Embed Size (px)
Citation preview

1
Handout for lecture on lymphoblastic neoplasms presented by Rob McKenna
• The following slides represent a near final version of the presentation that will be given in Maui, January 23,2018. Minor changes in slides and order of slides may appear in the actual lecture.
Lymphoblastic Neoplasms Presented by: Robert W. McKenna
Notice of Faculty DisclosureIn accordance with ACCME guidelines, any individual in aposition to influence and/or control the content of this CMEactivity has disclosed all relevant financial relationshipswithin the past 12 months with commercial interests thatprovide products and/or services related to the content ofthis CME activity.
The individual below have responded that they have norelevant financial relationship with commercial interest todisclose:
Robert W. McKenna, MD

2
Lymphoblastic Leukemia / Lymphoma(Acute Lymphoblastic Leukemia – ALL)
• Morphology and Immunophenotype
• Genetics
• WHO Classification‐2016
• Prognostic indicators– MRD
• Current status and future
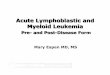
Lymphoblasts in two Patients with ALL
Lymphoblasts in two Patients with ALL

3
Cytoplasmic Granules in Lymphoblasts in ALL
t(9;22) B ALL Down Syndrome-B ALL
Hematogones
Bone marrow B‐cell precursors
Size and morphology bridge mature lymphocytes and neoplastic lymphoblasts
Large percentages seen in healthy infants and young children
Increased in ◦ Regenerating marrows◦ Autoimmune or congenital
cytopenias◦ Lymphoma, neuroblastoma◦ AIDS
Immunophenotyping
• Distinguishes ALL from AML and B from T ALL
• Identifies subsets of both B and T ALL
• Immunophenotypic prognostic / treatment groups
• T‐lymphoblastic higher risk
than B‐lymphoblastic
• Early T cell precursor leukemia, CD10(‐) B ALL, etc.
• MRD detection
B ALL
T ALL

4
Cytogenetics in ALL
• Defines prognostic and treatment groups– one of the most important factors in risk‐stratification treatment
• Defines categories of B lymphoblastic leukemia in WHO classification
Karyotype Abnormalities
• 75% of all cases
• 80% of B lymphoblastic leukemia
•50‐‐60% of T lymphoblastic leukemia
•Significantly higher by molecular cytogenetics (FISH)
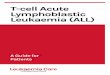
Frequency of specific genotypes in childhood lymphoblastic leukemia
Pui C et al. JCO 2011;29:551-565
Relationship of Cytogenetics to Prognosis in B ALL
Prognostic Group Cytogenetic Abnormality
• Low Risk Hyperdiploidy >50t(12;21)
• Intermediate Risk Hyperdiploidy 47‐50Diploid, 6q‐, t(1;19)9p abnormalities
• High Risk Hypodiploid‐Near Haploidt(9;22), t(4;11), t(5;14)t(17;19)

5
B Lymphoblastic Leukemia with Hyperdiploidy
B Lymphoblastic Leukemia with t(9;22)(q34;q11.2), BCR‐ABL1
Gene Expression Profile of 132 Pediatric ALLBlood. 2003; 102:2951‐2959

6
Complex genomic alterations and gene expression in
acute lymphoblastic leukemia with intrachromosomal
amplification of chromosome 21 Jon C. Strefford*†‡, Frederik W. van Delft†§¶, Hazel M. Robinson*, Helen Worley*, Olga Yiannikouris§¶, Rebecca Selzer , Todd Richmond , Ian Hann**, Tony Bellotti††, Manoj Raghavan¶, Bryan D. Young¶, Vaskar Saha†§¶, and Christine J. Harrison*†
We have previously identified a unique subtype of acute lympho- blastic leukemia (ALL) associated with a poor outcome and char- acterized by intrachromosomal amplification of chromosome 21 including the RUNX1 gene (iAMP21). In this study, array-based comparative genomic hybridization (aCGH) (n 10) detected a common region of amplification (CRA) between 33.192 and 39.796 Mb and a common region of deletion (CRD) between 43.7 and 47 Mb in 100% and 70% of iAMP21 patients, respectively. High- resolution genotypic analysis (n 3) identified allelic imbalances in the CRA. Supervised gene expression analysis showed a distinct signature for eight patients with iAMP21, with 10% of overex- pressed genes located within the CRA. The mean expression of these genes was significantly higher in iAMP21 when compared to other ALL samples (n 45). Although genomic copy number correlated with overall gene expression levels within areas of loss or gain, there was considerable individual variation. A unique subset of differentially expressed genes, outside the CRA and CRD, were identified when gene expression signatures of iAMP21 were compared to ALL samples with ETV6-RUNX1 fusion (n 21) or high hyperdiploidy with additional chromosomes 21 (n 23). From this analysis, LGMN was shown to be overexpressed in patients with iAMP21 (P 0.0012). Genomic and expression data has further characterized this ALL subtype, demonstrating high levels of 21q instability in these patients leading to proposals for mechanisms underlying this clinical phenotype and plausible alternative treatments. PNAS (2006); 103: 8167-72
Contributions of Newer Technologiesin Molecular Genetics
• High‐resolution genome‐wide analysis
– Provides new insights into pathobiology of ALL
– Identifies novel subtypes of leukemia, especially markers of high‐risk disease
– Potential targets for molecular based therapy
N Engl J Med 2009; 360:470-80

7
Deletion of IKZF1 in ALL
• Encodes lymphoid transcription factor IKAROS
• Frequent event (80%) in BCR‐ABL1 positive ALL
• Associated with MRD at day 29, relapse and poor outcome
• Poor outcome in both BCR‐ABL1 (+) and BCR‐ABL1 (‐) [“BCR‐ABL1‐like”] ALL
Blood 2010;115:5312-21
WHO Classification of Lymphoblastic Leukemia/Lymphoma‐‐2017
• B lymphoblastic leukemia/lymphoma, NOS
• B lymphoblastic leukemia/lymphoma with recurrent genetic abnormalities (9 categories)
• T lymphoblastic leukemia/lymphoma (1 subset)
• Natural killer cell leukemia/lymphoma (provisional)

8
B Lymphoblastic Leukemia/Lymphoma (B LL/L) With Recurrent Genetic Abnormalities
• B LL/L with t(9;22)(q34.1;q11.2); BCR‐ABL1
• B LL/L with t(v;11q23.3); KMT2A/MLL rearranged
• B LL/L with t(12;21)(p13.2;q22.1); ETV6‐RUNX1/TEL‐AML1
• B LL/L with hyperdiploidy
• BLL/L with hypodiploidy*• Near haploid
• Low hypodiploid
• B LL/L with t(5;14)(q31.1;q32.1); IGH/IL3
• B LL/L with (1;19)(q23;p13.3); TCF3‐PBX1/E2A‐PBX1
• B LL/L BCR‐ABL1‐like (provisional)*
• B LL/L with iAMP21 (provisional)*
B Lymphoblastic Leukemia/Lymphoma with Hypodiploidy (hypodiploid ALL)
• 5% of ALL; 1% with<45 chromosomes
– Near haploid (23‐29 chromosomes)
• RAS or receptor tyrosine kinase mutations
• Poor prognosis
– Low hypodiploid (33‐39 chromosomes)
• TP53 (some germline) and/or RB1 mutations
• ? Is low hypodiploid ALL a form of Li‐Fraumeni syndrome
• Poor prognosis
– High hypodiploid (40‐43 chromosomes)
– Near diploid (44‐45 chromosomes)
B Lymphoblastic Leukemia/Lymphoma with iAMP21
• 2% of B ALL; more common in older children
– Detected with FISH probe to RUNX1
– 5 or more copies of RUNX1 or 3 or more on a single abnormal chromosome
– 80% have other chromosome abnormalities (gains in X, abnormalities of 7)
– Deletions of RB1 and ETV6; rearrangement of CRLF2
– Constitutional Robertsonian translocation rob(15;21)q10;q10)c has 3000 fold increase in this leukemia; appears to involve chromothripsis
• Relatively poor prognosis with standard therapy

9
B Lymphoblastic Leukemia/Lymphoma, “BCR‐ABL1‐like”
• Lack the BCR‐ABL1 translocation but have a very similar gene expression profile to ALL with BCR‐ABL1
• 10‐25% of B ALL
–Frequency lowest in children with standard risk ALL
–Higher in those with high risk ALL, adolescents, and adults
–Higher in children with Downs, Hispanics and native Americans
Genetics of B lymphoblastic Leukemia/Lymphoma, “BCR‐ABL1‐like”
• Different types of chromosomal rearrangements
– Many different genes and partners involved
– May require complex laboratory analysis to identify these
• CRLF2 rearrangements account for about half
– Often show interstitial deletion of pseudoautosomal region Xp22.3 and Yp11.3
– Half of these have mutations of JAK2 or JAK1
• TK‐type translocations, ABL1 or other kinases
– Over 30 different partner genes described
• Many BCR‐ABL1‐like ALL show deletions or mutations in genes important to leukogenesis
– IKZF1 and CDKN2A/B
Treatment and Prognosis of B Lymphoblastic Leukemia/lymphoma, “BCR‐ABL1‐like”
• Overall poor prognosis
– Other high risk features• Older age; High WBC; MRD (+)
• High risk of relapse independent of all other risk factors
• Most have targetable lesions involving ABL or JAK‐STAT signaling pathways
– ABL, PDGFRB, etc‐‐‐‐Dasatinib
– CRLF2, JAK2, etc‐‐‐‐‐‐Ruxolitinib

10
T Lymphoblastic Leukemia/Lymphoma (T LL/L)
• T lymphoblastic leukemia/lymphoma (T LL/L)
– Early T‐cell precursor LL/L*
• Natural killer cell leukemia/lymphoma (provisional)*
T Lymphoblastic Leukemia
T Lymphoblastic Lymphoma

11
1205.310102401
T Lymphoblastic Lymphoma-Low Level BM Involvement
Flow Cytometry Histograms of BM From a Patient with Low Level Involvement with T Lymphoblastic Lymphoma
T Lymphoblastic leukemia/Lymphoma
• Improved prognosis with intensive chemotherapy regimens
• 65% to 75% overall survival in children
• Conventional cytogenetics studies are less contributory in identifying risk groups
• Immunophenotype and gene expression profile identify A sub‐set of TLL/L: Early T‐Cell Precursor Leukemia (ETP‐ALL)

12
Lancet Oncol. 2009; 10: 147-156
Early T‐Cell Precursor (ETP) Leukemia
• 10% to 15% of T ALL
• Derived from a subset of thymocytes that retain stem cell‐like features
• Distinctive phenotype
– CD1a‐, CD8‐,CD5weak with stem cell/myeloid agns.
• ETP related gene expression signature
Early T‐Cell Precursor LeukemiaCoustan‐Smith MS, etal. Lancet Oncol. 2009, 10:147‐56

13
Prognosis of Early T cell Precursor ALL (ETP‐ALL)
• Initial descriptions reported a very poor outcome compared with other T ALL
• More recent larger studies with more effective therapy show little or no effect on outcome for ETP‐ALL
• This despite higher rates of MRD following induction therapy
Prognostic Indicators In ALL
• Clinical
– Age
– Leukocyte count
– CNS involvement
• Immunophenotype
• Cytogenetics
• Rapidity and degree of cytoreduction and MRD
Minimal Residual Disease (MRD)
• Early treatment response is most important prognostic factor in ALL
• Early response reflects:
– Leukemic cell genetics
– Host pharmacodynamics and pharmacogenetics
– Effectiveness of treatment regimen
• Assessed by measurements of MRD

14
Sensitivity of Methods for Detection of Lymphoblasts in Bone Marrow
• Flow Cytometry ‐‐‐‐‐‐‐‐‐ 0.01% to 0.005%
• Molecular (PCR) ‐‐‐‐‐‐‐‐‐ 0.01% to 0.0001%
Diagnostic Marrow Following Induction Rx
Minimal Residual Disease in a Patient with B ALL (t(9;22)(q34;q11.2); BCR/ABL1)
0.01% B Lymphoblasts
Courtesy of Steven H. Kroft, M.D.
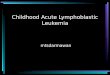
Prognostic Significance of End of Induction MRD in Patients with ALL
Borowitz MJ, etal. (2008) Blood; 111: 5477-5485

15
Prognostic Significance of End of Consolidation MRD in Patients with ALL
Borowitz MJ, etal. (2008)Blood; 111: 5477-5485
197 relapsed33 relapsed
COG Risk Classification of B ALL
• First assigned to “standard” or “high risk”– Patient age
– White blood cell count
• Cytogenetic abnormalities and MRD then refine risk classification
– Low• High hyperdiploidy, t(9;21)
– Standard/intermediate
– High• Age, WBC
– Very high• Hypodiploidy, Ph+ ALL, Ph‐like ALL, iAMP21, t(17;19)
• High level MRD after induction and persistent MRD at later time points
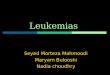
Five‐year survival rates for children less than 15 years old with ALL: 1960‐2004. SEER Cancer Statistics Review.

16
Prognosis for Children with ALL‐‐2016
• 10 to 20% of children with B ALL and 25 to 35% with T ALL are not cured
• Relapsed ALL remains the 4th commonest childhood malignancy
• Most common cause of cancer deaths in kids
• Further improvement by dose‐escalation will be limited by toxicities
• To improve cure rates further less toxic targeted approaches are necessary
– Eg., tyrosine kinase inhibitors, JAK inhibitors,
– CAR T‐cells (anti CD19 engineered T cells), etc.
Thank you! Questions?
Natural Killer(NK) Cell Lymphoblastic Leukemia/Lymphoma (provisional)
• Difficult to define– Many (CD56 +) reported cases
are now recognized as blastic plasmacytoid dendritic neoplasms
– May have a primitive immunophenotype indistinguishable from AML‐minimally differentiated (myeloid/NK acute leukemia)
– Early NK‐cell progenitors lack specific markers or overlap with T‐ALL (CD7, CD2, even CD5 and CD3 epsilon)‐distinction may be difficult
– More mature markers (CD16) are rarely expressed (CD94 or CD161 are not commonly tested
• May be considered in cases expressing CD56 and T‐associated antigens such as CD7, CD2 and even cCD3 if T‐cell and IG receptor genes are germline and blastic plasmacytoid dendritic cell leukemia is excluded– Hopefully wider availability of
more specific NK markers such as panels against KIRs will help clarify the disease
• Best considered a provisional entity