoon expressing your views about secondhand smoke.

Nineteen Year Old Sean Marsee'sTobacco Message
Talihina High School's most outstanding athlete, Sean Marsee had won 28track medals in the 400 meter relay while running the anchor leg. Hisclassmates honored him with a walnut plaque. After a ten month battlewith rapidly spreading cancer that started on his tongue, Sean Marsee diedat age 19.
A smokeless tobacco user since age 12, Sean refused to believe hismother's warnings that tobacco was hazardous, smoke or no smoke.
It was early on February 25th. Sean Marseesmiled a tired smile at his sister, pointed his indexfinger skyward, and an hour later, at age 19, Sean

Sean Marsee before the final battle.
Marsee was dead. Just ten months earlier, Sean,an 18 year-old high school senior and star of theschool track team, was just a weekend away fromcompeting in the state track finals, and just amonth away from graduation. It was then thatSean opened his mouth and showed his mother anugly sore on his tongue. His mother, a registerednurse, took one look and felt her heart sink.
A user of smokeless chewing tobacco and snuffsince age 12, rarely was Sean without a dip. Livingfrom nicotine fix to nicotine fix, he went through acan of snuff every day and a half. When Sean'smother finally discovered his secret she hit the roof. She tried explaining just how hazardous thattobacco was for him, smoke or no smoke, but Seanrefused to believe her. He argued that other boyson the track team were dipping. He argued that hiscoach knew and didn't seem to care. He argued that high profile sports stars were usingand marketing smokeless tobacco. How could it be dangerous, he pleaded. In the end,his mother simply dropped the subject.
But now, an angry red spot with a hard white core, about the size of a half-dollar, wasbeing worn by his tongue. "I'm sorry, Sean," said Dr. Carl Hook, the throat specialist. "It doesn't look good. We'll have to do a biopsy." Sean was stunned. Aside from hisaddiction to nicotine, he didn't drink, he didn't smoke and he took excellent care of hisbody; watching his diet, lifting weights and running five miles a day, six months a year. Now this. How could it be? "But I didn't know snuff could be that bad for you," Seansaid. "I'm afraid we'll have to remove that part of your tongue, Sean," Dr. Hook said. The high school senior was silent. "Can I still run in the state track meet this weekend?"he finally asked. "And graduate next month?" Dr. Hook nodded.
On May 16th, Dr. Hook performed the operation. More of Sean's tongue had to beremoved than was anticipated. Worse yet, the biopsy results were back and the tumortested positive for cancer. Arrangements were made for Sean to see a radiation therapist,but before therapy began, a newly swollen lymph node was found in Sean's neck. It wasan ominous sign that the cancer had spread. Radical neck surgery had now becomenecessary.
Dr. Hood gently recommend to Sean that he undergo the severest option: removing thelower jaw on the right side, as well as all lymph nodes, muscles and blood vessels exceptfor his artery. There might be some sinking, he explained, but the chin would support thegeneral planes of the face.
His mother began to cry. Sean was being asked to approve his own mutilation. This wasa teenager who was so concerned about his appearance that he'd even swallow his diprather than be caught spitting tobacco juice. They sat is silence for ten minutes. Then,dimly, she heard him say, "Not the jawbone. Don't take the jawbone." "Okay, Sean, "Dr. Hook said softly. "But the rest; that's the least we should do." On June 20th Seanunderwent his second surgery. It lasted eight hours.

At school, 150 students and teachers assembled in June to honor their most outstandingathlete. Sean could not be there to receive their award. His Coach and his assistantcame to Sean's home to present their gift, a walnut plaque. They tried not to stare at thehuge scar that ran like a railroad track from their star performer's earlobe to hisbreastbone. Smiling crookedly out of the other side of his mouth, Sean thanked them.
With five weeks of healing and radiation therapy behind him, in August Sean greeted Dr.Hood with enthusiasm, plainly happy to be alive. Miraculously, Sean had snapped back. He really believes his superb physical condition is going to lick it, Dr. Hook thought. Let'shope he's going to win this race too.
But in October Sean started having headaches. A CAT scan showed twin tentacles offresh malignancy, one snaking down his back, the other curling under the base of hisbrain. In November, Sean underwent surgery for the third time. It was the jawboneoperation he had feared - and more. After 10 hours on the operating room table, he hadfour huge drains coming from a foot long crescent wound, a breathing tube sticking out ofa hole in his throat, a feeding tube through his nose, and two tubes in his arm veins. Seanlooked at his mother as if to say, "My God, Mom, I didn't know it was going to hurt likethis."
The Marsees brought Sean home for Christmas. Even then, he remained optimistic untilthat day in January when he found new lumps in the left side of his cheek. His motheranswered the phone when the hospital called with the results of the biopsy. Sean knewthe news was bad by her silent tears as she listened. When she hung up, he was in herarms, and for the first time since the awful nightmare started, grit-tough Sean Marseebegan to sob. After a few minutes, he straightened and said, "Don't worry. I'm going tobe fine." Like the winning runner he was, he still had faith in his finishing kick.
One day Sean confessed to his mother that he still craved his snuff. "I catch myselfthinking," he said, "I'll just reach over and have a dip." Then he added that he wished hecould visit the high-school locker room to show the athletes "what you look like when youuse it." His appearance, he knew would be persuasive. A classmate who had come to seehim fainted dead away.
Shortly before Sean's death he told his mother that there must be a reason that Goddecided not to save him. Sean's mother believes that Sean's legacy is in having his storyspread and hopefully "keeping other kids from dying." When Sean became unable tospeak, a friend asked him if their was anything he wanted to share with other youngathletes. With pencil in hand Sean wrote, "Don't dip snuff." On the morning ofFebruary 25th, Sean Marsee, age nineteen, exhaled his last breath.
Compiled using photos, facts and extensive quotations from an October 1985Reader's Digest article by Jack Fincher, entitled "Sean Marsee's Smokeless
Death," located at pages 107 through 112.
Compiled by John R. Polito, Founder WhyQuit.com, June 2000

Youth Nicotine Addiction Warning Signs
WhyQuit.Com | About Us | Contact Us | Link to Us | What's New?
Last Updated on October 8, 2002 by John R. Polito

Page 9.5.1
Hooked! What Is It to Be Addicted?
Lesson 9-5
Lesson Objectives:
By the end of Lesson 9-5, students will be able to:
W Define addiction
W Identify nicotine as the addictive substance in tobacco
W Understand the difference between smoking prevention and cessation.
W Identify aspects of withdrawal
W Interview an adult who has quit smoking
W Compare information gained in interviews to aspects of addiction and withdraw-al learned in class
Materials: W One Addict’s Story: Bryan Curtis Handout (also on CD in “WebPages” folder)
W Graphic: the Addiction Cycle
Key Terms:
addiction: Extreme physiological and psychological dependence on a sub-stance such as tobacco, alcohol orother drug, that has progressed beyondvoluntary control. People who areaddicted often feel sick when they stop using this substance.
craving: An intense and prolonged desire;for those addicted to nicotine, it is usually manifested as an intense desirefor cigarettes or other tobacco product.
dependence: An altered physical or psychological state produced byrepeated use of a drug (such as nico-tine in tobacco products), and thatrequires continued use to avoid thephysical and psychological discomfortsof withdrawal.
nicotine: The active ingredient in tobaccoproducts that is the chief cause of phys-ical addiction through its effects onbrain chemistry.
smoking cessation: To stop smoking afterone has become addicted.
withdrawal symptoms: The range ofunpleasant physiological and emotionalreactions of the body in response towithholding a drug that the body hasbecome addicted to.
Introduction: This lesson covers the concept of addiction, and the role of nicotine in causing addiction to tobacco. Students are introduced to the mechanism ofnicotine addiction and its self-reinforcing nature (the Addiction Cycle), to dispel manyyoung people's’ misconceptions about their ability to avoid tobacco addiction.

Page 9.5.2
Lesson 9-5: Hooked! What Is It to Be Addicted?
Procedures:
1. Ask your students the following questions about the process of starting to smoke:
Why is it so important to talk to young people your age about smoking and
tobacco use?
W Most people who smoke started when they were young. Almost allsay they started smoking regularly before the age of 18.
Ask your students:
How many of you know someone your age who has tried smoking?
The Facts:
L95_10thGrade; Source: Monitoring the Future, 2004
L95_12thGrade; Source: Monitoring the Future, 2004
L95_8thGrade; Source: Monitoring the Future, 2004

Page 9.5.3
Lesson 9-5: Hooked! What Is It to Be Addicted?
The numbers are only slightly lower for Deaf youths. In a survey of over200 Deaf high school students in California, 45%, or nearly half, have tried
smoking at least once.
W Most smokers wish they had never tried smoking.
Ask your students:
How many times have you heard someone your agesay, “I don’t really smoke—just every so often with
friends, or at parties.”
The Facts: More than one out of every three young people who
ever try smoking a cigarette become regular, dailysmokers before leaving high school. About 22% of allhigh school students—more than one out of every
five—currently smokes.
Procedures (continued)
Teacher’s Note:Scientists make a careful distinctionbetween ever use and current use.Ever use is defined by having eversmoked a cigarette, even if just onepuff. Current users are those whoare actively using tobacco, either on
an occasional or regular basis.Current use is often measured by30-day prevalence—that is, the
number of people who have used atobacco product one or more times
within the past 30 days.
L95_Statistics; Source: Monitoring the Future, 2004
W Most young people who try smoking think they’ll be able to stopwhenever they want.
Ask your students:How many times have you heard someone your agesay, “Smoking is no big deal. I can quit later anytimeI want.”
The Facts: If you ask a high school student who smokes everyday if they think they will still be smoking in five
years, almost all of them say “no.” But if you talk to them again when they are adults, most will still be smoking.
L95_Boasting

Page 9.5.4
W Most smokers have a hard time quitting because nicotine is veryaddictive.
Ask your students:How many of you know a smoker who has tried to quit, but failed?
The Facts: By high school, nearly three out of every four regular smokers havealready tried to quit smoking, and failed.
Lesson 9-5: Hooked! What Is It to Be Addicted?
Procedures: (continued)
L95_Cartoon

Page 9.5.5
2. Explain to your class:In the previous lesson (9-4), we learned about many of the harmful effects of
smoking. We also learned in earlier lessons (9-2 and 9-3) why people still feelcompelled to smoke, even though they may know smoking and other tobacco usecan be harmful. So what is the main reason why people continue to smoke,
once they’ve started to smoke regularly?
The Answer:
Addiction
3. Ask your students:What is addiction, and how does it happen?
Explain to students that people often use the word “addiction” in a very general
way. They’ll say, “I’m addicted to pizza,” or “I’m addicted to that televisionshow,” referring to any behavior someone might find pleasurable and doingexcessively. However, when it comes to behaviors such as tobacco use or drug
use, “addiction” means something very different. With true addiction, the follow-ing things happen:
W The substance produces a pleasant feeling.
W Over time, you need to use more and more of the substance to obtain thispleasant feeling.
W If you stop using the substance, you will feel unpleasant feelings called
withdrawal symptoms. You will feel better only if you can use more of thesubstance.
W You will continue to use this substance to pursue this pleasant feeling and
avoid feeling bad, even if you know the substance is harming your body.
4. In tobacco, the drug nicotine is the substance that causes addiction to smokingand other tobacco use. Nicotine is found in all tobacco products: cigarettes,
cigars, pipe tobacco, smokeless (chewing) tobacco, bidis, kretek, etc.
Show the Addiction Cycle graphic of how a young person can quickly becomeaddicted to tobacco.
Pleasant feelings:
Smoking a cigarette may cause some initial dizziness or nausea as a personbecomes accustomed to inhaling smoke. But it also produces a pleasant sensa-
tion almost immediately. This sensation is caused by nicotine. Within seconds ofinhaling tobacco smoke (or placing a plug of smokeless tobacco in the mouth),
Lesson 9-5: Hooked! What Is It to Be Addicted?
Procedures: (continued)

Page 9.5.6
Lesson 9-5: Hooked! What Is It to Be Addicted?
Procedures: (continued)
nicotine is absorbed into the bloodstream where it quickly travels to the brain.Here, the nicotine causes chemical changes in the brain that produce the pleas-ant sensation. This pleasant feeling wears off quickly, and the smoker must inhale
more smoke to experience that pleasant feeling again. The desire for thesesequences of “nicotine hits” is what encourages more regular use.
The need to use more and more
As a person starts to use tobacco (and nicotine) regularly, their brain and bodybecome less sensitive to the pleasurable effects of nicotine. This is called build-
ing up tolerance, and means that the smoker or smokeless tobacco user needsto smoke (or chew) more, and more often, in order to receive the same pleasura-ble sensations as he did before.
Withdrawal symptoms
As the body becomes accustomed to nicotine, your body and brain cells becomedependent on the nicotine in tobacco. While nicotine may produce pleasurablesensations in the body, withholding nicotine starts to cause a number of
unpleasant sensations, which range from mild to severe:
W Feeling restless
W Feeling irritable, moody or tense
W Insomnia
W Headaches or dizziness
W Sweating and unsteadiness
W Nausea or physical illness
These physical symptoms are known as withdrawal symptoms. Withdrawal canbe a very uncomfortable feeling, and is the reason why most people find it so
difficult to quit smoking after becoming addicted to nicotine. To relieve thesewithdrawal symptoms, the smoker or tobacco user must smoke another cigarette,or place another plug of smokeless tobacco in their mouth.
Hooked!
Addiction can happen very quickly, especially in young people. Some teenagersstart experiencing withdrawal symptoms, even if they feel they are just “playingaround” and smoking a few cigarettes a week! When a person is dependent on
nicotine, they feel that they don't have a choice about using tobacco anymore.They feel they must use tobacco. They must plan where they go and what theydo so that they will be able to use the drug nicotine. It is like carrying a ball and
chain. Addiction creates a feeling of need—a craving-in your body and your brain.

Page 9.5.7
Lesson 9-5: Hooked! What Is It to Be Addicted?
Procedures: (continued)
People who are addicted to nicotine in tobacco will continue to smoke, even ifthey know they are doing great harm to their health. This is why you often hear
smokers say, “I know I should quit. But I can’t.”
L95_AddictionCycle
1Within seconds of inhaling,nicotine speeds its way to
your brain.
2In your brain, nicotinecauses the release of a
chemical called dopaminewhich stimulates feelings ofpleasure and relaxes you.
3But as soon as you stopsmoking, this stimulationwears off as the nicotinelevel in your body falls.
4Your brain starts to crave
another “hit” of nicotine—telling you to smoke another cigarette.
5Over time, your brainbecomes accustomed
to nicotine stimulation.Once this happens,
you experienceunpleasant withdrawal
symptoms if yournicotine craving is
not satisfied.
6So you smoke another
cigarette. And thecycle starts over again.
5. Most people who experiment with, and begin to casually use,
tobacco, plan to quit when they get older. But most peoplefind it very difficult to quit once they've become addicted.Research shows that nicotine is as addictive as cocaine and
heroin. Ask students to think about what this means.
Journal:
Knowing what you know about the harmful substances intobacco, what do you think about becoming addicted to
smoking? What do you think is the best way to avoid becoming addicted to tobacco?
One Addict’s Story:A moving account of the difficulty of
quitting—even in the face of thedeath of a loved one from lung
cancer—can be found at:
http://whyquit.com/whyquit/BryanLeeCurtis.html
or on the accompanying CD (in thefolder “WebPages”, titled “SmokingKills - Bryan Story”). The story is an
apt illustration of the absolute hold oftobacco addiction.

Smoking Kills
"He Wanted You to Know"
On the day of Bryan's death, June 3, wife Bobbie and sonBryan keep a bedside vigil. The recent photo of father andson is on the bed. [Times photo: V. Jane Windsor]
by Sue Landry
Bryan Curtis started smoking at 13, never thinking that 20 years later it wouldkill him and leave a wife and children alone. In his last weeks, he set out with amessage for young people.
ST. PETERSBURG -- Cigarette smoke hangs inthe air in the room where Bryan Lee Curtis liesdying of lung cancer.
His head, bald from chemotherapy, lolls on apillow. The bones of his cheeks and shouldersprotrude under taut skin. His eyes are open, but hecan no longer respond to his mother or his wife,Bobbie, who married him in a makeshift ceremonyin this room three weeks ago after doctors said

Bryan Lee Curtis, then 33, holds son BryanJr., 2, in this March 29 photo. Curtis woulddie about two months later. [Photo: CurtisFamily]
there was no hope.
In Bryan's emaciated hands, Bobbie has propped aphotograph taken just two months ago. It shows amuscular and seemingly healthy Bryan holding his2-year-old son, Bryan Jr. In the picture, he is 33.He turned 34 on May 10.
A pack of cigarettes and a lighter sit on a table nearBryan's bed in his mother's living room. Eventhough tobacco caused the cancer now eating through his lungs and liver, Bryan smokeduntil a week ago, when it became impossible.
Across the room, a 20-year-old nephew crushes out a cigarette in a large glass ashtraywhere the butt joins a dozen others. Bobbie Curtis says she'll try to stop after the funeral,but right now, it's just too difficult. Same for Bryan's mother, Louise Curtis.
"I just can't do it now," she says, although she hopes maybe she can after the funeral.
Bryan knew how hard it is to quit. But when he learned he would die because of his habit,he thought maybe he could persuade at least a few kids not to pick up that first cigarette.Maybe if they could see his sunken cheeks, how hard it was becoming to breathe, hisshriveled body, it might scare them enough.
So a man whose life was otherwise unremarkable set out in the last few weeks of his lifewith a mission.
* * *
Bryan started when he was just 13, building up to more than two packs a day. He talkedabout quitting from time to time, but never seriously tried.
Plenty of time for that, he figured. Older people got cancer. Not people in their 30s, notpeople who worked in construction, as a roofer, as a mechanic.
He had no health insurance. But he was more worried about his mother, 57, who hadsmoked since she was 25.
"He would say, "Mom, don't worry about me. Worry about yourself. I'm healthy,' "Louise Curtis remembers. "You think this would happen later, when you're 60 or 70 yearsold, not when you're his age."
He knew, only a few days after he went to the hospital on April 2 with severe abdominalpain, how wrong he had been. He had oat cell lung cancer that had spread to his liver. Heprobably had not had it long. Also called small cell lung cancer, it's an aggressive killerthat usually claims the lives of its victims within a few months.
While it seems unusual to the Curtis family, Dr. Jeffrey Paonessa, Bryan's oncologist, saidhe is seeing more lung cancer in young adults.
"We've seen lung cancer earlier and earlier because people are starting to smoke earlierand earlier," Paonessa said. Chemotherapy sometimes slows the process, but had little

effect in Bryan's case, he said.
Bryan also knew, a few days after the diagnosis, that he wanted somehow to try to save atleast one kid from the same fate. He sat down and talked with Bryan Jr. and his 9-year-old daughter, Amber, who already had been caught once with a cigarette. But he wantedto do more. Somehow, he had to get his story out.
When he still had some strength to leave the house, kids would stare.
"They'd come up and look at him because he looked so strange," Louise Curtis said."He'd look at them and say, "This is what happens to you when you smoke.'
"The kids would say, "Oh, man. I can't believe it,' " Louise Curtis said.
In the last few weeks, Bryan's mother has been the agent for his mission to accomplishsome good with the tragedy. She has called newspapers and radio and television stations,seeking someone willing to tell her son's story, willing to help give him the one thing hewanted before he died. Bryan never got to tell his story to the public. He spoke for the lasttime an hour before a visit from a Times reporter and photographer.
"I'm too skinny. I can't fight anymore," he whispered to his mother at 9 a.m. June 3. Hedied that day at 11:56 a.m., just nine weeks after the diagnosis.
Bryan Lee Curtis Sr. was buried at Memorial Park Cemetery in St. Petersburg on June 8,a rare cloudy day that threatened rain.
At the funeral service at nearby Blount, Curry and Roel Funeral Home, Bryan's casketwas open and 50 friends and relatives could see the devastating effects of the cancer.
Addiction is more powerful.
As the graveside ritual ended, a handful of relatives backed away from the gathering,pulled out packs of cigarettes and lit up.
Originally Published on June 15, 1999 in the St. Petersburg Times
Posted at www.WhyQuit.com on July 15, 1999

January 23, 2001 - "It's almost been 2 years now. We set and watch homemovies of us. His son is missing him too. Christmas was the worst. He had togo outside and show his dad what he got for Christmas. That really tore meup." Bobbie Jo Curtis
February 28, 2002 - Bobbie indicates that Bryan's mother was able to quitsmoking following her son's death. Bryan Jr. will turn six on August 23, 2002,at which time he will have been fatherless for more than half his life.
Email Bobbie and Bryan Jr.
Have you met Noni?
Have you heard 19 year old Sean's message ...
... or from those lucky enough to survive the worst scare of their life!
Why do two million middle-aged smokers smoke themselves to death each year?
Will you be one of them? Knowledge is power!

WhyQuit.Com | About Us | Contact Us | Link to Us | What's New?
Last Updated on August 10, 2003 byJohn R. Polito

The Addiction Cycle
Lesson 9-5 Graphic: The Addiction Cycle
1Within seconds of inhaling,nicotine speeds its way to
your brain.
2In your brain, nicotinecauses the release of a
chemical called dopaminewhich stimulates feelings ofpleasure and relaxes you.
3But as soon as you stopsmoking, this stimulationwears off as the nicotinelevel in your body falls.
4Your brain starts to crave
another “hit” of nicotine—telling you to smoke another cigarette.
5Over time, your brainbecomes accustomed
to nicotine stimulation.Once this happens,
you experienceunpleasant withdrawal
symptoms if yournicotine craving is
not satisfied.
6So you smoke another
cigarette. And thecycle starts over again.

Page 9.6.1
Knowing the Rules about SmokingLesson 9-6
Lesson Objectives:
By the end of Lesson 9-6, students will:
W be familiar with school policy related to smoking by reviewing the school's codeof conduct.
W know and understand the rules and regulations that govern tobacco use in theirlocal community.
Materials:
W School smoking policy in student or faculty handbook (if available)
Key Terms:
penalty: consequences of disregardingpolicies, or disobeying rules and regula-tions
policy: rules and regulations that governbehaviors such as smoking
Introduction: The goals of this lesson are to familiarize students with the school'stobacco use policies, to consider why such policies are important, and to think about the responsibilities leaders in the schools—students and educators—and in the broader community have to promote healthful and safe behavior.

Page 9.6.2
Lesson 9-6: Knowing the Rules about Smoking
Procedures:
1. Review the school policy related to smoking on campus:
W Is anyone allowed to smoke at school?
W Are there designated smoking areas?
W Can adults smoke at extra-curricular activities on campussuch as sports events? What about on weekends?
W What support does the school provide to help smokers quit?
W What are the consequences of students smoking?
2. Point out that students often interpret school rules as simply yet another
restriction on students’ behaviors. Yet what about smoking outside of school?
Ask your students:
W Are there rules outside of school that control where people may or may not smoke? What about smoking at
the mall? In the park? At the beach? In the workplace? Inrestaurants?
W Why do you think these rules were made?
Ask your class to consider rules governing smoking in
places beyond the school, including: the workplace,restaurants and bars, public spaces such as parks, etc.Students may interpret school rules as simply another
restriction on their behaviors. Point out the role of suchrestrictions in other aspects of regular life for everyone (e.g., working,shopping, going to the park or mall, seeing a movie, etc.). Point out that
rules seen as restricting student behaviors may also be seen as designed topromote health and discourage unhealthful behaviors.
3. Ask students to consider the following questions:
W Do older students influence younger students? In what ways? What aboutpopular students? Athletes?
W Do teachers and other adults at school influence students? In what ways?
W If a student who is on the basketball team or in a school club gets caughtsmoking, should they be excluded from games or club activities?
W Is it okay for some people to break smoking rules? Who?
W Do you think it is cool to break rules?
Teacher’s Note:Ask the students what they think
of these rules and regulations. Are they fair? Are they enforced?Are they enough? Do they need
to do more?
Data Resource:It is useful to be familiar with the
ordinances governing smoking andtobacco use in your local community.
Your community’s ordinances maybe listed on sites such as the following:
www.no-smoke.org/lists.html
In addition, some state and localgovernments and other private
agencies maintain state-specific lists,such as the following for New Jersey:
www.njgasp.org

Page 9.6.3
Lesson 9-6: Knowing the Rules about Smoking
4. Ask students to consider the following statement:
Some people have a strong influence on others because of who
they are or what they do. These people should have to behavemore responsibly to set good examples for others.
Divide the class into two groups. Each group will take opposite
positions on this statement—for and against.
Explain to students that they must argue these positions asthough they very firmly believe them! The discussion must include the following
rules:
W Be respectful of others
W Don't interrupt
Allow each team five minutes to express their views initially. Then allow eachteam an additional five minutes to provide a rebuttal statement to the otherteam’s arguments. Finally, ask each team to make a summary statement.
5. Facilitate a discussion to find out what the experience was like, what theylearned, and whether anyone’s opinions were swayed one way or another on this
issue.
Journal:
Who are the people that you look up to? Why do you look up to them? If they
did something that was unhealthy, unkind, or wrong, how would it affect yourfeelings and actions?
Procedures: (continued)
Teacher’s Note:You may have to provide an exam-
ple of, for example, a sports starwho behaves badly, or a movie star
who smokes. Are these peoplesometimes allowed to break the
rules? Why do you think this is so?

Page 9.7.1
Saying “No!” to Tobacco
Lesson 9-7
Lesson Objectives:
By the end of Lesson 9-7, students will be able to:
W Critically examine both tobacco and anti-tobacco advertising strategies
W Present arguments, via a composed letter to an imaginary person who is considering smoking, for being smoke-free
W Present strategies for refusing cigarettes when offered.
Materials:
W Anti-tobacco advertising samples (provided on CD)
W Stationery for letters
Introduction: In this lesson, students are asked to critically examine advertisingstrategies that have been undertaken by tobacco companies. They are also asked toexamine samples of anti-tobacco advertising that have borrowed similar strategies tomarket the ideas of avoiding tobacco. Students are encouraged to think about howthey are influenced and in turn can influence others when it comes to behaviors suchas tobacco use.

Page 9.7.2
Lesson 9-7: Saying “No!” to Tobacco
Procedures:
1. Review with your students the Tobacco Advertisement worksheets handed outin Lesson Module 9-3.
Ask first about instances in which students saw smoking or tobacco usage on television. As students relate the circumstances, ask them to think about how theact of smoking was portrayed. For example, a nervous character might be seen to
reach for a cigarette, portraying the notion of a “relaxing smoke”; or a popularcharacter may pull out a cigarette and light up in front of friends, portraying thenotion of “cool”; or a character may intimidate another by blowing smoke in the
other’s face, portraying the notion of “power”; ora character may be shown as looking foolishwhen they smoke, providing a negative portrayal
of smoking. Discuss how people’s views of smoking can be shaped by what they see on television and in the movies.
Ask students to review the places they observedtobacco advertisements. See who came up withthe greatest number of locations and types of
advertisements. If people noticed clothing,explain that these items are often promotionalitems—given away for free—that were once
distributed by the tobacco companies. Ask students to think about why a companywould give away a free shirt or hat. Discuss how
this type of marketing might influence a person’sdecision to buy certain products.
Ask students if anyone saw smoking in a movie.
Discuss with students that cigarette companiesused to pay to have their products displayed inmovies (product placement). Ask the students if
they think this type of advertising works or not.
Teacher’s Note:As part of the 1998 Tobacco Master SettlementAgreement that was reached between major tobaccocompanies and 46 states, the tobacco industry agreedto a number of new restrictions on tobacco advertis-ing (joining the ban on television advertisements fortobacco products). Included in these restrictions arebans on the use of cartoons in advertising or pack-aging for tobacco products; elimination of most out-door advertising, including billboards, and signs and placards in arenas, stadiums, shopping malls, andon transit (e.g., buses and trains); and forbids thesale or distribution of apparel and merchandise withbrand name logos (although many tobacco companiescontinue to give away free merchandise in exchangefor “points” or “coupons” that accrue with eachpurchase of cigarettes.
The Master Settlement Agreement also bans pay-ments to promote tobacco products in movies, ontelevision shows, in videos and video games, andother entertainment. Tobacco companies are alsoprohibited from brand name sponsorship of eventswith a significant youth audience (football, basket-ball, baseball, hockey and soccer).
You can read more about this at:
http://caag.state.ca.us/tobacco/resources/msasumm.htm
An Interesting Anecdote:Although it may be dated to discuss Steven Spielberg’smovie E.T., it may be instructive to relate the tale of howthe film boosted sales of a particular brand of candy. Inthe movie, the young boy Elliot uses candy to lure E.T.into his home. The scene established the bond betweenthe boy and the extra-terrestrial that is at the heart of thefilm. The scene shows E.T. making satisfying noises as itfollows and eats the colorful trail of candy into Elliot’sbedroom. The filmmakers approached the makers of
M&M candies to see if they could use that product in thefilm. But the Mars Candy company balked, unsure if theywanted their candy associated with a “space and aliens”movie. The filmmakers instead turned to the makers ofReese’s Pieces, and the distinctive orange packaging wasclearly displayed throughout the scene. After the releaseof the movie, sales of Reese’s Pieces jumped dramatically,even though the name of the product was never mentionedin the film.
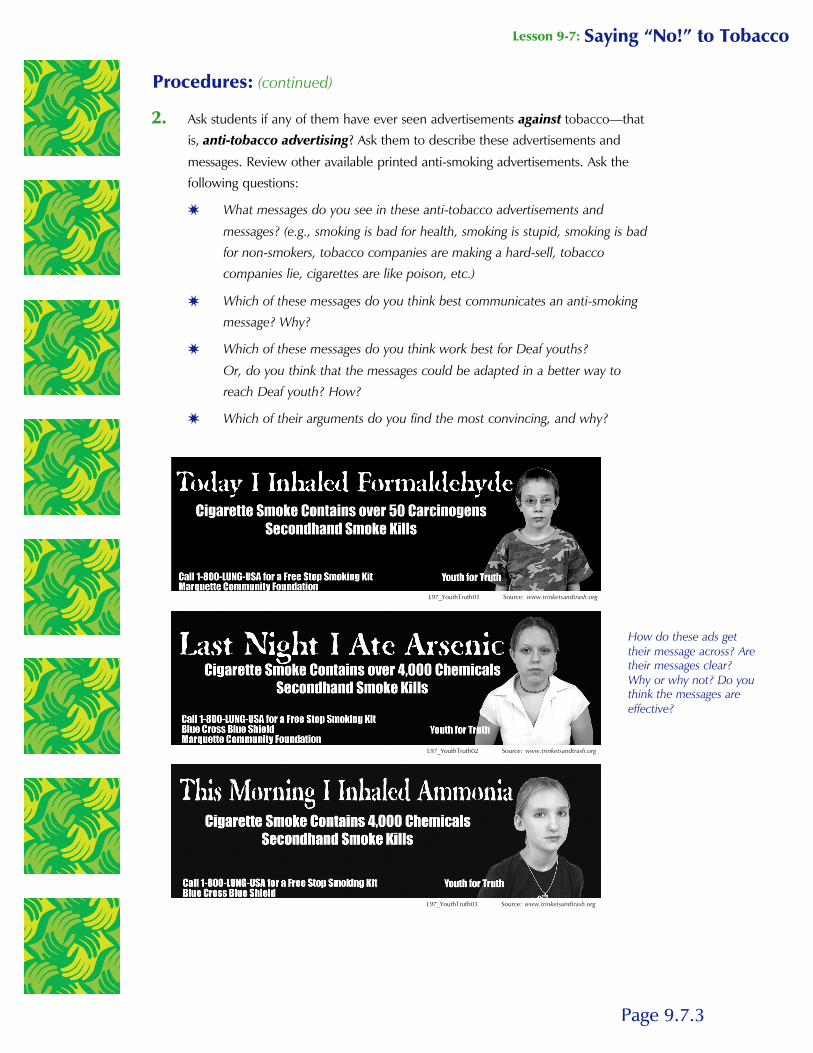
Page 9.7.3
Lesson 9-7: Saying “No!” to Tobacco
2. Ask students if any of them have ever seen advertisements against tobacco—thatis, anti-tobacco advertising? Ask them to describe these advertisements and
messages. Review other available printed anti-smoking advertisements. Ask thefollowing questions:
W What messages do you see in these anti-tobacco advertisements and
messages? (e.g., smoking is bad for health, smoking is stupid, smoking is badfor non-smokers, tobacco companies are making a hard-sell, tobacco companies lie, cigarettes are like poison, etc.)
W Which of these messages do you think best communicates an anti-smokingmessage? Why?
W Which of these messages do you think work best for Deaf youths?
Or, do you think that the messages could be adapted in a better way toreach Deaf youth? How?
W Which of their arguments do you find the most convincing, and why?
Procedures: (continued)
L97_YouthTruth01 Source: www.trinketsandtrash.org
L97_YouthTruth02 Source: www.trinketsandtrash.org
L97_YouthTruth03 Source: www.trinketsandtrash.org
How do these ads gettheir message across? Aretheir messages clear?Why or why not? Do youthink the messages areeffective?

Page 9.7.4
Lesson 9-7: Saying “No!” to Tobacco
Procedures: (continued)
What about these ads that usehumor? What do you think the mes-sages are? Are they effective? Why orwhy not?
s
What about this advertisement? Whodo you think the target is? Do youthink the message is clear?
L97_ButtsGross Source: www.trinketsandtrash.org
L97_JoeChemo Source: www.trinketsandtrash.org
L97_UtterFool Source: www.trinketsandtrash.org
L97_MarlboroCountry Source: www.trinketsandtrash.org
L97_Scent Source: www.trinketsandtrash.org
L97_Girnoneck Source: www.trinketsandtrash.org

Page 9.7.5
Lesson 9-7: Saying “No!” to Tobacco
Procedures: (continued)
L97_nightclub Source: The American Legacy Foundation L97_fence Source: The American Legacy Foundation
L97_ammonia Source: The American Legacy FoundationL97_karma Source: The American Legacy Foundation
L97_TruthCowboy Source: The American Legacy Foundation
Are you familiar with the Truth adver-tisements?
These advertisements were createdby the American Legacy Foundationas part of a campaign targeted especially at young people: The Truth Campaign.
The focus of these advertisementshas been to get the “truth” out abouttobacco, and that has been hiddenby the companies that make tobaccoproducts.
How convincing or effective arethese advertisements?
s
Teacher’s Note:Students can explore for themselves the American
Legacy Foundation’s website at:
www.thetruth.com

Page 9.7.6
Lesson 9-7: Saying “No!” to Tobacco
Procedures: (continued)
L97_Chinese02 Source: www.trinketsandtrash.org
L97_Thai01 Source: www.trinketsandtrash.org
L97_NoEscapeChinese Source: www.trinketsandtrash.org
L97_LatinoColorade Source: www.trinketsandtrash.org
L97_Japanese Source: www.trinketsandtrash.org
L97_NoEscape_English Source: www.trinketsandtrash.org
What about these messages aimed atdifferent ethnic groups? Looking justat those non-English advertisements,can you still figure out the messageof the ad? What might this say aboutthe need to reach out to thosegroups that are less literate inEnglish?
s

Page 9.7.7
3. Ask students to think about the best ways to reach Deaf youth like themselveswith anti-tobacco information. What would the best channels be? Television? The
internet? In school? Through plays or other popular entertainment? What aboutthe use of media that have been adopted by the Deaf, such as instant messaging,text messaging, the internet, and other communication modes?
Ask your students:
W If you were trying to reach the Deaf with anti-tobacco information, whichapproach would you use?
4. Ask students to review the facts and myths they have learned about smoking inLesson 9.5:
W Most smokers started when they were young.
By the 8th grade, 28%, or about 3 out of 10 persons say they have triedsmoking. By 10th grade, 43%, or about 4 out of 10 persons. By 12thgrade, 53%, or a little more than half of all young people say they have
tried smoking at least once.
Lesson 9-7: Saying “No!” to Tobacco
Procedures: (continued)
L97_weapon Source: www.trinketsandtrash.org
L97_ChewComponents Source: www.trinketsandtrash.org
What about these advertisements thatpoint to the content of cigarettes andsmokeless tobacco?
s L97_Frog

Page 9.7.8
W Most smokers wish they had never tried smoking.More than one out of every three young people who ever try smoking a
cigarette become regular, daily smokers before leaving high school.
W Most young smokers think they can stop whenever they want.If you ask a high school student who smokes every day if they think they
will still be smoking in five years, almost all of them say no. But if you talkto them again when they are adults, most will still be smoking.
W Most smokers have a hard time quitting because nicotine is very
addictive. By high school, nearly three out of every four regular smokershave already tried to quit smoking, and failed.
5. Review (from lessons 9-2 and 9-3) for your students some of the reasons why
young people start to smoke cigarettes or use tobacco.
6. The following exercise can be done individually or in groups.
Explain to students that a person their age named Jamie is thinking about
smoking. Jamie has not yet decided but feels a lot of pressure to smoke. The task for your students is to write a letter to Jamie to convince him NOTsmoke. Remind your students to think about the following:
W What anti-smoking messages do you find to be the most compelling?
W What strategies do you think Jamie can use to resist the pressure to smoke?
Remind students of the refusal skills that have been discussed in Lesson 9-2:
W Be direct
W Change the subject
W Think of a clever response
W Joke
W Walk Away or Avoid the Situation
W Blame an Adult
7. When the letters are complete, ask your students to share their letters with theclass. Discuss the range of ideas that were suggested.
Journal:
Did you ever do something because of peer pressure that you regretted later on?What would have stopped you? Who could have influenced you to make a different decision?
Procedures: (continued)
Lesson 9-7: Saying “No!” to Tobacco