Embed Size (px)
Citation preview

Handling Cytotoxic Drugs;A HEALTH AND SAFETY REVIEW

HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
OVERVIEWAnsell Healthcare Products LLC has an ongoing commitment to the development of quality hand barrier products and services for the healthcare industry. This self-study, Clinical Reference Manual: Handling Cytotoxic Drugs; a Health and Safety Review, is one in a series of continuing educational services provided by Ansell. This educational module examines glove use in handling cytotoxic drugs.
INTENDED AUDIENCEThe information contained in this self-study guidebook is intended for use by healthcare professionals who are responsible for or involved in the following activities related to this topic:
• Educating healthcare workers
• Establishing institutional or departmental policies and procedures
• Decision-making responsibilities for hand-barrier products
• Maintaining regulatory compliance with agencies such as OSHA, ANA and CDC
• Managing employee health and infection prevention services
PROGRAM OVERVIEWUpon completion of this educational activity, the learner should be able to:
• Discuss hazardous drugs used in chemotherapy
• Discuss standard testing method of material used in handling chemotherapy drugs
• Describe steps to prepare and administer cytotoxic drugs
• Describe the characteristics of good barrier protection of the different gloving materials available
• Discuss standard of practice to glove use in handling chemotherapy drugs

HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
INSTRUCTIONSAnsell Healthcare is a provider approved by the California Board of Registered Nursing, Provider # CEP 15538 for 2 contact hour(s). Obtaining full credit for this offering depends on completion of the self-study materials on-line as directed below.
Approval refers to recognition of educational activities only and does not imply endorsement of any product or company displayed in any form during the educational activity. To receive contact hours for this program, please go to the "Program Tests" area and complete the post-test. You will receive your certificate via email.
AN 85% PASSING SCORE IS REQUIRED FOR SUCCESSFUL COMPLETION
Any learner who does not successfully complete the post-test will be notified and given an opportunity to resubmit for certification.
For more information about our educational programs please contact Ansell Healthcare Educational Services at 1-732-3452162 or e-mail us at [email protected].
Planning Committee Members: Luce Ouellet, DESS, BSN, RN Patty Taylor RN, BA Pamela Werner, MBA, BSN, RN CNOR
As employees of Ansell; Mme Ouellet, Mrs. Taylor and Ms. Werner have declared an affiliation that could be perceived as posing a potential conflict of interest with development of this self-study module.
Roy Zacharius Jr., CST, BS, FAST
As an employee of The Meridian Institute, Mr. Zacharias has declared an affiliation that could be perceived as posing a potential conflict of interest with the development of this self-study module.
This module will include discussion of commercial products referenced in generic terms only.
Ansell Healthcare Products LLC
111 Wood Avenue South, Suite 210 Iselin, NJ 08830 USA Tel: 1-800-952-9916 www.ansellhealthcare.com

HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
; A
HE
ALT
H A
ND
SA
FETY
RE
VIE
W
CONTENTS Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Classes of Cytotoxic Drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Carcinogenic Agent Toxicology. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Securing Health Professionals; Handling Hazardous Drugs . . . . . . . . . . . . . . . . 3
The Standards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Effects of Chemicals on Gloves . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Testing for Glove Permeation by Chemotherapy Drugs. . . . . . . . . . . . . . . . . . . . 5
Interpreting Breakthrough Time . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Glove Selection in Handling Cytotoxic Drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Glove Fit and Sizing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Double Gloving . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Donning and Doffing Gloves . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Donning Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Closed Donning Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Open Donning Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Glove Removal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Removing Examination Gloves Safely. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Glove Recommendations in Handling Cytotoxic Drugs . . . . . . . . . . . . . . . . . . . 11
Drug Preparation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Working Securely with Cytostatics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Administering Cytostatics to Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Drug Administration; Glove use Recommendation . . . . . . . . . . . . . . . . . . . . . . 14
Drug Clean Up and General Handling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Summary of Glove Use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16

1
INTRODUCTION According to the World Health Organization (WHO), between now and 2030 the cancer rate is going to increase by 50% to about 13 million new cases a year, worldwide. The predicted increase in new cases will mainly be due to the existence of a steadily aging population in both developed and developing countries, but also to the current prevalence of smoking and the rise in numbers of those adopting unhealthy lifestyles1. One of the most frequently used treatments for cancer is chemotherapy.
Chemotherapy treatments are utilized in suppressing and/or inhibiting cell growth and division. It is used as an adjuvant to surgery, and/or treatment of metastatic cells. Unfortunately, it is well known that cytostatic agents are potentially hazardous for the manipulator (pharmacist, assistant, nurse, surgeon, pharmacy technicians, etc.)2. Cytostatics are known to be3:
• Mutagenic - induce or increase genetic mutations by causing changes in DNA. • Carcinogenic - cancer-causing in animal models, in patient population, or both. • Teratogenic - causing fertility impairment in animal studies or treated patients.
Some of the other potential effects are:
• Decrease in fertility • Fetal malformation • Abortion • Extra uterine pregnancy • High toxicity for certain organs
Handling cytotoxic drugs poses potential occupational risks. The occupational risk is highly dependent of the following criteria4:
• Intrinsic toxicity of cytostatic • Duration of exposure • Frequency of exposure • Handling method- before, during, and after use
CLASSES OF CYTOTOXIC DRUGSTraditional antineoplastic drugs, which still constitute most of the anticancer drugs used today, generally target either the DNA inside the nucleus of a cell directly, inhibit the synthesis of new DNA strands, or stop the mitotic processes of a cell. In the first case, the objective is to cause physical changes in the DNA itself, resulting in mutations of the DNA attempting to replicate. In the second case, these agents usually stop the synthesis of DNA by stopping the synthesis of the necessary building blocks of DNA. In the third case, the objective is to stop cell replication in one of the stages of mitosis, often by inhibiting synthesis or breakdown of the cellular structure.5

HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
; A
HE
ALT
H A
ND
SA
FETY
RE
VIE
W
2
I. Antineoplastic agents which directly attack DNA in the nucleus belong to the following categories:
A. Alkylating agents:
These agents directly alkylate or covalently modify the nitrogenous bases of DNA molecules. This can result in mispairing of bases, or loss of bases, or actual splitting of the DNA backbone.
Examples: • Altrtamine (Hexalen) • Busulfan (Myleran) • Carboplatin (Paraplatin) • Chlorambucil (Leukeran) • Cisplatin (Platinol) • Cyclophosphamide • Dacarbazine (DTIC) • Ifosfamide (Ifex) • Melphalan (Alkeran) • Oxiliplatin (Eloxatin) • Procarbazene (Matulane) • Telomozomide (Temodar) • ThioTEPA
B. Intercalating agents:
These agents bind tightly to the DNA double helix, preventing the unwinding of the double helix at that point.
Examples: • Dactinomycin (Cosmegen) • Daunorubicin (Cerubidine) • Doxorubicin (Adriamycin) • Plicamycin (Mithramycin)
C. DNA Topoisomerase inhibitors:
By inhibiting this enzyme involved in supercoiling, these agents somehow cause the actual scission or breakage of DNA strands in the nucleus.
Example: • Etoposide (VePesid, VP-16)
II. Antineoplastic agents which stop the synthesis of DNA precursors are:
A. Folic Acid antagonists:
These agents stop the formation of tetrahydrofolate, which is necessary for the synthesis of both purines and pyrimidines.
Example: • Methotrexate (MTX)
B. Purine antagonists:
These agents are competitive inhibitors of enzymes in the purine nucleotide synthetic pathways.
Examples: • Mercaptopurine (Purinethol) • Thioguanine (Tabloid)
C. Pyrimidine antagonists:
These agents are competitive inhibitors of enzymes in the pyrimidine nucleotide synthetic pathways.
Examples: • Floxuridine (FUDR) • Fluorouracil (5-FU) • Cytarabine (Cytosar, ARA-C)
D. Ribonucleotide diphosphate reductase inhibitors:
These agents will effectively interfere with DNA construction. These agents damage cells during S phase.
Example: • Hydroxyurea (Hydrea)

3
III. Antineoplastic agents which affect the synthesis or breakdown of the mitotic spindles belong to the general category of alkaloid antineoplastic drugs.
A. Alkaloids exert their actions on tubulin synthesis/breakdown:
Examples: • Vinblastine (Velban, Velsar) • Vincristine (Vincasar, Oncovin) • Pacitaxel (Taxol)
CARCINOGENIC AGENT TOXICOLOGYThe International Agency for Research on Cancer (IARC) is part of the WHO. Its major goal is to identify causes of cancer. The most widely used system for classifying carcinogens comes from the IARC. In the past 30 years, the IARC has evaluated the cancer-causing potential of more than 900 likely candidates, placing them into one of the following groups: 6 • Group 1: Carcinogenic to humans (109 agents) • Group 2A: Probably carcinogenic to humans (65 agents) • Group 2B: Possibly carcinogenic to humans (275 agents) • Group 3: Unclassifiable as to carcinogenicity in humans (503 agents) • Group 4: Probably not carcinogenic to humans (1 agent)
The hazards encountered during the preparation, administration, clean up and general handling of any cytotoxic drug have been well documented. Public concern is magnified by the perception that cancer risks are imposed upon workers, nurses and pharmacists that are involved in these procedures. The dangers of handling hazardous drugs come from
their inherent toxicity as well as the type of exposure that may occur in the workplace. Today that workplace environment may be a hospital clinic, other patient unit, a physician’s office, pharmacy, or in the patient’s home. Chemotherapy administration has also evolved over the years. Chemotherapy agents are administered via intravenous push as well as a continuous infusion through a variety of implanted access devices. Exposure, to the healthcare worker or a family member in the home, may be through ingestion of food that may have been exposed to the drug, inhalation of drug particles that may become aerosolized during preparation, handling of patient excreta during home care, or direct skin contact of the drug. Studies have been conducted to assess the indirect exposure of healthcare workers, i.e. nurses and pharmacists, to determine if there was any chromosomal damage to these workers that prepared and administered these drugs. This and other reports point to the need for excellent exposure control measures and excellent compliance to safe handling procedures.7
SECURING HEALTH PROFESSIONALS; HANDLING HAZARDOUS DRUGSThe Standards
The FDA Glove Guidance manual offers specific guidance for labeling exam gloves used in chemotherapy;

HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
; A
HE
ALT
H A
ND
SA
FETY
RE
VIE
W
4
“To market the glove for use in the handling and/or preparation of chemotherapeutic drugs, you should label the glove as a “Patient examination Glove” or “Surgeon’s glove” and tested for use with (name of chemotherapeutic drugs).
We recommend that you include the following labeling information: • Chemical resistance data (test method used, chemicals tested) for consumer review, if desired. • The statement “Gloves used forprotection against chemotherapy drug exposure should be selected specifically for the type of chemicals used” and instructions for users to review drug labeling or material safety data sheets for the chemicals being used to determine an adequate level of protection for the intended use.8
The Oncology Nurses Society mentions in their standards that “the use of a class II safety cabinet does not eliminate the need for PPE (Personal Protective Equipment).” “Because spills are possible during any handling, PPE must be used to prevent worker’s exposure.” Gowns made of materials that protect from Hazardous Drugs (HD) permeation and double gloves, tested to the ASTM standard 2005, are universally recommended for HD handling. USP 797 requires two pair of gloves, the outer one sterile, for compounding sterile preparations. When wearing double gloves, tuck the cuff of the inner glove under the gown sleeve and the cuff of the outer glove over the gown sleeve. Change the outer gloves immediately whenever contamination is suspected. Change both gloves if the outer glove is torn, punctured or contaminated by an obvious spill.
At the end of each batch, the outer gloves should be removed and sealed in a zipper-lock bag. Remove and discard the gown before removing the inner pair of gloves.”9
EFFECTS OF CHEMICALS ON GLOVESChemicals can penetrate, degrade, and/or permeate through a glove. All effects can happen at once. They can let chemicals through to skin. To understand, we must consider them one by one.
1. Penetration is defined as the movement of a chemical and/or micro-organism through porous materials, tears, pinholes or other imperfections or manufacturing defects in a protective glove material on a non-molecular level. It implies that you can see the holes.
2. Degradation is a deleterious change in one or more properties of a material. When degradation is caused by chemicals, the rubber swells, softens, and weakens and plastic shrinks, stiffens, or becomes brittle.
3. Permeation is the process by which a chemical moves through a protective glove material on a molecular level. It involves the following: a. Adsorption of the molecules of the chemical into the contacted or outer surface of a material b. Diffusion of the absorbed molecules in the material. c. Desorption of the molecules from the opposite or inner surface of the material
5
TESTING FOR GLOVE PERMEATION BY CHEMOTHERAPY DRUGSChemotherapy drugs can represent a significant health risk to healthcare personnel. Some chemotherapy drugs have been found to be carcinogenic, to cause chromosomal damage and may also cause damage to normal skin and necrosis of compromised skin. The most common exposures are the result of inadvertent ingestion of a drug on food, inhalation of drug dusts or droplets or direct skin contact. Proper training and the use of personal protective equipment such as suitable gloves are critical to the safety of healthcare workers who handle chemotherapy drugs.10
ASTM D 6978-05 is the test method specifically designed to test breakthrough times of cytostatic drugs on gloves. It is defined as “Standard of Practice for Assessment of Resistance of Medical Gloves to Permeation by Chemotherapy Drugs”.11 • Chemotherapy drugs used in testing incorporate a minimum of nine currently used clinical drugs • Test measurements using the thinnest area of the glove between palm and the cuff • Tested for up to 4 hours • Detection Limit is 0,01 µg (= 10 ng) / (cm² x min)
The ASTM F 739-07 “Resistance of protective clothing materials to permeation by liquids or gazes under continuous contact” is adapted to test chemicals breakthrough times on clothing used in the most industrial sector of activities.
• All chemicals • Test measurements using the palm of the glove • Tested for up to 2 hours • Detection Limit is 0,1 µg
Every glove may react differently in terms of permeation and therefore assumptions are not acceptable. Every cytostatic molecule may react differently in terms of permeation. Therefore, a claim as “Good for cytostatic handling” is dangerous and misleading. This is due to the physico-chemical heterogeneity of the cytostatics.
The Université Catholique de Louvain, Brussels, Belgium have developed a unique dynamic permeation device. They have tested gloves under dynamic physical conditions for stretching, tension, and rubbing.12
Not all drugs or combinations of drugs can be tested. Hence, Dr. Wallemcack’s study advised caution when working with lipophilic and low molecular weight cytotoxic agents. Lipophilic or 'lipid-loving' molecules are attracted to lipids. A substance is lipophilic if it is able to dissolve much more easily in lipid (a class of oily organic compounds) than in water, i.e. Taxol, Carmustine, ThioTEPA.
The Federal Drug Agency, Oncology Nurses Society as well as The Canadian Pharmacist Oncology Association recognizes the need to test gloves as per ASTM D6978-05 method.

HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
; A
HE
ALT
H A
ND
SA
FETY
RE
VIE
W
6
Device chamber used for permeation test cell ASTM F-739 within this method 13 Products tested for permeation as per ASTM F-739 often used in the oncology department for disinfecting are: • 70% isopropyl alcohol (IPA) • accelerated hydrogen peroxide (H2O2)
Products for decontamination are: • Hypochlorite sodium (bleach) • Sodium Thiosulfate • Mechloretamine (chlormetine).
INTERPRETING BREAKTHROUGH TIME Breakthrough time will measure how quickly a chemical can permeate a glove. It is specific for glove material type used in the test. Thinner gloves made from the same material will have a shorter break-through time. For tasks with inevitable contact, the breakthrough time is the maximum time the glove may be used before it should be discarded. If the work lasts for longer than the breakthrough time, gloves should be changed part-way through. You should allow a safety margin: stretching of gloves during use may mean that breakthrough occurs more quickly than in a test environment. Do not rely on touch to detect breakthrough. Skin exposure will occur long before any perceptible feeling of wetness on the inner surface of the glove.
It is important to note that: • Permeation results differ in time and average permeation rate. • The risk posed by a chemical permeating a glove is related not just to the speed at which it can diffuse through, but also the flow rate. A combination of a short breakthrough time and a low permeation rate may expose a glove wearer to less chemical than a combination of a longer breakthrough time and a much higher breakthrough rate, if the glove is not changed frequently enough. • Gloves should be changed before permeation occurs. Since permeation breakthrough in actual end use may occur sooner than breakthrough under lab test conditions, a margin of safety should be allowed when specifying glove change intervals based on lab data.
Always check the material safety data sheet (MSDS) for personal protective equipment requirements in selecting gloves specifically for the type of chemicals used. Verify permeation time and rate to choose the right glove. • As per ASTM F-739 in handling cleaning compounds • As per ASTM-D6978-05 in handling chemotherapy drugs
Permeation test chemicals mixed at any other concentrations will cause data to be generated that will give invalid comparisons when matched against data obtained using the standard concentrations.

7
GLOVE SELECTION IN HANDLING CYTOTOXIC DRUGS Informed use of PPE is a very critical component of a hospital’s health and safety program. Appropriate PPE includes gloves, gowns, face shields, masks, eye protection, and ventilation devices where there is likelihood of contact with potentially contaminated material.
When choosing a glove, the first consideration should be the barrier requirement related to the procedure or task at hand. Be aware of the level of exposure risk that the patient-care activities will require. Procedures that involve exposure to blood, bodily fluids, and other potentially hazardous material require a glove material that provides appropriate barrier protection.
When selecting a medical glove, the primary considerations should be the barrier protection, the fit and allergen content. If a glove does not provide an intact barrier, it is not doing its job. To maximize barrier effectiveness, you may wish to choose a glove manufacturer that is reliable and experienced, so that your gloves will be of consistent quality and regularly available.
In handling chemotherapy drugs with the current guidelines on double gloving, insuring a proper fit to the personnel may become a task in itself.
Glove Fit and Sizing
Having protective equipment that fits properly is absolutely vital to the safety of employees. Knowing how to accurately measure and choose glove sizes can increase safety and productivity in the workplace.
If gloves do not fit properly, it can often delay work or result in hand injuries. If the hand protection is too small, it may cause hand fatigue. If the protective material is stretched out, it is more likely to rip or tear during use which is costly to replace, as well as dangerous for the wearer. Gloves that are too small also decrease dexterity. On the other hand, gloves that are too large create safety issues.
It is imperative to understand how to appropriately measure the hand in order to get a glove that fits correctly. If the glove fits properly, it will provide the worker with maximum protection without compromising dexterity.
To find the appropriate glove size, use a tape measure to measure around the knuckles of the dominant hand. The inch measurement of your hand should correspond directly to the numbered sizes of the glove. For example, if you measure your hand to be 8 inches, you would wear a size 8 glove. If your hand measures over 8 inches it is wise to choose the next size up to avoid hand fatigue or discomfort from a glove that is too small. Some gloves come in lettered sizes such as XS, S, M, L, and XL. These can easily convert to a numerical size for simple selection.

HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
; A
HE
ALT
H A
ND
SA
FETY
RE
VIE
W
DOUBLE GLOVINGIs there a proper technique for double gloving? While double gloving sizing depends on individual needs, today three practices are common. Some people find that a larger glove inside with a smaller one outside works for them, or vice versa and others use the same size glove for both inside and outside glove. The aforementioned study published in the European Journal of Cardiothoracic Surgery found almost an equal distribution of glove sizes used by surgeons for double gloving: larger glove inside 31%, smaller glove inside 35% and both gloves the same size 31%.14
Donning and Doffing Gloves
Gloves made of various materials form an important part of our safety practices. End-users rely on gloves to protect their hands against corrosive or toxic chemicals, and potential infectious pathogens. We have repeatedly emphasized the importance of choosing gloves made of material appropriate for the hazardous substance(s) being handled. Users must also consider the level of dexterity needed for the anticipated manipulation.
The vast majority of end-users have developed the habit of putting on gloves for work involving hazardous substances. However, we are now seeing a problem of people not taking off gloves when they really should have done so. Although wearing gloves can prevent skin contact with hazardous chemicals, not taking them off at the right time may actually turn the used gloves into a source of contamination, and increase the risk of hazardous chemical exposure for the wearer and the environment. 15-16
DONNING TECHNIQUES
There are two techniques for donning sterile gloves, "Closed Donning" and "Open Donning".
Closed Donning Technique
1. Peel open the outer pack from the corners. The inner pack is sterile. Gripping it through your gown, open it to display the gloves.
8
Mens WomenInch cm Inch cm
XS 7 18 XS 6 15S 7 1/2-8 20 S 6 1/2 17M 8 1/2-9 23 M 7 18L 9 1/2-10 25 L 7 1/2 19XL 10 1/2-11 28 XL 8 20
See the table for numerical and lettered sizing relation.
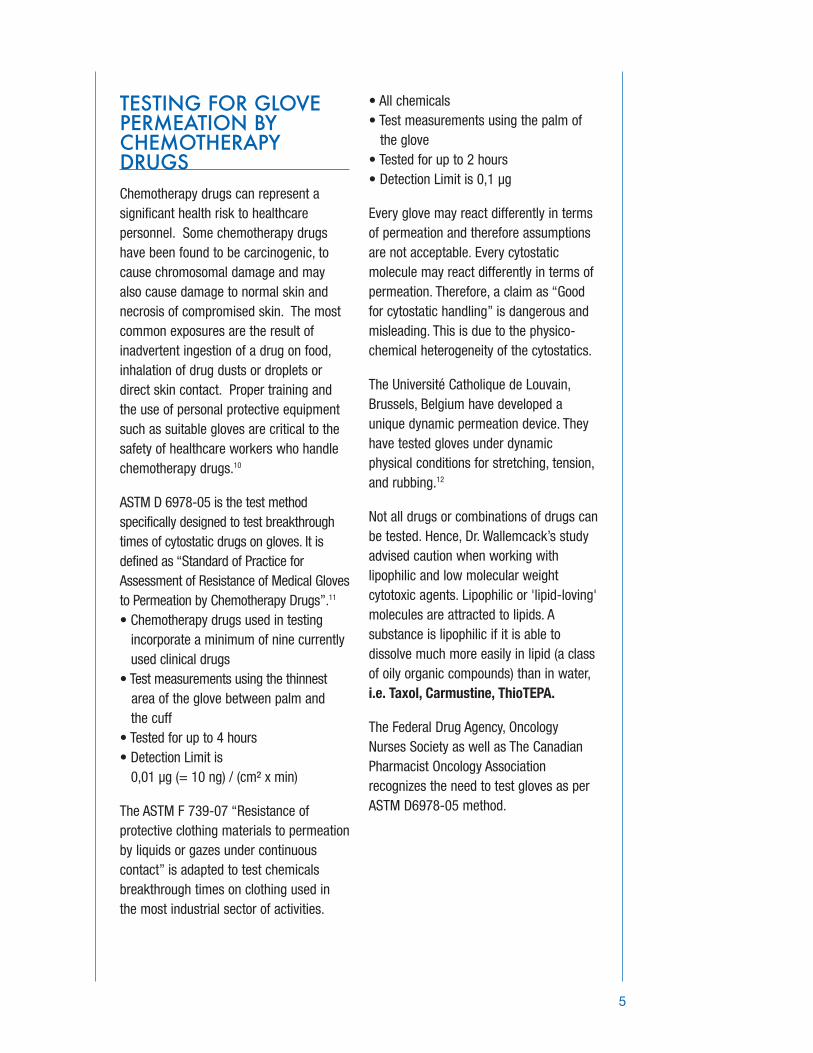
2. With your gown covering your fingers, use your right hand to remove the left glove. Hold your left hand palm up, fingers straight. Lay the glove on your left wrist, and grip the cuff with your left thumb.
3. Place your right thumb inside the top cuff edge. Make a fist with your right hand and stretch the glove over your left fingertips.
4. Keeping your left fingers straight, pull down the glove.
5. Repeat the above procedure to don the other glove, that is: use your gloved left hand to lay the right glove on your right wrist. Slide your left thumb inside the top of the cuff, make a fist, and stretch the cuff over your right fingertips. Pull down the sleeve and glove together.
Open Donning Technique
1. Pick up the cuff of the right glove with your left hand. Slide your right hand into the glove until you have a snug fit over the thumb joint and knuckles. Your bare left
hand should only touch the folded cuff - the rest of the glove remains sterile.
2. Slide your right fingertips into the folded cuff of the left glove. Pull out the glove and fit your right hand into it.
3. Unfold the cuffs down over your gown sleeves. Make sure your gloved fingertips do not touch your bare forearms or wrists.
Glove Removal
The key to removing both sterile and non-sterile gloves is
"Dirty to Dirty - Clean to Clean"
Contaminated surfaces only touch other contaminated surfaces: your bare hand, which is clean, touches only clean areas inside the other glove.
1. Take hold of the first glove at the wrist.
9

HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
; A
HE
ALT
H A
ND
SA
FETY
RE
VIE
W
2. Fold it over and peel it back, turning it inside out as it goes. Once the glove is off, hold it with your gloved hand.
3. To remove the other glove, place your bare fingers inside the cuff without touching the glove exterior. Peel the glove off from the inside, turning it inside out as it goes. Use it to envelope the other glove.
REMOVING EXAMINATION GLOVES SAFELY
As you remove the gloves, avoid allowing the outside surface of the gloves to come in contact with your skin, because the outer surface may have become contaminated. Avoid letting gloves snap, as this may cause contaminants to fly into your eyes or mouth or onto your skin or other people in the area. Remove used gloves before touching anything. Counter tops, faucets, pens and pencils are often contaminated because workers wearing gloves touch them.
The following is a common way of safely removing gloves.
1. With right hand, pinch palm of glove on left hand and pull left glove down and off fingers. Form left glove into a ball and hold in fist of right hand.
2. Insert one or two fingers of left ungloved hand under inside rim of right glove on palm side; push glove inside out and down onto fingers and over balled left glove.
10

3. Grasp gloves, which are now together and inside out, with left hand and remove from right hand. 4. Discard gloves in plastic bag and seal bag.
5. Wash hands thoroughly.
GLOVE RECOMMENDATIONS IN HANDLING CYTOTOXIC DRUGS
• Powder-free neoprene and nitrile examination gloves tested for D6978-05 are the best recommended choices during all activities around handling chemotherapy drugs as they also have better resistance to disinfecting and decontamination products than latex. • Surgical neoprene, nitrile, natural rubber, and polyisoprene gloves, tested using ASTM D-6978-05, are recommended when preparing and handling chemotherapy drugs. Please use a glove rated for the handling of specific chemotherapy drugs. • Polyvinyl chloride (PVC) gloves are NOT recommended for handling chemotherapy drugs. • Always use powder-free gloves. The dispersing of chemotherapy drugs into the surrounding air and the possibility of inhalation is a serious matter and should be treated as such. Also, glove powders may contaminate chemotherapy work areas. • If double gloving, insert first glove under the cuff and place the second glove over the cuff. If single gloving, place the
clean glove over the cuff of the gown. • Before handling chemotherapy drugs, always inspect gloves for holes, tears or any type of defect. Unless the film is intact, it cannot provide a barrier. • Although surgical gloves are recommended for preparation, administration, clean up and general handling, sterility is not always required, as for example, direct patient care, handling laundry, and housekeeping procedures.17 Gloves are available in non-sterile presentations for these purposes.
DRUG PREPARATION
Working Securely with Cytostatics
As the number of cancer patients rises, so does the use of chemotherapy treatment. While effective in treating disease, these drugs are also potentially hazardous for the oncology nurses, pharmacists and other healthcare professionals who handle them. Yet worldwide research indicates that insufficient care is being taken with cytostatic agents. Studies report widespread, low-level contamination of areas where cytostatic drugs are used. Traces of cytostatic drugs have been found on workbenches, floors, vials and exterior surfaces of safety cabinets and isolators – even on the floor outside preparation rooms. Once contamination with cytostatic drugs has occurred it is extremely difficult to eradicate.18
To better protect healthcare workers, heightened awareness of this serious problem must be combined with both improved cytostatic handling procedures and the use of appropriate hand protection. Here is a step by step guide to the safe preparation and administration of
11
HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
; A
HE
ALT
H A
ND
SA
FETY
RE
VIE
W
cytostatic mixtures, as well as recommendations for suitable hand protection.
Before actually preparing the cytostatic mixture, the following activities have been identified. These may be influenced by ruling protocols • Don special protective clothing including non-sterile examination gloves. [Photo 1] • Unpack all material. During the unpacking or handling of the vials, the healthcare worker’s hand should be protected as the outside surface of the vials might be contaminated with cytostatic drugs. [Photo 2] • Disinfect the work area. [Photo 3, 4] • Assemble and disinfect all material necessary to prepare the cytostatic drugs. [Photo 5, 6, 7]
Similar care should be taken in the Similar
Similar care should be taken in the preparation, administration and disposal of chemotherapy drugs. In addition to healthcare professionals, patients and persons that are directly involved in home care should also be taught these safety standards and guidelines. • Always wear gloves when handling the drug. • Avoid touching the drug. • Wash hands before putting gloves on and after wearing gloves. • Gloves used for protection against chemotherapy drugs must be selected. specifically for the type of chemicals used. • Use medical grade, sterile or non-sterile, gloves depending on the technique recommended by your healthcare facility. • Always use powder-free gloves. - Glove powders may contaminate chemotherapy work area. • Choose a natural rubber latex, nitrile or neoprene glove - Polyvinyl chloride (PVC) gloves are not recommended for handling chemotherapy drugs. • Use ASTM D6978-05 tested gloves that extend over the cuff of the protective gown. Please use a glove rated for the handling of the specific chemotherapy drugs. • Double gloving is strongly advised when there is a risk of exposure during preparation or administration of chemotherapy drugs.
12

- If double gloving, insert first glove under the cuff and place the second glove over the cuff. • Before handling chemotherapy drugs - Observe gloves for any break in barrier. - Change gloves after each use, tear, and puncture or medication spill or after 30 minutes of wear. • Upon removal, both gloves need to be turned inside out • Never flick, snap, or toss your gloves. • Follow recommendations implemented by your healthcare facility for the disposal of gloves.
Now you are ready for the reconstitution of the cytostatic mixture and transfer it to the perfusion set. • Don sterile gloves. [Photo 8, 9, 10, 11] • Disinfection of procedure material. [Photo 12] • Reconstitution of the cystostatic mixture. [Photo 13, 14, 15, 16] and, [Photo 17, 18, 19, 20] • Perform a final disinfection of end product. [Photo 21, 22] • Pack the product and label it. [Photo 23, 24]
13

HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
; A
HE
ALT
H A
ND
SA
FETY
RE
VIE
W
ADMINISTERING CYTOSTATICS TO PATIENTS
Once the cytostatic mixture has been prepared, it is administered to the patient following established guidelines. (Photo 25, 26)
Drug Administration; Glove Use Recommendation • Inspect glove for visible defects. • Wear high quality gloves that have been tested for use with the specific chemotherapy drugs to be used. • Double gloving is recommended. • Wash hands before putting on gloves. • Change contaminated gloves immediately. • Wash hands after removing gloves. • Dispose of gloves according to proper hospital toxic waste procedures.
Drug Clean Up and General Handling • Wear high quality gloves that have been tested for use with chemotherapy drugs when dealing with blood, vomitus, excreta and other bodily fluids from chemotherapy treated patients. • Discard gloves after each use. • Laundry personnel coming into contact with linen contaminated with chemotherapy drug patients’ body fluids should wear high quality gloves that have been tested for use with chemotherapy drugs. • Housekeeping personnel should wear high quality gloves that have been tested for use with chemotherapy drugs when handling waste containers. • Spills should only be cleaned up by personnel wearing a double layer of gloves. • Spill kits for use in responding to spills should include two (2) pairs of gloves; one outer pair of utility gloves and one inner pair of latex or synthetic gloves. • All personnel involved in any aspect of handling chemotherapy drugs must receive an orientation on chemotherapy drugs including proper use of protective equipment.
14
Summary of Glove Use
15
AREAS OF GLOVE USE
Open packagingStorageSterile drug preparationIntramuscular or subcutaneous injectionsIntravenous drug administrationPercutaneous drug administration Oral and nasal enteral tube drug administration Intraocular drug administrationGarbage disposalPost drug delivery patient care delivery - 2 daysPatient careSpillsCleanroom housekeepingCabinet cleaningDepartemental housekeepingHandling linen
HA
ND
LIN
G C
YTO
TOX
IC D
RU
GS
; A
HE
ALT
H A
ND
SA
FETY
RE
VIE
W
16
REFERENCES
1 http://www.who.int/gho/publications/world_health_statistics/EN_WHS2012_Full.pdf
2 American Society of health system pharmacists,2006.ASHP guidelines on handling hazardous drugs, American journal of health system Pharmacists, 63,1172-1193
3 Occupational health and safety Administration(1999) OSHA technical manual, Categorization of drugs as hazardous retrieved from http://www.osha.gov/dts/osta/otm_vi/otm_vi_2.htlm#2
4 Polovich M Ed. (2011) Safe handling of hazardous drugs (2nd ed.) Pittsburg, PA: Oncology Nursing Society.
5 Occupational health and safety Administration(1999) OSHA technical manual, Categorization of drugs as hazardous retrieved from http://www.osha.gov/dts/osta/otm_vi/otm_vi_2.htlm#2
6 http://monographs.iarc.fr/ENG/Classification/index.php
7 Polovich M Ed. (2011) Safe handling of hazardous drugs (2nd ed.) Pittsburg, PA: Oncology Nursing Society.
8 FDA Medical Glove guidance manual (2008) pg. 22-23
9 Polovich M Ed. (2011) Safe handling of hazardous drugs (2nd ed.) Pittsburg, PA: Oncology Nursing Society.
10 National Institute for Occupational safety and health (2004) Preventing occupational exposure to antineoplastic and other hazardous drugs in health care settings. Retrieved from http://www.cdc.gov/niosh/docs/2004-165
11 American safety and testing method; ASTM D-6978-05 “Practice for Assessment of Resistance of Medical Gloves to Permeation by Chemotherapy Drugs” (2005)
12 P.Wallemacq, PhD et al. Permeation of 13 cytotoxic agents through 13 different gloves under controlled dynamic conditions, AJHP March 15, 2006 Vol. 63, # 6 pg. 547-56
13 Ansell 8th edition Chemical resistance guide, Permeation and degradation data pg4
14 Hollaus PH, et al. Glove perforation rate in open lung surgery. European Journal of CardioThoracic Surgery. 1999; 15:461-464

3
15 Fransman,W.,Vermeulen,R.,Kromhout, H., Occupational dermal exposure to cyclophosphamide in Dutch hospital: a Pilot study. Annals of Occupational Hygiene (2004) 48,237-44
16 Fransman,W.,Vermeulen,R., Kromhout, H., Dermal exposure to cyclophosphamide in hospitals during preparation, nursing and cleaning activities. International Archives of Occupational and Environmental Health (2005) 78, 403-12
17 Occupational safety and health Administration (2002) Guidelines for laundry in health care facilities retrieved from http//www.osha.gov/od/ohs/otm_vi.2.htlm
18 By Celeste Caskey, Daniel J. Hurley, Raymond R. Liguori, Assessing environmental contamination by cytoxic drugs ; Chemical Health & Safety, September/October 2005; 26-28
17